-
BA O
R ma eaTa An imAlb , P Ign
OB te tG-p rialate tie
ST einrec ctdom coG-p patttiss whifen
RE tedvat life
teintionhe-p
liertrial
-cod en
PR
Cite A, e tam201
Ephanand pathophysiologic actions of estro-gen(ERtheily2
tracl
thesigofinoulation.3,4 Very recently, an orphan G-
f e 5
haeffl a
moredndcerlecM
an
breGPgroofEGF).13,14 Very recently, we have found
has been also shown that GPR30 mediates
and to compare it with a tamoxifen nave
FroGyBisOtGeRoUnIIN
SemLu
Re201
Re
Thi108
000 2doi
Research www.AJOG.orgnistic effect in breast cancer, it acts as
anestrogen agonist in the uterus.9 This ago-nistic effect of
tamoxifen can stimulate cellgrowth and proliferation in
endometrialtissue, enhancing the risk of
endometrialabnormalities,includingendometrialcarci-noma.10,11
Interestingly, the classic ER an-tagonists tamoxifen and
fulvestrant act asagonists for GPR3012 and stimulate cell
cohort. The role of GPR30 for tamoxifen-induced endometrial
abnormalities wasconfirmed in vitro, using endometrial car-cinoma
cell line.
MATERIALS AND METHODSMaterialsAll chemicals and antibiotics for
a cell
czuk), Lublin Medical University,blin, Poland.
ceived March 26, 2010; revised June 19,0; accepted July 21,
2010.
prints not available from the authors.
s study was supported in part by Grant931 from Deutsche
Krebshilfe.
2-9378/$36.00010 Published by Mosby, Inc.and function as
hormone-induciblenscription factors. In addition to thisassic or
genomic effect of estrogen,
nongenomic effects obeen demonstrated tates the proliferativein
breast, endometriacer cells (review6).
Breast cancer is thecer in women and is pgen-dependent.7 The eof
choice for breast canpatients remains the seceptor modulator
(SERthough tamoxifen has
m the Department of Obstetrics andnecology (Drs Ignatov,
Eggemann,choff, Costa, Ignatov, and Mr Smith),to-von-Guericke
University, Magdeburg,rmany; Department of Pathology (Drsessner and
Kalinski), Otto-von-Guerickeiversity, Magdeburg, Germany; and theD
Department of Gynecology (Drproliferation and growth:
10.1016/j.ajog.2010.07.034
Dstrogen. It hast GPR30 medi-ects of estrogennd ovarian can-
st common can-ominantly estro-ocrine treatmentpremenopausal
tive estrogen-re-) tamoxifen.8 Al-estrogen antago-
the tamoxifen stimulatory effects in endo-metrial carcinoma
cells in vitro14,16 and ishighly expressed in endometrial
carci-noma with poor prognosis.17
In this regard, the activation of GPR30may be a possible
mechanism leading toendometrial abnormalities in breast can-cer
patients after tamoxifen treatment. Weare the first to describe the
distribution ofGPR30 in endometrial tissue of patientstreated with
tamoxifen for breast cancerare mediated by 2 estrogen receptorss),
ER and ER, which belong tosteroid hormone receptor superfam-
protein-coupled receptor, GPR30, wasclaimed to be a new
membrane-boundestrogen receptor involved in the rapid
that GPR30/EGFR crosstalk is an impor-tant component of
tamoxifen agonistic ac-tivity in breast cancer cells.15 Moreover,
itSIC SCIENCE: GYNECOL
ole of GPR30 in endofter tamoxifen for brnja Ignatov, MD; Holm
Eggemann, MD;ert Roessner, MD; Serban D. Costa, MD
JECTIVE: This study was undertaken to evaluarotein-coupled
estrogen receptor in endometd with tamoxifen treatment of breast
cancer pa
UDY DESIGN: We investigated whether G-proteptor plays a role in
mediating proliferating effeetrial carcinoma cells. These results
wererotein-coupled estrogen receptor expressionue from a cohort of
95 breast cancer patients,or another adjuvant therapy.
SULTS: In vitro tamoxifen significantly stimulaed protein kinase
phosphorylation and cell pro
this article as: Ignatov T, Eggemann H,
Semczuk0;203:595.e9-16.
strogens are key regulators of differ-ent cellular processes
involved in the
ysiology of female reproductive tractd mammary gland.1 The
physiologicGY
etrial pathologyst cancer
drzej Semczuk, MD; Bobbie Smith; JoachhD; Thomas Kalinski, MD,
PhD; Atanas
he potential role ofpathology associ-nts.
-coupled estrogenof tamoxifen in en-mpared with theern in
endometrialo received tamox-
the mitogen-acti-ration of endome-
trial cell lines via G-prowas a significant correlaceptor
expression and t(P .006). Moreover, Gwas predictive of an earing or
suspect endome(P .019).
CONCLUSION: G-proteinrole in tamoxifen-induce
Key words: estrogen, G
t al. Role of GPR30 in endometrial pathology after
re are some rapid or nonclassicnaling effects, including
stimulationphospholipase C, cAMP, calcium,sitol phosphate, and ERK
upreg-. Particularly in cu
ECEMBER 2010 AmericanBischoff, MD;atov, MD
-coupled estrogen receptor. In vivo, therebetween
G-protein-coupled estrogen re-
tamoxifen-induced endometrial pathologyrotein-coupled estrogen
receptor positivitydevelopment of symptoms, such as
bleed-thickness, induced by tamoxifen therapy
upled estrogen receptor plays an importantdometrial
abnormalities.
30, tamoxifen
oxifen for breast cancer. Am J Obstet Gynecol
ast and endometrial cancer cells,R30 activates the human
epidermalwth factor receptor (EGFR) via releaseheparin-bound growth
factor (HB-lture, 4-OH-tamoxifen and 17--es-
Journal of Obstetrics& Gynecology 595.e9
-
traAldagochaniestiblatSigMedriwelanrea(K
CeHu(HcanVADMrum10the6-wpetamcelmestrThwitherincouscrcelifetotimcelaftolitro
ExanFowalinGPTT0.2CAper
fecThaftknblo
WeProproousamanbrawicu(RlutMAlutanwamistronha(Inlecnesfiedimgen
PaWevoteepri199steof
MthelinThgroifentierecgersusserpatoptriaTh22
memoGrnoifenfromesymthiweexapathyiantamdevectdedfiedendantria
Cagnfacobcal
ImImasofdethiglamamamaThpudilter(Vwedincoucovmo
EvimGPinthesho
Research Basic Science: Gynecology www.AJOG.org
59diol (E2), were obtained from Sigma-rich (Steinheim, Germany).
GPR30nist G1 was obtained from Calbio-
em (Darmstadt, Germany). GPR30tibody was purchased from
Antibod--online (Aachen, Germany). The an-odies against total and
phosphory-ed MAPK and -actin were from Cellnaling (Frankfurt am
Main, Germany).dium was obtained from Sigma-Al-ch. GPR30 antisense
oligonucleotidesre purchased from MWG-Medical (Mi-, Italy).
Lipofectamin 2000 transfectiongent was obtained from
Invitrogenarlsruhe, Germany).
ll cultureman endometrial carcinoma cellsEC-1A) were obtained
from Ameri-
Type Culture Collection (Manassas,). They were routinely
cultured inEM/F12 containing 5% fetal-calf se-
(FCS), 100 U/mL penicillin and0g/mL streptomycin. To perform
experiments, the cells were seeded inell plates at a density of
60,000 cells
r well. To test the effect of estradiol,oxifen and GPR30 agonist
G1, the
ls were treated with phenol red-freedium supplemented with
charcoal-ipped FCS 48 hours before the assay.en, cells were
incubated for 5 daysth 10 nM E2, 1 nM G1, and 100 nM. At
end of the treatment, the cells weresed twice with saline
solution andnted using a Coulter counter as de-
ibed.18 After treatment of HEC-1Als for 10 minutes with 100 nM
tamox-n, the phospho-MAPK (pMAPK) andal-MAPK (tMAPK) were detected
bymunoblotting. Furthermore, HEC-1Als were treated with 100 nM
tamoxifener transfection with GPR30 antisensegonucleotides
(GPR30/AS) or with con-l scrambled oligonucleotides (Con/AS).
periments with GPR30tisense oligonucleotidesr these experiments,
the cells wereshed twice in phosphate-buffered sa-e, then
transfected with 0.2 MR30 antisense oligonucleotide
(5=-GGGAAGTCACATCCAT-3=) or withM random control
(5=-GATCTCAG-CGGCAAAT-3=). The transfection was
formed with Lipofectamine 2000 trans- ifen
5.e10 American Journal of Obstetrics& Gynecologtion reagent
as previously described.19
e experiments were performed 24 hourser transfection. The
efficacy of GPR30ocking down was detected by Westerntting.
stern blottingtein cell lysis and Western blottingcedures were
performed as previ-
sly described.15 Briefly, 25 L of theples were separated by
SDS-PAGE
d blotted onto nitrocellulose mem-nes. The membranes were
blocked
th 3% dry milk in TBS/Tween and in-bated for 2 hours at room
temperatureT) with antibodies against GPR30, di-ed 1:1000, total or
phosphorylatedPK diluted 1: 2000, and -actin di-
ed 1:10000. A peroxidase-conjugatedtirabbit antibody, diluted
1:10,000,s used for a second incubation (30nutes). West Pico
Supersignal sub-ate (Perbio, Bonn, Germany) was leftthe membrane
until distinct bands
d developed. A MagicMark standardvitrogen) was used to identify
the mo-ular weights. The enhanced chemilumi-cence membrane images
were quanti-using the GeneGnome and GeneTools
age scanning and analysis package (Syn-e, Cambridge, UK).
tients and study designobtained ethical approval from Otto-
n-Guericke University Ethic Commit-. The study included 95
patients withmary breast cancer diagnosed between9 and 2004 in the
Department of Ob-
trics and Gynecology, University Schooledicine, Magdeburg,
Germany, and in
IInd Department of Gynecology, Lub-Medical University, Lublin,
Poland.
ey were classified into a tamoxifenup and 2 control groups. The
tamox-
group (group I) consisted of 48 pa-nts with ER-positive breast
cancer whoeived daily tamoxifen after breast sur-y and in whom
vaginal bleeding and/orpicious endometrial thickness was ob-ved at
the periodic checkup. All theseients had undergone endometrial
bi-sy. A biopsy was performed if endome-l thickness of5 mm was
determined.e first control group (group II) includedpatients who
also receive daily tamox-
, but did not have symptoms or endo- the
y DECEMBER 2010trial abnormalities. The daily dose of ta-xifen
for both groups was 20 mg.
oup III consisted of 25 patients who didt receive adjuvant
therapy with tamox-. The time to symptoms was calculated
m the beginning of tamoxifen treat-nt to the first time the
patients reportedptoms or suspicious endometrial
cknesswasobserved.Allpatientsunder-nt a periodic checkup with
gynecologicmination, followed by ultrasound. Theients in the
control groups underwent a
sterectomy because of prolapses,
ovar-,pelvic,orotherpathologynot linkedtooxifen therapy.
Endometrial tissueeloped from the curettages and hyster-
omieswasfixedinformalinandembed-in paraffin. The histology was
classi-as follows: normal/atrophic (inactive)ometrium, endometrial
hyperplasia
d/or endometrial polyp, and endome-l carcinoma.linicopathologic
data regarding di-osis and treatment, epidemiologic
tors, as well as follow-up data, weretained retrospectively from
the clini-records or the local physicians.
munohistochemistrymunohistochemistry was performedalready
described.20 Briefly, sectionsformalin-fixed and
paraffin-embed-
d breast cancer specimens (3.0 mck) were mounted on SuperFrost
Plusss slides (Menzel, Braunschweig, Ger-ny) and dried overnight. A
Bench-rk XT (Ventana, Unterhaching, Ger-ny) conducted the
immunostaining.e slides were incubated with affinity-rified rabbit
antibody against GPR30uted 1:500 for 32 minutes at 37C, af-
antigen retrieval with Protease Ientana) for 10 minutes. The
reactionsre visualized by 5,5==-di-aminobenzi-e (DAB) detection.
The slides werenterstained with hematoxylin anderslipped after
being embedded inunting medium.
aluation of GPR30munoreactivityR30 immunoreactivity was
detectedthe cytoplasm and in the nucleus of
cells. Some endometrial tissueswed clear GPR30 staining pattern
in
cytoplasm and weak expression in
-
thedenutheinmiobexpwitersififoltenitiv(ten(windgivIRGP
FI d E
A aimmof nmaER,
Igna
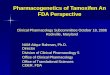
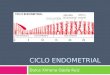
www.AJOG.org Basic Science: Gynecology Researchnucleus (Figure
1), whereas othersmonstrated higher expression in thecleus. In
contrast, the expression ofclassical ER was detected
exclusively
the nucleus. No detectable cytoplas-c or plasma membrane
staining wasserved for ER (Figure 1). The GPR30ression was
classified in accordance
th the dominant immunostaining pat-n. GPR30 immunoreactivity was
clas-ed as already described15,21 using thelowing grading system:
staining ex-sity was categorized as 1 (10% pos-e cells), 2 (10-50%
positive cells), or 350% positive cells), and staining in-sity was
categorized as 0 (negative), 1eak), 2 (moderate), or 3 (strong).
Theividual categories were multiplied toe a total immunoreactive
score (IRS).S scores ranged between 0 and 9.
IGURE 1mmunohistochemistry for GPR30 an
nd B, Example of moderate nuclear staining of Gunoreactivity is
moderately detected in both cytegative expression of GPR30 in the
nucleus comgnification 100; B, D, F, H, J, L: original maestrogen
receptors; GPR30, G-protein-coupled receptor.
tov. GPR30 and tamoxifen-induced endometrial pathology.R30
expression was classified as fol- sens: negative (IRS between 0 and
2), lowde (IRS 35), and high grade (IRS6-9). GPR30 protein
expression wasided into 3 categories: negative, when0% of the cells
showed negative orderate staining intensity; low grade,en 10-50% of
the cells demonstratedderate staining; high grade, when0% showed
strongly positive cells.
tistical analysise statistical calculations were performedng
SPSS version 13.0 (SPSS, Chicago,. Association between GPR30
expres-n and the tamoxifen-induced endome-l pathologies was
evaluated usinghers exact test or the 2 test. The inter-between the
start of tamoxifen treat-nt and the diagnosis of bleeding
and/orpicious endometrial thickness was cho-
R in endometrial tissue
0 with negative cytoplasmic staining and C and Dsm and nucleus
with G and H, moderate immund with moderate cytoplasmic staining
and K andcation 400.
J Obstet Gynecol 2010.as endpoint of the study. The associa-
ou
DECEMBER 2010 American Jn between GPR30 expression and theerval
was calculated by the Kaplan-ier survival method, and the equality
ofvival curves was tested by the log rankt. For paired
observations, statisticalalysis was carried out using Student tt.
Curve fittings were performed withsm program (GraphPad Software,
Sanego, CA). The results are expressed asans of 6 determinations
standard de-tion (SD). Results were considered sta-ically
significant if thePvalue was .05.
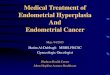
SULTS, G1, and tamoxifen stimulate cellwth and MAPK
phosphorylationendometrial cellse first examined the effects of
E2,R30 agonist G1, and the selective ERdulator tamoxifen on cell
growth. In
clear immunostaining of ER. E and F, GPR30activity of ER in the
nucleus. I and J, Exampleuclear ER expression. A, C, E, G, I, K:
originallowgradiv1mowhmo5
StaThusiIL)siotriaFisvalmesus
tiointMesurtesantesPriDimeviatist
REE2groinWGPmo
PR3 , nuopla orebine L, ngnifi
Amr set of experiments, all 3 tested sub-
ournal of Obstetrics& Gynecology 595.e11
-
stagrostrserG1
foranascreinccom(FiMA
TarevTomolifeweanoliThGPgaturesigenknanblogetmeprotri
EninWbutamogsamatibreuseanbume62groanmemotiewitieifeadme
FC ox
A,redCousepPhoantIgna
Research Basic Science: Gynecology www.AJOG.org
59nces significantly stimulated cellwth in HEC-1A (Figure 2, A).
The
ongest proliferation effect was ob-ved with E2. However, the
fact that
IGURE 2ell growth effects of E2, G1 and tam
HEC-1A cells were treated for 5 days with 10 nM-free medium
containing 5% charcoal-strippedlter counter. The experiments were
repeatedarate measurements SD. B, HEC-1A cells wespho-MAPK (pMAPK)
and total-MAPK (tMAPK)ibodies. Total MAPK was used as loading
controtov. GPR30 and tamoxifen-induced endometrial pathology., as a
highly specific agonist for in
5.e12 American Journal of Obstetrics& GynecologR30,
increased cell growth suggestedPR30-mediated cell proliferation.hen
we examined the effects of these
ubstances on MAPK phosphorylation
ifen in endometrial cancer cells
, 1 nM G1, and 100 nM tamoxifen in phenoll calf serum. The cells
were counted using aeast 3 times. Each data point is mean of 6eated
for 10 minutes with 100 nM tamoxifen.e detected by immunoblotting
using specificnormalize the pMAPK expression.J Obstet Gynecol
2010.HEC-1A cells. The cells were treated inh
y DECEMBER 201010 minutes with 10 nM E2, 1 nM G1,d 100 nM
tamoxifen or with mediuma control. There was a significant in-ase
in MAPK phosphorylation afterubation with all three substances
pared with the negative controlgure 2, B), whereas the level of
totalPK remained unchanged.
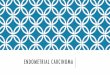
moxifen-induced cell growth isersed by knocking down
GPR30investigate the role of GPR30 in ta-xifen-induced endometrial
cell pro-ration in more detail, HEC-1A cellsre transfected with
GPR30-specifictisense oligonucleotides. Scrambledgonucleotides were
used as a control.e transfection of HEC-1A cells withR30 antisense
oligonucleotide abro-ed their response to tamoxifen (Fig-3, A),
suggesting that GPR30 takes a
nificant part in tamoxifen-induceddometrial cell proliferation.
GPR30ockdown and the specificity of GPR30tibody were confirmed by
Westernt analysis (Figure 3, B). Taken to-her, all these data
suggest an involve-nt of GPR30 signaling pathway in thecess of
tamoxifen-induced endome-
al proliferation in vitro.
dometrial pathologythe study groupe wanted to further analyze
the contri-tion of GPR30 to the development of
oxifen-induced endometrial pathol-y. For this purpose, we used
tissue
ples of patients who were symptom-c during tamoxifen treatment
forast cancer. As negative control, wed samples from women who
received
other adjuvant therapy or tamoxifent never developed symptoms.
Thean age of the whole study group was
.02 14.1 years, 54.94 12.8 years forup I, 71.73 10.9 years for
group II,
d 67.08 11.6 years for group III. Thedian follow up of the study
was 42nths (range, 577 months). All 95 pa-
nts received primary breast surgeryth or without radiotherapy.
The pa-nts in group I and II received tamox-n with or without
chemotherapy asjuvant treatment. The adjuvant treat-nt of group III
consisted of aromataseGPa G
T3 s
E2fetaat lre trwerl toAmibitor (n 17) or no hormonal treat-
-
methebeanciomo
Tdia
moseren
GPanenThspeshowhdemunifipreenofinGPmeIndeGPsiggrocasgrapo(40tiosultamog
Msitybeanabwimemewa[CGP(95nifisymthesiotamme(95increvfre
FG ucp
A,antwereptrancleGPR
Igna
www.AJOG.org Basic Science: Gynecology Researchnt (n 8) with or
without chemo-rapy. In group I, the median duration
tween the start of tamoxifen treatmentd the vaginal bleeding
and/or suspi-us endometrial sonography was 27nths (range, 559
months).he most common histopathologic
IGURE 3PR30 is important for tamoxifen-indroliferation in
endometrial cells
HEC-1A cells were treated with 100 nM tamoisense
oligonucleotides (GPR30/AS) or with contrre counted on day 5. Cells
treated only with mresents the mean SD of 6 independent meassfected
with GPR30 antisense oligonucleotidesotides (Con/AS) was detected
using immunoblot30, G-protein-coupled receptor.
tov. GPR30 and tamoxifen-induced endometrial pathology.gnosis in
the whole study population whs normal or atrophic endometrium
incases, followed by endometrial hyper-sia in 36 cases, endometrial
polyps incases and endometrial carcinoma in 1e (Table 1). The most
cases of endo-trial hyperplasia and polyps were ob-ved in group I
and II, namely, patients
ed
after transfection of the cells with GPR30crambled
oligonucleotides (Con/AS). The cellsium were used as control. Each
data pointments. B, GPR30 expression in HEC-1A cellsR30/AS) or with
control scrambled oligonu-. -actin used as loading control.
J Obstet Gynecol 2010.o received tamoxifen therapy. The exp
DECEMBER 2010 American Jst common histologic diagnosis ob-ved in
group III was normal/atrophicdometrium.
R30 protein expressiond tamoxifen-induceddometrial
abnormalitiesirty-eight (40.0%) of the investigatedcimens were
negative, 30 (31.6%)wed low-grade protein expression,ereas the rest
of 27 (28.4%) cases
monstrated high-grade GPR30 im-norectivity (Table 2). There was
a sig-cant relationship between GPR30 ex-ssion and the
tamoxifen-induced
dometrial pathology (P .006). In 2227 (81.5%) cases with high
grade and18 of 30 (60.0%) cases with low-gradeR30 expression, an
abnormal endo-trial histology was observed (Table 2).contrast,
endometrial pathology was
tected only in 13 of 38 (34.2%)R30-negative slides. The staining
wasnificantly stronger in the tamoxifenup (group I), where 38 of 48
(79.2%)es were GPR30 positive, high or lowde. In groups II and III,
the GPR30sitivity was observed in 9 of 22.9%) and in 10 of 25
(40.0%) sec-
ns, respectively (Table 3). These re-ts suggested involvement of
GPR30 inoxifen-induced endometrial pathol-
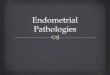
y in breast cancer patients.oreover, GPR30 expression inten-
correlated significantly with the timetween the start of
tamoxifen treatmentd the development of an endometrialnormality
(Figure 4). For the patientsth high-grade GPR30 expression thedian
duration of the tamoxifen treat-nt to the presenting of the
symptomss 27 months (95% confidence intervalI], 2331 months) and
for low-gradeR30 expression, it was 33 months% CI, 1353 months).
This was a sig-cantly shorter (P .019) period untilptoms developed,
compared withcases with negative GPR30 expres-
n. In this cases, the mean duration ofoxifen treatment until the
develop-
nt of symptomology was 59 months% CI, 46 66 months) (Figure 4).
Anrease in GPR30 expression grade wasersely associated with the
symptom-e time length of adjuvant tamoxifenwa42pla16casmeser
xifenol sed
ure(GPting
Amosure in breast cancer patients.
ournal of Obstetrics& Gynecology 595.e13
-
COIntiotamtrifirmbretam
LshocananbreThoftSinal2
uteagodeasencre
theagoful
UHEmoGPtiostimpotivReinenpustrSmtiosiocintheGPmepalatthetho
pretiss
Hciatrinifienwifoubeunifeis tlevmecana rbean
Tityverprefouplaredpamoposomsig
TD in
Hen
N. .........
E. .........
E. .........
E. .........
T %). .........
I gy. A
TAa
Ge
G(.
G(.
G(.
PG
Ip
iff
.........
.........
.........
Research Basic Science: Gynecology www.AJOG.org
59MMENTthe current study, we provided addi-nal evidence of the
role of GPR30 in
oxifen-agonistic activity in endome-al cell lines and, for the
first time, con-
ed them in endometrial tissue fromast cancer patients treated
withoxifen.arger epidemiological studies havewn that tamoxifen not
only signifi-tly reduces breast cancer recurrence
d mortality rate,22 but also preventsast cancer in high-risk
populations.9
erefore, tamoxifen is 1 of the mosten prescribed antineoplastic
drugs.ce the initial report of Fornander at
3 many works have shown that in therus, tamoxifen is
characterized withnistic properties and increased inci-
nce of endometrial abnormalities suchpolyps, endometrial
hyperplasia, anddometrial carcinoma.10,11 This risk in-ased with
the duration of tamoxifen
ABLE 1istribution of endometrial histology
istologyTamoxifGroup I
ormal/atrophic endometrium
3.........................................................................................................................
ndometrial hyperplasia
29.........................................................................................................................
ndometrial polyp
15.........................................................................................................................
ndometrial carcinoma
1.........................................................................................................................
otal 48
(50.5.........................................................................................................................
gnatov. GPR30 and tamoxifen-induced endometrial patholo
ABLE 2ssociation of GPR30 expressionnd endometrial
abnormalities
PR30xpression
Endometrial histology
Normaln (%)
Abnormaln (%)
PR30 negn 38)
25 (65.8) 13 (34.2)
..........................................................................................................
PR30 lown 30)
12 (40.0) 18 (60.0)
..........................................................................................................
PR30 highn 27)
5 (15.5) 12 (81.5)
..........................................................................................................
.006.PR30, G-protein-coupled receptor.
gnatov. GPR30 and tamoxifen-induced endometrial
athology. Am J Obstet Gynecol 2010. I
5.e14 American Journal of Obstetrics& Gynecolograpy. The
mechanism of tamoxifennistic activity in endometrium is not
ly understood.sing human endometrial carcinoma
C-1A cells, we demonstrated that ta-xifen can induce cell growth
in aR30-dependent manner. After activa-n by tamoxifen, GPR30 leads
to
ulation of cell proliferation, moressibly by crosstalks with
EGFR and ac-ation of MAPK phosphorylation.13,15
cently, 2 studies on the role of GPR30tamoxifen-induced
proliferation in
dometrial carcinoma cells have beenblished.14,16 These works
demon-ated results similar to ours. Recently,ith et al17 found a
significant correla-n between GPR30 and EGFR expres-n in 47
patients with endometrial car-oma, providing further evidence
of
potential role of the nonclassicalR30/EGFR-MAPK signaling in
endo-trial pathology. In our cohort of 95
tients, we observed a significant corre-ion between GPR30
expression and
tamoxifen-induced endometrial pa-logy (P .002), which is in
agree-nt with our results observed in vitro.
the study groups
Control groups
Group II Group III
16
23...........................................................................................................
5
2...........................................................................................................
1
0...........................................................................................................
0
0...........................................................................................................
22 (23.2%) 25
(26.3%)...........................................................................................................
m JObstet Gynecol 2010.
ABLE 3istribution of GPR30 expression in d
PR30 intensityTamoxifenGroup I n (%)
PR30 Neg n 41 10
(20.8).........................................................................................................................
PR30 Low n 25 17
(35.4).........................................................................................................................
PR30 High n 29 21
(43.8).........................................................................................................................
.002.PR30, G-protein-coupled receptor.gnatov. GPR30 and
tamoxifen-induced endometrial pathology. A
y DECEMBER 2010the best of our knowledge, this is thet study
evaluating the association ofR30 and tamoxifen-induced endo-trial
abnormalities in vivo and assess-the GPR30-mediated tamoxifen
ago-
tic effects. GPR30 immunoreactivitys detected in the cytoplasm
and in thecleus of the cells and has already beenscribed by
different research groups inast cancer.12,21,24,25 These resultsght
help us to definitely resolve the ex-ssion pattern of GPR30 in
differentues.igh-grade GPR30 staining was asso-
ted with an increased rate of endome-al polyps or hyperplasia
and was sig-cantly lower in normal and atrophic
dometrial tissue. It is in agreementth the work of Smith et
al,17 whond low levels of GPR30 expression in
nign endometrial tissue. Another factderlying the role of GPR30
in tamox-n-induced endometrial proliferationhe observation that
patients with highels of GPR30 expression had an endo-trial
abnormality develop signifi-tly faster. GPR30 expression showed
everse correlation to the length of timetween the start of
tamoxifen therapyd the development of symptoms.
he effect of tamoxifen agonist activ-on serum estradiol has been
contro-sially discussed in the literature. Inmenopausal women, it
has beennd that tamoxifen increases thesma estrogen level, whereas
it slightlyuced the free estradiol in postmeno-
usal women.26,27 In this context, ta-xifen can act as an agonist
only in
stmenopausal women. However,e other reports have not found
any
nificant difference in endometrial ab-
erent groups
Control
Group II n (%) Group III n (%)
13 (59.1) 15
(60.0)...........................................................................................................
6 (27.3) 7
(28.0)...........................................................................................................
3 (13.6) 3
(12.0)...........................................................................................................me
TD
G
G.
G.
G.
PGTofirsGPmeingniswanudebremim JObstet Gynecol 2010.
-
nowothohothoprewiwhinblaGPtrianthecoudifmoducouenoftwit
Tthaco
progen8. SgenNa9.
Fal.repand19910.trea47:11.JWmo19912.Opnalcou20013.torG-psigbre20014.Theateestcan15.SDnisMC12316.latitammoRe17.GPend20018.SchhigceplulagosCo19.Scbilimacou14920.proend10121.
FK pera tat
GPhigGPR
Igna
www.AJOG.org Basic Science: Gynecology Researchrmalities in pre-
and postmenopausalmen receiving tamoxifen.28,29 Al-ugh not
significant, several in our co-
rt who showed an endometrial pa-logy under tamoxifen therapy,
weremenopausal. This is in agreement
th our recent results observed in vitro,ere E2 induced GPR30
up-regulationMCF-7 breast cancer cell line.15 Le-nc et al30 have
recently confirmed thatR30 mRNA expression in endome-
al cell lines increased significantly inestrogen-rich milieu. In
this respect,controversial data in the literatureld be explained by
the influence of
ferent environmental factors on ta-xifen agonist effect.
However, E2-in-
ced up-regulation of GPR30 in vitrold explain our findings in
vivo that
dometrial abnormalities were moreen observed in premenopausal
womenh GPR30 immunoreactivity.aken together, these results suggestt
GPR30 might be an important
IGURE 4aplan-Meier plot for symptom-freeccording to the GPR30
expression s
R30 neg, negative receptor expression; GPR30 lh-grade receptor
expression. The log rank test w30, G-protein-coupled receptor.
tov. GPR30 and tamoxifen-induced endometrial pathology.mponent
in the molecular mecha-7. LChm of tamoxifen-induced endome-al
abnormalities. f
ERENCESall JM, Couse JF, Korach KS. The multifac-d mechanisms of
estradiol and estrogen re-tor signaling. J Biol Chem
2001;276:69-72.eato M, Klug J. Steroid hormone receptors:update.
Hum Reprod Update 2000;6:-36.mprota-Brears T, Whorton AR, Codazzi
F,k JD, Meyer T, McDonnell DP. Estrogen-uced activation of
mitogen-activated proteinase requires mobilization of intracellular
cal-m. Proc Natl Acad Sci U S A 1999;96:6-91.evelli A, Massobrio M,
Tesarik J. Non-omic actions of steroid hormones in repro-tive
tissues. Endocr Rev 1998;19:3-17.ae JM, Johnson MD. What does an
orphanrotein-coupled receptor have to do with es-en? Breast Cancer
Res 2005;7:243-4.rossnitz ER, Oprea TI, Sklar LA, ArterburnThe ins
and outs of GPR30: a transmem-ne estrogen receptor. J Steroid
Biocheml Biol 2008;109:350-3.
iodus
low-grade receptor expression; GPR30 high,used to calculate the
P value.
J Obstet Gynecol 2010.onning PE, Knappskog S, Staalesen
V,risanthar R, Lillehaug JR. Breast cancer
tribnin
DECEMBER 2010 American Jgnostication and prediction in the
post-omic era. Ann Oncol 2007;18:1293-306.hang Y. Molecular
mechanisms of oestro-and SERMs in endometrial carcinogenesis.
t Rev Cancer 2006;6:360-8.isher B, Costantino JP, Wickerham DL,
etTamoxifen for prevention of breast cancer:ort of the National
Surgical Adjuvant BreastBowel Project P-1 study. J Natl Cancer
Inst8;90:1371-88.Ismail SM. Pathology of endometriumted with
tamoxifen. J Clin Pathol 1994;827-33.Van Leeuwen FE, Benraadt J,
Coebergh, et al. Risk of endometrial cancer after ta-xifen
treatment of breast cancer. Lancet4;343:448-52.Prossnitz ER,
Arterburn JB, Smith HO,rea TI, Sklar LA, Hathaway HJ. Estrogen
sig-ing through the transmembrane G protein-pled receptor GPR30.
Annu Rev Physiol8;70:165-90.Filardo EJ. Epidermal growth factor
recep-(EGFR) transactivation by estrogen via therotein-coupled
receptor, GPR30: a novelnaling pathway with potential significance
forast cancer. J Steriod Biochem Mol Biol2;80:231-8.Vivacqua A,
Bonofiglio D, Recchia AG, et al.G protein-coupled receptor GPR30
medi-
s the proliferative effects induced by 17beta-radiol and
hydroxytamoxifen in endometrialcer cells. Mol Endocrinol
2006;20:631-46.Ignatov A, Ignatov T, Roessner A, Costa, Kalinski T.
Role of GPR30 in the mecha-ms of tamoxifen resistance in breast
cancerF-7 cells. Breast Cancer Res Treat 2010;:87-96.Lin BC, Suza
Wa M, Blind RD, et al. Stimu-ng theGPR30 estrogen receptor with a
noveloxifen analogue activates SF-1 and pro-tes endometrial cell
proliferation. Cancers 2009;69:5415-23.Smith HO, Leslie KK, Singh
M, et al.R30: a novel indicator of poor survival forometrial
carcinoma. Am J Obstet Gynecol7;196:386-9.Ignatov A, Lintzel J,
Kreienkamp HJ,aller HC. Sphingosine-1-phosphate is ah-affinity
ligand for the G protein-coupled re-tor GPR6 frommouse and induces
intracel-r CA2 release by activating the sphin-ine-kinase pathway.
Biochem Biophys Resmmun 2003;311:329-36.Ignatov A, Robert J,
Gregory-Evans C,haller HC. RANTES stimulates CA2 mo-zation and
inositol trisphosphate (IP3) for-tion in cells transfected with G
protein-pled receptor 75. Br J Pharmacol 2006;:490-7.Ignatov A,
Bischoff J, Ignatov T, et al. APCmoter hypermethylation is an early
event inometrial tumorigenesis. Cancer Sci 2010;:321-7.Filardo EJ,
Graeber CT, Quinn JA, et al. Dis-nistri
REF1. Hetecep3682. Ban2253. IYorindkinciu4684. Rgenduc5.
RG-ptrog6. PJB.braMo
ow,as
Amution of GPR30, a seven membrane-span-g estrogen receptor, in
primary breast can-
ournal of Obstetrics& Gynecology 595.e15
-
cer and its association with clinicopathologicdeterminants of
tumor progression. Clin CancerRes 2006;12:6359-66.22. Early Breast
Cancer Trialists CollaborativeGroup (EBCTCG). Effects of
chemotherapy andhormonal therapy for early breast cancer on
re-currence and 15-year survival: an overview ofthe randomised
trials. Lancet 2005;365:1687-717.23. Fornander T, Rutqvist LE,
Cedermark B, etal. Adjuvant tamoxifen in early breast
cancer:occurrence of new primary cancers. Lancet1989;1:117-20.24.
Revankar CM, Cimino DF, Sklar LA, Arter-burn JB, Prossnitz ER. A
transmembrane intra-
cellular estrogen receptor mediates rapid cellsignaling. Science
2005;307:1625-30.25. Thomas P, Pang Y, Filardo EJ, Dong J.Identity
of an estrogen membrane receptorcoupled to a G protein in human
breast cancercells. Endocrinology 2005;146:624-32.26. Lonning PE,
Johannessen DC, Lien EA,Ekse D, Fotsis T, Adlercreutz H. Influence
oftamoxifen on sex hormones, gonadotrophinsand sex hormone binding
globulin in postmeno-pausal breast cancer patients. J Steroid
Bio-chem Mol Biol 1995;52:491-6.27. Sunderland MC, Osborne CK.
Tamoxifen inpremenopausal patients with metastatic breastcancer: a
review. J Clin Oncol 1991;9:1283-97.
28. Cheng WF, Lin HH, Torng PL, Huang SC.Comparison of
endometrial changes amongsymptomatic tamoxifen-treated and
nontreatedpremenopausal and postmenopausal breastcancer patients.
Gynecol Oncol 1997;66:233-7.29. Swerdlow AJ, Jones ME. Tamoxifen
treat-ment for breast cancer and risk of endometrialcancer: a
case-control study. J Natl Cancer Inst2005;97:375-84.30. LeBlanc K,
Sexton E, Parent S, et al. Effectsof 4-hydroxytamoxifen, raloxifene
and ICI 182780 on survival of uterine cancer cell lines in
thepresence and absence of exogenous estro-gens. Int J Oncol
2007;30:477-87.
Research Basic Science: Gynecology www.AJOG.org
595.e16 American Journal of Obstetrics& Gynecology DECEMBER
2010
Role of GPR30 in endometrial pathology after tamoxifen for
breast cancerMATERIALS AND METHODSMaterialsCell cultureExperiments
with GPR30 antisense oligonucleotidesWestern blottingPatients and
study designImmunohistochemistryEvaluation of GPR30
immunoreactivityStatistical analysis
RESULTSE2, G1, and tamoxifen stimulate cell growth and MAPK
phosphorylation in endometrial cellsTamoxifen-induced cell growth
is reversed by knocking down GPR30Endometrial pathology in the
study groupGPR30 protein expression and tamoxifen-induced
endometrial abnormalities
COMMENTREFERENCES