Embed Size (px)
Citation preview

Rabu, 20 Mei 2020
ROLE OF CRP FOR SCREENING RESPIRATORY TRACT INFECTION
Prof. Dr. Aryati, dr., MS, SpPK(K)Ketua Umum Pengurus Pusat Perhimpunan Dokter Spesialis Patologi Klinik (PDS PatKLIn)

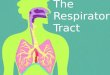
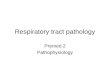
RESPIRATORY TRACT INFECTION
Respiratory tract infection (RTI) is defined as anyinfectious disease of the upper or lowerrespiratory tract.ü Upper respiratory tract infections (URTIs)
include the common cold, laryngitis,pharyngitis/tonsilitis, acute rhinitis, acuterhinosinusitis and acute otitis media.
ü Lower respiratory tract infections (LRTIs) includeacute bronchitis, bronchiolitis, pneumonia andtracheitis.
2

COMMON AGENTS OF RESPIRATORY TRACT INFECTIONS (Dasaraju & Liu, 1996)CLINICAL ILLNESS BACTERIA VIRUSES FUNGI
Common cold (rhinitis, coryza)
Rare RhinovirusesCoronavirusesParainfluenza Viruses
AdenovirusesRSVInfluenza
Rare
Pharyngitis and tonsilitis
Group A β hemolytic streptococcusCorynebacterium diphteriaeNeisseria gonorrhoea
Mycoplasma pneumoniaeMycoplasma hominis (type 1)Mixed anaerobes
AdenovirusCoxsackievirus AInfluenza virusRhinovirusesCoronaviruses
Parainfluenza VirusesEipstein Barr Virus; cytomegalovirusHerpes simplex virus
Candida albicans
Epiglottitis and laryngotracheitis
(croup);
Haemophilus influenzae type BCorynebacterium diphteriae
RSVParainfluenza Viruses
Rare
Bronchitis and bronchiolitis
Haemophilus influenzaeStreptococcus pneumoniaeMycoplasma pneumoniae
RSVParainfluenza VirusesAdenovirusHerpes simplex virus
Rare
Pneumonia Streptococcus pneumoniaeStaphylococcus aureusStreptococcus pyogenesHaemophilus influenzaeKlebsiella pneumoniaeEscherichia coliPseudomonas aeruginosaMycoplasma pneumoniae
Legionella sppAnaerobic bacteriaMycobacterium tuberculosisCoxiella burnettiChlamidya psittaciChlamidya trachomatisChlamidya pneumoniae
AdenovirusParainfluenza VirusesRSVInfluenza virusVaricella-zoster virusMeasles virus
CytomegalovirusHerpes simplex virusHantavirus
Histoplasma capsulatumBlastomyces dermatitidisParacoccidioidesCoccidioides immitisCandida albicansFilobasidiellaCryptococcus neoformansAspergillusPneumocystis carinii 3

Respiratory tract infection
Rhodes et al, 2011. DOI: 10.1038/nrrheum.2011.37 4

5Gambar 1. Respon terhadap inflamasi (Reinhart et al. Clinical Microbiology Review. 2012; 25 : 609-634)
PATOGENESIS

BLOOD SMEAR EVALUATION (BSE)
Toxic granule Vacuolization
7

BIOMARKER OF INFLAMMATION
8

ACUTE PHASE PROTEIN (APP)
They are produced from the liver as apart of immediate response to
infection or tissue injury.
9
alpha 1 antitrypsin
CRP (C-reactive Protein)
Fibronectin
Haptoglobin
Lactoferrin
Procalcitonin (PCT)

INFLAMMATORY MARKERS
10

C-REACTIVE PROTEIN
11

STRUKTUR CRP
ü Produced as homopentameric protein, termedas native CRP (nCRP)
ü Will irreversibly dissociate at sites ofinflammation/ infection into five separatemonomers, termed monomeric CRP (mCRP)
ü Synthesized (primarily) in liver hepatocytes,but alse by:• Smooth muscle cells• Macrophages• Endothelial cells• Lymphocytes• Adipocytes
Sproston & Ashworth, 2018. doi: 10.3389/fimmu.2018.00754
12

C-REACTIVE PROTEIN
13
• Synthesized within 6-8 hours of exposure to an infective process or tissuedamage
• Half life 19hrs and may reach to 1000 fold during an acute phaseresponse
• Peaks at 36–50 hours. It decreased when there was no stimuli
• It has higher sensitivity and specificity than total neutrophils and I/T ratio (immature granulocyte to total).

14
CRP mempunyai kelebihan dibandingkan LED, kenaikan suhu tubuh atau protein fase akut yang lain (a1-anti-trypsin, a1-acid glukoprotein, haptoglobin)
CRP meningkat dalam waktu 6-8 jam setelah adanya stimulus, mencapai puncak setelah 36-50 jam, dipertahankan selama masihada proses radang, inflamasi atau nekrosis jaringan dan menurundengan curam segera setelah proses radang, inflamasi atau nekrosismenghilang.
Keuntungan penentuan CRP, tidak dipengaruhi oleh obat-obatan kortikosteroid atau obat anti radang lain.

HOW TO EVALUATE THE CRP RESULT
15
< 10 mg/L • Normal concentration10 - 25 mg/L • Increased but diagnostically of less
importance• During antibiotic treatment CRP should be reduced below this level• Does not exclude bacterial infection if the disease has lasted short• Take a new sample some hours later
25 - 50 mg/L • There is “something”. Bacterial or viral?
50 - 100 mg/L • Common in bacterial infections• Seldom seen with viral infections
> 100 mg/L • Fairly common in bacterial infections

CRP PADA RESPIRATORY INFECTION
16

Ruiz-Gonzales, 2016. http://dx.doi.org/10.1155/2016/2198745 17

18

19

20Song et al, 2011. DOI:10.1111/j.1750-2659.2011.00269.x
CRP: a cutoff of 86,5 mg/L best differentiated concomitant⁄secondary bacterial pneumonia from primary influenzapneumonia (sensitivity 81,8% and specificity 59,3%)

21

CRP PADA COVID-19
22

Tan et al, 2020. DOI: 10.1002/jmv.25871 23
Stage 1 : Initial stageStage 2 : Progression stageStage 3 : Peak stageStage 4 : Recovery stage
“CRP increased significantly at the initial stage in severe COVID-19 patients; while still no significant difference in the CT scores were found between the severe and mild groups”

CRP meningkat>10mg/L pada seluruhpasien dengan rata-rata CRP 23,5 mg/L pada kelompok pasienCOVID-19 kritis
24
Liu et al, 2020

• Both CRP levels and diameter of the largestlung lesion increased with diseaseprogression.
• CRP levels were positively correlated withlung lesions and severe presentation(correlation coefficient = 0.873,0.734, P ˂ 0.001).
25

METODE PEMERIKSAAN CRP
26

27
METODE PEMERIKSAAN CRP
• Kualitatif• Semi
kuantitatif
Kuantitatif
Latex agglutination
• Enzyme immunoassay• Immunoturbidimetry (PETIA)• Nephelometry• Reflectometry Immunoassay
Aryati, 2018

28
• Prinsip : reaksi aglutinasi antara antibodi anti human CRP dan CRP pada sampel
Sampel + goat IgG antihuman CRP berlapispartikel latex à komplek antigen-antibodi à
aglutinasi
Semikuantitatif : titrasi sampel dengan two fold dilution
Latex agglutination
Aryati, 2018

29
• Prinsip : solid phase enzyme-linked immunosorbent assay Sampel + mouse monoclonal anti CRP antibody
(solid phase)
+ goat anti-CRP antibody berlabel HRP
Perubahan warna (biru) à ELISA reader
Enzyme Immunoassay
Inkubasi, washing
Substrat TMB
Aryati, 2018

30
• Prinsip : reaksi antara antibodi spesifikmenghasilkan komplek imun tidak terlarut
Sampel + antibodi monoklonal anti-CRP àkomplek antigen-antibodià kekeruhan
Spectrophotometer
Konsentrasi dalam sampel
Immunoturbidimetry (PETIA)
Aryati, 2018PETIA = Particle Enhanced Turbidimetric Immunoassay

31
• Prinsip : reaksi antara analit terlarut danantibodi anti CRP yang terikat dengan partikelpolystyrene
Sampel + partikel latex berlapis antibodimonoklonal anti-CRP àkomplek antigen-antibodi
dengan partikel latex
Light scaterring (nephelometric)
Konsentrasi dalam sampel
Nephelometry
Aryati, 2018

REFLECTOMETRY IMMUNOASSAY
Brand NycoCard™ Reader II Afinion 2TM
Made in Norway Norway
Sample typeWhole blood Whole bloodSerum, Plasma Serum, Plasma
Principle Immunometric assay – measurement reflecto meter Immunomatric assay – measurement reflecto meter
Time to results 3 minutes (all process) 3 minutes (all process)
Sample Volume 5µL 2.5µL
Touch Screen No Yes
Automatic Process Semi automatic Yes
Measuring RangeSerum/Plasma: 5-160 mg/L Serum/Plasma: 5-160 mg/LWhole blood : 5-200 mg/L Whole blood : 5-200 mg/L
Steps 5 3
Storage 2-8oC until expiry, 15-25oC 6 weeks unopened 2-8oC until expiry (12 months), 15-25oC 28 days unopened
Setting No. need set up instrument No. need set up instrumentCode number No Yes so the result will not false positive
Time to Room Temperature At least 10 minutes to reach 15-25oC At least 15 minutes to reach 18-30oC
Controls Black Calibration, White Calibration, 2 levels control Automatic calibration, 2 levels Afinion Controls

CRP POINT OF CARE TESTING - AFINION
§ 2.5 µL sample volume§ 3 minute test time§ Sample materials whole blood, serum or plasma§ Highly accurate results§ with automatic hematocrit correction
§ Measuring range whole blood; 5-200 mg/L§ No interference from common antibiotics and painkillers§ 4 week room temperature storage
33

34

TAKE HOME MESSAGECRP merupakan acute phase reactant yang diproduksiterhadap infeksi/inflamasi, merupakan marker inflamasi(termasuk infeksi bakterial, nekrosis jaringan, autoimun)
CRP dapat digunakan sebagai skrining respiratory tract infection
Di era pandemi Covid-19, CRP dapat sebagai terjadinyaderajat penyakit yang berat
Diperlukan analisis menyeluruh dengan kondisi klinis, biomarker lain serta radiologis untuk tatalaksana diagnosis respiratory tract infection
35

TANGGAL PANDUAN
7 Maret 2020 Manajemen Spesimen Dan Diagnosis Laboratorium KasusSuspek 2019-ncov
7 Maret 2020 Pencegahan Dan Pengendalian Infeksi Pada Suspek Infeksi2019-ncov
19 Maret 2020 Press Release Kewaspadaan Tes Cepat (Rapid Test) COVID-19 Igm/Igg Berbasis Serologi
21 Maret 2020 Alur Pemeriksaan Rapid Test Sars-Cov-2 (COVID-19) Usulan PDS Patklin
25 Maret 2020 Panduan Tatalaksana Pemeriksaan Rapid Test Antibody Sars-cov-2 Metode Imunokromatografi
20 April 2020 Daftar Rapid Test Serologi COVID-19 Yang SudahTerdaftar di FDA Negara
21 April 2020 Revisi Panduan Pemeriksaan Rapid Test Antibodi MetodeImunokromatografi
22 April 2020 Panduan Tatalaksana Pemeriksaan Tes Cepat Molekuler(TCM) dan Polymerase Chain Reaction (PCR) SARS-CoV-2 36
Berbagai Panduan COVID-19 oleh PDS PatKLIn

37
1. Email : [email protected]. Facebook : [email protected]. Website : www.pdspatklin.or.id4. Youtube : PDS PatKLIn Dokter Patologi Klinik5. Instagram : DOKTER PATOLOGI KLINIK6. Twitter : www.twitter.com/patologi_klinik

38
TERIMA KASIH