Embed Size (px)
Citation preview

Role of Bronchopulmonary Lavage in the
Treatment of Respiratory Failure: A Review* Robert M. Rogers, M.D., F.C.C.P.,' " Milton S. Braunstein, M.D.? and John F . Shuman, M.D.f
large part of our therapeutic effort in the A ,,en, of respiratory failure is directed at enhancing the clearance of secretions from the lung. Such procedures as nasotracheal suctioning, tracheostomy, bronchoscopy, chest physiotherapy and postural drainage are used with varying de- grees of success.
Over the last few years, we have gained expe- rience with the technique of volume controlled bronchopulmonary lavage which can remove large quantities of material from the airways and alveoli in a short period of time. Although the procedure was first reported in 1965,' published clinical ex- perience remains limited. In view of the potential applications of this procedure in the treatment of respiratory failure, it seems appropriate to review the technical, physiologic and clinical aspects of bronchopulmonary lavage at this time.
Endobronchial therapy for pneumonia was sug- gested in 1915 by Kline and Winternitz2 following claims by earlier investigator^^.^ that the introduc- tion of saline solution into the lungs of dogs produced no deleterious effects. Winternitz and Smith5 were able to remove from the lungs of dogs with lavage more than 90 percent of previously
'From the Hospital of the University of Pennsylvania (De- partments of Medicine and Physiology), Philadelphia. Supported in part by US Public Health Service grant (HE08805-OB), Clinical Research Center, Division of Re- search Facilities and Resources, National Institutes of Health ant (3MOI FR-40) and grants from the Pennsyl- vania ~ c r s c i c Society and the National Tuberculosis and Respiratory Disease Association.
*'Professor of Medicine, University of Oklahoma Medical Center, Oklahoma City.
tFellow in Pulmonary Disease. Reprint requests: Dr. Rogers, University of Oklahoma Health Sciences Center, PO Box 26901, Oklahoma Ci ty
instilled nonpathogenic bacteria or starch. Virulent pneumococci instilled into dog lungs could also be removed in the same large quantities, but the development of pneumonia was not prevented, and the authors suggested the use of endobronchial antiseptics in the future. Vicente,6 in 1928, was the first to describe a technique whereby a catheter was placed into the dependent lung of an awake human patient breathing room air in the lateral decubitus position. Saline solution was flushed into the de- pendent lung through the catheter to aid in removal of secretions (Fig 1 ) . Figure 1 pictures the depen- dent lung filled with fluid, but this is obviously not accurate since degassing was not employed and numerous bubbles would be present. Vicente treated such conditions as bronchiectasis, chronic bronchitis, asthma, and lung abscesses, publishing extensively on his experience with this technique between 1928-36. No similar reports of lavage in humans (other than bronchos~opic~-'~) were re- ported until 1963 when Ramirez-R and col- l e a g u e ~ ' ~ ~ ' ~ introduced the technique of "segmen- tal flooding" for the treatment of alveolar
FIGURE 1. Diagram of a patient during lavage with the tech- nique of Garcia Vicenle. (From Rev Prog de la Clinica, julio, 1928).
CHEST, VOL. 62, NO. 5, NOVEMBER 1972 SUPPLEMENT (PART 2) 95s
Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21550/ on 04/28/2017

ROGERS, BRAUNSTEIN, SHUMAN
proteinosis. This technique involves the introduc- tion of 50 to 100 ml saline solution into various lung segments via a transtracheal polyethylene catheter (Fig 2). Both segmental lavage and bron- choscopic lavage remove some secretions directly, but depend primarily on the patient's vigorous coughmg and expectoration.
Kylstra,1"18 interested in the lung as an ex- change surface for dialysis, demonstrated that pro- longed survival in dogs was possible following lavage of one lobe. Subsequently, Fi~dey'~ per- formed segmental lavage in man for diagnostic and research purposes using a cuffed radiopaque cathe- ter. With this work as a background, Ram.ire~-Rl*~~ developed a technique whereby an entire lung could be lavaged while the other lung was venti- lated. Kylstra and co-workers2' subsequently uti- lized a similar technique for lavage in human dis- ease which represents a modification of the technique he perfected in dogs. We will limit our discussion in this paper to volume controlled bron- chopulmonary lavage, also called "massive bron- chopulmonary lavage" and "total bronchopulmo- nary lavage." This procedure has two major advantages over those previously mentioned:
FIGURE 2. Diagram illustrating the technique of segmental flooding as first utilized by Ramirez-R for the treatment of alveolar proteinosis. (From Arch Int Med 112:419, 1963).
1 ) adequate alveolar ventilation can be maintained by ventilating the non-lavaged lung; 2) it can be assumed that the fluid reaches essentially all areas of the lung since the lavaged lung is gas free and f led with fluid.
In all our lavages, we have utilized the volume controlled technique of Kylstra and colleagues,Zl and our description will be limited to this approach. Their technique differs slightly from that of Rarnirez-R, which has been described in detail elsewhere.20 We perform all lavages using general anesthesia with supplemental topical anesthesia of the larynx and trachea. A high inspired oxygen level (FI*), preferably 95 to 98 percent, is used. The hazard of the repeated use of halothane is considered in choosing an anesthetic. Patients are carefully monitored throughout ;he procedure. The use of an esophageal stethoscope, electrocardiographic monitor, and frequent arterial blood gas determinations is routine. A Car- lens catheter is placed isolating the two lungs, and proper positioning is verified by auscultation and bronchospirometry. During spontaneous breathing, after placement of the Car- lens catheter, bronchospirometric measurements of oxygen consumption of each lung are made. Following these mea- surements, ventilation is controlled to maintain normal P a m level.
With the patient in the lateral decubitus position (Fig 3), the lung to be lavaged is isolated from the anesthesia-oxygen supply by clamping the tubing and connecting it to the saline delivery system. At one minute intervals, a volume of saline solution equal to the measured oxygen consumption of that lung is allowed to flow into the lung by gravity. It is assumed that in this manner, complete degassing of the lung can be accomplished without significant creation of air pockets or turbulence such as might occur if saline were added at a rate exceeding the measured oxygen consumption. It is also hoped
FIGURE 3. Diagram of patient during bronchopulmonary lavage. The patient is in the lateral decubitus position. Saline solution flows into and out of the lung by gravity, while the non-lavaged lung is ventilated with oxygen. (From Med Clin NA 54755, 1970).
CHEST, VOL. 62, NO. 5, NOVEMBER 1972 SUPPLEMENT (PART 2)
Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21550/ on 04/28/2017

ROLE OF BRONCHOPULMONARY LAVAGE 97s
that this will prevent extensive atelectasis, since ideally, the end result will be a lung "distended" by fluid which has replaced the gas without atelectasis intervening. When the volume of saline in the lung is equal to the functional residual capacity (FRC) of that lung, volumes of 300 to 500 ml of saline solution are allowed to flow rapidly into the lung, after which a similar volume is drained into the bottle by gravity (Fig 3). Total volumes of fluid have ranged from 5 to 25 liters. Following the last instillation, as much fluid as possible is drained from the lung. The Trendelenburg position and endotracheal suctioning through the Carlens catheter are used to augment drainage. In every case, an amount of saline solution at least equal to the residual volume of the lavaged lung has remained in that lung following the procedure and is absorbed or expectorated over the next 24 to 48 hours.
The patient is taken to the recovery room receiving sup- plemental oxygen which is continued for 24 hours, the need being determined by serial Pa- measurements. Elective mechanical ventilation is continued in cases where the pa- tient was in respiratory failure before lavage. Asthmatics who have had severe bronchospasm following lavage have also been ventilated for up to 48 hours. For these cases, the Carlens tube is replaced with an endotracheal tube.
Winternitz and Smith,5.22 interested in war gas poisoning, demonstrated that the pathologic changes following introduction of isotonic saline into dog lungs were minimal and had resolved by four days. K y l ~ t r a l ~ - ' ~ has confirmed the paucity of histologic changes following lavage in dogs. A report of minor light and electron microscopic changes in the dog lung following lavage with saline solution, at room temperature and without degassing,23 is difficult to evaluate because the technique is so different from volume controlled bronchopulmonary lavage. A more detailed re- portz4 of minor light and electron microscopic changes in the dog lung following saline solution lavage has also been published. These same investi- gators, however, also stated that no such histologic changes were found in dog lungs examined after segmental saline solution lavage if the volume of solution was 300 rnl or less,lQ and on the basis of these observations they have performed segmental lavages in man. It seems reasonable, therefore, to conclude that minor transient histologic changes are present immediately post lavage, although no con- firmatory histologic studies in humans are available for obvious reasons.
be increased and this could lead to cardiac failure; 2 ) significant hypoxia might result because the blood perfusing the saline solution filled lung is not exposed to oxygen; 3 ) surfactant might be removed by lavage, causing a decrease in compliance; 4 ) other pulmonary function tests might be impaired by the saline solution remaining in the lung at the completion of lavage, irritation of the airway by the catheters, or removal or displacement of surfactant.
Absorption of Saline
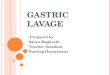
The quantity of saline solution absorbed during lavage appears to be insignificant in man1 and a n i m a l ~ . ' ~ - ' ~ * ~ ~ Figure 4 illustrates the amount of fluid which is recoverable from dog lungs after instillation of 100 ml of distilled water, isotonic saline solution, serum, and sea water. Saline solution has a half-life of one hour, while distilled water is instantaneously absorbed, 90 percent of dog serum is absorbed in 20 minutes, and sea water actually draws additional water into the lungs. This slow absorption can probably be attributed to the in- herent resistance of the alveolar capillary mem- brane to the absorption of ionic solutions26-27 and the diminished pulmonary blood flow to the lung being lavaged ( see below ) .
We have carefully observed pre- and post lavage electrolytes, hematocrit, weight, intake, and output, in our patients and have concluded that there is little fluid or electrolyte absorption other than the residual saline solution left in the lung at the completion of lavage (200 ml to 1500 ml) . The ab- sorption of this small amount of saline solution has caused no significant clinical problem.
We found, as did o t h e r ~ , ~ ~ - ~ O that venous ad- mixture varied during lavage. It was clear that the percentage of venous admixture was largest when the lung was partially filled with saline solution and least when the lung was filled to total lung capacity (TLC) . In a series of patients, we were able to demonstrate that when the hydrostatic pressure in the airway of the lavaged lung exceeded pulmonary artery pressure, perfusion of that lung approached zero, and when the airwav Dressure of the fluid . A
filled lung fell below pulmonary artery pres- sure, perfusion returned and venous admixture in-
We are unaware of any systematic evaluation of c rea~ed.~ ' This is a situation analogous to the the effects of lavage containing medications, and zone I lung of West32 and consistent with earlier therefore will limit our discussion to saline solution. observations on the relationship between alveolar Saline might conceivably be harmful in one or pressure and blood flow in dogs.33," It is clear several ways: 1) if rapid absorption of the solution from these findings that shunting can be minimized occurs, the circulating intravascular volume would by extending the time periods when the fluid
CHEST, VOL. 62, NO. 5, NOVEMBER 1972 SUPPLEMENT (PART 2)
Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21550/ on 04/28/2017

98s ROGERS, BRAUNSTEIN, SHUMAN
FIGURE 4. In this figure is plotted the volume change in ml of fluid (ordinate) in the air spaces against time in minutes (abscissa) after instillation of 100 ml each of 1) normal saline solution, 2) dog serum, 3) sea water, 4) distilled water. Note that the half-life of saline solution is approximately one hour, dog serum is absorbed much more rapidly (90 percent in 20 minutes), and distilled water is absorbed almost instantane- ously. Sea water (3) actually causes an immediate increase in fluid to over 180 ml (off scale) with return to the original volume of 100 ml at 40 minutes.
volume is close to TLC, and decreasing the time for drainage, at which time lung volume is close to FRC. Thus, with the use of 99 percent oxygen to ventilate the nonlavaged lung and careful monitor- ing of arterial blood gases, lavage can be safely performed in the severely ill respiratory patient.
Recooery of Surfactant in Lavage Efluent
It has been shown in dogs that the introduction of saline solution into the alveolar spaces causes a reduction in lung compliance which is due to increased surface forces.35 In these studies, the
surface tension of lung extracts was higher in fluid instilled lobes than in nonfluid instilled lobes, sug- gesting that the fluid inactivated or displaced pul- monary surfactant. These findings were consistent with the observation that a stable foam can be obtained in fluid that has been instilled and with- drawn from the alveoli.36 Subsequently, several investigator^^^*^^^^^ have been able to obtain min- imum surface tension values of less than 13 dyneslcm, indicating the presence of surfactant in the lavage effluent of animals. Both instillation of saline solution35 and saline lavage".36 in dogs have produced an acute shift to the right of the pressure-volume curves of the lavaged lung, a finding consistent with decreased surfactant.
Studies of lavage effluent in humans, however, have been less clear. Kylstra and colleague^^^ studied the surface tension of lavage effluents from a normal volunteer and four patients with asthma and found minimal surface tensions in excess of 12 dyneslcm in the mixed effluent of lavage fluid. In alveolar proteinosis, Ramirez-R20 was unable to find surface active material in nine of ten washings. We have examined the lavage effluent of 14 lavages in ten patients40 (seven with asthma and three with alveolar proteinosis ) . Our technique differed from Kylstra's in that we collected the effluent serially in 1500 ml bottles and centrifuged a 500 ml aliquot of each bottle. The centrifugate was resus- pended in 40 ml of saline solution and placed in a modified Wilhelmy balance. In every patient's effluent, we found minimum surface tension below 13 dyneslcm in at least one bottle, and in two to five bottles in seven patients. In order to simulate the mixed effluent examined by Kylstra, we com- bined all 1500 ml bottles into a large container and examined a 500 ml centrifuged specimen on the Wilhelmy balance. Minimum surface tension values were similar to those reported by K y l ~ t r a . ~ ~ We concluded that since in animal work only 100 to 500 ml of lavage effluent is utilized while 6 to 27 liters is used in humans, the latter volume so dilutes the surfactant present that it cannot be measured in the mixed effluent.
We have also noted a shift in the pressure-volume curve down and to the right immediately post- lavage. However, this returned to normal by 24 to 72 hours.41 This acute shift of the curve down and to the right has also been reported in a normal human volunteell and is consistent with increased surface forces.
Effect of Lavage on Pulmonary Function
We have measured vital capacity (VC) and maximum mid-expiratory flow rate (MMEFR) dur-
CHEST, VOL. 62, NO. 5, NOVEMBER 1972 SUPPLEMENT (PART 2)
Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21550/ on 04/28/2017

ROLE OF BRONCHOPULMONARY LAVAGE 99s
ing the immediate 72 hours post lavage in eight instances. The VC decreased in the first ten hours (range of change 0 to 1.5 L) , and this decrease tended to last up to 24 hours. Between 24 and 48 hours postlavage, all patients had attained or exceeded their prelavage values. Similar changes were noted in MMEFR. In patients with alveolar proteinosis, the decrease in VC and MMEFR was less than in patients with asthma and the return to normal occurred earlier.
One patient had severe, persistent hypoxemia throughout one lavage, but had nine additional lavages with no oxygenation problem. In all our other patients, adequate oxygenation during lav- age was easily accomplished. Hypercarbia oc- curred during lavage more frequently in the asthma patients and usually could be easily corrected by increasing the ventilation to the non-lavaged lung. During the immediate postlavage period, most pa- tients required only high inspired oxygen concen- tration. However, two asthmatics and one alveolar proteinosis patient required mechanical ventilation for 6-12 hours postlavage.
Currently, this procedure has been utilized in humans for the treatment of alveolar proteinosis,
Table 1-Bronchopulrnonary
bronchial asthma, cystic fibrosis, chronic bronchitis, desquamative interstitial pneumonitis, unresolved pneumonia, Goodpasture's syndrome and inhalation of radioactive particles. Table 1 tabulates the clini- cal experience with bronchopulmonary lavage re- ported to date. There has been only one death reported during or postlavage and this patient died of a pulmonary embolism which is difficult to relate to the procedure per se. Lavage has been suggested, but not performed in other clinical conditions such as aspiration pneumonia, alveolar microlithiasis, allergic bronchopulmonary aspergillosis, Pneumo- c!ystis carinii infestation, and bronchiectasis. Re- moval of excessive secretions or abnormal material in these diseases might be expected to lead to at least temporary improvement in lung function and, in many cases, provide valuable time for the em- ployment of other therapeutic measures. It is to be expected that the transient adverse effects of lavage will be offset by the substantial improvement in pulmonary function that will result from the re- moval of significant quantities of secretions. We will review our own experience and the published experience with lavage in the diseases for which it has been used. In addition, we will review some of the theoretic and pathophysiologic reasons to con- sider it in other diseases.
Lavage Performed in Man
Disease No. Patients No. Lavages Investigator
Alveolar proteinosis Alveolar proteinosis Alveolar proteinosis Alveolar proteinosis Alveolar proteinosis Alveolar proteinosis Alveolar proteinosis
Asthma Asthma Asthma and chronic bronchitis Asthma and bronchitis Asthma Chronic bronchitis
Cystic fibrosis Cystic fibrosis
M i S c e U a m Bronchiectssia Unresolved pneumonia Normal volunteer Goodpasture's syndrome Desquamative interstitial pneumonitis Accidental inhalation of radioactive particles
Ramirez-R, et all Ramirex-R, et all0 Ramirez-R, et a144 Ramirez-R, et a143 Wasserman, et a12' Smith, et aIB Rogers, e t alas*
Ramirez-R, et all Ramirez-R, et Ramirez-R, ct aI3O Kylstra, et n12' Rogers, e t alM* R a m i r e ~ - R ~ ~
Kyhtra, et a121 Rogers, et a1
Kylstra, et aI2l Ramirez-R4 Kylntra, et aI2l Rogers, et aIz6 Rogrrs, et al* Muggenburysl
*current report
CHEST, VOL. 62, NO. 5, NOVEMBER 1972 SUPPLEMENT (PART 2)
Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21550/ on 04/28/2017

ROGERS, BRAUNSTEIN, SHUMAN
FIGURE 5. Lung biopsy specimen from a patient with pulmo- nary alveolar proteinosis. The alveoli are completely 6lled with PAS staining amorphous material and the alveolar lining cells and interstitiurn are normal (X 325).
Pulrnonuy Alveolar Proteinosis
The first "volume controlled bronchopulmonary lavage was performed on a patient who had alveo- lar proteinosis.' Alveolar proteinosis* is a rare pulmonary disease of unknown etiology which has a unique pathologic picture-&, alveolar spaces filled with a PAS-positive, lipid rich "proteinaceous" ma- terial, and no abnormality of the alveolar wall, interstitial spaces, conducting airways, or pleural surfaces (Fig 5). The most common symptom experienced by all our patients has been dyspnea on exertion. Other symptoms, such as productive or nonproductive cough, chest pain, and hemoptysis, are less frequent and often seem to be related to superimposed infections. The degree of symp- tomatology ranges from minimal or none to severe respiratory failure which can be fatal. Physical findings are nonspecific and include cyanosis and fine inspiratory rales with some dullness to percus- sion. Mild to severe hypoxemia with reduction in carbon monoxide single breath diffusing capacity and minimal decrease in lung volumes are the
consistent abnormalities in pulmonary function. Removal of the "proteinaceous" material from the alveolar spaces is the goal of lavage and the large amount of sediment in the effluent makes it clear that one can accomplish this (Fig 6A and B). Clinical improvement has been consistently re- ported;1~19~28~29~*~u improvement in the chest roentgenogram is also common, but did not occur in all of our patients despite significant clinical im- provement. We have performed 28 lavages on six patients which brings the total number of patients to 27 and the number of lavages to 103.& Each of our patients showed clinical improvement ac- companied by a rise in resting arterial partial pres- sure of oxygen on room air and 100 percent oxygen. A typical patient's results are summarized in Figure 7. She had dramatic clinical, roentgenographic and physiologic improvement after four lavages.
Since the symptoms in patients with alveolar proteinosis range from minimum to severe, not all patients with the disease are candidates for lavage, especially since spontaneous remissions have been noted. We have reserved lavage for those patients with moderate to severe dyspnea on exertion. We feel that lavage is the treatment of choice in these patients, and nebulized enzymes, etc, are not indi- cated.
Bronchial Asthma
Status Asthmaticus. When death occurs in status asthmaticus, one usually finds at postmortem ex-
FIGURE 6. Effluent lavage fluid from patient with alveolar proteinosis. A, left) shortly after lavage. B, right) after stand- ing for several hours. Note the large amount of sediment in the lx~ttom of the bottle (500-750 ml). ( From Med Clin NA 54755, 1970).
CHEST, VOL. 62, NO. 5, NOVEMBER 1972 SUPPLEMENT (PART 2)
Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21550/ on 04/28/2017

ROLE OF BRONCHOPULMONARY LAVAGE
FIGURE 7. Results of blood gas studies and vital capacity mea- surements on a patient with alveolar proteinosis before and after lavage. Note the rise in arterial P e on room air, exercise and 100 percent oxygen and the increase in vital capacity. The improvement in pulmonary function was accompanied by a marked clinical improvement. ( From Med Clin NA 54: 755,1970).
amination thick, tenacious mucus plugs obstructing airways that vary in size from lobar bronchi to bronchioles.'"@ These mucus plugs are felt to contribute to the severe hypoxemia and hypercarbia which is noted prior to death. Bronchoscopists have
removed these plugs by suctioning through the bronchoscope, usually after instillation of saline solution.g10 Drawbacks of the bronchoscopic ap- proach include: 1) limited access to peripheral airways because of rigidity of the instrument, and 2) inability to assist ventilation mechanically during the procedure. On the other hand, with broncho- pulmonary lavage, the lung is filled with saline solution; hence, all affected airways are lavaged and adequate ventilation can be maintained by the other lung. This conclusion, of course, is valid only if one is able to control the bronchospasm.
Figure 8 pictures bronchial casts from the lavage fluid of a severe asthmatic. The large casts were present in the first effluent (Fig 8A), while sub- sequent effluent contained the very small mucus plugs noted in Figure 8B. These smaller plugs appear to represent Curschrnann spirals (Fig 8C and D). The cells noted in these specimens proved to be predominantly eosinophils, although macro- phages were also noted when the specimens were examined under higher power magnification in fixed stain section. We have not identified bacteria or fungus in this material to date.
Subacute or Chronic Asthma. The rationale for the use of bronchopulmonary lavage in subacute or chronic asthma is less certain. The approach is
FIGURE 8. A and B, upper left and right) Bronchial casts from the lavage fluid effluent of a &ere asthmatic. C, lower left) casts in B magnified X 30. D, lower right) casts in B magnified x 90. (From Med Clin NA 547.55, 1970).
CHEST, VOL. 62, NO. 5, NOVEMBER 1972 SUPPLEMENT (PART 2)
Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21550/ on 04/28/2017

ROGERS, BRAUNSTEIN, SHUMAN
reasonable if one assumes that antigenic material has been deposited deep in the lungs, where it cannot be removed because of increased viscosity of mucus, impaired mucociliary movement, or de- creased effectiveness of cough. Its presence might be causing continued release of a bronchoconstric- tive material such as histamine, and therefore be responsible for the chronic, persistent symptoms of the patient. This, of course, is all supposition, and one should not embark upon treatment of patients in this situation without a clear-cut protocol from which information can be gained regarding effec- tiveness, indications for treatment, etc.
We have performed 12 volume controlled lavages on seven patients with bronchial asthma. Five of these patients were treated during a period of severe status asthmaticus which was unresponsive to the usual measures, including bronchodilators and high dose steroids. Casts of large and small airways were present in the effluent, and there were usually several hundred smaller ones which mea- sured as small as respiratory bronchioles. Each patient showed clinical improvement, although in some it was not apparent for 4 to 12 hours post- lavage, and two patients required mechanical venti- lation for 4 to 12 hours postlavage. The longterm effects of lavage in this group, as well as in the three other asthmatics ( lavaged because of chronic mod- erate wheezing requiring high doses of steroids, is uncertain. One patient was able to stop all medica- tion for one year, but then had a severe attack which was not reversible by lavage and required a high dose of steroids to reverse. In several others, the amount of medications and the number of hospital admissions per year were reduced; how- ever, the group was too small to draw any firm conclusions. KylstraZ1 has reported pulmonary function studies on 18 patients with asthma and chronic asthmatic bronchitis before and after lavage. "Substantial" improvement occurred in ten patients, and mean data indicated sigmficant in- creases in vital capacity, FEVI and Paoz. Ramirez- R and Obenour30 have also lavaged patients with moderately severe asthma and felt that the proce- dure had promise.
It should be noted that in the severely ill patient, lavage is frequently' very difficult. Degassing is often incomplete, as indicated by bubbles present in the lavage effluent. Bronchospasm may be severe and adequate ventilation with one lung may not be feasible. Most patients, in fact, require intensive intravenous bronchodilator therapy (usually with aminophylline) and steroids before, during and
immediately after lavage. Because of the above factors, we recommend that lavage be reserved primarily for the intractable asthmatic when other measures have not succeeded and mucus plugging is felt to be an important factor threatening survival of the patient. Careful monitoring during the pro- cedure is imperative, and a positive pressure ma- chine may be necessary to ventilate the nonlavaged lung during the procedure because of the high inflation pressures required.
Cystic Fibrosis
Most of the therapeutic efforts in the treatment of cystic fibrosis are directed toward the removal of the thick, viscous secretions which obstruct the airways and result in a progressive deterioration of pulmonary function. Limited forms of bronchial lavage with acetylcysteine50 and saline solution51 have been recommended, but saline solution alone is probably preferable because high concentrations of acetylcysteine can be h a z a r d o u ~ . ~ ~ Volume con- trolled lavage of an entire lung in the manner which we have described is at present limited to older children with larynges and tracheas large enough to accommodate a Carlens catheter. We have per- formed only one lavage on one patient who did not return for followup studies, so we do not know if his pulmonary function improved. Kylstra21 reported ten patients with cystic fibrosis treated with volume controlled lavage. Substantial clinical improvement with decreased sputum volume and viscosity oc- curred in eight of the ten. In only five, however, was there a rise in arterial POZ, and improvements in lung volumes and flow rates were less common. Fever during the first 24 hours postlavage was universal.
Although removal of the viscous secretions which accumulate and produce deterioration of pulmo- nary function in this disease would theoretically be of great benefit, the use of bronchopulmonary lavage for this purpose must still be considered experimental. If the technical problems of perform- ing a lavage in a child with a small larynx and trachea can be overcome, the procedure may have more applicability. In this regard, simultaneous bilateral lung lavage has been successfully per- formed in children using partial cardiopulmonary bypass,52 and dogs have survived bilateral lavage with hyperbarically oxygenated ~ a l i n e , ~ ~ , ~ ~ al- though the latter has led to severe respiratory acidosis.
Chronic Obstructiue Lung Disease
The rationale for the use of lavage in chronic obstructive lung disease is the hope that removal of
CHEST, VOL. 62, NO. 5, NOVEMBER 1972 SUPPLEMENT (PART 2)
Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21550/ on 04/28/2017

ROLE OF BRONCHOPULMONARY LAVAGE
thick, purulent secretions will improve pulmonary function.
Limited forms of lavage have yielded margina18,0 or no success. Ramirez-R and ObenouP have lavaged entire lungs of five patients with chronic bronchitis. Although mild to moderate hypoxemia was present none of the patients had hypercap- nia prelavage. Immediately postlavage, however, severe hypoxemia and mild to moderate hyper- capnia was common. Although a subjective clinical response occurred, no more than a transient physiologic improvement in one patient could be documented.
One might conclude that the mucosal edema, increased mucus gland hypertrophy, infection, bronchospasm and diminished elastic recoil play a more important role in the clinical picture of chronic obstructive lung disease than secretions in the airway. The slight improvement one might expect is probably offset by trapping of a large amount of saline solutionig in the lung and devel- opment of infiltrates" which could be due to dissemination of infection or retained saline. It is therefore difficult at this time to recommend bron- chopulmonary lavage for chronic obstructive pul- monary diseases other than asthma.
Other Diseases
KylstraZ1 lavaged four patients with bronchiec- tasis and reported a decrease in the daily volume of sputum postlavage. However, he stated that "there was not enough quantitative data to substantiate the clinical impression that lung lavage was of benefit to them."
Rogers and Tantumm have lavaged a patient with Goodpasture's syndrome in renal and respira- tory failure. The patient's clinical course was not altered and she died following cardiac arrest 58 hours postlavage. We have recently lavaged a patient with desquarnative interstitial pneurnonitis whose steroids had to be discontinued due to severe osteoporosis and multiple vertebral fractures. It is noteworthy that the procedure was successful in removing moderate quantities of desquamated alveolar cells (Fig 9). However, her clinical course has not been noticeably altered to date. Lavage has also been successful in the removal of inhaled radioactive particles in dogsm and in a single patient following accidental exposure.61
Segmental or other forms of limited lavage may have potential in the treatment of lung abscesses and aspergill~mas,~ and in obtaining cells for diagnostic purposes. Bronchopulmonary lavage may
CHEST, VOL. 62, NO: 5, NOVEMBER 1972 SUP
be useful in the treatment of overwhleming pneu- monia~, aspiration pneumonias, Pneumocystis catinii infestation, pulmonary alveolar microlithi- asis, allergic aspergillosis, and alveolar cell carci- noma. We are not aware of any trials of lavage in these diseases and would like to discuss some of the theoretical considerations of lavage in the treatment of aspiration pneumonia.
Pneumonia
In spite of considerable advances in antimicrobial therapy and respiratory physiology, pneumonia re- mains a leading muse of death.% Bacterial pneu- monia in previously healthy young adults is un- common, but the disease continues to attack the elderly and the debilitated, as well as patients with diabetes mellitus, alcoholism, congestive heart fail- ure, and chronic lung disease. Although the in- cidence of Gram-negative pneumonias is increas- ing,56,67 many cases of pneumonia sensitive to the commonly used antibiotics do not resolve possibly because of the patient's inability to clear secretions. If this is the case, debridement of the airways and alveoli might be expected to benefit these patients.
Early attempts to prevent the development of
'PL
FIGURE 9. Lavage effluent from a patient with desquamative interstitial pneumonitis. Note the large numbers of granular pneumocytes ( x 325).
.EMENT (PART 2)
Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21550/ on 04/28/2017

104s ROGERS, BRAUNSTEIN, SHUMAN
pneumonia in dogs by irrigation with saline solution following the instillation of pneumococci were un- suc~essful.~ In fact, these irrigations appeared to worsen the subsequent pneumonia. A patient with unresolved bacterial pneumonia lavaged by Ramirez-R et all developed fever postlavage. In light of our present knowledge, the possibility of spreading infection to uninvolved areas of the lung must be considered, and an animal model is cur- rently being developed in our laboratory to try to answer the question, as well as define the value of antibiotics in the lavage fluid.
There appears to be little potential for the use of lavage in the treatment of viral pneumonias. The early invasion of respiratory epithelial cells, the diffuse involvement of the lung interstitium and the relative unimportance of secretions suggest that it would not be helpful. Furthermore, the instillation of fluid into the lungs of mice infected with influenza virus has been shown to worsen the i n f e ~ t i o n . ~ ~ . ~ ~
Aspiration Pneumonia
Aspiration of gastric contents, a potentially lethal complication of general anesthesia, was initially described by Mendelsona3 in 1946. It also occurs in patients who are debilitated or in coma, or have neurologic disorders of the pharynx, and has been noted with improperly functioning nasogastric or endotracheal tubes. Large pieces of solid material can be removed by bronchoscopy, whereas small pieces and liquid material may lie beyond the reach of the bronchoscope. Aspiration of liquid vomitus may produce an acute chemical pulmonary edema with diffuse pulmonary infiltration, diminished lung compliance, bronchospasm, and severe hypoxemia, which may be uncorrected by increasing inspired oxygen concentration (ie, right-to-left shunt). The large shunt has been attributed to alveolar instabili- ty and collapse, and the clinical picture is that of the respiratory distress syndrome of adults (see Sugerman, Rogers-this issue ) .
The demonstration that the severity of the clini- cal and pathologic picture of aspiration pneumonia is related to the pH of the aspirated fluids4sm has led to the speculation that lavage might be used to dilute or neutralize the aspirated acid.' In addition, the demonstration that systemic steroid therapy is of value has led to the suggestion that steroids be included in the lavage fluid.66
A limited pilot studya1 suggested that volume controlled lavage of an entire lung may be benefi- cial in experimentally induced aspiration pneumo- nitis of Beagle dogs; however, the data are very preliminary. Since the chemical damage from acid
is immediate, and the acid is neutralized within ten minutesa7 by the lung tissues, the use of lavage in aspiration pneumonia would seem to be useful only for the removal of particulate matter which is beyond the reach of the bronchoscope. The addi- tion of steroids to the lavage fluid is based upon the assumption that the ratio of lung tissue to serum steroid concentrations is higher after local adminis- tration than it is after systemic administration. This has never been demonstrated and in fact, the rate of absorption of steroids from lavage fluid has not been quantitated.
At the present time, the most efficacious thera- peutic modalities available for the treatment of aspiration pneumonia continue to be systemic steroids, prompt treatment of complicating infec- tion, careful monitoring of fluid and electrolyte balance, and administration of oxygen and ventila- fory support as needed, and, when indicated, the judicious use of positive end-expiratory pressure ventilatory support.
Bronchopulmonary lavage is a technique where- by large amounts of material can be removed from the airways and alveoli. The use of a double lumen catheter permits adequate gas exchange while one lung is being lavaged. The procedure has been performed safely even in the presence of severe hypoxemia and may have applicability to many diseases in which debridement of small airways and alveoli is desirable. Acute histologic changes and changes in compliance associated with increased surface forces are transient.
The principal indication for lavage is pulmonary alveolar proteinosis and we feel that lavage is the treatment of choice for this disease. Dramatic improvement may occur in status asthmaticus, but management is difficult and lavage should be re- served for those cases unresponsive to more con- servative therapy. Insufficient data are available with respect to other diseases to draw conclusions regarding the usefulness of lavage. Preliminary observations, however, are encouraging, particular- ly with cystic fibrosis.
ACKNOWLEDGMENTS: The authors wish to thank the following people for their help: Miss Barbara Alpern, Mr. Roscoe Woods, Mr. Mark Eisenstock, Mrs. Sandra Penzkover, and Mr. Alan Zubrow.
1 Ramirez-R J, Kieffer RF, Ball WC: Bronchopulmonary lavage in man. Ann Int Med 63:819, 1965
2 Kline BS, Winternitz MC: Studies upon experimental pneumonia in rabbits. VIII. Intra vitam staining in ex-
CHEST, VOL. 62, NO. 5, NOVEMBER 1972 SUPPLEMENT (PART 2)
Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21550/ on 04/28/2017

ROLE OF BRONCHOPULMONARY LAVAGE
perimental pneumonia, and the circulation in the pneu- monic lung. J Exp Med 21:311, 1915
3 Lamar RV, hleltzer SJ: Experimental pneumonia by in- trabroncbial insufflation. J Exp Med 15:133, 1912
4 Wollstein M, Meltzer SJ: Effect of intrabronchial insuffla- tion of solutions of some inorganic salts. J Exp Med 28:551, 1918
5 Winternitz MC, Smith GH: Intratracheal pulmonary ir- rigation. Contributions to Medical and Biological Re- search Dedicated to Sir William Osler 11. New York, Paul B. Hoeber 1919 p 1255
6 Vicente G: Sobre una technica simplificada en la terapeu- tica intrapulmonar. Rev Progr de la Clinica, julio 1928
7 Simenstad J, Calway C, MacLean L: The treatment of aspiration and atelectasis by tracheobronchial lavage. Surg Gynec Obvtet 115:721, 1962
8 Thompson HT, Pryor W: Bronchial lavage in the treat- ment of obstructive lung disease. Lancet 11: 8, 1964
9 Thompson HT, Pryor W, Hill J: Bronchial lavage in the treatment of obstructive lung disease. Thorax 21:557, 1966
10 Lefemine AA, Browning J, Stewart S: Bronchoscopy and bronchial lavage for obstructive ventilatory insufficiency. Ann Thracic Surg 4:308, 1967
11 Birley DM: The management of bronchial lavage. Bio- Med Eng 1 :346,1967
12 Cezeaux G, Telford J, Harrison G, et al: Bronchial lavage in cystic fibrosis. JAMA 199:73, 1967
13 Ramirez-R J, Schultz RB, Dutton RE: Pulmonary alveolar proteinosis. A new technique and rationale for treatment. Arch Int Med 112:419, 1963
14 Ramirez-R J, Campbell GD: Pulmonary alveolar pro- teinosis. Endobronchial treatment. Ann Int Med 63:429, 1965
15 Kylstra JA: Lavage of the lung. Acta Physiol Pharmacol Neerl7: 163, 1958
16 Kylstra JA: Lavage of the lung. 11. Acta Physiol Phar- macol Neerl8:326, 1959
17 Kylstra JA: Lavage of the lung. Trans Am Soc Art Intern Organs 5:23, 1959
18 Kylstra JA: Simplified technique of lavage of the lung. Results in dogs. Acta Physiol Pharmacol Neerl 9:225, 1960
19 Finley TN, Swenson EW, Curran WS, et al: Broncho- pulmonary lavage in normal subjects and patients with obstructive lung disease. Ann Int Med 66:651, 1967
20 Ramirez-R J: Pulmonary alveolar proteinosis. Treatment by massive bronchopulmonary lavage. Arch Int Med 119: 147, 1967
21 Kylstra JA, Rausch DC, Hall KD, et al: Volume-con- trolled lung lavage in the treatment of asthma, bronchiec- tasis, and mucoviscoidosis. Am Rev Resp Dis 103:651, 1971
22 Winternitz MC, Smith GH: Collected studies on the pathology of war gas poisoning. New Haven, Yale Uni- versity Press, 1920, p 145
23 Huber GL, Edmunds LH, Jr, Finley TN: Acute effects of saline lung washing on pulmonary mwhanics and mor- phology. Surg Forum 17: 113, 1966
24 Huber GL, Edmunds LH, Jr, Finley TN: Effect of ex- perimental saline lavage on pulmonary mechanics and morphology. Am Rev Resp Dis 104:337, 1971
25 Rogers RM, Tantum KR: Bronchopulmonary lavage. A "new" approach to old problems. Med Clin NA 54:755, 1970
26 Chinard FP: The permeability characteristics of the pul-
monary blood-gas bamer. In Caro CC ( e d ) : Advances in Respiratory Physiology. Baltimore, Williams and Wilkins, 1966, p 106-147
27 Taylor AE, Guyton AC, Bishop VS: Permeability of the alveolar membrane to solutes. Circulation Res 16:353, 1965
28 Wasserman K, Blank N, Fletcher G: Lung lavage (alveo- lar washing) in alveolar proteinosis. Am J Med 44:611, 1968
29 Smith JD, Millen EJ, Safar P, et al: Intrathoracic pres- sure, pulmonary vascular pressure and gas exchange dur- ing pulmonary lavage. Anesth 33:401, 1970
30 Ramirez-R J, Obenour WH Jr: Bronchopulmonary lavage in asthma and chronic bronchitis: Clinical and physiologic observations. Chest 59: 146, 1971
31 Rogers RM, Szidon JP, Shelburne J, et al: Hemodynamic response of the pulmonary circulation to bronchopul- monary lavage in man. New Eng J Med, in press
32 West JB, Dollery CT, Naimark A: Distribution of blood flow in isolated lung: Relation to vascular and alveolar pressures. J Appl Physiol 19:713, 1964
33 Banister J, Torrance RW: The effects of the tracheal pressure upon flow: Pressure relations in the va~cular bed of isolated lungs. Quart J Exp Physio145:352, 1960
34 Permutt S, Bromberger-Barnes B, Bane HN: Alveolar pressure, pulmonary venous pressure and the vascular waterfall. Med Thorac 19:239, 1962
35 Johnson JWC, Pemutt S, Sipple JH, et al: Effect of intra- alveolar fluid on pulmonary surface tension properties. J Appl Physiol 19:769, 1964
36 Pattle RE: Properties, function and origin of the alveolar lining layer. Nature, 175: 1125, 1955
37 Wetton R, Velasquez BJ, DuBois AB: Lung washings in living dogs: Surface activity in sedimentary fraction. J Appl Physiol22:372, 1967
38 Cavagna GA, Velasquez BJ, Wetton R, et al: Cellular absorption of pulmonary surface-active material. J Appl Physiol22 :982, 1967
39 Bondurant S, Miller DA: A method for protecting sur- face active extracts of mammalian lung. J Appl Physiol 17:167, 1962
40 Rogers RM, Sonne JE: Demonstration of surface active material in human lung lavage effluent. Clin Res 18:490, 1970
41 Rogers RM, Sonne JE, Shuman JF, et al: Immediate effects of saline lavage on pulmonary mechanics and gas exchange in patients with alveolar proteinosis and asthma. Clin Res 19:519, 1971
42 Rosen SH, Castleman B, Liebow AA: Pulmonary alveolar proteinosis. New Eng J Med 258: 1123, 1958
43 Ramirez-R J: Alveolar proteinosis: importance of pul- monary lavage. Am Rev Resp Dis 103:666, 1971
44 Ramirez-R J: Bronchopulmonary lavage. Dis Chest 50:581, 1966
45 Rogers RM, Shuman JF, Braunstein MS: The effects of bronchopulmonary lavage on pulmonary function in al- veolar proteinosis. In preparation
46 Bohrod MG: Pathologic manifestations of allergic and related mechanisms in diseases of the lungs. Int Arch Allergy 13:39, 1958
47 Broom B: Intermittent positive pressure respiration and therapeutic bronchial lavage in intractable status asth- maticus. Lancet 1 :899, 1960
48 Feldman R: Recognition and treatment of potentially fatal asthma. Ann Int Med 57:29, 1962
49 O'Brien MM, Ferguson MH: Unexpected death in bron-
CHEST, VOL. 62, NO. 5, NOVEMBER 1972 SUPPLEMENT (PART 2)
Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21550/ on 04/28/2017

ROGERS, BRAUNSTEIN, SHUMAN
chial asthma. A warning sign with a clinico-pathologic correlation. Ann Int Med 53: 1162, 1960
50 Hackett RR, Reas HW: A radical approach to therapy for the pulmonary complications of cystic fibrosis. Anesthesi- ology 26:248, 1965
51 Cezeaux G Jr, Telford J, Harrison G, et al: Bronchial lavage in cystic fibrosis. JAMA 199:73, 1967
52 Seard C, Wasserman K, Benfield JR, et al: Simultaneous bilateral lung lavage (alveolar washing) using partial cardiopulmonary bypass. Am Rev Resp Dis 101:877, 1970
53 Kylstra JA, Paganelli CV, Lanphier EH: Pulmonary gas exchange in dogs ventilated with hyperbarically oxy- genated liquid. J Appl Physio121: 177, 1966
54 Blenkarn GD, Hayes JA: Bilateral lung lavage with hyperbarically oxygenated saline in dogs. J Appl Physiol 29:786, 1970
55 Vital Statistics of the United States 1967. U.S. Depart- ment of Health, Education and Welfare, Washington, 1969
56 Tillotson JR, Lerner AM: Pneumonia caused by Gram- negative bacilli. Medicine 45:65, 1966
57 Pierce AK, Edmunson B, McGee G, et al: An analysis of factors predisposing to gram-negative bacillary necrotiz- ing pneumonia. Am Rev Resp Dis 94:309, 1968
58 Taylor RM: Experimental infection with influenza. A
virus in mice. The increase in intrapulmonary virus after inoculation and the influence of other factors thereon. J Exp Med 73:43, 1941
59 Harford CG: Influenza viral pneumonia of human beings. Am J Med 29:907, 1960
60 Pfleger RC, Wilson AJ, Cuddihy RG, et al: Bronchopul- monary lavage for removal of inhaled insoluble materials from the lung. Dis Chest 56:524, 1969
61 Fission Product Inhalation Program Annual Report 1970- 1971. Lovelace Foundation for Medical Education and Research, Albuquerque, New Mexico, November, 1971
62 Ramirez-R J: Pulmonary aspergilloma. Endobronchial treatment. New Eng J Med 271 :1281, 1964
63 Mendelson CL: The aspiration of stomach contents into the lungs during obstetric anesthesia. Am J Obstet Gynec 52:191, 1946
64 Teabeaut JR, 11: Aspiration of gastric contents: Experi- mental study. Am J Path 28:51, 1952
65 Bannister WK, Sattelaro AJ, Otis RD: Therapeutic as- pects of aspiration pneumonitis in experimental animals. Anesthesiology 22:440, 1961
66 Lewinski A: Evaluation of methods employed in the treatment of the chemical pneumonitis of aspiration. Anesthesiology 26:37, 1965
67 Awe WC, Fletcher WS, Jacob SW: The pathophysiology of aspiration pneumonitis. Surgery 60:232, 1966
CHEST, VOL. 62, NO. 5, NOVEMBER 1972 SUPPLEMENT (PART 2)
Downloaded From: http://journal.publications.chestnet.org/pdfaccess.ashx?url=/data/journals/chest/21550/ on 04/28/2017