Embed Size (px)
Citation preview

Role of Anticoagulants in ACS
Bashir Hanif, MD, FACC, FSCAIMedical Director
Chief of CardiologyTabba Heart Institute

Overview
• Brief Epidemiology and Pathophysiology
• Overview of Anticoagulants used in ACS
• Is there Evidence• What the Guidelines say?• Innovative Ideas from South Korea


* Based on data from the ARIC study of the National Heart, Lung, and Blood Institute, 1987-1994. Includes Americans hospitalized with definite or probable MI or fatal CHD, not including silent MIs. ACS indicates acute coronary syndrome; MI, myocardial infarction; ARIC, Atherosclerotic Risk in Communities; and CHD, coronary heart disease. From American Heart Association. Heart Disease and Stroke Statistics—2003 Update.
Epidemiology of ACS in the United States
• Single largest cause of death– 515,204 US deaths in 2000– 1 in every 5 US deaths
• Incidence– 1,100,000 Americans will have a new or recurrent
coronary attack each year and about 45% will die*– 550,000 new cases of angina per year
• Prevalence– 12,900,000 with a history of MI, angina, or both


Hospitalizations in the U.S. Due to ACS
Acute Coronary Syndromes*
1.57 Million Hospital Admissions - ACS
UA/NSTEMI† STEMI
1.24 million Admissions per year
0.33 million Admissions per year
*Primary and secondary diagnoses. †About 0.57 million NSTEMI and 0.67 million UA.Heart Disease and Stroke Statistics – 2007 Update. Circulation 2007; 115:69–171.

Causes of UA/NSTEMI*
• Thrombus or thromboembolism, usually arising on disrupted or eroded plaque– Occlusive thrombus, usually with collateral vessels†– Subtotally occlusive thrombus on pre-existing plaque– Distal microvascular thromboembolism from plaque-
associated thrombus – Thromboembolism from plaque erosion
• Non–plaque-associated coronary thromboembolism• Dynamic obstruction (coronary spasm‡ or
vascoconstriction) of epicardial and/or microvascular vessels
• Progressive mechanical obstruction to coronary flow• Coronary arterial inflammation• Secondary UA• Coronary artery dissection§
*These causes are not mutually exclusive; some patients have 2 or more causes. †DeWood MA, et al. N Engl J Med 1986;315:417–23. ‡May occur on top of an atherosclerotic plaque, producing missed-etiology angina or UA/NSTEMI. §Rare. Modified with permission from Braunwald E. Circulation 1998;98:2219–22. Anderson JL, et al. J Am Coll Cardiol. 2007;50:e1-e157, Table 3.

Plaque rupture
Platelet adhesion
Platelet activation
Partially occlusive arterial thrombosis & unstable angina
Microembolization & non-ST-segment elevation MI
Totally occlusive arterial thrombosis & ST-segment elevation MI
Pathogenesis of ACS
White HD. Am J Cardiol 1997;80 (4A):2B-10B.


Thrombus Formation and ACS
UA NQMI STE-MI
Plaque Disruption/Fissure/Erosion
Thrombus Formation
Non-ST-Segment Elevation Acute Coronary Syndrome (ACS)
ST-Segment Elevation (ACS)
Old Terminology:
NewTerminology:

Plaque RupturePlaque Rupture
ThrombusThrombus
Distal EmbolizationDistal Embolization Serotonin ReleaseSerotonin Release
VasoconstrictionVasoconstrictionMechanical PluggingMechanical Plugging
Mechanical Vasoconstrictive

The Role of the Platelet in Non-ST-segment The Role of the Platelet in Non-ST-segment Elevation Acute Coronary Syndromes Elevation Acute Coronary Syndromes
(NSTE ACS)(NSTE ACS)
The Role of the Platelet in Non-ST-segment The Role of the Platelet in Non-ST-segment Elevation Acute Coronary Syndromes Elevation Acute Coronary Syndromes
(NSTE ACS)(NSTE ACS)
Results from cross-linking of platelets by fibrinogen at
platelet receptors GP IIb-IIIaat site of plaque rupture
Platelet
Fibrinogen
Rupturedplaque
GP IIb-IIIa
Generally caused by partially-occlusive, platelet-rich thrombus in a coronary artery
Unobstructedlumen
Thrombus
Artery wall
Van de Werf F. Throm Haemost 1997;78(1):210-213.

The Role of the Thrombus in ST-segment Elevation MI (STEMI)
Results from stabilization by fibrin mesh of a platelet
aggregate at site of plaque rupture
platelet
RBC
fibrin mesh
Generally caused by a completely occlusive
thrombus in a coronary artery
Van de Werf F. Throm Haemost 1997;78(1):210-213.



Another Innovative IdeaNice way of Buttering!!!


Anticoagulants
• Heparins– Unfractionated heparin (UFH)– Low molecular weight heparin (LMWH)
• Enoxaparin, Dalteparin
• Factor X-A Inhibitor– Fondaparinux
• Direct Thrombin Inhibitors– Bivalirudin: reversible binding– Lepirudin: irreversible binding– Argatroban: reversible binding– Hirudin

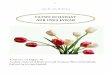
Anticoagulation is like a performance beam
Both efficacy and safety are important.
If you fail to balance efficacy and safety patient may get hurt
Anticoagulants and Gymnastics

Dose (concentration) of Anticoagulant
Optimal Safety and EfficacyThrombosis
Bleeding
The Search for an Anticoagulant That Balances Safety and Efficacy

Unfractionated Heparin
An unbranched heteropolysaccharide Chain

Unfractionated Heparin (UFH)
• Binds antithrombin & inhibits clotting factors Xa & IIa (thrombin)
• IV bolus followed by infusion, adjust according to aPTT or antifactor Xa levels
• Can be used in patients with renal dysfunction



Unfractionated Heparin (UFH)
• NSTE ACS– preferred anticoagulant following
angiography in patients undergoing CABG (Class 1)
– option for patients undergoing planned early angiography & revascularization (Class 1)
– may be used in patients in whom an initial conservative strategy is planned (Class 1)
• 1st line anticoagulant for STE ACS & PCI– administered with a fibrin selective
fibrinolytic (Class 1)

Unfractionated Heparin (UFH)
• Contraindications:– history of heparin induced
thrombocytopenia (HIT)– active bleeding– severe bleeding risk – recent stroke
• Adverse effects: – bleeding – HIT


Enoxaparin• Shorter chain length compared to UFH
– more predictable effects– Binds antithrombin, inhibits factors Xa & IIa
• Contraindications:– active bleeding, severe bleeding risk– history of HIT– recent stroke – CrCl < 15 ml/min– avoid in CABG patients
• Dose: 1 mg/kg every 12 hrs (renal adjustment required)
• Adverse effects: bleeding & HIT (lesser extent than UFH)

Enoxaparin• STEMI
– not studied in primary PCI (Class 2b as alternative to UFH)
• NSTEMI ACS– option for patients undergoing planned early
angiography and revascularization (Class 2a)• UFH recommended over enoxaparin or fondaparinux
(Class 1b)– may be used in patients in whom an initial
conservative strategy is planned (Class 1)• fondaparinux recommended over enoxaparin (Class
1a)• enoxaparin recommended over UFH (Class 1b)
Schünemann HJ, Hirsh J, Guyatt G, et al. Executive Summary: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest. 2008;133;71-109.

Comparison of LMWHs & UFHComparison of LMWHs & UFHComparison of LMWHs & UFHComparison of LMWHs & UFH
LMWHs UFH
MW 4,500-6,000 15,000 anti Xa:anti IIa 2:1 - 20:1 1:1
Bioavailability 85 - 95 % 30 %
Half - life 1.5 - 4.5 1 - 1.5 (dd)
APPT Monitoring NO YES
Non-specific binding ++ ++++
Incidence of HIT ++ +++
Inhibited by PF4 LESS YES

Limitations with Current Anticoagulation Therapy
Agent Disadvantages
Heparin • Parenteral administration• Risk of heparin-induced thrombocytopenia (HIT)• Narrow therapeutic window (low bioavailability,
short half-life)
Warfarin • Requires frequent monitoring due to:– Narrow therapeutic window– Unpredictable pharmacology – Multiple drug–drug and food–drug
interactions– Increased risk of major and minor bleeds
LMWH • Parenteral administration• Risk of heparin-induced thrombocytopenia (HIT)
Indirect Xa Inhibitor(e.g. fondaparinux)
• Parenteral administration• Long half-life• Limitations related to special patient
populations
Direct Thrombin Inhibitors
• Parenteral administration• Current applications limited to cardiovascular
managementAlbans S et al. Eur J Clin Invest 2005;35(Suppl 1):12-20.

Innovative IdeaTo overcome limitations!!!

The Evidence


RR: Death/MI
ASA Alone 68/655=10.4%
Heparin + ASA 55/698=7.9%
0.1 1 10
Summary Relative Risk
0.67 (0.44-0.1.02)
Theroux
RISC
Cohen 1990
ATACS
Holdright
Gurfinkel
Comparison of Heparin + ASA vs ASA Alone
ASA indicates acetylsalicylic acid; RISC, Research on InStability in Coronary artery disease; ATACS, Antithrombotic Therapy in Acute Company Syndromes; RR, relative risk; and MI, myocardial infarction.Data from Oler A, Whooley MA, Oler J, et al. Adding heparin to aspirin reduces the incidence of myocardial infarction and death in patients with unstable angina: a meta-analysis. JAMA. 1996;276:811-815. Slide reproduced with permission from Cannon CP. Atherothrombosis slide compendium. Available at: www.theheart.org.

Enoxaparin1mg/kg q 12 HSubcutaneous
+ ASA
Enoxaparin1mg/kg q 12 HSubcutaneous
+ ASA
UFHIV dose-adjusted
+ ASA
UFHIV dose-adjusted
+ ASA
Follow-up VisitDay 14
Follow-up VisitDay 14
Follow-up VisitDay 14
Follow-up VisitDay 14
Follow-up CallDay 30
Follow-up CallDay 30
Follow-up CallDay 30
Follow-up CallDay 30
Unstable AnginaNon-Q-Wave MI
Treatment Phasemin 48 H, max 8 Days
Follow-up Phase
ESSENCE: Study Design
Cohen, et al. NEJM 1997;337:447-52
(n=1564)
(n=1607)

30
25
20
15
10
Time (Days)
HeparinEnoxaparin
5
0
% D
eath
, M
I or
RA
1 3 5 7 9 11 13 15 17 19 21 23 2527 29 31
19.819.8%%
16.616.6%%RRR 16.2 RRR 16.2
% % P=0.019P=0.019
23.323.3%%
19.819.8%%RRR 15 % RRR 15 %
P=0.016P=0.016
ESSENCEAll Randomized
Cohen, et al. NEJM 1997;337:447-52

ESSENCE 1 Year Data
0
5
10
15
20
25
30
35
40
3 months 6 months 9 months 1 year
UFH Enoxaparin
% I
nci
den
ce o
f T
rip
le E
nd
poi
nt
p=0.023p=0.042
p=0.033p=0.022
Goodman SG, et al. JACC 2000;36:693-8
(n= 1564) (n=1607)

Fixed Dose
Placebo q 12 hr SC
Fixed Dose
Placebo q 12 hr SC
Enoxaparin30 mg IV bolus +
1mg/kg SC q 12 hr
UFH70 U/kg IV bolus +
15 U/kg/hr IV 72h
Fixed Dose < 65 kg > 65 kg 40 mg 60 mg
q 12 hr SCUnstable AnginaNon-Q Wave MI
24 h
Acute Phasemin 72H, max 8
Days
Chronic Phase
TIMI 11 BStudy Design
ASA
43 days
Antman et al, Circulation 1999;100:1593-601
(n=1953)
(n=1957)

Dea
th,
MI
or
Urg
ent
Rev
ascu
lari
zati
on
Unfractionated HeparinEnoxaparin (Lovenox)
Days
20
16
12
8
4
2 4 6 8 10 12 140
16.7%
14.2 %
p = 0.03
Relative Risk Reduction = 15%
TIMI 11B: Enoxaparin vs. Heparin in NSTE-ACSTIMI 11B: Enoxaparin vs. Heparin in NSTE-ACS
Adapted from Antman EM, et al. Circulation. 1999;100:1593-1601.

TIMI 11B-ESSENCE Meta-Analysis Death/MI
0.50.5 11 220.60.6 0.70.7 0.80.8 0.90.9Odds RatioOdds RatioEnox BetterEnox Better UFH BetterUFH Better
DayDayOROR % % pp
NN UFH(%)
UFH(%)
Enox (%)
Enox (%)
OVERALLOVERALL
ESSENCEESSENCE
TIMI 11BTIMI 11B
88
0.77(0.62-0.96)
0.77(0.62-0.96)
2323 0.020.0270817081
39103910
31713171
BB
BB
5.35.3 4.14.1
OVERALLOVERALL
ESSENCEESSENCE
TIMI 11BTIMI 11B
1414
0.79(0.65-0.96)
0.79(0.65-0.96)
2121 0.020.0270817081
39103910
31713171 BB
BB
6.56.5 5.25.2
OVERALLOVERALL
ESSENCEESSENCE
TIMI 11BTIMI 11B
4343
0.82(0.69-0.98)
0.82(0.69-0.98)
1818 0.020.0270817081
39103910
31713171 BB
BB
8.68.6 7.17.1



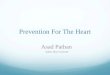
Enoxaparin in STEMI: ExTRACT-TIMI 25
STEMI < 6 hourslytic eligible
Lytic choice by physician (TNK,TPA, rPA, SK)
UFHbolus 60 U/kg infusion
12 U/kg/h for ≥ 48 hours
Enoxaparin< 75 y: 30 mg IV bolus
sc 1.0 mg/kg q 12h (Hosp DC)≥ 75 y: No bolus
sc 0.75 mg/kg q 12h (Hosp DC)CrCl ≤ 30: 1.0 mg/kg q 24 h
Double-blind double dummy phase
Day 30Primary Efficacy Endpoint: Death or non fatal MIPrimary Safety Endpoint: TIMI Major Hemorrhage
Acetylsalicylic acid (ASA)
TNK: Tenecteplase; TPA: Tissue plasminogen activator; rPA: Reteplase; SK: Streptokinase; UFH: Unfractionated heparin; CrCl: Creatinine clearance
STEMI: ST-segment elevation myocardial infarction;MI:Myocardialinfarction; TIMI:Thrombolysis in Myocardial Infarction

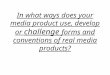
ExTRACT-TIMI 25Primary endpoint: Death or non fatal MI
RR: 0.83, (0.77–0.90)p<0.0001
Enoxaparin
UFH
0 5 10 15 20 25 30
Days
0
3
6
9
12
15
Pri
mary
En
dp
oin
t (
%)
RR: 0.90(0.80–1.01)
p=0.08
RR: 0.77(0.71– 0.85)p<0.0001
48 h 8 days
9.9%
12.0%
4.7%
5.2%
7.2%
9.3%
Lost to follow up = 3
206 events
*ITT: Intent-to-treat
Antman EM et al. for the ExTRACT-TIMI 25 Investigators. N Engl J Med 2006;354:1477-88

JAMA 2004

Innovative Idea!!!!

Fondaparinux
• Inhibits factor Xa and Thrombin– less likely to cause HIT than UFH,
LMWH
• STE ACS– alternative to UFH in patients not
undergoing reperfusion (Class 1) or receiving fibrinolytics (Class 2b)
– not recommended for use alone in 1˚ PCI (Class 1a)
Schünemann HJ, Hirsh J, Guyatt G, et al. Executive Summary: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines (8th Edition). Chest. 2008;133;71-109.


Fondaparinux
• NSTE ACS– option for patients undergoing
planned early angiography & revascularization with PCI
– option for patients in whom an initial conservative strategy is planned
– preferred agent for patients with high risk for bleeding (Class 1)

The OASIS 5 Study
N Engl J Med 2006;354:1464-76

OASIS 5: A Randomized, Double-Blind, Double-Dummy Trial
20,078 Patients with NSTE ACS, Chest discomfort < 24 hours2 of 3: Age>60, ST Segment Δ, cardiac markers
Fondaparinux2.5 mg subcut daily up to 8 days or hospital
discharge
Aspirin, Clopidogrel, GPIIb/IIIa inhibitor, planned Cath/PCI as per local practice
Randomization
Enoxaparin1 mg/kg subcut bid for 2-8 days
1 mg/kg subcut daily if ClCr<30mL/min
Michelangelo OASIS 5 Steering Committee. Am Heart J 2005;150:1107.e1-.e10 OASIS 5 Investigators. N Engl J Med2006;354: 1464-76
Mean treatment : 5.4 daysMean time to PCI: 2.4 days
ExcludeAge < 21Any contra-ind to EnoxHem stroke< 12 mo.Creat> 3 mg/dL/265 umol/L
Mean treatment : 5.2 daysMean time to PCI: 2.6 days


OAISIS - 6

LMWH: Advantages
• More predictable anticoagulant response
• Better bioavailability at low doses
• Dose-independent clearance mechanism
• Longer ½ life
• Less binding to plasma proteins and to proteins released from activated platelets and endothelial cells
• Less binding to endothelium
• Less binding to macrophages
• Less binding to macrophages

LMWH-Conclusion
• Use of LMWH has been established as a first-line choice in the treatment of UA/NSTEMI
• "increasing evidence suggests that it may supplant unfractionated heparin as an anticoagulant in the setting of PCI and STEMI."

Excellent Innovative Idea!!!!

Thrombin Inhibitors
Weitz JI, Buller HR Circulation 2002;8:1004

Direct Thrombin Inhibitors
• Developed to overcome the inability of the heparin antithrombin complex to inactivate bound thrombin
• Hirudin• Bivalirudin• Argatroban

Direct Thrombin Inhibitors
• Inhibit clot-bound & circulating thrombin• Does not bind plasma proteins• More predictable response than UFH• Antiplatelet activity• NSTE ACS
– Bivalirudin: option in patients undergoing planned early angiography & revascularization (Class 1)

Direct Thrombin Inhibitors• ACUITY trial (Acute Catheterization and Urgent
Intervention Triage StrategY) • Moderate to high risk patients with ACS
undergoing invasive intervention (n=13,819) evaluated after 1 year
• 3 groups: – bivalirudin– bivalirudin + GP IIb/IIIa inhibitor– heparin/enoxaparin + GP IIb/IIIa inhibitor
• Outcomes: death, MI, unplanned revascularization
White HD, Ohman EM, Lincoff AM, et al. Safety and efficacy of bivalirudin with and without glycoprotein IIb/IIIa inhibitors in patients with acute coronary syndromes undergoing percutaneous coronary intervention 1-year results from the ACUITY (Acute Catheterization and Urgent Intervention Triage strategy) trial. J Am Coll Cardio. 2008;52(10):807-14.

Direct Thrombin Inhibitors
• ACUITY results: – no difference in incidence of ischemic events
or mortality at 1 year between the 3 regimens
– 43% relative risk reduction for major bleeding in bivalirudin monotherapy group at 30 days compared to UFH or enoxaparin + GP IIb/IIIa inhibitor
– bilvalirudin alone can replace UFH or enoxaparin + GP IIb/IIIa inhibitor in moderate to high risk ACS patients undergoing PCI
White HD, Ohman EM, Lincoff AM, et al. Safety and efficacy of bivalirudin with and without glycoprotein IIb/IIIa inhibitors in patients with acute coronary syndromes undergoing percutaneous coronary intervention 1-year results from the ACUITY (Acute Catheterization and Urgent Intervention Triage strategy) trial. J Am Coll Cardio. 2008;52(10):807-14.


Metaanalysis of contemporary TrialsBivalirudin alone vs UFH/Enox +GpIIb/IIIa
• ACUITY- PCI• REPLACE II• PROTECT TIMI- 30

Concept of Biosimilarity

• Biologics are made from a variety of natural resources—human, animal, and microorganism—and may be produced by biotechnology methods– Epoetin – Insulin – Growth hormone (GH)– Granulocyte colony stimulating factor (G-CSF)– Cytokines– Low Molecular Weight Heparins
• Enoxaparin (e.g Clexane)• Dalteparin (e.g Fragmin)• Tinzaparin (e.g Innohep)
Concept of Biosimilarity

SASAT (South Asian Society on Atherosclerosis & Thrombosis) Recommendations
LMWHs are biological agents and therefore cannot be True Generics. Some substandard products were also withdrawn due to compositional variations
Efficacy and safety of biosimilar LMWH to originator
LMWH to be demonstrated through prospective, randomized double blind versus originator to show noninferiority or therapeutic equivalence
If a biosimilar does not satisfy the criteria defined for the full clinical trial or for the stringent pharmacokinetic assessments, it should therefore not be designated a biosimilar
NATF (North American Thrombosis Forum) Recommendations


Guidelines


ACC/AHA Recommendations for Antithrombin Therapy in Patients with
NSTE-ACS• Class I
– Anticoagulation with subcutaneous LMWH or intravenous UFH should be added to antiplatelet therapy
– Dose of UFH 60-70 U/kg (max 5000) IV followed by infusion of 12-15 U/kg/hr (initial max 1000 U/hr) titrated to aPTT 1.5-2.5 times control
– Dose of enoxaparin 1 mg/kg subcutaneously q12 hr; the first dose may be preceded by a 30-mg IV bolus
• Class IIa– Enoxaparin is preferable to UFH as an anticoagulant
unless CABG is planned within 24 hours
Available at: www.acc.org/clinical/guidelines/unstable/unstable.pdf.

Guidelines for the Use of Enoxaparin in Patients with NSTE-ACS
• 1 mg/kg SQ q12 hours (actual body weight)– An initial 30 mg IV dose can be considered
• Adjust dosing if CrCl <30 cc/min – 1 mg/kg SQ q24 hours
• Do not follow PTT; do not adjust based on PTT• Stop if platelets by 50% or below
100,000/mm3
• If patient to undergo PCI:– 0-8 hours since last SQ dose: no additional
antithrombin therapy– 8-12 hours since last SQ dose: 0.3 mg/kg IV
immediately prior to PCI

Guidelines - Anticoagulant TherapyAnticoagulant therapy should be added to antiplatelet therapy in UA/NSTEMI patients as soon as possible after presentation.
•For patients in whom a conservative strategy is selected, regimens using either enoxaparin* or UFH (Level of Evidence: A) or fondaparinux (Level of Evidence: B) have established efficacy. (Box C1)
•In patients in whom a conservative strategy is selected and who have an increased risk of bleeding, fondaparinux is preferable. (Box C1)
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
*Limited data are available for the use of other low-molecular-weight heparins (LMWHs), e.g., dalteparin.
New Drugs

Guidelines - Anticoagulant Therapy
For UA/NSTEMI patients in whom an initial conservative strategy is selected, enoxaparin* or fondaparinux is preferable to UFH as anticoagulant therapy, unless CABG is planned within 24 h.
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII
*Limited data are available for the use of other low-molecular-weight heparins (LMWHs), e.g., dalteparin.

Guidelines – Anticoagulants in ACS
b. If, after stress testing, the patient is classified as being at low risk (Box E2), the instructions noted below should be followed in preparation for discharge (Box K):
1. Continue ASA indefinitely. (Level of Evidence: A)
2. Continue clopidogrel for at least 1 month (Level of Evidence: A) and ideally up to 1 year. (Level of Evidence: B)
3. Discontinue IV GP IIb/IIIa inhibitor if started previously. (Level of Evidence: A)
4. Continue UFH for 48 h or administer enoxaparin or fondaparinux for the duration
of hospitalization, up to 8 d, and then discontinue anticoagulant therapy. (Level of Evidence: A)
III IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIII IIaIIaIIa IIbIIbIIb IIIIIIIIIIIaIIaIIa IIbIIbIIb IIIIIIIII


Key points
• In daily practice, you willencounter diverse antithrombin therapies.
• Current guidelines justify an array ofagents, depending on individual priorities.
• Workflow• Concomitant antiplatelet therapy• Cost• The penalties for switching are likely less
than once anticipated.

Do your choices effect outcomes?

Was it something I said?
Hope not!!!!!

Thank You for your attention

FOR