Embed Size (px)
DESCRIPTION
PCP as a Syndrome Pj CMV Bacteria TB Viruses
Citation preview

Robin J GreenPhD, DSc
New Insights into the Bugs in the Airway of HIV-infected Children with Lung Disease

The Diseases to Consider
PCPALRTIHIV-associated bronchiectasisBronchiolitis / Pneumonia
*
**
*
* No mention of TB
*

PCP as a Syndrome
Pj
CMV
Bacteria
TB
Viruses

Bacteria (blood culture): • 5 (7.9%) non-survivors • 8 (12.7%) survivors (p=0.508)
Bacteria (NBBAL): • 6 (9.5%) non-survivors • 13 (20.6%) survivors (p=1.00)
Bacterial Co-infection in PCP
Kitchin O, et al. Pediatr Crit Care Med 2012;13:517-9

Respiratory viruses: • 1 (1.6%) non-survivors • 8 (12.7%) survivors (p=0.256)
Viral Co-infection in PCP
Kitchin O, et al. Pediatr Crit Care Med 2012;13:517-9

Cytomegalovirus and Risk of Death
Kitchin O, et al. Pediatr Crit Care Med 2012;13:517-9
CMV Status Alive Dead Total
CMV (-) 25 (56.82) 3 (15.79) 28 (44.44)
CMV <log 4 8 (18.18) 3 (15.79) 11 (17.46)
CMV >log 4 11 (25) 13 (68.42) 24 (38.10)
Total 44 (100) 19 (100) 63 (100)
Fisher’s exact 0.002

Zampoli M, et al1 Goussard P, et al2 Kitchin P, et al3
n 202 25 63Age(months) 3,2 3.3 3,7HIV 61.4% 100% 84%Mortality 38% 72% 30%PJP(+)/CMV 36% 32% 33%Other viruses RSV, Adeno, PIV PIV3 RSV,PIV3, IV, Adeno
CMV(+) 66% 63% 55%CMV VL>log 4Culture(+)
35/47 (74%) 15/25 (60%) 24/63 (38%)
CMV> log4 (survived) 17/47(36%) ? 11/63(25%)
Treated 23/44 1/24 all IPPV in days ? 14.4 (5-31) 14.1 (10.4-17.9)CMV pn(deaths) ? 13.5 days 12.9 days
1. Zampoli M, et al. Pediatr Infect Dis J 2011;30:413–417 2. Goussard P, et al. Pediatr Pulmonol 2010; 45:650–655 3. Kitchin O, et al. Pediatr Crit Care Med 2012;13:517-9

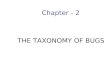
Serum Cytokines
IL-10 IL-1B IP-10 TNFa0
1000
2000
3000
4000
5000
6000
PCPBronchiectasis
P<.001
P=.0078
Green RJ, et al. J Antiviral Antiretroviral 2012;13:516-519

New Data from SBAH
Survival 5% in 2005Survival 70% in 2009Survival 82% in 2012 - 2015
Reasons for improved survival:Lung protective ventilationOral steroidsGanciclovirEarly ARV introduction (BUT NOT WITHOUT PRICE)
Cloete J, et al. S Afr J Child Health 2015;in press

ALRTI’sPneumonian = 58 (54.7%)
Bronchiolitisn = 48 (45.3%)
X2 p value
Cough 53 (91.4%) 46 (95.8%) 0.358Wheeze 14 (24.1%) 27 (56.3%) 0.001Shortness of breath 45 (77.6%) 38 (79.2%) 0.844
Fever 31 (53.4%) 29 (60.4%) 0.471Runny nose 22 (37.9%) 25 (52.1%) 0.144Nasal congestion 36 (62.1%) 31 (64.6%) 0.789Sneeze 18 (31.%) 18 (37.5%) 0.484Current antibiotics 49 (84.5%) 25 (52.1%) 0.001
HIV status 14 (24.1%) 1 (2.1%) 0.001
Abbott S, et al. SATS 2014

Viral Results
Abbott S, et al. SATS 2014
NS for all comparisonsRespiratory viruses identified in nasopharyngeal aspirates of cases and controls (n=158)

HRV Prevalence
Abbott S, et al. SATS 2014

Abbott S, et al. SATS 2014

HRV
Adeno
virus
RSV
Bocav
irus
Corona
virus
Parainf
luenz
a viru
s
Influe
nza v
irus
Metapn
uemov
irus
0.0
10.0
20.0
30.0
40.0
50.0
60.053.3
20.0
0.0
13.3
20.0 20.0
0.0
6.7
49.4
34.1 30.6
24.7
10.68.2 9.4
7.1
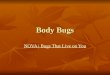
HIV-Infected (n=15)
HIV-Uninfected (n=85)
Per
cent
(%) w
ithin
HIV
-infe
cted
and
uni
nfec
ted
case
s P<0.001
Abbott S, et al. SATS 2014
Respiratory viruses identified in nasopharyngeal aspirates of HIV-infected and HIV-uninfected cases (n=100)

P<0.001
Sikazwe CT, et al. 9th International Respiratory Syncytial Virus Symposium 2014
RSV Viral Load

Sikazwe CT, et al. 9th International Respiratory Syncytial Virus Symposium 2014
RSV Subtypes and Disease

16s rRNA Bacterial Load in ALRTI’s
HIV-infected HIV-uninfected P HRV + HRV - P
7.22 X 106 4.93 X 106 0.047 5.95 X 106 3.96 X 106 0.049
Annamaly A, et al. ATS 2014
68% higher in HIV-infected children
67% higher in HRV-positive children

Abbott S, et al. SATS 2015
Cytokines in ALRTI’s HIV-infected vs. Uninfected• IL-13, IL-4, IL-5, TNF-α, IFN-α, IFN-γ,
MIP-1α significantly lower in HIV-infected cases
• IP-10 and MIG significantly higher in HIV-infected cases

HIV-associated Bronchiectasis
Masekela R, et al. SAMJ 2009;99:822-825 Masekela R, et al. IJTBLD 2012;16:114-119
Only one viral culture of Parainfluenza type 2

23
Haemophilus influenzae
Pseudomonas sp.
Vosloo S, et al 2015;unpublished
Bronchiectasis Airway Microbiome

Serum TREM-1
Masekela R, et al. Ped Pulmonol 2015;50:333-339

Conclusion
• Many childhood ALRTI’s have identifiable viral and bacterial organisms
• The relative contribution of each species to disease is not clear
• In HIV-infected children there is a greater relative abundance of bacteria, even in obvious viral disease
• Acute viral bronchiolitis (RSV) occurs less commonly in HIV-infected children …..

Conclusion• … But many normal children harbor viruses and bacteria
• Organisms in HIV-associated bronchiectasis are different to CF-associated bronchiectasis, possibly reflecting different immune responses
• Cytokine data does not support the pro/anti-inflammatory model (but IP-10 important in ALRTI’s)
All these conclusions may have implications for management and vaccine prevention

Thank You• Prof Refiloe Masekela
• Dr Teshni Moodley
• Dr Omolemo Kitchin
• Dr Salome Abbott
• Dr Alicia Annamaly / Prof Peter le Souef
• Dr Jeane Cloete
• Ms Solize Vosloo / Prof Fanus Venter
• Prof Max Klein