An Update on Statistical Issues Associated with the International Harmonization of Technical Standards for Clinical Trials (ICH). Robert O’Neill , Ph.D. Director, Office of Biostatistics, CDER, FDA. 22nd Spring Symposium, New Jersey Chapter of ASA, Wed. June 6,2001. Outline of talk. - PowerPoint PPT Presentation
template
An Update on Statistical Issues Associated with the
International Harmonization of Technical Standards for Clinical
Trials (ICH)
Robert ONeill , Ph.D.Director, Office of Biostatistics, CDER,
FDA
22nd Spring Symposium, New Jersey Chapter of ASA, Wed. June
6,2001
Outline of talk
International Harmonization of technical standards: efficacy,
safety, quality statistics - where does it fit inResources - who
are the people and what are the processesA focus on a few ICH
Guidances of interestA few issues of particular statistical
concernThe future - where do we go from here
Harmonization of technical standards
ICH (Europe, Japan, United States)Began in 1989; ICH 1 in Brussels
1991ICH continues todayOutside of ICHAPEC - Bridging study
initiative , Teipei meetingCanada, observers, WHO
Statistical Resources in the ICH regions
United StatesCDER, CBEREuropeU.K., Germany, SwedenCPMPJapanMHW;
advisors, universityChina, Taiwan, Canada, Korea
Web addresses for information and guidances
www.fda.gov/cder/guidance/index.htmwww.ifpma.org/ich1www.emea.eu.int/
ICH Guidances with statistical content
E1; Extent of population exposure to assess clinical safetyE3;
structure and content of clinical study reports (CONSORT
statement)E4; Dose-response information to support drug
registrationE5; Ethnic factors in the acceptability of foreign
clinical dataE9; Statistical principles for clinical trialsE10;
Choice of control groupE11; Clinical investigation of medicinal
products in the pediatric population
ICH Guidances with statistical content
SafetycarcinogenicityQualityStability (expiration dating) : Q1A,
Q1E
New initiatives from the European Regulators (CPMP)- Points to
Consider Documents
On Validity and Interpretation of Meta-Analyses, and One Pivotal
Study (Jan, 2001)On Missing Data (April, 2001)On Choice of deltaOn
switching between superiority and non-inferiority On some
multiplicity issues and related topics in clinical trials
Efficacy Working Party (EWP) Points to ConsiderCPMP/EWP/1776/99
Points to Consider on Missing Data (Released for Consultation
January 2001) CPMP/EWP/2330/99 Points to Consider on Validity and
Interpretation of Meta-Analyses, and one Pivotal study ( released
for consultation October 2000) CPMP/EWP/482/99 Points to Consider
on Switching between Superiority and Non-inferiority (Adopted July
2000)
ICH E9Statistical Principles for Clinical Trials: Contents
Introduction ( Purpose, scope, direction )Considerations for
Overall Clinical DevelopmentStudy Design ConsiderationsStudy
ConductData AnalysisEvaluation of safety and
tolerabilityReportingGlossary of terms
Study Design: A Major Focus of the Guideline
Prior planningProtocol considerations
Prospective Planning
Design of the trialAnalysis of outcomes
Confirmatory Study vs. Exploratory Study
A hypothesis stated in advance and evaluatedData driven
findings
Design Issues
EndpointsComparisonsChoice of study typeChoice of control
groupSuperiorityNon-inferiorityEquivalenceSample sizeAssumptions,
sensitivity analysis
Choice of Study Type
Parallel group designCross-over designFactorial designMulticenter
design
Analysis: Outcome Assessment
Multiple endpointsAdjustments
Assessing Bias and Robustness of Study Results
Analysis sets
Analysis Sets
ITT principleAll randomized populationFull Analysis populationPer
Protocol
Data Analysis Considerations
Prespecification of the AnalysisAnalysis setsFull analysis setPer
Protocol SetRoles of the Different Analysis SetsMissing Values and
Outliers
Statistical Analysis Plan (SAP)
A more technical and detailed elaboration of the principal features
stated in the protocol.Detailed procedures for executing the
statistical analysis of the primary and secondary variables and
other data.Should be reviewed and possibly updated during blind
review, and finalized before breaking the blind.Results from
analyses envisaged in the protocol (including amendments) regarded
as confirmatory.May be written as a separate document.
Analysis Sets
The ideal: the set of subjects whose data are to be included in the
analysis:all subjects randomized into the trialsatisfied entry
criteriafollowed all trial procedures perfectlyno loss to
follow-upcomplete data records
Used to describe the analysis set which is complete as possible
and as close as possible to the intention to treat principleMay be
reasonable to eliminate from the set of ALL randomized subjects,
those who fail to take at least one dose, or those without data
post randomization.Reasons for eliminating any randomized subject
should be justified and the analysis is not complete unless the
potential biases arising from exclusions are addressed and
reasonably dismissed.
Full Analysis Set
Sometimes described as:Valid cases, efficacy sample, evaluable
subjectsDefines a subset of the subjects in the full analysis
setMay maximize the opportunity for a new treatment to show
additional efficacyMay or may not be conservativeBias arises from
adherence to protocol related to treatment and/or outcome
Per Protocol Set
Advantageous to demonstrate a lack of sensitivity of the
principal trial results to alternative choices of the set of
subjects analyzed.The full analysis set and per protocol set play
different roles in superiority trials, and in equivalence or
non-inferiority trials.Full analysis set is primary analysis in
superiority trials - avoids optimistic efficacy estimate from per
protocol which excludes non-compliers. Full analysis set not always
conservative in equivalence trial
Roles of the Different Analysis Sets
Impact on Drug Development
On sponsor design and analysis of clinical trials used as evidence
to support claimsOn regulatory advice and evaluation of sponsor
protocols and completed clinical trialsOn maximizing quality and
utility of clinical studies in later phases of drug developmentOn
multidisciplinary understanding of key concepts and issues Enhanced
attention to planning and protocol considerations
Will the Guideline Help to Avoid Problem Areas in the Future -
Maybe !
Not a substitute for professional advice-will require professional
understanding and implementation of the principles statedWill not
assure correct analysis and interpretationMost of the guideline
topics reflect areas where problems have been observed frequently
in clinical trials in drug development
ICH : Chemistry
Q1E: Bracketing and Matrixing Designs for Stability Testing of Drug
Substances and Drug Products:Considerable new work, including
extensive simulations to evaluate size of studies and the ability
to detect important changes to expiration date setting (incomplete
blocks, alias, etc).
ICH E10: Choice of Control Group and Related Design Issues in
Clinical Trials
Section 1.5 is very statistically oriented involving issues
like:Assay sensitivtyHistorical evidence of sensitivity to drug
effectsChoice of a margin for a non-inferiority (dont show a
difference ) trial.
Assay Sensitivity in Non-inferiority designs
Assay sensitivity is a property of a clinical trial defined as the
ability to distinguish an effective treatment from a less effective
or ineffective treatmentNote that this property is more than just
the statistical power of a study to demonstrate an effect - it also
deals with the conduct and circumstances of a trial
The presence of assay sensitivity in a non-inferiority trial may
be deduced from two determinations
1) Historical evidence of sensitivity to drug effects, I.e., that
similarly designed trials in the past regularly distinguished
effective treatments from less effective or ineffective treatments,
and2) Appropriate trial conduct, I.e. that the conduct of the trial
(current) did not undermine its ability to distinguish effective
treatments from less effective or ineffective treatments. [can be
fully evaluated only after the active control non-inferiority trial
is completed.]
Successful use of a non-inferiority trial thus involves four
critical steps
1) Determining that historical evidence of sensitivity to drug
effect exists. Without this determination, demonstration of
efficacy from a showing of non-inferiority is not possible and
should not be attempted.2) Designing a trial. Important details of
the trial design, e.g. study population, concomitant therapy,
endpoints, run-in periods, should adhere closely to the design of
the placebo-controlled trials for which historical sensitivity to
drug effects has been determined.
Successful use of a non-inferiority trial thus involves four
critical steps (cont.)
3) Setting a margin. An acceptable non-inferiority margin should be
defined, taking into account the historical data and relevant
clinical and statistical considerations.4) Conducting the trial.
The trial conduct should also adhere closely to that of the
historical trials and should be of high quality.
Choosing the Non-inferiority margin
Prior to the trial, a non-inferiority margin, sometimes called a
delta, is selected.This margin is the degree of inferiority of the
test treatments to the control that the trial will attempt to
exclude statistically.The margin chosen cannot be greater than the
smallest effect size that the active drug would be reliably
expected to have compared with placebo in the setting of the
planned trial. [based on both statistical reasoning and clinical
judgement, should reflect uncertainties in evidence and be suitably
conservative.]
Outline of the Issues
What is the the non-inferiority designWhat are the various
objectives of the designComplexities in choosing the margin of
treatment effect - it depends upon the strength of evidence for the
treatment effect of the active controlLiterature on historical
controls, and on the heterogeneity of treatment effects among
studiesThe statistical approaches to each objective, and their
critical assumptionsCautions and concluding remarks
Non-Inferiority Design
A study design used to show that a new treatment produces a
therapeutic response that is no less than a pre-specified amount of
a proven treatment (active control), from which it is then inferred
that the new treatment is effective. The new treatment could be
similar or more effective than the existing proven treatmentA
non-inferiority margin is pre-selected as the allowable reduction
in therapeutic response. The margin is chosen based on the
historical evidence of the efficacy of the active control and other
clinical and statistical considerations relevant to the new
treatment and the current study.ICH - E10: This delta can not be
greater than the smallest effect size that the active drug would be
reliably expected to have compared with placebo in the setting of a
planned trial. - the concept of reliably and repeatedly being able
demonstrate a treatment effect of a specified size !
Non-Inferiority Design (contd)
A test treatment is declared clinically non-inferior to the active
control if:the trial has the necessary assay sensitivity for the
trial to be valid for non-inferiority testingthe one-sided 97.5
confidence interval is entirely to the right of -
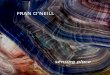
Inference for Non-Inferiority
Delta Limits & 95% Confidence Intervals
0
Control Better
Test Agent Better
Non-inferiority shown
Non-inferiority shown
Non-inferiority not shown
Non-inferiority shown/superiority could be claimed
-
Treatment Difference
What are the various objectives of the non-inferiority
design
To prove efficacy of test treatment by indirect inference from the
active control treatmentTo establish a similarity of effect to a
known very effective therapy - e.g. anti-infectivesTo infer that
the test treatment would have been superior to an imputed placebo ;
ie. had a placebo group been included for comparison in the current
trial. - a new and controversial area - choice of margin is the
key
What is the Evidence supporting the treatment effect of the
active control, and how convincing is it ?
Large treatment effects vs. small or modest effectsLarge treatment
effects - anti-infectivesModest treatment effects - difficulties in
reliably demonstrating the effect - Sensitivity to drug
effectsAmount of prior study data available to estimate an
effectOne single studySeveral studies, of different sizes and
qualityNo estimate or study directly on the comparator - standard
of care
How is the margin chosen based upon prior study data
For a large treatment effect, it is easier - a clinical decision of
how similar a response rate is needed to justify efficacy of a test
treatment - e.g. anti-infectives is an example.For modest and
variable effects, it is more difficult ; and some approaches
suggest margin selection based upon several objectives.
Complexities in choosing the margin (how much of the control
treatment effect to give up)
Margins can be chosen depending upon which of these questions is
addressed:how much of the treatment effect of the comparator can be
preserved in order to indirectly conclude the test treatment is
effective - a clinical decision for very large effects; a
statistical problem for small and modest effectshow much of a
treatment effect would one require for the test treatment to be
superior to placebo, had a placebo been used in the current active
control study - a lesser standard than the above
How convincing is the prior evidence of a treatment effect
?
Do clinical trials of the comparator treatment consistently and
reliably demonstrate a treatment effect - when they do not, what is
the reason ?Study is too small to detect the effect - under powered
for a modest effect sizeThe treatment effect is variable, and the
estimate of the magnitude will vary from study to study, sometimes
with NO effect in a given study - a BIG problem for active
controlled studies (Sensitivity to drug effect)
How do you know which treatment effect size is appropriate for
the current active control ?
How much protection should be built into the choice of the
margin to account for unknown bias and uncertainty in study
differences ?
Inherently, the answer relies upon historical controls and their
applicability to the current study
Choice of the margins should take into account all sources of
variability as well as the potential biases associated with
non-comparability of the current study with the historical
comparisons.A need to balance the building in of bias in the
comparison and quantifying the amount of treatment effect
preserved, as a function of the relative amount of data from the
historical studies and the current study
Use of historical controls in current RCTs
Pocock,S. The combination of randomized and historical controls in
clinical trials. J. Chronic Diseases 1976, 29 pp.175-188Lists 6
conditions to be met for valid use of historical controls with
controls in current trialOnly if all these conditions are met can
one safely use the historical controls as part of a randomized
trial. Otherwise, the risk of a substantial bias occurring in
treatment comparisons cannot be ignored.
Importance of the assumption of constancy of the active control
treatment effect derived from historical studies
It is relevant to the design and sample size of the current study,
to the choice of the margin, to the amount of bias built into the
comparisons, to the amount of effect size one can preserve (both of
these are likely confounded), and to the statistical uncertainty of
the conclusion.Before one can decide on how much of the effect to
preserve, one should estimate an effect size for which there is
evidence of a consistent demonstration that effect size
exists.
Explaining Heterogeneity among independent studies : Lessons
from meta-analyses
Variation in baseline risk as an explanation of heterogeneity in
meta-analysis, S.D. Walter, Stat. In Medicine, 16, 2883-2900
(1997)An empirical study of the effect of the control rate as a
predictor of treatment efficacy in meta-analysis of clinical
trials, Schmid,Lau,McIntosh and Cappelleri, Stat. In Medicine, 17,
1923-1942 (1998)
Explaining Heterogeneity among independent studies : Lessons
from meta-analyses (cont.)
Explaining heterogeneity in meta-analysis: a comparison of methods.
Thompson and Sharp, Stat. In Medicine, 18, 2693-2708
(1999)Assessing the potential for bias in meta-analysis due to
selective reporting of subgroup analyses within studies. Hahn,
Williamson, Hutton, Garner and Flynn, Stat. In Medicine, 19,
3325-3336 (2000)
Explaining Heterogeneity among independent studies : Lessons
from meta-analyses (cont.)
Large trials vs. meta-analysis of smaller trials - How do their
results compare ? Cappelleri, Ioannidis, Schmid, de Ferranti,
Aubert, Chalmers, Lau. JAMA, 16 1332-1338, 1996Discordance between
meta-analysis and large-scale randomized controlled trials:
examples from the management of acute myocardial infarction. Borzak
and Ridker, Ann. Internal Med.,123, 873-877 (1995)Discrepancies
between meta-analysis and subsequent large randomized controlled
trials. LeLorier, Gregoire, Benhaddad, Lapierre,Derderian. NEJM,
337, 536-42 (1997)
Use of meta-analysis - necessary but not sufficient
Distinguish under powered studies from well powered studies for a
common effect size - if possibleHow many trials are consistent with
no effect, rather than an effect of some sizeDetermine between
trial variability as an additional factor to consider in choosing a
conservative marginHow do you know if the current study comes from
the same trial population, and where does it rest in the trial
distribution - critical to assumptions for control group rate and
constancy of treatment effectResorting to meta-analysis of all
studies, when few individual studies reject null, tells you
something !
Three approaches to the problem
Indirect confidence interval comparisons (ICIC) (CBER/FDA type
method, etc.) - thrombolytic agents in the treatment of acute
MIVirtual method (Hasselblad & Kong, Fisher, etc.) -
Clopidogrel, aspirin, placebo
Bayesian approach (Gould, Simon, etc.)- treatment of unstable
angina and non-Q wave MI
When may it not be possible to estimate a margin or to use the
non-inferiority design to infer efficacy ?
There is a known creep in the standard of care over time and/or the
active control treatment, which renders any past estimates of
active control treatment effects not comparable or valid for the
current comparison, under conditions of medical practice in the new
current studye.g. use of surfactants in neonatal
treatment
ICH E5
Ethnic Factors in the Acceptability of Foreign Clinical
Data
Key Features of E5
Operational definition of ethnic factorsClinical Data Package
Fulfilling Regulatory Requirements in New RegionExtrapolation of
Foreign Clinical Data to New Region (role of ethnic
factors)Bridging StudiesGlobal Development Strategies
Ethnic Factor Definition
intrinsic factors: characteristics associated with the drug
recipient (ADME studies)race, age, gender, organ dysfunction,
genetic polymorphismextrinsic factors: characteristics associated
with the environment and culture in which one lives (clinical
outcomes)clinical trial conduct, diet, tobacco and alcohol use,
compliance with prescribed medications
Assessing a medicines sensitivity to ethnic factors(part of the
screening process)
Properties of a compound making it more likely to be
sensitive:Metabolism by enzymes known to show genetic
polymorphismHigh likelihood of use in a setting of multiple
co-medications
Assessment of the Clinical Data Package (CDP) for
acceptability
Question 1: Meets regulatory requirements - yes/noQuestion 2:
Extrapolation of foreign data appropriate - yes/noQuestion 3:
Further clinical study (ies) needed for acceptability by the new
region - yes/noQuestion 4: Acceptability in the new region -
yes/no
Meets regulatory requirements
Issues of evidenceConfirmatory evidence; two or more studies
showing treatment effectsInterpreting results of foreign clinical
trials which provide that evidence (may be one study, or all
studies, or part of a study)Which study designs provide
evidenceActive control / non-inferiority designsPlacebo or active
control / show a difference designs
The sources of data for an application (implementation)
All clinical studies for efficacy performed in foreign regionOne
study in the United States, one or more foreign clinical
studiesMulti-center/ multi-region clinical trials form the basis
for efficacy
Considerations for evaluating clinical efficacy between
regions
Study design differences Magnitude of treatment effect sizesEffect
size variability; subgroup differencesImpact of intrinsic factors -
determined when ?Impact of Extrinsic factorstrial conduct and
monitoringusage of concomitant medicationsprotocol
adherence
Bridging Studies
WhenWhyWhat type
E5 is purposely vague on how to do this or what their design should
be
Study design and study objectives(need examples and
experience)
What type of bridging study would be helpful for extrapolation
-PK/PDAnother clinical trial of the primary clinical
endpointequivalence/non-inferiority: treatment effect acceptably
close - margin or deltadose response study superiority design -
estimate treatment effect size for comparison
E5 allows for a new study in the new region - why is that needed
?
When all the clinical data is derived from a foreign region and
extrapolation is an issueWhen the experience with clinical trials
in that region is minimalWhen there is concern with ability to
confirm a finding from a study(ies)A confirmatory clinical trial is
the bridging study
Developmental Strategies for Global Development
Early vs. later strategiesDesigning population pk/pd into clinical
studiesPlanning to explain effect size differences among
regionsDesign of bridging studies early in development
Study Design
Better planning in Phase I, II, III and more efficient study
designs to address several subgroup questions simultaneouslyDesign
Phase III with some knowledge of PK / PD differences in Phase I /
IIAddress multiple questions simultaneously for efficiency (age,
gender, ethnic)
Study Design
Assessing the influence of ethnic factors in each study Phase (I,
II, III) and to identify earlier and account for, by design, the
influence of ethnic factorsEthnic factors as another subgroupAge,
gender, renal status, etc.Ethnic factors integrated withDose
responseGeriatricsPopulation exposure for safety
Remarks
Little experience at this time with bridging studiesLittle
experience with Japanese trials in NDA applications, or trials from
AsiaMore experience with foreign trials from Europe - possible
heterogeneity of treatment effects being evaluated; concern for
experience in new regions like Eastern Europe
The future
Appears to be increasingly dependent on statistical input, methods,
study design, interpretation , etc.Statistical resources (people)
are needed in the regulatory agencies in all countries/regions
serious about inference - not always present , maintained - cannot
develop guidance documents and consensus positions without this,nor
rely on guidances aloneGlobal drug development is beginning to
recognize the need for early planning for multi-regional inference
- the questions and study designs are just unfolding