-
journal of orthopaedic & sports physical therapy | volume 40
| number 3 | march 2010 | 133
[ research report ]
1Associate Professor, University of Puget Sound, School of
Physical Therapy, Tacoma, WA. 2Assistant Professor, US Army-Baylor
University Doctoral Program in Physical Therapy, Fort Sam Houston,
TX. 3Physical Therapy Element Chief, United States Air Force,
Sheppard Air Force Base, TX. 4Director of Rehabilitation
Department, Northern Navajo Medical Center, Shiprock, NM.
5Associate Professor, Department of Physical Therapy, Texas State
University, San Marcos, TX. This study was approved by The
Institutional Review Boards of Brooke Army Medical Center and
Wilford Hall Medical Center. The opinions or assertions contained
herein are the private views of the authors and are not to be
construed as official or as reflecting the views of the Departments
of the Army, Air Force, or Defense. Address correspondence to Dr
Robert E. Boyles, Associate Professor, University of Puget Sound,
School of Physical Therapy, 1500 N Warner St, #1070, Tacoma, WA
98416. E-mail: [email protected]
RobeRt e. boyles, PT, DSc1 • Michael J. Walker, PT, DSc2 • Brian
a. Young, PT, DSc3 Joseph B. strunce, PT, DSc4 • roBert s. Wainner,
PT, PhD5
The Guide to Physical Therapist Prac-tice1 outlines several
physical therapy interventions suitable for the manage-ment of
patients with mechanical neck pain. These interventions include
man-ual physical therapy, exercise, traction, physical agents, and
mechanical and electrotherapeutic modalities.1 Despite their common
use, existing research has produced insufficient evidence regarding
the effectiveness of these interventions and the clinical
decision-making strate-gies to guide their use.15-18 Current best
evidence supports the multimodal use of manual physical therapy
(MPT), includ-
Mechanical neck pain is defined as pain that can be provoked by
neck movements or
provocative tests.2 Neck pain is a common musculoskeletal
complaint, with a reported lifetime prevalence of 22% to 67%10 and
a point prevalence of 13% to 22%.34 Up to 41% of patients with neck
pain seek care from a general practitioner and 33% from a physical
therapist.31
The Addition of Cervical Thrust Manipulations to a Manual
Physical Therapy Approach in Patients Treated for Mechanical
Neck Pain: A Secondary Analysis
t stuDY Design: Secondary analysis of a randomized clinical
trial (RCT).
t oBJectiVes: To perform a secondary analysis on the treatment
arm of a larger RCT to determine differences in treatment outcomes,
adverse reac-tions, and effect sizes between patients who re-ceived
cervical thrust manipulation and those who received only nonthrust
manipulation as part of an impairment-based, multimodal treatment
program of manual physical therapy (MPT) and exercise for patients
with mechanical neck pain.
t BackgrounD: A treatment regimen of MPT and exercise has been
effective in patients with mechanical neck pain. Limited research
has com-pared the effectiveness of cervical thrust manipu-lations
and nonthrust mobilizations for this patient population, and no
studies have investigated the added benefit of cervical thrust
manipulations as part of an overall MPT treatment plan.
t MethoDs: Treatment outcomes from 47 patients in the treatment
arm of a larger RCT, with a primary complaint of mechanical neck
pain, were analyzed. Twenty-three patients (49%) received cervical
thrust manipulations as part of their MPT treatment, and 24
patients (51%) received only cer-vical nonthrust mobilizations. All
patients received up to 6 clinic sessions, twice weekly for 3
weeks, and a home exercise program. Primary outcome measures were
the Neck Disability Index (NDI), 2
visual analog scales for cervical and upper extremity pain, and
a 15-point global rating of change scale. Blinded outcome
measurements were collected at baseline and at 3-, 6- and 52-week
follow-ups.
t results: Consistent with the larger RCT, both subgroups in
this secondary analysis demonstrat-ed improvement in short- and
long-term pain and disability scores. Low statistical power (β.28)
and the resultant small effect size indices (–0.21 to 0.17)
preclude the identification of any between-group differences. No
serious adverse reactions were reported by patients in either
subgroup.
t conclusions: Clinically meaningful and statistically
significant improvements in both sub-groups of patients over time
suggest that cervical thrust manipulation, as part of the MPT
treatment plan, did not influence the results of the treatment arm
of the larger RCT from which this study was drawn. Although no
between-group differences can be identified, the small observed
effect sizes in this study may benefit future studies with sample
size estimation for larger RCTs and indicate the need to
incorporate clinical prediction rule criteria as a means to improve
statistical power.
t leVel oF eViDence: Therapy, level 4. J Orthop Sports Phys Ther
2010;40(3):133-140. doi:10.2519/jospt.2010.3106
t keY WorDs: cervical spine, manual therapy, mobilization
ing cervical thrust and/or non-thrust manipulation, and exercise
for patients with cervicogenic
headache and mechanical neck pain.5,17,18 Hoving et al21,22 and
Korthals-de Bos et al28 reported
SUPPLEMENTAL VIDEO ONLINE
40-03 Boyles.indd 133 2/17/10 2:49:30 PM
-
134 | march 2010 | volume 40 | number 3 | journal of orthopaedic
& sports physical therapy
[ research report ]
examination of the cervical spine and upper quarter prior to
randomization, where demographic information, self-report measures,
and physical exam measurements (ie, cervical range of mo-tion,
passive accessory mobility and pain provocation testing, cervical
special test-ing, etc) were collected. The self-report scores from
the 47 patients (31% female; mean SD age, 48.8 14.1 years)
as-signed to the MPT and exercise group of the RCT were analyzed
for the purposes of this secondary analysis.
interventionsPatients within the treatment arm re-ceived MPT and
exercise directed at im-pairments of the cervical spine, thoracic
spine, and adjacent ribs, as identified by the treating physical
therapist. The spe-cific manual interventions applied (which
included the use of thrust and nonthrust techniques) and the
intervention param-eters used (grade, duration, and repeti-tions)
were solely based on the clinical reasoning and decision making of
the treating therapists. Although numerous cervical manipulative
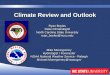
techniques exist, 2 techniques were predominantly used. Spinal
stiffness in flexion, described as “opening restrictions,” was
treated in flexion with a translatory thrust gapping manipulation
applied to the contralater-al side of the restricted motion segment
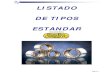
(Figure 1 , online ViDeo). Spinal stiffness in extension, described
as “closing restric-tions,” was treated in extension with a
caudally and slightly medially directed
an impairment-based, multimodal treat-ment program of MPT and
exercise for patients with mechanical neck pain.
MethoDs
subjects
ninety-four patients referred to 3 outpatient military treatment
facilities with a primary complaint
of neck pain were included in the initial multicenter RCT.38
Inclusion criteria for this RCT were the following: a primary
complaint of neck pain, with or without unilateral upper extremity
symptoms; age greater than 18 years; a Neck Disabil-ity Index (NDI)
score equal to or greater than 10 points; and a composite visual
analog scale (VAS) pain score equal to or greater than 30 mm, as
derived from 3 separate 100-mm pain scales measuring the patient’s
cervical, upper extremity, and average 24-hour pain scores.
Patients were excluded if they had a whiplash in-jury within the
past 6 weeks, a history of spinal tumors, spinal infection,
cervical spine fracture, or previous neck surgery, a pending legal
action regarding their neck pain, a diagnosis of central cervical
spinal stenosis, bilateral upper extremity symp-toms, or 2 positive
neurological findings at the same nerve root level.
Eligible patients were randomly as-signed to 2 treatment groups:
MPT and exercise (n = 47) or minimal interven-tion (n = 47). Each
patient underwent a standardized history and physical
superior patient perceived recovery and cost effectiveness when
using cervical nonthrust manipulations as compared to general
practitioner care or physical therapy that did not include
nonthrust manipulations for patients with neck pain greater than 2
weeks in duration. Cervical thrust manipulation and exercise
resulted in better patient outcomes and satisfaction levels when
compared to the use of manipulation or exercise alone.3,12 In a
recent randomized controlled trial, Walker et al38 compared the
effectiveness of MPT and exercise to a minimal in-tervention
approach in 94 patients with acute, subacute, or chronic mechanical
neck pain with or without upper extrem-ity symptoms. Unlike
previous studies, the MPT techniques included both thrust and
nonthrust manipulations applied to the cervical spine, thoracic
spine, and ad-jacent ribs. Walker et al33 demonstrated significant
short-term (3- and 6-week) and long-term (1-year) improvements in
pain, disability, and patient perceived recovery following up to 6
treatment ses-sions consisting of a multimodal use of MPT and
exercise.
Three studies4,23,37 have directly com-pared the effectiveness
of cervical thrust manipulation versus nonthrust manipu-lation for
the treatment of patients with acute, subacute, and chronic neck
pain. No differences in short- and long-term pain relief and
disability were reported in these trials when comparing these MPT
interventions.18 Despite these similar re-sults, Hurwitz et al24
reported that adverse reactions were more common in patients
following cervical thrust manipulation, and that these adverse
reactions negatively affected patient satisfaction, perceived
im-provement, and pain and disability scores at subsequent
follow-up visits.
The purpose of this study was to per-form a secondary analysis
on the treat-ment arm of a larger RCT38 to determine differences in
treatment outcomes, ad-verse reactions, and effect sizes between
patients who received cervical thrust manipulation and those who
received only nonthrust manipulation, as part of
Figure 1. Cervical thrust gapping manipulation in flexion for
left C4-5 opening restriction (online ViDeo).
Figure 2. Cervical thrust manipulation in extension for right
C4-5 closing restriction (online ViDeo).
40-03 Boyles.indd 134 2/17/10 2:49:31 PM
-
journal of orthopaedic & sports physical therapy | volume 40
| number 3 | march 2010 | 135
thrust to the ipsilateral dysfunctional seg-ment (Figure 2,
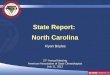
online ViDeo). Additionally, and to a lesser extent, a
nonphysiologic, or upslope, thrust manipulation tech-nique was used
at the treating therapist’s discretion (Figure 3, online
ViDeo).
In addition to MPT, all patients re-ceived 3 basic clinic and
home exercises: cervical rotation range of motion, cervi-cal
retraction (chin tucks), and deep neck
flexor strengthening. The therapist could add additional
exercises as needed to tar-get specific impairments or reinforce
the manual interventions. Patients received up to 6 sessions, twice
weekly for 3 weeks. Treatment sessions were limited to 1 hour for
the initial examination and treatment and to 30 minutes for
subsequent follow-up sessions. The 8 physical therapists providing
treatment were either faculty or fellows in the US Army-Baylor
University Post-Professional Doctoral Program for Orthopaedic
Manual Physical Therapy.
For this secondary analysis, patient outcome data from these 47
patients were separated into 2 groups based on the type of cervical
MPT provided: (1) patients who received cervical thrust
manipula-tion as part of their treatment (thrust group, n = 23
[49%]) and (2) patients who received only cervical nonthrust
manipulations (nonthrust group, n = 24 [51%]). Patients within this
treatment arm were not randomized with respect
to the inclusion or exclusion of cervical thrust manipulations.
All patients receiv-ing cervical thrust manipulation also re-ceived
cervical nonthrust manipulations during their treatment
duration.
Baseline comparisons (taBle 1) of clin-ical and demographic
characteristics re-vealed statistically significant differences
between the 2 groups in age (nonthrust group being older [P =.02])
and base-line NDI scores. The difference in NDI scores was
statistically significant but not clinically meaningful (thrust
group hav-ing a higher NDI score [P =.05]). The difference in
symptom duration (mean difference, 1166 days), while clinically
significant, was not statistically signifi-cant. Although the
distribution of pa-tients with acute, subacute, and chronic neck
pain was similar between groups, the nonthrust group had 6 patients
with symptoms greater than 5 years in du-ration as compared to 1
patient in the thrust group.
taBle 1 Baseline Demographic and Clinical Variables*
Abbreviations: NDI, neck disability index; ROM, range of motion;
UE, upper extremity; VAS, visual analog scale.* Values expressed as
mean SD unless otherwise noted.† Indicates significant (P.05)
difference between groups using independent t tests.
Demographic and clinical Variables all patients (n = 47) thrust
(n = 23) nonthrust only (n = 24) significance (P Value)
Age (y) 48.8 14.1 44.0 11.1 53.5 15.3 .02†
Gender, female (n) 31 15 16 .92
Symptom duration (d) 1082.4 2256.7 487.0 447.2 1653.0 3049.5
.08
Acute, 30 d (n) 7 3 4 .73
Subacute, 30-90 d (n) 9 5 4 .66
Chronic, 90 d (n) 31 15 16 .92
Imaging performed (n) 31 13 18 .18
Headaches (n) 27 14 13 .64
UE symptoms (n) 31 13 18 .18
Cumulative ROM (deg) 255.3 56.8 263.6 59.2 247.3 54.5 .35
Flexion 44.9 14.1 46.3 13.9 43.6 14.5 .51
Extension 42.7 14.3 45.1 16.7 40.3 11.5 .26
Right rotation 53.0 14.2 55.8 12.7 50.4 15.3 .20
Left rotation 48.8 14.8 50.6 15.6 47.1 14.1 .42
Right sidebending 32.7 12.8 32.8 13.3 32.6 12.5 .95
Left sidebending 33.1 12.5 33.0 13.6 33.3 11.7 .93
Initial NDI (0-50 points) 15.6 4.5 16.9 5.2 14.4 3.3 .05†
Cervical VAS (0-100 mm) 53.5 20.7 57.4 23.1 49.7 17.7 .21
UE VAS (0-100 mm) 25.3 24.9 23.4 27.1 27.2 23.0 .61
Figure 3. Cervical thrust manipulation using nonphysiologic
(upslope) techniques to right C4-5 (online ViDeo).
40-03 Boyles.indd 135 2/17/10 2:49:32 PM
-
136 | march 2010 | volume 40 | number 3 | journal of orthopaedic
& sports physical therapy
[ research report ]
outcome MeasuresPrimary outcome measures consisted of the NDI, a
VAS for cervical pain, a VAS for upper extremity pain, and the
patient-perceived global rating of change (GRC). The NDI and VAS
measures were com-pleted at baseline, upon treatment com-pletion at
3 weeks, and at 6-week and 1-year follow-ups. The GRC was
com-pleted at the 3 follow-up periods. Recent clinical trials22,28
and a systematic review18 have used these 3 common outcome
mea-sures to assess pain intensity, disability, and perceived
recovery in patients with mechanical neck pain.
The NDI was selected to assess the pa-tient’s self-reported
disability due to me-chanical neck pain.29,36 The NDI has been
found to have high test-retest reliability, internal
consistency,32,3629 and good con-current validity with the McGill
Pain Questionnaire and patient-perceived im-provement.36 Stratford
et al32 analyzed the NDI in relation to patient decision mak-ing
and found both the minimal clinically important difference (MCID),
the small-est change in a scale that is meaningful to patients, and
the minimal detectable
change (MDC), the smallest amount of change that represents a
change beyond measurement error, to be 5 raw points or 10
percentage points. Cleland et al8 compared the psychometric
properties of the NDI and the Numeric Pain Rating Scale (NPRS) in
patients with mechani-cal neck pain and found them both to be
responsive and to display fair to moder-ate test-retest
reliability. They also found the NDI to have a higher MDC score
than previously reported (19%). Young et al40 reported similar
results to Cleland et al,8 with the MDC found to be 10 raw score
points on the NDI.
The 100-mm VAS, where 0 represent-ed “no pain” and 100
represented “worst pain imaginable,” was used to assess cer-vical
and upper extremity pain intensi-ties. The VAS has reported
test-retest reliability between 0.95 to 0.9730 and an MCID of 12 mm
(3 mm at a 95% CI),27 regardless of the severity of pain initially
reported.
The patient-perceived GRC25,26 was used to assess the patient’s
perception of change in their condition. The GRC is a 15-point
scale ranging from –7 to +7,
where 0 represents no change, –7 indi-cates that the patient is
“a very great deal worse,” and +7 indicates that the patient is “a
very great deal better.” Juniper et al26 proposed the following
classifications based on a patient’s GRC score: 0, 1, or –1 had no
change; 2 to 3 had minimal change; 4 to 5 had moderate change; and
6 to 7 had a large change in their condition.
Data analysisBased on the manual interventions used, patients
were divided into 2 groups for data analysis. Twenty-three patients
received cervical high-velocity thrust (thrust group) as part of
their treatment, and 24 patients received only nonthrust techniques
(nonthrust group). NDI and VAS variables were analyzed using a
2-by-4 mixed-model multivariate analysis of covariance (MANCOVA)
and univariate analyses of covariance (ANCOVA), with covariates of
age and duration of symp-toms (α = .05). A separate 2-by-3
mixed-model MANCOVA and ANCOVA were performed to include baseline
NDI scores as an additional covariate in the model.
taBle 2Adjusted Mean Scores, Mean Differences, and
Effect Size Indices for Primary Outcome Measures*
Abbreviations: CI, confidence interval; NDI, neck disability
index; UE, upper extremity; VAS, visual analog scale.* Values are
means (95% CIs) unless otherwise noted. Adjusted values based on
covariates of age, symptom duration, and baseline NDI scores.†
Effect sizes of 0.2, 0.5, and 0.8 correspond to small, medium, and
large differences, respectively. Positive mean differences and
effect sizes denote an advantage towards the thrust group.
Measure/Follow-up thrust Mean nonthrust-only Mean Mean
Difference (95% ci) effect size† (95% ci)
NDI (0-50)
Baseline 17.1 (15.2 to 19.0) 14.1 (12.3 to 16.0) 3.0 (0.3 to
5.6) 0.66 (0.06 to 1.23)
3 wk 6.2 (4.0 to 8.5) 6.4 (4.2 to 8.6) –0.2 (–3.3 to 3.0) –0.04
(–0.61 to 0.54)
6 wk 6.3 (4.3 to 8.4) 5.5 (3.5 to 7.5) 0.8 (–2.1 to 3.7) 0.17
(–0.41 to 0.74)
1 y 5.2 (2.8 to 7.6) 6.4 (4.1 to 8.8) –1.2 (–4.6 to 2.2) –0.21
(–0.78 to 0.37)
Cervical VAS (0-100 mm)
Baseline 56.5 (47.3 to 65.6) 50.6 (41.7 to 59.5) 5.9 (–6.9 to
18.6) 0.27 (–0.31 to 0.84)
3 wk 14.7 (6.4 to 22.9) 13.7 (5.7 to 21.8) 0.9 (–10.6 to 12.5)
0.05 (–0.52 to 0.62)
6 wk 16.3 (8.6 to 24.1) 15.2 (7.6 to 22.8) 1.1 (–9.7 to 12.0)
0.06 (–0.51 to 0.63)
1 y 17.2 (7.9 to 26.6) 19.8 (10.6 to 28.9) –2.5 (–15.6 to 10.5)
–0.11 (–0.68 to 0.46)
UE VAS (0-100 mm)
Baseline 21.5 (10.5 to 32.5) 29.0 (18.2 to 39.8) –7.5 (–22.9 to
7.9) –0.29 (–0.86 to 0.29)
3 wk 6.9 (0.9 to 12.8) 7.6 (1.8 to 13.4) –0.7 (–9.0 to 7.6)
–0.05 (–0.62 to 0.52)
6 wk 8.5 (1.7 to 15.4) 6.7 (0.1 to 13.6) 1.7 (–7.9 to 11.3) 0.10
(–0.47 to 0.67)
1 y 8.6 (–0.4 to 17.6) 11.5 (2.7 to 20.3) –2.9 (–15.5 to 9.7)
–0.14 (–0.71 to 0.44)
40-03 Boyles.indd 136 2/17/10 2:49:32 PM
-
journal of orthopaedic & sports physical therapy | volume 40
| number 3 | march 2010 | 137
Dichotomized GRC scores were used to classify patients as a
success or nonsuc-cess at each follow-up interval. Patients that
rated their improvement at or above 6 (“a great deal better”) were
considered a success, while patients that rated their change at 5
(“quite a bit better”) or below were a nonsuccess. These success
rates were compared using the chi-square sta-tistic (α = .05).
results
there were no significant in-teractions for either the
multivari-ate or univariate analyses, but there
was a significant main effect with respect to time for all
variables in both analyses (P.05). None of the covariate variables
was significant (α = .05), indicating that these variables did not
significantly add to the model and resulted in similar ad-justed
and unadjusted means (differences of 0.5 points for NDI means and
2.5 mm for VAS scores). Adjusted mean dif-ferences are listed in
taBle 2, along with the effect size index for all between-group
comparisons, which was small. Observed power was low for both the
MANCOVA (β.28) and ANCOVA (β.44) proce-dures. Figure 4 depicts the
improvement in cervical pain over time for both inter-vention
groups and the nonsignificant interaction effect between groups.
This graph is representative of the changes observed in the NDI and
upper extrem-ity VAS pain scores.
There were no significant differences between the 2 groups for
treatment suc-cess rates based on patient-perceived GRC scores
(P.28) (Figure 5).
Patients reported no adverse treat-ment effects, regardless of
which manual physical therapy technique was used.
Discussion
this study is a secondary analy-sis of the treatment arm of a
larger RCT,38 in which patients with me-
chanical neck pain achieved significant short- and long-term
improvements in
pain and disability following treatment with MPT and exercise.
Consistent with these findings, both the thrust and non-thrust
subgroups in this analysis dem-onstrated similar improvements over
time in short- and long-term clinical outcomes, with no statistical
or clini-cally significant differences between the groups (taBle
2). At first glance, a similar outcome between the 2 groups might
in-dicate that there was a lack of influence by a subset of
patients for whom thrust manipulation was indicated, or that, if
such a subgroup existed, the influence was minimal. However, an
equally plau-sible explanation is that the nonsignifi-cant results
were due to a relatively small, heterogeneous sample.
The mean differences between groups at each follow-up interval
(taBle 2) are smaller than the established MCID for each outcome
measure (12 mm for the VAS and 5 points for the NDI).
Addi-tionally, the observed effect size indices were small (–0.21
to 0.17), with large 95% confidence intervals that include null
values for each outcome measure and time interval. Effect size
indices less than 0.2 typically indicate small clinical differences
that are neither clinically nor statistically significant.
Caution, however, must be exercised when interpreting these data
based on study limitations. This is an underpow-ered secondary
analysis (β.28 and β.44) that prohibits any definitive state-
57.4
14.0 13.7 14.2
49.7
14.417.8
22.6
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
Cerv
ical
VAS
Pai
n Sc
ores
(mm
)
Thrust Nonthrust only
Baseline 3 wk 6 wk 1 yr
Figure 4. Cervical visual analog scale (VAS) pain scores. Values
expressed in millimeters (scale, 0-100 mm). Nonsignificant
interaction effect with analysis of covariance ANCOVA (P = .73).
Significant main effect for time (P.05) demonstrates improvement in
cervical pain for both groups.
0
10
20
30
40
50
60
70
80
Trea
tmen
t Suc
cess
(%)
Thrust Nonthrust only
3 wk 6 wk 1 yr
Figure 5. Global rating of change treatment success rates (where
GRC 6). *Values expressed as a percentage. †No observed differences
with chi-square analysis (P.28) for all time intervals.
40-03 Boyles.indd 137 2/17/10 2:49:34 PM
-
138 | march 2010 | volume 40 | number 3 | journal of orthopaedic
& sports physical therapy
[ research report ]ment regarding the presence or absence of a
treatment advantage of one approach over the other. Given the
results of previ-ous studies demonstrating the effective-ness of
both thrust3,12 and nonthrust21,22 procedures, a small effect size
is not to be unexpected when comparing differences between cervical
thrust and nonthrust manipulation as part of a larger treatment
plan. If this is indeed the case, a larger and possibly more
homogenous sample would be necessary to determine the clinical and
statistical relevance in observed dif-ferences between these
interventions. For example, Hurwitz et al23 compared thrust versus
nonthrust manipulation in a large RCT involving 336 patients with
neck pain. Even with this larger sample size, they were unable to
detect clinical and statistically meaningful differences be-tween
the 2 interventions. Their findings are consistent with our own,
including similar mean differences and confidence intervals for
pain and disability. Taken collectively, these trials underscore
the need for future studies to incorporate criteria associating
thrust manipulation with successful outcomes6,34 rather than simply
increasing sample size. Due to the rare but potentially serious
complications that have been reported following cervical thrust
manipulation, as well as perceived harm,19,20 a stronger case might
be made for the use of nonthrust procedures if they are shown to be
equally effective, even though nonthrust procedures are still not
without associated complications.11
In a recent RCT, Gonzalez-Iglesias et al14 reported that
patients with neck pain who received thoracic spine thrust
manipulations had significantly great-er improvements in pain,
motion, and disability than a control group up to 4 weeks following
treatment. Cleland et al9 reported that thrust manipulation of the
thoracic spine was significantly more ef-fective than nonthrust
manipulation for reducing pain and disability in patients with
mechanical neck pain. Although similar to our study in sample size
(n = 60) and patient presentation (mean age, 43.3 years; 55%
female), Cleland et al7
had sufficient power and effect sizes to detect these
between-group differences. High-velocity, low-amplitude thrust
techniques appear to be more effective than low-velocity,
variable-amplitude nonthrust manipulation techniques in overcoming
the relative stiffness/im-mobility found in the thoracic spine. In
contrast, cervical thrust and nonthrust manipulation techniques
appear to have similar treatment effects when applied as part of an
ongoing treatment program to the smaller, more mobile facet joints
within the cervical spine.23 However, when used as a single-session
interven-tion, Vernon et al35 concluded in a recent systematic
review that thrust manipula-tion, as compared to nonthrust manual
therapy, demonstrates superior changes in 100-mm VAS change scores
and larger effect sizes in patients with nonradicular chronic neck
pain.
Clinical decision making regarding the use of thrust
manipulation is of in-terest. Another significant limitation of
this study is the inherent selection bias in this nonrandomized
post hoc analysis. Although subjects were randomly as-signed to the
MPT and exercise group in the larger RCT,38 the inclusion of
cervical thrust manipulation was at the discretion of the treating
physical therapist. Physi-cal therapists in our study chose to
ma-nipulate patients who were younger (P = .02) and had more
reported disability (P = .05) and less symptom chronicity (P = .08)
than patients receiving only non-thrust manipulations. Although
adjusting for these covariates (age, duration, and baseline NDI
scores) did not add to our statistical model, observed differences
in these variables suggest that they were considered as part of the
physical thera-pist’s clinical decision-making process for when to
administer cervical thrust manipulation. It may be that physical
therapists in this study performed cervi-cal thrust techniques on
patients whom they perceived to be more responsive or presented
with less relative risk (“safer”) towards this intervention.
Clinical prediction rules (CPR) have
been developed to assist in the clinical decision making
associated with the di-agnosis and treatment of several
muscu-loskeletal conditions. A CPR consisting of clinical
examination items has been reported to identify patients with LBP
who are more likely to respond to lum-bar manipulation.6,13
Similarly, Cleland and colleagues7 have reported a develop-mental
CPR for patients with neck pain who benefit from thrust
manipulation to the thoracic spine. Tseng and colleagues33 reported
on predicted responders to cer-vical manipulation, but this has yet
to be validated. Identifying a relevant sub-group of patients with
neck pain who re-spond to cervical thrust manipulation, if one
exists, would not only be useful for clinical decision making but
would also help adequately plan future clinical trials. Future
studies that compare the relative effectiveness of cervical thrust
manipula-tion to nonthrust manipulation to treat patients with neck
pain must consider the lack of significance and small effect sizes
reported to date.23 Incorporating ex-isting7,39 and future
developmental CPR criteria that identify a subset of patients who
would benefit from cervical thrust manipulation would not only help
deter-mine the validity of developmental CPRs but may help
determine if there is a clini-cally meaningful difference between
the 2 interventions for a subgroup of patients.
conclusion
this secondary analysis of 2 subgroups of patients with
me-chanical neck pain demonstrated
short- and long-term improvements in pain and disability
following a treatment regimen of MPT and exercise. The inclu-sion
or exclusion of cervical thrust ma-nipulation into the MPT
treatment plan did not influence the results of the treat-ment arm
of the larger RCT from which this study was drawn. While the
methods used in this study limits our conclusions, our small
observed effect sizes may ben-efit future researchers with sample
size estimation for larger RCTs and suggest
40-03 Boyles.indd 138 2/17/10 2:49:35 PM
-
journal of orthopaedic & sports physical therapy | volume 40
| number 3 | march 2010 | 139
the need to incorporate developmental CPR criteria as a means to
improve sta-tistical power. t
keY pointsFinDings: Patients who received thrust manipulation to
the cervical spine had similar short- and long-term results in all
outcome scores of NDI, VAS, and GRC compared to those patients who
received cervical nonthrust manipula-tions. Neither group reported
adverse effects from either thrust or nonthrust cervical
manipulations.iMplications: Both approaches appear to be equally
effective and safe in this pa-tient population.caution: This is a
secondary analysis performed on a relatively small number of
patients from a larger RCT.
reFerences
1. Guide to Physical Therapist Practice. Second Edition.
American Physical Therapy Association. Phys Ther.
2001;81:9-746.
2. Bogduk N. Neck pain. Aust Fam Physician. 1984;13:26-30.
3. Bronfort G, Evans R, Nelson B, Aker PD, Gold-smith CH, Vernon
H. A randomized clinical trial of exercise and spinal manipulation
for patients with chronic neck pain. Spine (Phila Pa 1976).
2001;26:788-797; discussion 798-789.
4. Cassidy JD, Lopes AA, Yong-Hing K. The imme-diate effect of
manipulation versus mobilization on pain and range of motion in the
cervical spine: a randomized controlled trial. J Manipula-tive
Physiol Ther. 1992;15:570-575.
5. Childs JD, Cleland JA, Elliott JM, et al. Neck pain: Clinical
practice guidelines linked to the International Classification of
Functioning, Dis-ability, and Health from the Orthopedic Section of
the American Physical Therapy Association. J Orthop Sports Phys
Ther. 2008;38:A1-A34.
6. Childs JD, Fritz JM, Flynn TW, et al. A clinical prediction
rule to identify patients with low back pain most likely to benefit
from spinal ma-nipulation: a validation study. Ann Intern Med.
2004;141:920-928.
7. Cleland JA, Childs JD, Fritz JM, Whitman JM, Eberhart SL.
Development of a clinical predic-tion rule for guiding treatment of
a subgroup of patients with neck pain: use of thoracic spine
manipulation, exercise, and patient educa-tion. Phys Ther.
2007;87:9-23. http://dx.doi.org/10.2522/ptj.20060155
8. Cleland JA, Childs JD, Whitman JM. Psycho-metric properties
of the Neck Disability Index
and Numeric Pain Rating Scale in patients with mechanical neck
pain. Arch Phys Med Rehabil. 2008;89:69-74.
http://dx.doi.org/10.1016/j.apmr.2007.08.126
9. Cleland JA, Glynn P, Whitman JM, Eberhart SL, MacDonald C,
Childs JD. Short-term ef-fects of thrust versus nonthrust
mobilization/manipulation directed at the thoracic spine in
patients with neck pain: a randomized clinical trial. Phys Ther.
2007;87:431-440. http://dx.doi.org/10.2522/ptj.20060217
10. Cote P, Cassidy JD, Carroll L. The Saskatchewan Health and
Back Pain Survey. The prevalence of neck pain and related
disability in Saskatchewan adults. Spine (Phila Pa 1976).
1998;23:1689-1698.
11. Di Fabio RP. Manipulation of the cervical spine: risks and
benefits. Phys Ther. 1999;79:50-65.
12. Evans R, Bronfort G, Nelson B, Goldsmith CH. Two-year
follow-up of a randomized clinical trial of spinal manipulation and
two types of exercise for patients with chronic neck pain. Spine
(Phila Pa 1976). 2002;27:2383-2389.
http://dx.doi.org/10.1097/01.BRS.0000030192.39326.FF
13. Flynn T, Fritz J, Whitman J, et al. A clinical prediction
rule for classifying patients with low back pain who demonstrate
short-term improve-ment with spinal manipulation. Spine (Phila Pa
1976). 2002;27:2835-2843.
http://dx.doi.org/10.1097/01.BRS.0000035681.33747.8D
14. Gonzalez-Iglesias J, Fernandez-de-las-Penas C, Cleland JA,
Gutierrez-Vega Mdel R. Thoracic spine manipulation for the
management of pa-tients with neck pain: a randomized clinical
trial. J Orthop Sports Phys Ther. 2009;39:20-27.
15. Gross AR, Aker PD, Goldsmith CH, Peloso P. Pa-tient
education for mechanical neck disorders. Cochrane Database Syst
Rev. 2000;CD000962. http://dx.doi.org/10.1002/14651858.CD000962
16. Gross AR, Aker PD, Goldsmith CH, Peloso P. Physical medicine
modalities for me-chanical neck disorders. Cochrane Database Syst
Rev. 2000;CD000961. http://dx.doi.org/10.1002/14651858.CD000961
17. Gross AR, Goldsmith C, Hoving JL, et al. Con-servative
management of mechanical neck disorders: a systematic review. J
Rheumatol. 2007;34:1083-1102.
18. Gross AR, Hoving JL, Haines TA, et al. A Co-chrane review of
manipulation and mobilization for mechanical neck disorders. Spine
(Phila Pa 1976). 2004;29:1541-1548.
19. Haldeman S, Kohlbeck FJ, McGregor M. Risk fac-tors and
precipitating neck movements causing vertebrobasilar artery
dissection after cervical trauma and spinal manipulation. Spine
(Phila Pa 1976). 1999;24:785-794.
20. Haldeman S, Kohlbeck FJ, McGregor M. Un-predictability of
cerebrovascular ischemia associated with cervical spine
manipulation therapy: a review of sixty-four cases after cervi-cal
spine manipulation. Spine (Phila Pa 1976). 2002;27:49-55.
21. Hoving JL, de Vet HC, Koes BW, et al. Manual therapy,
physical therapy, or continued care
by the general practitioner for patients with neck pain:
long-term results from a prag-matic randomized clinical trial. Clin
J Pain. 2006;22:370-377.
http://dx.doi.org/10.1097/01.ajp.0000180185.79382.3f
22. Hoving JL, Koes BW, de Vet HC, et al. Manual therapy,
physical therapy, or continued care by a general practitioner for
patients with neck pain. A randomized, controlled trial. Ann Intern
Med. 2002;136:713-722.
23. Hurwitz EL, Morgenstern H, Harber P, Komin-ski GF, Yu F,
Adams AH. A randomized trial of chiropractic manipulation and
mobilization for patients with neck pain: clinical outcomes from
the UCLA neck-pain study. Am J Public Health.
2002;92:1634-1641.
24. Hurwitz EL, Morgenstern H, Vassilaki M, Chiang LM. Adverse
reactions to chiropractic treatment and their effects on
satisfaction and clinical outcomes among patients enrolled in the
UCLA Neck Pain Study. J Manipulative Physiol Ther. 2004;27:16-25.
http://dx.doi.org/10.1016/j.jmpt.2003.11.002
25. Jaeschke R, Singer J, Guyatt GH. Measurement of health
status. Ascertaining the minimal clini-cally important difference.
Control Clin Trials. 1989;10:407-415.
26. Juniper EF, Guyatt GH, Willan A, Griffith LE. Determining a
minimal important change in a disease-specific Quality of Life
Questionnaire. J Clin Epidemiol. 1994;47:81-87.
27. Kelly AM. The minimum clinically significant difference in
visual analogue scale pain score does not differ with severity of
pain. Emerg Med J. 2001;18:205-207.
28. Korthals-de Bos IB, Hoving JL, van Tulder MW, et al. Cost
effectiveness of physiotherapy, manual therapy, and general
practitioner care for neck pain: economic evaluation alongside a
randomised controlled trial. Bmj. 2003;326:911.
http://dx.doi.org/10.1136/bmj.326.7395.911
29. MacDermid JC, Walton DM, Avery S, et al. Mea-surement
properties of the neck disability index: a systematic review. J
Orthop Sports Phys Ther. 2009;39:400-417.
http://dx.doi.org/10.2519/jospt.2009.2930
30. McCormack HM, Horne DJ, Sheather S. Clinical applications of
visual analogue scales: a critical review. Psychol Med.
1988;18:1007-1019.
31. Picavet HS, Schouten JS. Musculoskeletal pain in the
Netherlands: prevalences, consequences and risk groups, the
DMC(3)-study. Pain. 2003;102:167-178.
32. Stratford PW, Riddle DL, Binkley JM, Spadoni G, Westaway MD,
Padfield B. Using the Neck Disability Index to make decisions
concern-ing individual patients. Physiother Canada.
1999;51:107-112.
33. Tseng YL, Wang WT, Chen WY, Hou TJ, Chen TC, Lieu FK.
Predictors for the immediate respond-ers to cervical manipulation
in patients with neck pain. Man Ther. 2006;11:306-315.
http://dx.doi.org/10.1016/j.math.2005.08.009
34. van der Donk J, Schouten JS, Passchier J, van Romunde LK,
Valkenburg HA. The associations
40-03 Boyles.indd 139 2/17/10 2:49:36 PM
-
140 | march 2010 | volume 40 | number 3 | journal of orthopaedic
& sports physical therapy
[ research report ]
@ More inForMationwww.jospt.org
gorithm. Am J Phys Med Rehabil. 2003;82:203-218; quiz 219-221.
http://dx.doi.org/10.1097/01.PHM.0000052700.48757.CF
40. Young BA, Walker MJ, Strunce JB, Boyles RE, Whitman JM,
Childs JD. Responsiveness of the Neck Disability Index in patients
with mechani-cal neck disorders. Spine J. 2009;9:802-808.
http://dx.doi.org/10.1016/j.spinee.2009.06.002
fect of spinal manipulation in the treatment of chronic neck
pain: a pilot study. J Manipulative Physiol Ther.
1990;13:13-16.
38. Walker MJ, Boyles RE, Young BA, et al. The effectiveness of
manual physical therapy and exercise for mechanical neck pain: a
ran-domized clinical trial. Spine (Phila Pa 1976).
2008;33:2371-2378.
http://dx.doi.org/10.1097/BRS.0b013e318183391e
39. Wang WT, Olson SL, Campbell AH, Hanten WP, Gleeson PB.
Effectiveness of physical therapy for patients with neck pain: an
individualized approach using a clinical decision-making al-
of neck pain with radiological abnormalities of the cervical
spine and personality traits in a gen-eral population. J Rheumatol.
1991;18:1884-1889.
35. Vernon H, Humphreys BK. Chronic mechanical neck pain in
adults treated by manual therapy: a systematic review of change
scores in random-ized controlled trials of a single session. J Man
Manip Ther. 2008;16:E42-52.
36. Vernon H, Mior S. The Neck Disability Index: a study of
reliability and validity. J Manipulative Physiol Ther.
1991;14:409-415.
37. Vernon HT, Aker P, Burns S, Viljakaanen S, Short L. Pressure
pain threshold evaluation of the ef-
EARN CEUs With JOSPT’s Read for Credit ProgramJOSPT’s Read for
Credit (RFC) program invites Journal readers to study and analyze
selected JOSPT articles and successfully complete online quizzes
about them for continuing education credit. To participate in the
program:
1. Go to www.jospt.org and click on “Read for Credit” in the
left-hand navigation column that runs throughout the site or on the
link in the “Read for Credit” box in the right-hand column of the
home page. 2. Choose an article to study and when ready, click
“Take Exam” for that article. 3. Login and pay for the quiz by
credit card. 4. Take the quiz. 5. Evaluate the RFC experience and
receive a personalized certificate of continuing education
credits.
The RFC program o�ers you 2 opportunities to pass the quiz. You
may review all of your answers—including the questions you missed.
You receive 0.2 CEUs, or 2 contact hours, for each quiz passed. The
Journal website maintains a history of the quizzes you have taken
and the credits and certificates you have been awarded in the “My
CEUs” section of your “My JOSPT” account.
40-03 Boyles.indd 140 2/17/10 2:49:38 PM
133JOSPTmar10.p1134JOSPTmar10.p1135JOSPTmar10.p1136JOSPTmar10.p1137JOSPTmar10.p1138JOSPTmar10.p1139JOSPTmar10.p1140JOSPTmar10.p1





![Dr Tom Boyles ADULT GUIDELINES [Read-Only] Guidelines - T Boyles.pdf · 2017. 11. 22. · Title: Microsoft PowerPoint - Dr Tom Boyles ADULT GUIDELINES [Read-Only] Author: fiona Created](https://img.pdfslide.us/doc/110x75/60c07d4ec6a8f803cb683efc/dr-tom-boyles-adult-guidelines-read-only-guidelines-t-boylespdf-2017-11.jpg)