Embed Size (px)
Citation preview
Oral Anticoagulation For Deep Venous Thrombosis and Pulmonary Embolism
Robby FerranteWNE Pharmacy Candidate
Objectives
Review the clotting cascade and the effect of various anticoagulants on this cascade
Discuss oral anticoagulants that are used to treat DVT/PE.
Analyze the use of these agents and their place in DVT/PE therapy.
Deep Venous Thrombosis Deep vein
thrombosis (DVT) occurs when a blood clot forms in one or more deep veins
Symptoms usually occur in legs Can cause leg pain or
swelling May occur without any
symptoms.
Common causes: Immobility Traumatic Injury Surgery Obesity Prolonged travel Pregnancy Thrombophilia
Pulmonary Embolism1
Blockage of 1+ pulmonary arteries by a substance that has traveled from elsewhere in the body
Causes impaired blood flow
Increased pressure in the right ventricle
Symptoms Dyspnea Acute chest pain Increased heart rate Cough Abnormal breathing
sounds Low blood pressure Cardiac arrest
Prophylactic Treatment2
Generally, parenteral heparins or warfarin are used prophylactically.
NOAC are becoming more commonly used as warfarin use is decreasing
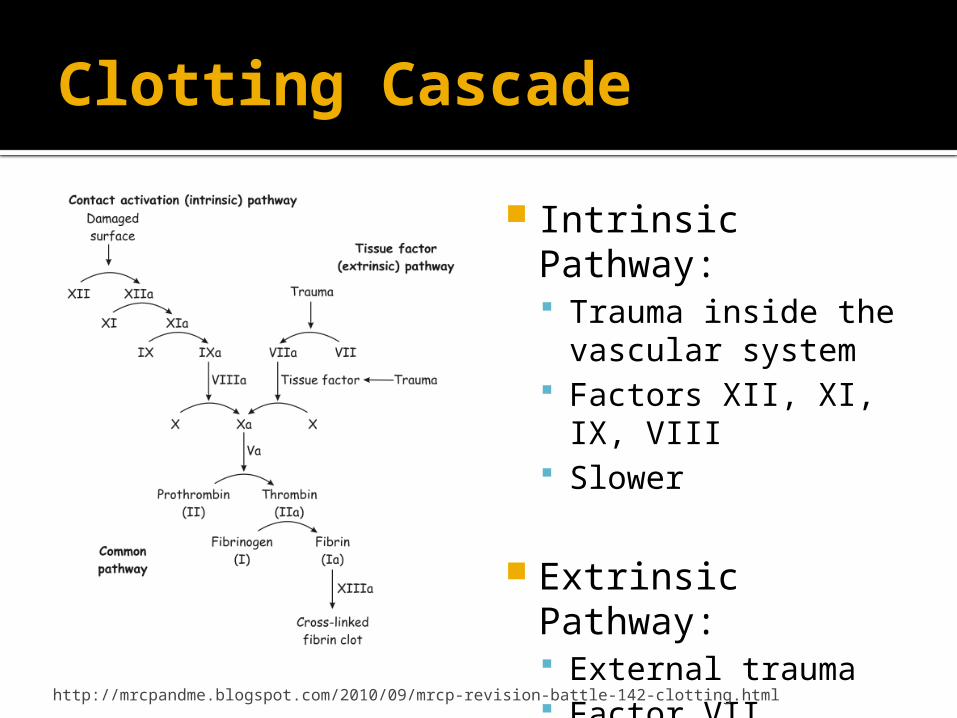
Clotting Cascade
Intrinsic Pathway: Trauma inside the
vascular system Factors XII, XI, IX,
VIII Slower
Extrinsic Pathway: External trauma Factor VII Quicker
http://mrcpandme.blogspot.com/2010/09/mrcp-revision-battle-142-clotting.html
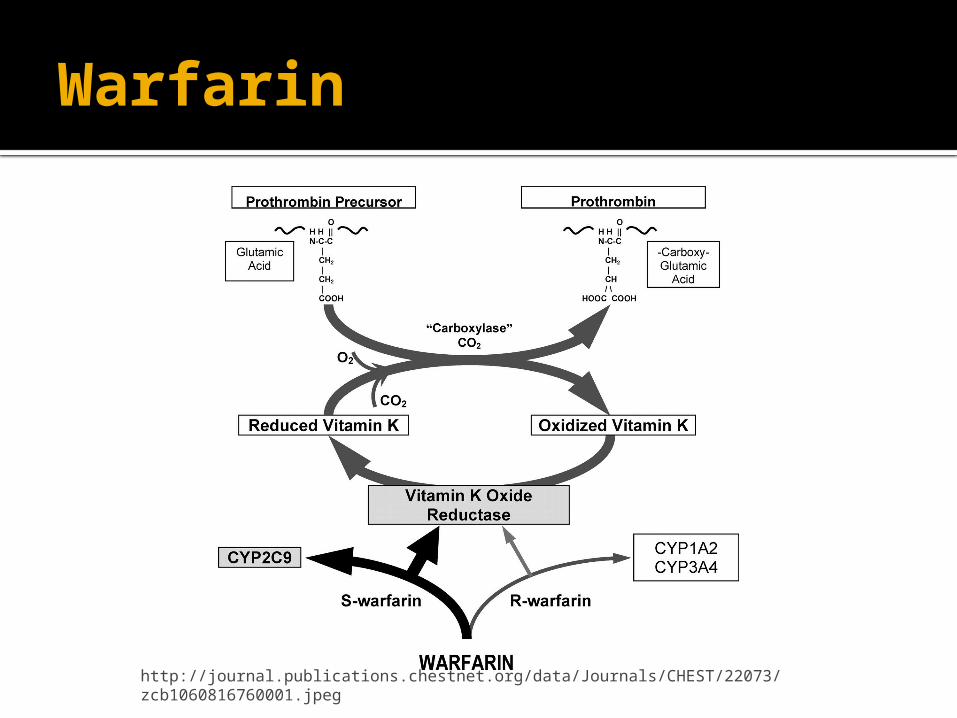
Warfarin
http://journal.publications.chestnet.org/data/Journals/CHEST/22073/zcb1060816760001.jpeg
Warfarin3
Vitamin K antagonists are the standard treatment therapy. Relative risk
reduction of ~85% vs placebo
Recurrence risk of ~3%
Major bleeding risk ~2.1% during first 6 months
There are critiques of warfarin therapy: Monitoring Small therapeutic
window Effect of diet Multiple drug
interactions
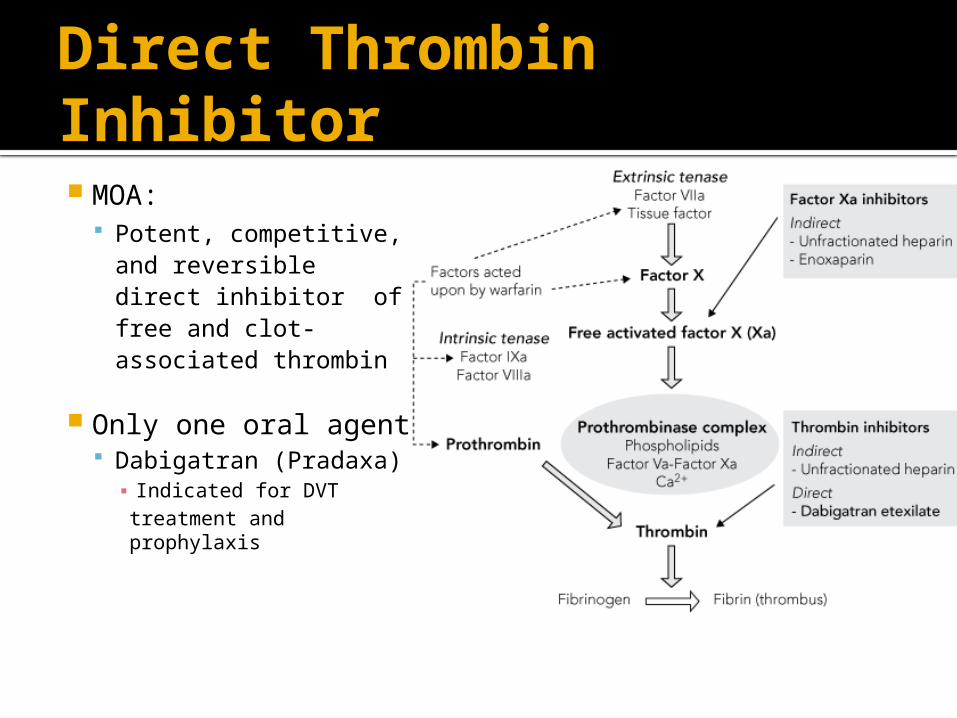
Direct Thrombin Inhibitor MOA:
Potent, competitive, and reversible direct inhibitor of free and clot- associated thrombin
Only one oral agent Dabigatran (Pradaxa)▪ Indicated for DVT treatment and prophylaxis
Dabigatran4
Dose for DVT/PE prophylaxis: CrCl > 30 mL/min▪ 150 mg Orally, twice a day
CrCl 15-30 mL/min ▪ 75 mg Orally, twice a day
Administration: Must be swallowed whole Not to be used in NG tube Keep in original container (120 days)
Dabigatran ADME
Absorption Tmax = 1-6 hours Food does not effect bioavailability
Distribution ~ 35% protein bound
Metabolism Prodrug hydrolyzed by the liver Hepatic metabolism and PGP substrate
Excretion Renal excretion (80%) Dialyzable T ½ = 12-17 hours
Dabigatran
Black Box Warning: Premature discontinuation increases risk
of thrombotic event. Epidural or spinal hematomas may occur
in patients undergoing neuraxial anesthesia.
Re-Cover Trial5
2539 patients in randomized double blind noninferiority trial
150 mg Dabigatran BID 30/1274 (2.4%) had recurrent VT 20 patients had major bleed
Warfarin; INR 2-3 27/1265 (2.1%) had recurrent VT 24 patients with major bleed
Factor Xa Inhibitors
Oral Options: Rivaroxaban (Xarelto) Apixaban (Apixaban) Edoxaban (Only in Japan)▪ Will not discuss edoxaban
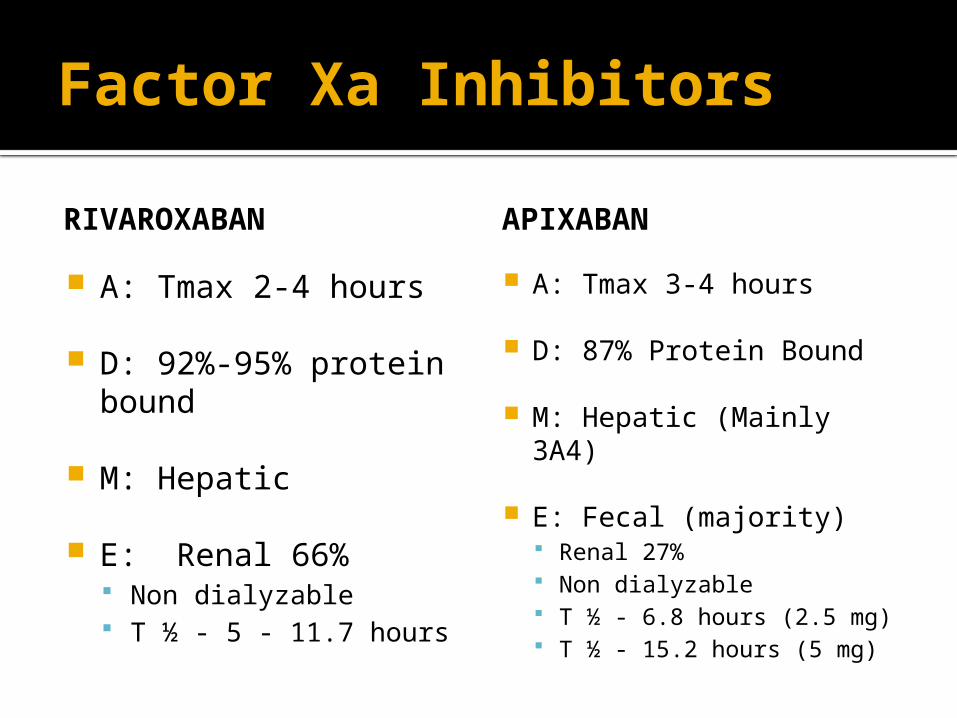
Factor Xa Inhibitors
RIVAROXABAN
A: Tmax 2-4 hours
D: 92%-95% protein bound
M: Hepatic
E: Renal 66% Non dialyzable T ½ - 5 - 11.7 hours
APIXABAN
A: Tmax 3-4 hours
D: 87% Protein Bound
M: Hepatic (Mainly 3A4)
E: Fecal (majority) Renal 27% Non dialyzable T ½ - 6.8 hours (2.5 mg) T ½ - 15.2 hours (5 mg)
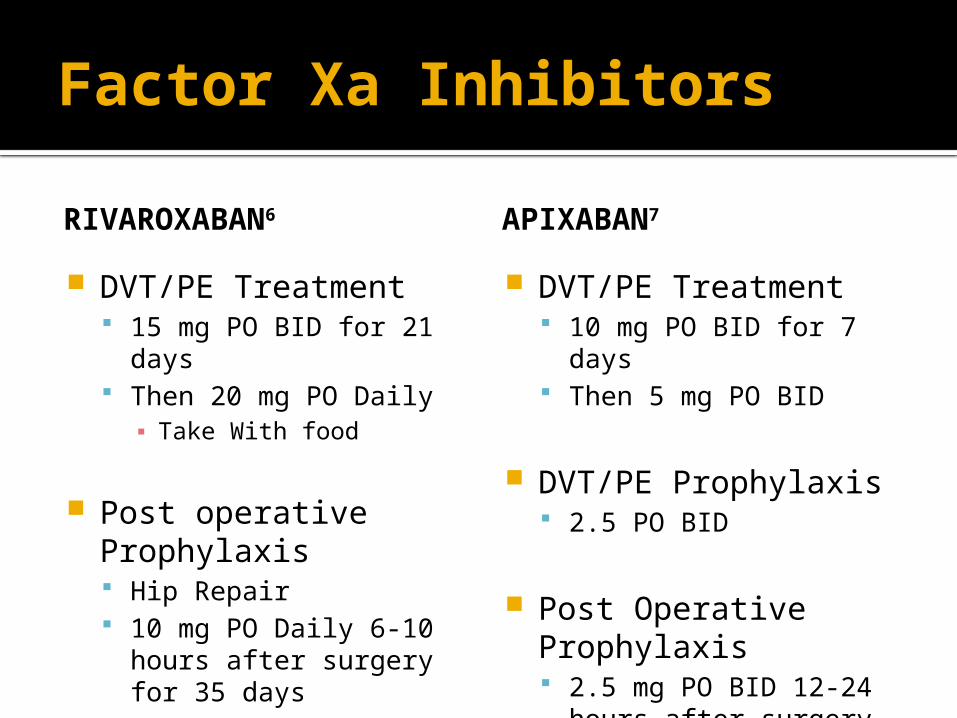
Factor Xa Inhibitors
RIVAROXABAN6
DVT/PE Treatment 15 mg PO BID for 21
days Then 20 mg PO Daily ▪ Take With food
Post operative Prophylaxis Hip Repair 10 mg PO Daily 6-10
hours after surgery for 35 days
APIXABAN7
DVT/PE Treatment 10 mg PO BID for 7 days Then 5 mg PO BID
DVT/PE Prophylaxis 2.5 PO BID
Post Operative Prophylaxis 2.5 mg PO BID 12-24
hours after surgery for 35 days
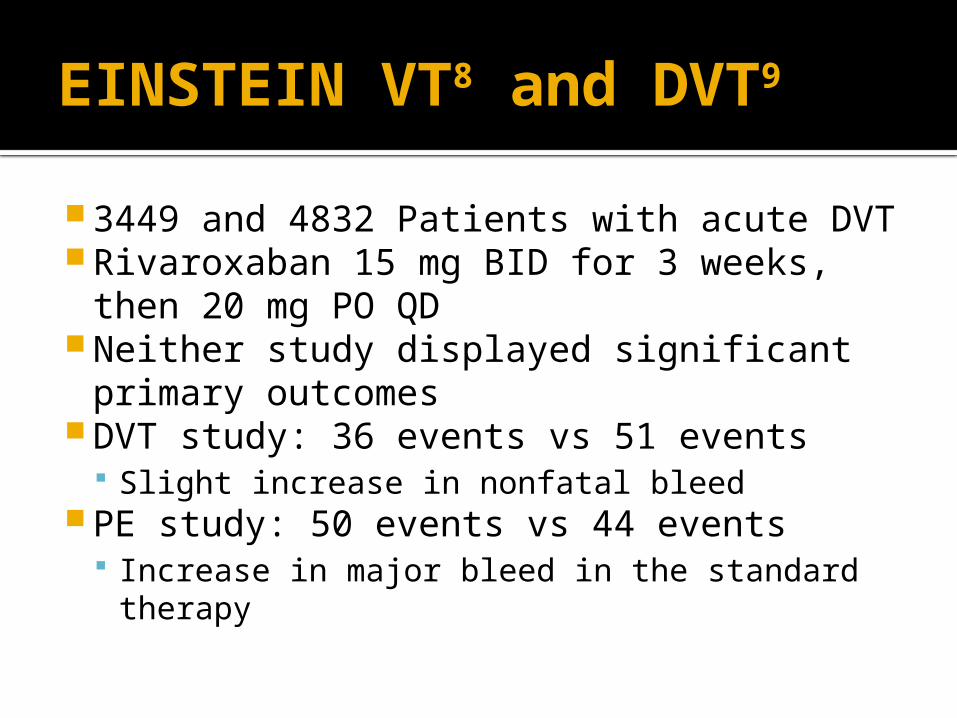
EINSTEIN VT8 and DVT9
3449 and 4832 Patients with acute DVT Rivaroxaban 15 mg BID for 3 weeks,
then 20 mg PO QD Neither study displayed significant
primary outcomes DVT study: 36 events vs 51 events
Slight increase in nonfatal bleed PE study: 50 events vs 44 events
Increase in major bleed in the standard therapy
Amplify Study10
5395 patients involved in the study with acute VT
Apixaban 10 mg BID for 7 days, then 5 mg BID
Primary Endpoiont – recurrent VT or VT related death. 59 events vs 71 events (2.3% vs 2.7%)
Thank You Nadine!
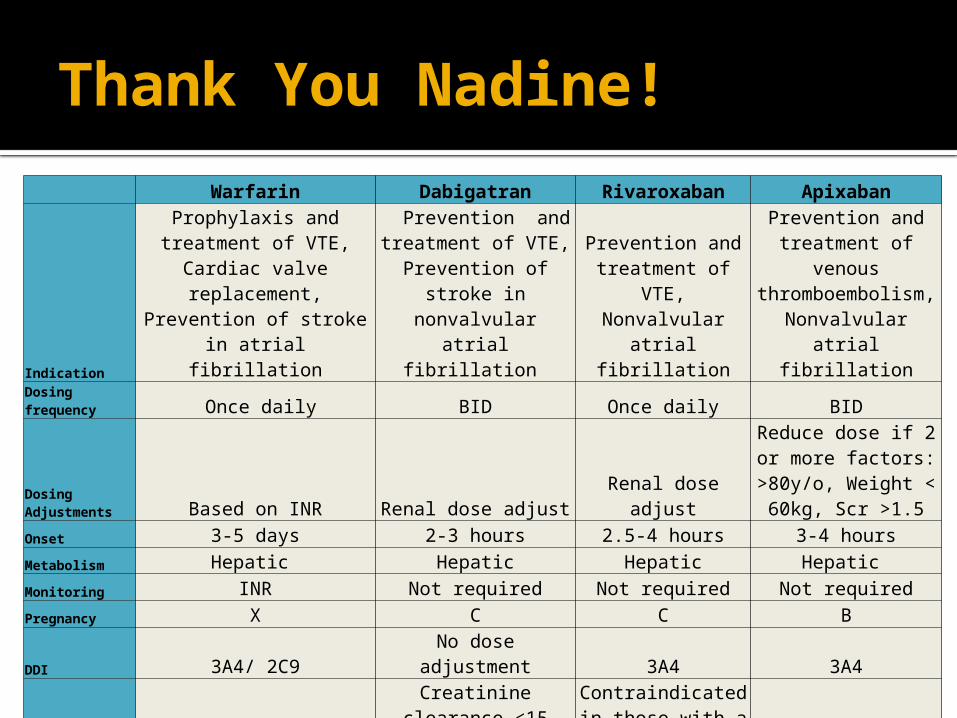
Warfarin Dabigatran Rivaroxaban Apixaban
Indication
Prophylaxis and treatment of VTE, Cardiac valve
replacement, Prevention of stroke in atrial fibrillation
Prevention and treatment of VTE,
Prevention of stroke in nonvalvular atrial
fibrillation
Prevention and treatment of VTE, Nonvalvular atrial
fibrillation
Prevention and treatment of venous thromboembolism, Nonvalvular atrial
fibrillation
Dosing frequency Once daily BID Once daily BID
Dosing Adjustments Based on INR Renal dose adjust Renal dose adjust
Reduce dose if 2 or more factors: >80y/o,
Weight < 60kg, Scr >1.5
Onset 3-5 days 2-3 hours 2.5-4 hours 3-4 hours
Metabolism Hepatic Hepatic Hepatic Hepatic
Monitoring INR Not required Not required Not required
Pregnancy X C C B
DDI 3A4/ 2C9 No dose adjustment 3A4 3A4
Contraindication Bleeding
Creatinine clearance <15 mL/min , Hemodialysis
dependent
Contraindicated in those with a
creatinine clearance <15 mL/min N/A
Antidote Vitamin K None None None
ADE Dyspesia, GI bleeding
Meta-Analysis (NOAC vs VKA)3
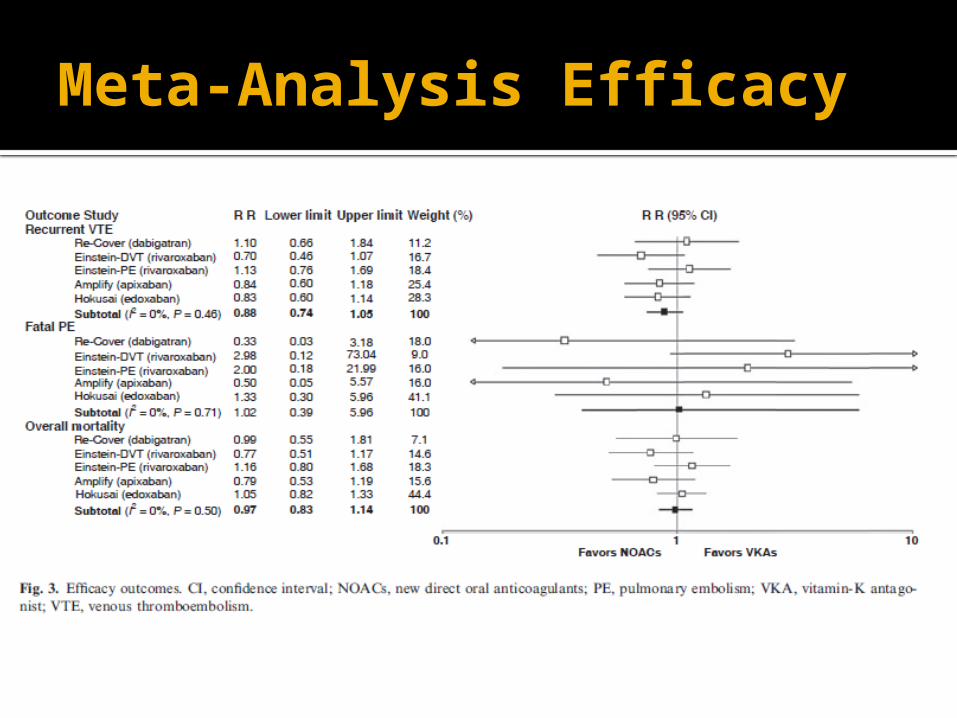
Meta-Analysis Efficacy
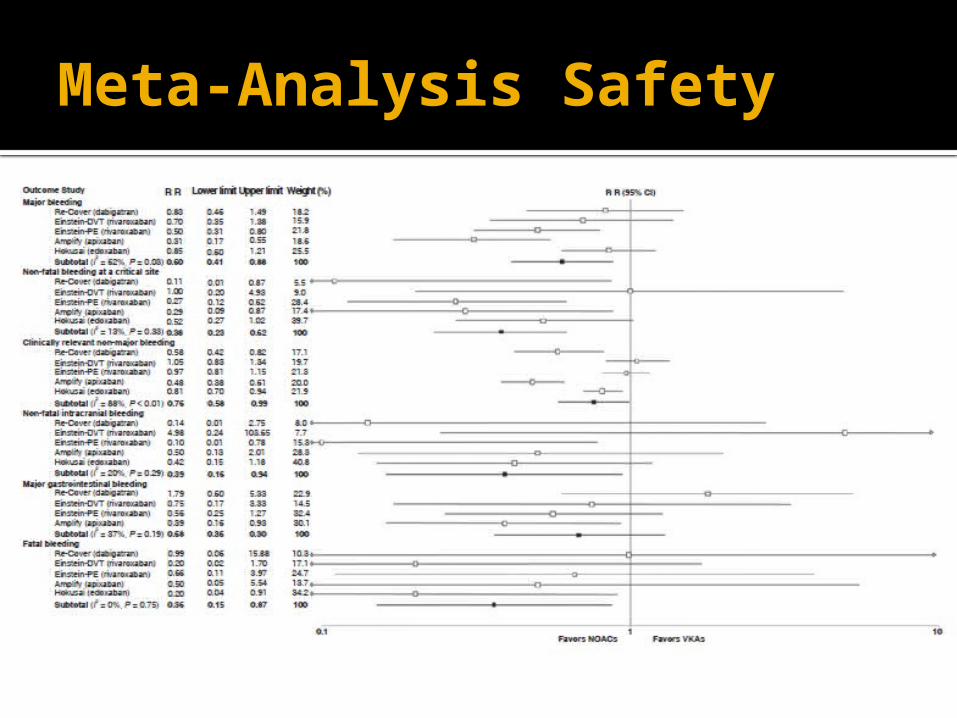
Meta-Analysis Safety
Conclusion
Almost all comparisons between NOACs and VKAs were relatively similar
Few significant differences
Depending on patient factors, NOACs are a viable option and have proven to be non-inferior while also potentially reducing bleeding risk.
References
1.) Deep Vein Thrombosis (DVT) / Pulmonary Embolism (PE) Data and Statistics. Atlanta Georgia. Center of Disease Control and Prevention. Published 8 June, 2012. www.cdc.gov/ncbddd/dvt/data.html
2.) Kirley K, Oato DM, Kornfield R, et al. National trends in oral anticoagulant use in the United States, 2007 to 2011. Circ Cardiovasc Qual Outcomes 2012; 5(5): 615-21
3.) Van Der Hulle J, Koolman J, Den Exter PL, et al. Effectiveness and Safety of Novel Oral Anticoagulants as Compared With Vitamin K Antagonists in the Treatment of Acute Symptomatic Venous Thromboembolism: A Systematic review and Meta-Analysis. J Thromb Haemost 2014; 12: 320-8
4.) 1. Product Information: PRADAXA(R) oral capsules, dabigatran etexilate mesylate oral capsules. Boehringer Ingelheim Pharmaceuticals, Inc. (Per FDA), Ridgefield, CT, 2012.
5.) Sam Schulman, M.D., Clive Kearon, M.D., Ajay K. Kakkar, M.D., et al. Dabigatran versus Warfarin in the Treatment of Acute Venous Thromboembolism. N Engl J Med 2009; 361:2342-2352
References
6.) Product Information: XARELTO(R) oral tablets, rivaroxaban oral tablets. Janssen Pharmaceuticals, Inc. (per manufacturer), Titusville, NJ, 2012.
7). Product Information: ELIQUIS(R) oral tablets , apixaban oral tablets. Bristol-Myers Squibb Company (per FDA), Princeton, NJ, 2014
8.) The EINSTEIN Investigators. Oral Rivaroxaban for Symptomatic Venous Thromboembolism. N Engl J Med 2010; 363:2499-2510
9.) The EINSTEIN–PE Investigators. Oral Rivaroxaban for the Treatment of Symptomatic Pulmonary Embolism.N Engl J Med 2012; 366:1287-1297
10.) Giancarlo Agnelli, M.D., Harry R. Buller, M.D., Ph.D., Alexander Cohen, M.D., et al. Oral Apixaban for the Treatment of Acute Venous Thromboembolism. N Engl J Med 2013; 369:799-808
Questions?