Embed Size (px)
Citation preview
RO-ILS: Radiation Oncology Incident Learning System®
1
Cindy Tomlinson Senior Manager for Security and Safety, ASTRO
Florida Chapter of AAPM Annual Meeting
April 30, 2016
Objectives/Outline
• History and background of RO-ILS. • Current status of RO-ILS. • Aggregate data. • Findings. • Legal challenges. • Future plans.
2

RO-ILS Timeline
Patient Safety and Quality Improvement Act
2005
RO-ILS established by ASTRO and AAPM
2011
RO-ILS Launch
June 19, 2014
IOM Report: To Err is Human
2000
RO-ILS Beta Testing
2013-2014
PSO’s formed by AHRQ
2009 2010
ASTRO launches Target Safely Campaign
3
RO-ILS: Radiation Oncology Incident Learning System
The mission of RO-ILS is to facilitate safer and higher quality care in radiation oncology by providing a
mechanism for shared learning in a secure and non-punitive environment.
4
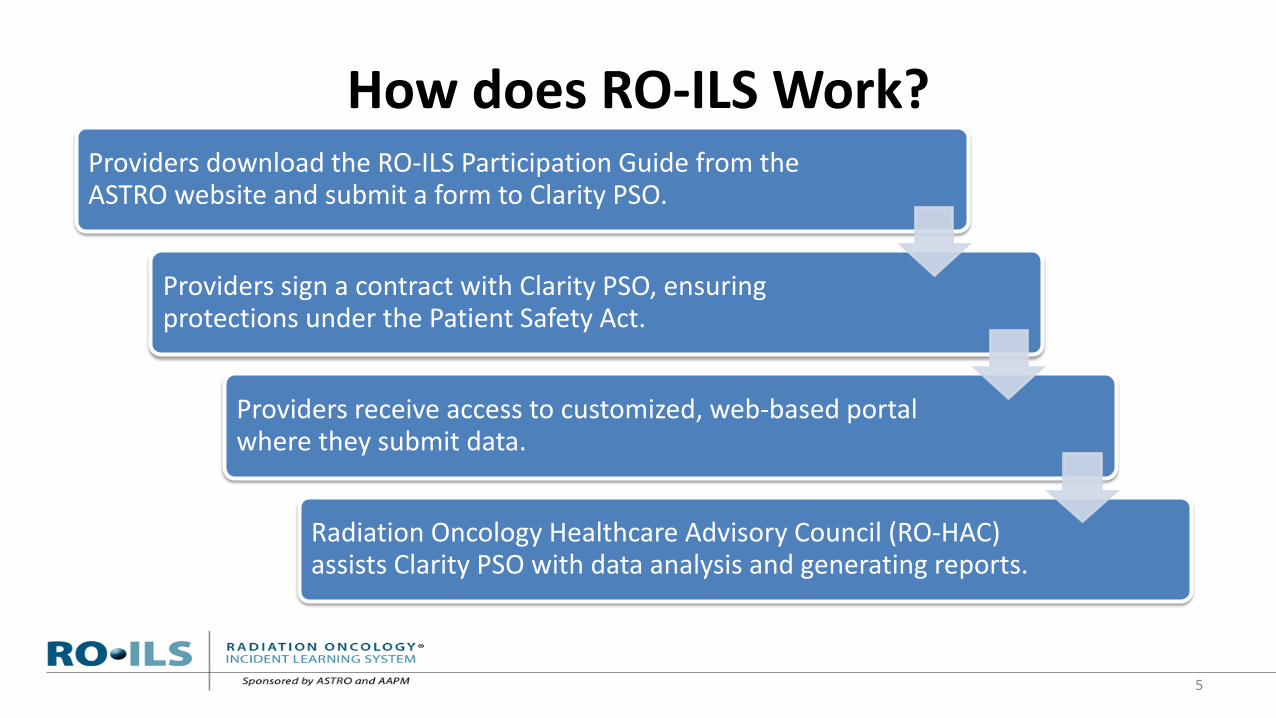
How does RO-ILS Work? Providers download the RO-ILS Participation Guide from the ASTRO website and submit a form to Clarity PSO.
Providers sign a contract with Clarity PSO, ensuring protections under the Patient Safety Act.
Providers receive access to customized, web-based portal where they submit data.
Radiation Oncology Healthcare Advisory Council (RO-HAC) assists Clarity PSO with data analysis and generating reports.
5

Program Update • 208 facilities participating. • 63 facilities currently working through the contracting process. • 1,699 reports submitted.
As of April 14, 2016 6
0
50
100
150
200
250
Num
ber o
f Fac
ilitie
s
RO-ILS Participation

Participating Facilities Practice Setting
7
[CATEGORY NAME]
[CATEGORY NAME]
[CATEGORY NAME]
[CATEGORY NAME]
[CATEGORY NAME]
31%
8%
49%
2%
10%
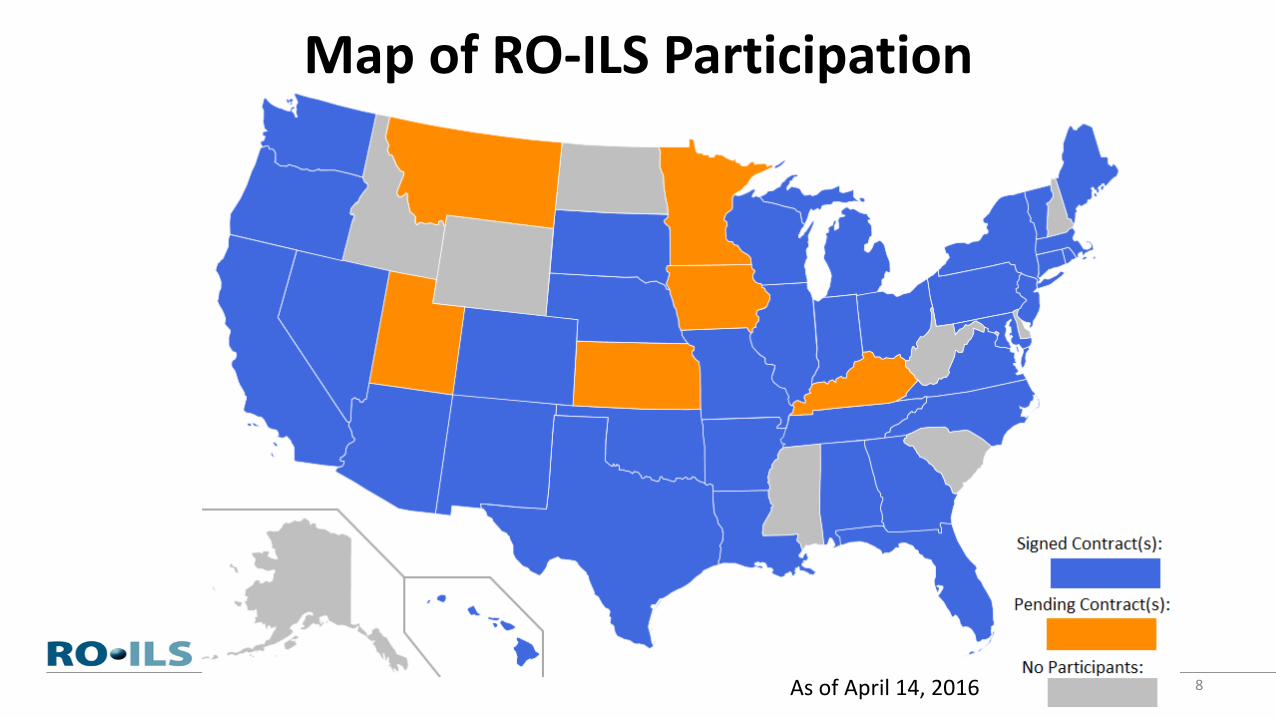
Map of RO-ILS Participation
As of April 14, 2016 8
Program Update
• RO-ILS: Radiation Oncology Incident Learning System: A report from the first year of experience, Practical Radiation Oncology, September-October 2015, Volume 5, Issue 5, Pages 312–318.
• The 2015 Year in Review was published on the ASTRO website. • RO-ILS participants receive “Tips of the Month”:
• Staff support services in the wake of an incident. • Developing and utilizing hashtags (#) for internal tracking of events. • Utilizing the RO-ILS analysis wizard to create internal reports.
9

Healthcare SafetyZone® Portal
• RO-ILS is built on Clarity PSO’s Healthcare SafetyZone® Portal platform.
• Consists of two sections: – Submit Event: short form meant to capture basic event
information. – My Review: longer form designed for in-depth data entry.
• Required questions must be answered before submission to PSO for analysis.
10

11
• Brachytherapy • External Beam • Radiopharmaceutical • Other
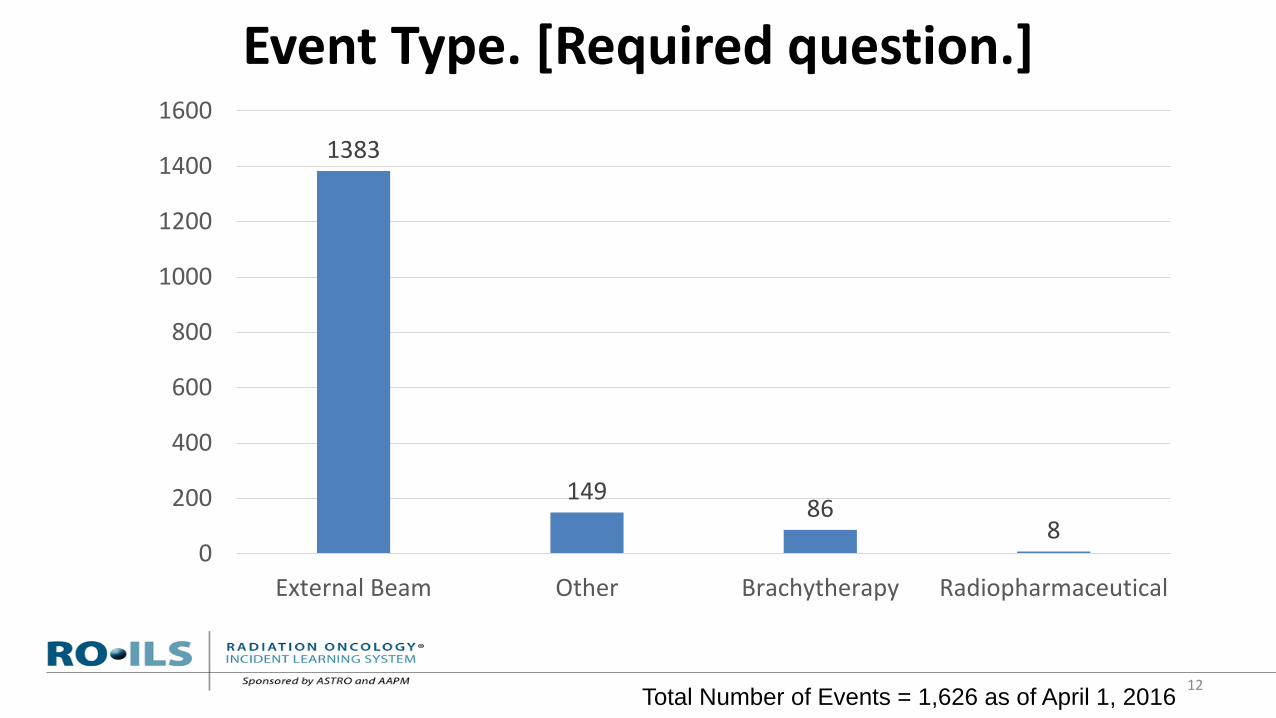
Event Type. [Required question.]
Total Number of Events = 1,626 as of April 1, 2016 12
1383
149 86
8 0
200
400
600
800
1000
1200
1400
1600
External Beam Other Brachytherapy Radiopharmaceutical

13
• Incident that reached the patient: A safety-related event that reached the patient, with or without harm
• Near-miss event: A safety event that did not reach the patient • Unsafe condition: Any condition that increases the probability
of a safety event.

What is being reported? [Required question.]
Total Number of Events = 1,626 as of April 1, 2016 14
585 556 485
0
100
200
300
400
500
600
700
Incident that reached thepatient
Near-miss Unsafe condition

15
• Patient Assessment • Imaging for RT Planning • Treatment Planning • Pre-treatment Review and Verification • Treatment Delivery • On-treatment Quality Management • Post-treatment Completion • Equipment and Software Quality Management

In what workflow step was the event first discovered?
16
426
369
154
82 63 57 44 42
19
370
0
50
100
150
200
250
300
350
400
450
Pre-TreatmentReview andVerification
TreatmentDelivery
On-TreatmentQuality
Management
TreatmentPlanning
Simulation Post-TreatmentCompletion
Imaging for RTPlanning
PatientAssessment
Equipment andSoftwareQuality
Management
Unanswered
Total Number of Events = 1,626 as of April 1, 2016
17

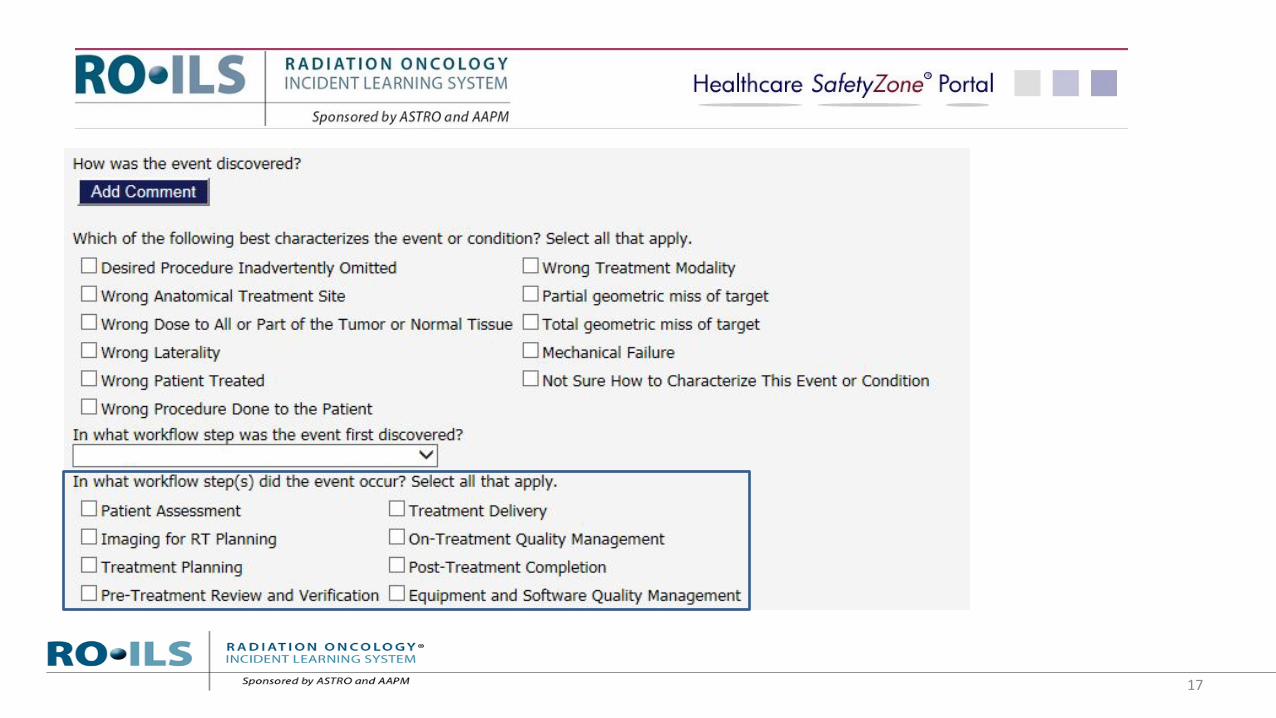
In what workflow step(s) did the event occur? Select all that apply.
18
494
350
266
149 98
69 33 17
383
0
100
200
300
400
500
600
TreatmentPlanning
TreatmentDelivery
Pre-TreatmentReview andVerification
Imaging for RTPlanning
PatientAssessment
On-TreatmentQuality
Management
Equipment andSoftware Quality
Management
Post-TreatmentCompletion
Unanswered
Total Number of Events = 1,626 as of April 1, 2016
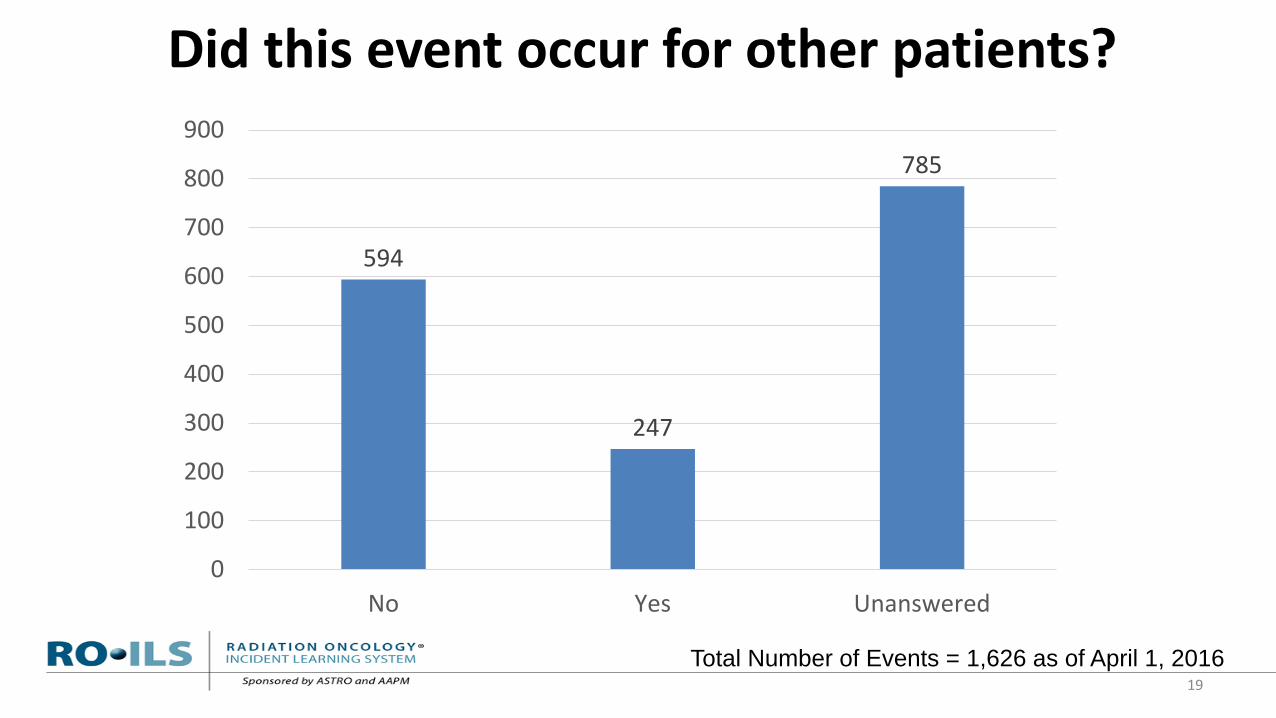
Did this event occur for other patients?
Total Number of Events = 1,626 as of April 1, 2016 19
594
247
785
0
100
200
300
400
500
600
700
800
900
No Yes Unanswered
20
21
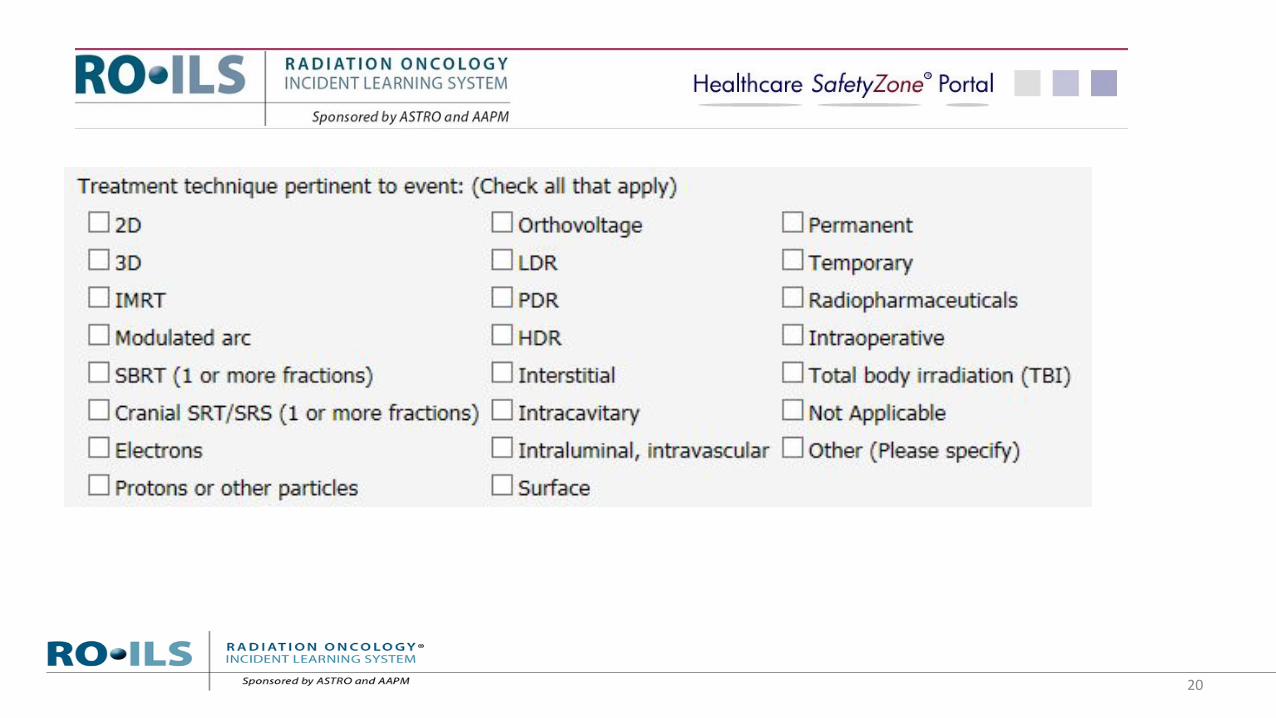
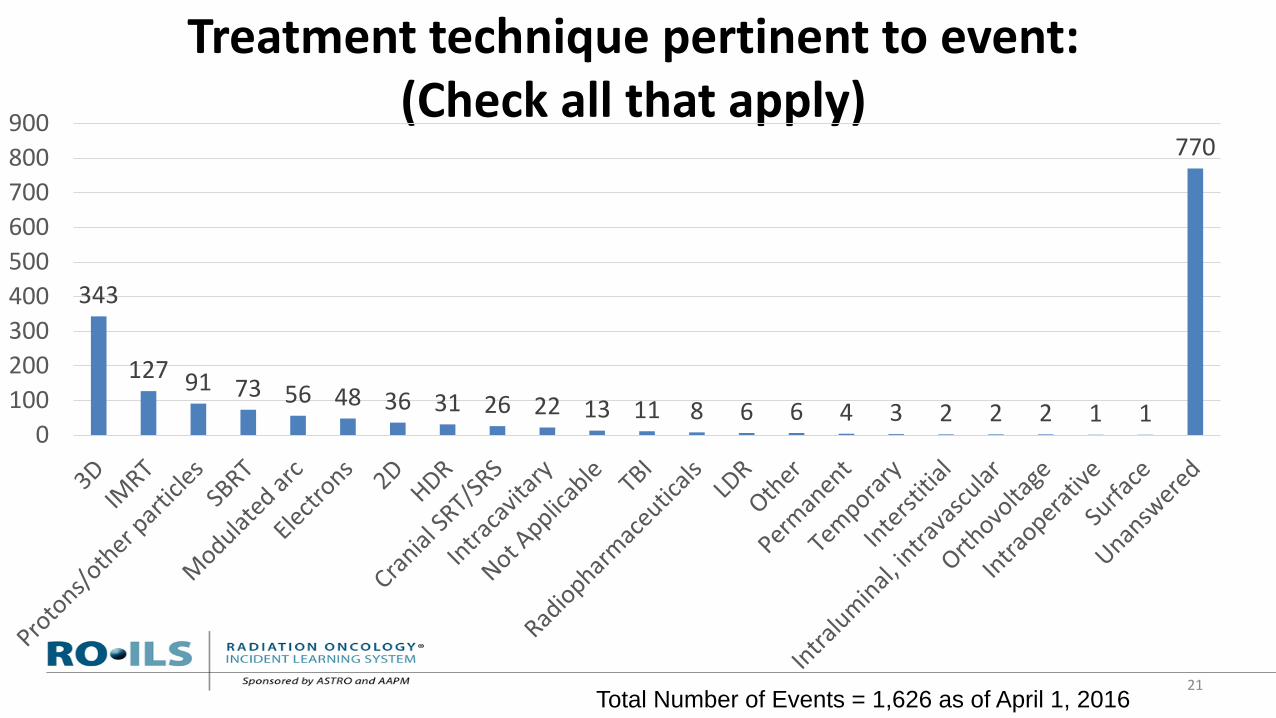
Treatment technique pertinent to event: (Check all that apply)
343
127 91 73 56 48 36 31 26 22 13 11 8 6 6 4 3 2 2 2 1 1
770
0100200300400500600700800900
Total Number of Events = 1,626 as of April 1, 2016
22

23
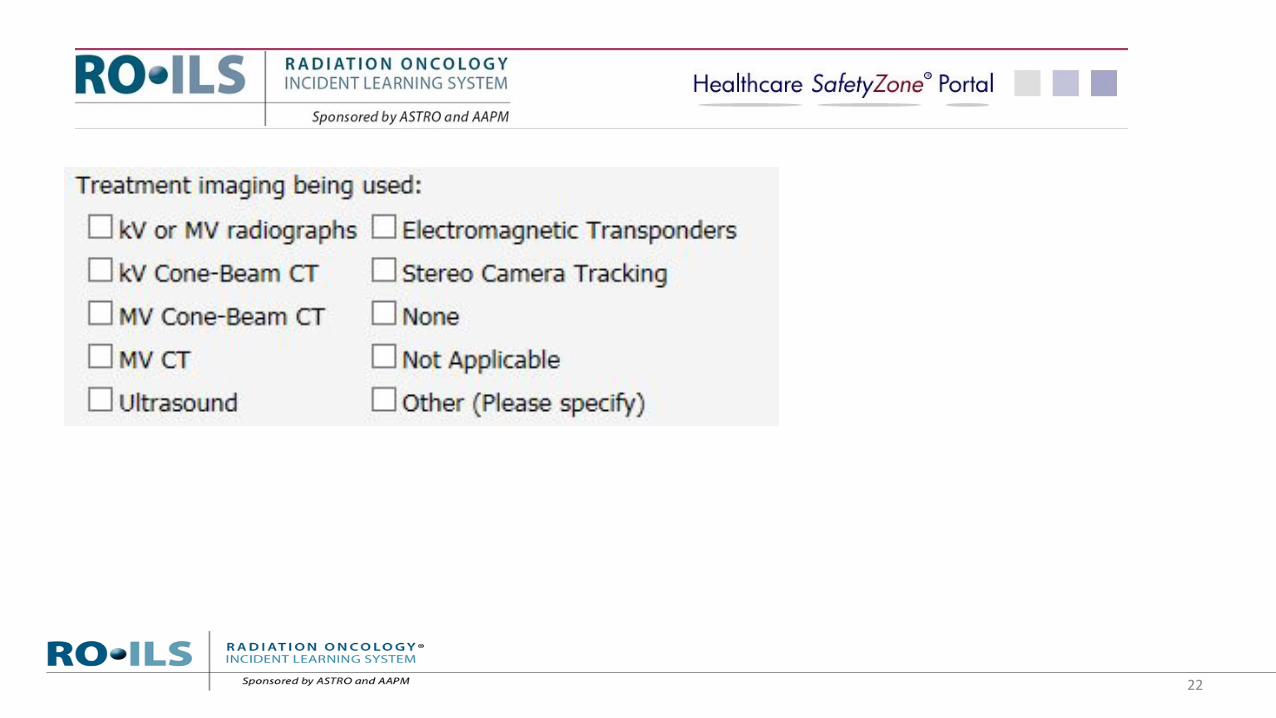
Treatment imaging being used:
383
150 56 39 10 7 7 4 3
1012
0
200
400
600
800
1000
1200
Total Number of Events = 1,626 as of April 1, 2016

24
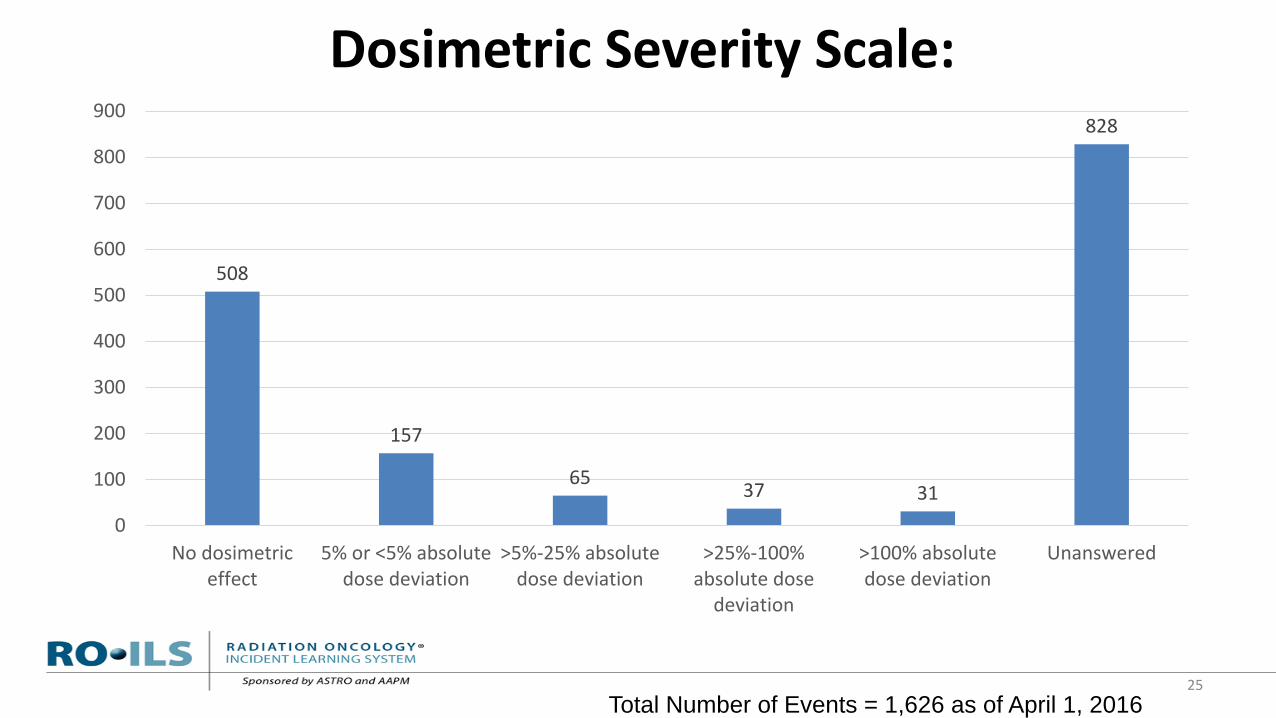
• No dosimetric effect • 5% or <5% absolute dose deviation • >5%-25% absolute dose deviation • >25%-100% absolute dose deviation • Unanswered
25
Dosimetric Severity Scale:
Total Number of Events = 1,626 as of April 1, 2016
508
157
65 37 31
828
0
100
200
300
400
500
600
700
800
900
No dosimetriceffect
5% or <5% absolutedose deviation
>5%-25% absolutedose deviation
>25%-100%absolute dose
deviation
>100% absolutedose deviation
Unanswered

26
• Administrator • Attending Radiation Oncologist • Dosimetrist • Manager • Nurse, NP or PA • Other Physician • Physicist • Radiation Therapist • Resident Radiation Oncologist • Other
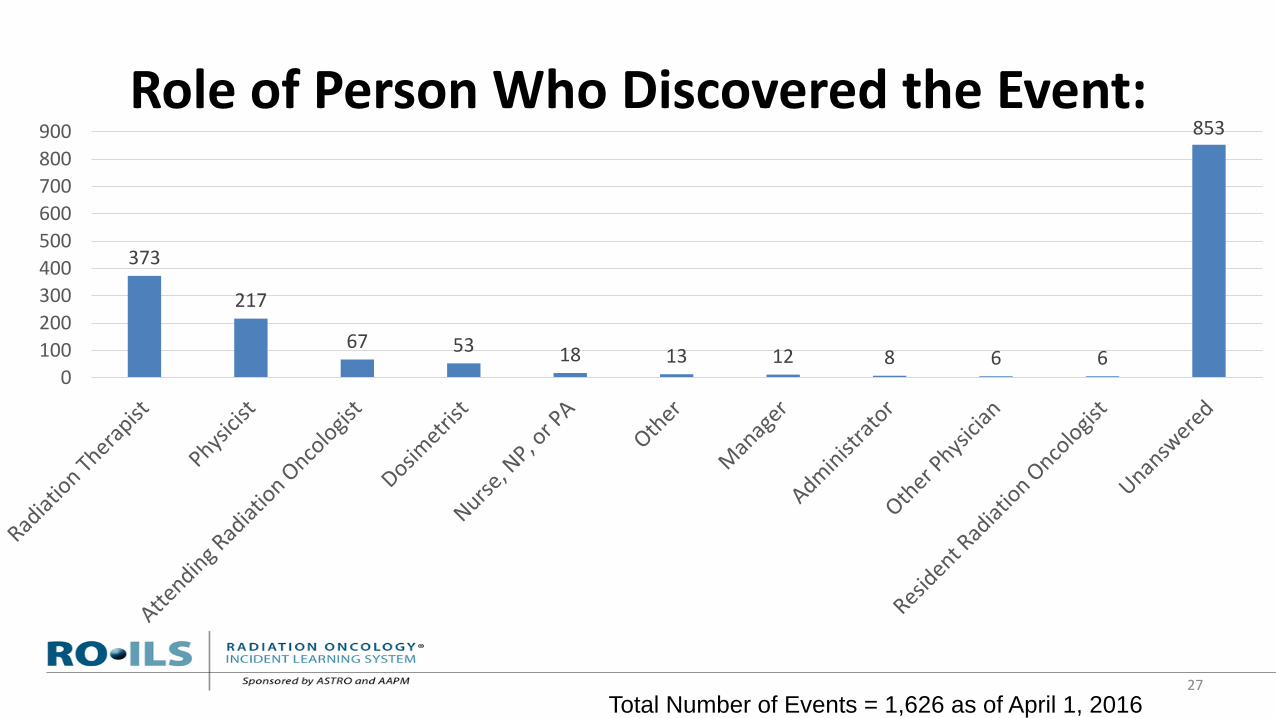
Role of Person Who Discovered the Event:
27
373
217
67 53 18 13 12 8 6 6
853
0100200300400500600700800900
Total Number of Events = 1,626 as of April 1, 2016
Revised Data Elements – Process
• Began reviewing current data elements in June 2015. – Participant survey results. – Review by RO-HAC, RO-ILS Steering Committee, ASTRO MDQA
Subcommittee. – Inter-rater reliability study. – Review by RO-HAC, RO-ILS Steering Committee, ASTRO MDQA
Subcommittee, ASTRO CAQC leadership.
• Revised data elements coming Summer 2016.
28
Revised Data Elements – What to Expect
• Fewer overall questions. • Significant branching logic – only see pertinent questions. • More required data elements. • More user friendly. • Additional educational materials will also be released in
Summer 2016.
29

RO-HAC Reports
• Issued five quarterly reports, with one in progress.
• Reports consist of: • Report card. • Data analysis and case review. • Aggregate trending graphs.
• Facility-specific reports: Q2 2015, Q4 2015.
30
General RO-HAC Findings • Communication. A recurring issue and appears to be a significant driver of error. • Training and education. A number of reports centered on missteps made involving
students/trainees not remedied by staff. • Policies and procedures. Events are related to failure to following, not lack of appropriate
policies or procedures. • Wrong site or dose. Recurring theme meriting root cause analysis. • Incorrect isocenter. Events with incorrect isocenter are largely near-miss events (identified
prior to treatment), they reveal an error pathway that can cause serious harm to patients. • Changes to plan. Changing a patient’s treatment once under way appears to be a risk-prone
process. • Hastiness to commence procedure. Root cause of many incidents, leading to near misses or
patient incidents. • Review of plans. The review of plans plays a key role in preventing errors from impacting
patients. • Many QA processes are effective in catching near misses.
31

Case Study #1: Old CT Simulation Set
32
• Dosimetrist checking CT simulations notices a patient’s CT set was not imported.
• Dosimetrist checks plan tracker; patient’s plan status said “Plan Approved.”
• Upon further investigation, it was determined that the MD resident drew on the patient’s old CT sim the day before.
• Attending MD and planning dosimetrist did not notice and were finalizing plan on the wrong CT sim.
• Plan was copied on to the new CT sim and blocks/volumes had to be modified due to tumor growth.
33
Case Study #1: Recommendations
• Planning scan could be given names that clearly identify the date of the scan and the site being treated.
• It would be useful to have planning systems warn that a new plan is being created on an old scan and ask for confirmation. • If your planning system does not currently do that, consider
submitting a product improvement suggestion to the manufacturer.
Case Study #2: Mispositioned Treatment
34
• A single fraction of a patient’s palliative treatment to the thoracic spine was incorrectly delivered to the previously irradiated lumbar spine based on old tattoos located in the lumbar region.
• The shift from the old tattoos to the new treatment volume planned in dosimetry was approved by physics and the radiation oncologist, but did not occur correctly when it came time for the patient’s treatment delivery.
• Poor quality portal images in an area without readily visible anatomic landmarks were approved by the physician and the treatment was delivered before the error was appreciated.
Case Study #2: Recommendations
35
• Planning and safe delivery of treatment to a target shifted from skin landmarks requires careful communications and documentation among team members.
• Lean staffing and busyness in simulation were contributing factors to this event.
• CBCT may in certain cases offer a more reliable tool than portal imaging for confirmation of correct field placement.

Case Study #3: Incorrect Vertebral Body Treated
36
• A patient was being treated with a fractionated dose of 4Gy for 5 fractions for the palliation of bone metastasis in the thoracic-lumbar spine.
• The incorrect vertebral body was treated for 2 of the 5 fractions. • Cone-beam CT was used to perform the alignment. • The automatic image alignment algorithm locked onto the incorrect
vertebral body, thus resulting in a large shift of the patient. • The incident was discovered on the third fraction.

Case Study #3: Recommendations
37
• Policies and procedures should be clear regarding the actions to take when large shifts are indicated from IGRT imaging.
• Some centers have adopted policies that require a secondary verification of patient setup when the shifts are larger than a specified amount.
• Use a cone-beam CT setting that captures a larger extent of anatomy where appropriate.
• One vendor supplies a “topogram” to specify the superior-inferior extent of the scan.
• Another vendor has predefined settings ranging up to 26 cm in this dimension. • Use of kilovoltage (kV) or megavoltage (MV) planar images to verify alignment in
addition to cone-beam CT. • These planar images can show a larger extent of anatomy and reduce the
likelihood of aligning to a wrong vertebral body.
Case Study #4: Fractions and dose inverted
38
• A patient presented for his first radiation fraction, was placed on the table, and during time-out it was realized that this was to be fraction 1 of 180 fractions.
• The prescription was for 180 cGy x 42 fractions = 7,560 cGy. Instead, the plan that was generated, and subsequently approved by the physician and physics was 42 cGy x 180 fractions = 7,560 cGy.
• While the total dose, and the dose-volume histograms (DVHs) and isodose lines were correct, the fraction size was incorrect.
• The patient had to be taken off the table and replanned.
Case Study #4: Recommendations
39
• Utilize a standard system for writing the prescription. • Where possible, utilize units.
• 180 x 42 is not sufficient. • ASTRO is finalizing a White Paper on Standardizing Dose Prescriptions. • Recommendation from the draft paper:
“[W]e recommend all radiation prescriptions contain the following information in this order, with these units, without intervening additional data”:
Treatment Site
Method of Delivery
Dose per Fraction (cGy)
Total Number of Fractions
Total Dose (cGy)
Legal Challenges to the PSQIA
• Charles v. Southern Baptist Hospital (Florida). • Tibbs v. Bunnell (Kentucky). • Carron v. Rosenthal (Rhode Island). • Illinois Department of Financial and Professional Regulation v.
Walgreen Co. (Illinois).
40
Facts of Charles v. Southern Baptist Hospital • The Charles family claimed that Marie Charles suffered a catastrophic
neurological injury due to Southern Baptist's negligence. • Southern Baptist Hospital of Florida, Inc. reports incidents to PSO Florida. • The Charles family requested documents under Florida’s Amendment 7. • Southern Baptist handed over some of the requested documents, but not
all, claiming privilege under the Patient Safety Act. • The Charles family moved to compel production, arguing that the
documents in question were not privileged because they were collected for the purpose of complying with Florida state law.
41

Timeline of Charles v. Southern Baptist Hospital
• Trial judge found that information collected for state or federal record keeping or reporting is not PSWP. Granted motion to compel production of documents.
• Southern Baptist appealed decision. – ASTRO signed onto a “friend of the court” brief supporting Southern
Baptist. • Appellate Court found that the information the hospital entered
into its PSES qualified as PSWP and was protected, despite Florida laws requiring the same information to be gathered and maintained.
42

Timeline of Charles v. Southern Baptist Hospital (Continued)
• Appellate court said that absent an allegation that a provider has failed to comply with its state reporting or record keeping requirements, the trail court should not “rummage through” a PSES in search of documents that could possibly serve a dual purpose.
• Patient Safety Act preempts Amendment 7. • Documents that meet the definition of PSWP are categorically
protected and excluded from production under PSQIA. • Charles filed appeal to the Supreme Court of Florida.
43

The Law in Question – “Amendment 7” • “Patients’ right to know about adverse medical incidents”
– Article 10, section 25, of the Florida Constitution. – Passed by voter referendum in 2004.
• Patients have a right to access any records made or received in the course of business by a health care facility or provider relating to any adverse medical incident.
• In providing such access, the identity of patients involved in the incidents shall not be disclosed, and any privacy restrictions imposed by federal law shall be maintained.
44

“Amendment 7” – Adverse Medical Incident
• “The phrase ‘adverse medical incident’ means medical negligence, intentional misconduct, and any other act, neglect, or default of a health care facility or health care provider that caused or could have caused injury to or death of a patient, including, but not limited to, those incidents that are required by state or federal law to be reported to any governmental agency or body, and incidents that are reported to or reviewed by any health care facility peer review, risk management, quality assurance, credentials, or similar committee, or any representative of any such committees.”
45
Tibbs v. Bunnell • Following the death of a patient, a hospital prepared an incident
report and submitted it to a PSO. • The estate of the deceased sought the incident report. • The trial court found that the Patient Safety Act did not apply and
ordered the report turned over under Kentucky law. • The hospital filed an appeal. • The appeals court found that the Patient Safety Act preempted
Kentucky law and the reports were privileged to the extent that it contained “self-examining analysis”.
• The hospital appealed the partial victory to the Kentucky Supreme Court arguing that the reports were fully privileged.
46
Tibbs v. Bunnell (Continued) • Kentucky Supreme Court held that incident reports may be privileged even if
they do not contain a “self-examining analysis”. However, the reports may be discoverable if they are prepared pursuant to state laws requiring their preparation in connection with the state’s regulation of health-care facilities.
• The hospital asked for a rehearing of the Kentucky Supreme Court, which was denied.
• The hospital has filed an appeal to the US Supreme Court. – ASTRO signed on to a “friend of the court” brief supporting the hospital’s petition to
the US Supreme Court. • The US Supreme Court is waiting to see if the United States Solicitor General
will submit a brief in support of the hospital.
47
Carron v. Rosenthal • Medical malpractice suit following the death of an infant. • Under the Rhode Island Patient Safety Act, a law similar to the
federal Patient Safety Act, the hospital submitted an incident report to its PSO following the infant's death.
• A trial court ordered the hospital to show the incident report to its nurses to refresh their memory of the incident prior to being deposed by the plaintiff.
• The hospital has filed an appeal to the Rhode Island Supreme Court.
48
Illinois Department of Financial and Professional Regulation (IDFPR) v. Walgreen Co.
• The issue in this case was whether the privilege against non-disclosure set forth in the Patient Safety Act preempt Illinois state laws.
• IDFPR issued subpoenas to Walgreens following a report that three pharmacists may have violated the Pharmacy Practice Act.
• Walgreens responded that the only documents it had were reports it had prepared under the Patient Safety Act for purposes of submission to a PSO and that they were privileged from discovery.
49

Illinois Department of Financial and Professional Regulation (IDFPR) v. Walgreen Co. (Continued)
• IDFPR sought a court order to compel production, but the trial judge found that the reports were privileged under the Patient Safety Act.
• Trial judge dismissed the case. • IDFPR appealed, but the Illinois Appellate Court affirmed.
50

Where are we going? • Revised data elements coming summer 2016. • Update educational materials. • Continue RO-HAC quarterly reports. • Develop the capacity to allow participants to transfer data from other incident
learning systems to RO-ILS. • Continue to monitor legal challenges to the Patient Safety Act. • ASTRO 2016 Annual Meeting sessions:
– “RO-ILS® and APEx®: Instruments for Quality Improvement” – “Role of Promoting Professionalism as Part of Safety Culture: Structuring an Effective
Program” – RO-ILS User Meeting – RO-ILS Safe Table
51
www.astro.org/ROILS [email protected]
Program Contact: Cindy Tomlinson
Senior Manager for Security and Safety [email protected]
703.839.7366
52