Embed Size (px)
Citation preview
Contents RISK MODELS ...................................................................................................................................................... 1 BACKGROUND..................................................................................................................................................... 1 MORTALITY MODEL ........................................................................................................................................... 2
Approach ............................................................................................................................................................ 2 Proposed changes ............................................................................................................................................ 2 Model Performance .......................................................................................................................................... 3
BLEEDING MODEL .............................................................................................................................................. 6 Approach ............................................................................................................................................................ 6 Bleeding Definition ............................................................................................................................................ 6 Proposed changes ............................................................................................................................................ 6 Model Performance .......................................................................................................................................... 8
PERFORMANCE MEASURES ......................................................................................................................... 10 BACKGROUND ............................................................................................................................................... 10 Measure 1: Comprehensive Documentation of Indications for PCI......................................................... 10 Measure 2: Assessment of Candidacy for Dual-Antiplatelet Therapy ..................................................... 11 Measure 3: Use of Embolic Protection Devices in the Treatment of Saphenous Vein Bypass Graft Disease ............................................................................................................................................................. 12 Measure 4: Documentation of Pre-procedural Glomerular Filtration Rate and Contrast Dose Used During the Procedure ...................................................................................................................................... 13 Measure 5: Post procedural Optimal Medical Therapy Composite .......................................................... 14 Measure 6: Cardiac Rehabilitation Patient Referral ................................................................................... 16 Measure 7: Annual Hospital PCI Volume .................................................................................................... 18
REFERENCES .................................................................................................................................................... 20
RISK MODELS
BACKGROUND The American College of Cardiology Foundation’s (ACCF) National Cardiovascular Data Registry (NCDR) uses statistical models to provide risk-adjusted outcomes to participating hospitals. The results of these models can be used to benchmark performance and enhance quality improvement efforts. The NCDR CathPCI Registry has several models currently approved by the Science and Quality Oversight Committee (SQOC). Two of the Episode of Care level models are the focus of this review and comment period. The first model is the in-hospital risk-adjusted mortality identified using data submitted to the registry by participating sites. The second model presented is the in-hospital risk-adjusted bleeding. In March 2015, a workgroup was established to update these risk models and develop well performing models with a more parsimonious set of data elements. Analytic support for the models was provided by staff from the Mid-America Heart Institute (MAHI). The risk adjusted mortality (RAM) model methodology (Brennan J, Curtis JP, Dai D, et al., 2013) (1) and risk-adjusted bleeding (RAB) model methodology (Rao SV, McCoy LA, Spertus JA, et al, 2013) (2) that the CathPCI Registry currently reports are both publically available in the literature.
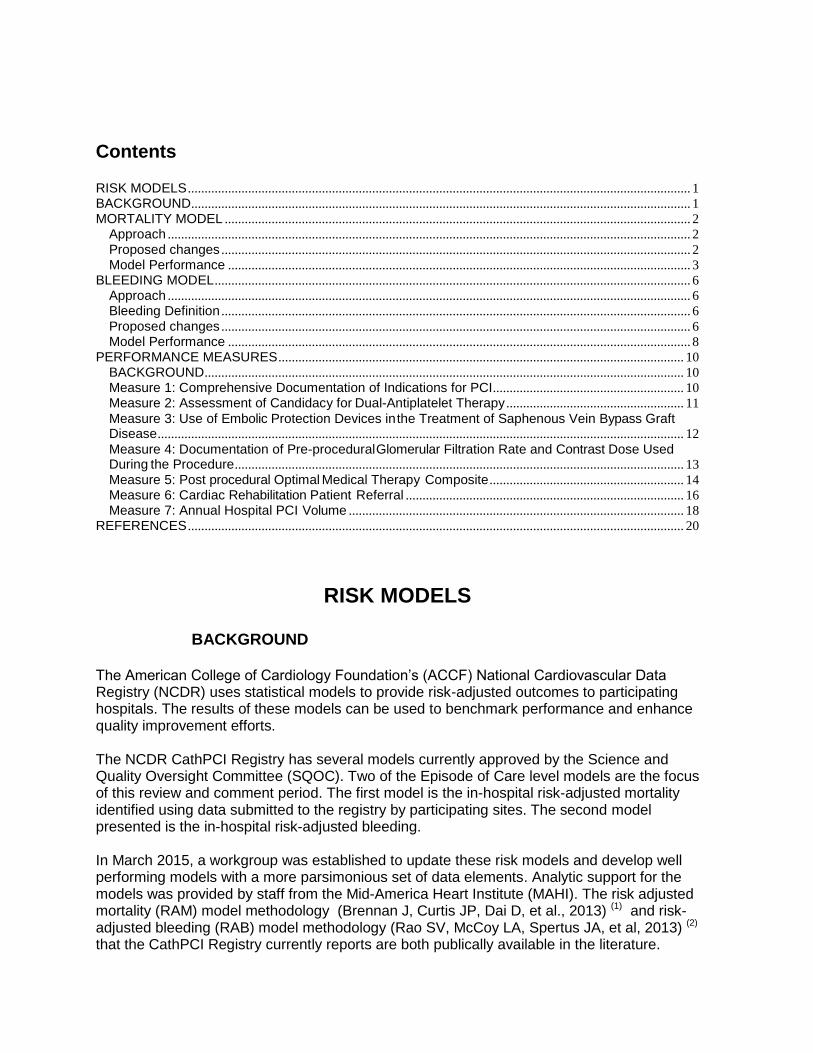
MORTALITY MODEL Approach The new models were derived and validated using CathPCI Registry Version 4.4 using the Harrell approach of retaining the most significant variables. (Figure 1)
Figure 1. Inpatient Risk- adjusted Mortality Modeling Approach
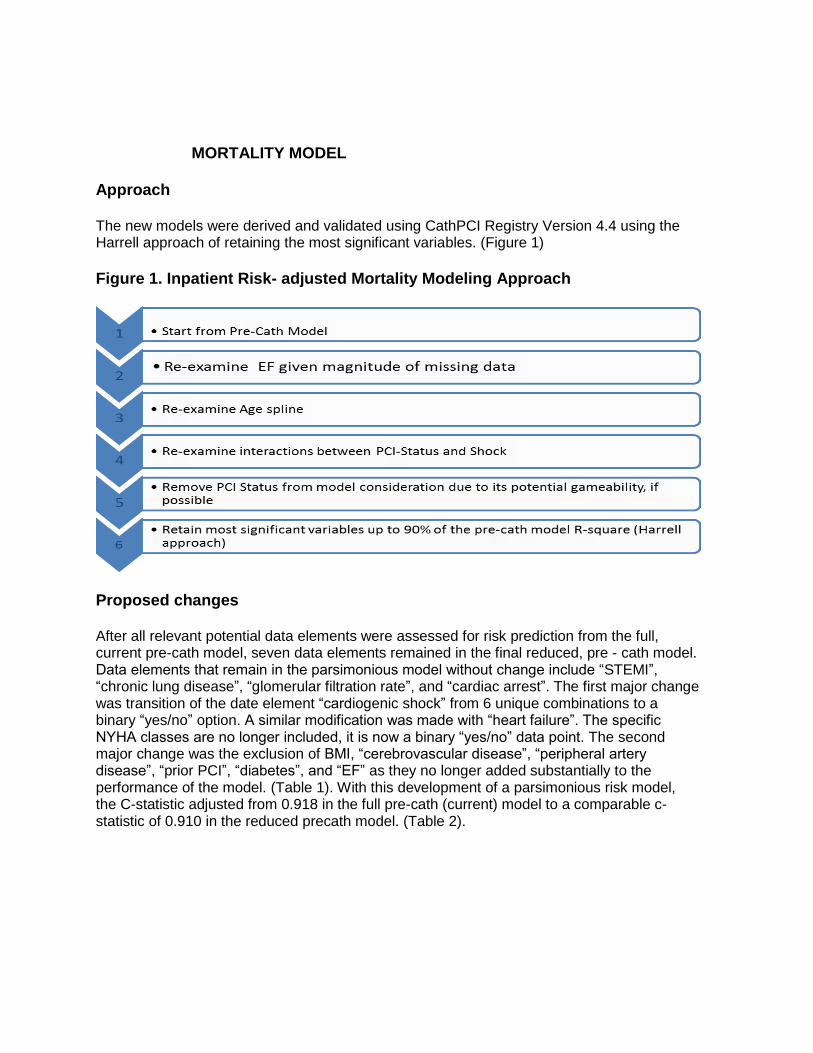
Proposed changes After all relevant potential data elements were assessed for risk prediction from the full, current pre-cath model, seven data elements remained in the final reduced, pre - cath model. Data elements that remain in the parsimonious model without change include “STEMI”, “chronic lung disease”, “glomerular filtration rate”, and “cardiac arrest”. The first major change was transition of the date element “cardiogenic shock” from 6 unique combinations to a binary “yes/no” option. A similar modification was made with “heart failure”. The specific NYHA classes are no longer included, it is now a binary “yes/no” data point. The second major change was the exclusion of BMI, “cerebrovascular disease”, “peripheral artery disease”, “prior PCI”, “diabetes”, and “EF” as they no longer added substantially to the performance of the model. (Table 1). With this development of a parsimonious risk model, the C-statistic adjusted from 0.918 in the full pre-cath (current) model to a comparable c-statistic of 0.910 in the reduced precath model. (Table 2).
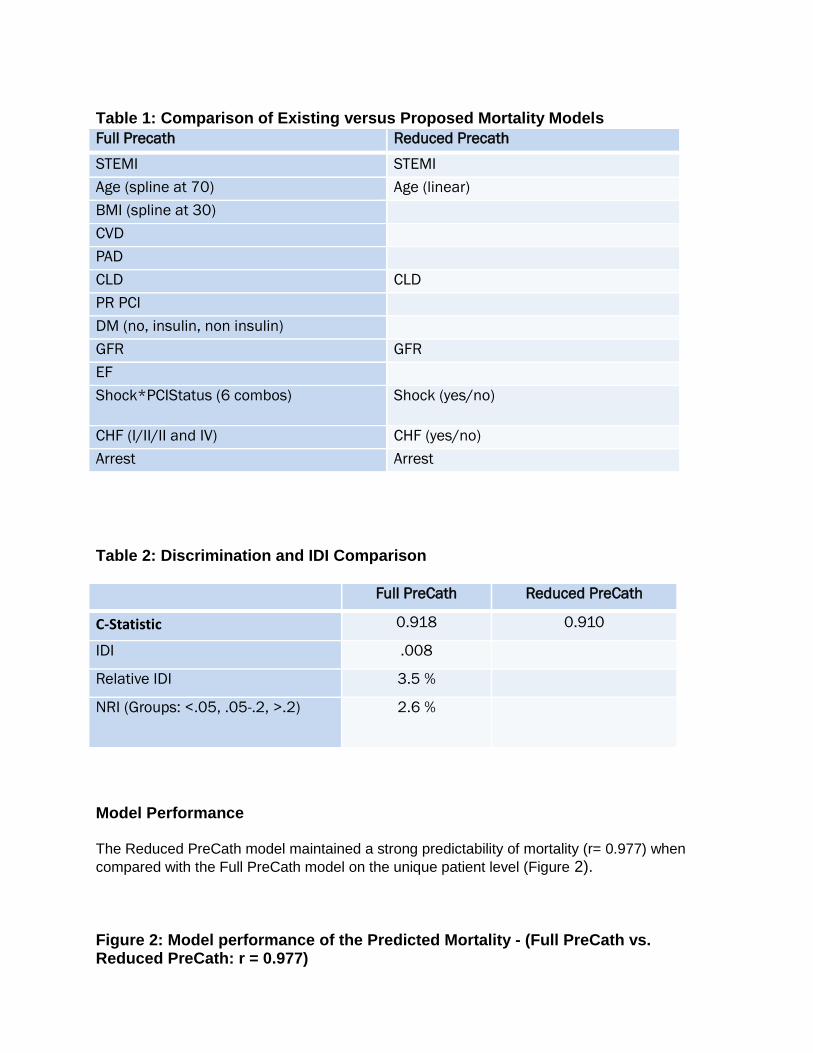
Table 1: Comparison of Existing versus Proposed Mortality Models
Table 2: Discrimination and IDI Comparison
Full PreCath Reduced PreCath
C-Statistic 0.918 0.910
IDI .008
Relative IDI 3.5 %
NRI (Groups: <.05, .05-.2, >.2) 2.6 %
Model Performance The Reduced PreCath model maintained a strong predictability of mortality (r= 0.977) when
compared with the Full PreCath model on the unique patient level (Figure 2). Figure 2: Model performance of the Predicted Mortality - (Full PreCath vs. Reduced PreCath: r = 0.977)
Full Precath Reduced Precath
STEMI STEMI
Age (spline at 70) Age (linear)
BMI (spline at 30)
CVD
PAD
CLD CLD
PR PCI
DM (no, insulin, non insulin)
GFR GFR
EF
Shock*PCIStatus (6 combos) Shock (yes/no)
CHF (I/II/II and IV) CHF (yes/no)
Arrest Arrest
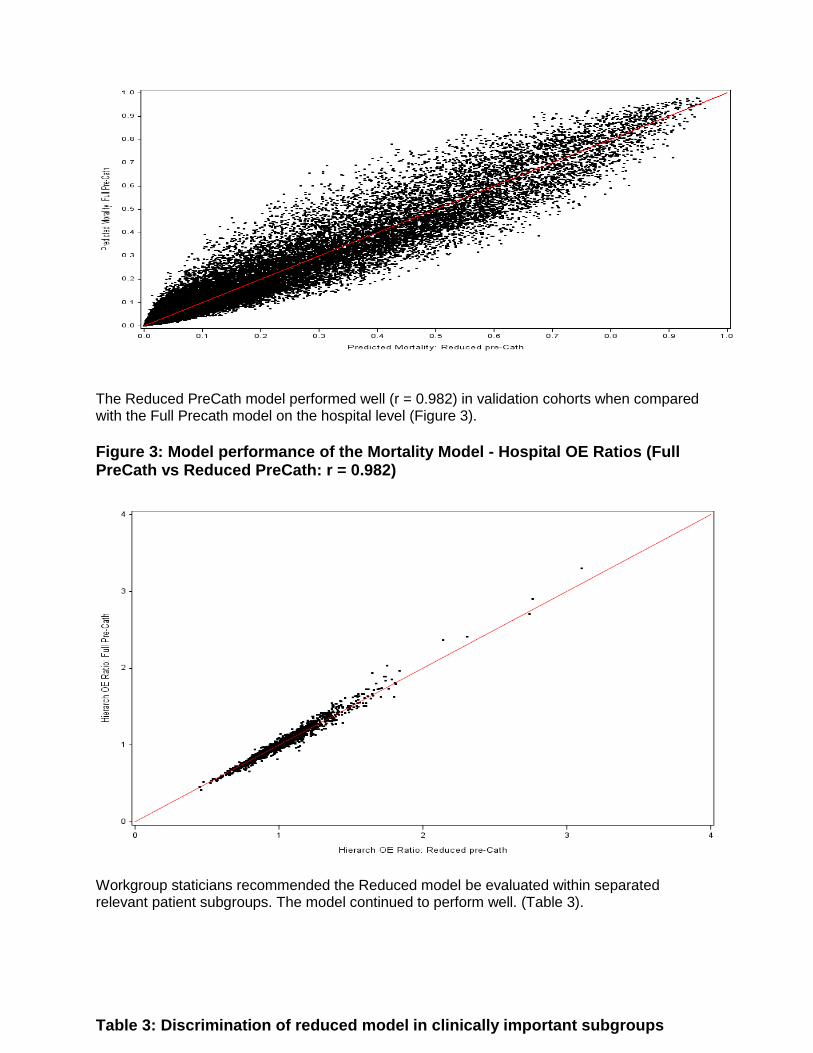
The Reduced PreCath model performed well (r = 0.982) in validation cohorts when compared with the Full Precath model on the hospital level (Figure 3).
Figure 3: Model performance of the Mortality Model - Hospital OE Ratios (Full PreCath vs Reduced PreCath: r = 0.982)
Workgroup staticians recommended the Reduced model be evaluated within separated relevant patient subgroups. The model continued to perform well. (Table 3).
Table 3: Discrimination of reduced model in clinically important subgroups
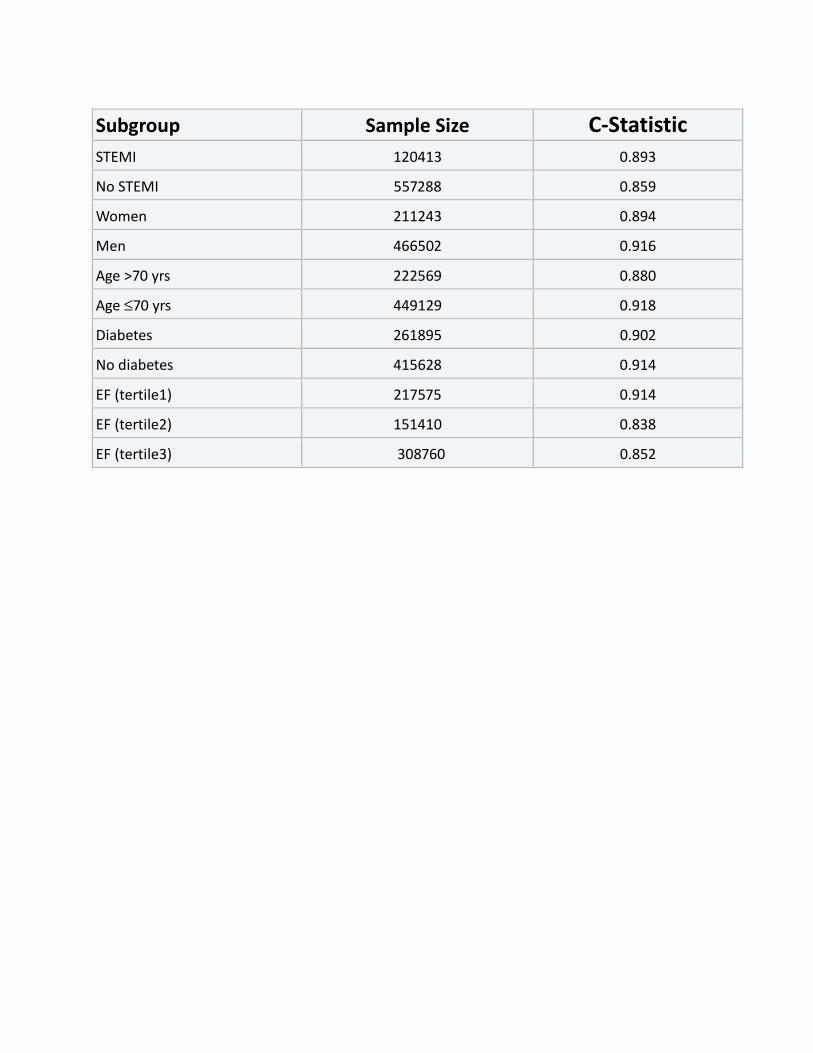
Subgroup Sample Size C-Statistic
STEMI 120413 0.893
No STEMI 557288 0.859
Women 211243 0.894
Men 466502 0.916
Age >70 yrs 222569 0.880
Age ≤70 yrs 449129 0.918
Diabetes 261895 0.902
No diabetes 415628 0.914
EF (tertile1) 217575 0.914
EF (tertile2) 151410 0.838
EF (tertile3) 308760 0.852
BLEEDING MODEL Approach
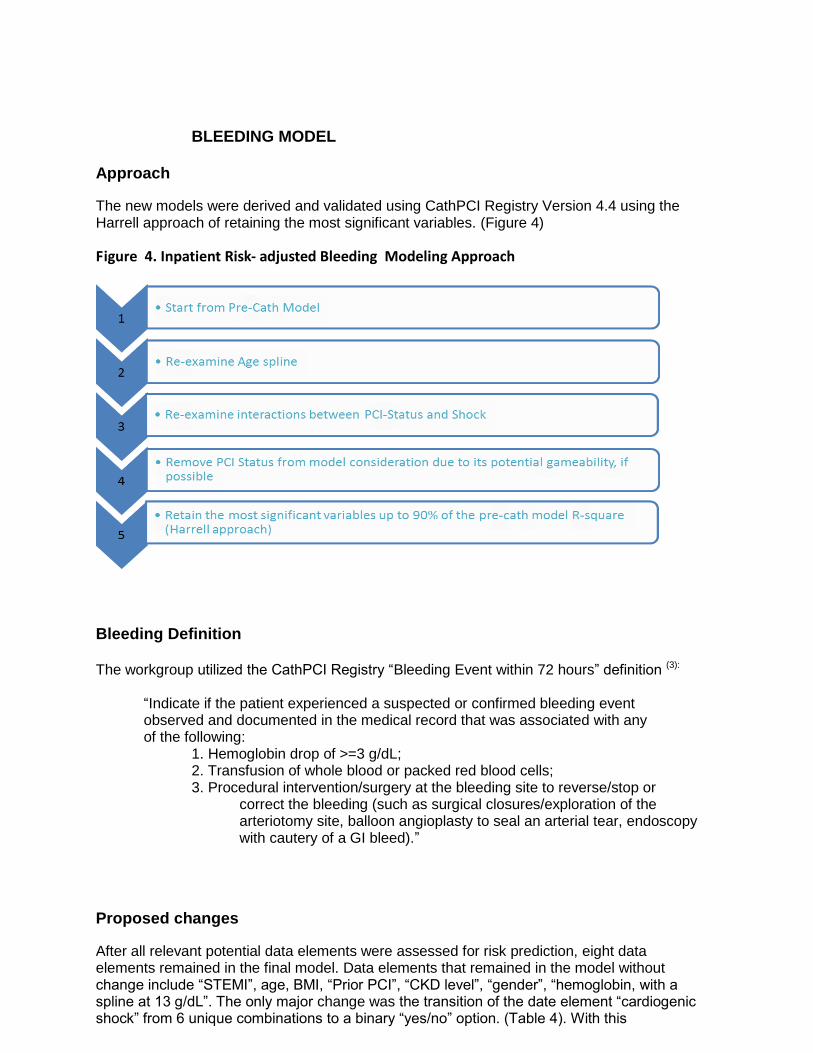
The new models were derived and validated using CathPCI Registry Version 4.4 using the Harrell approach of retaining the most significant variables. (Figure 4)
Figure 4. Inpatient Risk- adjusted Bleeding Modeling Approach
Bleeding Definition The workgroup utilized the CathPCI Registry “Bleeding Event within 72 hours” definition (3):
“Indicate if the patient experienced a suspected or confirmed bleeding event observed and documented in the medical record that was associated with any of the following:
1. Hemoglobin drop of >=3 g/dL; 2. Transfusion of whole blood or packed red blood cells; 3. Procedural intervention/surgery at the bleeding site to reverse/stop or
correct the bleeding (such as surgical closures/exploration of the arteriotomy site, balloon angioplasty to seal an arterial tear, endoscopy with cautery of a GI bleed).”
Proposed changes
After all relevant potential data elements were assessed for risk prediction, eight data elements remained in the final model. Data elements that remained in the model without change include “STEMI”, age, BMI, “Prior PCI”, “CKD level”, “gender”, “hemoglobin, with a spline at 13 g/dL”. The only major change was the transition of the date element “cardiogenic shock” from 6 unique combinations to a binary “yes/no” option. (Table 4). With this
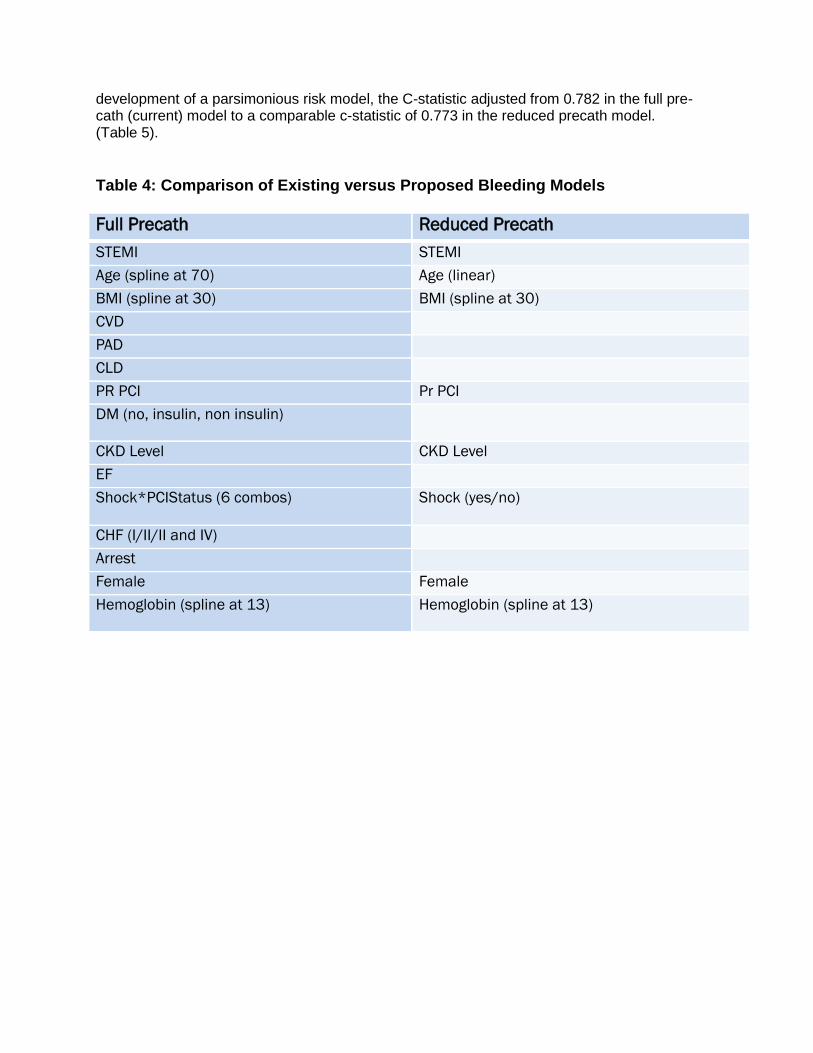
development of a parsimonious risk model, the C-statistic adjusted from 0.782 in the full pre-cath (current) model to a comparable c-statistic of 0.773 in the reduced precath model. (Table 5).
Table 4: Comparison of Existing versus Proposed Bleeding Models
Full Precath Reduced Precath STEMI STEMI
Age (spline at 70) Age (linear)
BMI (spline at 30) BMI (spline at 30)
CVD
PAD
CLD
PR PCI Pr PCI
DM (no, insulin, non insulin)
CKD Level CKD Level
EF
Shock*PCIStatus (6 combos) Shock (yes/no)
CHF (I/II/II and IV)
Arrest
Female Female
Hemoglobin (spline at 13) Hemoglobin (spline at 13)
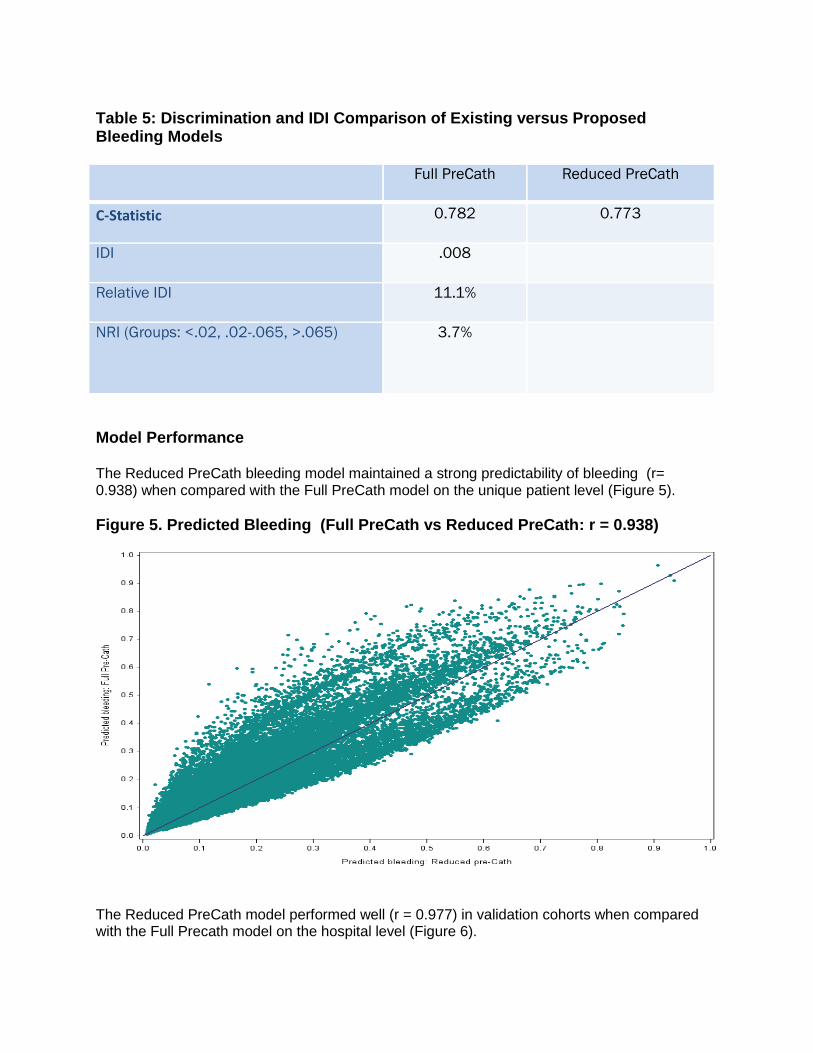
Table 5: Discrimination and IDI Comparison of Existing versus Proposed Bleeding Models
Full PreCath Reduced PreCath
C-Statistic 0.782 0.773
IDI .008
Relative IDI 11.1%
NRI (Groups: <.02, .02-.065, >.065) 3.7%
Model Performance The Reduced PreCath bleeding model maintained a strong predictability of bleeding (r= 0.938) when compared with the Full PreCath model on the unique patient level (Figure 5).
Figure 5. Predicted Bleeding (Full PreCath vs Reduced PreCath: r = 0.938)
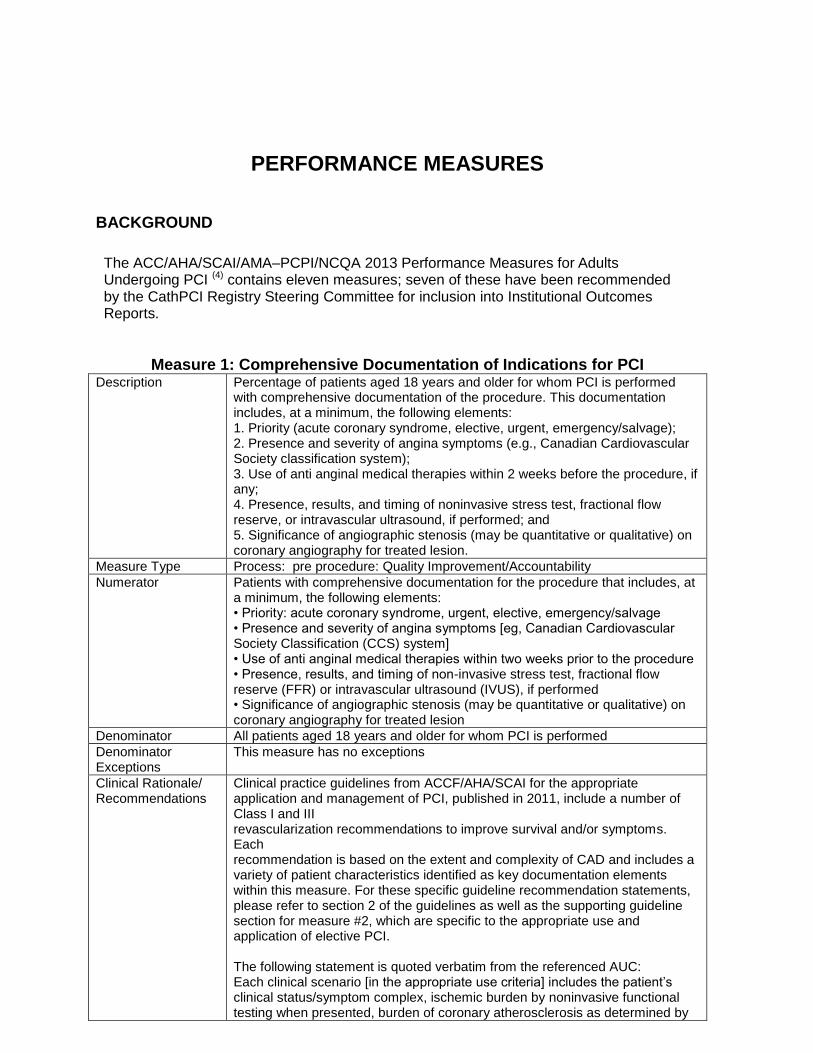
The Reduced PreCath model performed well (r = 0.977) in validation cohorts when compared with the Full Precath model on the hospital level (Figure 6).
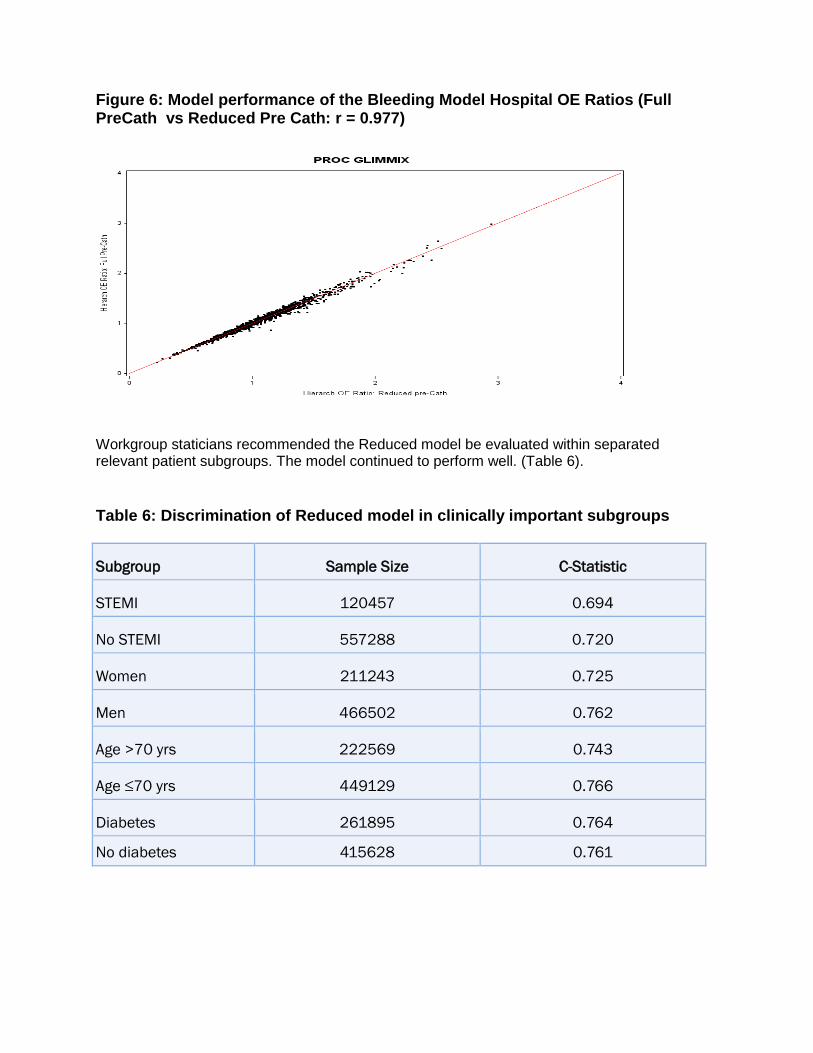
Figure 6: Model performance of the Bleeding Model Hospital OE Ratios (Full PreCath vs Reduced Pre Cath: r = 0.977)
Workgroup staticians recommended the Reduced model be evaluated within separated relevant patient subgroups. The model continued to perform well. (Table 6).
Table 6: Discrimination of Reduced model in clinically important subgroups
Subgroup Sample Size C-Statistic
STEMI 120457 0.694
No STEMI 557288 0.720
Women 211243 0.725
Men 466502 0.762
Age >70 yrs 222569 0.743
Age ≤70 yrs 449129 0.766
Diabetes 261895 0.764
No diabetes 415628 0.761
PERFORMANCE MEASURES
BACKGROUND
The ACC/AHA/SCAI/AMA–PCPI/NCQA 2013 Performance Measures for Adults Undergoing PCI (4) contains eleven measures; seven of these have been recommended by the CathPCI Registry Steering Committee for inclusion into Institutional Outcomes Reports.
Measure 1: Comprehensive Documentation of Indications for PCI Description Percentage of patients aged 18 years and older for whom PCI is performed
with comprehensive documentation of the procedure. This documentation includes, at a minimum, the following elements: 1. Priority (acute coronary syndrome, elective, urgent, emergency/salvage); 2. Presence and severity of angina symptoms (e.g., Canadian Cardiovascular Society classification system); 3. Use of anti anginal medical therapies within 2 weeks before the procedure, if any; 4. Presence, results, and timing of noninvasive stress test, fractional flow reserve, or intravascular ultrasound, if performed; and 5. Significance of angiographic stenosis (may be quantitative or qualitative) on coronary angiography for treated lesion.
Measure Type Process: pre procedure: Quality Improvement/Accountability
Numerator Patients with comprehensive documentation for the procedure that includes, at a minimum, the following elements: • Priority: acute coronary syndrome, urgent, elective, emergency/salvage • Presence and severity of angina symptoms [eg, Canadian Cardiovascular Society Classification (CCS) system] • Use of anti anginal medical therapies within two weeks prior to the procedure • Presence, results, and timing of non-invasive stress test, fractional flow reserve (FFR) or intravascular ultrasound (IVUS), if performed • Significance of angiographic stenosis (may be quantitative or qualitative) on coronary angiography for treated lesion
Denominator All patients aged 18 years and older for whom PCI is performed
Denominator Exceptions
This measure has no exceptions
Clinical Rationale/ Recommendations
Clinical practice guidelines from ACCF/AHA/SCAI for the appropriate application and management of PCI, published in 2011, include a number of Class I and III revascularization recommendations to improve survival and/or symptoms. Each recommendation is based on the extent and complexity of CAD and includes a variety of patient characteristics identified as key documentation elements within this measure. For these specific guideline recommendation statements, please refer to section 2 of the guidelines as well as the supporting guideline section for measure #2, which are specific to the appropriate use and application of elective PCI. The following statement is quoted verbatim from the referenced AUC: Each clinical scenario [in the appropriate use criteria] includes the patient’s clinical status/symptom complex, ischemic burden by noninvasive functional testing when presented, burden of coronary atherosclerosis as determined by
angiography, and intensity of medical therapy in the determination of the appropriate use of coronary revascularization. (ACCF/SCAI/STS/AATS/AHA/ASNC/HFSA/SCCT, 2012)
Relevant Citations Nallamothu BK, Tommaso CL, Anderson HV, Anderson JL, Cleveland JC, Dudley RA, Duffy PL, Faxon DP, Gurm HS, Hamilton LA, Jensen NC, Josephson RA, Malenka DJ, Maniu CV, McCabe KW, Mortimer JD, Patel MR, Persell SD, Rumsfeld JS, Shunk KA, Smith SC, Stanko SJ, Watts B. ACC/AHA/SCAI/AMA–Convened PCPI/NCQA 2013 performance measures for adults undergoing percutaneous coronary intervention: a report of the American College of Cardiology/American Heart Association Task Force on Performance Measures, the Society for Cardiovascular Angiography and Interventions, the American Medical Association–Convened Physician Consortium for Performance Improvement, and the National Committee for Quality Assurance. J Am Coll Cardiol 2014;63:722–45. Levine GN, Bates ER, Blankenship JC, et al. 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. J Am Coll Cardiol 2011; 58:e44–122. Patel MR, Dehmer GJ, Hirshfeld JW, Smith PK, Spertus JA. ACCF/SCAI/STS/AATS/AHA/ASNC/HFSA/SCCT 2012 appropriate use criteria for coronary revascularization focused update: a report of the American College of Cardiology Foundation Appropriate Use Criteria Task Force, Society for Cardiovascular Angiography and Interventions, Society of Thoracic Surgeons, American Association for Thoracic Surgery, American Heart Association, American Society of Nuclear Cardiology, and the Society of Cardiovascular Computed Tomography. J Am Coll Cardiol 2012;59:857– 81.
Measure 2: Assessment of Candidacy for Dual-Antiplatelet Therapy
Description Percentage of patients aged 18 years and older for whom PCI is performed
who have documentation in the medical record that an assessment of candidacy for initiation and duration of dual antiplatelet therapy was performed prior to the procedure.
Measure Type Process: pre procedure, safety
Numerator Patients who have documentation in the medical record that an assessment of candidacy* for initiation and duration of dual antiplatelet therapy (DAPT) was performed prior to the procedure. *Examples of assessment may include (but are not limited to) consideration of the following medical and personal issues, such as: • High risk of bleeding • Anticipated invasive or surgical procedures requiring early discontinuation of therapy • Accessibility of medications (eg, cost considerations) • Adherence with medications
Denominator All patients aged 18 years and older for whom PCI is performed
Denominator Exclusion
None
Denominator Exceptions
Documentation of medical reason(s) for not performing an assessment of candidacy for long-term dual antiplatelet therapy (eg, patient unresponsive,
emergency PCI with insufficient time prior to the procedure, other medical reasons)
Clinical Rationale/ Recommendations
The following evidence statements are quoted verbatim from the referenced clinical guidelines. Before implantation of DES, the interventional cardiologist should discuss with the patient the need for and duration of DAPT and the ability of the patient to comply with and tolerate DAPT. (Class I, Level of Evidence: C) (ACCF/AHA/SCAI, 2011) Patients should be counseled on the need for and risks of DAPT before placement of intracoronary stents, especially DES, and alternative therapies should be pursued if patients are unwilling or unable to comply with the recommended duration of DAPT. (Class I, Level of Evidence: C) (ACCF/AHA/SCAI, 2011) PCI with coronary stenting should not be performed if the patient is not likely to be able to tolerate and comply with DAPT.(Class III, Level of Evidence: B) (ACCF/AHA/SCAI, 2011) DES should not be implanted if the patient is not likely to be able to tolerate and comply with prolonged DAPT or this cannot be determined before stent implantation. (Class III, Level of Evidence: B) (ACCF/AHA/SCAI, 2011)
Relevant Citations Nallamothu BK, Tommaso CL, Anderson HV, Anderson JL, Cleveland JC, Dudley RA, Duffy PL, Faxon DP, Gurm HS, Hamilton LA, Jensen NC, Josephson RA, Malenka DJ, Maniu CV, McCabe KW, Mortimer JD, Patel MR, Persell SD, Rumsfeld JS, Shunk KA, Smith SC, Stanko SJ, Watts B. ACC/AHA/SCAI/AMA–Convened PCPI/NCQA 2013 performance measures for adults undergoing percutaneous coronary intervention: a report of the American College of Cardiology/American Heart Association Task Force on Performance Measures, the Society for Cardiovascular Angiography and Interventions, the American Medical Association–Convened Physician Consortium for Performance Improvement, and the National Committee for Quality Assurance. J Am Coll Cardiol 2014;63:722–45. Levine GN, Bates ER, Blankenship JC, et al. 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. J Am Coll Cardiol 2011; 58:e44–122.
Measure 3: Use of Embolic Protection Devices in the Treatment of Saphenous
Vein Bypass Graft Disease
Description Percentage of patients aged 18 years and older for whom saphenous vein
graft PCI is performed who received an embolic protection device during the procedure.
Measure Type Process: procedural (QI only)
Numerator Patients who received an embolic protection device during the procedure
Denominator All patients aged 18 years and older for whom saphenous vein graft PCI is performed
Denominator Exclusion
None
Denominator Exceptions
Documentation of medical reason(s) for not receiving an embolic protection device during the procedure (eg, anatomic considerations, other medical reasons).
Clinical Rationale/ Recommendations
The following evidence statements are quoted verbatim from the referenced clinical guidelines. Embolic protection devices (EPDs) should be used during saphenous vein graft (SVG) PCI when technically feasible. (Class I, Level of Evidence: B) (ACCF/AHA/SCAI, 2011)
Relevant Citations Nallamothu BK, Tommaso CL, Anderson HV, Anderson JL, Cleveland JC, Dudley RA, Duffy PL, Faxon DP, Gurm HS, Hamilton LA, Jensen NC, Josephson RA, Malenka DJ, Maniu CV, McCabe KW, Mortimer JD, Patel MR, Persell SD, Rumsfeld JS, Shunk KA, Smith SC, Stanko SJ, Watts B. ACC/AHA/SCAI/AMA–Convened PCPI/NCQA 2013 performance measures for adults undergoing percutaneous coronary intervention: a report of the American College of Cardiology/American Heart Association Task Force on Performance Measures, the Society for Cardiovascular Angiography and Interventions, the American Medical Association–Convened Physician Consortium for Performance Improvement, and the National Committee for Quality Assurance. J Am Coll Cardiol 2014;63:722–45. Levine GN, Bates ER, Blankenship JC, et al. 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. J Am Coll Cardiol 2011; 58:e44–122.
Measure 4: Documentation of Pre-procedural Glomerular Filtration Rate and
Contrast Dose Used During the Procedure
Description Percentage of patients aged 18 years and older for whom PCI is performed
who have both preprocedural estimated glomerular filtration rate (GFR) or an indication that the patient is on dialysis AND contrast dose administered documented in the catheterization report or procedure notes.
Measure Type Process: post procedure, safety (QI only)
Numerator Patients who have both pre-procedural estimated glomerular filtration rate (GFR) or an indication that the patient is on dialysis AND contrast dose administered* documented in the catheterization report or procedure notes. *Contrast dose administered should include the total dose used during both diagnostic and interventional procedures that occur during the same catheterization laboratory session.
Denominator All patients aged 18 years and older for whom PCI is performed
Denominator None
Exclusion Criteria
Denominator Exceptions
None
Clinical Rationale/ Recommendations
The following evidence statements are quoted verbatim from the referenced clinical guidelines. In patients undergoing PCI, the glomerular filtration rate should be estimated and the dosage of renally cleared medications should be adjusted. (Class I, Level of Evidence: B) (ACCF/AHA/SCAI, 2011) Calculation of the contrast volume to [creatinine clearance (CrCl)] ratio is useful to predict the maximum volume of contrast media that can be given without significantly increasing the risk of contrast-associated nephropathy. (Class I, Level of Evidence: B) (ACCF/AHA, 2011)
Relevant Citations Nallamothu BK, Tommaso CL, Anderson HV, Anderson JL, Cleveland JC, Dudley RA, Duffy PL, Faxon DP, Gurm HS, Hamilton LA, Jensen NC, Josephson RA, Malenka DJ, Maniu CV, McCabe KW, Mortimer JD, Patel MR, Persell SD, Rumsfeld JS, Shunk KA, Smith SC, Stanko SJ, Watts B. ACC/AHA/SCAI/AMA–Convened PCPI/NCQA 2013 performance measures for adults undergoing percutaneous coronary intervention: a report of the American College of Cardiology/American Heart Association Task Force on Performance Measures, the Society for Cardiovascular Angiography and Interventions, the American Medical Association–Convened Physician Consortium for Performance Improvement, and the National Committee for Quality Assurance. J Am Coll Cardiol 2014;63:722–45. Levine GN, Bates ER, Blankenship JC, et al. 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. J Am Coll Cardiol 2011; 58:e44–122. Wright RS, Anderson JL, Adams CD, Bridges CR, Casey DE Jr, Ettinger SM, Fesmire FM, Ganiats TG, Jneid H, Lincoff AM, Peterson ED, Philippides GJ, Theroux P, Wenger NK, Zidar JP. 2011 ACCF/AHA focused update of the guidelines for the management of patients with unstable angina/non–ST-elevation myocardial infarction (updating the2007 guideline): a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol 2011;57:1920–59.
Measure 5: Post procedural Optimal Medical Therapy Composite
New Measure (7) Post procedural Optimal Medical Therapy Composite
Description Percentage of patients aged 18 years and older for whom PCI is performed who are prescribed optimal medical therapy at discharge
Measure Type Process post procedural
Numerator Patients who are prescribed* all of the medications, for which they are eligible, at discharge.
*Prescribed may include prescription given to the patient for medications at discharge OR patient already taking medications as documented in current medication list.
Denominator All patients aged 18 years and older for whom PCI is performed who are eligible for any of the following medications (ie, patient has no contraindication, allergy, intolerance): • Aspirin • P2Y12 inhibitor (only for PCIs with stenting) • Statin
Denominator Exclusion
Patients who expired
Patients who left against medical advice
Patient discharged to hospice or for whom comfort care measures only is documented
Patient transferred to another acute care hospital
Clinical Rationale/ Recommendations
The following evidence statements are quoted verbatim from the referenced clinical guidelines. After PCI, use of aspirin should be continued indefinitely. (Class I, Level of Evidence: A)(ACCF/AHA/SCAI, 2011) The duration of P2Y12 inhibitor therapy after stent implantation should generally be as follows: a. In patients receiving a stent (BMS or DES) during PCI for ACS, P2Y12 inhibitor therapy should be given for at least 12 months. Options include clopidogrel 75 mg daily, prasugrel 10 mg daily, and ticagrelor 90 mg twice daily. (Class I, Level of Evidence: B) b. In patients receiving DES for a non-ACS indication, clopidogrel 75 mg daily should be given for at least 12 months if the patient is not at high risk of bleeding. (Class I, Level of Evidence: B) c. In patients receiving BMS for a non-ACS indication, clopidogrel should be given for a minimum of 1 month and ideally up to 12months (unless the patient is at increased risk of bleeding; then it should be given for a minimum of 2 weeks). (Class I, Level of Evidence: B) (ACCF/AHA/SCAI, 2011) A lipid profile in all patients [with coronary and other atherosclerotic vascular disease] should be established, and for hospitalized patients, lipid lowering therapy as recommended below should be initiated before discharge. (Class I, Level of Evidence: B) (AHA/ACCF, 2011) In addition to therapeutic lifestyle changes, statin therapy should be prescribed in the absence of contraindications or documented adverse effects. (Class I, Level of Evidence: A)(AHA/ACCF, 2011)
Relevant Citations Nallamothu BK, Tommaso CL, Anderson HV, Anderson JL, Cleveland JC, Dudley RA, Duffy PL, Faxon DP, Gurm HS, Hamilton LA, Jensen NC, Josephson RA, Malenka DJ, Maniu CV, McCabe KW, Mortimer JD, Patel MR, Persell SD, Rumsfeld JS, Shunk KA, Smith SC, Stanko SJ, Watts B. ACC/AHA/SCAI/AMA–Convened PCPI/NCQA 2013 performance measures for adults undergoing percutaneous coronary intervention: a report of the American College of Cardiology/American Heart Association
Task Force on Performance Measures, the Society for Cardiovascular Angiography and Interventions, the American Medical Association–Convened Physician Consortium for Performance Improvement, and the National Committee for Quality Assurance. J Am Coll Cardiol 2014;63:722–45. Smith SC Jr, Benjamin EJ, Bonow RO, et al. AHA/ACCF secondary prevention and risk reduction therapy for patients with coronary and other atherosclerotic vascular disease: 2011 update: a guideline from the American Heart Association and American College of Cardiology Foundation. Circulation. 2011;124:
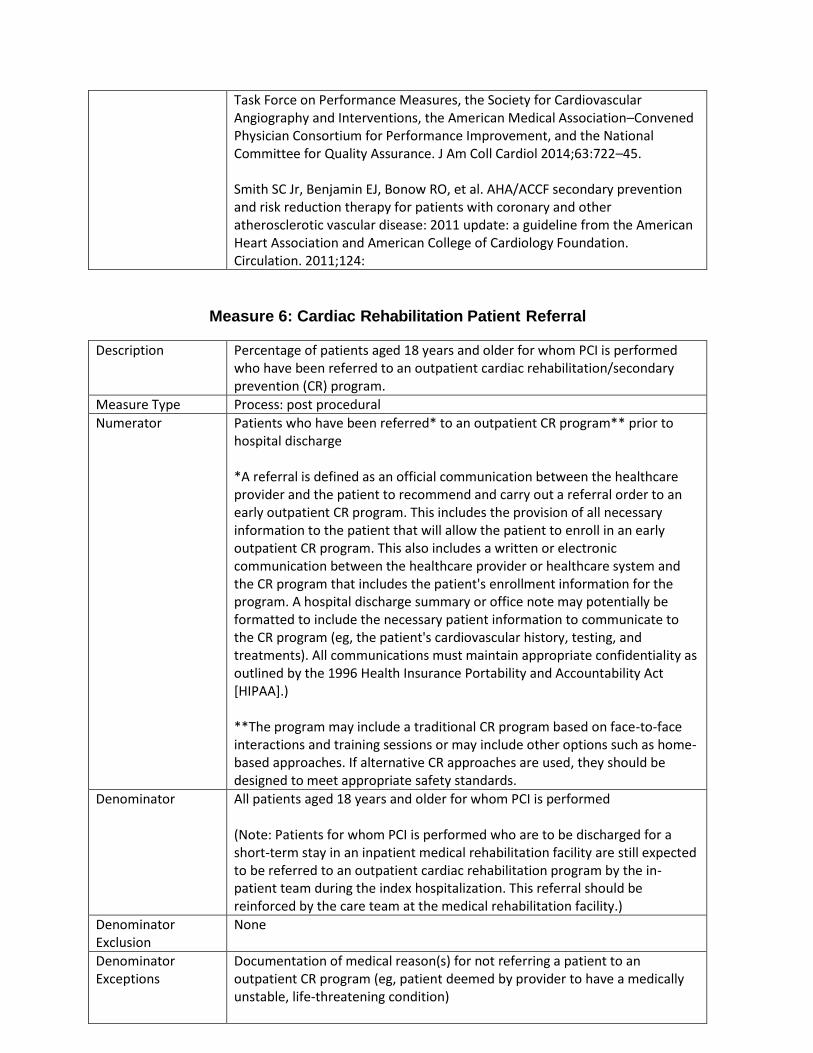
Measure 6: Cardiac Rehabilitation Patient Referral
Description Percentage of patients aged 18 years and older for whom PCI is performed who have been referred to an outpatient cardiac rehabilitation/secondary prevention (CR) program.
Measure Type Process: post procedural
Numerator Patients who have been referred* to an outpatient CR program** prior to hospital discharge *A referral is defined as an official communication between the healthcare provider and the patient to recommend and carry out a referral order to an early outpatient CR program. This includes the provision of all necessary information to the patient that will allow the patient to enroll in an early outpatient CR program. This also includes a written or electronic communication between the healthcare provider or healthcare system and the CR program that includes the patient's enrollment information for the program. A hospital discharge summary or office note may potentially be formatted to include the necessary patient information to communicate to the CR program (eg, the patient's cardiovascular history, testing, and treatments). All communications must maintain appropriate confidentiality as outlined by the 1996 Health Insurance Portability and Accountability Act [HIPAA].) **The program may include a traditional CR program based on face-to-face interactions and training sessions or may include other options such as home-based approaches. If alternative CR approaches are used, they should be designed to meet appropriate safety standards.
Denominator All patients aged 18 years and older for whom PCI is performed (Note: Patients for whom PCI is performed who are to be discharged for a short-term stay in an inpatient medical rehabilitation facility are still expected to be referred to an outpatient cardiac rehabilitation program by the in-patient team during the index hospitalization. This referral should be reinforced by the care team at the medical rehabilitation facility.)
Denominator Exclusion
None
Denominator Exceptions
Documentation of medical reason(s) for not referring a patient to an outpatient CR program (eg, patient deemed by provider to have a medically unstable, life-threatening condition)
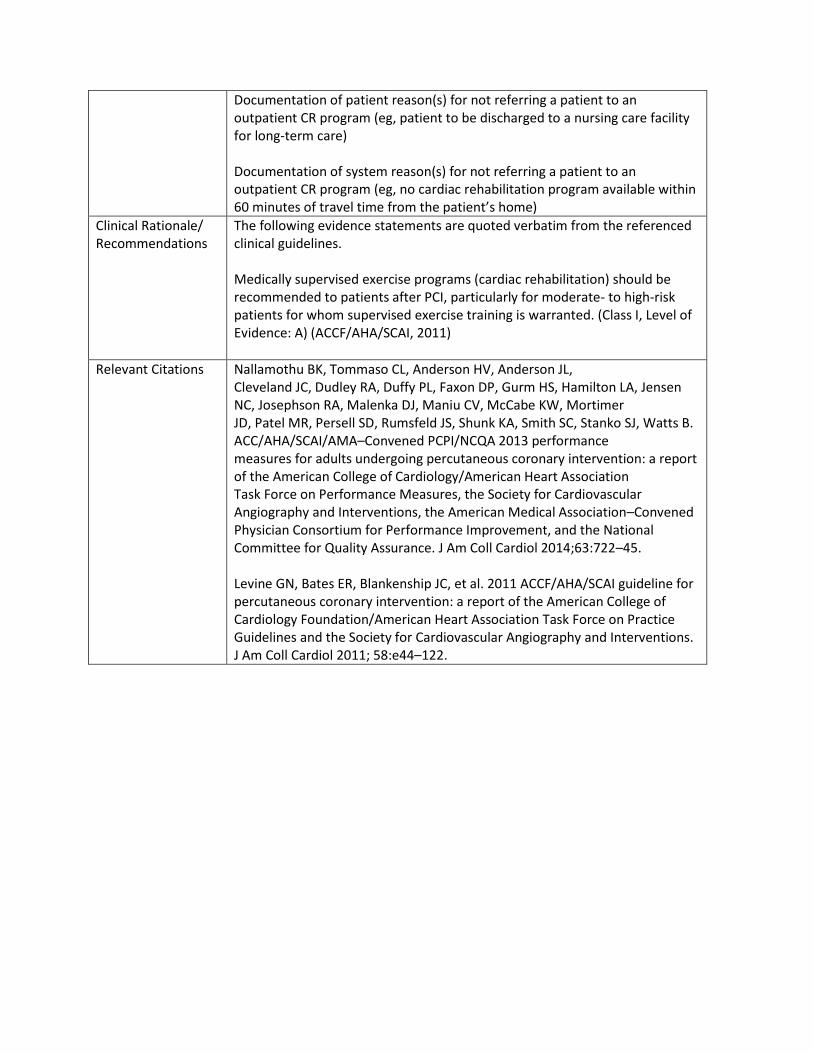
Documentation of patient reason(s) for not referring a patient to an outpatient CR program (eg, patient to be discharged to a nursing care facility for long-term care) Documentation of system reason(s) for not referring a patient to an outpatient CR program (eg, no cardiac rehabilitation program available within 60 minutes of travel time from the patient’s home)
Clinical Rationale/ Recommendations
The following evidence statements are quoted verbatim from the referenced clinical guidelines. Medically supervised exercise programs (cardiac rehabilitation) should be recommended to patients after PCI, particularly for moderate- to high-risk patients for whom supervised exercise training is warranted. (Class I, Level of Evidence: A) (ACCF/AHA/SCAI, 2011)
Relevant Citations Nallamothu BK, Tommaso CL, Anderson HV, Anderson JL, Cleveland JC, Dudley RA, Duffy PL, Faxon DP, Gurm HS, Hamilton LA, Jensen NC, Josephson RA, Malenka DJ, Maniu CV, McCabe KW, Mortimer JD, Patel MR, Persell SD, Rumsfeld JS, Shunk KA, Smith SC, Stanko SJ, Watts B. ACC/AHA/SCAI/AMA–Convened PCPI/NCQA 2013 performance measures for adults undergoing percutaneous coronary intervention: a report of the American College of Cardiology/American Heart Association Task Force on Performance Measures, the Society for Cardiovascular Angiography and Interventions, the American Medical Association–Convened Physician Consortium for Performance Improvement, and the National Committee for Quality Assurance. J Am Coll Cardiol 2014;63:722–45. Levine GN, Bates ER, Blankenship JC, et al. 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. J Am Coll Cardiol 2011; 58:e44–122.
18
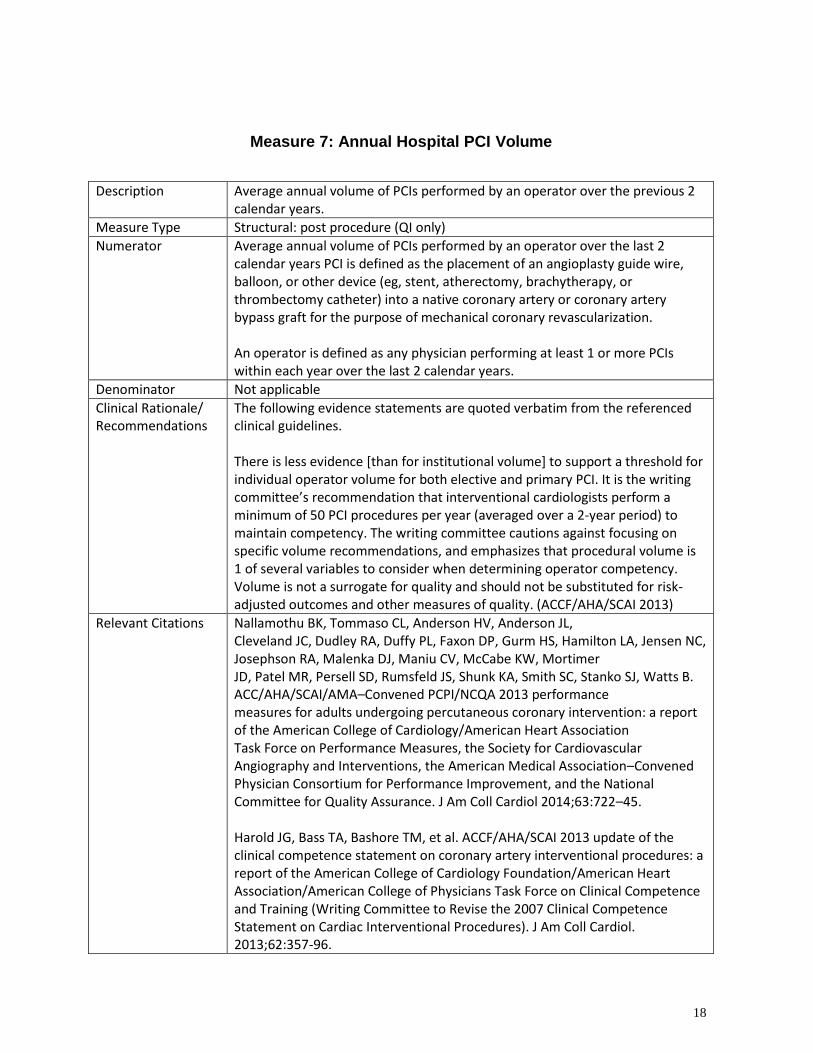
Measure 7: Annual Hospital PCI Volume
Description Average annual volume of PCIs performed by an operator over the previous 2 calendar years.
Measure Type Structural: post procedure (QI only)
Numerator Average annual volume of PCIs performed by an operator over the last 2 calendar years PCI is defined as the placement of an angioplasty guide wire, balloon, or other device (eg, stent, atherectomy, brachytherapy, or thrombectomy catheter) into a native coronary artery or coronary artery bypass graft for the purpose of mechanical coronary revascularization. An operator is defined as any physician performing at least 1 or more PCIs within each year over the last 2 calendar years.
Denominator Not applicable
Clinical Rationale/ Recommendations
The following evidence statements are quoted verbatim from the referenced clinical guidelines. There is less evidence [than for institutional volume] to support a threshold for individual operator volume for both elective and primary PCI. It is the writing committee’s recommendation that interventional cardiologists perform a minimum of 50 PCI procedures per year (averaged over a 2-year period) to maintain competency. The writing committee cautions against focusing on specific volume recommendations, and emphasizes that procedural volume is 1 of several variables to consider when determining operator competency. Volume is not a surrogate for quality and should not be substituted for risk-adjusted outcomes and other measures of quality. (ACCF/AHA/SCAI 2013)
Relevant Citations Nallamothu BK, Tommaso CL, Anderson HV, Anderson JL, Cleveland JC, Dudley RA, Duffy PL, Faxon DP, Gurm HS, Hamilton LA, Jensen NC, Josephson RA, Malenka DJ, Maniu CV, McCabe KW, Mortimer JD, Patel MR, Persell SD, Rumsfeld JS, Shunk KA, Smith SC, Stanko SJ, Watts B. ACC/AHA/SCAI/AMA–Convened PCPI/NCQA 2013 performance measures for adults undergoing percutaneous coronary intervention: a report of the American College of Cardiology/American Heart Association Task Force on Performance Measures, the Society for Cardiovascular Angiography and Interventions, the American Medical Association–Convened Physician Consortium for Performance Improvement, and the National Committee for Quality Assurance. J Am Coll Cardiol 2014;63:722–45. Harold JG, Bass TA, Bashore TM, et al. ACCF/AHA/SCAI 2013 update of the clinical competence statement on coronary artery interventional procedures: a report of the American College of Cardiology Foundation/American Heart Association/American College of Physicians Task Force on Clinical Competence and Training (Writing Committee to Revise the 2007 Clinical Competence Statement on Cardiac Interventional Procedures). J Am Coll Cardiol. 2013;62:357-96.

19
20
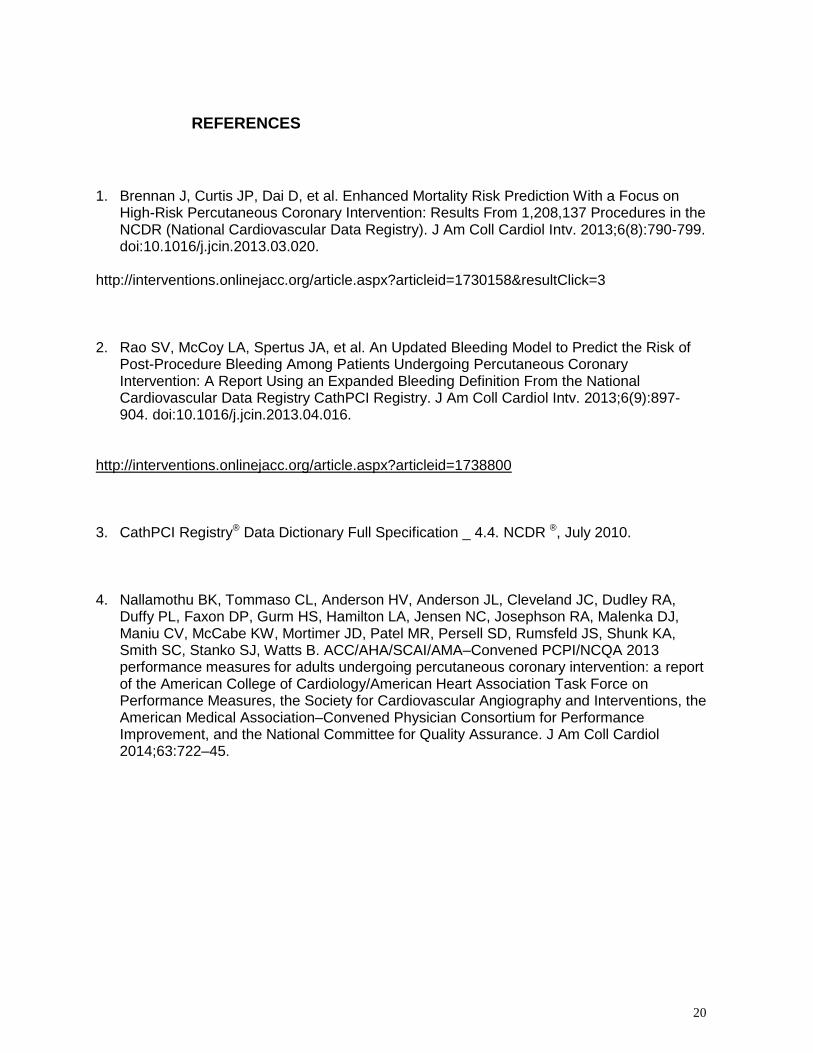
REFERENCES
1. Brennan J, Curtis JP, Dai D, et al. Enhanced Mortality Risk Prediction With a Focus on
High-Risk Percutaneous Coronary Intervention: Results From 1,208,137 Procedures in the NCDR (National Cardiovascular Data Registry). J Am Coll Cardiol Intv. 2013;6(8):790-799. doi:10.1016/j.jcin.2013.03.020.
http://interventions.onlinejacc.org/article.aspx?articleid=1730158&resultClick=3 2. Rao SV, McCoy LA, Spertus JA, et al. An Updated Bleeding Model to Predict the Risk of
Post-Procedure Bleeding Among Patients Undergoing Percutaneous Coronary Intervention: A Report Using an Expanded Bleeding Definition From the National Cardiovascular Data Registry CathPCI Registry. J Am Coll Cardiol Intv. 2013;6(9):897-904. doi:10.1016/j.jcin.2013.04.016.
http://interventions.onlinejacc.org/article.aspx?articleid=1738800 3. CathPCI Registry® Data Dictionary Full Specification _ 4.4. NCDR ®, July 2010. 4. Nallamothu BK, Tommaso CL, Anderson HV, Anderson JL, Cleveland JC, Dudley RA,
Duffy PL, Faxon DP, Gurm HS, Hamilton LA, Jensen NC, Josephson RA, Malenka DJ, Maniu CV, McCabe KW, Mortimer JD, Patel MR, Persell SD, Rumsfeld JS, Shunk KA, Smith SC, Stanko SJ, Watts B. ACC/AHA/SCAI/AMA–Convened PCPI/NCQA 2013 performance measures for adults undergoing percutaneous coronary intervention: a report of the American College of Cardiology/American Heart Association Task Force on Performance Measures, the Society for Cardiovascular Angiography and Interventions, the American Medical Association–Convened Physician Consortium for Performance Improvement, and the National Committee for Quality Assurance. J Am Coll Cardiol 2014;63:722–45.