Embed Size (px)
Citation preview

RISK MANAGEMENTRISK MANAGEMENTIN THEIN THE
CORRECTIONAL SETTINGCORRECTIONAL SETTING
Jacqueline MooreJacqueline MoorePresident Moore and AssociatesPresident Moore and Associates
February 2006February 2006

What is Risk Management?What is Risk Management?
Risk management is the process of using Risk management is the process of using policies, procedures, protocols and policies, procedures, protocols and
systems to reduce the likelihood of errors systems to reduce the likelihood of errors and/or adverse outcomesand/or adverse outcomes

Where might you see risk Where might you see risk management being used?management being used?

• Nuclear Power IndustryNuclear Power Industry
• Most types of manufacturingMost types of manufacturing
• Automobile designAutomobile design
• SurgerySurgery
• HospitalsHospitals

Egg
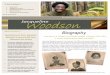
RISK MANGAMENT DIAGRAM
Egg

ARREST DIVERT

ARREST DIVERT
CUSTODY INTAKE SCREEN

ARREST DIVERT
CUSTODY INTAKE SCREEN
NURSING INTAKE SCREEN

ARREST DIVERT
CUSTODY INTAKE SCREEN
NURSING INTAKE SCREEN
MEDICAL INTAKE SCREEN

ARREST DIVERT
CUSTODY INTAKE SCREEN
NURSING INTAKE SCREEN
MEDICAL INTAKE SCREEN
SICK CALL REQUEST SYSTEM

ARREST DIVERT
CUSTODY INTAKE SCREEN
NURSING INTAKE SCREEN
MEDICAL INTAKE SCREEN
SICK CALL REQUEST SYSTEM
HOUSING SYSTEM

ARREST DIVERT
CUSTODY INTAKE SCREEN
NURSING INTAKE SCREEN
MEDICAL INTAKE SCREEN
SICK CALL REQUEST SYSTEM
HOUSING SYSTEM
CUSTODY OBSERVATION

ARREST DIVERT
CUSTODY INTAKE SCREEN
NURSING INTAKE SCREEN
MEDICAL INTAKE SCREEN
SICK CALL REQUEST SYSTEM
HOUSING SYSTEM
CUSTODY OBSERVATION
CUSTODY AND HC COMMUNICATION

ARREST DIVERT
CUSTODY INTAKE SCREEN
NURSING INTAKE SCREEN
MEDICAL INTAKE SCREEN
SICK CALL REQUEST SYSTEM
HOUSING SYSTEM
CUSTODY OBSERVATION
CUSTODY AND HC COMMUNICATION

Scenario OneScenario OneBackgroundBackground
• 18 year old male who has been 18 year old male who has been incarcerated for one month. Jail has 40 incarcerated for one month. Jail has 40 hour per week nursing and on call care hour per week nursing and on call care after hours. after hours.
• No medical problems noted at intakeNo medical problems noted at intake
• One month later he complains of One month later he complains of abdominal pain. States he has a history abdominal pain. States he has a history of umbilical hernia.of umbilical hernia.
• Nurse exam shows no sign of umbilical Nurse exam shows no sign of umbilical hernia.hernia.
• What do you do next?What do you do next?

Physical ExamPhysical Exam
• PE revealed no protrusions re umbilical PE revealed no protrusions re umbilical areaarea
• Abdomen non-tenderAbdomen non-tender• Bowel movements normalBowel movements normal• Vital signs T 97.6, P96 skin warm and Vital signs T 97.6, P96 skin warm and
drydry• Inmate unable to say where he had Inmate unable to say where he had
previously sought treatmentpreviously sought treatment• Inmate given Motrin Inmate given Motrin

• Inmate back to clinic with complaints Inmate back to clinic with complaints of abdominal pain and vomitingof abdominal pain and vomiting
• There is no exam table in treatment There is no exam table in treatment room, patient requested to lie on room, patient requested to lie on floorfloor
• Palpation indicated negative Palpation indicated negative McBurneys SignMcBurneys Sign
Next DayNext Day

Four days laterFour days later
• Contacts nurse again in 4 days. Says Contacts nurse again in 4 days. Says pain is worse.pain is worse.
• Mother contacts facility stating her Mother contacts facility stating her son is in severe pain.son is in severe pain.
• Nurse examines patient. No Nurse examines patient. No evidence of umbilical hernia.evidence of umbilical hernia.
• What do you do next?What do you do next?

Day 5Day 5
• Patient complains of vomiting on day Patient complains of vomiting on day 5. Nurse examines patient. 5. Nurse examines patient. Documents no signs of umbilical Documents no signs of umbilical hernia. Calls MD and gets order for hernia. Calls MD and gets order for phenergan which patient vomits up phenergan which patient vomits up within 30 minutes.within 30 minutes.
• What do you do next?What do you do next?

Day 6Day 6
• Nurse visit. Patient still complaining of Nurse visit. Patient still complaining of abdominal pain and sick to stomach. abdominal pain and sick to stomach. Nurse documents bowel sounds in all Nurse documents bowel sounds in all 4 quadrants.4 quadrants.
• No rebound tenderness. No rebound tenderness.
• No signs of umbilical hernia.No signs of umbilical hernia.
• What do you do next?What do you do next?

Day 7Day 7
• Custody staff report “spitting up Custody staff report “spitting up brown stuff in cup”. Told by health brown stuff in cup”. Told by health care staff he's been checked and is care staff he's been checked and is OK.OK.

Day 8Day 8
• Patient states “unable to pee”. UA Patient states “unable to pee”. UA shows ketones and slight WBC's.shows ketones and slight WBC's.
• Physician called, orders CBC and blood Physician called, orders CBC and blood sugar stat.sugar stat.
• WBC normal except slight left shift. WBC normal except slight left shift. Glucose normal.Glucose normal.
• Nurse reports to MD white blood count Nurse reports to MD white blood count normal but does not fax results.normal but does not fax results.
• VS T 97.4, P 100, BP 116/66 R18.VS T 97.4, P 100, BP 116/66 R18.• What do you do next?What do you do next?

• Guards call nursing staff in the Guards call nursing staff in the evening because patient still evening because patient still continues to complain of abdominal continues to complain of abdominal pain. Told that everything is all right.pain. Told that everything is all right.
• Nurse reports to officer that blood Nurse reports to officer that blood work is normal.work is normal.
• What do you do next?What do you do next?

Day 9Day 9• Officers do not check on inmate through Officers do not check on inmate through
the night.the night.• Custody calls nurse to find out when he's Custody calls nurse to find out when he's
coming in? (Sat.) Tells nurse he needs to coming in? (Sat.) Tells nurse he needs to see patient that day.see patient that day.
• Officer reports that inmate has vomited Officer reports that inmate has vomited coffee ground material.coffee ground material.
• Nurse reports at noon. Patient collapses Nurse reports at noon. Patient collapses and dies. Noted to be “cold” by EMT's. and dies. Noted to be “cold” by EMT's. Bloody vomit all over cell.Bloody vomit all over cell.
• What is the Diagnosis?What is the Diagnosis?• Where would risk management have Where would risk management have
helped in this case?helped in this case?

Where is the Liability Where is the Liability and with Whom? and with Whom?

Inconsistency in CareInconsistency in Care
• EMS reports patient was expired on EMS reports patient was expired on arrivalarrival
• Nurse reports P 70 R12Nurse reports P 70 R12• MD indicates she never saw copy of lab MD indicates she never saw copy of lab
workwork• Nurse types nurse’s notes from home Nurse types nurse’s notes from home
and adds them to the chart as late entryand adds them to the chart as late entry• Officers never started CPROfficers never started CPR• Nursing Protocol not followedNursing Protocol not followed

ConclusionsConclusions
• Cause of Death Cause of Death – Ruptured appendix with peritonitisRuptured appendix with peritonitis
• Deliberate indifference case filed Deliberate indifference case filed – Providers careless and reckless and failed Providers careless and reckless and failed
to comply with applicable standards of careto comply with applicable standards of care
• Case settled September 2005Case settled September 2005

Scenario 2Scenario 2BackgroundBackground
• 17 year old white male adjudicated to 17 year old white male adjudicated to juvenile academy on 12/28/98. Program juvenile academy on 12/28/98. Program has strong emphasis on sports.has strong emphasis on sports.
• April 5, 1999 following Easter Break youth April 5, 1999 following Easter Break youth returns to juvenile academy and is ill has returns to juvenile academy and is ill has symptoms of cough, chill, nasal stuffiness, symptoms of cough, chill, nasal stuffiness, diarrhea, upset stomachdiarrhea, upset stomach
• Mother calls school to inform them of Mother calls school to inform them of son’s illnessson’s illness
• What would you do? What would you do?

Juvenile AcademyJuvenile Academy
• Youth placed in infirmaryYouth placed in infirmary
• Treated by EMT with over the counter Treated by EMT with over the counter medicinemedicine
• 4/7/99 Temperature reading is 104.3 4/7/99 Temperature reading is 104.3 at 6:40 AMat 6:40 AM
• EMT puts cool compresses on youth’s EMT puts cool compresses on youth’s forehead and provides OTC medicineforehead and provides OTC medicine

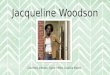
Temperature ChartTemperature Chart4/7-4/8/994/7-4/8/99
104.3
99.4 99.1 99.1 99100
96.2
92
94
96
98
100
102
104
106
6:40AM
8:00 10:50AM
14:00 15:00 8:00 16:45

4/8/994/8/99
• Youth seen by school physicianYouth seen by school physician• Temperature100 degrees F at 8 AMTemperature100 degrees F at 8 AM• At 4:45 PM temperature 96.2 degrees At 4:45 PM temperature 96.2 degrees
FF• Youth is disoriented, unable to provide Youth is disoriented, unable to provide
MD with history of why he was present MD with history of why he was present at sick callat sick call
• MD orders patient to go to ER for MD orders patient to go to ER for evaluationevaluation

ER FiascoER Fiasco• EMT notifies youths parents that EMT notifies youths parents that
youth is to go to the ERyouth is to go to the ER• EMT advised supervisor that youth EMT advised supervisor that youth
is to be transported to ERis to be transported to ER• Youth refuses to go to ER states he Youth refuses to go to ER states he
feels better. Temperature 97.4feels better. Temperature 97.4• Parents notified that youth does Parents notified that youth does
not want to go to the ERnot want to go to the ER• Youth placed in infirmary. EMT Youth placed in infirmary. EMT
tells officer to watch youthtells officer to watch youth

Next MorningNext MorningApril 9, 1999April 9, 1999
• Youth disorientedYouth disoriented• Officer moved youth out of infirmaryOfficer moved youth out of infirmary• Youth fell to floor when getting out of bedYouth fell to floor when getting out of bed• No vital signs were taken during the nightNo vital signs were taken during the night• Youth urinated and defecated on himselfYouth urinated and defecated on himself• EMS calledEMS called• Transferred to tertiary hospital craniotomy Transferred to tertiary hospital craniotomy
performedperformed• Today patient suffers from speech and brain Today patient suffers from speech and brain
damagedamage

What Went WrongWhat Went Wrong

What were the ProblemsWhat were the Problemswith this care? with this care?
• Lack of Adequate AssessmentLack of Adequate Assessment– No notations of nuchal rigidityNo notations of nuchal rigidity– Incomplete vital signs no pulse or BP Incomplete vital signs no pulse or BP
(slowing of pulse indicative of increased (slowing of pulse indicative of increased intracranial pressureintracranial pressure
– No notations made re headaches, No notations made re headaches, photophobia, irritability, malaise, photophobia, irritability, malaise, change in LOC, chills or sudden changes change in LOC, chills or sudden changes in body temperaturein body temperature

Poor Monitoring of Poor Monitoring of TemperatureTemperature• Temperature readings over 102 Temperature readings over 102
degreesdegrees
• No attempt to contact physician No attempt to contact physician when temperature reached 104 when temperature reached 104 degreesdegrees
• Intermittent fever diurnal variations Intermittent fever diurnal variations frequently seen in pyrogenic frequently seen in pyrogenic infectionsinfections

Inadequate ChartingInadequate Charting
• OTC medication given but we do not OTC medication given but we do not know drug, strength, frequency or how it know drug, strength, frequency or how it affected temperatureaffected temperature
• Facility was unable to find medication logFacility was unable to find medication log
• Physician did not have access to medical Physician did not have access to medical record when he examined the patientrecord when he examined the patient

Inadequate Staffing and Inadequate Staffing and TrainingTraining
• Only two EMTs assigned to medical Only two EMTs assigned to medical unitunit
• No training in chronic or infectious No training in chronic or infectious diseasesdiseases
• No nursing oversightNo nursing oversight• EMTS frequently pulled to perform EMTS frequently pulled to perform
other assignments e.g. transport, other assignments e.g. transport, assistance on field with sports etc. assistance on field with sports etc.
• No medical staff on the night shiftNo medical staff on the night shift

Failure to follow ordersFailure to follow orders
• MD assessed patient incapable of MD assessed patient incapable of answering questionsanswering questions
• Youth had altered medical status, with Youth had altered medical status, with high fever, and upper respiratory infectionhigh fever, and upper respiratory infection
• Supervisors of Academy made aware of Supervisors of Academy made aware of transport ordertransport order
• No communication to MD that indicates No communication to MD that indicates youth not sent to ERyouth not sent to ER
• Customary practice of academy to cancel Customary practice of academy to cancel off-site appointmentsoff-site appointments

Lack of AutonomyLack of Autonomy
• Patient moved out of infirmary Patient moved out of infirmary without notification of medical staffwithout notification of medical staff
• No procedures in place of admission No procedures in place of admission or discharge of youth to infirmaryor discharge of youth to infirmary
• Patient not monitored by night shiftPatient not monitored by night shift
• Supervisors are in charge of medical Supervisors are in charge of medical unitunit

Failure to CommunicateFailure to Communicate
• Officer indicates EMT did not tell him Officer indicates EMT did not tell him to monitor patientto monitor patient
• EMT indicates he told officer to EMT indicates he told officer to monitor patientmonitor patient
• Nothing recordedNothing recorded• No clear policy on communication No clear policy on communication
between clinician and facility between clinician and facility administration re medical needs of administration re medical needs of youthyouth

ConsentConsent
• EMT unaware of State Statute re EMT unaware of State Statute re informed consentinformed consent
• Supervisor did not clarify State Supervisor did not clarify State Statute on consent for medical staffStatute on consent for medical staff
• What else could have been done? What else could have been done?
• Could parents have gone to the ER?Could parents have gone to the ER?

Arrest DIVERT
INTAKE SCREEN
NURSING SCREEN
MEDICAL SCREEN
MEDICATION SYSTEM
Egg
SICK CALL REQUEST
HOUSING
OFFICER OBSERVATION
CUSTODY/HC COMMUNICATION
RISK MANGAMENT DIAGRAM

Scenario 3Scenario 3
• Native American died of seizures in Native American died of seizures in transport van.transport van.
• He was in leg irons and belly chains He was in leg irons and belly chains when he arrived at the jail.when he arrived at the jail.

BackgroundBackground
• Patient had been in jail several times Patient had been in jail several times previouslypreviously
• Known alcoholicKnown alcoholic
• Previous charges were domestic violencePrevious charges were domestic violence
• Current charge manslaughterCurrent charge manslaughter
• Had prior medical records indicating seizureHad prior medical records indicating seizure
• Had been brought to a mental health Had been brought to a mental health facility soon after arrest for a competency facility soon after arrest for a competency hearinghearing

On the road to MeccaOn the road to Mecca
• Patient started breathing funny and shaking Patient started breathing funny and shaking violentlyviolently
• Transport officers were present in major cityTransport officers were present in major city
• Hospital was two blocks awayHospital was two blocks away
• Jail was two hours awayJail was two hours away
• Officers called LPN who worked at small jailOfficers called LPN who worked at small jail
• What did she say to do?What did she say to do?

Prior Medical HistoryPrior Medical History
• Inmate was known to nurse, she indicated Inmate was known to nurse, she indicated to officer that he had had seizures to officer that he had had seizures previouslypreviously
• Nurse advised officer to keep patient in Nurse advised officer to keep patient in upright position and if more than 3 upright position and if more than 3 seizures occurred in 20 minutes to seek seizures occurred in 20 minutes to seek medical assistancemedical assistance
• Officer noted bubbly breath of inmate.Officer noted bubbly breath of inmate.
• What should officers do? What should officers do?

Continuing SegaContinuing Sega
• Officer called other transport officer Officer called other transport officer who was in the Federal Marshals who was in the Federal Marshals BuildingBuilding
• Inmate continued to have seizures-Inmate continued to have seizures-his arms and legs became tense, his arms and legs became tense, patient was described as patient was described as unresponsiveunresponsive
• What should the deputy do? What should the deputy do?

What did the Deputy Do?What did the Deputy Do?
• He called the nurse a second timeHe called the nurse a second time
• He called the other transport officer He called the other transport officer urging him to hurryurging him to hurry
• Nurse called ER doctor indicating Nurse called ER doctor indicating patient was having petit mal seizurespatient was having petit mal seizures
• What is your assessment now?What is your assessment now?

Sega ContinuesSega Continues
• Officer calls nurse third time and Officer calls nurse third time and asked if they should go to the asked if they should go to the hospitalhospital
• Nurse assured Deputy that the Nurse assured Deputy that the inmate would be fine just monitor his inmate would be fine just monitor his breathingbreathing
• Patient has another seizurePatient has another seizure
• What should they do now?What should they do now?

Road trip ObservationsRoad trip Observations• Deputy calls nurse fourth time patient now Deputy calls nurse fourth time patient now
foaming at the mouthfoaming at the mouth• Nurse indicates this was normal behavior for a Nurse indicates this was normal behavior for a
seizure patientseizure patient• Deputies drive on- --patient continues to have Deputies drive on- --patient continues to have
small seizuressmall seizures• Patient falls from his seat and wedges himself Patient falls from his seat and wedges himself
between seats of vanbetween seats of van• Patient is no longer breathingPatient is no longer breathing• Deputies indicate they can’t dislodge patient from Deputies indicate they can’t dislodge patient from
the seatthe seat• What should deputies do now?What should deputies do now?

End of the roadEnd of the road
• Officers continue at great speed Officers continue at great speed along the highwayalong the highway
• Jail lieutenant driving at great speed Jail lieutenant driving at great speed along the road to meet transport vanalong the road to meet transport van
• EMS notifiedEMS notified• All converge within 5 minute spanAll converge within 5 minute span• EMTs unable to locate a pulseEMTs unable to locate a pulse• Patient transported back to jailPatient transported back to jail

Your opinionsYour opinions
• Personnel not qualified to make decisionsPersonnel not qualified to make decisions– LPN LPN – Nurse had only one day of ER training in course Nurse had only one day of ER training in course
workwork– Did not know how to access seizureDid not know how to access seizure– Did not ask for sufficient informationDid not ask for sufficient information– Misdiagnosed seizure as petit malMisdiagnosed seizure as petit mal– Patient had grand mal seizures in jail previouslyPatient had grand mal seizures in jail previously– Did not know the purpose of medication she Did not know the purpose of medication she
gave patientgave patient

Lack of Appropriate intake Lack of Appropriate intake procedures at jailprocedures at jail
• Patient arrested ten times in five year spanPatient arrested ten times in five year span
• Inconsistency in intake records re alcohol Inconsistency in intake records re alcohol abuse even though patient heavy abuse even though patient heavy substance abusersubstance abuser
• Sometimes patient too drunk to sign intake Sometimes patient too drunk to sign intake formsforms
• No indication on medical history that No indication on medical history that patient had seizure disorder even though patient had seizure disorder even though he was on Neurontinhe was on Neurontin

Withdrawal AssessmentWithdrawal Assessment• What should you look for ?What should you look for ?
• When should it occur?When should it occur?
• Patient had auditory hallucinationsPatient had auditory hallucinations
• At mental health facility patient At mental health facility patient described as disoriented, cloud of described as disoriented, cloud of sensoriumsensorium
• Seizure activity what is the causeSeizure activity what is the cause– Epilepsy, DT, was patient mentally retarded Epilepsy, DT, was patient mentally retarded

Response to Emergency Response to Emergency SeizureSeizure• Training of OfficersTraining of Officers
• Response of NurseResponse of Nurse– Pertinent history Pertinent history – Questions relevant to seizuresQuestions relevant to seizures– Decision-making SkillsDecision-making Skills
•Call to ER vs on-site physician Call to ER vs on-site physician

Lack of ER equipment and Lack of ER equipment and proceduresprocedures
• No emergency equipment in vanNo emergency equipment in van
• Offender had AIDSOffender had AIDS

Inconsistency with MD Inconsistency with MD ResponseResponse
• Nurse relied on ER physicianNurse relied on ER physician
• Physician did not do adequate Physician did not do adequate assessmentassessment
• MD believed patient dying of AIDSMD believed patient dying of AIDS
• Prior bad experiences with patient at Prior bad experiences with patient at hospitalhospital

Lack of Continuity of CareLack of Continuity of Care
• No Prior medical recordsNo Prior medical records
• Transfer form incompleteTransfer form incomplete
• Outpatient records from AIDS Outpatient records from AIDS treatment not availabletreatment not available
• Not seen by psychiatrist or physician Not seen by psychiatrist or physician while at jailwhile at jail

Arrest DIVERT
INTAKE SCREEN
NURSING SCREEN
MEDICAL SCREEN
MEDICATION SYSTEM
Egg
SICK CALL REQUEST
HOUSING
OFFICER OBSERVATION
CUSTODY/HC COMMUNICATION
RISK MANGAMENT DIAGRAM

SummarySummary• Risk management when properly applied Risk management when properly applied
can be a powerful tool in preventing can be a powerful tool in preventing adverse outcomes.adverse outcomes.
• To work appropriately, you not only have to To work appropriately, you not only have to have the steps for risk management in have the steps for risk management in place, you need to be sure they are being place, you need to be sure they are being used.used.
• For risk management to work, providers For risk management to work, providers need to be educated about each step need to be educated about each step including it’s rationale. including it’s rationale.
• To practice Good Risk Management is also To practice Good Risk Management is also to practice GOOD HEALTH CARE.to practice GOOD HEALTH CARE.