Embed Size (px)
Citation preview

Risk Management and Safety in Health Care Organizations
Fadi El-Jardali, MPH, PhDOctober 2016
Day 1
1
Objectives � to increase the knowledge to effectively implement risk
management and safety approaches and tools
� to prepare participants to develop risk management and safety plan for your organizations.
� provide participants with hands on experience and practical knowledge on risk management and safety in hospitals
2

Learning outcomes � Understand the system approach related Risk
Management and Safety in health organizations� develop the knowledge regarding different type of risks
in the health care organizations� Understand and apply the risk management steps
including identifying, analyzing, evaluating, treating, monitoring and communicating risk
� Conduct risk assessment using the Severity Assessment Code (SAC) score
3
Learning Outcomes (Cont’d)� Apply skills to implement common tools for identifying and addressing
the root causes of critical incidences in organizations� Failure mode and effects analysis (FMEA)
� Apply incident reporting and investigation by using the incident reporting system
� Develop skills to fill incident report� Develop corrective action plan based on risk quantification results � Apply skills on ‘HOW’ to effectively develop, implement a risk
management and safety plan � Devise strategies to implementing the plan� Identify indicators for risk management and safety plans to measure
successes4

When you usually get to the end of the day, you always find two things…
1. You didn’t accomplish everything you imagined you would.
2. Your day wasn’t anything like how you’d imagined.
This distinction between Work as Imagined (WAI) and Work As
Done (WAD) is … everywhere
Thanks to Drs. Jeffrey Braithwaite and David Marx
What they do seems perfectly logical, obvious and feasible.
In health care, those doing WAI have designed, mandated or encouraged a bewildering range of tools, techniques and methods, to reduce harm to patients.
E.g., root cause analysis, hand hygiene campaigns, failure modes effects analysis ...
And there’s lots of others
…

But the rate of harm has flatlined at 10%
Meanwhile work is getting done, often despite all the policies, rules and mandates

WAD—workarounds
WAD—fragmentationDoctors in Emergency Departments in a study:�Were interrupted 6.6 times per hour.�Were interrupted in 11% of all tasks.�Multitasked for 12.8% of the time.

Doctors in Emergency Departments in a study:§ Spent on average 1:26 minutes on any one
task.§ When interrupted, spent more time on
tasks.§ And … failed to return to approximately
18.5% of interrupted tasks.
So work-as-imagined often have some sort of linear, mechanistic view of the system.
Instead, health care is a complex adaptive system delivered by people on the front line who flex and adjust to the
circumstances.
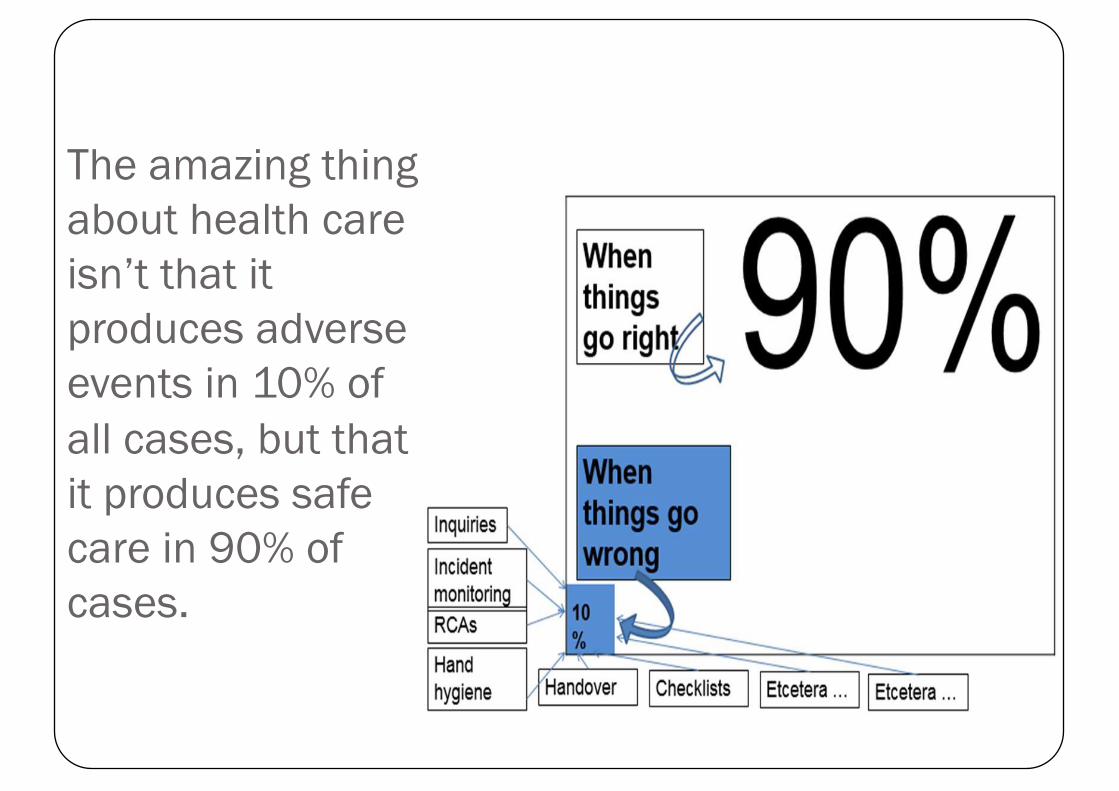
The amazing thing about health care isn’t that it produces adverse events in 10% of all cases, but that it produces safe care in 90% of cases.

Few people have ever looked at why things go right so often
What none of them know is that there are 600+ policies in operation right now, meant to “guide” their work.
Then when we observe their behaviours and see them taking patients’ histories, or giving out medications, or doing procedures, or taking x-rays of patients, or tending to their needs, or caring for them …
We can notice instead a lot of fraught, time-pressed, relentlessly busy work going on virtually across the entire shift.

Sometimes it never, ever unfolds like a policy or procedure says it should.
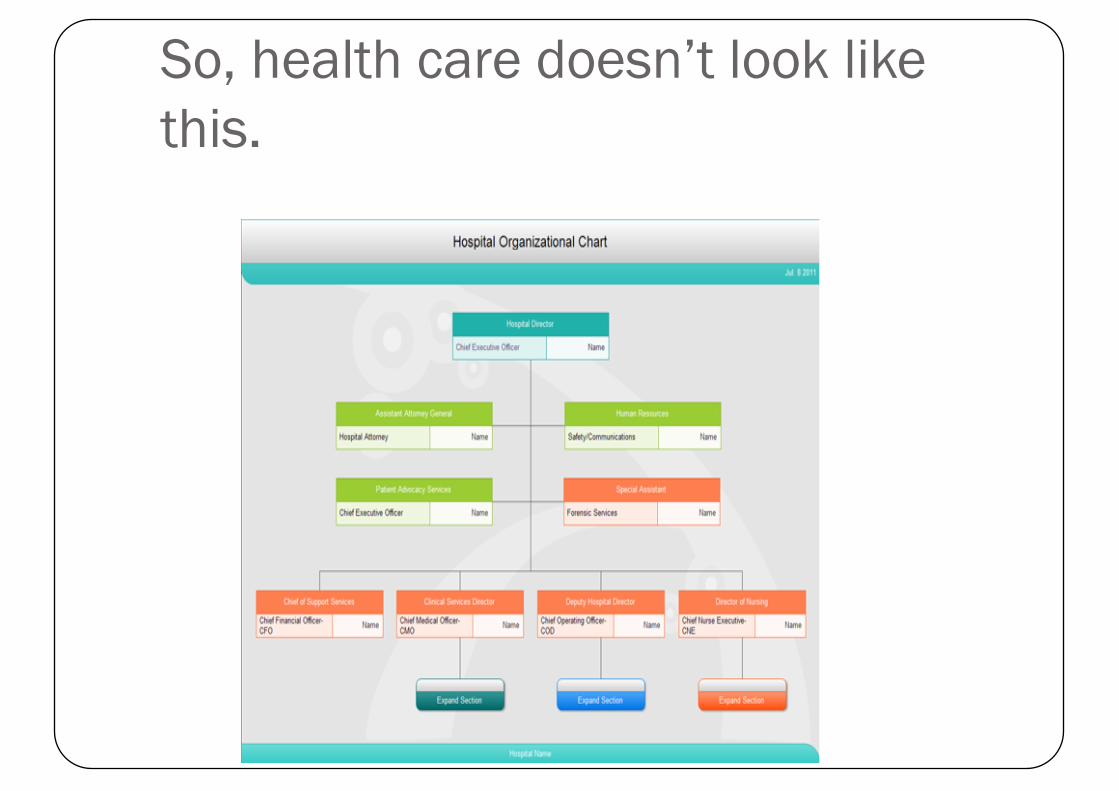
So, health care doesn’t look like this.
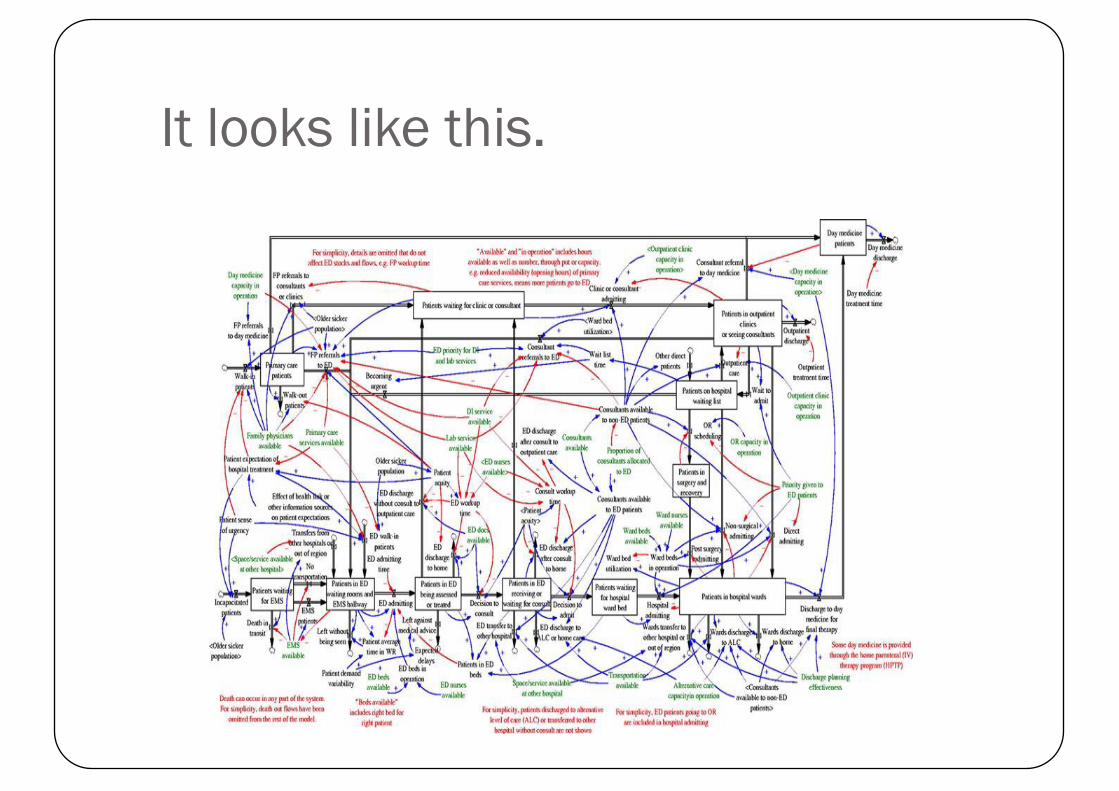
It looks like this.
And therefore the only real solution is to try and reconcile work-as-imagined and work-as-done.
A health system where the work-as-imagined policies, regulations, standards etc are much closer to an understanding of how work is actually done.

SUBWAY SAFETY – NEW YORK CITY
THE PROBLEM, AND THE SOLUTION

WHAT ABOUT BETTER SYSTEM DESIGN?

YET, IT’S NOT ONLY ABOUT SYSTEM DESIGN

Architecture examples
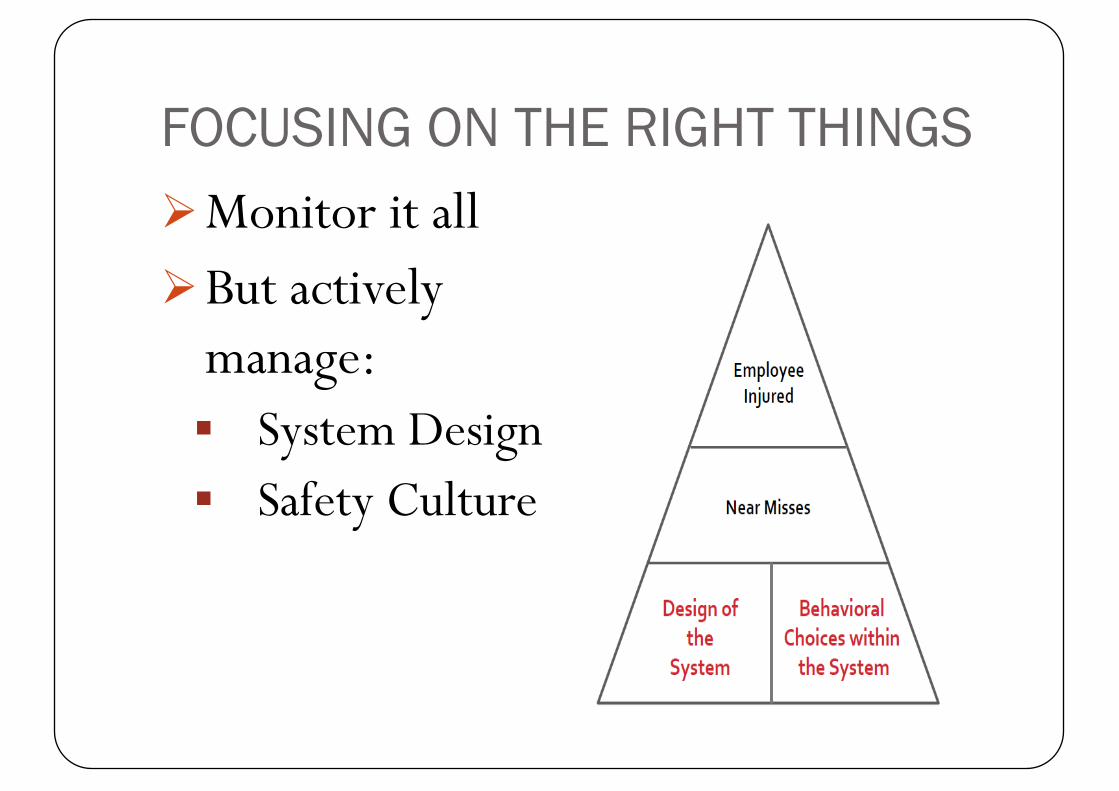
FOCUSING ON THE RIGHT THINGSØMonitor it allØBut actively
manage:§ System Design§ Safety Culture
SAFETY � How do we prevent
backing over a child?
Solutions
� TECHNOLOGICAL SYSTEMS
� •Backup camera� •Backup sensor with
automatic breaking� •Backup horn
� PROCEDURAL SYSTEMS� •Walk around back of car
before getting in� •Use a spotter
Yet, the most simple of steps, the walk around, most drivers do not do
Is that our “culture?”

An Organization’s Goal Should Be� To prevent or minimize risk of harm to patients, staff,
visitors, and volunteers, thereby reducing or eliminating any potential losses including financial ones
� Risk Management is about harm reduction which could be achieved by risk identification, risk assessment, risk control and evaluation
35

Risk Management in Healthcare Institutions
� Risk management in the healthcare industry is increasingly becoming an important area of concern for hospital governing boards, administrators, medical practitioners, insurers, consumer organizations and other key stakeholders.
� “Hospitals, medical institutions and medical professionals must take pro active actions to ensure the minimization and elimination of medical errors”
� Risk management in health care emerged as a result of the malpractice crisis of the 1970s.
36
Risk Management in Healthcare Institutions
� Objectives of include:� The delivery of safe and quality healthcare to patients� Ensuring safety among patients, staff and visitors� Identifying and controlling hazards and injuries� Protection of assets and other resources
37
Risk Management is a Proactive Strategy
Its components include:�Risk identification�Risk assessment�Risk control�Evaluation of risk management activities
38

Evaluation of Risk Management Activities� Organizations should regularly ask itself: How effective
is our risk management system?� Organization’s risk management practices need to be
evaluated. This includes:� Reviewing the frequency and severity of losses� Analyzing incident and occurrence trends� Reviewing policies and procedures that might prevent
or minimize risk� Assessing new or increased risk� Assessing the effectiveness of risk management
education and communication strategies
39
“We cannot change the human condition, but we can change the conditions under which humans work.” (Reason 2000)
40
41
Identify patient safety issues in your organization
Exercise
42
From a Traditional View to a System Approach
� Person approach to patient safety (practitioner as potential culprit to be blamed)
� System approach to patient safety
43
Some Reasons Why Errors Occur
� Complexity of health care processes
� Complexity of health care work environments
� Lack of consistent administration practices
� Deferred maintenance
� Clumsy technology
� Limited knowledge
� Poor application of knowledge
� Fatigue
� Sub-optimal teamwork
� Attention distraction
� Inadequate training
� Reliance on memory
� Poor handwriting
System Factors Human Factors

44
Multi-Causal Theory “Swiss Cheese” diagram (Reason, 1991)
AdverseEvent
DEFENSES
Lack of Procedures
Punitive policies
Mixed Messages
Production Pressures
Zero fault tolerance
Sporadic Training
Attention Distractions
Clumsy Technology
Deferred MaintenanceTriggers

45
w Untested Equipment
w Changing Patient Population
wTailored to fit
wIS Support
w Loss of Situational Awareness
w Method of Report
wLayout of Unit
wNoise Level
Failures in theSystem
OrganizationalFactors
Procedures
Communication Patterns
Environment
The “Swiss Cheese”Model of Accident Causation

46
Two Ends of Health Care Systems
SharpEnd
BluntEnd
PATIENT
• Practitioners• Tools of the Trade
• Physical Infrastructure
• Financing, policies
• Health Plans, Payers...
•Regulations ...
47
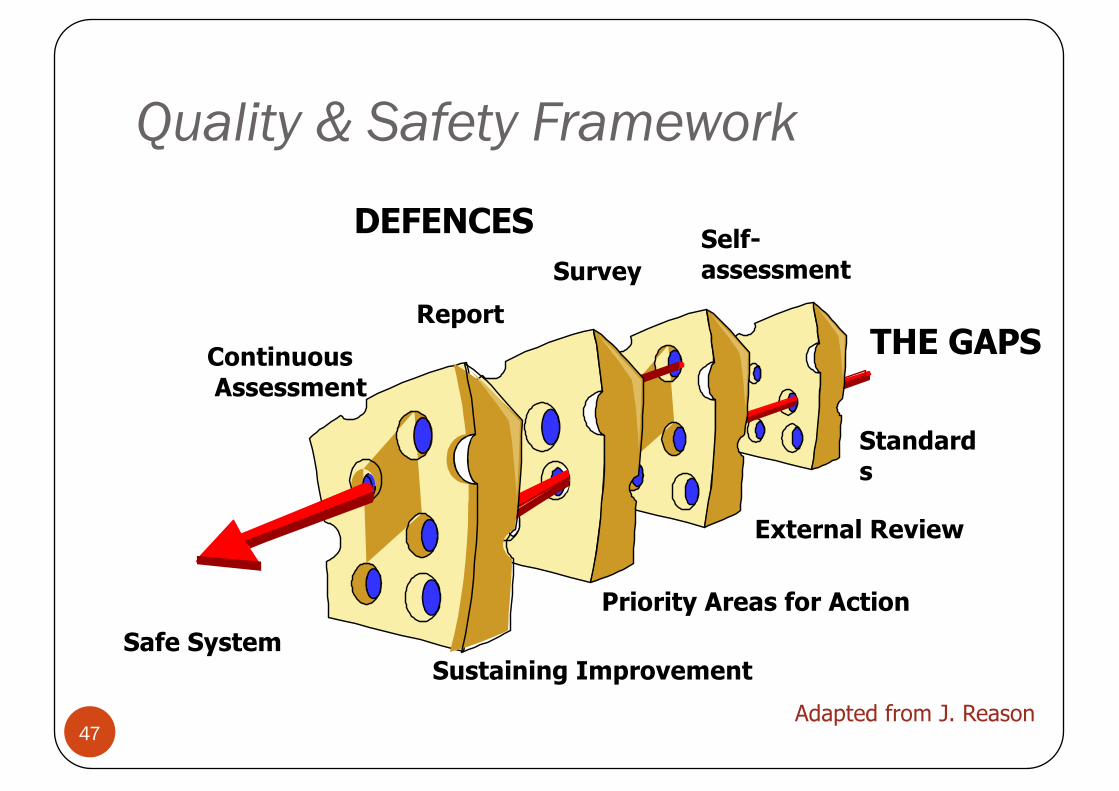
Quality & Safety Framework
Safe System
DEFENCES Self-assessmentSurvey
ReportContinuousAssessment
THE GAPS
Standards
External Review
Priority Areas for Action
Sustaining ImprovementAdapted from J. Reason
48
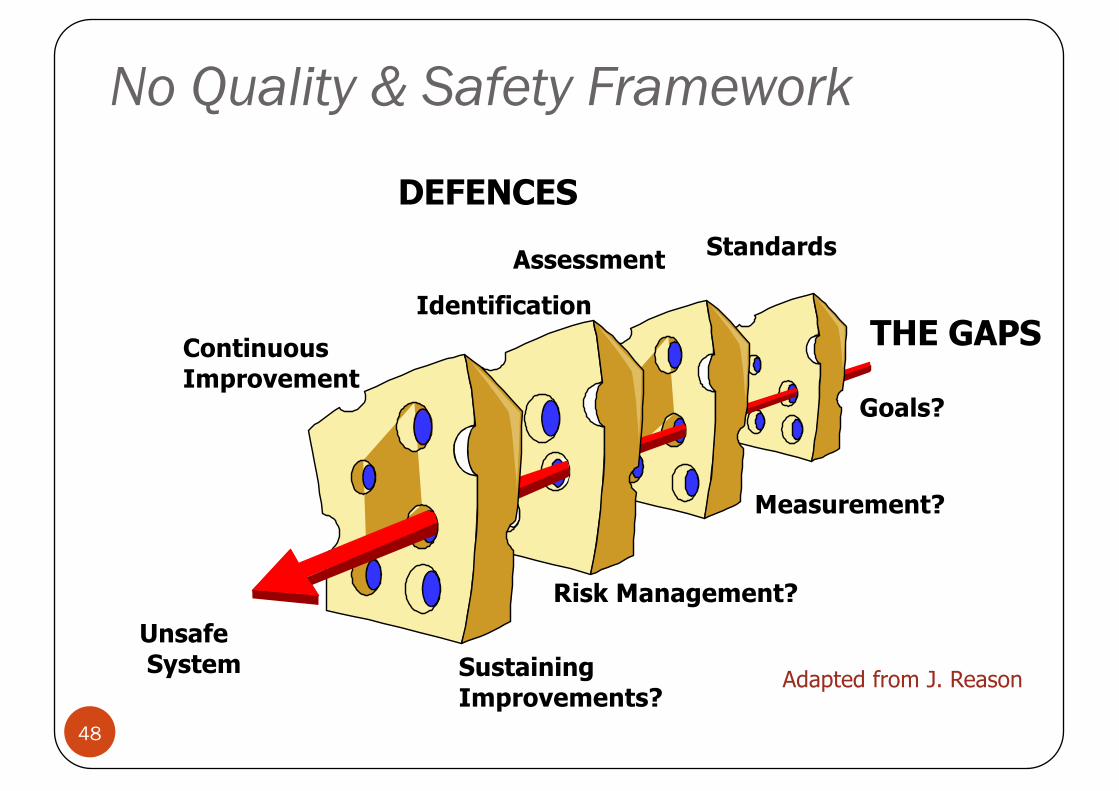
No Quality & Safety Framework
UnsafeSystem
DEFENCESStandardsAssessment
IdentificationContinuous Improvement
THE GAPS
Goals?
Measurement?
Risk Management?
Sustaining Improvements?
Adapted from J. Reason

49
Life at the Sharp End
1st Defense(distracted nurse)
2nd Defense(pharmacy)
3rd Defense(another distracted nurse)
Latent failure(understaffing)
TRIGGER(wrong drug prescribed)
Latent failure(no Rx tracking)
Latent failure(understaffing)
EVENT
PATIENT SAFETY
50
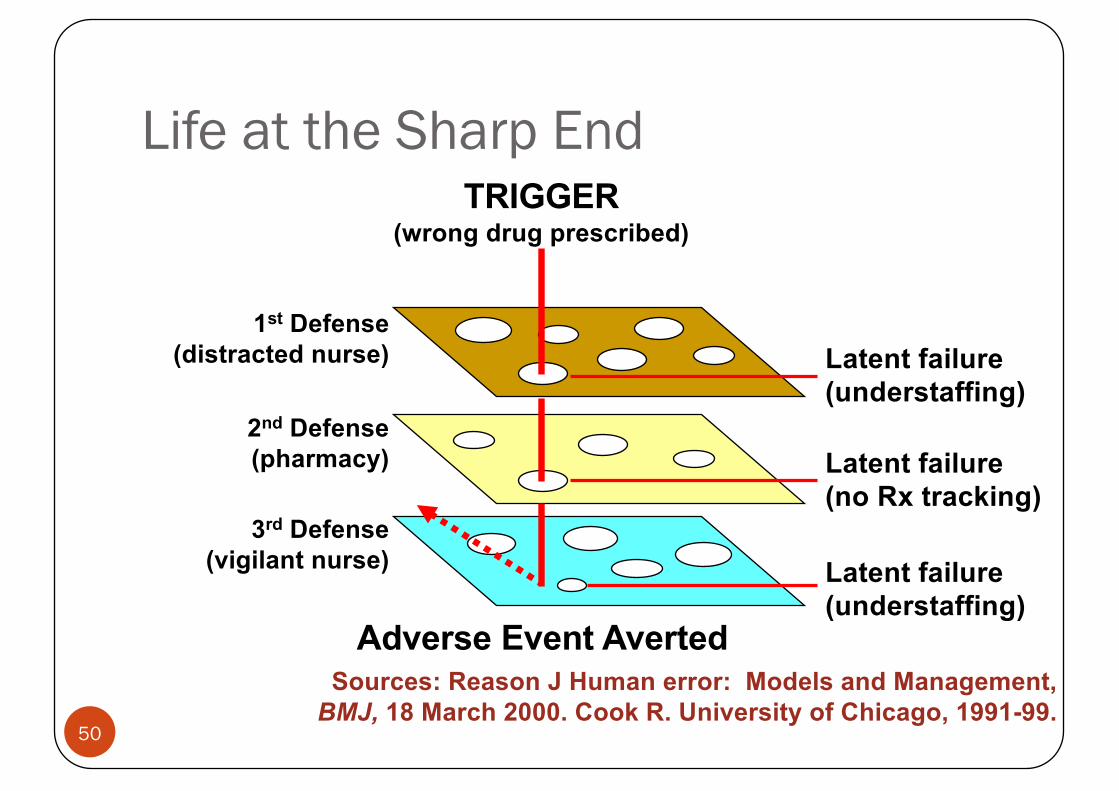
Life at the Sharp End
1st Defense(distracted nurse)
2nd Defense(pharmacy)
3rd Defense(vigilant nurse)
Latent failure(understaffing)
Adverse Event Averted
TRIGGER(wrong drug prescribed)
Latent failure(no Rx tracking)
Latent failure(understaffing)
Sources: Reason J Human error: Models and Management, BMJ, 18 March 2000. Cook R. University of Chicago, 1991-99.

51
Life at the Sharp End
1st Defense Template
Adverse Event Averted
TRIGGER(wrong drug prescribed)
Standardized approaches can reduce variability
and improve system efficiency
52
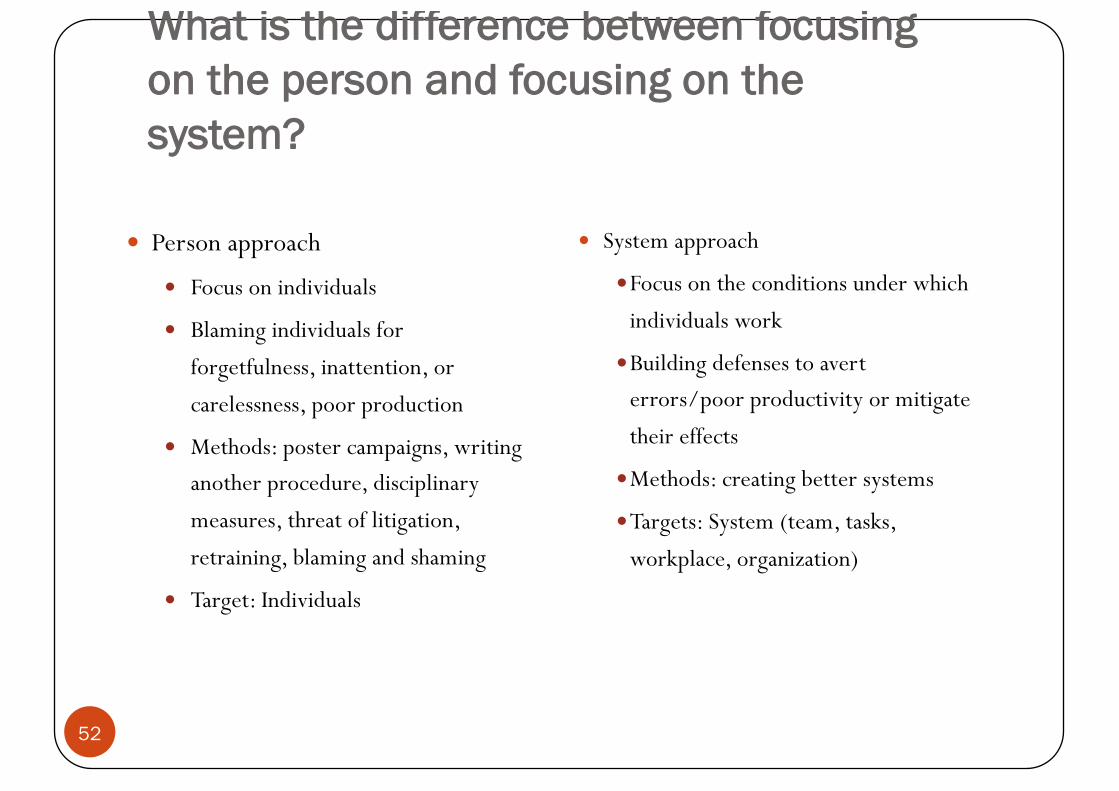
What is the difference between focusing on the person and focusing on the system?
� Person approach
� Focus on individuals
� Blaming individuals for
forgetfulness, inattention, or
carelessness, poor production
� Methods: poster campaigns, writing another procedure, disciplinary
measures, threat of litigation,
retraining, blaming and shaming
� Target: Individuals
� System approach
�Focus on the conditions under which
individuals work
�Building defenses to avert errors/poor productivity or mitigate
their effects
�Methods: creating better systems
�Targets: System (team, tasks,
workplace, organization)

System Approach to Human Error� Humans are fallible and errors are to be expected, even in the
best organisations.
� Focus: conditions under which individuals work
53
System Approach to Human Error� Counter-measures based on assumption that though we cannot
change the human condition, we can change the conditions under which humans work� by building system defences to avert errors or mitigate their effect
� When an adverse event occurs, the important issue is not who blundered, but how and why the defences failed.
54
Errors are inevitable
………….but most are preventable
55

56
Not Who caused the accidentbut What caused the accident?
“Medical errors most often result from a complex interplay of multiple factors. Only rarely are they due to the carelessness or misconduct of single
individuals.”
Lucien L. Leape, M.D.

57
“We cannot change the human condition, but we can change the
conditions under which humans work.” (Reason 2000)

58
Questions Surveyors Might Ask
� Is there a reporting policy and process for actual and potential
adverse events?
Are improvements made following incident investigation and
follow-up
Risk Management
�Focus on the system rather than the individual incident
� Is anticipatory not reactive in emphasis� Incident investigation and reporting supports
risk management by monitoring it
59
concepts---
� Hazard versus Risk� Safety culture & the elements of a safe and healthy work
environment� Classification (categorization) of hazards in a hospital� The individual versus the work environment (Who is our
concern?)
60
I. Hazard vs. Risk- 1� Hazard is any activity, situation or, substance that can cause
harm. It is a potential source of risk.
� Risk is the probability (odds) of a hazard causing harm.
61

What is Risk?
The chance of something happening that will have an impact on the objectives. It is measured in terms of consequences and likelihood
62

What is Risk? � Risk is the possibility of exposure to such factors as financial
loss, physical damage, injury or delay as a consequence of action or a lack of it.
� The level of risk exposure is the combination of the likelihood of risk occurring and consequences if it does occur.
63
What is Risk? � Risks and their consequences might include, but are not limited to:
� Breach of legal or contractual responsibility� Breach of security� A threat to physical safety� An adverse event during the care process� Deficiencies in financial controls and reporting� Failure of a project to reach its objectives� Failure of equipment or computer system� Fraud� Patient or family dissatisfaction� Unfavorable publicity
� In any healthcare organization risks can arise from internal and external sources
64
Hazard vs. Risk- 2
Risk = Hazard x f (Exposure)
65

Describing risk – the ‘3 C’s’Risk is inherently negative, implying the possibility of
adverse consequences. 1. Describe the potential consequences if the risk
were to materialise2. Describe the causal factors that could make the risk
materialise3. Ensure that the context of the risk is clear, e.g. is the
risk ‘target’ well defined (e.g. staff, patient, department, hospital, etc.) and is the ‘nature’ of the risk clear (e.g. financial, safety, physical loss, perception, etc.)
66
Which of the following are adequate descriptions of risk?
� Risk to patients due to errors and unsafe clinical practice caused by reduced skill base and competence of junior and middle grade medical staff
� Needlestick injury� OSH� Reduced staff retention and increased sickness absence due to
reduction in morale caused by increased workload, pressure and stress to achieve targets
� Inadequate patient transfer� Budget overrun and financial deficit due to cost of introducing new
technologies/medicines as required by NICE guidance� Medication error
67
Why Risk Management?
The culture, process and structures that are directed towards the effective management of potential opportunities and adverse effects
68

Risk Management: The Reactive Versus Proactive approach
� Hypothetically—a patient who receives medicine that causes a point of care false high blood sugar. The patient receives treatment for the high blood sugar and shortly thereafter experiences hypoglycemia, which leads to the patient coding.
� In a reactive system, the patient would be coded and would potentially have devastating injuries because the staff and physicians were unaware of this false high blood sugar.
� Adversely, in a proactive system, the staff and physicians would have been educated on this medication, thereby causing a repeat laboratory blood glucose level, which would have been normal. This normal level would have prevented the treatment, keeping the patient safe.
� By educating the staff and physicians, an adverse event causing patient harm was avoided.
69
Accreditation Requirements� The hospital must have a documented risk management plan
that includes but not limited to:� Information Technology service loss� Major equipment failure� Credit withdrawal/loan arrangements from external
financiers� Staff negligence and malpractice, etc.
70

Healthcare Risk Categories
71

A. Patient Care-related Risks1. Inappropriate or incorrectly performed medical treatment 2. Confidentiality and appropriate release of information3. Protection from abuse, neglect and assault4. Securing appropriate informed patient consent for
treatment5. Nondiscriminatory treatment
72
A. Patient Care-related Risks6. Protection of patient valuables from loss or damage7. Appropriate triage and transfer of patients from ER8. Patient participation in research studies 9. Utilization review decisions (timing of discharge, provision
of medically necessary services)10. Access to care
73
B. Employee-related Risks1. Occupational illness and injury
� Infections� Exposure to toxic chemicals� Electrical hazards� Sprains and back injuries� Burnout
2. Allegations of discrimination in recruitment, hiring, and promotion based on age, race, sex, national origin, disability; wrongful termination
3. Sexual harassment4. Impaired physicians and other providers who pose a threat to
patient or employee safety74

C. Risks related to visitors
1. Infections2. Injuries caused by slips, falls, and other
mishaps
75
D. Property-related Risks1. Buildings and valuable equipment: risk of losses due to fires,
floods, etc2. Paper and/or electronic records (patient, business and
financial): risk of damage, destruction3. Cash, cheques, valuables: risk of loss of theft4. Property and liability losses due to operation of ambulances,
trucks, cars owned or leased by the organization
76

E. Financial Risks
1. Risks associated with new ventures or services2. Continued financial viability of organization's traditional
services3. Liability imposed from suits by stakeholders
77

78
Reducing harm by identifying and controlling hazards
79
What is a hazard?� In safety, a HAZARD is anything that can put somebody or
something at risk of damage or injury or harm.
� In medicine, hazards are called risk factors.
80
Why focus on hazards and harm?� In medicine, if we want to reduce the incidence rate of a disease
we
� Look for risk factors
� Figure out how they contribute to the disease
� Figure out how to reduce or eliminate the risk factor.
� In safety, if we want to reduce adverse events, we
� Look for hazards
� Figure out they contribute to the adverse events
� Figure out how to reduce or eliminate the hazard.
81
How do you identify safety hazards?� Proactive techniques, such as Healthcare Failure Mode and Effect Analysis
(preventive medicine)
� Focused upon complex, face-paced areas of the hospital
� Accomplished prior to implementing new software or new devices
� Reactive techniques, such as Root Cause Analysis (RCA) (acute care medicine)
� Based on reports of close calls
� Based on reports of injuries
82
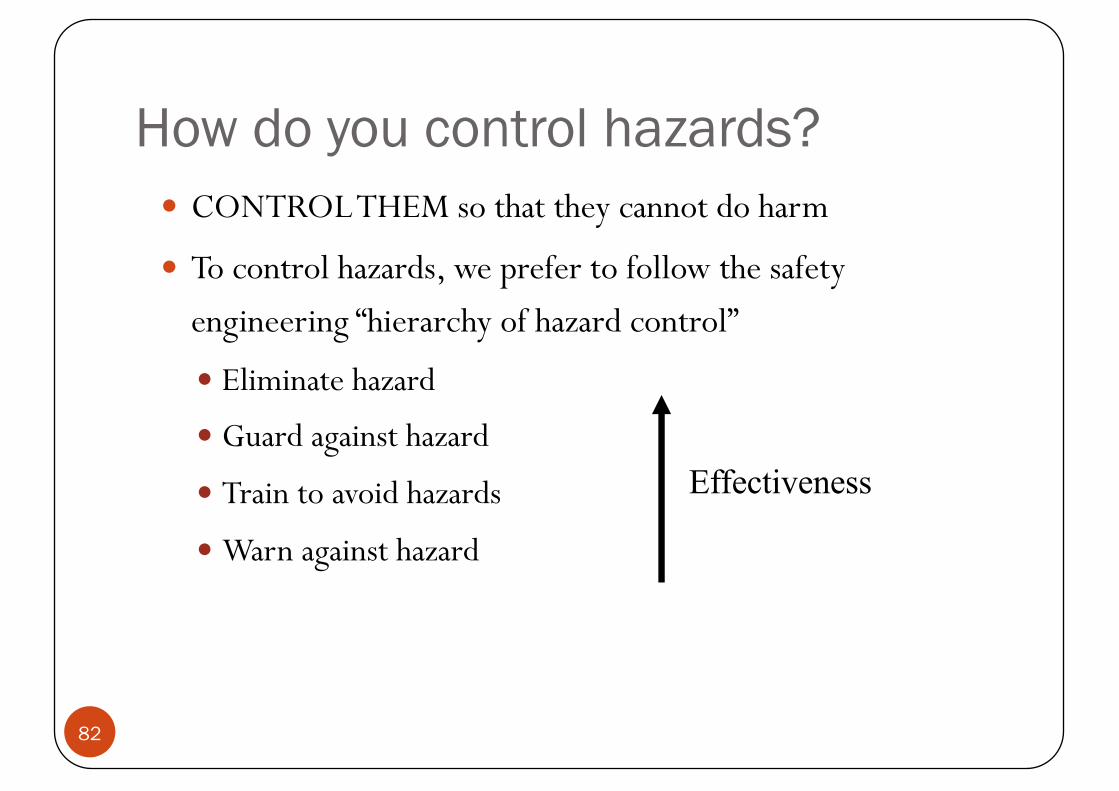
How do you control hazards?� CONTROL THEM so that they cannot do harm
� To control hazards, we prefer to follow the safety engineering “hierarchy of hazard control”
� Eliminate hazard
� Guard against hazard
� Train to avoid hazards
� Warn against hazard
Effectiveness

Barriers, Controls and Defences• Checking the drug dosage before
administering• Checking the temperature of a bath
Human Action Barriers
• Protocols and procedures e.g.• Implementation of a drug administration policy
• Supervision and training
Administrative Barriers
• Lead apron for radiographers• Bed side rails
Physical Barriers
• Isolation of MRSA patients (placement)Natural Barriers time, distance,
placement83

Contributory Factors1. Individual factors2. Team and social factors3. Communication factors4. Task factors5. Education and training factors6. Equipment and resources factors7. Working conditions8. Organizational and strategic factors9. Patient factors
84
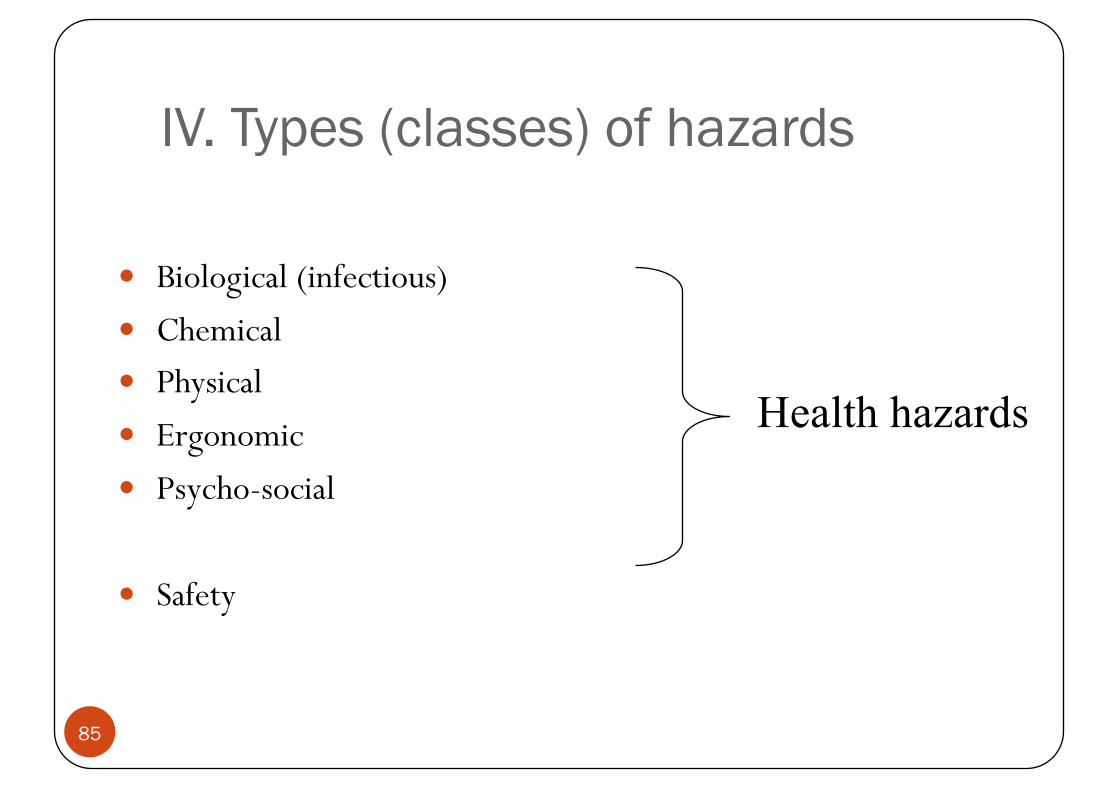
IV. Types (classes) of hazards
� Biological (infectious)� Chemical� Physical � Ergonomic� Psycho-social
� Safety
Health hazards
85
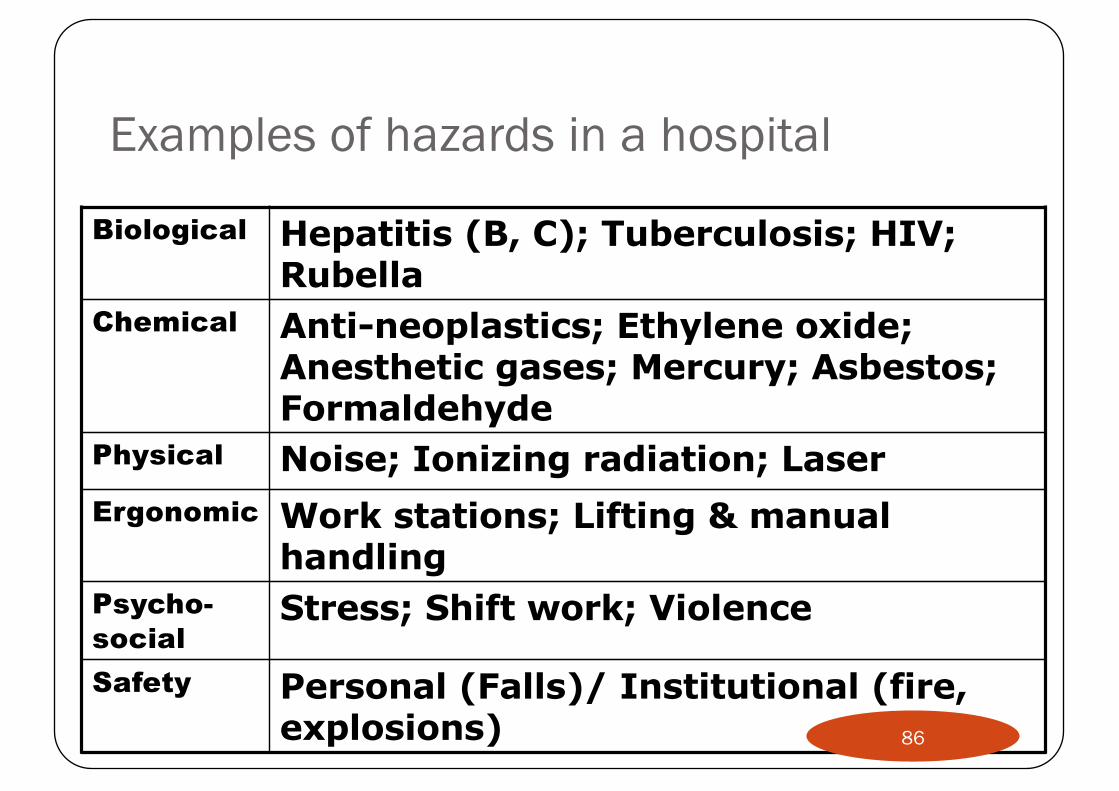
Examples of hazards in a hospital
Biological Hepatitis (B, C); Tuberculosis; HIV; Rubella
Chemical Anti-neoplastics; Ethylene oxide; Anesthetic gases; Mercury; Asbestos; Formaldehyde
Physical Noise; Ionizing radiation; LaserErgonomic Work stations; Lifting & manual
handlingPsycho-social
Stress; Shift work; Violence
Safety Personal (Falls)/ Institutional (fire, explosions) 86
Risk perception
87
Risk perception
88

Risk perception
89

90
91

92

93
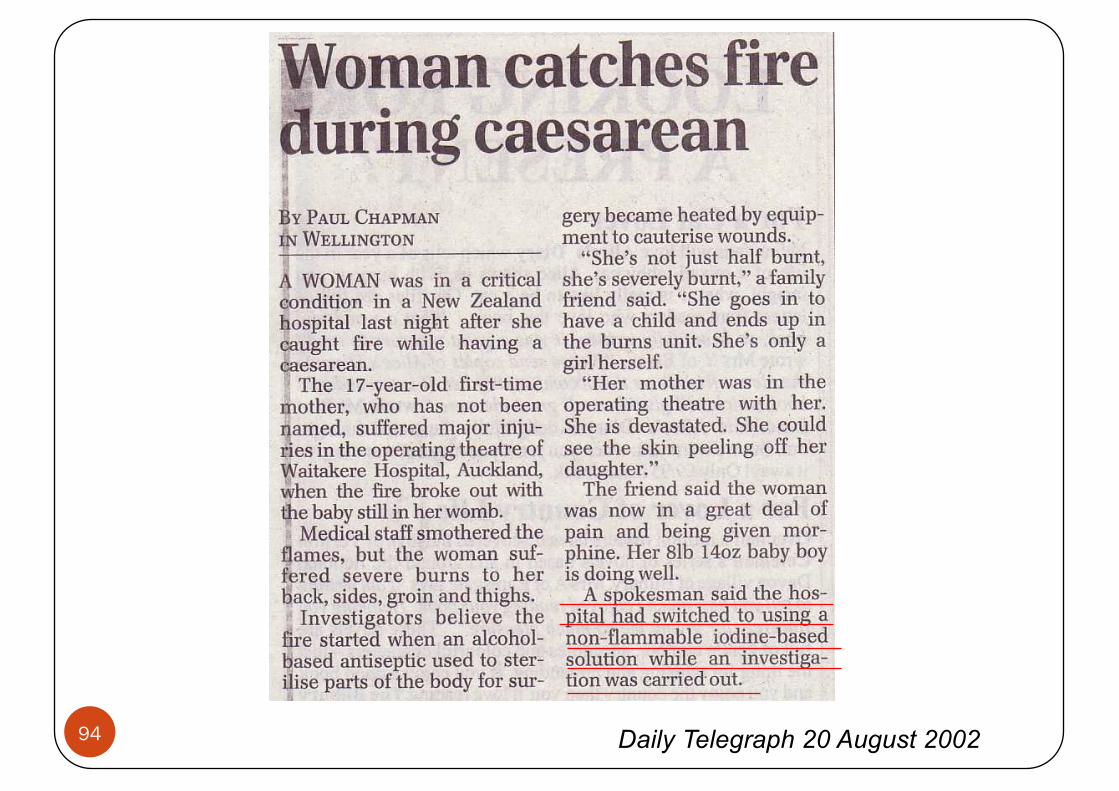
Daily Telegraph 20 August 200294

Clinicians � Premature discharge of patients leading to death or poor
outcome due to bed shortage� Delay or missed diagnosis/treatment resulting in increased
mortality & morbidity� Risk of harming patients associated with invasive procedures� Long waiting lists resulting in increased morbidity &
complaints� Medication error� Harm to staff due to violent patients
95
Anaesthetists (1)� Risk associated with equipment failure� Risk associated with inadequate supervision of trainees� Risk of giving the wrong drug to patient due to mislabeling� Risk of overdosing patient� Risk of making unsound judgement after long hours of duty
96
Anaesthetists (2)� Risk of malfunctioning of resuscitation equipment due to
lack of maintenance� Risk of improper use of Level I rapid transfuser in
emergency due to inadequate training� Risk of staff injury and equipment failure due to cables &
power cords lying on the OT floor � Risk of injury to staff
� Bumping of head against theatre light� Slip & fall after mopping of OR
97
Radiology/Pathology� Risk associated with missing specimen or X ray films� Patient Identification
� Medication, Xray & Path reports� Miss labeling of specimen
� Risk associated with Equipment Maintenance & Validation
� Risk associated with Manual handling� Risk associated with chemical waste handling� Risk associated with understaffing
98
IT Concerns
� Non-human events: these events typically happen on an unpredictable basis without direct human influence
� local infrastructure failure: Emergency room is disconnected from the network backbone but some emergency help must be provided to patients.
� major industrial accidents: A large number of injuries must be treated while a power failure caused by that accident hinders provision of health care
� natural disasters: They may cause injury to the local community as well as to the local infrastructure. A power failure may hinder the operation of the medical equipment, but many injuries flood the emergency room at the same time.
99

24-Elements that Increase Risk in the ED:
� hour operation (someone has to work night shifts)� EDs frequently operate in excess of capacity� Patient-provider relationship not established� ED patients are high acuity� Multiple distractions to providers in the ED� No provider continuity due to shift work� Patients are stressed, not always in ED of own free will� Long patient waits
100

Strategic ‘challenges’ for Hospital
� Epidemics � Resources availability
• Funding• Beds• Staffing
� People capacity� Service expansion/demand� New technology� Evolution of cluster management
101

How to control hazards…
�RISK MANAGEMENT
�For example, in the case of occupational health and safety (OHS):�Hazard mapping�Job safety (hazard) analysis
102
Example of Effective RISK MANAGEMENT (OHS related)� Leadership and support, with a broader role for OHS
committee (specialists) � Developing knowledge, ability and motivation � Solid, local understanding of OHS principles. � Proactive, systematic and comprehensive identification of
hazards, assessment and control of risks. � Solutions to control risks
103
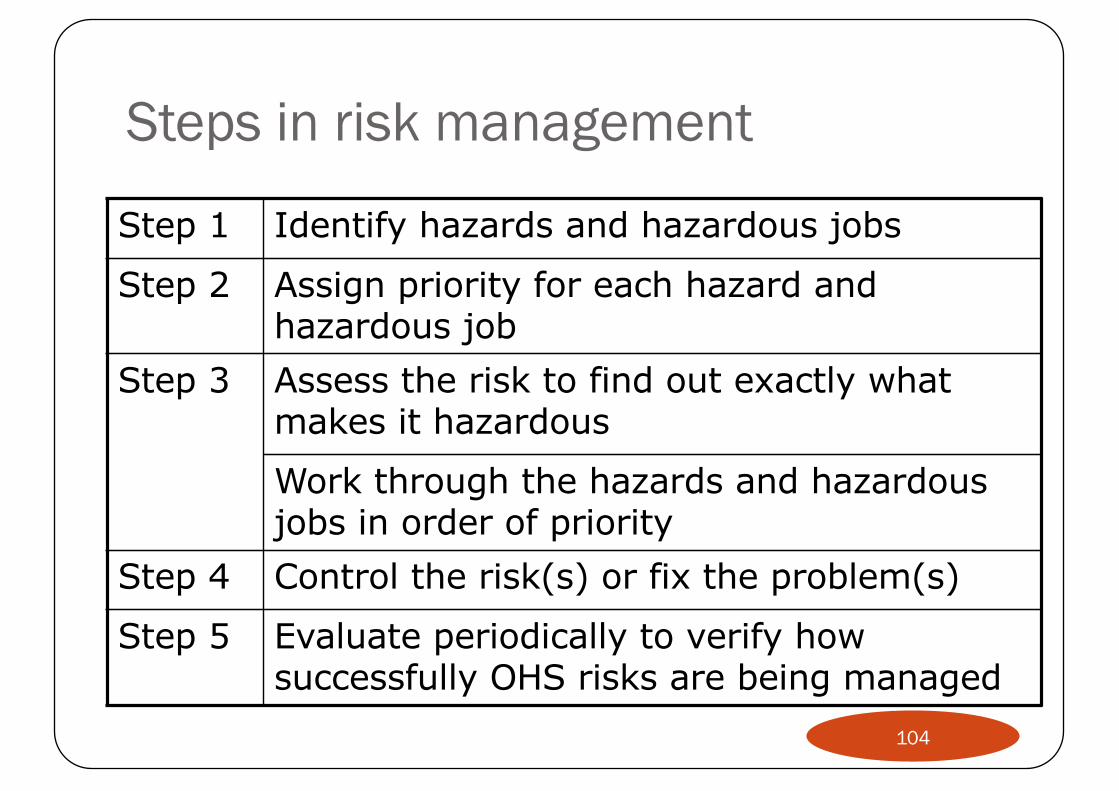
Steps in risk management
Step 1 Identify hazards and hazardous jobs
Step 2 Assign priority for each hazard and hazardous job
Step 3 Assess the risk to find out exactly what makes it hazardous
Work through the hazards and hazardous jobs in order of priority
Step 4 Control the risk(s) or fix the problem(s)
Step 5 Evaluate periodically to verify how successfully OHS risks are being managed
104

Hospital hazards by group at risk
HAZARD Staff Patient GuestBiological
Chemical
Physical
Ergonomic
Psycho-socialSafety
105

Who is the staff?� Office workers � Clerks on floors� Physicians� Physicians-in-training� Medical students� Nurses/ Midwives� Nursing students� Orderlies/nursing assistants� Nursing supervisors� Pharmacists� Nutritionists� Social workers
� Lab technologists� Radiology technicians� Protection officers� Housekeeping� Drivers� Staff in laundry� Staff in kitchen� Staff in restaurants� Mortician� Technicians (electricity,
painting, plumbing, mechanic)
106
How do we group people (staff)?
� Knowledge and Skill (What they know) � Work Process (Process or activity) � Business Function (Basic function in the organization)� Time (When work is done– shifts)� Output (Service provided) � Client/Patient (Type of patient) � Place
107
Patient safety
� Fall protection� Prevention of “uncontrolled” self injury� No access or exposure to drugs, biohazards, radiation, or
leftover needles� No hospital-acquired infections� Clear exit routes in case of emergencies � Knowledge of where to report emergencies
108
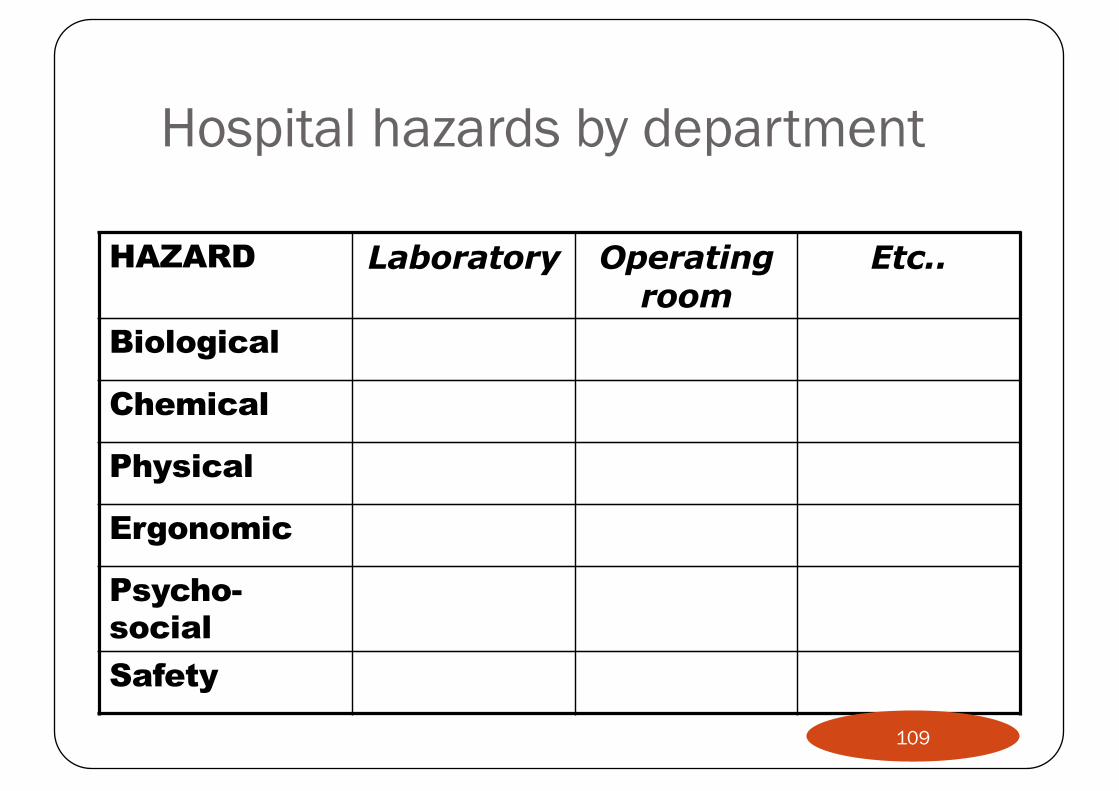
Hospital hazards by department
HAZARD Laboratory Operating room
Etc..
Biological
Chemical
Physical
Ergonomic
Psycho-socialSafety
109

110
111

112

113
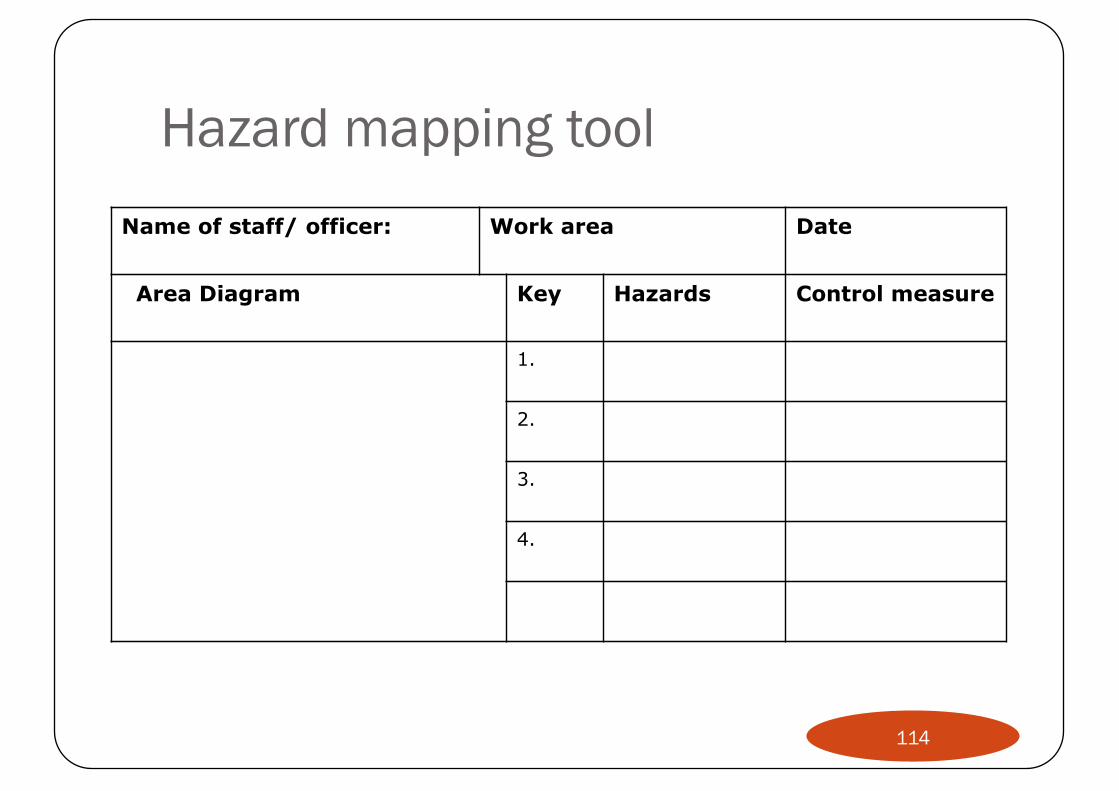
Hazard mapping toolName of staff/ officer: Work area Date
Area Diagram Key Hazards Control measure
1.
2.
3.
4.
114

Hazard mapping chart
Almost never
Slight Moderate SevereFrequency
Low
Moderate
High
Severity
Retain
Transfer
Reduce/Prevent
Avoid
115
Job Hazard (Safety) Analysis� Best if employee is observed doing the job
� The job, not the individual, is being studied� Clearly explained to the employee
� The work procedure is broken into several specific tasks
� Each separate task should be analyzed to complete a job safety analysis for that procedure
� The correct work procedure is presented in a step-by-step outline
� Employee who carries out the tasks should be consulted in developing the procedure
116
Control measures
�Engineering/ structural control�Administrative changes�Personal measures
117

Engineering/ structural control
� Assumption: Best not to depend on people for prevention but to change and redesign the work environment
� Examples:� Hoods� Anti-slippery floors� Positive pressure ventilation� Building codes
� Stairs, Light, Doors, Floor…� Disabled-friendly
118
Administrative control
� Training and awareness� Maintenance� Reduction of duration of exposure/ Rotating employees� Modify job descriptions/ Change work practices� Staff management
� Shift� Relief
119

Personal measures
� Least effective and require ongoing training and awareness programs
� Use of gloves and goggles� Proper disposal of needles and biohazards� Use of proper masks and overalls� Personal hygiene
� Washing hands is best method to control spread of infections in a hospital
� Abide by regulations such as no entry to radiology rooms
120
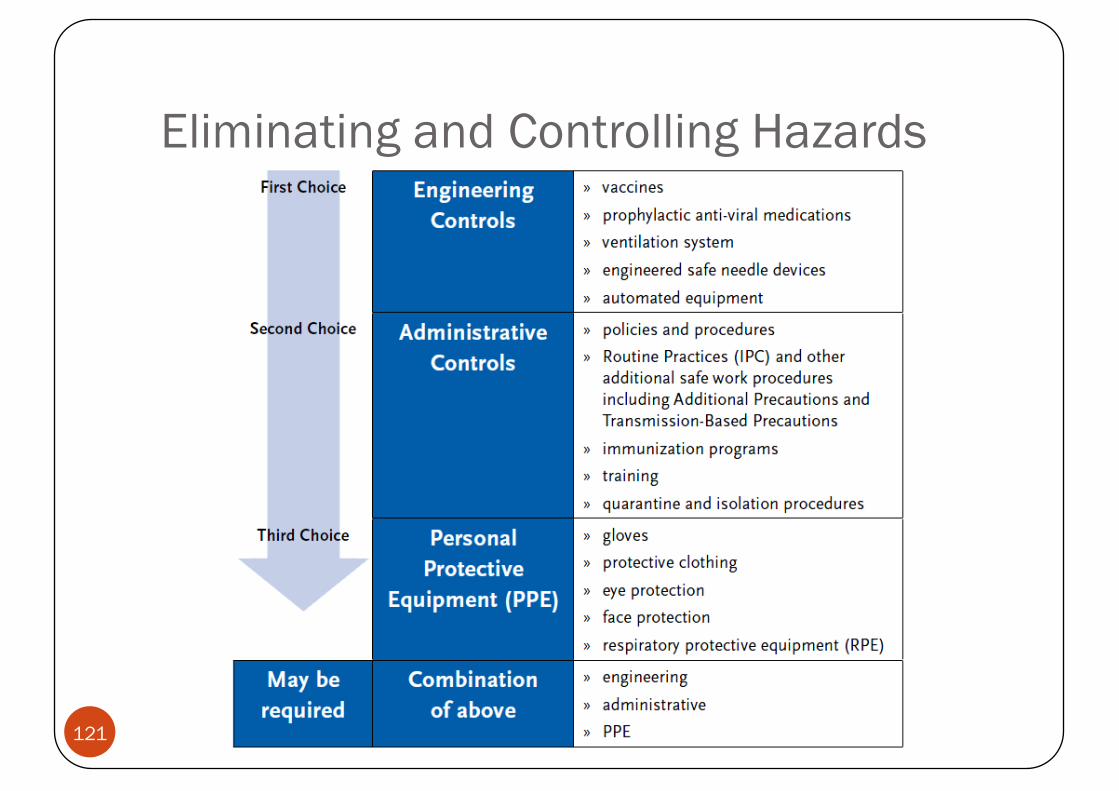
Eliminating and Controlling Hazards
121
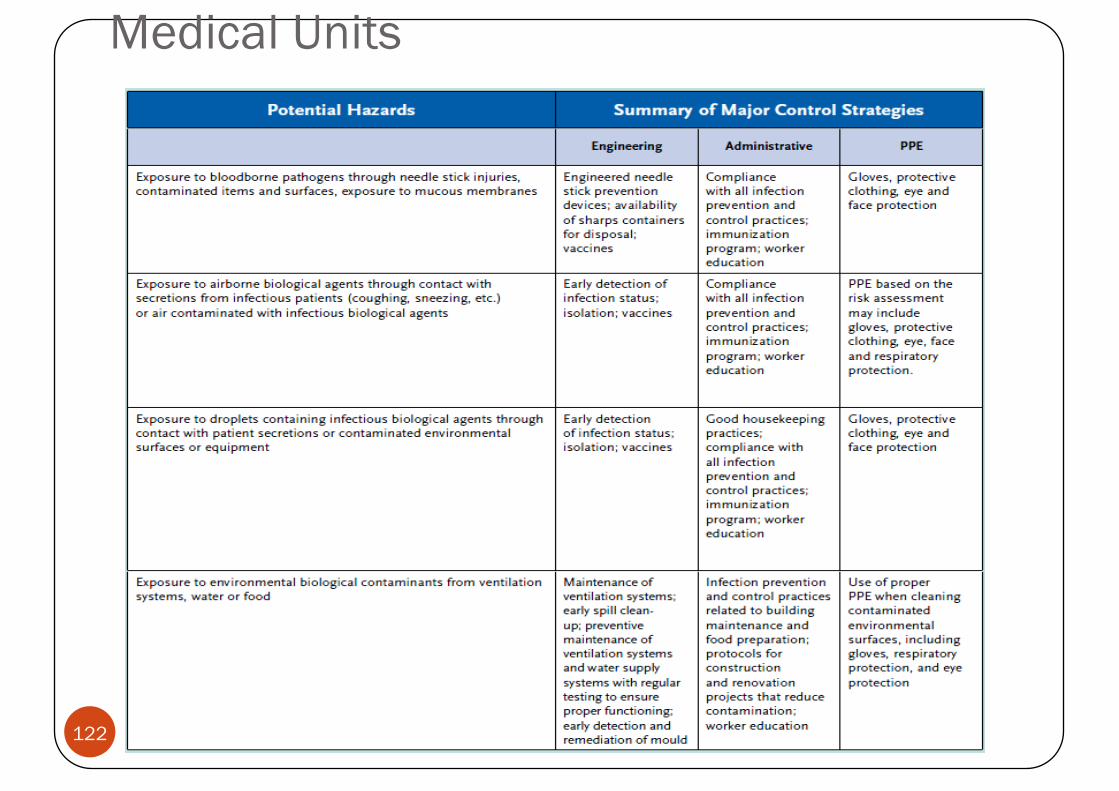
Medical Units
122
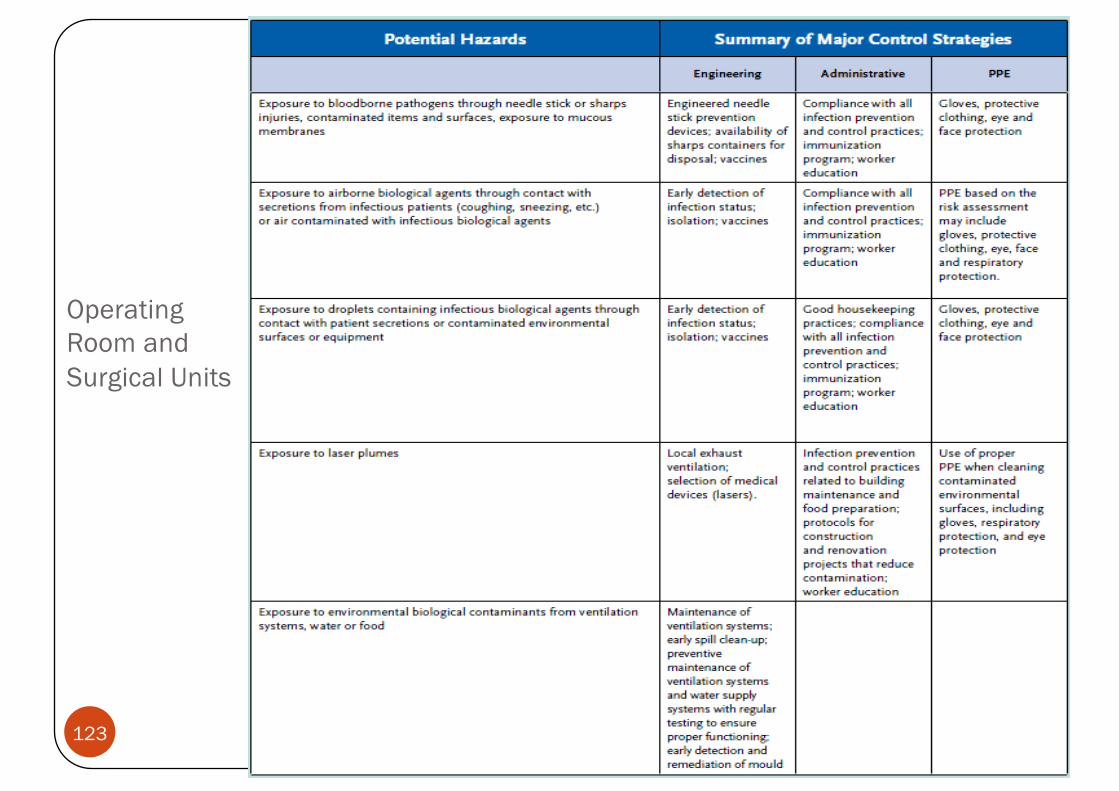
Operating Room and Surgical Units
123

Emergency Rooms
124
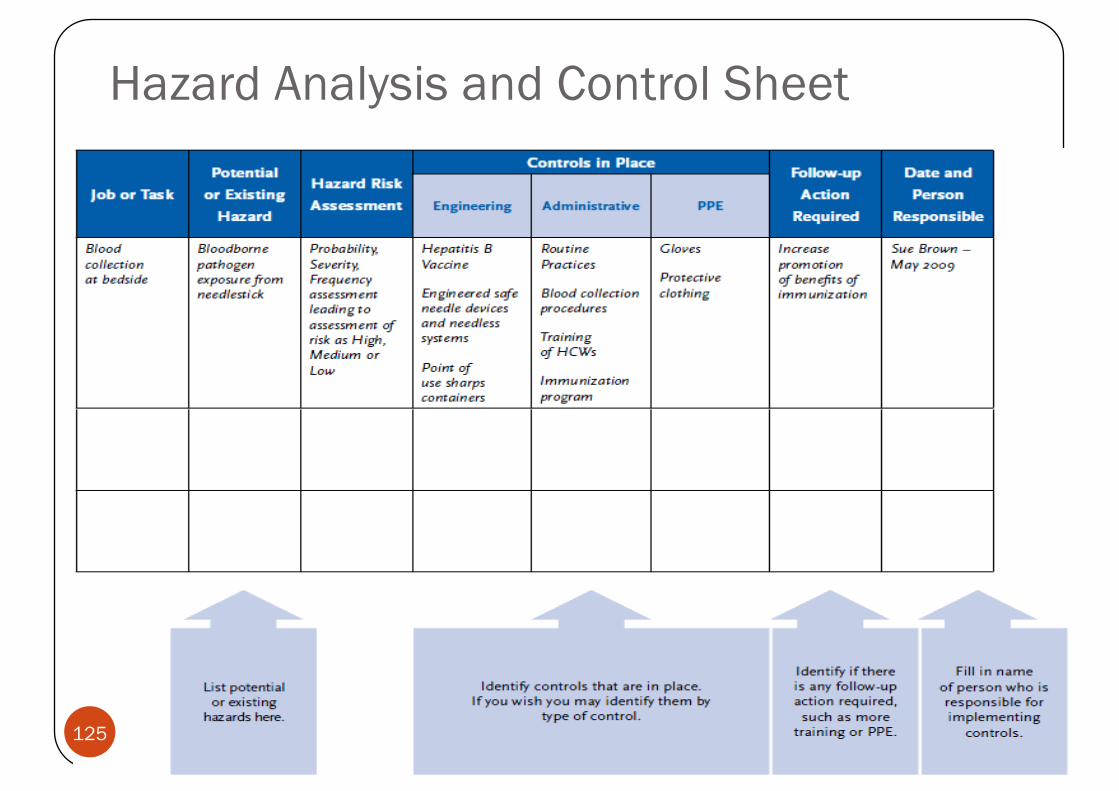
Hazard Analysis and Control Sheet
125

Training
�General�Workplace/ job specific
126
Orientation manual
� Commitment of hospital to health and safety of its employees, patients, and guests
� Orientation to different departments and activities in the hospital
� Analysis of potential hazards in one’s job� Options for prevention and control� Access to information about hazards
� Incident and accident reporting
127
Topics for training
� Emergencies (e.g., fire)� Work-related accidents� Fall protection� Hazardous material� Ergonomics� Bloodborne pathogen exposure� Radiation� Lab safety� Personal protection
128

Hazard communication� Inventories� Material Safety Data Sheet� Warning/ Signs and labels
� Containers� Departments� Exits
� Training� Employee’s right to know� Procedure in case of emergency
129

130
1. Think about yourself and your colleagues – list 3 issues or concerns you have at work.
2. Now think about patients – list 3 issues or concerns you might have in relation to the safety or quality of care provided to patients in your department, hospital, PHC, etc.
3. Finally, think about your organisation– list 3 issues or concerns………..
Excercise
131

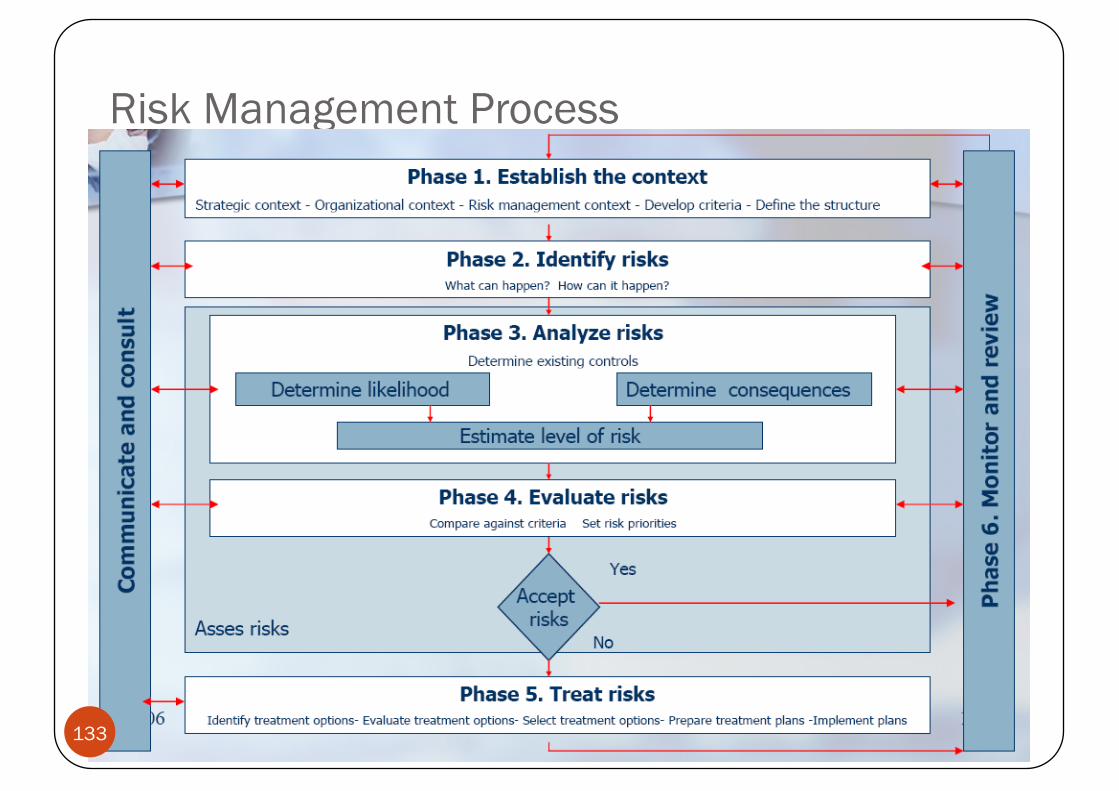
Risk Management Process
Systematic application of management policies, procedures and practices to the tasks of establishing the context, identifying, analyzing, evaluating, treating, monitoring and communicating risk
132
Risk Management Process
133

Risk Management Process:Phase 1. Establish the Context
� Establishing the context involves the following steps:
1. Establish the strategic context2. Establish the organizational context3. Establish risk management context4. Develop risk evaluation criteria5. Define the structure
134
Risk Management Process:Phase 2. Identify Risks)
� Comprehensive identification using a well-structured systematic process is critical because a potential risk is not identified at this stage is excluded from further analysis and treatment.
� All risks should be identified whether or not they are under the control of the organization.
135


138
Information Sources for Risk Identification
1. Incident reporting
2. Generic occurrence screening
3. Patient complaints and satisfaction survey results
4. Claims data of prior professional liability, property and casualty, and workers’ compensation
139

Information Sources for Risk Identification
5. Surveys by accrediting bodies, insurers, or risk management consultants
6. Licensure surveys
7. Information from facility’s infection control and quality improvement functions
8. Workplace inspections/audits
140
Information Sources for Risk Identification
1. Incident reporting2. Generic occurrence screens3. Patient complaints/satisfaction surveys4. Claims5. Accreditation/insurers surveys6. Licensure surveys7. Infection/QI reports8. Workplace inspections/audits9. Informal discussions
141

Risk Management Process:Phase 3. Analyze Risks� The objectives of risk analysis are:
� Separate minor acceptable risks from major risks� Provide data to assist in the evaluation and treatment
of risks� Risk analysis includes determining existing controls by
identifying existing management, technical systems and procedures to control risks, and assess their strength and weaknesses.
142

Risk analysisis the process of determining � the potential severity of the loss associated with an identified
risk, and
� the probability that such a loss will occur
143
Severity Assessment Code (SAC) Adapted
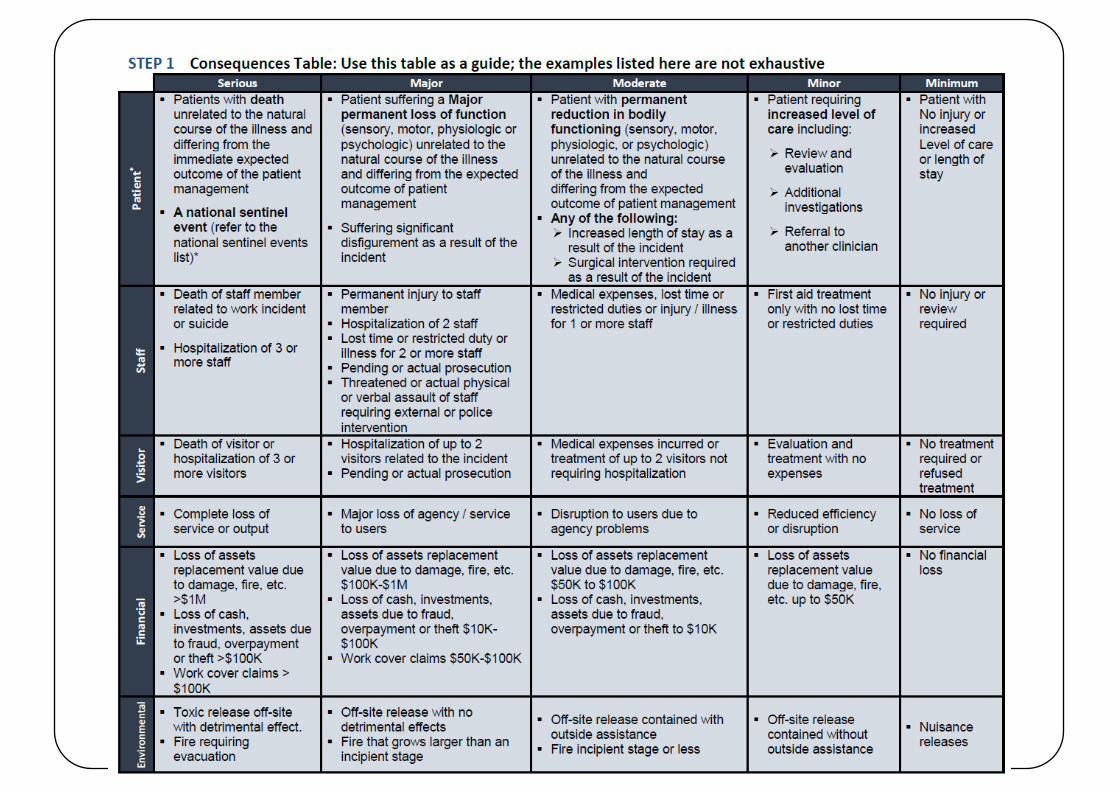
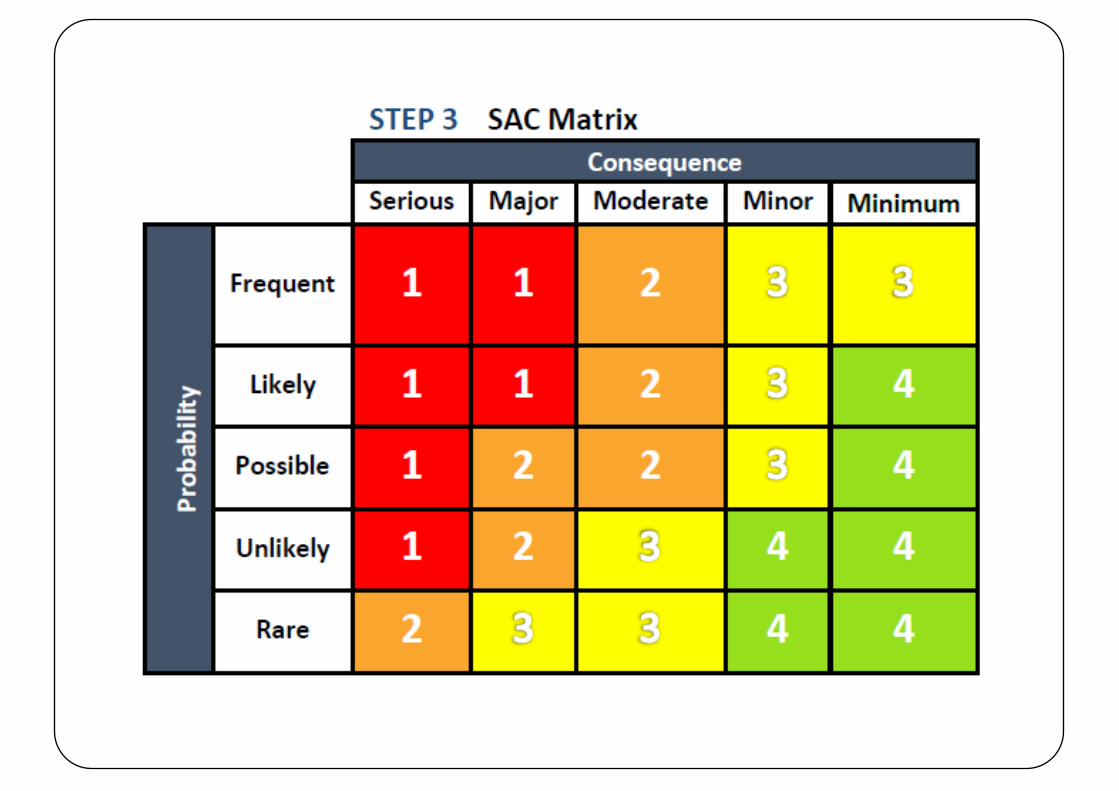


SAC Consequence Score1. Actual consequence2. Potential consequence (worst case scenario if incident
recurred)
149

Assessing the level of Risk � Two elements are determined when assessing the level of risk
posed by the risk that has been identified;
� (i) The likelihood that a risk may occur or reoccur.
� (ii) The impact of harm to service users, staff, services, environment or the organization.
150

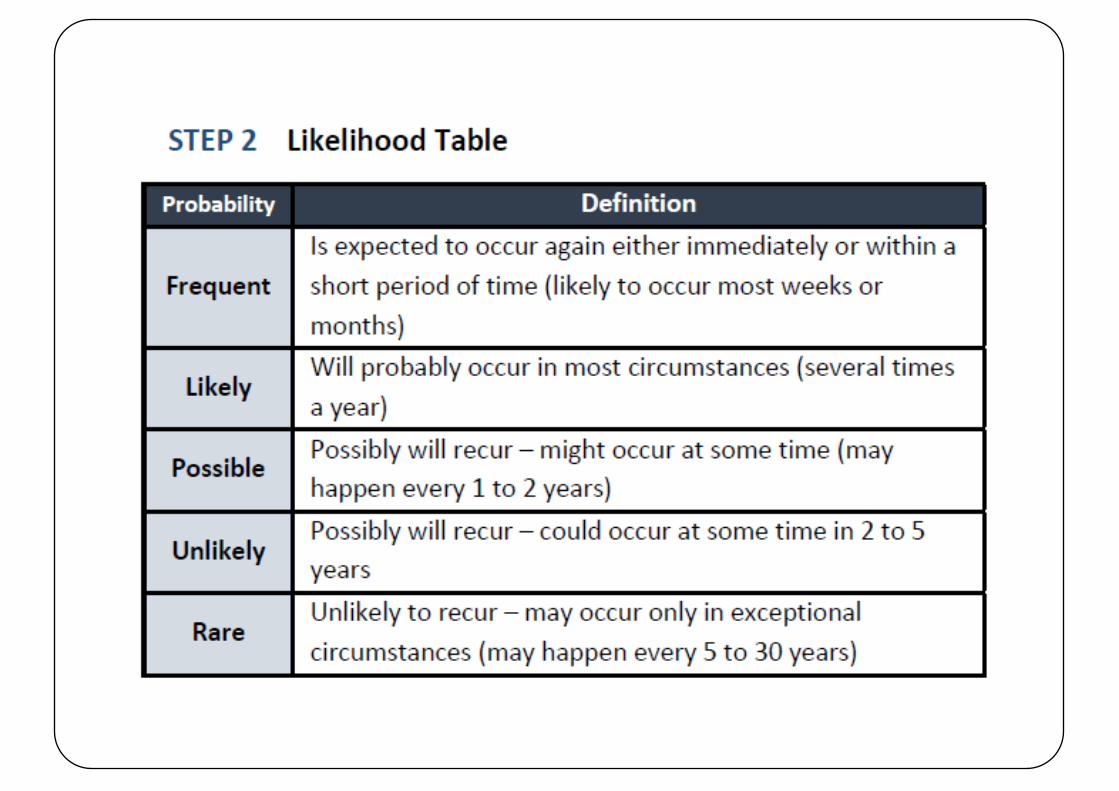
Likelihood Scoring� Likelihood scoring is based on the expertise, knowledge and actual
experience of the group scoring the likelihood. In assessing likelihood, it is important to consider the nature of the risk. Risks are assessed on the probability of future occurrence; how likely is the risk to occur? How frequently has this occurred?
� It should be noted that in assessing risk, the likelihood of a particular risk materializing depends upon the effectiveness of existing controls. In assessing the likelihood, consideration should be given to the number and robustness of existing controls in place, with evidence available to support this assessment. Generally the higher the degree of controls in place, the lower the likelihood.
� The assessment of likelihood of a risk occurring is assigned a number from 1-5, with 1 indicating that there is a remote possibility of its occurring and 5 indicating that it is almost certain to occur.
151
Exercise
152
Wrap up Day 1
153





























