Embed Size (px)
Citation preview

©2017 MFMER | slide-1
Biopsy interpretation of liver tumorsRish K. Pai MD, PhDProfessor of Laboratory Medicine & PathologyMayo Clinic ArizonaFlorida Society of Pathology Summer [email protected]
©2017 MFMER | slide-2
Liver mass biopsies: Diagnostic issues
• Cirrhotics versus non-cirrhotics
• Malignant tumor in the liver• How to approach these biopsies and confirm or exclude HCC• Subtypes of HCC and mixed tumors• Well-differentiated HCC
• Recognize and correctly classify benign lesions• Recognize lesional tissue• Hepatocellular adenoma• Focal nodular hyperplasia
©2017 MFMER | slide-3
Liver mass biopsies: Upfront work
•Have standard protocols for a biopsy of a liver mass
• If multiple cores are taken, separate into differentblocks
• If a big core, divide and separate into two blocks
•Cut unstained slides upfront to avoid wasting tissue
•Don’t use up all the tissue:• Reserve tissue for molecular testing
1
2
3

©2017 MFMER | slide-4
Cirrhotic liver• Hepatocellular carcinoma
• Cholangiocarcinoma
• Mixed HCC/Cholangiocarcinoma
• Macroregenerative nodule(only on explant)
• Dysplastic nodule (only onexplant)
Non-Cirrhotic liver• < 50 y:
• Hepatocellular adenoma
• Focal nodular hyperplasia
• Hepatocellular carcinoma
• Other primary tumors
• Metastases
• > 50 y:• Metastases
• Hepatocellular carcinoma
• Cholangiocarcinoma
• Focal nodular hyperplasia
• Other primary tumors
Classification of liver tumors: Context!
©2017 MFMER | slide-5
A note on Dysplastic nodules
• Dysplastic nodule is only diagnosed in the setting ofknown cirrhosis – very rare to diagnose on needlebiopsy (only safely diagnose on explants/resections).
• Dysplastic nodule:• Foci of small cell change (increased N:C ratio)• Focal loss of reticulin• Increased arteries within the lesion
©2017 MFMER | slide-6
Screening for HCC: Imaging for pathologists
• Ultrasound for cirrhotic patients every 6 months• 94% sensitivity for HCC (only 63% for early HCC)
• CT or MRI is then performed to further classify and determine extent of disease
• HCCs have increased arteries compared to surrounding liver: Brighter inarterial phase and darker in portal venous phase
Arterial phase Equillibrium Portal venous phase
4
5
6

©2017 MFMER | slide-7
Cirrhotic liver: Screening for HCC• LI-RADS system (also known as OPTN classification)
Adv Anat Pathol. 2015 Sep;22(5) 314-22.
©2017 MFMER | slide-8
Title
• Text
©2017 MFMER | slide-9
• Extended Toronto Criteria (for those patients beyond Milan criteria: single tumor ≤ 5cm, 2-3 tumors none >3cm, no vascular invasion and/or extrahepatic spread)
• Tumor confined to liver• No radiologic evidence of biliary or venous thrombus• No cancer-related symptoms• Biopsy of the largest tumor is not poorly differentiated
• Patients meeting this extended criteria did as well as those withinMilan criteria
Cirrhotic liver: HCC
7
8
9

©2017 MFMER | slide-10
• Macrotrabecular pattern of growth is also associated withpoor prognosis
Grading Hepatocellular carcinomaGrade Global assessment Criteria
1 Well differentiated • Tumor cells resemble normal liver• Hepatocellular adenoma or dysplastic
nodule may have to be distinguished
• Cytoplasm: ranges from abundant and eosinophilic to moderate and basophilic
• Nuclei: minimal to mild nuclear atypia• Reticulin: Limited reticulin loss, relatively thin
plates2 Moderately
differentiated• Clearly malignant. • Morphology still suggests hepatocellular
differentiation.
• Cytoplasm: ranges from abundant and eosinophilic to moderate and basophilic
• Nuclei: moderate nuclear atypia; occasional multinucleated tumor cells are acceptable
• Reticulin: More prominent loss3 Poorly differentiated • Clearly malignant.
• Morphology is not specific for hepatocellular differentiation
• Cytoplasm: ranges from moderate to scant, usually basophilic
• Nuclei: marked nuclear pleomorphism, may include anaplastic giant cells
• Reticulin: Variable
• 68 year old cirrhotic male with an atypical liver mass by imaging.
Case 1:
©2017 MFMER | slide-12
Masses in Cirrhotic liver: Approach• Hepatocellular? Gland forming? Both? Not sure?
Histology Hepatocyte markers
Glypican-3 Reticulin Others
Hepatocellular Maybe (high-grade tumors)
Maybe (high and low-grade tumors)
Maybe (low-grade tumors)
Not usually
Gland forming Not usually No No Sometimes
Both Yes Yes No Yes (CK7, CK19, MOC-31)
Not sure Yes Yes No Yes (CK7, CK19, others)
10
11
12

©2017 MFMER | slide-13
• Abnormal architecture: thickened trabecularcords
• Increased N:C ratio
• Nuclear atypia (interpret with caution)
• Increased arteries within the lesion
• Abundant pseudoacinar structures
Histologic features of HCC
Moderately differentiated hepatocellular carcinoma
Growth patterns in HCCMacrotrabecular pattern
Pseudoacinar pattern
Trabecular pattern
Solid pattern
13
14
15

©2017 MFMER | slide-16
Bile formation in a malignant tumor = HCC
• 68 yo cirrhotic male with a 2.5 cm lesion withwashout but no arterial enhancement.
Case 2:
Cirrhotic background
16
17
18

©2017 MFMER | slide-19
©2017 MFMER | slide-20
•Clearly hepatocellular
•Favor neoplastic (probably HCC)• Increased N:C ratio• Pseudoacinar structures• Nuclear atypia (least useful)• Arteriolization
•How to prove malignancy?
Case 2:
©2017 MFMER | slide-21
Marker HCC G1 HCC G2 HCC G3 Caveat
Reticulin (loss or thickened cords)
++(may be focal)
+++ +++Steatosis can distort reticulin, can be difficult to interpret
CD34+++
(sinusoidal expression)
+++(sinusoidal expression)
+++(sinusoidal expression)
May be positive in dysplastic nodules and adenomas
Glypican 3++
(62%)+++
(80%)+++
(85%)Positive in some AdenoCA and germ cell tumors
Glutamine synthetase(Diffuse)
++(60%)
N/A N/ADiffuse GS can be seen in some HCA, dysplastic nodules, AdenoCA
HSP70(nuclear)
++(60%)
N/A N/AHigh background, occasionally dysplasticnodules and AdenoCA
Modern Pathology (2016) 29, 283–292
Markers of hepatocellular malignancy
19
20
21

HSP70 Glypican-3
CD34Glutamine synthetase
Reticulin: Thickened cords, fragmentation
Normal reticulin
©2017 MFMER | slide-24
• 68 yo cirrhotic male with a 2.5 cm lesion withwashout but no arterial enhancement.
• Diagnosis: Well-differentiated hepatocellularcarcinoma (based on reticulin stain)
Case 2:
22
23
24

©2017 MFMER | slide-25
Mild steatosis Moderate steatosis Severe steatosis
©2017 MFMER | slide-26
*
*
* Non-Cirrhotic liver
Morphologic variants of HCC
Gastroenterol Clin North Am. 2017 Jun;46(2):365-391.
Steatohepatitic HCC• Occurs mainly in patients with underlying NASH• 50% of tumor must have steatohepatitic features• No affect on prognosis.
Clear cell HCC• Clear cells filled
with glycogen• Better prognosis
25
26
27

©2017 MFMER | slide-28
Cirrhotic-like HCC• Difficult to identify
grossly and radiologically
• HCC grows in a small nodular pattern
©2017 MFMER | slide-30
• 65 yo cirrhotic male with an atypical liver mass during HCC screening.
Case 3:
28
29
30

Cholangiocarcinoma
HCC area? Solid cholangio?
©2017 MFMER | slide-32
• Hepatocellular? Gland forming? Both? Not sure?Histology Hepatocyte
markersGlypican-3 Reticulin Others
Hepatocellular Maybe (high-grade tumors)
Maybe (high and low-grade tumors)
Maybe (low-grade tumors)
Not usually
Gland forming Not usually No No Sometimes
Both Yes Yes No Yes (CK7, CK19, MOC-31)
Not sure Yes Yes No Yes (CK7, CK19, others)
Masses in Cirrhotic liver: Approach
©2017 MFMER | slide-33
Marker HCC G1 HCC G2 HCC G3 Caveat
Hep-par1 (HSA)+++
(100%)+++
(98%)++
(64%)Positive in some
AdenoCA
Arginase-1+++
(100%)+++
(100%)+++
(97%)Positive in some
AdenoCA
CD10 or pCEA+++
(canalicular)(92%)
+++(canalicular)
(88%)
+(canalicular)
(54%)
Membranous and cytoplasmic reactivity
in many tumors
BSEP+++
(canalicular)(92%)
+++(canalicular)
(95%)
+(canalicular)
(45%)Not well characterized
Arch Pathol Lab Med. 2015;139:1028–1034;
Markers of Hepatocyte differentiation
31
32
33

©2017 MFMER | slide-34
Marker HCC Cholangiocarcinoma
CK7 +/- +++
CK19 +/- +++
Hep-Par1/HSA +++ -
Arginase1 ++++ -
pCEA or CD10 Canalicular Variable but no canalicular
Glypican-3 ++ +/-
MOC-31 - ++
HCC versus Cholangiocarcinoma
©2017 MFMER | slide-35
CK7: Hepatoid area CK7: Cholangio area
CD10: Normal liver
CD10
Hep-par1/HSA Arginase1
34
35
36

Glypican-3: Hepatoid area
Glypican-3: Cholangio area
©2017 MFMER | slide-38
• 65 yo cirrhotic male with an atypical liver mass duringHCC screening.
• Diagnosis: Combined hepatocellular carcinoma andcholangiocarcinoma (cHCC-CCA)
Case 3:
©2017 MFMER | slide-39
• Combined HCC/Cholangiocarcinoma (cHCC-CCA)• Primary liver cancer with distinct HCC and CCA components• Must occurring within the same tumor nodule.• H&E based diagnosis with IHC support; no cutoff %• Higher frequency after transarterial chemoembolization
• Intermediate cell carcinoma• Primary liver cancer containing intermediate cells only• H&E and IHC based diagnosis (very rare)
• Other variants such as combined HCC/Cholangiocarcinoma with stem cell features and cholangiolocarcinoma are no longer recognized as distinct entities
• Cholangiolocarcinoma is recognized as a subtype of intrahepaticcholangiocarcinoma
Brunt et al. Hepatology. 2018
Combined HCC-cholangiocarcinomacHCC-CCA
37
38
39

©2017 MFMER | slide-40
• Hepatocellular? Gland forming? Both? Not sure?
Histology Hepatocyte markers
Glypican-3 Reticulin Others
Hepatocellular Maybe (high-grade tumors)
Maybe (high and low-grade tumors)
Maybe (low-grade tumors)
Not usually
Gland forming Not usually No No Yes (CK7 mainly)
Both Yes Yes No Yes (CK7, CK19, MOC-31)
Not sure Yes Yes No Yes (CK7, CK19, others)
Masses in Cirrhotic liver: Approach
©2017 MFMER | slide-41
• Hepatoid/heptocellular? Gland forming? Can’t tell?
Histology Hepatocyte markers
Glypican-3 Cytokeratins Other markers
Hepatoid/hepatocellular Yes Yes (interpret with caution)
Maybe No (but depends on history)
Gland forming No No Yes (CK7, CK20) Yes: Usually CDX2, SATB2, TTF1 (others depend on history)
Can’t tell Yes Maybe Yes (Cam5.2, CK7, others)
Not yet, unstainedslides, do IHC in phases
Malignant masses in Non-cirrhotic liver
©2017 MFMER | slide-42
• 53 yo female with a liver mass. Liver is non-cirrhotic
Case 4:
40
41
42

©2017 MFMER | slide-43
• Hepatoid/hepatocellular? Gland forming? Can’t tell?Histology Hepatocyte
markersGlypican-3 Cytokeratins Other markers
Hepatoid/ hepatocellular
Yes Yes (interpret with caution)
Maybe No (but depends on history)
Gland forming No No Yes (CK7, CK20) Yes: Usually CDX2, SATB2, TTF1 (others depend on history)
Can’t tell Yes Maybe Yes (Cam5.2, CK7, others)
Not yet, unstainedslides, do IHC in phases
Malignant masses in Non-cirrhotic liver
©2017 MFMER | slide-44
CK7 Hep-par1
Glypican-3 Arginase-1
©2017 MFMER | slide-45
• Cholangiocarcinoma?
• Metastatic hepatoid carcinoma?
• Combined HCC-cholangiocarcinoma?
• Variant of hepatocellular carcinoma?
Diagnosis?
43
44
45

©2017 MFMER | slide-46
Mod Pathol. 2013 Jun;26(6):782-91.
Scirrhous Hepatocellular Carcinoma
CK7 CD68
Fibrolamellar Carcinoma(DNAJB1-PRKACA Fusion)
Normal liver
Abnormal
Case 5: 40 yo female with a liver mass
46
47
48

Features• Sinusoidal dilatation• Portal tract-like structures
with inflammation, multiple arteries and rare bile ductules (no true bile ducts)
• No fibrous bands or larger arteries
©2017 MFMER | slide-50
Reticulin: Normal trabecular thickness
©2017 MFMER | slide-51
Differential Fibrous bands with large arteries
Isolated “naked” small arteries
Bile ductules
Trabecular thickness
Well-differentiated Hepatocellular carcinoma
Not usually Yes No Abnormal
Hepatocellularadenoma
No Yes Sometimes Normal
Focal nodular hyperplasia
Yes Rarely Yes Normal
Low-grade” hepatocellular masses in Non-cirrhotic liver
49
50
51

©2017 MFMER | slide-52
• Increasing incidence since widespread use of oralcontraceptives
• Other risk factors: anabolic steroids, glycogen storagedisease, FAP, MODY3
• F>>>M
• Low-risk of malignant transformation
• Symptoms: pain, bleed, infarct, rupture
• Treatment: Avoid OCP and pregnancy; surgery
Hepatocellular adenomas (HCA)
©2017 MFMER | slide-53
• Morphologic and molecular subtypes• HNF1a mutated HCA
• Biallelic mutations in HNF1A (90% somatic, 10% germline)
• Inflammatory HCA• Constitutive activation of Stat3 due to mutations in pro-inflammatory
pathways• May also develop CTNNB1 mutations and progress to HCC
• b-catenin mutated HCA• 3 different mutation types occur in CTNNB1 (weakly active, mod active, and
highly active)• High risk of malignant transformation to HCC
• HCA-unclassified
Hepatocellular adenomas (HCA)
©2017 MFMER | slide-54
HNF1α mutated HCA
InflammatoryHCA
β-catenin mutated HCA
Unclassified HCA
β-catenin mutated Inflammatory HCA
~35%
~40%
~15%
~10%
Hepatocellular adenomas (HCA): Subtypes
52
53
54

©2017 MFMER | slide-55
Hepatocellular adenomas: subtypesSubtype Histologic features LFABP CRP/SAA Glutamine
Synthetaseβ-catenin
H-HCA • Steatosis Loss Patchy Perivenular Membranous
IHCA • Inflamed portal-tractlike structures with arteries
• Ductular reaction• Sinusoidal dilatation
Retained Diffuselypositive
Perivenular Membranous
β-IHCA • Inflamed portal-tractlike structures with arteries
• Ductular reaction• Sinusoidal dilatation
Retained Diffuselypositive
Diffuse or “Starry sky”
Rare positive nuclei, may be membranous
β-HCA • Atypia Retained Patchy Diffuse or “starry sky”
Rare positive nuclei
U-HCA • Variable Retained Patchy Perivenular Membranous
Features• Sinusoidal dilatation• Portal tract-like
structures with inflammation, multiplearteries and rare bileductules (no true bile ducts)
• No fibrous bands orlarger arteries
Favor inflammatory HCA
C-reactive protein
LFABP
Glutamine synthetase
Beta-catenin
55
56
57

©2017 MFMER | slide-58
• 40 yo female with a liver mass
• Diagnosis: Inflammatory hepatocellular adenoma (nofeatures suggestive of beta-catenin mutation)
Case 5:
©2017 MFMER | slide-59
Does classification matter?
• Subtypes have different risk of malignant degeneration (β-HCA and β-IHCA) and associations.
• But…… classification hasn’t changed treatment guidelines
• Treatment algorithm:• Resect > 5cm to prevent bleeding and malignancy• Resect “adenomas” in men• Resect those growing after withdrawal of oral
contraceptives
©2017 MFMER | slide-60
58
59
60

Case 6: 28 yo female with multiple liver nodules
©2017 MFMER | slide-62
©2017 MFMER | slide-63
CRP Glutamine synthetase
Beta catenin LFABP
Inflammatory HCA
61
62
63

©2017 MFMER | slide-65
©2017 MFMER | slide-66
CRP Glutamine synthetase
Beta catenin LFABP
HNF1α inactivated HCA
64
65
66

HNF1α inactivated HCA Inflammatory HCA
©2017 MFMER | slide-68
• Multiple HCAs – usually greater than 10 visualized by MRI• May have many micro-nodules (usually identified by
IHC)
• Any subtype may occur but usually H-HCA and IHCA
• Risk of malignant transformation depends on HCA subtype
• When innumerable, liver transplantation may beconsidered
Hepatic adenomatosis
• 53 year old non-cirrhotic male with a liver mass
Case 7:
67
68
69

©2017 MFMER | slide-71
Mostly preserved?Focal fragmentation
©2017 MFMER | slide-72
Glutamine synthetase Glypican-3
HSP-70Beta-Catenin
70
71
72

©2017 MFMER | slide-73
• 53 year old non-cirrhotic male with a liver mass.
• Diagnosis?• Beta-catenin mutated HCA in a male?• Well differentiated hepatocellular neoplasm of uncertain
malignant potential/Atypical hepatocellular neoplasm?• Well-differentiated HCC?
Case 7:
©2017 MFMER | slide-74
• Well differentiated hepatocellular neoplasm of uncertain malignantpotential/Atypical hepatocellular neoplasm
• On resection: try to classify definitively as either HCA or HCC
Hum Pathol. 2014 Mar;45(3):658-60.
Case 7:
Case 7: Resection – Well-diff HCC
73
74
75

©2017 MFMER | slide-76
• 60 yo male with a history of colorectal carcinoma with 5liver lesions
Case 8:
76
77
78

©2017 MFMER | slide-80
CK7: Highlights ductules
79
80
81

©2017 MFMER | slide-82
Differential Fibrous bands with large arteries
Isolated “naked” small arteries
Bile ductules
Trabecular thickness
Well-differentiated Hepatocellular carcinoma
Not usually Yes No Abnormal
Hepatocellularadenoma
No Yes Sometimes Normal
Focal nodular hyperplasia
Yes Rarely Yes Normal
Low-grade” hepatocellular masses in Non-cirrhotic liver
©2017 MFMER | slide-83
Modern Pathology (2014) 27, 62–72
FNH versus Inflammatory HCA
©2017 MFMER | slide-84
Liver international. 2009.
Glutamine synthetase in FNH
82
83
84

©2017 MFMER | slide-85
Pseudo map-like Map-like
FNH versus Inflammatory HCA
Glutamine synthetase
©2017 MFMER | slide-87
Glutamine synthetase: Geographic/map-like pattern
85
86
87
©2017 MFMER | slide-88
• 60 yo male with a history of colorectal carcinoma with 5liver lesions
• Diagnosis: Focal nodular hyperplasia
Case 8
©2017 MFMER | slide-89
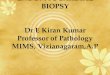
• FNH nodules are thought to develop as localized overgrowth ofliver parenchyma resulting from an anomalous arterial branch.
• Cavernous hemangiomas occur in a significant % of patients with FNH
• Usually > 5cm, those < 3cm may not have a central scar
• OCS may promote growth
• Rarely cause symptoms
• Manage conservatively and only resect the rare symptomatic FNH or a lesion where the imaging is not typical
Focal nodular hyperplasia
©2017 MFMER | slide-90
88
89
90

©2017 MFMER | slide-91
• Cirrhotics versus non-cirrhotics
• Malignant tumor in the liver• How to approach these biopsies and confirm or exclude HCC• Subtypes of HCC and mixed tumors• Well-differentiated HCC
• Recognize and correctly classify benign lesions• Recognize lesional tissue• Hepatocellular adenoma• Focal nodular hyperplasia
Liver mass biopsies: Diagnostic issues
©2017 MFMER | slide-92
Questions & Discussion
91
92