Embed Size (px)
Citation preview

RIPC for multiorgan salvage in clinical settings: Evolution of concept,evidences and mechanisms
Puneet Kaur Randhawa, Anjana Bali, Amteshwar Singh Jaggi nQ1
Department of Pharmaceutical Sciences and Drug Research, Punjabi University, Patiala 147002, India
a r t i c l e i n f o
Article history:Received 2 June 2014Received in revised form12 August 2014Accepted 18 August 2014
Keywords:Remote ischemic preconditioningHeartKidneyHypoxia inducible factorInflammation
a b s t r a c t
Ischemic preconditioning is an intrinsic process in which preconditioning ischemia (ischemia of shorterduration) protects the organs against the subsequent index ischemia (sustained ischemia). Remoteischemic preconditioning (RIPC) is an innovative treatment approach in which interspersed cycles ofpreconditioning ischemia followed by reperfusion to a remote organ (other than target organ) protectthe target organ against index ischemia and reperfusion-induced injury. RIPC of various organs toprovide multi-organ salvage became a successful approach in numerous species of animals. Conse-quently, the concept of RIPC evolved in clinical setups, and provided beneficial effects in alleviatingischemia-reperfusion-induced injury in various remote organs, including myocardium. Clinically, RIPCstimulus is generally delivered by inflating the blood pressure cuff tied on the upper arm 20 mm greaterthan the systolic blood pressure, rendering the forearm ischemic for 5 min, followed 5 min reperfusionby deflating the cuff. This cycle is repeated for 3–4 consecutive periods to precondition the tissue andimprove the survival. The institution of RIPC is beneficial in mitigating myocardial injury in patientsundergoing various surgical interventions including coronary artery bypass graft surgery, abdominalaortic aneurysm repair, percutaneous coronary intervention, heart valve surgery, drug-eluting stentimplantation, kidney transplantation, elective decompression surgery. The involvement of hypoxiainducible factor-1α (HIF-1α), ATP-sensitive potassium channels, signal transducer and activator oftranscription (STAT), matrix metalloproteinases, O-linked β-N-acetylglucosamine (O-GlcNAc) levels,autonomous nervous system in mediating RIPC-induced cardioprotective effects has been exploredclinically. However, comprehensive studies are required to elucidate the other possible mechanismsresponsible for producing multi-organ protection during RIPC.
& 2014 Elsevier B.V. All rights reserved.
Contents
1. Introduction . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22. Evolution of concept . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 23. Clinical evidences of beneficial effects of RIPC in surgical interventions in different organs: . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 4
3.1. Myocardial injury . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 43.2. Neuronal injury . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 53.3. Renal injury . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 63.4. Intestinal and pulmonary injury . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 6
4. Possible mechanisms for beneficial effects of RIPC . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 74.1. Hypoxia Inducible factor-1α . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 74.2. ATP-sensitive potassium channels (KATP channels) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 74.3. Matrix metalloproteinases. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 94.4. O-linked β-N-acetylglucosamine (O-GlcNAc) . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 104.5. Signal transducer and activator of transcription (STAT). . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 104.6. Autonomous nervous system . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 114.7. Inflammatory gene expression . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 11
123456789
101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960616263646566
Contents lists available at ScienceDirect
journal homepage: www.elsevier.com/locate/ejphar
European Journal of Pharmacology
http://dx.doi.org/10.1016/j.ejphar.2014.08.0160014-2999/& 2014 Elsevier B.V. All rights reserved.
n Corresponding author. Mobile: þ91 9501016036.E-mail address: [email protected] (A. Singh Jaggi).
Please cite this article as: Kaur Randhawa, P., et al., RIPC for multiorgan salvage in clinical settings: Evolution of concept, evidencesand mechanisms. Eur J Pharmacol (2014), http://dx.doi.org/10.1016/j.ejphar.2014.08.016i
European Journal of Pharmacology ∎ (∎∎∎∎) ∎∎∎–∎∎∎

4.7.1. Decrease in cytokines, apoptosis and related inflammatory processes . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 114.7.2. Increase in neutrophil infiltration . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 124.7.3. Increase in cytokine expression . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 124.7.4. Bradykinin . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 124.7.5. Possible reasons for contradictory reports and recommendations for future research . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12
5. Conclusion . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 12Uncited references . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13Acknowledgments . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13References . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 13
1. Introduction
Ischemia is a vascular disease that is characterized by restric-tion in blood supply, causing shortage of oxygen and vitalnutrients, thus hampering normal cellular metabolism. Establish-ment of circulation is necessary to resuscitate the tissues andeventually, protect them from cell death after transient absence ofoxygen and nutrients in the blood. Prolonged occurrence ofischemia and thereafter, reperfusion results in ischemia-reperfusion-induced injury as a result of release of oxygen freeradicals, cytokines and increase in the expression of adhesionmolecules (Kukielka et al., 1993; Welbourn et al., 1991). Intrao-perative ischemia-reperfusion-induced injury is one of the funda-mental causes in the perpetuation of transitory and delayed organdysfunction (Błogowski et al., 2012; Xie et al., 2012). Therefore, forthe sake of providing protection to the organs against ischemia-reperfusion injury, development of a novel therapeutic approach isthe need of the hour.
RIPC is a treatment strategy in which alternate cycles ofpreconditioning ischemia followed by reperfusion are deliveredto a remote organ (other than heart) which protects the heartagainst subsequent index ischemia (sustained ischemia) andreperfusion induced injury (Gho et al., 1996; Przyklenk, 2013).PrecQ3 linically, short episodes of occlusion and reperfusion of thearteries such as cerebral, mesenteric, intestinal (Wang et al., 2008),renQ4 al (Diwan et al., 2008a, 2008b; Kant et al., 2008), abdominalaorta (Taliyan et al., 2010), skeletal muscle (Liem et al., 2003)produce preconditioning of myocardium against sustained ische-mia and reperfusion in various animals like mice, rats etc. How-ever, these approaches may not be directly translated in clinicalsettings. In clinical setups, the best utilized way for providingmyocardial protection is rendering the forelimb (skeletal muscle)ischemic by applying blood pressure cuff on the upper arm. This isadvantageous as it is a non-invasive and clinically feasible techni-que except for surgical procedures. Furthermore, upper limb ismore resistant to ischemic insult as even a mild ischemia to vitalorgans can result in non-reversible cellular injury.
In clinical setup, RIPC is generally initiated by inflating bloodpressure cuff tied on the upper arm 20 mm Hg greater thansystolic arterial pressure, rendering the forearm ischemic for5 min followed by 5 min intermittent reperfusion. This cycle maybe repeated for three to four consecutive periods (Cheung et al.,2006; D'Ascenzo et al., 2014; Karuppasamy et al., 2011). However,different scientists have made modifications in the protocol toinduce ischemia-reperfusion injury of varying degrees. The con-cept of RIPC came into existence in clinical settings when Cheunget al. subjected 17 children with congenital heart defects to RIPCand this treatment strategy significantly attenuated troponinlevels (a chief indicator of myocardial injury) (Cheung et al.,2006). Furthermore, studies conducted by other researchers havereported reduction in neuroQ5 nal (Gonzalez et al., 2013; Hu et al.,2010), kidney (Er et al., 2013; Walsh et al., 2009; Wu et al., 2013),intestinal and pulmonary injury (Li et al., 2013) in individuals after
being subjected to RIPC stimulus (Table 1). RIPC stimulus has alsoimproved the initial distance covered in patients with complaintsof intermittent claudication (pain in legs during walking) in thelower limbs (Saes et al., 2013).
The involvement of hypoxia inducible factor-1α (HIF-1α)(Albrecht et al., 2013), ATP-sensitive potassium channels, (KATP
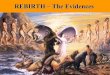
channels) (Loukogeorgakis et al., 2007), signal transducer andactivator of transcription (STAT) (Heusch et al., 2012), matrixmetalloproteinases (MMPs) (Zitta et al., 2012), O-linked β-N-acetylglucosamine (O-GlcNAc) levels (Jensen et al., 2013), auton-omous nervous system (ANS) (Loukogeorgakis et al., 2005) inmediating RIPC-induced cardioprotective effects have beenexplored clinically (Fig. 1). The present review describes theevidences and possible mechanisms of RIPC-induced multiorgansalvage from ischemia-reperfusion injury in clinical settings.
2. Evolution of concept
Ischemic preconditioning is a therapeutic strategy brought intonotice in 1986 by Murry, Jennings and Reimer in order to alleviateischemia-reperfusion-induced injury (Murry et al., 1986). Murry etal. demonstrated that short ischemic episodes to an organ (in theform of ischemic preconditioning) afford protection against sus-tained ischemia and reperfusion injury (Murry et al., 1986). Thisconcept has been expanded to include pharmacological precondi-tioning (Khanna et al., 2008). Remote preconditioning stimulus(repeated cycles of non-lethal ischemia and reperfusion to adistant tissue) can be delivered before, during or after lethalsustained ischemia for RIPC (RIPC) (Kant et al., 2008), remoteischemic perconditioning (Czigany et al., 2013) or remote ischemicpost-conditioning (RIPostC) (Crimi et al., 2013; Heusch, 2013)respectively. Our own laboratory has demonstrated cardioprotec-tive effects of remote renal preconditioning in rats RIPC (Diwan etal., 2008a, 2008b; Kant et al., 2008). The concept of intra-cardiacpreconditioning came into limelight when Przyklenk et al. demon-strated that 4 cycles of 5 min occlusion and reperfusion of the leftcircumflex artery led to a reduction in infarct size followingsustained occlusion of left anterior descending coronary artery(Przyklenk et al., 1993). This finding led to the emanation of RIPC,which has been explored in numerous species of animals in orderto provide multiorgan salvage. Similarly, preclinical studies havebeen conducted to evaluate the potential of RIPostC and remoteperconditioning to alleviate ischemia-reperfusion-induced injury.In clinical settings, RIPostC has provided benefits in attenuatingischemia-reperfusion-induced injury in adults and children under-going percutaneous coronary intervention/heart surgery (Crimi etal., 2013; Zhong et al., 2013). Likewise, remote ischemic percondi-tioning is another treatment approach which has led to significantreduction in myocardial injury in patients undergoing valvereplacement (Li et al., 2010). However, remote ischemic percondi-tioning treatment strategy has not been translated extensively intoclinical set-ups for reducing ischemia-reperfusion-induced injury.
123456789
101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960616263646566
P. Kaur Randhawa et al. / European Journal of Pharmacology ∎ (∎∎∎∎) ∎∎∎–∎∎∎2
Please cite this article as: Kaur Randhawa, P., et al., RIPC for multiorgan salvage in clinical settings: Evolution of concept, evidencesand mechanisms. Eur J Pharmacol (2014), http://dx.doi.org/10.1016/j.ejphar.2014.08.016i

123456789
101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960616263646566
Table 1Clinical evidences and role of RIPC in attenuating multiorgan injury.
S.no.
RIPC protocol Groupsize
Primary outcomeparameter
Clinical applications References
1. � 4 alternate cycles of ischemia (5 min) and reperfusion(5 min) by inflating (20 mm Hg greater than systolic B.P.)and deflating (releasing the valve) the blood pressure bloodpressure cuff tied on the upper arm
166 Increase in myocardialsalvage index
Percutaneous coronary intervention Bøtker et al.(2010)
� 3 alternate cycles of ischemia (5 min) and reperfusion(5 min) by inflating (upto 200 mm Hg) and deflating(releasing the valve) the blood pressure cuff tied on theupper arm
44 cTnI release Hoole et al.(2009a, 2009b)
2. � 2 cycles of sequential cross clamping of right and left iliacvessel for 10 min
41 cTnI, creatinine level Abdominal aortic aneurysm repair Ali et al. (2007)
� 2 cycles of lower limb ischemia an reperfusion (each10 min)
18 urinary retinol bindingprotein, albumin/creatinine
Walsh et al.(2009)
� 3 alternate cycles of ischemia (5 min) and reperfusion(5 min) by inflating and deflating (releasing the valve) theblood pressure cuff tied on the upper arm
62 arterial-alveolar oxygentension ratio
Li et al. (2013)
3. � 3 alternate cycles of ischemia (5 min) and reperfusion(5 min) by inflating (20 mm Hg greater than systolic B.P.)and deflating (releasing the valve) the blood pressure cufftied on the upper arm
50; 12 CK-MB; TnI concentration Coronary artery bypass graft (CABG)surgery: blunted myocardial and renalinjury
Ali et al. (2010),Heusch et al.(2012)
� 3 alternate cycles of ischemia (5 min) and reperfusion(5 min) by inflating (upto 200 mm Hg) and deflating(releasing the valve) the blood pressure cuff tied on theupper arm
27; 27 TnT release Hausenloy et al.(2007),Thielmann et al.(2010)
4. � 3 alternate cycles of ischemia (5 min) and reperfusion(5 min) by inflating (20 mm Hg greater than systolic B.P.)and deflating (releasing the valve) the blood pressure cufftied on the upper arm
38 cTnI levels Heart valve surgery Xie et al. (2012)
5. � 4 alternate cycles of ischemia (5 min) and reperfusion(5 min) by inflating (20 mm Hg greater than systolic B.P.)and deflating (releasing the valve) the blood pressure cufftied on the upper arm
17 cTnI levels Tetralogy of Fallot, aortic regurgitation,ventricular and atrial septal defects,transposition of the great arteries
Cheung et al.(2006)
6. � 4 alternate cycles of ischemia (5 min) and reperfusion(5 min) by inflating (50 mm Hg greater than systolic B.P.)and deflating (releasing the valve) the blood pressure cufftied on the upper arm
50 serum creatinine,glomerular filtration
Elective coronary angiography Er et al. (2013)
7. � 4 alternate cycles of ischemia (5 min) and reperfusion(5 min) by inflating (upto 200 mm Hg) and deflating(releasing the valve) the blood pressure cuff tied on thelower limb before and after anastomoses (RIPCþRPostC)
35 cTnI levels Off-pump coronary artery bypass graftsurgery
Hong et al.(2012)
8. � 3 alternate cycles of ischemia (5 min) and reperfusion(5 min) by inflating (upto 200 mm Hg) and deflating(releasing the valve) the blood pressure cuff tied on theupper arm
101 cTnI release Elective coronary stent implantation Luo et al. (2013)
9. � 3 alternate cycles of ischemia (5 min) and reperfusion(5 min) by clamping and declamping the exposed externaliliac artery
24 creatinine level, urineneutrophil gelatinaseassociated lipocalin, eGFR
Kidney transplantation Wu et al. (2013)
10. � 3 alternate cycles of ischemia (5 min) and reperfusion(5 min) by inflating (upto 200 mm Hg) and deflating(releasing the valve) the blood pressure cuff tied on theupper arm before every hemodialysis session
17 cTnI release Hemodialysis Park et al. (2013)
11. � 3 alternate cycles of ischemia (5 min) and reperfusion(5 min) by inflating (20 mm Hg greater than systolic B.P.)and deflating (releasing the valve) the blood pressure cufftied on the upper arm
20 S-100B release, neuron-specific enolase release
Elective decompression surgery Hu et al. (2013)
P. Kaur Randhawa et al. / European Journal of Pharmacology ∎ (∎∎∎∎) ∎∎∎–∎∎∎ 3
Please cite this article as: Kaur Randhawa, P., et al., RIPC for multiorgan salvage in clinical settings: Evolution of concept, evidencesand mechanisms. Eur J Pharmacol (2014), http://dx.doi.org/10.1016/j.ejphar.2014.08.016i

3. Clinical evidences of beneficial effects of RIPC in surgicalinterventions in different organs:
3.1. Myocardial injury
Myocardial injury is a common drawback encountered duringvarious cardiac surgeries employing cardiopulmonary bypass thattakes over the function of the heart and lungs during surgery inorder to maintain circulation of blood. Degree of myocardial injuryis assessed by making measurements of cardiac markers thatreveal the functional status of the heart. The widely used specificand sensitive biomarkers for evaluating heart function includecardiac troponin and creatinine kinase levels. Cardiac troponin I(cTnI) and T (cTnT) are components of the contractile machinery ofcardiac cells and are expressed extensively in heart. RIPC has beenwidely used to alleviate myocardial injury after carrying outvarious surgical interventions. The usage of RIPC for attenuatingmyocardial injury in clinical setups began when Cheung et al.conducted a randomized, controlled trial that involved recruit-ment of thirty seven children with congenital heart defects,including ventricular and atrial septal defects, aortic regurgitation,tetralogy of Fallot, and transposition of the great arteries. RIPCtreatment in seventeen children led to decrease in levels of cTnIpostoperatively and also decreased inotropic requirement, sug-gesting reduced myocardial injury and lesser degree of myocardialdysfunction (Cheung et al., 2006).
Ali et al. conducted a randomized double blind study on 82patients undergoing abdominal aortic aneurysm repair. Sequentialcross clamping of the right and left iliac vessel for 10 min eachfollowed by intermittent reperfusion for 10 min (providing lowerlimb ischemia of 20 min) served as RIPC stimulus in forty onepatients. RIPC reduced the absolute risk of myocardial injury by27% (23% in patients with previous MI) and myocardial infarctionby 22% (18% in patients with previous MI) in terms of cTnI levels.Additionally, mean cTnI area under the curve was significantlylower in the remote preconditioned patients (Ali et al., 2007).The same group of scientists revealed that RIPC treatment strategyalleviated creatine kinase (CK-MB) levels in 50 patients withdouble and triple vessel coronary artery disease undergoingcoronary artery bypass graft (CABG) surgery. The decline in CK-MB levels at 8, 16, 24 and 48 h, post-surgery indicated that RIPCled to reduction of myocardial injury (Ali et al., 2010).
RIPC has also been shown to decrease postsurgery cTnI releasein forty four patients undergoing elective percutaneous coronaryinterv Q6ention (Hoole et al., 2009a, 2009b). A single center rando-mized controlled trial organized by Botker et al. evaluated thatremote conditioning enhanced myocardial salvage in 166 adultpatients with suspected acute myocardial infarction, receivingpercutaneous coronary intervention. Remote conditioning wasprovided while the patients were being transported to the hospi-tal, but primary percutaneous coronary intervention took place inthe hospital. Increase in the myocardial salvage index after remoteconditioning (30 days after primary percutaneous coronary inter-vention) was the primary endpoint. Myocardial perfusion imagingwas used to measure the proportion of the area at risk salvaged byremote conditioning. However, no significant improvement insecondary end points which included final infarct size, leftventricular ejection fraction (after 30 days), cTnT release (after90–102 h), corrected TIMI (Thrombolysis in Myocardial Infarction)frame count, ST-segment resolution (after 90 min) were reported.Likewise, no improvement in major adverse coronary coronaryevents including re-infarction, heart failure and death wasreported within and 30 days after receiving percutaneous coron-ary Q7intervention (Bøtker et al., 2010).
RIPC treatment has been shown to significantly attenuatemyocardial injury in terms of decreased serum TnT release at 6,12, 24, 48, 72 h post-surgery in 27 patients who underwent electivecoronary artery bypass graft surgery (Hausenloy et al., 2007).Likewise, a meta-analysis revealed that RIPC reduces the releaseof TnI or TnT in 704 patients (9 studies) undergoing coronary arterybypass graft (CABG) surgery (D'Ascenzo et al., 2012). Same group ofscientists conducted another meta-analysis (five studies with 731patients) and reported that RIPC reduces the chances of peri-procedural myocardial infarction with more benefits especiallywhen RIPC stimulus is delivered on the lower limb (D'Ascenzo etal., 2014). It has been reported by Alreja et al. on pooling data from17 clinical trials that RIPC exerts favorable effects in patientsundergoing cardiovascular interventions in terms of reduction inserological markers of myocardial injury (cTnT/cTnI and CK-MB).Moreover, a lower incidence of perioperative myocardial infarctionin patients undergoing surgery has been documented (Alreja et al.,2012). Hong et al. evaluated the rationale of combining RIPC withremote ischemic postconditioning (RIPostC) in thirty five patients(total patients¼70) undergoing off-pump coronary artery bypass
123456789
101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960616263646566
Upper limb
ISCHEMIA REMOTE PRECONDITIONING
HIFKATP Opening STAT-5 P O-GlcNAc MMPs
Kidney Lower limbIntestineHeart
Calcium eNOS ApoptosisAkt
MULTI ORGAN PROTECTION
InflammationP
Brain
Fig. 1. Representation of RIPC-induced multi-organ protection and possible mechanisms.
P. Kaur Randhawa et al. / European Journal of Pharmacology ∎ (∎∎∎∎) ∎∎∎–∎∎∎4
Please cite this article as: Kaur Randhawa, P., et al., RIPC for multiorgan salvage in clinical settings: Evolution of concept, evidencesand mechanisms. Eur J Pharmacol (2014), http://dx.doi.org/10.1016/j.ejphar.2014.08.016i

graft surgery (OPCAB). 4 cycles of 5-min ischemia and 5-minreperfusion RIPCþRIPostC, given to the lower limb before anasto-moses (RIPC) and after anastomoses (RIPostC) reduced postopera-tive serum troponin I levels. It was seen that RIPCþRIPostC bylower limb ischemia decreased postoperative myocardial enzymeelevation by almost half postoperatively, in patients undergoing off-pump coronary artery bypass graft surgery (Hong et al., 2012).Twelve patients undergoing coronary artery bypass surgery con-firmed protection against ischemia-reperfusion injury depicted byreduced serum troponin I concentrations (Heusch et al., 2012). RIPCstimulus in 38 adult patients (31–72 years) undergoing mitral valve,aortic valve or tricuspid valve surgery resulted in improvement inpostsurgical cardiac function. As cTnI concentration was reducedafter RIPC, this indicated that RIPC reduces myocardial injury andimproves cardiac function in patients undergoing heart valvesurgery (Xie et al., 2012). Another recent report has described thatRIPC significantly attenuates serum cTnI levels in 18 patientsundergoing cardiac surgery with cardiopulmonary bypass (Zitta etal., 2014). Furthermore, on pooling data from 25 randomizedcontrol trials (16 cardiac; 6 renal; 3 pulmonary), it was found thatRIPC provided significant cardiac protection, but no renal/pulmon-ary protection in patients undergoing cardiopulmonary bypasssurgery (Haji et al., 2014).
RIPC stimulus caused a reduction in the incidence of post-procedural cTnI release after elective percutaneous coronaryintervention (PCI) and provided not only short term, but also longterm benefits. It was seen that RIPC stimulus reduced majoradverse cardiac and cerebral events (MACCE) at 6 months in 110patients and for 6 yrs in 95 patients (Davies et al., 2013). Further,RIPC stimulus preceding PCI significantly improved endothelialfunction (assessed by flow-mediated dilation test) in patients withacute myocardial infarction (Manchurov et al., 2014). In addition,Zografos and co-workers have demonstrated that even single cycleof RIPC stimulus immediately before ad hoc PCI (coronary angio-plasty and PCI in the same procedure) alleviated periproceduralcTnI release and PCI-related myocardial infarction (Zografos et al.,2014). RIPC exerted protective effect in hemodialysis-(HD) inducedmyocardial injury in seventeen chronic hemodialysis patients.cTnT levels, an index of myocardial injury tended to decrease fromday 2 in the RIPC group till day 28 after RIPC treatment, indicatinga protective effect against hemodialysis-induced ischemia (Park etal., 2014). By the same token, RIPC treatment exerted cardiopro-tective effect in 101 patients undergoing drug-eluting stentimplantation. cTnI release and myocardial infarction was signifi-cantly reduced at 16 h after elective coronary stent implantation inpatients subjected to RIPC stimulus (Luo et al., 2013). Thielmann etal. published that RIPC stimulus led to myocardial protection in121 patients undergoing elective coronary artery bypass graftsurgery in a single centered, double blind study. RIPC treatmentled to a reduction in serum cTnI concentrations, depicted frommean cTnI area under the curve in the first 72 h after coronaryartery bypass graft surgery. RIPC also exerted long term protectiveeffects as it curtailed the chances of all cause mortality (mainsafety end point), major adverse cardiac or cerebrovascular eventsand repeat re-vascularization after coronary artery bypass graftsurgery (Thielmann et al., 2013).
On the contrary, there are a few reports which negate the role ofRIPC in inducing cardiac protection. It has been reported that RIPCdid not produce protection against myocardial injury in 65 patientsundergoing off pump coronary artery bypass graft surgery as reduc-tion in the troponin levels was not significant (Hong et al., 2010). Bythe same token, a single center, randomized, controlled studyconducted on patients undergoing human coronary artery bypasssurgery revealed that RIPC did not decrease serum cTnI level,creatinine level, urinary albumin–creatinine ratios, pO(2):FiO(2) (par-tial pressure of oxygen/fraction of inspired oxygen) (Rahman et al.,
2010). Furthermore, it has also been reported that late RIPC did notprovide clinically relevant cardioprotection to 12 children undergoingcardiopulmonary bypass in terms of concentrations of serologicalmarkers i.e. N-terminal pro-B-type natriuretic peptide and cardiactroponin I (Pavione et al., 2012). Also, RIPC stimulus delivered totwenty seven infants undergoing ventricular septal defect (VSD)repair with concomitant pulmonary hypertension did not improvemyocardial injury in terms of TnI release (Lee et al., 2012).
In another randomized, double blind controlled study RIPCstimulus given to 96 adults undergoing high risk surgery did notattenuate myocardial injury in terms of levels of high-sensitivitytroponin T (hsTNT). Moreover, it also did not reduce inotroperequirements in high-risk cardiac surgery patients (Young et al.,2012). Additionally, another report suggests that RIPC did notattenuate ischemic left ventricular dysfunction as contractility andejection fraction did not improve significantly in twenty patientswith single vessel coronary disease (Hoole et al., 2009). Besidesthis, it has been reported that RIPC improved haemodynamics, butdid not reduce myocardial injury in eighty patients undergoingcoronary artery bypass surgery 48 h, postsurgery in terms oftroponin I and creatine kinase-MB concentrations (Lomivorotovet al., 2012). Further, a meta analysis from 23 studies (15 cardiacsurgery; 4 percutaneous coronary intervention; 4 vascular sur-gery) with 1878 patients revealed that RIPC reduced the incidenceof peri-procedural myocardial infarctions, as well as the release oftroponin but did it not reduce major adverse cardiovascular eventsand mortality (Brevoord et al., 2012). It has been reported thatRIPC immediately percutaneous coronary intervention did notexert cardioprotective effect in patients (47) in terms of myone-crosis, high-sensitivity C-reactive protein (hsCRP), myocardialinfarction and mortality (Prasad et al., 2013).
3.2. Neuronal injury
Neuronal injury is usually assessed by measuring serum/cere-bro-spinal fluid concentration of enzymes like neuronal specificenolase (NSE) and S-100 B (Hardemark et al., 1989). Neuron specificenolase enzyme is exclusively expressed in mature neurons andcells of neuronal origin. Elevation in the levels of neuron specificenolase can be used to diagnose and predict certain cerebrovasculardiseases and their severity. Another protein, S-100 calcium bindingprotein B, belonging to S-100 family, is abundantly expressed onastrocytes, therefore, can be used to judge neuropathologicalconditions. Upsurge in levels of S-100 B in the serum is a sensitiveindicator for determining neuronal injury. RIPC has led to reduc-tions in neuronal injury in twenty adult cervical spondyloticmyelopathy patients undergoing elective decompression surgery.Neuron-specific enolase release of 6, 24, 72, and 120 h post-surgeryand S-100B release in serum at 6 h and 1 day after surgery(indicators of neuronal injury) was attenuated after carrying outRIPC (Hu et al., 2010). RIPC in patients with aneurysmal subarach-noid hemorrhage (SAH) led to a reduction of lactate/pyruvate (L/P)ratio as well as glycerol levels, which persisted for 25–54 h. More-over, intracranial pressure and transcranial doppler morphologicalclustering and analysis of intracranial pulse metrics suggested thatRIPC caused transient vasodilation (Gonzalez et al., 2013). It is wellknown that once anaerobic conditions prevail, pyruvate, which isthe substrate for oxidative phosphorylation cannot be utilized, itslevel increases and it is diverted to the formation of lactate. Fewstudies have found out that serum lactate/pyruvate is an excellentindicator of adequacy of cellular oxygenation. Arterial lactate/pyruvate ratio is a reflection of cytoplasmic and mitochondrialredox state (Levy et al., 2000; Kapoor et al., 2011). Abnormal lactate/pyruvate ratio is associated with organ dysfunction and can be usedfor predicting postoperative organ dysfunction. A substantialincrease in myocardial glycerol release seems to be a marker of
123456789
101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960616263646566
P. Kaur Randhawa et al. / European Journal of Pharmacology ∎ (∎∎∎∎) ∎∎∎–∎∎∎ 5
Please cite this article as: Kaur Randhawa, P., et al., RIPC for multiorgan salvage in clinical settings: Evolution of concept, evidencesand mechanisms. Eur J Pharmacol (2014), http://dx.doi.org/10.1016/j.ejphar.2014.08.016i

ischemic metabolism and may prove to be an indicator of reperfu-sion injury (Metzsch et al., 2006). Glycerol is also an indicator ofadipose tissue lipolysis induced by nor-adrenaline as a result ofmyocardial ischemia (Carlstrom and Christensson, 1971). Cerebralmetabolic effects suggested protection from ischemia and cellmembrane preservation lasting up to 2 days following RIPC(Gonzalez et al., 2013).
Based on RIPC strategy, it has been reported by Connolly et al.that chronic limb hypoperfusion induced by peripheral vasculardisease (PVD) can potentially produce a neuroprotective effect inacute ischemic stroke. It has been reported that patients withperipheral vascular disease (n¼26) had favorable scores in termsof National Institute of Health Stroke Scale (NIHSS), modifiedRankin scale (mRS). Furthermore, smaller infarct volume, lowermortality rate at admission as well as at discharge has also beenreported. It was noted that patients with peripheral vasculardisease had better outcome following acute cerebral ischemia.This suggests that chronic hypoperfusion of the lower extremitiesis caused by PVD in such a manner that it serves as stimulus thatmay be sufficient to induce the neuroprotective effects. Addition-ally, this study supports the postulate that RIPC may have shield-ing effect in human ischemic stroke (Connolly et al., 2013).
3.3. Renal injury
Acute kidney injury is a common complication during cardiacsurgery using cardiopulmonary bypass. Renal injury is evaluatedby analyzing various parameters that include serum/urine creati-nine, urinary retinol binding protein, albumin to creatinine ratio,glomerular filtration rate (GFR), urine neutrophil gelatinase asso-ciated lipocalin. Creatinine is removed chiefly by kidneys primarilyby glomerular filtration and if filtration is defective, creatininelevels in the blood are elevated (Mehta et al., 2007). Therefore,creatinine levels in blood/urine can give an indication of functionalstatus of kidney and moreover, creatinine clearance can becorrelated with glomerular filtration rate. Higher levels of creati-nine indicate a lower glomerular filtration rate and thus decreasedcapability of the kidneys to excrete waste metabolites. Malfunc-tional kidney secretes albumin into the urine, hence albumin tocreatinine ratio is one of the widely used parameters to assesskidney function. Retinol Binding Protein is a low molecular weight(21 kDa) protein that transports retinol from the liver to peripheraltissues. It undergoes extensive tubular reabsorption therefore;very small amount is excreted in urine. An elevation in the amountin the urine indicates proximal tubule injury/dysfunction (Bernardet al., 1987). Hence, measurement of urinary retinol bindingprotein is a useful aid for monitoring kidney disease. Likewise,the expression of neutrophil gelatinase-associated lipocalin(NGAL) protein is also used for assessing kidney damage asneutrophil gelatinase-associated lipocalin protein level is signifi-cantly increased in kidney tubules of humans after ischemic injury.
RIPC attenuated kidney injury as a reduction in creatinine levelwas noted in 41 patients (total¼82) undergoing abdominal aorticaneurysm repair. Ultimately, this led to reduction in absolute riskof renal impairment by 23%. Moreover, mean creatinine area undercurve was significantly lower in patients who received RIPCstimulus (Ali et al., 2007). A randomized, single-blind, controlledstudy conducted on 120 patients undergoing cardiac surgerybrought into picture that RIPC stimulus delivered to 59 patientsprevented acute kidney injury in 47 patients, indicated by allevia-tion in the levels of serum creatinine 48 h post-surgery(Zimmerman et al., 2011). A randomized, double blind, controlledtrial involving 50 patients (total patients¼100) with impairedrenal function revealed that RIPC stimulus forbade contrastmedium-induced acute kidney injury in the 44 patients. Signifi-cant improvement in kidney function as observed from the
biomarkers of kidney injury, i.e. serum creatinine and glomerularfiltration rate has been reported. Hence, RIPC carried out beforeusing contrast medium led to a reduction in kidney injury (Er etal., 2013; Gassanov et al., 2014). Likewise, a study that involvedrecruitment of forty-eight patients referred for kidney transplan-tation, unfolded the fact that remote ischemic conditioningstimulus led to attenuation of kidney injury in 24 patientssubjected to remote ischemic conditioning stimulus. Induction ofremote ischemic conditioning was carried out by three alternate 5-min cycles of ischemia and reperfusion caused by clamping anddeclamping of the exposed external iliac artery. Remote ischemicconditioning stimulus attenuated transplantation-associatedischemia-reperfusion injury, thus, enhanced the early recovery ofrenal function in recipients after kidney transplantation. Likewise,remote ischemic conditioning treatment also mitigated thechances of acute rejection, delayed graft rejection in 24 patients.Remote ischemic conditioning treatment attenuated the serumcreatinine level (from 2 h to 30 days), urine neutrophil gelatinaseassociated lipocalin from (2–48 h). Furthermore, RIPC enhancedthe estimated glomerular filtration rate (from 2 h to 30 days).However, graft histopathology after RIPC did not show significantimprovement (Wu et al., 2014). By pooling the data from 17clinical trials, it was brought into notice that RIPC treatmentcaused significant reduction in serum creatinine in patients under-going cardiovascular interventions (Alreja et al., 2012). However, insome instances, RIPC did reduce myocardial injury, but did notalleviate renal injury in 38 patients undergoing complex valvularsurgery (Choi et al., 2011). Likewise, RIPC stimulus delivered toeighteen patients undergoing endovascular aneurysm repair(EVAR) for the treatment of abdominal aortic aneurysm (approxi-mately 6.370.8 cm in diameter), led to reduction in urinaryretinol binding protein (3, 24, 48 h postoperatively) that was notstatistically significant and thus, could not confirm reduction inrenal injury (Walsh et al., 2009). In addition to this, RIPC stimulusdelivered to 54 children undergoing surgery for complex conge-nital heart disease could not afford to improve kidney function.This was suggested as no improvement in terms of renalbiomarkers-plasma creatinine, estimated glomerular filtrationrate, plasma cystatin C, plasma and urinary neutrophilgelatinase-associated lipocalin, initiation of dialysis and urinaryoutput was seen. Additionally, RIPC did not improve secondaryend points of the study which include postoperative bloodpressure measurement, inotropic score, morbidity and mortality(Pedersen et al., 2012). Furthermore, in a randomised, double blindcontrolled study RIPC stimulus given to 48 adults (total¼96)undergoing high risk surgery did not attenuate acute kidney injury(AKI) in terms of levels of creatinine levels (Young et al., 2012).However, non significant reduction in post operative release ofcreatinine has been reported in the trials primarily evaluatingcreatinine (D'Ascenzo et al., 2012). A recent meta analysis (13 trialswith 1334 participants) revealed that RIPC did not lead tosignificant reduction in the risk for AKI in patients undergoingcardiac and vascular interventions and suggested the usage ofadequately powered trials for future evidence (Yang et al., 2014).
3.4. Intestinal and pulmonary injury
Intestinal injury is analyzed by various parameters that includeserum intestinal fatty acid-binding protein, endotoxin levels, diamineoxidase. Intestinal fatty acid-binding protein is a cytosolic, watersoluble protein present in mature enterocyte and its levels areelevated in blood when enterocyte dies (Kanda et al., 1996). Diamineoxidase activity is another marker of intestinal injury, as circulatinglevels indicate mucosal maturation and integrity. Diamine oxidaseenzyme is an enzyme exclusively found in upper villi cells of theintestinal mucosa. Damage to intestinal mucosa causes significant
123456789
101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960616263646566
P. Kaur Randhawa et al. / European Journal of Pharmacology ∎ (∎∎∎∎) ∎∎∎–∎∎∎6
Please cite this article as: Kaur Randhawa, P., et al., RIPC for multiorgan salvage in clinical settings: Evolution of concept, evidencesand mechanisms. Eur J Pharmacol (2014), http://dx.doi.org/10.1016/j.ejphar.2014.08.016i

reduction in the levels ofQ8 diamine oxidase (Luk et al., 1981).Alteration in the levels of intestinal biomarkers is accompanied bya significant increase in the levels of endotoxins (Grimaldi et al.,2013). RIPC significantly attenuated the severity of intestinal andpulmonary injury in thirty one patients (total¼62) undergoingelective open infrarenal abdominal aortic aneurysm repair. Anincrease in arterial-alveolar oxygen tension ratio (primary end point)that is an index of gas exchange, was also been reported in responseto RIPC Moreover, endotoxin level, serum intestinal fatty acid-binding protein was attenuated and diamine oxidase activity wassignificantly increased indicating the decrease in severity of intestinalinjury (Li et al., 2013). By the same token, RIPC also attenuated acutelung injury in 108 patients undergoing elective thoracic pulmonaryresection under one-lung ventilation with propofol-remifentanilanesthesia. RIPC remarkably increased PaO2/FIO2 (ratio of partialpressure of arterial oxygen and fraction of inspired oxygen). Further-more, RIPC significantly attenuated IL-6, TNF-α level at 6, 12, 24, 48 hpostoperatively and malondialdehyde levels at 60 min after one-lungventilation and 30 min after re-expansion (Li et al., 2014). Veryrecently Camara-Lemarroy proposed that RIPC can lead to significantreduction in transfusion-related acute lung iQ9 njury (Camara-Lemarroy,2014). On the contrary, it has been reported that combination ofRIPCþRIPostC did not improve lung function in twenty sevenpatients undergoing complex valvular cardiac surgery in terms ofratio between partial pressure of oxygen in arterial blood (PaO2) andpercentage of oxygen participating in gas-exchange (FiO2) (Kim et al.,2012). The variation in response observed in terms of tissue protec-tion after RIPC treatment in patients undergoing surgical interven-tions is unclear (Young et al., 2012).
4. Possible mechanisms for beneficial effects of RIPC
RIPC has provided beneficial effects in alleviating ischemia-reperfusion-induced injury in various remote organs. The potentialmechanisms involved in providing RIPC-induced mutiorgan pro-tection have not been widely explored in clinical settings. How-ever, clinically observed multiorgan protection can be correlatedwith preclinical studies of RIPC to unveil the possible mechanismsinvolved in RIPC-induced tissue protection in clinical set-ups. Themechanisms involved in providing RIPC-induced cardioprotectionare quite complex and interlinked therefore it is difficult to pointout a particular trigger for initiating the cascade of signaling. Thepotential mechanisms explored clinically include the following.
4.1. Hypoxia Inducible factor-1α
Hypoxia Inducible factor (HIF) is a transcriptional factor thatrespond to changes in oxygen in the available environment andplays a key role in adapting to conditions like ischemia. HIFcomprises of an inducible HIF-1α subunit (susceptible to changesin oxygen concentration) and constitutive HIF-1β subunit. Condi-tions like ischemia result in the formation of a heterodimer that isafterwards translocated into the nucleus, where it acts as atranscriptional activator of the target genes (Kant et al., 2013).There has been a clinical study demonstrating that RIPC stimulussignificantly increases the levels of HIF-1α that in turn providesmyocardial protection (Albrecht et al., 2013). The role of HIF-1α inRIPC-induced cardioprotection in the above stated clinical report issupported by preclinical studies pinpointing the role of HIF-1α inconferring cardioprotection (Cai et al., 2013; Czibik et al., 2011;Kant et al., 2008). Our own study has shown the critical role ofHIF-1α in producing cardioprotection during remote renal pre-conditioning in rats (Kant et al., 2008). Cai et al. demonstrated thatRIPC stimulus (intermittent clamping and declamping of femoralartery) failed to confer cardioprotection in heterozygous
HIF-1α þ /� mice indicating that myocardial protection is depen-dent on HIF-1α gene expression (Cai et al., 2013).
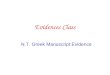
Albrecht et al. attributed RIPC-induced cardioprotective effectsin humans to up regulation of HIF-1α, along with activation ofother multiple pathways including enhanced procaspase-3 (inac-tive form) and reduced effectors caspase-3 and 7; increasedmyeloperoxidase activity, and increased IL-1β, IL-8 and TNF-αlevels (discussed below in inflammation section) (Albrecht et al.,2013). Although, authors did not explore the interrelationshipamong these multiple signaling pathways, yet such relationshipmay exist which needs further investigation. Our preclinical studyproposed that HIF may trigger NF-kB signaling to produce RIPC-induced cardioprotection in rats (Kant et al., 2008) and there areabundant reports linking NF-kB activation with inflammation(Oeckinghaus and Ghosh, 2009), which raise the possibility thatHIF signaling is linked to inflammation in RIPC. Moreover, a studyof Cai et al. also linked HIF-1α mediated cardioprotection duringRIPC to inflammatory cytokines. The authors attributed the loss ofRIPC-induced cardioprotection in HIF-1α þ /� mice to diminishedcirculating IL-10 levels and reduced Akt phosphorylation at serine-473. Intramuscular injection of AdCA5 (recombinant adenovirusthat encodes a constitutively active form of HIF-1α) into the hindlimb of mice was shown to significantly increase IL-10 levels;while HIF-1 inhibition by different means (pharmacological orgene silencing) reduced IL-10 levels suggesting that HIF-1αexpression in the hind limb is necessary to augment plasma IL-10 levels and confer cardioprotection (Cai et al., 2013). Using IL-10knockout mice and anti-IL-10 antibodies, same group of research-ers demonstrated that RIPC-induced late cardioprotection is due toup-regulation of IL-10 expression in the heart and gastrocnemiusmuscle. In addition, the authors also reported that RIPC activatesAkt and endothelial nitric oxide synthase in the heart (after 24 h)which was abolished by anti-IL-10 receptor antibodies suggestingthat RIPC triggers IL-10 transcription followed by activation of Akt/eNOS signaling pathway (Cai et al., 2012). Based on these, it maybe proposed that RIPC confers cardioprotection by increasing HIF-1α protein levels, which consequently trigger multiple signalingpathways including alteration in cytokines transcription to mod-ulate inflammation and apoptosis (Fig. 2).
4.2. ATP-sensitive potassium channels (KATP channels)
One of the major effectors for providing myocardial protectionafter subjecting the individuals to RIPC stimulus may include
123456789
101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960616263646566
Remote Ischemic Preconditioning
HIF 1α - HIF-1βDimer
Transcriptional changes(NF- B)
IL-10
Akt
CARDIOPROTECTION
P
eNOS Signalling
k
Fig. 2. RIPC causes dimerization of HIF 1α-HIF-1β subunits, which are thentranslocated into the nucleus where the dimer acts as a transcriptional activatorof NF-κB, which provides cardioprotection via increasing IL-10 levels and Akt/eNOSsignaling.
P. Kaur Randhawa et al. / European Journal of Pharmacology ∎ (∎∎∎∎) ∎∎∎–∎∎∎ 7
Please cite this article as: Kaur Randhawa, P., et al., RIPC for multiorgan salvage in clinical settings: Evolution of concept, evidencesand mechanisms. Eur J Pharmacol (2014), http://dx.doi.org/10.1016/j.ejphar.2014.08.016i

activation of ATP sensitive potassium channels (Loukogeorgakis etal., 2007). These channels are heteromultimers of sulfonylureareceptor (SUR) and KIR6.X subunits associated with a 1:1 stoichio-metry as a tetramer. Kir6.0 subfamily subunit is a member of theinwardly rectifying Kþ channel family; and a SUR subunit is amember of the ATP-binding cassette (ABC) protein super-family(Seino, 1999). Changes in [ATP]i and [ADP]i gate the channel andKATP channel is usually inhibited by intracellular ATP and opensduring periods of energy depletion (Babenko et al., 1998). Animalstudies have revealed that KATP channels are present on thesarcolemma (plasma membrane) of cardiac myocytes. Further-more, KATP channels similar to surface KATP also exist on the innermitochondrial membrane and exhibit properties remarkably simi-lar to those of the KATP on the plasma membranes (Beavis et al.,1993; Paucek et al., 1992).
It has been reported that both RIPC and remote ischemic postconditioning (RIPostC) elicit myocardial protection in patients bymeans of activation of KATP channels (Loukogeorgakis et al., 2007).It is well established that the opening of KATP channels and theconsequent decrease in intracellular calcium concentration resultsin vasodilation. Such vasodilation can be emulated by cromakalimadministration (KATP channel opener) and blocked by administra-tion glibenclamide (non selective KATP channel blocker) (Daut etal., 1990). Loukogeorgakis et al. correlated the changes in flow-mediated dilation with KATP channels opening/blockade toindirectly demonstrate the involvement of KATP channels inischemia-reperfusion-injury and RIPC/RIPostC-mediated cardio-protective effects. Ischemia-reperfusion-induced injury wasshown to significantly reduce flow mediated dilation in patients,probably due to blockade of KATP channels. However, RIPC andRIPostC stimuli were associated with restoration of ischemia-reperfusion-induced decrease in flow mediated dilation, probablydue to the opening of KATP channels. The involvement of KATP
channels opening in RIPC/RIPostC was also demonstrated directlyby administering glibenclamide, which was shown to completely
abrogate the protective responses of RIPC and RIPostC in patients(Loukogeorgakis et al., 2007).
There have been number of preclinical studies supporting thecritical role of KATP channels in RIPC-induced cardioprotection(Diwan et al., 2008; Jones et al., 2009; Konstantinov et al., 2005;Kristiansen et al., 2005; Pell et al., 1998; Wu et al., 2011). It hasbeen reported that RIPC-mediated alleviation of ischemia-reperfusion-induced injury in the donor heart after orthotopicheart transplantation is abolished by pretreatment with gliben-clamide (Konstantinov et al., 2005). Kristiansen et al. demon-strated the involvement of mitochondrial KATP channels, but notsarcolemmal KATP channels, in providing RIPC-induced cardiopro-tection as glibenclamide and 5-HD (mitochondrial KATP blocker),but not HMR-1098 (sarcolemmal KATP blocker), abolished thecardioprotective effects of RIPC in the explanted rat hearts(Kristiansen et al., 2005). An earlier study also reported abrogationof the cardioprotective effects of RIPC in the presenc Q10e of 5-HD (Pellet al., 1998). Additionally, remote preconditioning of trauma-induced cardioprotection was shown to be mediated via activationof mitochondrial KATP channels as administration of 5-HD com-pletely abrogated myocardial protection (Jones et al., 2009).The study from our laboratory has also demonstrated that openingof KATP channels is involved in producing remote renalpreconditioning-induced cardioprotection in rats (Diwan et al.,2008). In addition to studies showing the role of mitochondrialKATP channels in early phase of RIPC, a study of Wu et al.demonstrated alleviation of delayed cardioprotective effects ofRIPC with 5-HD pretreatment suggesting the role of these chan-nels in early as well as late phase of RIPC (Wu et al., 2011).
Though clinical study of Loukogeorgakis et al. did not explorethe interrelationship of KATP channels with other cardioprotectivemediators, yet, preclinical study of Shahid et al. revealed theinterrelationship of these channels among other mediators(Shahid et al., 2008). Shahid et al. demonstrated the existenceof an interrelationship between activation of mitochondrial KATP
123456789
101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960616263646566
Remote Ischemic Preconditioning
Opening of mitochondrial KATP
channels
Dissipation of mitochondrial membrane potential
Driving force for Ca2+ uptake via mitochondrial Ca+
uniporter
Limits Mitochondrial Ca2+
CARDIOPROTECTION
eNOS
NO
Nitrite
Mitochondrial Ca2+ uniporter
Generation of free radicals
Redox Signalling
Fig. 3. RIPC stimulus initiates eNOS signaling and NO thus released causes opening of mitochondrial KATP channels to trigger redox signaling and cause dissipation ofmitochondrial membrane potential which inturn decreases the driving force for calcium intake via mitochondrial calcium uniporter (MCU). Further, RIPC directly inhibitsMCU which limits mitochondrial calcium overload in the myocytes and provides myocardial protection.
P. Kaur Randhawa et al. / European Journal of Pharmacology ∎ (∎∎∎∎) ∎∎∎–∎∎∎8
Please cite this article as: Kaur Randhawa, P., et al., RIPC for multiorgan salvage in clinical settings: Evolution of concept, evidencesand mechanisms. Eur J Pharmacol (2014), http://dx.doi.org/10.1016/j.ejphar.2014.08.016i

channels, NO release and generation of free radicals in conferringcardioprotection via RIPC stimulus. Pretreatment with 5-HD,l-NAME (NOS inhibitor) and N-acetylcystein (ROS scavenger)abolished RIPC-induced cardioprotection in rats. Furthermore,infusion of l-arginine and diazoxide (KATP channel opener) wasshown to confer cardioprotection that was abolished by 5-HD andNAC administration, respectively. Based on these, the authorsproposed that RIPC-induced cardioprotection is mediated byaugumented synthesis of NO (upstream molecule) with subse-quent activation of mitochondrial KATP channels and generation offree radicals (Shahid et al., 2008). The role of endothelial nitricoxide synthase (eNOS) and NO in eliciting RIPC-induced organprotection has also described using eNOS knockout mice andpharmacological blockers of eNOS (L-NAME) (Abu-Amara et al.,2011; Zhao et al., 2007) and it has been described that RIPCstimulates eNOS to generate NO that is subsequently oxidized tonitrite to elicit myocardial protection (Rassaf et al., 2014). Earlierstudies have demonstrated the key role of endogenous freeradicals in RIPC-induced cardioprotection (Chen et al., 2005;Weinbrenner et al., 2004). A study of Wu et al. described anincrease in antioxidant enzymes (total superoxide dismutase,manganese-superoxide dismutase (Mn-SOD) and glutathione per-oxidase) in heart following non-invasive delayed RIPC in mito-chondrial KATP channel (opening of these channels) dependentmanner as pretreatment with 5-HD was shown to abolish cardi-oprotection and decrease antioxidant enzymes in heart. Anincrease in antioxidant capability of heart was shown to confergreater resistance to ischemia-reperfusion injury (Wu et al., 2011).However, it is in contrast to earlier report of Shahid et al. whichdescribed the role of oxidative free radicals in mediating RIPC-induced cardioprotection in KATP dependent manner. In fact,mitochondrial KATP channels are redox sensors and decreasegeneration of free radicals in response to increased local levels ofoxidants (Facundo et al., 2007). Furthermore, opening of mito-chondrial KATP channels causes an increase in the production ofprotective reactive oxygen species during preconditioning phasefollowed by decreased generation during reperfusion phase(Colantuono et al., 2008). Likewise, another report suggested thatopening of KATP channels causes transient increase in reactiveoxygen species in the preconditioning phase and production ofreactive oxygen species is attenuated on subsequent exposure toprolonged ischemic insult (Matejíková et al., 2009). ThQ11 erefore, it isproposed that opening of KATP channels during remote precondi-tioning may lead to cardioprotection by transiently increasing theproduction of reactive oxygen species in such a way that onsubsequent exposure of prolonged ischemia, generation of reactiveoxygen species is attenuated.
Though, there is no direct study describing the role of KATP
and mitochondrial Ca2þ uniporter (MCU) in RIPC, yet, a relation-ship may exist between these that need experimental investiga-tion. There have been studies suggesting that opening ofmitochondrial KATP channels may dissipate mitochondrial mem-brane potential to decrease the driving force for calcium intakeinside the mitochondria via mitochondrial Ca2þ uniporter (Liu etal., 1998). There has been a report describing that inhibition ofmitochondrial Ca2þ uniporter opening elicits RIPC-induced cardi-oprotection limits mitochondrial Ca2þ concentration (Xu et al.,2007). However, the direct role of KATP channels in dissipatingmitochondrial membrane potential and decreasing the drivingforce for calcium intake via mitochondrial Ca2þ uniporter needfurther investigation (Fig. 3).
4.3. Matrix metalloproteinases
Further, increase in expression of tissue inhibitor of matrixmetalloproteinases (TIMP), which inhibit curb MMP activity by
binding them in a stoichiometric ratio of 1:1 (Brew et al., 2000)has been observed (Konstantinov et al., 2004).
Matrix metalloproteinases (MMPs) are Zn2þ-dependent endo-peptidases that degrade various extracellular matrix proteins tomodulate physiological as well as pathological processes, includingmorphogenesis, angiogenesis, tissue repair, arthritis and metastasis(Jackson et al., 2001). MMPs have been broadly classified into5 major classes that include collagenases, gelatinases, stromelysins,matrilysins and membrane type MMPs. Of the diverse family ofenzymes, MMP-2 (gelatinase A) and MMP-9 (gelatinase B) play animperative role in numerous cardiovascular disorders (Schulz,2007; Spinale et al., 2000). MMPs have the capability to cleavematrix components in the heart, therefore, may cause degradationof fibrillar collagen, extracellular matrix to promote myocardialremodeling and cardiac dysfunction (Li et al., 2000).
Previous clinical studies have shown a correlation between anincrease in MMP expression and fibrosis indicating that MMP isinvolved in atrial remodeling in patients su Q12ffering from mitral valvedisease (Anné et al., 2005; Nakano et al., 2004). A role of MMP inRIPC-induced cardioprotection was demonstrated by a study show-ing that administration of sera obtained from RIPC-subjected patientsprotected the cultured human intestinal cells from hypoxia-induceddamage. Administration of the resulting sera significantly reducedthe activity of MMP-2 and MMP-9 suggesting that attenuation ofMMP-2 and MMP-9 activity may be involved in affording RIPC-induced cardioprotection (Zitta et al., 2012).
Additionally, a very recent study has suggested that RIPC-induced cardioprotection in eighteen patients is associated withalleviation in the levels of MMP-2 and MMP-9 in cardiac tissue(Zitta et al., 2014). The key role of MMP in RIPC-mediatedcardioprotection in patients is supported by various preclinicalstudies revealing that up-regulation of the activity of variousMMPs in the heart may contribute to ischemia-induced myocar-dial injury (Cheung et al., 2000; Peterson et al., 2000). Deletion ofMMP-9 gene is shown to reduce the infarct size in both hetero-zygotic (þ /�) and homozygotic (� /�) animals by 17.5% and 35.4%,respectively. Moreover, several fold increase in expression of tissueinhibitors of metalloproteinases (TIMP-1), an endogenous inhibi-tor of MMP, has also been seen in heterozygotic and homozygoticMMP-9 gene knock out animals. Along with it, myeloperoxidaseactivity (a key marker of acute inflammation) was also shown tobe reduced by 44% in homozygotic MMP-9 gene knockout animals(Romanic et al., 2002). Therefore, it may be possible to suggest thatischemia-induced up-regulation of MMP 9 may induce inflamma-tion to contribute in myocardial injury. The role of these MMP ininducing ischemic brain injury has also been described as thelevels of MMP-9 are shown to be up-regulated in acute cerebralischemic conditions (Ulrich et al., 2013). Furthermore, a possiblerole of MMP-2 in mediating blood brain barrier disruption has alsobeen suggested (Liu et al., 2012). The release and up-regulation ofkey molecules of inflammation including cytokines, chemokines,adhesion molecules, growth factors and peroxynitrites may be themajor contribu Q13ting factor in MMP-mediated myocardial injury(Cauwe and Opdenakker, 2010; Gao et al., 2003). Proinflammatorycytokines may in turn further cause brisk and enhanced release ofMMPs indicating the development of the vicious cycle of MMPactivation and cytokine generation (Gao et al., 2003). It is mani-fested that TnI and MMP-2 are localized within thin myofilamentsof cardiomyocytes and TnI has been considered as a critical targetfor proteolytic cleavage by MMP-2. Studies have shown thatinhibition of this enzyme leads to decreased troponin degradation,which is subsequently followed by improvement in the mechan-ical function of the heart (Wang et al., 2002).
Based on these, it may be suggested that inhibition of MMP-2and MMP-9 during RIPC may induce cardioprotection by mitigat-ing degradation of various structural and functional proteins and
123456789
101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960616263646566
P. Kaur Randhawa et al. / European Journal of Pharmacology ∎ (∎∎∎∎) ∎∎∎–∎∎∎ 9
Please cite this article as: Kaur Randhawa, P., et al., RIPC for multiorgan salvage in clinical settings: Evolution of concept, evidencesand mechanisms. Eur J Pharmacol (2014), http://dx.doi.org/10.1016/j.ejphar.2014.08.016i

decreasing the production of cytokines and other chemotacticfactors.
4.4. O-linked β-N-acetylglucosamine (O-GlcNAc)
Hexosamine biosynthesis pathway is a glucose sensor pathwaythat utilizes glucose to form uridine 50-diphosphate-N-acetylglu-cosamine (UDP-GlcNAc), which is a substrate for O-GlcNAc trans-ferase (OGT) for O-glycosylation. OGT catalyzes reversible post-translational modification by attaching GlcNAc via O-linkage tospecific serine and threonine residues on numerous cytoplasmicand nuclear proteins. On the other hand, O-GlcNAcase is a solubleand highly conserved enzyme that catalyzes the removal of sugarfrom the modified proteins (Champattanachai et al., 2008; Olivier-Van Stichelen et al., 2012). Glutamine: fructose-6-phosphateamidotransferase (GFAT) monitors the entry of glucose into thehexosamine biosynthesis pathway, and activation of this pathwaymay increase O-GlcNAc levels.
In clinical set up, augmentation of O-GlcNAc signaling has beenreported in both diabetic and non-diabetic patients subjected toRIPC. The increase in O-GlcNAc signaling has been correlated withcardioprotection as administration of GFAT inhibitor (azaserine)completely abrogated the cardioprotective effects of RIPC (Jensenet al., 2013). This suggests that augmentation of O-GlcNAc levelsvia hexosamine biosynthesis pathway flux is one the possiblemechanisms of myocardial protective effects of RIPC. Administra-tion of glucosamine (precursor of UDP-GlcNAc) causes channelingof glucose metabolism via an accessory pathway i.e. hexosaminebiosynthesis pathway to significantly increase the levels of O-GlcNAc during ischemic as well as reperfusion phase and producecardioprotective effects (Fulop et al., 2007). There are experimen-tal studies showing the tissue protective effects of O-GlcNAc.Administration of glucosamine is shown to produce improvementin a rat model of trauma-hemorrhage in O-GlcNAc dependentpathway (Yang et al., 2006; Zou et al., 2009). Furthermore,intravenous administration of PUGNAc (O-(2-acetamido-2-deoxy-d-glucopyranosylidene) amino-N-phenylcarbamate) has beenshown to improve cardiac function and organ perfusion aftertrauma-hemorrhage, which is secondary to O-GlcNcase inhibitionand increase in O-GlcNAc (Zou et al., 2007). Other studies havealso shown that glucosamine and PUGNAc increase the levelsof O-GlcNAc-modified proteins in the right carotid balloon injurymodel (Xing et al., 2008). In addition, adenoviral over-expressionof O-GlcNAc transferase (AdOGT)/pharmacological inhibitionof O-GlcNAcase are shown to raise O-GlcNAc levels and attenuatepost-hypoxic damage (Ngoh et al., 2009).
Exogenous glutamine has been shown to produce cardiopro-tective action due to the upsurge of O-GlcNAc levels by activatinghexosamine biosynthesis pathway flux (Liu et al., 2007; Lauzieret al., 2013). Administration of azaserine (inhibitor of GFAT) andalloxan (O-GlcNAc transferase inhibitor) not only completelyeverted the cardioprotection, but also prohibited the rise in O-GlcNAc levels (Lauzier et al., 2013; Liu et al., 2007). Glutamine isrequired for metabolizing glucose via GFAT, which carries outconversion of fructose-6-phosphate to glucosamine-6-phosphateutilizing glutamine. Therefore, glutamine-induced cardioprotec-tion could be due to increased flux through HBP pathway andenhanced O-GlcNAc mediated post-translational modification ofproteins.
There have been various mechanisms to induce protectiveeffects in various organs via OGlcNAc signaling. It has beenreported that adenoviral over-expression of O-GlcNAc transferase(AdOGT)/pharmacological inhibition of O-GlcNAcase increases O-GlcNAc levels and reduces the activation of endoplasmicreticulum-induced C/EBP homologous protein (CHOP) to preventmyocyte death (Ngoh et al., 2009). Genetic deletion of O-GlcNAc
transferase is shown to abate post-translational modification ofvoltage-dependent anion channels (VDAC) located on the outermitochondrial membrane, which results in loss of mitochondrialmembrane potential and mPTP formation. It is quite possible thatO-glycosylation of VDAC (component of mPTP) may preservemitochondrial membrane potential and prevent mitochondrialpermeability transition pore (mPTP) formation. This indicates thatprevention of mitochondrial permeability transition pore forma-tion is one of the critical targets of O-GlcNAc signaling forimproved survival during the hypoxia-reoxygenation phase incardiac myocytes (Ngoh et al., 2008). It has been reported thatpost-translationally modified VDAC on mitochondrial membraneare more resistant to calcium induced swelling (Jones et al., 2008).In contrast to above report stating the indispensability of VDAC inmPTP formation, Baines et al. described that VDAC are in factdispensable for mitochondrial dependent cell death (Baines et al.,2007). Apart from preventing mPTP formation, O-glycosylation ofvarious proteins may exert cardioprotective effects by activatingvarious other signaling pathways. O-GlcNAc signaling-mediatedcardioprotective effects may also be due to induction of HSP40 andHSP70 protein expression (Okubo et al., 2001; Peng et al., 2010).Furthermore, significant increase in O-GlcNAc levels after gluco-samine administration could be directly correlated to increasedp38 MAPK phosphorylation and improvement in the functionalrecovery after ischemic insult (Fulop et al., 2007). Furthermore,increase in O-GlcNAc modified proteins decreases proinflamma-tory mediator expression, reduces infiltration of monocytes andneutrophils indicating their plausible involvement in providinganti-inflammatory as well as vasoprotective response (Xing et al.,2008). This is further supported by an augmentation in the levelsof post translationally modified proteins and attenuated NF-kBsignaling (Zou et al., 2009) (Fig. 4). This suggests that O-glycosylation of proteins leads to significant reduction in cascadeof biochemical events that propagate to an inflammatory response.Other possible mechanisms include attenuation of Ang-II inducedincrease in calcium, which is detrimental and induces cell death(Nagy et al., 2006). In addition, increased O-GlcNAc levels alsoreduce calpain-mediated proteolysis of α-fodrin and Ca2þ/calmo-dulin dependent protein kinase II during reperfusion (Liu et al.,2007).
Thus, it is hypothesized that increased O-GlcNAc signalingduring RIPC may exert cardioprotective action by reducing mPTPformation, decreasing intracellular calcium overload, attenuatingC/EBP homologous protein (CHOP) activation, increasing theexpression of HSP40 and HSP70, attenuating NFkB signaling,decreasing proinflammatory mediator expression, infiltration ofmonocytes and neutrophils.
4.5. Signal transducer and activator of transcription (STAT)
Signal transducer and activator of transcription (STAT) moni-tors various aspects of growth and differentiation. It is well knownthat the binding of ligands like cytokines causes activation ofintracellular Janus Kinase that consequently phosphorylates aspecific tyrosine residue in the STAT protein, ultimately leadingto dimerization. The dimerized form subsequently activates tran-scription of certain cytokine-inducible genes (Shuai et al., 1993;Mohr et al., 2012). In contrast to well defined role of STAT 3 and5 in ischemic preconditioning-induced cardioprotective effects,there have been few studies exploring the role of STAT in RIPC. Inclinical settings, signal transducer and activator of transcription-5(STAT-5) phosphorylation was increased in the heart after carryingout RIPC in 12 patients suggesting that protection afforded by theRIPC stimulus may be the result of the augmentation of STAT-5signaling pathway (Heusch et al., 2012). The same group ofworkers reported that propofol (as anesthetic agent) abolishes
123456789
101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960616263646566
P. Kaur Randhawa et al. / European Journal of Pharmacology ∎ (∎∎∎∎) ∎∎∎–∎∎∎10
Please cite this article as: Kaur Randhawa, P., et al., RIPC for multiorgan salvage in clinical settings: Evolution of concept, evidencesand mechanisms. Eur J Pharmacol (2014), http://dx.doi.org/10.1016/j.ejphar.2014.08.016i

RIPC-induced cardioprotection during coronary artery bypass graftsurgery possibly by interfering with phosphorylation of STAT-5suggesting the importance of STAT-5 signaling in mediating RIPC-induced cardioprotection in clinical settings (Kottenberg et al.,2014). Therefore, further experimental investigations areneeded to assert the role of STAT-5 in mediating RIPC-inducedcardioprotection.
4.6. Autonomous nervous system
There is a plausible involvement of autonomous nervoussystem in providing early and late cardioprotection effects of RIPC.Involvement of neuronal component in providing RIPC-inducedcardioprotection was indicated as administration of trimetaphan(autonomic ganglion blocker) mitigated early and late precondi-tioning in humans (Loukogeorgakis et al., 2005). Animal studieshave also suggested the involvement of parasympathetic nervoussystem in mediating remote hind limb ischemic preconditioninginduced myocardial protection (Donato et al., 2013). It has beenshown that sectioning of femoral nerve, sciatic nerve and spinalcord (in order to induce hind limb deafferentation) annihilatedRIPC-induced reduction in infarct size suggesting the role ofafferent neural pathway in mediating cardioprotective effects.Likewise, sectioning of the vagus nerve and administration ofatropine completely abrogated RIPC induced cardioprotection andsuggested the involvement of efferent parasympathetic neuralpathways. Thus, it is proposed that RIPC causes activation ofneural afferent pathways and the cardioprotective signal reachesthe myocardium via a neural efferent pathway (through vagusnerve) (Donato et al., 2013). However, Jones et al. reported thatadministration of hexamethonium (ganglion blocker) abolishesthe protective effects of remote preconditioning and correlated the
attenuation of RIPC effects with the blockade of sympatheticneurons (Jones et al., 2009). However, the role of blockade ofparasympathetic neurons, (due to the ganglionic blocker) inattenuating RIPC cannot be ruled out. Further investigations needto be carried out in order to explore the role of sympatheticnervous system in rendering the tissue resistant to ischemia-reperfusion-induced injury.
4.7. Inflammatory gene expression
Ischemia-reperfusion-induced injury is characterized by sig-nificant increase in inflammatory cell response and RIPC-inducedcardioprotection has also been linked with modulation of theseinflammatory responses.
4.7.1. Decrease in cytokines, apoptosis and related inflammatoryprocesses
Konstantinov et al. demonstrated that administration of RIPCstimulus is associated with significant change in the expression ofapproximately 169 genes regulating inflammation in 4 healthyvolunteers (Konstantinov et al., 2004). The authors demonstratedsignificant reduction in cytokine generation as a consequence ofRIPC due to significant suppression of the enzymes involved inTNF-α synthesis including MAPK-activated protein kinase 2, MAP/ERK kinase kinase 2, mitogen-activated protein kinase 8(Konstantinov et al., 2004). RIPC was shown to significantly reducethe expression of apoptosis regulating genes, enzymes and mole-cules including reduction in the gene expression of caspase-8,caspase-8-associated protein 2 and up-regulation of calpastatin(endogenous calpain inhibitor) (Konstantinov et al., 2004). Arecent study by Albrecht et al. has also attributed RIPC-induced
123456789
101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960616263646566
Remote Ischemic Preconditioning
OGTOGlcNAcaseGFAT
O-GlcNAc Signalling
CARDIOPROTECTION
O-glycosylation of VDAC
Survival of cardiomyocytes
Calpain mediated protolysis of Ca2+ and calmodulin dependent
protein kinase
P38 MAPK P
HSP40HSP70
expression
NF-KB signalling
Expression of pro-inflammatory cytokines
Infiltration of monocyte and neutrophils
Anti-inflammatory vasoprotective response
Preserve mitochondrial
potential
mPTPFormation
Apoptosis
Activation of C/EBP homologus
protein
Fig. 4. RIPC stimulus causes increase in OGT and GFAT activity whereas diminishes OGlcNAcase activity which leads to enhanced OGlcNAc signaling. Increased OGlcNAclevels cause post-translational modification of voltage dependent anion channels (VDAC) on outer mitochondrial membrane. O-glycosylation of VDAC preservesmitochondrial membrane potential and prevents mitochondrial permeability transition pore (mPTP) formation and thus apoptosis. Enhanced O-GlcNAc signaling alsoreduces calpain mediated proteolysis of α-fodrin and Ca2þ/calmodulin dependent protein kinase II and thus apoptosis; hence increases the survival of cardiomyocytes.Furthermore, increase in O-GlcNAc levels causes phosphorylation of MAPK p38 and induce increase in expression of HSP 40 and HSP 70 to mediate cardioprotection.Increased OGlcNAc signaling also reduces activation of endoplasmic reticulum induced C/EBP homologous protein (CHOP) to mitigate myocyte death. Additionally,augumented OGlcNAc levels attenuate NF-kB signaling which thereafter reduces expression of proinfammatory cytokines. This in-turn attenuates infiltration of monocytesand neutrophils and elicits anti-inflammatory and vasoprotective response thereby conferring cardioprotection.
P. Kaur Randhawa et al. / European Journal of Pharmacology ∎ (∎∎∎∎) ∎∎∎–∎∎∎ 11
Please cite this article as: Kaur Randhawa, P., et al., RIPC for multiorgan salvage in clinical settings: Evolution of concept, evidencesand mechanisms. Eur J Pharmacol (2014), http://dx.doi.org/10.1016/j.ejphar.2014.08.016i

cardioprotective effects in humans to reduction in apoptosis as aconsequence of enhanced levels of procaspase-3 (inactive form)and reduced activity of effectors caspase-3 and 7 in the cardiactissue (Albrecht et al., 2013). In response to RIPC, various mole-cules responsible for chemotaxis, adhesion, migration and infiltra-tion of leukocytes are also reduced including decrease in theexpression of CD 11b (involved in cell adhesion, chemotaxis andphagocytosis), TM7LN4, SLP-76 (involved in chemotaxis and mastcell activation), α-4 integrin (an adhesion molecule), A disintegrinand metalloprotease 8, A disintegrin and metalloprotease 10,platelet-endothelial cell adhesion molecule, chemokine CC recep-tor 2a (involved in migration and infiltration of leukocytes) andphosphoinositide 3-kinase (regulating neutrophil infiltration)(Konstantinov et al., 2004). Moreover, reduction in the expressionof soluble N-ethylmaleimide-sensitive fusion protein attachmentprotein receptors (SNAREs) was also documented (Konstantinov etal., 2004). SNARE is a ternary complex composed of SNAP-23,syntaxin and VAMP and is responsible for mast cell and neutrophilexocytosis. Transposition of SNAP-23 from the cell surface of thesecretory granules membrane is indispensible for the formationof ternary SNARE complexQ14 and exocytosis (Guo et al., 1998;Wesolowski and Paumet, 2014). The authors also demonstratedthe reduction of others components including SNAP-23 and VAMP3 in response to RIPC (Konstantinov et al., 2004).
4.7.2. Increase in neutrophil infiltrationIn contrast to many documented studies showing tissue
destructive role of neutrophils (Jordan et al., 1999), Albrechtet al. attributed the cardioprotective effects of RIPC to increasedneutrophil infiltration, assessed in terms of increased myeloper-oxidase activity (a key marker of neutrophil infiltration) duringRIPC. Neutrophils are involved in tissue damage via excessiverelease of oxidants and proteases; however, these are also key partof host defense and protect host tissue via defensins, myeloper-oxidase and proteolytic enzymes (Jordan et al., 1999; Kobayashiand DeLeo, 2009). Accordingly, neutrophils may have both tissueprotective and destructive role depending upon the extent ofneutrophil infiltration in tissues. Based on this, the authorsproposed that per se increase in neutrophil count may not produceonly negative effect, but may also exert positive influence on theaffected cardiac tissue during the initial reperfusion phase. How-ever, the above described protective role of neutrophil infiltrationin RIPC needs further investigations.
4.7.3. Increase in cytokine expressionIn contrast to the report of Konstantinov et al. regarding
the decreased expression of enzymes responsible for TNF-α, therehave been some clinical reports suggesting an increase in cyto-kines in response to RIPC (Shimizu et al., 2010; Albrecht et al.,2013). Shimizu et al. described an increase in TNF-α, IL-6, IL-β andIL-10 levels in the blood of 5 healthy volunteers on 10th day ofRIPC stimulus (Shimizu et al., 2010). Similarly, Albrecht et al. alsoattributed RIPC-induced cardioprotective effects to increasedlevels of low weight cytokines including IL-1β, IL-8 and TNF-α(Albrecht et al., 2013). Although, the role of increased TNF-α levelin mediating RIPC-induced cardioprotection cannot be explainedby direct studies, yet it can be comprehended using otherpreclinical studies that transient increase in TNF-α level mayprevent the sustained rise in TNF-α level (Ginis et al., 2002). Thismay be analogous to redox signaling in RIPC during whichtransient rise in free radicals (as a part of redox signaling) mayprevent the sustained generation of free radicals during reperfu-sion phase to confer cardioprotection (explained earlier). Never-theless, experimental studies are required to support the above
contention that transient rise in TNF-α level may trigger beneficialeffects in RIPC by inhibiting subsequent synthesis of TNF-α.
4.7.4. BradykininThe putative role of bradykinin (endogenous peptide) in
mediating RIPC-induced cardioprotection has been explored clini-cally by various researchers. It was seen that RIPC stimulusdecreased the expression of kinin receptors (B1 and B2) oncirculating neutrophils in healthy volunteers as well as in patientsundergoing heart surgery (Saxena et al., 2011, 2013). Nevertheless,this decrease in the expression of B1 and B2 receptors was notassociated with cardioprotective effects in terms of serum CK-MB,TnI, C-reactive protein and lactate levels (Saxena et al., 2013).Furthermore, it has also been reported that RIPC abrogatesischemia-reperfusion-induced endothelial dependent vasomotordysfunction which is not blocked by administering HOE-140(bradykinin antagonist) suggesting no major involvement ofendogenous bradykinin in RIPC-induced cardioprotection inhumans (Pedersen et al., 2011). However, preclinical studiessuggest the key role of bradykinin in mediating RIPC-inducedcardioprotection (Heinen et al., 2011; Schoemaker et al., 2000;Wolfrum et al., 2002). Therefore, further clinical investigationsare needed to assert the role of bradykinin in RIPC-inducedcardioprotection.
4.7.5. Possible reasons for contradictory reports andrecommendations for future research
There have been limited clinical studies correlating RIPC andinflammatory responses and the reports from these studies arecontradictory to certain extent with respect to changes in expres-sion of cytokines and neutrophil infiltration. The report ofKonstantinov et al. documented decrease in TNF-α level and otherinflammatory markers in response to RIPC (Konstantinov et al.,2004), which seems to be contradictory to the report of Albrecht etal. documenting an increase in TNF-α level and neutrophil infiltra-tion in RIPC-induced cardioprotection (Albrecht et al., 2013).Furthermore, the report of Pavione et al. negated the changes ingene expression of inflammatory cytokines such as IL-8, IL-10 andIκB α in response to RIPC treatment (Pavione et al., 2012). Theseopposite changes regarding the expression of cytokines in RIPCstudies may be multi-factorial and difficult to explain at this point.It may be possible that these seemingly opposite changes regard-ing inflammatory changes during RIPC are due to single/limitedpoint sampling in these studies in which inflammatory changeswere observed only a single point of time instead of extendedsampling at multiple points of times. RIPC triggered beneficialpathway may be quite complex and may involve multiple cascadeof signaling. Determination of cytokine expression or otherinflammatory mediators at a given point of time (single pointsampling) may not yield a conclusive result regarding the tem-poral changes occurring over a wider range of a given phenom-enon. Accordingly, more conclusive hypothesis may be drawnregarding the exact role of inflammatory cytokines in RIPC fromthe experimental studies in which changes in inflammatorymarkers are observed over an extended period of time.
5. Conclusion
RIPC became a successful approach in numerous species ofanimals in order to provide multiorgan salvage. Consequently,RIPC evolved in clinical settings and provided beneficial effects inalleviating ischemia-reperfusion-induced injury in various remoteorgans. There are several reports emphasizing the role of RIPC inconferring cardioprotection, renoprotection, while undergoingvarious surgical/non surgical interventions that include coronary
123456789
101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960616263646566
P. Kaur Randhawa et al. / European Journal of Pharmacology ∎ (∎∎∎∎) ∎∎∎–∎∎∎12
Please cite this article as: Kaur Randhawa, P., et al., RIPC for multiorgan salvage in clinical settings: Evolution of concept, evidencesand mechanisms. Eur J Pharmacol (2014), http://dx.doi.org/10.1016/j.ejphar.2014.08.016i

artery bypass graft surgery, abdominal aortic aneurysm repair,percutaneous coronary intervention, heart valve surgery, drug-eluting stent implantation, kidney transplantation etc. Further-more, RIPC treatment strategy has attenuated neuronal injury inpatients undergoing elective decompression surgery. In addition tothis, RIPC also led to reduction of intestinal and pulmonary injuryin patients undergoing elective open infrarenal abdominal aorticaneurysm repair. The involvement of hypoxia inducible factor-1α(HIF-1α), ATP-sensitive potassium channels, (KATP channels), signaltransducer and activator of transcription (STAT), matrix metallo-proteinases (MMPs), O-linked β-N-acetylglucosamine (O-GlcNAc)levels, autonomous nervous system (ANS) in mediating RIPC-induced cardioprotective effects has been explored clinically.Therefore, it is quite possible that use of this strategy may becomewidespread in the coming years for mitigating ischemia-reperfusion-induced injury in various remote organs but thepotential mechanisms involved still need to be elucidated.
UncitedQ2 references
Chandrasekar et al. (2000), Gross et al. (2013), Heusch (2010),Keane and Strieter (2000), Koretzky et al. (2006), Kotlyarov et al.(2002), Liu et al. (2006), Pan and Li (2011), Peri et al. (2010), Rehniand Singh (2012), Sarkar et al. (2012), Vibjerg Jensen et al. (2013).
Acknowledgments
The authors are thankful to Department of Science and Tech-nology F. no. SB/SO/HS/0004/2013, New Delhi foQ15 r their grate-fulness for providing us financial assistance and Department ofPharmaceutical Sciences and Drug Research, Punjabi University,Patiala, India for supporting us.
References
Abu-Amara, M., Yang, S.Y., Quaglia, A., Rowley, P., Fuller, B., Seifalian, A., Davidson,B., 2011. Role of endothelial nitric oxide synthase in remote ischemic pre-conditioning of the mouse liver. Liver Transpl. 17, 610–619.
Albrecht, M., Zitta, K., Bein, B., Wennemuth, G., Broch, O., Renner, J., Schuett, T.,Lauer, F., Maahs, D., Hummitzsch, L., Cremer, J., Zacharowski, K., Meybohm, P.,2013. RIPC regulates HIF-1α levels, apoptosis and inflammation in heart tissueof cardiosurgical patients: a pilot experimental study. Basic Res. Cardiol. 108,314.
Ali, N., Rizwi, F., Iqbal, A., Rashid, A., 2010. Induced remote ischemic pre-conditioning on ischemia-reperfusion injury in patients undergoing coronaryartery bypass. J. Coll. Physicians Surg. Pak. 20, 427–431.
Ali, Z.A., Callaghan, C.J., Lim, E., Ali, A.A., Nouraei, S.A., Akthar, A.M., Boyle, J.R., Varty,K., Kharbanda, R.K., Dutka, D.P., Gaunt, M.E., 2007. RIPC reduces myocardial andrenal injury after elective abdominal aortic aneurysm repair: a randomizedcontrolled trial. Circulation 116, 98–105.
Alreja, G., Bugano, D., Lotfi, A., 2012. Effect of RIPC on myocardial and renal injury:meta-analysis of randomized controlled trials. J. Invasive Cardiol. 24, 42–48.
Anné, W., Willems, R., Roskams, T., Sergeant, P., Herijgers, P., Holemans, P., Ector, H.,Heidbüchel, H., 2005. Matrix metalloproteinases and atrial remodeling inpatients with mitral valve disease and atrial fibrillation. Cardiovasc. Res. 67,655–666.
Babenko, A.P., Aguilar-Bryan, L., Bryan, J., 1998. A view of sur/KIR6.X, KATP channels.Annu. Rev. Physiol. 60, 667–687.
Baines, C.P., Kaiser, R.A., Sheiko, T., Craigen, W.J., Molkentin, J.D., 2007. Voltage-dependent anion channels are dispensable for mitochondrial-dependent celldeath. Nat. Cell Biol. 9, 550–555.
Beavis, A.D., Lu, Y., Garlid, K.D., 1993. On the regulation of Kþ uniport in intactmitochondria by adenine nucleotides and nucleotide analogs. J. Biol. Chem.268, 997–1004.
Bernard, A.M., Vyskocil, A.A., Mahieu, P., Lauwerys, R.R., 1987. Assessment ofurinary retinol-binding protein as an index of proximal tubular injury. Clin.Chem. 33, 775–779.
Błogowski, W., Dołęgowska, B., Sałata, D., Budkowska, M., Domanski, L., Starzyńska,T., 2012. Clinical analysis of perioperative complement activity during ischemia/reperfusion injury following renal transplantation. Clin. J. Am. Soc. Nephrol. 7,1843–1851.
Bøtker, H.E., Kharbanda, R., Schmidt, M.R., Bøttcher, M., Kaltoft, A.K., Terkelsen, C.J.,Munk, K., Andersen, N.H., Hansen, T.M., Trautner, S., Lassen, J.F., Christiansen, E.H.,
Krusell, A.N., Kristensen, S.D., Thuesen, L., Nielsen, S.S., Rehling, M., Sørensen, H.T.,Redington, A.N., Nielsen, T.T., 2010. Remote ischaemic conditioning before hospitaladmission, as a complement to angioplasty, and effect on myocardial salvage inpatients with acute myocardial infarction: a randomised trial. Lancet 375, 727–734.
Brevoord, D., Kranke, P., Kuijpers, M., Weber, N., Hollmann, M., Preckel, B., 2012.Remote ischemic conditioning to protect against ischemia-reperfusion injury: asystematic review and meta-analysis. PLoS One 7, e42179.
Brew, K., Dinakarpandian, D., Nagase, H., 2000. Tissue inhibitors of metalloprotei-nases: evolution, structure and function. Biochim. Biophys. Acta 1477, 267–283.
Cai, Z., Luo, W., Zhan, H., Semenza, G.L., 2013. Hypoxia-inducible factor 1 is requiredfor remote ischemic preconditioning of the heart. Proc. Natl. Acad. Sci. USA 110,17462–17467.
Cai, Z.P., Parajuli, N., Zheng, X., Becker, L., 2012. Remote ischemic preconditioningconfers late protection against myocardial ischemia-reperfusion injury in miceby upregulating interleukin-10. Basic Res. Cardiol. 107, 277.
Camara-Lemarroy, C.R., 2014. Remote ischemic preconditioning as prevention oftransfusion-related acute lung injury. Med. Hypotheses Jun 7. pii: S0306-9877(14)00220-5. http://dx.doi.org/%2010.1016/j.mehy.2014.05.016. (Epub ahead ofprint).
Carlstrom, S., Christensson, B., 1971. Plasma glycerol concentration in patients withmyocardial ischemia and arrhythmias. Br. Heart J. 33, 884–888.
Cauwe, B., Opdenakker, G., 2010. Intracellular substrate cleavage: a novel dimen-sion in the biochemistry, biology and pathology of matrix metalloproteinases.Crit. Rev. Biochem. Mol. Biol. 45, 351–423.
Champattanachai, V., Marchase, R.B., Chatham, J.C., 2008. Glucosamine protectsneonatal cardiomyocytes from ischemia-reperfusion injury via increased pro-tein O-GlcNAc and increased mitochondrial Bcl-2. Am. J. Physiol. Cell Physiol.294, 1509–1520.
Chandrasekar, N., Jasti, S., Alfred-Yung, W.K., Ali-Osman, F., Dinh, D.H., Olivero, W.C.,Gujrati, M., Kyritsis, A.P., Nicolson, G.L., Rao, J.S., Mohanam, S., 2000. Modulationof endothelial cell morphogenesis in vitro by MMP-9 during glial-endothelialcell interactions. Clin. Exp. Metastasis 18, 337–342.
Chen, Y.S., Chien, C.T., Ma, M.C., Tseng, Y.Z., Lin, F.Y., Wang, S.S., Chen, C.F., 2005.Protection “outside the box” (skeletal remote preconditioning) in rat model istriggered by free radical pathway. J. Surg. Res. 126, 92–101.
Cheung, M.M., Kharbanda, R.K., Konstantinov, I.E., Shimizu, M., Frndova, H., Li, J.,Holtby, H.M., Cox, P.N., Smallhorn, J.F., Van Arsdell, G.S., Redington, A.N., 2006.Randomized controlled trial of the effects of RIPC on children undergoing cardiacsurgery: first clinical application in humans. J. Am. Coll. Cardiol. 47, 2277–2282.
Cheung, P.Y., Sawicki, G., Wozniak, M., Wang, W., Radomski, M.W., Schulz, R., 2000.Matrix metalloproteinase-2 contributes to ischemia-reperfusion injury in theheart. Circulation 101, 1833–1839.
Choi, Y.S., Shim, J.K., Kim, J.C., Kang, K.S., Seo, Y.H., Ahn, K.R., Kwak, Y.L., 2011. Effectof RIPC on renal dysfunction after complex valvular heart surgery: a rando-mized controlled trial. J. Thorac. Cardiovasc. Surg. 142, 148–154.
Colantuono, G., Tiravanti, E.A., Di Venosa, N., Cazzato, A., Rastaldo, R., Cagiano, R.,D'Agostino, D., Federici, A., Fiore, T., 2008. Hyperoxia confers myocardialprotection in mechanically ventilated rats through the generation of freeradicals and opening of mitochondrial ATP-sensitive potassium channels. Clin.Exp. Pharmacol. Physiol. 35, 64–71.
Connolly, M., Bilgin-Freiert, A., Ellingson, B., Dusick, J.R., Liebeskind, D., Saver, J.,Gonzalez, N.R., 2013. Peripheral vascular disease as RIPC, for acute stroke. Clin.Neurol. Neurosurg. 115, 2124–2129.
Crimi, G., Pica, S., Raineri, C., Bramucci, E., De Ferrari, G.M., Klersy, C., Ferlini, M.,Marinoni, B., Repetto, A., Romeo, M., Rosti, V., Massa, M., Raisaro, A., Leonardi,S., Rubartelli, P., Oltrona Visconti, L., Ferrario, M., 2013. Remote ischemic post-conditioning of the lower limb during primary percutaneous coronary inter-vention safely reduces enzymatic infarct size in anterior myocardial infarction:a randomized controlled trial. JACC Cardiovasc. Interv. 6, 1055–1063.
Czibik, G., Gravning, J., Martinov, V., Ishaq, B., Knudsen, E., Attramadal, H., Valen, G.,2011. Gene therapy with hypoxia-inducible factor 1 alpha in skeletal muscle iscardioprotective in vivo. Life Sci. 88, 543–550.
Czigany, Z., Turoczi, Z., Onody, P., Harsanyi, L., Lotz, G., Hegedus, V., Szijarto, A.,2013. Remote ischemic perconditioning protects the liver from ischemia-reperfusion injury. J. Surg. Res. 185, 605–613.
D'Ascenzo, F., Cavallero, E., Moretti, C., Omedè, P., Sciuto, F., Rahman, I.A., Bonser, R.S., Yunseok, J., Wagner, R., Freiberger, T., Kunst, G., Marber, M.S., Thielmann, M.,Ji, B., Amr, Y.M., Modena, M.G., Zoccai, G.B., Sheiban, I., Gaita, F., 2012. Remoteischaemic preconditioning in coronary artery bypass surgery: a meta-analysis.Heart 98, 1267–1271.
D'Ascenzo, F., Moretti, C., Omedè, P., Cerrato, E., Cavallero, E., Er, F., Presutti, D.G.,Colombo, F., Crimi, G., Conrotto, F., Dinicolantonio, J.J., Chen, S., Prasad, A.,Biondi Zoccai, G., Gaita, F., 2014. Cardiac remote ischaemic preconditioningreduces periprocedural myocardial infarction for patients undergoing percuta-neous coronary interventions: a meta-analysis of randomised clinical trials.Euro Interv. 9, 1463–1471.
Daut, J., Maier-Rudolph, W., von Beckerath, N., Mehrke, G., Günther, K., Goedel-Meinen, L., 1990. Hypoxic dilation of coronary arteries is mediated by ATP-sensitive potassium channels. Science 247, 1341–1344.
Davies, W.R., Brown, A.J., Watson, W., McCormick, L.M., West, N.E., Dutka, D.P.,Hoole, S.P., 2013. RIPC improves outcome at 6 years after elective percutaneouscoronary intervention: the CRISP stent trial long-term follow-up. Circ. Cardio-vasc. Interv. 6, 246–251.
Diwan, V., Jaggi, A.S., Singh, M., Singh, N., Singh, D., 2008a. Possible involvement oferythropoietin in remote renal preconditioning-induced cardioprotection inrats. J. Cardiovasc. Pharmacol. 51, 126–130.
123456789
101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960616263646566
P. Kaur Randhawa et al. / European Journal of Pharmacology ∎ (∎∎∎∎) ∎∎∎–∎∎∎ 13
Please cite this article as: Kaur Randhawa, P., et al., RIPC for multiorgan salvage in clinical settings: Evolution of concept, evidencesand mechanisms. Eur J Pharmacol (2014), http://dx.doi.org/10.1016/j.ejphar.2014.08.016i

Diwan, V., Kant, R., Jaggi, A.S., Singh, N., Singh, D., 2008b. Signal mechanismactivated by erythropoietin preconditioning and remote renal preconditioning-induced cardioprotection. Mol. Cell. Biochem. 315, 195–201.
Donato, M., Buchholz, B., Rodríguez, M., Pérez, V., Inserte, J., García-Dorado, D.,Gelpi, R.J., 2013. Role of the parasympathetic nervous system in cardioprotec-tion by remote hindlimb ischaemic preconditioning. Exp. Physiol. 98, 425–434.
Er, F., Nia, A.M., Dopp, H., Dahlem, K.M., Caglayan, E., Erdmann, E., Gassanov, N.,Hellmich, M., Burst, V., Kubacki, T., Benzing, T., 2013. Response to letterregarding article, “Ischemic preconditioning for prevention of contrastmedium-induced nephropathy: randomized Pilot RenPro-Trial (Renal Protec-tion Trial)”. Circulation 127, 536.
Facundo, H.T., de Paula, J.G., Kowaltowski, A.J., 2007. Mitochondrial ATP-sensitiveKþ channels are redox-sensitive pathways that control reactive oxygen speciesproduction. Free Radic. Biol. Med. 42, 1039–1048.
Fulop, N., Zhang, Z., Marchase, R.B., Chatham, J.C., 2007. Glucosamine cardioprotec-tion in perfused rat hearts associated with increased O-linked N-acetylgluco-samine protein modification and altered p38 activation. Am. J. Physiol. HeartCirc. Physiol. 292, 2227–2236.
Gao, C.Q., Sawicki, G., Suarez-Pinzon, W.L., Csont, T., Wozniak, M., Ferdinandy, P.,Schulz, R., 2003. Matrix metalloproteinase-2 mediates cytokine-induced myo-cardial contractile dysfunction. Cardiovasc. Res. 57, 426–433.
Gassanov, N., Nia, A.M., Caglayan, E., Er, F., 2014. Remote ischemic preconditioningand renoprotection: from myth to a novel therapeutic option? J. Am. Soc.Nephrol. 25, 216–224.
Gho, B.C., Schoemaker, R.G., van den Doel, M.A., Duncker, D.J., Verdouw, P.D., 1996.Myocardial protection by brief ischemia in noncardiac tissue. Circulation 94,2193–2200.
Ginis, I., Jaiswal, R., Klimanis, D., Liu, J., Greenspon, J., Hallenbeck, J.M., 2002. TNF-alpha-induced tolerance to ischemic injury involves differential control of NF-kB transactivation: the role of NF-kB association with p300 adaptor. J. Cereb.Blood Flow Metab. 22, 142–152.
Gonzalez, N.R., Hamilton, R., Bilgin-Freiert, A., Dusick, J., Vespa, P., Hu, X., Asgari, S.,2013. Cerebral hemodynamic and metabolic effects of RIPC in patients withsubarachnoid hemorrhage. Acta Neurochir. Suppl. 115, 193–198.
Grimaldi, D., Guivarch, E., Neveux, N., Fichet, J., Pène, F., Marx, J.S., Chiche, J.D.,Cynober, L., Mira, J.P., Cariou, A., 2013. Markers of intestinal injury areassociated with endotoxemia in successfully resuscitated patients. Resuscita-tion 84, 60–65.
Gross, E.R., Hsu, A.K., Urban, T.J., Mochly-Rosen, D., Gross, G.J., 2013. Nociceptive-induced myocardial remote conditioning is mediated by neuronal gammaprotein kinase C. Basic Res. Cardiol. 108, 381.
Guo, Z., Turner, C., Castle, D., 1998. Relocation of the t-SNARE SNAP-23 fromlamellipodia-like cell surface projections regulates compound exocytosis inmast cells. Cell 94, 537–548.
Haji, Mohd., Yasin, N.A., Herbison, P., Saxena, P., Praporski, S., Konstantinov, I.E.,2014. The role of RIPC in organ protection after cardiac surgery: a meta-analysis. J. Surg. Res. 186, 207–216.
Hardemark, H.G., Ericsson, N., Kotwica, Z., Rundstrom, G., Mendel-Hartvig, I.,Olsson, Y., Pahlman, S., Persson, L., 1989. S-100 protein and neuron-specificenolase in CSF after experimental traumatic or focal ischemic brain damage.J. Neurosurg. 71, 727–731.
Hausenloy, D.J., Mwamure, P.K., Venugopal, V., Harris, J., Barnard, M., Grundy, E.,Ashley, E., Vichare, S., Di Salvo, C., Kolvekar, S., Hayward, M., Keogh, B.,MacAllister, R.J., Yellon, D.M., 2007. Effect of remote ischaemic preconditioningon myocardial injury in patients undergoing coronary artery bypass graftsurgery: a randomised controlled trial. Lancet 370, 575–579.
Heinen, N.M., Pütz, V.E., Görgens, J.I., Huhn, R., Grüber, Y., Barthuber, C., Preckel, B.,Pannen, B.H., Bauer, I., 2011. Cardioprotection by remote ischemic precondi-tioning exhibits a signaling pattern different from local ischemic precondition-ing. Shock 36, 45–53.
Heusch, G., 2010. RIPC reduces myocardial injury after coronary artery bypasssurgery with crystalloid cardioplegic arrest. Basic Res. Cardiol. 105, 657–664.
Heusch, G., 2013. Cardioprotection: chances and challenges of its translation to theclinic. Lancet 81, 166–175.
Heusch, G., Musiolik, J., Kottenberg, E., Peters, J., Jakob, H., Thielmann, M., 2012.STAT5 activation and cardioprotection by RIPC in humans: short communica-tion. Circ. Res. 110, 111–115.
Hong, D.M., Jeon, Y., Lee, C.S., Kim, H.J., Lee, J.M., Bahk, J.H., Kim, K.B., Hwang, H.Y., 2012.Effects of RIPC with postconditioning in patients undergoing off-pump coronaryartery bypass surgery—randomized controlled trial. Circ. J. 76, 884–890.
Hoole, S.P., Heck, P.M., Sharples, L., Khan, S.N., Duehmke, R., Densem, C.G., Clarke, S.C., Shapiro, L.M., Schofield, P.M., O'Sullivan, M., Dutka, D.P., 2009a. Cardiac RIPCin Coronary Stenting (CRISP Stent) study: a prospective, randomized controltrial. Circulation 119, 820–827.
Hoole, S.P., Khan, S.N., White, P.A., Heck, P.M., Kharbanda, R.K., Densem, C.G., Clarke,S.C., Shapiro, L.M., Schofield, P.M., O'Sullivan, M., Dutka, D.P., 2009b. Remoteischaemic pre-conditioning does not attenuate ischaemic left ventriculardysfunction in humans. Eur. J. Heart Fail. 11, 497–505.
Hu, S., Dong, H.L., Li, Y.Z., Luo, Z.J., Sun, L., Yang, Q.Z., Yang, L.F., Xiong, L., Daut, J.,Maier-Rudolph, W., von Beckerath, N., Mehrke, G., Günther, K., Goedel-Meinen,L., 2010. Effects of RIPC on biochemical markers and neurologic outcomes inpatients undergoing elective cervical decompression surgery: a prospectiverandomized controlled trial. J. Neurosurg. Anesthesiol. 22, 46–52.
Jackson, C., Nguyen, M., Arkell, J., Sambrook, P., 2001. Selective matrix metallopro-teinase (MMP) inhibition in rheumatoid arthritis—targetting gelatinase Aactivation. Inflamm. Res. 50, 183–186.
Jensen, R.V., Zachara, N.E., Nielsen, P.H., Kimose, H.H., Kristiansen, S.B., Bøtker, H.E.,2013. Impact of O-GlcNAc on cardioprotection by remote ischaemic precondi-tioning in non-diabetic and diabetic patients. Cardiovasc. Res. 97, 369–378.
Jones, W.K., Fan, G.C., Liao, S., Zhang, J.M., Wang, Y., Weintraub, N.L., Kranias, E.G.,Schultz, J.E., Lorenz, J., Ren, X., 2009. Peripheral nociception associated withsurgical incision elicits remote nonischemic cardioprotection via neurogenicactivation of protein kinase C signaling. Circulation 120, 1–9.
Jones, S.P., Zachara, N.E., Ngoh, G.A., Hill, B.G., Teshima, Y., Bhatnagar, A., Hart, G.W.,Marbán, E., 2008. Cardioprotection by N-acetylglucosamine linkage to cellularproteins. Circulation 117, 1172–1182.
Jordan, J.E., Zhao, Z.Q., Vinten-Johansen, J., 1999. The role of neutrophils inmyocardial ischemia-reperfusion injury. Cardiovasc. Res. 43, 860–878.
Kanda, T., Fujii, H., Tani, T., Murakami, H., Suda, T., Sakai, Y., Ono, T., Hatakeyama, K.,1996. Intestinal fatty acid-binding protein is a useful diagnostic marker formesenteric infarction in humans. Gastroenterology 110, 339–343.
Kant, R., Bali, A., Singh, N., Jaggi, A.S., 2013. Prolyl 4 hydroxylase: a critical target inthe pathophysiology of diseases. Korean J. Physiol. Pharmacol. 17, 111–120.
Kant, R., Diwan, V., Jaggi, A.S., Singh, N., Singh, D., 2008. Remote renalpreconditioning-induced cardioprotection: a key role of hypoxia induciblefactor-prolyl 4-hydroxylases. Mol. Cell. Biochem. 312, 25–31.
Kapoor, P., Mandal, B., Chowdhury, U., Singh, S., Kiran, U., 2011. Changes inmyocardial lactate, pyruvate and lactate-pyruvate ratio during cardiopulmon-ary bypass for elective adult cardiac surgery: early indicator of morbidity. J.Anaesthesiol. Clin. Pharmacol. 27, 225–232.
Karuppasamy, P., Chaubey, S., Dew, T., Musto, R., Sherwood, R., Desai, J., John, L.,Shah, A.M., Marber, M.S., Kunst, G., 2011. Remote intermittent ischemia beforecoronary artery bypass graft surgery: a strategy to reduce injury and inflam-mation? Basic Res. Cardiol. 106, 511–519.
Keane, M.P., Strieter, R.M., 2000. Chemokine signaling in inflammation. Crit. CareMed. 28, 13–26.
Khanna, G., Diwan, V., Singh, M., Singh, N., Jaggi, A.S., 2008. Reduction of ischemic,pharmacological and remote preconditioning effects by an antioxidant N-acetylcysteine pretreatment in isolated rat heart. Yakugaku Zasshi 128, 469–477.
Kim, J.C., Shim, J.K., Lee, S., Yoo, Y.C., Yang, S.Y., Kwak, Y.L., 2012. Effect of combinedRIPC and postconditioning on pulmonary function in valvular heart surgery.Chest 142, 467–475.
Kobayashi, S.D., DeLeo, F.R., 2009. Role of neutrophils in innate immunity: asystems biology-level approach. Wiley Interdiscip. Rev. Syst. Biol. Med. 1,309–333.
Konstantinov, I.E., Arab, S., Kharbanda, R.K., Li, J., Cheung, M.M., Cherepanov, V.,Downey, G.P., Liu, P.P., Cukerman, E., Coles, J.G., Redington, A.N., 2004. The RIPCstimulus modifies inflammatory gene expression in humans. Physiol. Genomics19, 143–150.
Konstantinov, I.E., Li, J., Cheung, M.M., Shimizu, M., Stokoe, J., Kharbanda, R.K.,Redington, A.N., 2005. Remote ischemic preconditioning of the recipientreduces myocardial ischemia-reperfusion injury of the denervated donor heartvia a Katp channel-dependent mechanism. Transplantation 79, 1691–1695.
Koretzky, G.A., Abtahian, F., Silverman, M.A., 2006. SLP76 and SLP65: complexregulation of signalling in lymphocytes and beyond. Nat. Rev. Immunol. 6,67–78.
Kotlyarov, A., Yannoni, Y., Fritz, S., Laass, K., Telliez, J.B., Pitman, D., Lin, L.L., Gaestel,M., 2002. Distinct cellular functions of MK2. Mol. Cell. Biol. 22, 4827–4835.
Kottenberg, E., Musiolik, J., Thielmann, M., Jakob, H., Peters, J., Heusch, G., 2014.Interference of propofol with signal transducer and activator of transcription5 activation and cardioprotection by RIPC during coronary artery bypassgrafting. J. Thorac. Cardiovasc. Surg. 147, 376–382.
Kristiansen, S.B., Henning, O., Kharbanda, R.K., Nielsen-Kudsk, J.E., Schmidt, M.R.,Redington, A.N., Nielsen, T.T., Botker, H.E., 2005. Remote preconditioningreduces ischemic injury in the explanted heart by a KATP channel-dependentmechanism. Am. J. Physiol. Heart Circ. Physiol. 288, 1252–1256.
Kukielka, G.L., Hawkins, H.K., Michael, L., Manning, A.M., Youker, K., Lane, C.,Entman, M.L., Smith, C.W., Anderson, D.C., 1993. Regulation of intercellularadhesion molecule-1 (ICAM-1) in ischemic and reperfused canine myocardium.J. Clin. Invest. 92, 1504–1516.
Lauzier, B., Vaillant, F., Merlen, C., Gélinas, R., Bouchard, B., Rivard, M.E., Labarthe, F.,Dolinsky, V.W., Dyck, J.R., Allen, B.G., Chatham, J.C., Des Rosiers, C., 2013.Metabolic effects of glutamine on the heart: anaplerosis versus the hexosaminebiosynthetic pathway. J. Mol. Cell. Cardiol. 55, 92–100.
Lee, J.H., Park, Y.H., Byon, H.J., Kim, H.S., Kim, C.S., Kim, J.T., 2012. Effect of remoteischaemic preconditioning on ischaemic-reperfusion injury in pulmonaryhypertensive infants receiving ventricular septal defect repair. Br. J. Anaesth.108, 223–228.
Levy, B., Sadoune, L.O., Gelot, A.M., Bollaert, P.E., Nabet, P., Larcan, A., 2000.Evolution of lactate/pyruvate and arterial ketone body ratios in the early courseof catecholamine-treated septic shock. Crit. Care Med. 28, 114–119.
Li, C., Li, Y.S., Xu, M., Wen, S.H., Yao, X., Wu, Y., Huang, C.Y., Huang, W.Q., Liu, K.X.,2013. Limb RIPC for intestinal and pulmonary protection during elective openinfrarenal abdominal aortic aneurysm repair: a randomized controlled trial.Anesthesiology 118, 842–852.
Li, C., Xu, M., Wu, Y., Li, Y.S., Huang, W.Q., Liu, K.X., 2014. Limb remote ischemicpreconditioning attenuates lung injury after pulmonary resection underpropofol-remifentanil anesthesia: a randomized controlled study. Anesthesiol-ogy 121, 249–259.
Li, L., Luo, W., Huang, L., Zhang, W., Gao, Y., Jiang, H., Zhang, C., Long, L., Chen, S.,2010. Remote perconditioning reduces myocardial injury in adult valve repla-cement: a randomized controlled trial. J. Surg. Res. 164, e21–e26.
123456789
101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960616263646566
P. Kaur Randhawa et al. / European Journal of Pharmacology ∎ (∎∎∎∎) ∎∎∎–∎∎∎14
Please cite this article as: Kaur Randhawa, P., et al., RIPC for multiorgan salvage in clinical settings: Evolution of concept, evidencesand mechanisms. Eur J Pharmacol (2014), http://dx.doi.org/10.1016/j.ejphar.2014.08.016i

Li, Y.Y., McTiernan, C.F., Feldman, A.M., 2000. Interplay of matrix metalloprotei-nases, tissue inhibitors of metalloproteinases and their regulators in cardiacmatrix remodeling. Cardiovasc. Res. 46, 214–224.
Liu, J., Jin, X., Liu, K.J., Liu, W., 2012. Matrix metalloproteinase-2-mediated occludindegradation and caveolin-1-mediated claudin-5 redistribution contribute to blood-brain barrier damage in early ischemic stroke stage. J. Neurosci. 32, 3044–3057.
Liu, J., Marchase, R.B., Chatham, J.C., 2007. Glutamine-induced protection of isolatedrat heart from ischemia/reperfusion injury is mediated via the hexosaminebiosynthesis pathway and increased protein O-GlcNAc levels. J. Mol. Cell.Cardiol. 42, 177–185.
Liu, J., Pang, Y., Chang, T., Bounelis, P., Chatham, J.C., Marchase, R.B., 2006. Increasedhexosamine biosynthesis and protein O-GlcNAc levels associated with myocardialprotection against calcium paradox and ischemia. J. Mol. Cell. Cardiol. 40, 303–312.
Liu, Y., Sato, T., O'Rourke, B., Marban, E., 1998. Mitochondrial ATP-dependentpotassium channels: novel effectors of cardioprotection? Circulation 97,2463–2469.
Lomivorotov, V.V., Shmyrev, V.A., Nepomnyaschih, V.A., Ponomarev, D.N., Knyaz-kova, L.G., Lomivorotov, V.N., Karaskov, A.M., 2012. Remote ischaemic precon-ditioning does not protect the heart in patients undergoing coronary arterybypass grafting. Interact. Cardiovasc. Thorac. Surg. 15, 18–22.
Loukogeorgakis, S.P., Panagiotidou, A.T., Broadhead, M.W., Donald, A., Deanfield, J.E.,MacAllister, R.J., 2005. RIPC provides early and late protection against endothe-lial ischemia-reperfusion injury in humans: role of the autonomic nervoussystem. J. Am. Coll. Cardiol. 46, 450–456.
Loukogeorgakis, S.P., Williams, R., Panagiotidou, A.T., Kolvekar, S.K., Donald, A., Cole,T.J., Yellon, D.M., Deanfield, J.E., MacAllister, R.J., 2007. Transient limb ischemiainduces remote preconditioning and remote postconditioning in humans by a K(ATP)-channel dependent mechanism. Circulation 116, 1386–1395.
Luk, G.D., Vaughan, W.P., Burke, P.J., Baylin, S.B., 1981. Diamine oxidase as a plasmamarker of rat intestinal mucosal injury and regeneration after administration of1-beta-D-arabinofuranosylcytosine. Cancer Res. 41, 2334–2337.
Luo, S.J., Zhou, Y.J., Shi, D.M., Ge, H.L., Wang, J.L., Liu, R.F., 2013. RIPC reducesmyocardial injury in patients undergoing coronary stent implantation. Can. J.Cardiol. 29, 1084–1089.
Manchurov, V., Ryazankina, N., Khmara, T., Skrypnik, D., Reztsov, R., Vasilieva, E.,Shpektor, A., 2014. Remote ischemic preconditioning and endothelial functionin patients with acute myocardial infarction and primary PCI. Am. J. Med. 127,670–673.
Matejíková, J., Ravingerová, T., Pancza, D., Carnická, S., Kolár, F., 2009. MitochondrialKATP opening confers protection against lethal myocardial injury andischaemia-induced arrhythmias in the rat heart via PI3K/Akt-dependent and-independent mechanisms. Can. J. Physiol. Pharmacol. 87, 1055–1062.
Mehta, R.L., Kellum, J.A., Shah, S.V., Molitoris, B.A., Ronco, C., Warnock, D.G., Levin,A., 2007. Acute Kidney Injury Network: report of an initiative to improveoutcomes in acute kidney injury. Crit. Care 11, R31.
Metzsch, C., Liao, Q., Steen, S., Algotsson, L., 2006. Myocardial glycerol release,arrhythmias and hemodynamic instability during regional ischemia-reperfusion in an open chest pig model. Acta Anaesthesiol. Scand. 50, 99–107.
Mohr, A., Chatain, N., Domoszlai, T., Rinis, N., Sommerauer, M., Vogt, M., Müller-Newen, G., 2012. Dynamics and non-canonical aspects of JAK/STAT signalling.Eur. J. Cell Biol. 91, 524–532.
Murry, C.E., Jennings, R.B., Reimer, K.A., 1986. Preconditioning with ischemia: adelay of lethal cell injury in ischemic myocardium. Circulation 74, 1124–1136.
Nagy, T., Champattanachai, V., Marchase, R.B., Chatham, J.C., 2006. Glucosamineinhibits angiotensin II-induced cytoplasmic Ca2þ elevation in neonatal cardi-omyocytes via protein-associated O-linked N-acetylglucosamine. Am. J. Physiol.Cell. Physiol. 290, C57–C65.
Nakano, Y., Niida, S., Dote, K., Takenaka, S., Hirao, H., Miura, F., Ishida, M., Shingu, T.,Sueda, T., Yoshizumi, M., Chayama, K., 2004. Matrix metalloproteinase-9contributes to human atrial remodeling during atrial fibrillation. J. Am. Coll.Cardiol. 43, 818–825.
Ngoh, G.A., Hamid, T., Prabhu, S.D., Jones, S.P., 2009. O-GlcNAc signaling attenuatesER stress-induced cardiomyocyte death. Am. J. Physiol. Heart Circ. Physiol. 297,H1711–H1719.
Ngoh, G.A., Watson, L.J., Facundo, H.T., Dillmann, W., Jones, S.P., 2008. Non-canonical glycosyltransferase modulates post-hypoxic cardiac myocyte deathand mitochondrial permeability transition. J. Mol. Cell. Cardiol. 45, 313–325.
Okubo, S., Wildner, O., Shah, M.R., Chelliah, J.C., Hess, M.L., Kukreja, R.C., 2001. Genetransfer of heat-shock protein 70 reduces infarct size in vivo after ischemia/reperfusion in the rabbit heart. Circulation 103, 877–881.
Olivier-Van Stichelen, S., Guinez, C., Mir, A.M., Perez-Cervera, Y., Liu, C., Michalski, J.C., Lefebvre, T., 2012. The hexosamine biosynthetic pathway and O-GlcNAcylation drive the expression of β-catenin and cell proliferation. Am. J.Physiol. Endocrinol. Metab. 302, E417–E424.
Pan, S.J., Li, L.R., 2011. Adenosine A2 receptors are involved in the activation of ATP-sensitive Kþ currents during metabolic inhibition in guinea pig ventricularmyocytes. Can. J. Physiol. Pharmacol. 89, 187–196.
Park, J., Ann, S.H., Chung, H.C., Lee, J.S., Kim, S.J., Garg, S., Shin, E.S., 2014. RIPC inhemodialysis: a pilot study. Heart Vessel. 29, 58–64.
Paucek, P., Mironova, G., Mahdi, F., Beavis, A.D., Woldegiorgis, G., Garlid, K.D., 1992.Reconstitution and partial purification of the glibenclamide-sensitive, ATP-dependent Kþ channel from rat liver and beef heart mitochondria. J. Biol.Chem. 267, 2606–2609.
Pavione, M.A., Carmona, F., de Castro, M., Carlotti, A.P., 2012. Late RIPC in childrenundergoing cardiopulmonary bypass: a randomized controlled trial. J. Thorac.Cardiovasc. Surg. 144, 178–183.
Pedersen, C.M., Schmidt, M.R., Barnes, G., Botker, H.E., Kharbanda, R.K., Newby, D.E.,Cruden, N.L., 2011. Bradykinin does not mediate remote ischaemic precondi-tioning or ischaemia-reperfusion injury in vivo in man. Heart 97, 1857–1861.
Pedersen, K.R., Ravn, H.B., Povlsen, J.V., Schmidt, M.R., Erlandsen, E.J., Hjortdal, V.E.,2012. Failure of RIPC to reduce the risk of postoperative acute kidney injury inchildren undergoing operation for complex congenital heart disease: a rando-mized single-center study. J. Thorac. Cardiovasc. Surg. 143, 576–583.
Pell, T.J., Baxter, G.F., Yellon, D.M., Drew, G.M., 1998. Renal ischemia preconditionsmyocardium: role of adenosine receptors and ATP-sensitive potassium chan-nels. Am. J. Physiol. 275, H1542–H1547.
Peng, W., Zhang, Y., Zheng, M., Cheng, H., Zhu, W., Cao, C.M., Xiao, R.P., 2010.Cardioprotection by CaMKII-deltaB is mediated by phosphorylation of heatshock factor 1 and subsequent expression of inducible heat shock protein 70.Circ. Res. 106, 102–110.
Peri, F., Piazza, M., Calabrese, V., Damore, G., Cighetti, R., 2010. Exploring theLPS/TLR4 signal pathway with small molecules. Biochem. Soc. Trans. 38,1390–1395.
Peterson, J.T., Li, H., Dillon, L., Bryant, J.W., 2000. Evolution of matrix metallopro-tease and tissue inhibitor expression during heart failure progression in theinfarcted rat. Cardiovasc. Res. 46, 307–315.
Prasad, A., Gössl, M., Hoyt, J., Lennon, R.J., Polk, L., Simari, R., Holmes Jr., D.R., Rihal,C.S., Lerman, A., 2013. Remote ischemic preconditioning immediately beforepercutaneous coronary intervention does not impact myocardial necrosis,inflammatory response, and circulating endothelial progenitor cell counts: asingle center randomized sham controlled trial. Catheter. Cardiovasc. Interv. 81,930–936.
Przyklenk, K., Baurer, B., Ovize, M., Kloner, R.A., Whittaker, P., 1993. Regionalischemic “preconditioning” protects remote virgin myocardium from subse-quent sustained coronary occlusion. Circulation 87, 893–899.
Przyklenk, K., Reduction of myocardial infarct size with Q16ischemic “conditioning”:physiologic and technical considerations. Anesth. Analg. 117, 891–901.
Rahman, I.A., Mascaro, J.G., Steeds, R.P., Frenneaux, M.P., Nightingale, P., Gosling, P.,Townsend, P., Townend, J.N., Green, D., Bonser, R.S., 2010. RIPC in humancoronary artery bypass surgery: from promise to disappointment? Circulation.122, S53–S59.
Rassaf, T., Totzeck, M., Hendgen-Cotta, U.B., Shiva, S., Heusch, G., Kelm, M., 2014.Circulating nitrite contributes to cardioprotection by remote ischemic precon-ditioning. Circ. Res. 114, 1601–1610.
Rehni, A.K., Singh, T.G., 2012. Involvement of CCR-2 chemokine receptor activationin ischemic preconditioning and postconditioning of brain in mice. Cytokine 60,83–89.
Romanic, A.M., Harrison, S.M., Bao, W., Burns-Kurtis, C.L., Pickering, S., Gu, J., Grau,E., Mao, J., Sathe, G.M., Ohlstein, E.H., Yue, T.L., 2002. Myocardial protectionfrom ischemia/reperfusion injury by targeted deletion of matrixmetalloproteinase-9. Cardiovasc. Res. 54, 549–558.
Saes, G.F., Zerati, A.E., Wolosker, N., Ragazzo, L., Rosoky, R.M., Ritti-Dias, R.M.,Cucato, G.G., Chehuen, M., Farah, B.Q., Puech-Leão, P., 2013. RIPC in patientswith intermittent claudication. Clinics (Sao Paulo) 68, 495–499.
Sarkar, K., Cai, Z., Gupta, R., Parajuli, N., Fox-Talbot, K., Darshan, M.S., Gonzalez, F.J.,Semenza, G.L., 2012. Hypoxia-inducible factor 1 transcriptional activity inendothelial cells is required for acute phase cardioprotection induced byischemic preconditioning. Proc. Natl. Acad. Sci. USA 109, 10504–10509.
Saxena, P., Aggarwal, S., Misso, N.L., Passage, J., Newman, M.A., Thompson, P.J.,d'Udekem, Y., Praporski, S., Konstantinov, I.E., 2013. Remote ischaemic pre-conditioning down-regulates kinin receptor expression in neutrophils ofpatients undergoing heart surgeryInteract. Cardiovasc. Thorac. Surg. 17,653–658.
Saxena, P., Shaw, O.M., Misso, N.L., Naran, A., Shehatha, J., Newman, M.A.,d'Udekem, Y., Thompson, P.J., Konstantinov, I.E., 2011. RIPC stimulus decreasesthe expression of kinin receptors in human neutrophils. J. Surg. Res. 171,311–316.
Schulz, R., 2007. Intracellular targets of matrix metalloproteinase-2 in cardiacdisease: rationale and therapeutic approaches. Annu. Rev. Pharmacol. Toxicol.47, 211–242.
Seino, S., 1999. ATP-sensitive potassium channels: a model of heteromultimericpotassium channel/receptor assemblies. Annu. Rev. Physiol. 61, 337–362.
Shahid, M., Tauseef, M., Sharma, K.K., Fahim, M., 2008. Brief femoral arteryischaemia provides protection against myocardial ischaemia-reperfusion injuryin rats: the possible mechanisms. Exp. Physiol. 93, 954–968.
Shimizu, M., Saxena, P., Konstantinov, I.E., Cherepanov, V., Cheung, M.M., Wearden,P., Zhangdong, H., Schmidt, M., Downey, G.P., Redington, A.N., 2010. RIPCdecreases adhesion and selectively modifies functional responses of humanneutrophils. J. Surg. Res. 158, 155–161.
Shuai, K., Ziemiecki, A., Wilks, A.F., Harpur, A.G., Sadowski, H.B., Gilman, M.Z.,Darnell, J.E., 1993. Polypeptide signalling to the nucleus through tyrosinephosphorylation of Jak and Stat proteins. Nature 366, 580–583.
Spinale, F.G., Coker, M.L., Bond, B.R., Zellner, J.L., 2000. Myocardial matrix degrada-tion and metalloproteinase activation in the failing heart: a potential ther-apeutic target. Cardiovasc. Res. 46, 225–238.
Taliyan, R., Singh, M., Sharma, P.L., Yadav, H.N., Sidhu, K.S., 2010. Possible involve-ment of α1-adrenergic receptor and K(ATP) channels in cardioprotective effectof remote aortic preconditioning in isolated rat heart. J. Cardiovasc. Dis. Res. 1,145–151.
Thielmann, M., Kottenberg, E., Kleinbongard, P., Wendt, D., Gedik, N., Pasa, S., Price,V., Tsagakis, K., Neuhäuser, M., Peters, J., Jakob, H., Heusch, G., 2013. Cardio-protective and prognostic effects of remote ischaemic preconditioning in
123456789
101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960616263646566
P. Kaur Randhawa et al. / European Journal of Pharmacology ∎ (∎∎∎∎) ∎∎∎–∎∎∎ 15
Please cite this article as: Kaur Randhawa, P., et al., RIPC for multiorgan salvage in clinical settings: Evolution of concept, evidencesand mechanisms. Eur J Pharmacol (2014), http://dx.doi.org/10.1016/j.ejphar.2014.08.016i

patients undergoing coronary artery bypass surgery: a single-centre rando-mised, double-blind, controlled trial. Lancet 382, 597–604.
Ulrich, N.H., Dehmel, T., Wittsack, H.J., Kieseier, B.C., Seitz, R.J., 2013. Peripheralblood levels of matrix metalloproteinase-9 predict lesion volume in acutestroke. Neurol. Sci. 34, 379–382.
Vibjerg Jensen, R., Johnsen, J., Buus Kristiansen, S., Zachara, N.E., Bøtker, H.E., 2013.Ischemic preconditioning increases myocardial O-GlcNAc glycosylation. Scand.Cardiovasc. J. 47, 168–174.
Walsh, S.R., Boyle, J.R., Tang, T.Y., Sadat, U., Cooper, D.G., Lapsley, M., Norden, A.G.,Varty, K., Hayes, P.D., Gaunt, M.E., 2009. RIPC for renal and cardiac protectionduring endovascular aneurysm repair: a randomized controlled trial. J. Endo-vasc. Ther. 16, 680–689.
Wang, L., Du, F., Wang, X., 2008. TNF-alpha induces two distinct caspase-8activation pathways. Cell 133, 693–703.
Wang, W., Schulze, C.J., Suarez-Pinzon, W.L., Dyck, J.R., Sawicki, G., Schulz, R., 2002.Intracellular action of matrix metalloproteinase-2 accounts for acute myocar-dial ischemia and reperfusion injury. Circulation 106, 1543–1549.
Weinbrenner, C., Schulze, F., Sárváry, L., Strasser, R.H., 2004. Remote precondition-ing by infrarenal aortic occlusion is operative via delta1-opioid receptors andfree radicals in vivo in the rat heart. Cardiovasc. Res. 61, 591–599.
Welbourn, C.R., Goldman, G., Paterson, I.S., Valeri, C.R., Shepro, D., Hechtman, H.B.,1991. Pathophysiology of ischaemia reperfusion injury: central role of theneutrophil. Br. J. Surg. 78, 651–655.
Wesolowski, J., Paumet, F., 2014. Escherichia coli exposure inhibits exocytic SNARE-mediated membrane fusion in mast cells. Traffic 15, 516–530.
Wolfrum, S., Schneider, K., Heidbreder, M., Nienstedt, J., Dominiak, P., Dendorfer, A.,2002. Remote preconditioning protects the heart by activating myocardialPKCepsilon-isoform. Cardiovasc. Res. 55, 583–589.
Wu, J., Feng, X., Huang, H., Shou, Z., Zhang, X., Wang, R., Chen, Y., Chen, J., 2014.Remote ischemic conditioning enhanced the early recovery of renal function inrecipients after kidney transplantation: a randomized controlled trial. J. Surg.Res. 88, 303–308.
Wu, Y.N., Yu, H., Zhu, X.H., Yuan, H.J., Kang, Y., Jiao, J.J., Gao, W.Z., Liu, Y.X., Lou, J.S.,2011. Noninvasive delayed limb ischemic preconditioning attenuates myocar-dial ischemia-reperfusion injury in rats by a mitochondrial K(ATP) channel-dependent mechanism. Physiol. Res. 60, 271–279.
Xie, J.J., Liao, X.L., Chen, W.G., Huang, D.D., Chang, F.J., Chen, W., Luo, Z.L., Wang, Z.P.,Ou, J.S., 2012. Remote ischaemic preconditioning reduces myocardial injury inpatients undergoing heart valve surgery: randomised controlled trial. Heart 98,384–388.
Xing, D., Feng, W., Nöt, L.G., Miller, A.P., Zhang, Y., Chen, Y.F., Majid-Hassan, E.,Chatham, J.C., Oparil, S., 2008. Increased protein O-GlcNAc modification inhibitsinflammatory and neointimal responses to acute endoluminal arterial injury.Am. J. Physiol. Heart Circ. Physiol. 295, H335–H342.
Yang, S., Zou, L.Y., Bounelis, P., Chaudry, I., Chatham, J.C., Marchase, R.B., 2006.Glucosamine administration during resuscitation improves organ function aftertrauma hemorrhage. Shock 25, 600–607.
Yang, Y., Lang, X.B., Zhang, P., Lv, R., Wang, Y.F., Chen, J.H., 2014. Remote ische Q17micpreconditioning for prevention of acute kidney injury: a meta-analysis ofrandomized controlled trials. Am. J. Kidney. Dis. , http://dx.doi.org/10.1053/j.ajkd.2014.04.029 (pii S0272-6386, 00877-4, (Epub ahead of print).).
Young, P.J., Dalley, P., Garden, A., Horrocks, C., La Flamme, A., Mahon, B., Miller, J.,Pilcher, J., Weatherall, M., Williams, J., Young, W., Beasley, R., 2012. A pilot studyinvestigating the effects of RIPC in high-risk cardiac surgery using a randomisedcontrolled double-blind protocol. Basic Res. Cardiol. 107, 256.
Zhao, H.G., Sun, X.C., Xian, X.H., Li, W.B., Zhang, M., Li, Q.J., 2007. The role of nitricoxide in the neuroprotection of limb ischemic preconditioning in rats. Neu-rochem. Res. 32, 1919–1926.
Zhong, H., Gao, Z., Chen, M., Zhao, J., Wang, F., Li, L., Dong, H., Liu, L., Wang, Q.,Xiong, L., 2013. Cardioprotective effect of remote ischemic postconditioning onchildren undergoing cardiac surgery: a randomized controlled trial. Paediatr.Anaesth. 23, 726–733.
Zimmerman, R.F., Ezeanuna, P.U., Kane, J.C., Cleland, C.D., Kempananjappa, T.J.,Lucas, F.L., Kramer, R.S., 2011. Ischemic preconditioning at a remote siteprevents acute kidney injury in patients following cardiac surgery. KidneyInt. 80, 861–867.
Zitta, K., Meybohm, P., Bein, B., Heinrich, C., Renner, J., Cremer, J., Steinfath, M.,Scholz, J., Albrecht, M., 2012. Serum from patients undergoing RIPC protectscultured human intestinal cells from hypoxia-induced damage: involvement ofmatrixmetalloproteinase-2 and -9. Mol. Med. 18, 29–37.
Zografos, T.A., Katritsis, G.D., Tsiafoutis, I., Bourboulis, N., Katsivas, A., Katritsis, D.G.,2014. Effect of one-cycle remote ischemic preconditioning to reduce myocardialinjury during percutaneous coronary intervention. Am. J. Cardiol. 113,2013–2017.
Zou, L., Yang, S., Champattanachai, V., Hu, S., Chaudry, I.H., Marchase, R.B., Chatham,J.C., 2009. Glucosamine improves cardiac function following trauma-hemorrhage by increased protein O-GlcNAcylation and attenuation of NF-{kappa}B signaling. Am. J. Physiol. Heart Circ. Physiol. 296, H515–H523.
123456789
1011121314151617181920212223242526272829303132
P. Kaur Randhawa et al. / European Journal of Pharmacology ∎ (∎∎∎∎) ∎∎∎–∎∎∎16
Please cite this article as: Kaur Randhawa, P., et al., RIPC for multiorgan salvage in clinical settings: Evolution of concept, evidencesand mechanisms. Eur J Pharmacol (2014), http://dx.doi.org/10.1016/j.ejphar.2014.08.016i