Embed Size (px)
Citation preview
S298 The Journal of Heart and Lung Transplantation, Vol 32, No 4S, April 2014
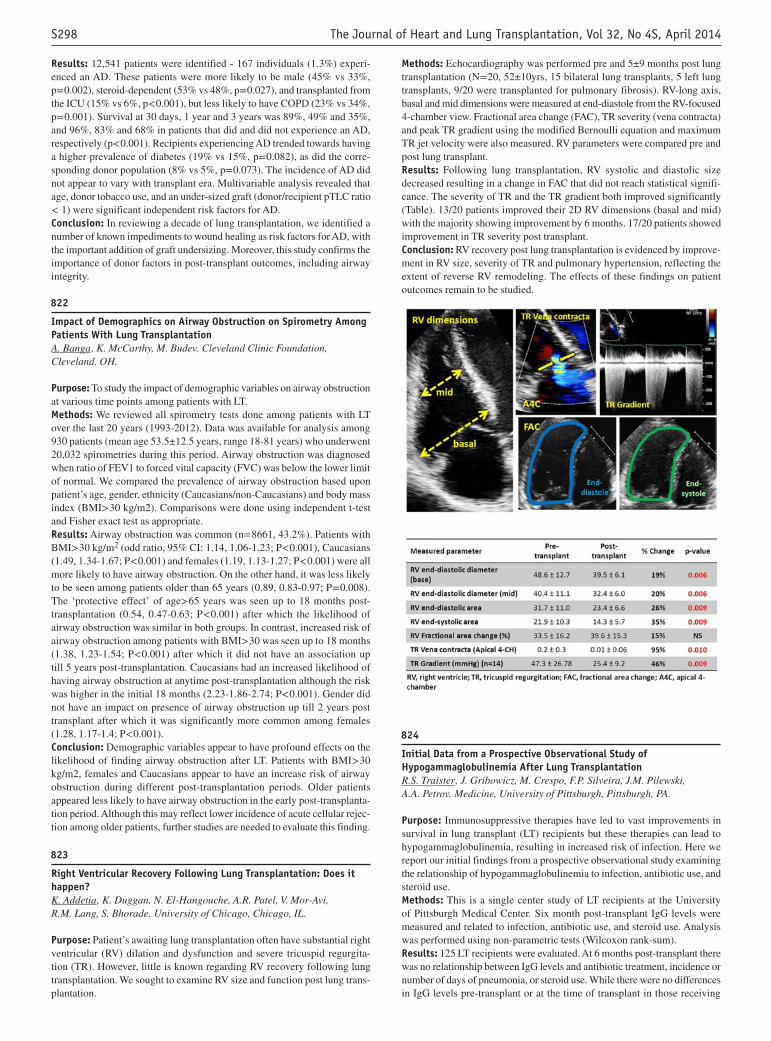
Methods: Echocardiography was performed pre and 5±9 months post lung transplantation (N= 20, 52±10yrs, 15 bilateral lung transplants, 5 left lung transplants, 9/20 were transplanted for pulmonary fibrosis). RV-long axis, basal and mid dimensions were measured at end-diastole from the RV-focused 4-chamber view. Fractional area change (FAC), TR severity (vena contracta) and peak TR gradient using the modified Bernoulli equation and maximum TR jet velocity were also measured. RV parameters were compared pre and post lung transplant.Results: Following lung transplantation, RV systolic and diastolic size decreased resulting in a change in FAC that did not reach statistical signifi-cance. The severity of TR and the TR gradient both improved significantly (Table). 13/20 patients improved their 2D RV dimensions (basal and mid) with the majority showing improvement by 6 months. 17/20 patients showed improvement in TR severity post transplant.Conclusion: RV recovery post lung transplantation is evidenced by improve-ment in RV size, severity of TR and pulmonary hypertension, reflecting the extent of reverse RV remodeling. The effects of these findings on patient outcomes remain to be studied.
(824)
Initial Data from a Prospective Observational Study of Hypogammaglobulinemia After Lung TransplantationR.S. Traister , J. Gribowicz, M. Crespo, F.P. Silveira, J.M. Pilewski, A.A. Petrov. Medicine, University of Pittsburgh, Pittsburgh, PA.
Purpose: Immunosuppressive therapies have led to vast improvements in survival in lung transplant (LT) recipients but these therapies can lead to hypogammaglobulinemia, resulting in increased risk of infection. Here we report our initial findings from a prospective observational study examining the relationship of hypogammaglobulinemia to infection, antibiotic use, and steroid use.Methods: This is a single center study of LT recipients at the University of Pittsburgh Medical Center. Six month post-transplant IgG levels were measured and related to infection, antibiotic use, and steroid use. Analysis was performed using non-parametric tests (Wilcoxon rank-sum).Results: 125 LT recipients were evaluated. At 6 months post-transplant there was no relationship between IgG levels and antibiotic treatment, incidence or number of days of pneumonia, or steroid use. While there were no differences in IgG levels pre-transplant or at the time of transplant in those receiving
Results: 12,541 patients were identified - 167 individuals (1.3%) experi-enced an AD. These patients were more likely to be male (45% vs 33%, p= 0.002), steroid-dependent (53% vs 48%, p= 0.027), and transplanted from the ICU (15% vs 6%, p< 0.001), but less likely to have COPD (23% vs 34%, p= 0.001). Survival at 30 days, 1 year and 3 years was 89%, 49% and 35%, and 96%, 83% and 68% in patients that did and did not experience an AD, respectively (p< 0.001). Recipients experiencing AD trended towards having a higher prevalence of diabetes (19% vs 15%, p= 0.082), as did the corre-sponding donor population (8% vs 5%, p= 0.073). The incidence of AD did not appear to vary with transplant era. Multivariable analysis revealed that age, donor tobacco use, and an under-sized graft (donor/recipient pTLC ratio < 1) were significant independent risk factors for AD.Conclusion: In reviewing a decade of lung transplantation, we identified a number of known impediments to wound healing as risk factors for AD, with the important addition of graft undersizing. Moreover, this study confirms the importance of donor factors in post-transplant outcomes, including airway integrity.
(822)
Impact of Demographics on Airway Obstruction on Spirometry Among Patients With Lung TransplantationA. Banga , K. McCarthy, M. Budev. Cleveland Clinic Foundation, Cleveland, OH.
Purpose: To study the impact of demographic variables on airway obstruction at various time points among patients with LT.Methods: We reviewed all spirometry tests done among patients with LT over the last 20 years (1993-2012). Data was available for analysis among 930 patients (mean age 53.5±12.5 years, range 18-81 years) who underwent 20,032 spirometries during this period. Airway obstruction was diagnosed when ratio of FEV1 to forced vital capacity (FVC) was below the lower limit of normal. We compared the prevalence of airway obstruction based upon patient’s age, gender, ethnicity (Caucasians/non-Caucasians) and body mass index (BMI> 30 kg/m2). Comparisons were done using independent t-test and Fisher exact test as appropriate.Results: Airway obstruction was common (n= 8661, 43.2%). Patients with BMI> 30 kg/m2 (odd ratio, 95% CI: 1.14, 1.06-1.23; P< 0.001), Caucasians (1.49, 1.34-1.67; P< 0.001) and females (1.19, 1.13-1.27; P< 0.001) were all more likely to have airway obstruction. On the other hand, it was less likely to be seen among patients older than 65 years (0.89, 0.83-0.97; P= 0.008). The ‘protective effect’ of age> 65 years was seen up to 18 months post-transplantation (0.54, 0.47-0.63; P< 0.001) after which the likelihood of airway obstruction was similar in both groups. In contrast, increased risk of airway obstruction among patients with BMI> 30 was seen up to 18 months (1.38, 1.23-1.54; P< 0.001) after which it did not have an association up till 5 years post-transplantation. Caucasians had an increased likelihood of having airway obstruction at anytime post-transplantation although the risk was higher in the initial 18 months (2.23-1.86-2.74; P< 0.001). Gender did not have an impact on presence of airway obstruction up till 2 years post transplant after which it was significantly more common among females (1.28, 1.17-1.4; P< 0.001).Conclusion: Demographic variables appear to have profound effects on the likelihood of finding airway obstruction after LT. Patients with BMI> 30 kg/m2, females and Caucasians appear to have an increase risk of airway obstruction during different post-transplantation periods. Older patients appeared less likely to have airway obstruction in the early post-transplanta-tion period. Although this may reflect lower incidence of acute cellular rejec-tion among older patients, further studies are needed to evaluate this finding.
(823)
Right Ventricular Recovery Following Lung Transplantation: Does it happen?K. Addetia , K. Duggan, N. El-Hangouche, A.R. Patel, V. Mor-Avi, R.M. Lang, S. Bhorade. University of Chicago, Chicago, IL.
Purpose: Patient’s awaiting lung transplantation often have substantial right ventricular (RV) dilation and dysfunction and severe tricuspid regurgita-tion (TR). However, little is known regarding RV recovery following lung transplantation. We sought to examine RV size and function post lung trans-plantation.




























![Kidney Transplantation (Renal Transplantation) Auto Saved]](https://img.pdfslide.us/doc/110x75/577d22b31a28ab4e1e9807d7/kidney-transplantation-renal-transplantation-auto-saved.jpg)
