Embed Size (px)
Citation preview
Pulmonary Hypertension and Venous Thrombo-embolic Disease
A1479JACC April 1, 2014
Volume 63, Issue 12
RigHt ventRicUlaR RecoveRy following lUng tRansPlantation: does it HaPPen?
Poster ContributionsHall CSaturday, March 29, 2014, 10:00 a.m.-10:45 a.m.
Session Title: Pulmonary Hypertension and Pulmonary Thrombo-embolic Disease IAbstract Category: 23. Pulmonary Hypertension and Pulmonary Thrombo-embolic DiseasePresentation Number: 1116-212
Authors: Karima Addetia, Karen Duggan, Nadia El Hangouche, Sangeeta Bhorade, Victor Mor-Avi, Roberto Lang, Amit Patel, University of Chicago, Chicago, IL, USA
Background: Patient’s awaiting lung transplantation often have substantial right ventricular (RV) dilation and dysfunction and severe tricuspid regurgitation (TR). However, little is known regarding RV recovery following lung transplantation. We sought to examine RV size and function post lung transplantation
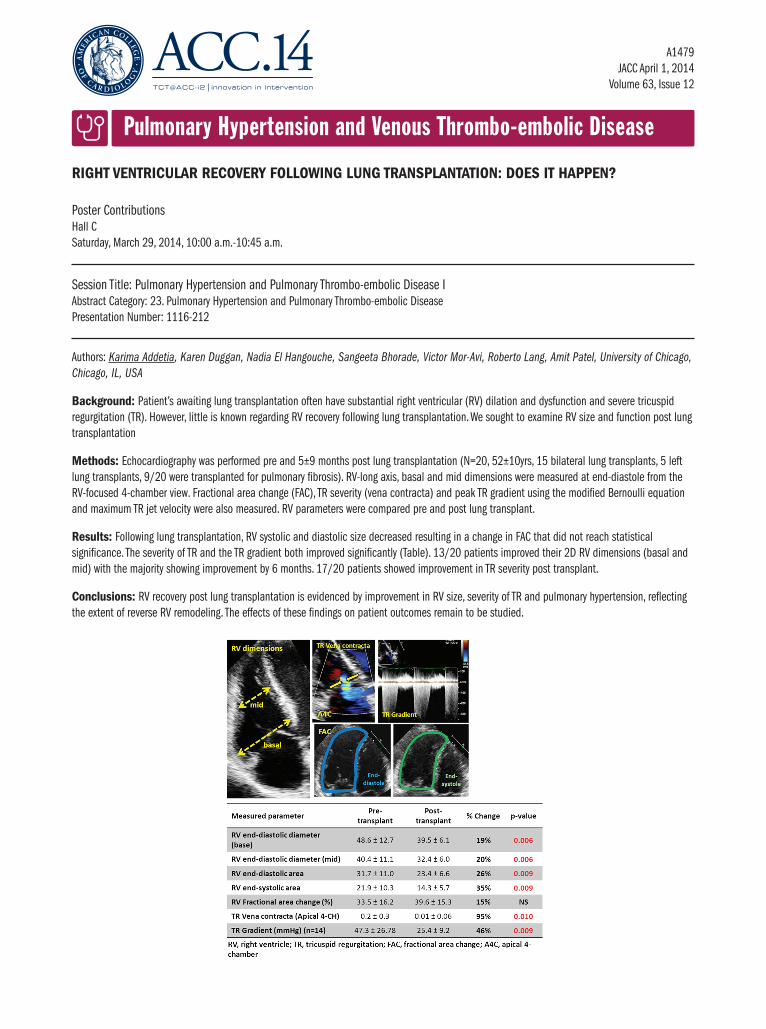
methods: Echocardiography was performed pre and 5±9 months post lung transplantation (N=20, 52±10yrs, 15 bilateral lung transplants, 5 left lung transplants, 9/20 were transplanted for pulmonary fibrosis). RV-long axis, basal and mid dimensions were measured at end-diastole from the RV-focused 4-chamber view. Fractional area change (FAC), TR severity (vena contracta) and peak TR gradient using the modified Bernoulli equation and maximum TR jet velocity were also measured. RV parameters were compared pre and post lung transplant.
Results: Following lung transplantation, RV systolic and diastolic size decreased resulting in a change in FAC that did not reach statistical significance. The severity of TR and the TR gradient both improved significantly (Table). 13/20 patients improved their 2D RV dimensions (basal and mid) with the majority showing improvement by 6 months. 17/20 patients showed improvement in TR severity post transplant.
conclusions: RV recovery post lung transplantation is evidenced by improvement in RV size, severity of TR and pulmonary hypertension, reflecting the extent of reverse RV remodeling. The effects of these findings on patient outcomes remain to be studied.






















![Kidney Transplantation (Renal Transplantation) Auto Saved]](https://img.pdfslide.us/doc/110x75/577d22b31a28ab4e1e9807d7/kidney-transplantation-renal-transplantation-auto-saved.jpg)






