Embed Size (px)
Citation preview
RIACH RESOURCES
FOR. CHILD
H E A LT H
MotheKraii
MATERNAL TETANUS: MAGNITUDE, EPIDEMIOLOGY AND CONTROL
OF A NEGLECTED CAUSE OF
MATERNAL MORTALITY
REACH/MotherCare
1A,
Al' o
All
Maternal Tetanus:
Magnitude, Epidemiology and Control
of a Neglected Cause of
Maternal Mortality
REACH/MotherCare
Vincent Fauveau, MD, MPH Masuma Mamdani, MPH Robert Ste.iglass, MPH
Marjorie A. Koblinsky, PhD
REACH 1616 N. Foit Myer Drive, llth Floor
Arlington, VA 22209 USA
A.I.D. Contract No.: DPE 5982-Z-00-9034
MotherCare 1616 N. Fort Myer Drive, 11th Floor
Arlington, VA 22209 USA
A.I.D. Contract No.: DPE 5966-Z-00-8083-00
ACKNOWLEDGEMENTS
This study was initiated and funded by the Resources for Child Health (REACH) and MotherCare Projects of John Snow, Inc. under contracts (numbers DPE 5982-Z-00-9034-00 and DPE 5966-Z-00-8083-00) with the United States Agency for International Development. The assistance of Dr. A. Galazka, Dr. J. Lawson, and Robert Weierbach in reviewing the manuscript was greatly appreciated. Special thanks also to Nancy Cylke, JSI Librarian, for checking references and to Paul Boyum of the REACH Project for editing.
Cover drawings are provided courtesy of the World Health Organization.
TABLE OF CONTENTS
ABSTRACT ....................................... ......... i
A. INTRODUCTION ........................................... 1
B. SOURCES OF DATA ........................................ 1
C. ETIOLOGY AND PATHOGENESIS ............................... 2
D. CLINICAL FEATURES ....................................... 2 D . 1. Incubation .......................................... 2 D.2. Symptoms and complications ............................... 3 D .3. Case fatality ......................................... 3 D.4. Differential diagnosis ................................... 3
E. EPIDEMIOLOGY: DISTRIBUTION AND RISK FACTORS .................. 4 E. 1. Geographic distribution of matemal tetanus ........................ 4
E.1.1. Asia ...... ................ ... ............... 4 E.1.2. Africa ....................................... 4 E.1.3. South America and the Caribbean . ...................... 5
E.2. Distribution of tetanus spores .................................. 5 E.3. Distribution of pregnancies', abortions, and traditional practices .......... 5
E.3.1. Health services (access, utilization & quality of care) .......... 6 E.4. Distribution of portals of entry .............................. 6 E.5. Age, parity. m~r:al status ..... ........................... 7 E.6. Socioeconomic status .................................... 7 E.7. Seasonal variation ..................................... 8 E.8. Relationship with neonatal tetanus ............................ 8 E.9. Reporting problems and extrapolation attempts .................... 8
F. CONTROL MEASURES ........................................... 8 F.1. Curative measures ..................................... 8 F.2. Preventive measures ..................................... 9
TABLE 1: Maternal tetanus studies reviewed ............................. 11
TABLE 2: Etiologic distribution of maternal tetanus in published studies ............ 12
TABLE 3: Case fatality ratios (CFRs) .................................. 13
TABLE 4: Proportion of maternal deaths due to maternal tetanus ................ 14
REFERENCES ............................................... 15
ABSTRACT
Maternal tetanus, defined as tetanus occurring during pregnancy or within six weeks after any typeof pregnancy termination, is one of the most easily preventable causes of maternal mortality. It includes postpartum or puerperal tetanus resulting from septic procedures during delivery,postabortal tetanus resulting from septic abortion, and tetanus incidental to pregnancy, resulting from any type of wound during pregnancy. The magnitude of its contribution to maternal mortalityin developing countries is unclear and probably underestimated by the few community-nased studies that have reported cases so far.
This review of published and unpublished hospital and community studies concludes that: between 15,000 and 30,000 cases of maternal tetanus occur each year with a predominance of postpartum or puerperal cases; the number of postabortal tetanus cases reported is as largely underestimated as the number of induced abortions; the case fatality ratio is on the zverage 75% in the absence of treatment; tetanus antitoxin and cleaning of the wounded portal of entry are key components of case management, and; universal and adequate coverage of repiroductive-aged women by tetanus toxoid is the most cost-effective way to eliminate this often neglected cause of maternal death. The extent to which political and financial resources are mobilized will determine whether or not 150,000 to 300,000 women will die of maternal tetanus during the 1990's.
A. INTRODUCTION
The World Health Organization estimates that 500,000 women die annually from complications of pregnancy, abortion and childbirth, 99% of them in developing countries (WHO 1986). In view of te magnitude of the problem of maternal mortality, it is tempting to focus on the few specific causes, if any, that can be averted through simple and effective control measures. Maternal tetanus is one of them, but the importance of its contribution to maternal mortality and morbidity is still unknl3wn. We define as maternal tetanus any case of clinical tetanus occurring to a woman during pregnancy or during the six weeks following the termination of a pregnancy, regardless of the way it was terminated. This definition, in line with the recent discussions on the definition of a maternal death, includes three main categories that we propose as a convenient classification for future comparativestudies: i/ postpartum or puerperal tetanus (PPT), usually resulting from septic proceduresduring delivery, ii/ postabortal tetanus (PAT),, following septic maneuvers during induced abortion, and iii/ tetanus during pregnancy (PRT), generally a result of inoculation through a non-genital portal of entry. This latter category is included in the definition for three reasons: it is often accounted for in studies of maternal mortality and may represent a sizeable proportion of maternal tetanus in certain settings; it is often impossible to determine the underlying cause of the inoculation (i.e. pregnancy or concomitan: cause); and this category shares similar management and preventive features as the other two.
To date, much attention has been focused on neonatal tetanus and very littie is known about maternal tetanus. As part of a World Bank review of health sector priorities for the 1990s,Steinglass et al. (1991) calculated a preliminary estimate of 30,000 women dying annuallyfrom maternal tetanus, and called for a global review of the problem. The last publishedreviews of the subject date from 1941 for postabortal tetanus (Weinstein & ..-nctham) and from 1955 for puerperal tetanus (Adams & Morton).
Yet maternal tetanus is completely preventable if efforts are made to ,,each complete coverage of reproductive-aged women with adequate tetanus vaccination. The paucity of publications on maternal tetanus in the infectious disease literature as well as in the maternal health literature reflects the relative state of neglect of the issue. This may be due in part to the absence of good epidemiological surveillance and good clinical data in areas where the disease is most common, and in part to the sensitive and confidential nature of this disease, often the result of an illegal abortion. In this paper we review published and unpublished studies of maternal tetanus in the developing world, estimate the magnitude of the problem worldwide, describe distribution and risk factors, summarize clinical and therapeutic patterns, and discuss specific control measures.
B. SOURCES OF DATA
There are four distinct sources of data concerning maternal tetanus: 1/ hospital studies analyzing series of admissions and deaths in tetanus-specialized wards; 2/ single case studies published in obstetric or infectious disease literature and relating unusual forms; 3/hospital-based studies of maternal deaths occurring in obstetric wards; and 4/ community-based studies analyzing maternal deaths collected through surveillance systems.Table 1 summarizes the distribution by type of the 60 studies from developing countries reviewed for this assessment (not all of them reported cases of maternal tetanus). In addition, seven studies ieporting maternal tetanus in developed countries were also reviewed. The earliest report of puerperal tetanus was that by Sepet (1898) who reviewed 125 cases for the Congress of Gynecology and Obstetrics in Marseilles, France. In the present review, we found a total of 1101 published cases of maternal tetanus reported from developing
1
countries between 1958 and 1990, and an additional 21 cases reported from developedcountries between 1941 and 1964. Out of the cases reported from developing countries,47% were found in India, 4% in Bangladesh, 1%in other Asian countries, 34% in Nigeria,9% in Senegal, 3% in other parts of Africa, and 1% in Latin America. Details of clinical patterns, including portal of entry and case fatality, are available for 484 cases (44% of the total), The etiologic distribution of maternal tetanus in published studies specifying this information is as follows: 67% postpartum, 27% postabortal, and 6% incidental to pregnancy (Table 2).
C. ETIOLOGY AND PATHOGENESIS
Tetanus is due to an ubiquitous, gram-positive, rod-shaped, anaerobic, spore-formingbacillus called Clostridium tetani. It has the property of producing an exotoxin called tetanospasmin, which is responsible for all the clinical symptoms of the disease. Its natural habitat is soil, mostly moist and rich soil manured by animal feces. The bacillus is found in the feces of most mammals, principally horses and cows but also sheep and goats. Under environmentally harsh conditions, it forms spores that are extremely resistant to physical and chemical destruction and can survive many years in dirt and dust. Boiling, autoclaving less than ten minutes, and cleaning instruments with quaternary ammonium compounds, alcohol or phenol does not kill tetanus spores. Tetanus infection results from the introduction of spores in the body through accidental or surgical wound, or through the genital tract. Once in a wet, poorly oxygenated, necrotic tissue such as retained placenta, spores germinate and start producing toxins. These toxins progress along neural paths to reach the spinal cord and the central nervous system where they affect the control of vital functions.
D. CLINICAL FEATURES
D.I. Incubation
The incubation period is the time between the introduction of spores in the body and the first clinical symptoms. It vari's from a few days (not less than three) to several weeks. The duration of incubation is deteimined by the distance between the portal of entry and the central nervous sytem, .he intensity of infection, and a number of defense mechanisms. In turn, the duration uf incubation, as well as the interval between first symptoms and generalised spasms (the period of onset) determine the seuerity of the disease and thefefore the prognosis. These factors also determine the length of time spent in the hospital and the cost of treatment (Bennett 1976; Newman et al 1975; Vaishnava et al 1964). In a review of17 postabortal tetanus patients in South Africa, the mean incubation period was 11.8 days,with a range of between 4 and 42 days; the mean duration of stay in hospital was 36.7 days,ranging from 15 to 55 day,, (BenneL( 1976). A definite inverse relationship was noted between the time the symptoms took to develop, and the duration of stay in hospital. In addition, in all three patieaits who died, the symptoms of tetanus started less than 10 daysafter the abortion. Iii a hospital-based study in Nigeria, the duration of the disease frorn the time of admission until death varied from a few hours to 50 days, with 9 out of 12 deaths occurring within 10 days (Adadevoh & Akinla 1970). The average duration of incubation and hospitalization for the 14 postpartum tetanus cases observed in Dakar, Senegal, were 17 and 26 days respectively (Diop-Mar et al. 1985). According to Chen et al (1974), who reported three cases of postpartum tetanus in Bangladesh, the incubation period ranged from two to three weeks.
2
D.2. Symptoms and complications
The clinical diagnosis of maternal tetanus is generally not as straightforward as that of neonatal tetanus, because there are several clinical forms which can be misleading, particularly in the early stages of the disease. There were three degrees of severity in the cases reviewed. The mild forms had long incubation periods, and trismus (lockjaw), neck stiffness and risus sardonicus were the only symptoms. There were no convulsions and no general toxic disturbances such as hyperpyrexia. The prognosis was generally good with no case fatality. Moderate forms were characterized by generalized spasmodic contractions with opisthotonus, but they were only provoked by externalstimuli such as skin punctures,naso-pharyngeal suction, loud noise or intense light. There was abdominal pain and backache, but no fever. The prognosis was less good. In the severe forms, with short incubation periods, generalized convulsions were spontaneous and long-lasting, with frequent episodes of apnea, cyanosis and asphyxia. There were central nervous system disturbances such as hyperpyrexia, tachycardia or cardiac arrest. Even with specialized intensive care including respiratory assistance, the prognosis was extremely poor. Vaginal bleeding and discharge were found in all postpartum and postabortal cases, although bacteriological examination of the vaginal discharge did not help in the diagnosis.
D.3. Case ftEality
In this review, the case fatality ratio (CFR), defined as the ratio of deaths over one hundred diagnosed cases, had a median of 52% (range 16-80) in hospital studies in Africa and 54% (range 42-64) in Asia (Table 3). The lowest reported figures were 16% in Cape Town, reportedly due to the presence of an intensive care unit (Benett 1976). Other hospital studies reported moderate CFRs of 20% in Tanzania (Ayim 1972), 45% in Nigeria (Adeuja & Osuntokun 1971), 44% in Nigeria (Adadevoh & Akinla 1970), 50% and 33% in India (Vakil 1976, cited in Bytchenko 1966), and 48% in Senegal (Rey 1968). CFRs as high as 64% were reported by Patel in India (cited in Bytchenko 1966), 72% by Bhatt & Anwikar in India (1962). Earlier reviews of maternal tetanus in Europe and the USA before 1960 showed CFRs of between 57% and 85% in postabortal tetanus and between 75% and 100% in postpartum tetanus (Weinstein & Beachem 1941, Adams & Morton 1955). In contrast, CFRs in this review were generally lower for postpartum tetanus than for postabortal tetanus. This is probably because the former were referred to hospital at a relatively earlier stage and thus had less associated bacterial infection, and also because illegaly induced abortion carries a greater degree of cortamination.
D.4. Differential diagnosis
The diagnosis of maternal tetanus in its mild form (lockjaw) must exclude dental and pharyngeal abscesses, mandibular fracture or arthritis, diphtheria and mumps. In the more severe forms with opisthotonos and generalized symptoms, it is necessary to exclude meningitis, strychnine poisoning, epilepsy, tetany, hysteria, retroperitoneal abscess, and rabies. In case of a postabortal tetanus, other septic complications of induced abortion must also be considered, including septicemia due to Clostridium perfringens. In community-based studies the cause of death is assessed retrospectively by interviewing relatives and attendants about symptoms preceding death. Confusion between eclamptic and tetanic fits is conceivable, particularly during the period between 2 and 14 days after delivery. Precise information on timing of symptoms is crucial, however, because postpartum eclampsia rarely occurs more than 4 days after delivery, while postpartum tetanus cannot occur earlier than 4 days after delivery.
3
E. EPIDEMIOLOGY: DISTRIBUTION AND RISK FACTORS
The distribution of maternal tetanus depends on the distribution of spores, of pregnancies,and of accidental contact between spores and pregnant or postpartum women.
E.1. Geographic distribution of maternal tetanus
E.I.1. Asia
Several community-based maternal mortality studies undertaken in Bangladesh between 1967 and 1985 - four in Matlab and one in Jamalpur district - renorted that between one and about 10% of the maternal deaths were due to tetanus, mainly postpartum (Chen et al. 1974, Fauveau et al. 1988, Lindpainter et al. 1982, Khan et al. 1986a; Table 4). In these studies, lefanus-attributable maternal mortality rates ranged from 9 to 56 per 100,000 live births. Results of othercommunity-based studies undertaken in Indonesia (Fortney et al. 1988) and India (Bbatia et al. 1986) showed between 4.7% and 2.8% of the maternal deaths to be due to postpartum tetanus; tetanus-attributable maternal mortality rates were 34 and 22 per100,000 live births, respectively.
Several hospital-based studies undertaken during the early 1960s in Asia - seven in India and one each in Japan Singapore, and Vietnam - have shown that postpartum and postabortal tetanus collectively accounted for between 3.3% and 22.2% (3 to 113 cases) of all cases of tetanus, with high CFRs rznging fiom 64% to 72% (quoted in Bytchenko 1966).In a review of 981 tetanus patients admitted to one New Delh. hospital from 1963 to 1965, Suri (1967) noted that postabortal and postpartum tetanus accounted for 47% of the 150 cases occurring in women 15 to 50 years of age, 25% of the 280 female non-neonatal cases, and 7% of all tetanus cases.
E.1.2. Africa
There was only one community-based study (in Menoufia, Egypt) where 0.2% of all maternal deaths were reported to be due to postpartum tetanus (Fortney et al. 1988; Gadalla et al. 1987). The tetanus attributable maternal mortality rate was about 4 per 100,000 live births.
Most cf the available dckta for Africa is from hospital-based studies, mainly from Nigeriawhere from 1% to 10% of the maternal deaths were due to tetanus. In one Nigerianhospital-based study, of the 72 tetanus patients in whom the uterus was determined to be the portal of entry, 52 (72%) contracted postpartum tetanus following unhygienic delivery at home, and 12 (16.7%) developed tetanus following illegally induced abortion (Adeuja & Osuntokun 1971). Maternal tetanus accounted for 20% of the 100 cases of tetanus treated at Ibadan, Nigeria, in 1954-55 (Johnstone 1958).
Reported cases of postabortal tetanus appear to be more common in Africa than in Asia. In a review of 12,736 cases of abortion admitted over a 15-year period (1972-1986) in one Nigerian hospital, 0.4% (53) were reported to have died of illegally induced abortion and 3.8% (2) of these deaths were due to tetanus (Adetoro 1989). Between January 1965 and June 1972, a total of 13,681 patients with incomplete abortions were admitted to Groote Schuur Hospital in Cape Town, South Africa (Bennett 1976). The reported incidence of postabortal tetanus was 1.3% of all incomplete abortions, accounting for 34.7% of all cases of tetanus in women of childbearing age; the CFR was about 17.6%, which appears to be the lowest reported so far. In another study in Nigeria, of the 27 cases of maternal tetanus ;xe,- at Lagos University Teaching Hospital between 1963 and 1967, 81 % were postabortal
4
following illegally induced abortion (Adadevoh & Akinla 1970). The CFR was 20% for postpartum tetanus and 52% for postabortal tetanus. In Zaria, Northern Nigeria, Harrison (1985) reported 4 out of 219 maternal deaths (1.8%) to be due to tetmius.
E.1.3. Soath America and the Caribbean
There is not much information available on maternal tetanus in the Caribbean. We found one case report of tetanus following an unsafe abortion in Barbados (Newman et al. 1975).As tie ratio of abortion to live births is high in Latin America (Rochat et al. 1985), it maybe fair to assume that relatively more maternal tetanus is postabortal rather than postpartum. There was only one community-based study from Brazil where nostabortal tetanus accounted for about 5% of the non-neonatal cases of tetanus (Tavares 1980).
E.2. Distribution of tetanus spores
While factors influencing the distrit-ution of C. tetani spores in human environments are not fully known, some climates, soils, and agricultural economies, particularly those raisingcattle, are associated with higher risk than others (Bytchenko 1966). In fact, in some placesthe incidence of tetanus in animals may be a useful indirect indicator of potential human risk (Schofield 1986). Alternatively, the presence and density of cattle in a rural environment might be used as a presumptive risk of developing tetanus (Smucker et al. 1980). In general, unimmunized rural populptions are said to develop tetanus at higher rates than urban populations (Suri 1967, Suleiman 1982).
E.3. Distribution of pregnancies. abortion, and traditional Dractict.9
The overall numbers and rates of pregnancies are in general highest in the poorest regionsof the developing world and, within these regions, in the poorest socioeconomic classes. In these groups, means to limit family size and to space pregnancies are not available, or not utilized, or limited to traditional and frequently unsafe practices. Though abortion is illegal in a number of developing countries -- Ethiopia, Mexico, Nigeria, Bangladesh, etc. - large numbers of abortions are performed, particularly in the rural areas, by unqualifiedmedical practitioners (Khan et al. 1984, Lawson et al. 1990, Liskin 1980, Adetoro 1989).Even where abortion laws are less restrictive, as in India, abortion services are not alwaysreadily available ard abortion-related morbidity and mortality appears to be quite common (Bhatia 1985, Dutta 1980). The most frequent major complication of unsafe abortion includes infection and bleeding linked to incomplete abortions and/or introduction of bacteria into the uterus (Editorial 1989, Liskin 1980). In sub-Saharan Africa and India, tetanus is reported to be a major complication and is usually fatal (Liskin 1980). In the absence of timely and effective medical back-up, the resulting morbidity and mortality associated with these complications is high, and at times may lead to the removal of the damaged uterus. Invariably, reported incidence of deaths or complications due to induced abortions is underestimated. During 1984-85 in Ananthapur, India, hospital-based deaths due to septicabortions accounted for 7.5% and 12.5% of maternal deaths in urban and rural patientsrespectively (Bhatia 1985). Of the maternal deaths occurring in rural homes, 17.2% were due to septic abortion. Postabortal sepsis (21 %) was one of the major causes of maternal mortality in southern Tanzania (Price 1984). A number of studies from Latin America have shown that from 30% to 40% of maternal deaths may be due to ,omplications of illegalabortions (Kwast 1987). Similar results are shown in the available community-basedmaternal mortality studies. During 1982-83, septic abortion accounted for 17% of all maternal deaths in Tangail p:.trict (Alauddin 1986) and for 21 % in Jamapur District of Bangladesh (Khan et al. 1986a). In a study in Addis Ababa, Ethiopia, septic abortion, accounting for 54% of direct obstetric deaths, was noted to be the main cause of maternal mortality (Kwast et al. 1986). A majority (92%) of them were illegally induced. Overall,
5
based on a survey covering 60 developing countries in 1977, Rochat et al. (1980) estimated that about 13.7 million induced aborions occur each year, yielding a ratio of 207 abortions per 1000 live births ranging from 9 in East Africa to 325 in Latin America. It is likely that the incidence of postabortal tetanus closely follows the incidence of septic abortion, thoughmuch of both goes unreported.
A majority of the births in most developing countries, in particular in the rural areas, takes place at home, usually assisted by relatives or traditional birth attendants (TBAs). A varietyof beliefs and customs applied at childbirth tend to carry high risks of maternal mortalityand morbidity (Lettenmaier et al. 1988). Frequent vaginal examinations with unclean hands, and the application of dung and herbal medicines to the vulva or the vagina are some of the practices which may cause genital infection and tetanus in the postpartum period. In a hospital-based study in Delhi, almost all the postpartum cases of tetanus occurred among women whose deliveries were assisted at h3me by TBAs; CFR in this group was 59% as compared to 40% in non-postpartum women with tetanus in the same age group (Vaishnava et al. 1964). It is noteworthy that about 80% of the postpartum cases came from rural areas and the rest mostly from Old Delhi where sanitary conditions are usually quite poor. In another hospital-based study from India, all of the 16 obstetric tetanus cases who came from the rural areas were attributed to deliveries or abortions conducted by untrained TBAs and 6 of the 8 urban obstetric cases had home deliveries (Mamtani et al. 1978).
E.3.1. Health services (access, utilization & quality of care)
The majority of maternal deaths are from rural areas and for the most part related to inaccessibility and poor utilization of health services (Agoestina & Soejoenoes 1989; Acsadi & Johnson-Acsadi 1990; Fauveau & Blanchet 1989; Harrison 1985; Lunan 1988).
In the Zaria study in Northern Nigeria, all four cases of maternal tetanus occurred in unbooked patients (Harrison 1985). In Matlab, Bangladesh, all of the six reported cases of maternal tetanus were from the comparison area with a low coverage of health services, including tetanus toxoid immunization (Fauveau, unpublished).
E.4. Distribution of portals of entry
The majority of maternal tetanus cases has been attributed to contamination of the puerperal uterus due to unhygienic delivery practices or to abortion induced by vaginal insertion of roots, twigs or herbs (Diop-Mar et al. 1985, Okonofua et al. 1989; Adadevoh & Akinla 1970; Adetoro 1989; Adeuja & Osuntokun 1971; Bennett 1976; Newman & Jacobs 1975; Khan et al. 1986b; Liskin 1980; Measham et al. 1981).
Female circumcision which is practised in different parts of the world carries a high risk of tetanus infection. The role of female circumcision in maternal tetanus, however, is limited and has never been documented.
Maternal tetanus may follow surgery, mainly when cesarean sections or other operations are performed with improperly sterilized instruments, or when infected dust reaches the wound. Such situations, however, have not been specifically described in the publications reviewed.
In the particular case of tetanus incidental to pregnancy, the portal of entry was not necessarily genital. In a review of 1,019 cases of tetanus observed during 1982 and 1983 in Dakar, Senegal, Diop-Mar et al. (1985) report 116 cases (11%) after intramuscular injection, five of them during pregnancy. The most cormmon injection was quinine(Quinimax). They also report an increasing proportion of such cases, with a short incubation and a high CFR of 80%. Reviewing 25 cases of tetanus during pregnancy in
6
Senegal, Zohoun (1975) reports 64% inoculated by intramuscular injection. Other possibleportals of entry include chronic otitis, ear piercing, and chronic leg ulcer includingguinea-worm ulcer in Nigeria (Adeuja & Osuntokun 1971).
E.5. Age, ai marital status
The age and parity distribution of maternal tetanus depends on age and parity distribution of the nregnaait women most at risk of delivering at home under unhygienic and unsanitaryconditions. It also depends on the practice of illegally induced abortion in a given country.In a community-based study in Addis Ababa, Ethiopia, Kwast et al. (1986) found that six (46%) of the 13 women who died from abortion - mainly induced illegally - were single,and four (31 %)were below 20 years of age. In a hospital-based study in Cape Town, South Africa, nearly 50% of the maternal tetanus patients -- most of them postabortal -were under 25 years of age, paralleling the age distribution of pregnant women normally delivering in the hospital (Bennett 1976). In one study in Nigeria, a majority of the maternal tetanus patients were young single women (Adadevoh & Akinla 1970). Likewise, a majority of the patients in another hospital-based study in Nigeria were young unmarried students whe did not have easy access to contraceptives and feared expulsion from school on the grounds of pregnancy (Adetoro 1989). In contrast, women seeking induced abortions in Asia appear to be usually older married women of high parity. In Ananthapur, India, deaths due to abortions were more frequent in the 30-44 age group than in the 15-29 age group (Bhatia 1986). In a community-based study in rural Bangladesh, the practice of induced abortion was positively related to age and parity: associated mortality per 1,000 live births in women aged 35 years and above was more than 12 times that of women below 25 years of age, and was more than seven times greater at parity five than at parity zero (Khan et al. 1986b). However, as observed in another community-based study in Matlab, abortion-related deaths were most common in women aged 35-39 years, but 70% of all deaths during pregnancy among unmarried women were due to complications of an induced abortion, a proportion 2.6 times greater than for married women (Fauveau & Blanchet 1989). Women admitted to Dhaka Medical College Hospital, Bangladesh, for incompleteinduced abortion were in their late twenties (mean age 28 years) and about 84% of them were married with on the average four live births (Khan et al. 1984). Data collected in Tangail, Bangladesh, showed women to be relatively younger and of lower parity: women undergoing an induced abortion were, on the average, 27 years old; six were primigravida and two had previous pregnancies (Alauddin 1986).
E.6. Socioeconomic status
None of the reviewed studies showed evidence of a relationship between maternal tetanus and socioeconomic status. In general, socioeconomic disadvantage, social problems, low status of women are important determinants of maternal mortality and induced abortion, and therefore maternal tetanus. In Ananthapur, India, the maternal mortality ratio was noted to be 22 per 1000 live births in the most socioeconomically deprived villages compared to 5 in the most developed ones (Bhatia 1986). In Addis Ababa, Ethiopia, women of high socioeconomic status more commonly made use of antenatal care than those of low socioeconomic status (Kwast et al. 1986). Moreover, the risk of dying was between three to six times greater for poor women, maids, divorced and widowed women when compared to those with a per capita income above the poverty line.
7
E.7. Seasonal vari&&Qn
Several autho have noted seasonal variation in tetanus incidence, particu!arly neonatal tetanus, though no adequate explanation can be given for it.
Incountries the size of Kenya or India, for example, in which there are many different ethnic customs and agricultural practices, the factors influencing the incidence of the disease vary from place to place. For all tetanus cases, the season of peak incidence usuallycoincides with !he warm, damp season and the time of the most intensive work in the fields (Bytchenko 1966). A study in Kenya showed that most of the tetanus cases occurred in areas of high rainfall where the population density was high and the amount of land under cultivation greatest (Baker 1963). The peak of admissions for tetanus coincided with the hot season during the period of greatest agricultural activity. In Indian studies the maximum number of tetanus patients were registered during the monsoon season (Barua 1961, quotedin Bytchenko 1966; Vaishnava et al. 1964).
E.8. Relationship with neonatal tetanus
In one prospective community-based study from Matlab, Bangladesh, it was reported that "in each case where the mother died from tetanus, the infant also died from neonatal tetanus" (Chen et al. 1974). Another instance in which both the mother and newborn died of tetanus was reported from Hawai (Milnor 1928, quoted in Adams & Morton 1955).
E.9. Reporting problems and extrapolation attempts
Maternal deaths have been shown to be underreported wherever they have been validated by independent studies (Walker et al. 1990; Kwast et al. 1986; Bhatia 1986). Compulsoryregistration of tetanus morbidity and mortality has not been established in most developingcountries, and all forms of tetanus remain also substantially underreported (Baker 1963; Bytchenko 1966; Stanfield & Galazka 1985). Postpartum tetanus probably follows the same patterns of underreporting as maternal deaths, while postabortal tetanus, linked to induced abortion, is likely to be even more underreported. Table 4 attempts to extrapolate from available community-based data an estimate of the number of deaths due to maternal tetanus that can be expected to occur annually worldwide. If an average of 3.1% of all maternal deaths are due to maternal tetanus, and 500,000 maternal deaths occur annually, it can be calculated that at least 15,000 maternal tetanus deaths occur each year in the world. Takinginto account a likely high proportion of underreporting, perhaps as much as 1 out of 2 maternal tetanus, the range may be 15,000 to 30,000.
F. CONTROL MEASURES
F.1. Curative measures
There is no curative treatment per se for tetanus, including, maternal tetanus. The guidingprinciples for case management remain i/to prevent more toxin from being released and reaching the central nervous system, and ii/to control the symptoms caused by the toxin already in the central nervous system until spontaneous recovery. The first priorities are therefore to inject antitoxin and to clean the wound sit,. Antitoxin will neutralize circulatingtoxin that has not yet been fixed on the nerve tissues. Antitoxin most commonly found in developing countries is of equine origin and carries a risk of allergic reaction. To avoid this risk one can use the classic Bezredka method of progressive injection, but it is safer to use
8
human tetanus immunoglobulin. Human immunoglobulin, however, is still vey, expensive. Surgical debridement of the wound is essential if a wound or an abscess has teen found.
In cases of postpartum and postabortal tetanus, dilatation and curettage are necessary to remove necrotic tissue and retained placenta. All authors except two (Adams & Morton 1955, Ayim 1972) agreed on this. Hysterectomy has been proposed but it does not seem to bring significant benefits. Antibiotics are recommended if the patient is seen early enough, to attack the germs still in the infected wound. Penicillin is the classical choice, but must be avoided intramuscularly, because repeated injections might provoke spasmodic contractions. Metronidazole has recently been proposed as an alternative. The second line of attack aims at helping the patient pass through the acute neurologic phase: it involves simple sedation in minor cases, and muscle relaxation (by barbiturates, chlorpromazine, diazepam, curare, or a combination of these drugs) in severe moderate cases, with tracheostomy and artificial ventilation in positive pressure. Maintenance of proper hydration, and hyper-caloric feeding (through nasogastric tube or gastrostomy) are also essential components of the treatment.
The whole process of case management described above requires levels of technical competence and cost that are only found in well-trained intensive care units (Rey et al. 1981). Some developing countries have started to develop such units in central or provincial hospitals, but this should not set a standard to be followed at any cost. Clearly preference should be given to preventive measures.
F.2. Preventive measures
deally, simple avoidance of introducing tetanus spores (i.e. dust or dirt) into the genital tract during pregnancy, delivery, abortion or the postpartum period should prevent the incidence of maternal tetanus. Several interventions can be combined to reach this goal: training medical staff, midwives, traditional birth attendants and community health workers in clean obstetric procedures, distributing simple delivery kits to women who intend to deliver at home, providing safe abortion methods, promoting family planning to reduce unwanted pregnancies. Such programs have been promoted in most developing countries as part of primary health care. In most developing countries, however, and particularly in the poorest ones, progress will be slow and efforts should be focussed on the immunization of women with tetanus toxoid (Ross 1986, REACH 1900).
Considerable progress has been achieved in the past thirty years in developing immunization programs to protect newborn infants from neonatal tetanus (Newell et al. 1966, Schofield 1986, EPI 1991). An effective, stable, cheap toxoid has been available for more than 50 years, and is produced by many developing countries. The current challenge is to make good quality vaccine available to all women in developing countries entering their reproductive age. That women need to be protected in their own right against the septic risks associated with pregnancy and delivery needs to be emphasized.
Schofield (1986) anc Steinglass et al. (1991) provide comprehensive reviews of possible strategies for controlling tetanus and their cost-effectiveness. In general, at the very least, one should aim for continuous immunization of all women of childbearing age, whether pregnant or not. This can be done through static MCH clinics where adequate refrigeration is present and women come to the clinic, or through mobile teams with the assistance of village midwives and/or community volunteers.
Not only integration of immunization programs with MCH services is needed, but tetanus toxoid coverage should be a fundamental performance indicator for MCH services. The definition of a "tully immunized child" should include the concept of a child who not only
9
has directly received all required vaccinations, but who also was born protected from tetanus to a woman herself protected from the risk of maternal tetanus. The cost for this particular protection is affordable by most countries when integrated with EPI. The extent to which political and financial resources are mobilized will determine whether or not 150,000 to 300,000 women will die of maternal tetanus during the 1990s.
10
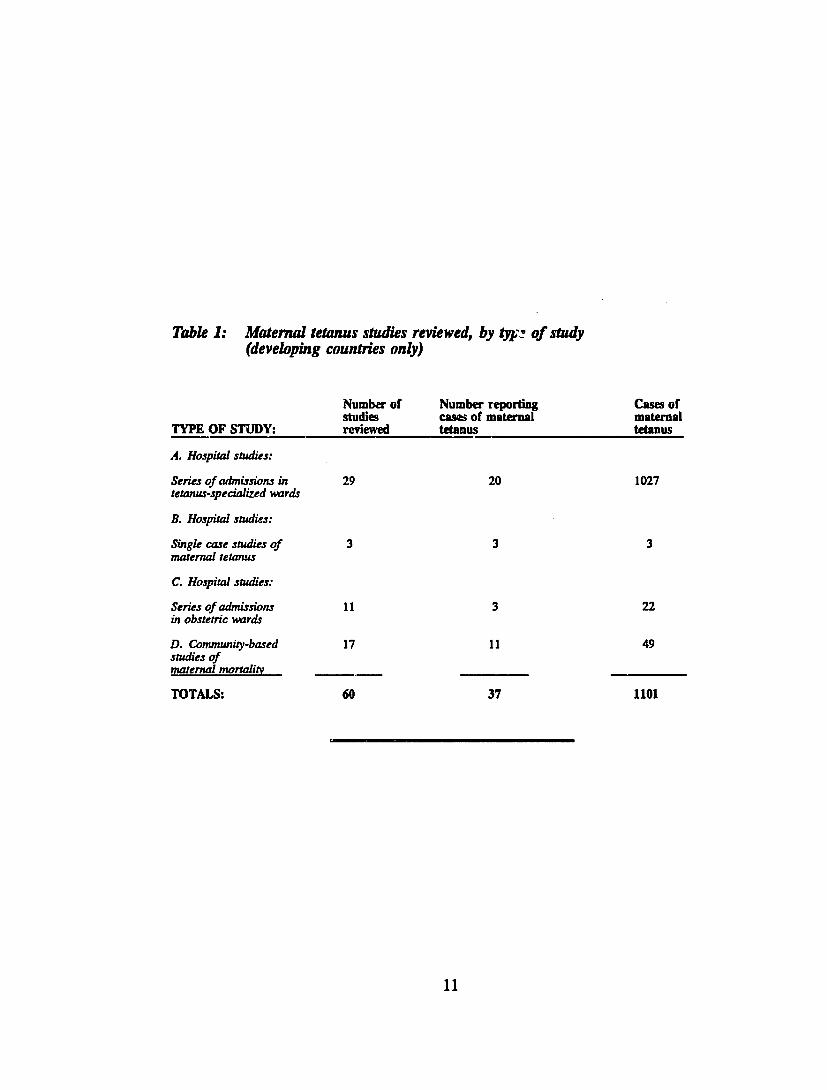
Table 1: Maternaltetanus studies reviewed, by typ.! of study (developing countries only)
Number of Number reporting Cases of studies cases of maternal maternal
TYPE OF STUDY: reviewed tetanus tetanus
A. Hospital studies:
Seriesof admissionsin 29 20 1027 tetanus-specializedwards
B. Hospital studies:
Single case studies of 3 3 3 maternaltetanus
C. Hospital studies:
Series ofadmissions 11 3 22 in obstetricwards
D. Community-based 17 11 49 studies of maternalmortality
TOTALS: 60 37 1101
11
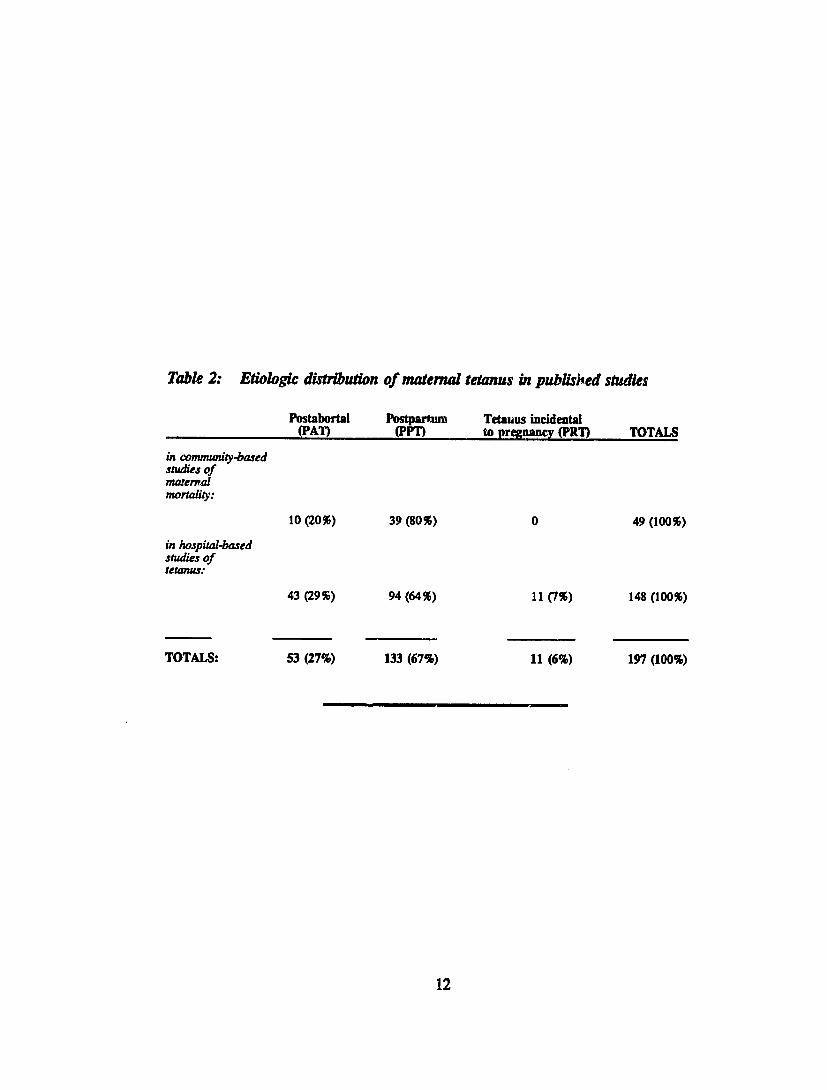
Table 2: Etiologic distributionof maternaltetanus in publisled studies
Postabortal Postmrtum Tetanus incidental (PAI) (PIT) to pregnancy (PRI) TOTALS
in community-based studiesof matenal mortality:
10 (20%) 39 (80%) 0 49 (100%)
in hospital-based studies of tetanus:
43 (29%) 94 (64%) 11 (7%) 148 (100%)
TOTALS: 53 (27%) 133 (67%) 11(6%) 197 (100%)
12
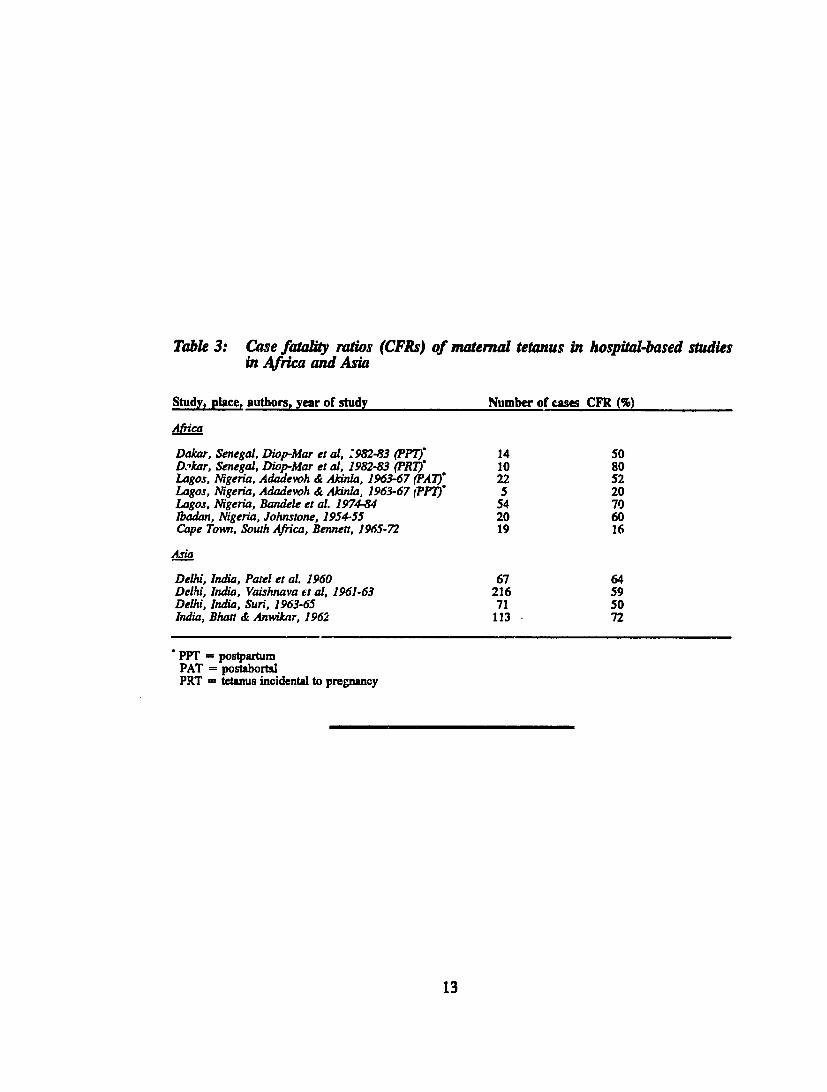
Table 3: Casefatality ratios (CFRs) of maternal tetanus in hospital-basedstudies in Afra andAsia
Study, place, authors, year of study Number of cases CFR (%)
Dakar,Senegal, Diop-Mar et a, :982-83 (PP): 14 50 DTkar, Senegal, Diop-Mar et al, 1982-83 (R) Lagos, Nigeria, Adadevoh & Akinla, 1963-67 (PA)"
10 22
80 52
Lagos, Nigeria, Adadevoh & Akinla, 1963-67 rPP) 5 20 Lagos, Nigeria, Bandele et al. 1974-84 54 70 lbadan, Nigeria,Johnstone, 1954-55 20 60 Cape Town, South Africa, Bennett, 1965-72 19 16
Asia
Delhi, India, Patel et al. 1960 67 64 Delhi, India, Vaishnava et al, 1961-63 216 59 Delhi, India, Sue., 1963-65 71 50 India, Bhatt & Anwikar, 1962 113 72
PPT = postpartum PAT = postabortal PRT tetanus incidental to pregnancy
13
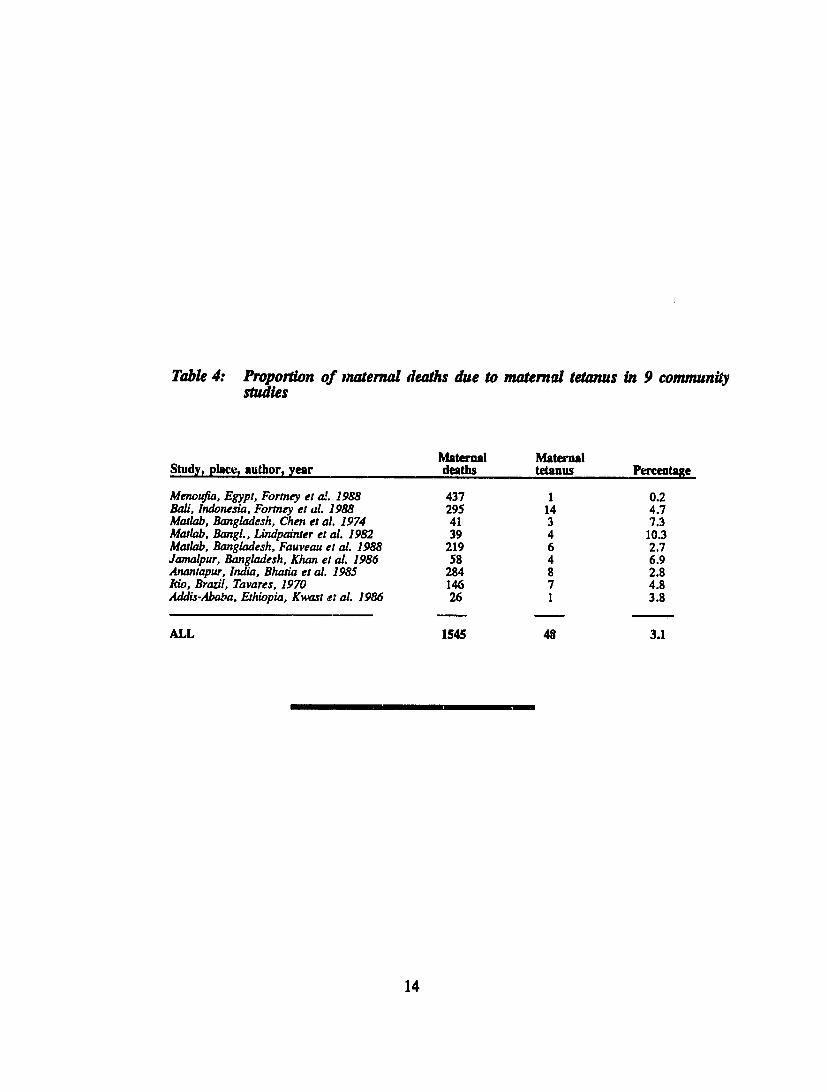
Table 4: Proportion of maternal deaths due to maternal tetanus in 9 community studies
Maternal Maternal Study, place, author, year deaths tetanus Percentage
Menoufia, Egypt, Fortney et a!. 1988 437 1 0.2 Bali, Indonesia, Formney et al. 1988 295 14 4.7 Matlab, Bangladesh, Chen et al. 1974 41 3 7.3 Matlab, Bangl., Lindpainteret al. 1982 39 4 10.3 Matlab, Bangladesh, Fauveauet al. 1988 219 6 2.7 Jamalpur,Bangladesh, Khan et al. 1986 58 4 6.9 Anantapur, India, Bhatia et al. 1985 284 8 2.8 Rio, Brazil, Tavares, 1970 146 7 4.8 Addis-Ababa, Ethiopia, Kwast e: al. 1986 26 1 3.8
ALL 1545 48 3.1
14
REFERENCES
Acsadi, G.T.F. & Johnson-Acsadi, G. (1990). Safe motherhood in south Asia: sociocultural and demographic aspects of maternal health. Background paper prepared for the Safe Motherhood South Asia Conference: Lahore, Pakistan 24-28 March 1990. New York: Acsadi Associates.
Adadevoh, K.B. & Akinla, 0. (1970). Postabortal and postpartum tetanus. The Journal of Obstetrics and Gynaecology of the British Commonwealth, 77, 1019-1023.
Adams, J.Q. & Morton, R.F. (1955). Puerperal tetanus. American Journal of Obstetrics and Gynecology, 69, 169-173.
Adetoro, 0.0. (1987). Maternal mortality - a twelve-year survey at the University of Ilorin teaching hospital (U.I.T.H.), Ilorin, Nigeria. International Jou:rnal of Gynaecology and Obstetrics, 25, 93-98.
Adetoro, 0.0. (1989). A 15-year study of illegally induced abortion mortalfiy at Ilorin, Nigeria.International Journal of Gynaecology and Obstetrics, 29, 65-72.
Adeuja, A.O.G. & Osuntokun, B.O. (1971). Tetanus in the adult Nigerians. A review of 503 patients. East African Medical Journal, 48(12), 683-691.
Agoestina, T. & Soejoenoes, A. (1989). Technical report on the study of maternal and perinatalmortality, Central Java Province, Republic of Indonesia. Jakarta: BKS PENFIN.
Alauddin, M. (1986). Maternal mortality in rural Bangladesh: the Tangail district. Studies in Family Planning, 17(1), 13-21. Ayim, E.N. (1972). The management of tetanus - A study of 51 cases treated at Muhimbili Hospital, Dar es Salaam. East African Medical Journal 49(2), 170-76.
Bahari, C. & Friedman, S. (1964) Puerperal Tetanus. Report of a case. Gynecologia 158: 42-50.
Baker, W.C. (1963). A note on the epidemiology of tetanus in Kenya. East African Medical Medical Journal, 40(4), 127-131.
Bandele, E.O., Akinyanju, 0.0., Bojuwoye, B.J. (1991). An analysis of tetanus deaths in Lagos.Journal of the National Medical Association, 83, 55-58.
Bennett, M.J. (1976). Postabortal and postpartum tetanus. A review of 19 cases. South African Medical Journal, 24 March 76, 513-516. bhatia, J.C. (1986). A study of maternal mortality in Anantapur district, Andhra Pradesh, India. Bangalore, Indian Intitute of D-velopment.
Bhatt, A.N. & Anwikar, A.K. (1962) Journal of the Medical Association of India, 38: 71-75.
Boerma, T. (1987). The magnitude of the maternal mortality problem in sub-Saharan Africa. Social Science and Medicine, 24(6), 551-558.
Bullough, C.H.W. (1981). Analysis of maternal deaths in the central region of Malawi. East African Medical Journal, 58, 25-36.
15
Bytchenko, B. (1966). Geographical distribution of tetanus in the world, 1951-60. Bulletin of the World Health Organization, 34, 71-104.
Caffrey, K.T. (1979). Maternal mortality - a continuing challenge in tropical practice. East African Medical Journal, 56, 274-277.
Chen, L.C., Gesche, M.C., Ahmed, S., Chowdhury, A.I. & Mosley, W.H. (1974). Maternal mortality in rural Bangladesh. Studies in Family Planning, 5(11), 334-341.
Coeytaux, F.M. (1988). Induced abortion in sub-Saharan Africa: what we do and do not know. Studies in Family Planning, 19(3), 186-190.
Dare, F.O. & Makinde, 0.0. (1989). Tetanus in pregnancy in a Nigerian woman - a case report. Tropical Doctor, April 89, 81-82.
Diop-Mar, I., Sow, Ab., Badiane, B. & Coll, A.M. (1985). Clinical aspects of tetanus in Africa with 1,019 cases in Dakar (1982-1983). In G. Nistico, P. Mastroeni & M. Pitzurra (Eds.), Seventh international conference on tetanus (pp. 499-507). Roma: Gangemi Publishing Co.
Dutta, R. (1980). Abortion in India, with particular reference to West Bengal. Journal of Biosocial Science, 12, 191-200.
Eckmann, L.(ed) (1966). Principles on tetanus. Proceedings of the international conference on tetanus, July 15-19 1966, Bern. Bern and Stuttgart: Hans Huber Publishers.
Editorial. (1987). Maternal health in subsaharan Africa. The Lancet, January 31, 255-257.
Editorial. (1989). The impact of unsafe abortion in the developing world. Outlook, 7(3), 2-7.
Expanded Programme on Immunization. (1991) Progress on the global plan for NNT elimination. Report to the 14th Meeting of the Global Advisory Group, 14-18 October 1991, Antalya, Turkey.
Fauveau, V., Koenig, M.A., Chakraborty, J. & Chowdhury, A.I. (1988). Causes of maternal mortality in rural Bangladesh, 1976-85. Bulletin of World Health Organization, 66(5), 643-651.
Fauveau, V., Wojtyniak, B., Koenig, M.A., Chakraborty, J. & Chowdhury, A.I. (1989). Epidemiology and cause of deaths among women in rural Bangladesh. International Journal of Epidemiology, 18(1), 139-145.
Fauveau, V. & Blanchet, T. (1989). Deaths from injuries and induced abortion among rural Bangladeshi women. Social Science and Medicine, 29(9), 1121-1127.
Firoz, G. (1978). A study of neonatal, postpartum and postabortal tetanus in one thana of rural Bangladesh. (Unpublished)
Fortney, J.A., Susanti, I., Gadalla, S., Saleh, S., Feldbium, P.J. & Potts, M. (1988). Maternal mortality in Indonesia and Egypt. International Journal of Gynecology & Obstetrics, 26, 21-32.
Gadalla, S., Fortney, J.A., Saleh, S., Kane, T. & Potts, M. (1987). Maternal mortality in Egypt. Journal of Tropical Pediatrics, 33(4), 11-13.
16
Grech, E.S., Galea, J.& Tnissell, R.R. (1975). Maternal mortality. In S.A. Hall & B.W. Longlands (Eds.), Uganda Atlas of Disease Distribution (pp.126-129). Nairobi: East African Publishing House.
Harrison, K.A. (1985). Childbearing, health and social priority: a survey of 22774 consecutive hospital births in Zaria, Northern Nigeria. British Journal of Obstetrics anti Gynaecology, 92 (supp.no.5), 1-119.
Holmdahl, M.H. & Thoren, L. (1962) Tetanus in pregnancy (report of a case). American Journal of Obstetrics and Gynecology. 84, 339-41.
Januszkiewicz, J., Galazka, A., Adamczyk, J., Sporzynska, Z. (1973). Severe tetanus in late pregnancy. Scandinavian Journal of Infectious Diseases 5: 233-35.
Johnstone, D.D. (1958). Tetanus in Nigeria: review of 100 cases treated in Ibadan. British Medical Journal, 1, 12-16.
Justesen, A. (1985). An analysis of maternal mortality in Muhimbili Medical Centre, Dar es Salaam, July 1984. Journal of Obstetrics and Gynecology of Eastern and Central Africa, 4, 5-8.
Khan, A.R., Begum, S.F., Covington, D.L., Janovitz, B., James, S. & Potts, M. (1984). Risks and costs of illegally induced abortion in Bangladesh. Journal of Biosocial Science, 16, 89-98.
Khan, A.R., Akhter Jahan, F. & Firoza Begum, S. (1986a). Maternal mortality in rural Bangladesh: the Jamalpur district. Studies in Family Planning, 17(1), 7-12.
Khan, A.R, Rochat, R.W., Akhter Jahan, F. & Feroza Begum, S. (1986b). Induced abortion in a rural area of Bangladesh. Studies in Family Planning, 17(2), 95-99.
Kwast, B.E. (1989). Maternal mortality: levels, causes and promising interventions. Journal of Biosocial Science, Supplement 10, 51-67.
Kwast, B.E. (1988). Unsafe motherhood: a monumental challenge. Leiderdorp: Kwast.
Kwast, B.E., Rochat, R.W. & Kidane-Mariam, W. (1986). Maternal mortality in Addis Ababa,Ethiopia. Studies in Family Planning, 17(6), 288-301.
Lawson, H.L., Atrash, H.K. & Hogue, C.J.R. (1990). Maternal mortality in Mexico. (Unpublished)
Lettenmaier, C., Liskin, S., C'arch, C. & Harris, J.A. (1988). Mothers' lives matter: maternal health in the community. Population Reports, Series L, Number 7, 1,"/Z(2), 1-31.
Lindpainter, L.S., Jahan, lNT., Satterthwaite, A.P. & Zimicki, S.(1982). Maternal-related mortalityin Matlab Thana, Bangladesh, 1982. Dhaka, International Centre for Diarrhoeal Disease Research, Bangladesh.
Liskin, S.(1980). Complications of abortion in developing countries. Population Reports, Series F, No.7, 105-155.
Lunan, C.B. (1988). Maternal health services in Bangladesh. Assignment report, 22 January - 20 February 1988. (Unpublished)
17
Mahler, H. (1987). The safe motherhood initiative: a call to action. The Lancet, March 21, 668-670.
Makokha, A.E. (1980). Maternal mortality at Kenyatta National Hospital 1972-77. East African Medical Journal, 57, 451-451.
Mamtani, R., Malhotra, P., Gupta, P.S. & Jain, K. (1978). A comparative study of urban and rural tetanus in adults. International Journal of Epidemiology, 7, 185-188.
Measham, A.R., Rosenberg, MoJ., Khan, A.R., Obaidullah, M., Rochat, R.W. & Jabeen, S. (1981). Complications from induced abortion in Bangladesh related to types of practitioner and methods, and impact on mortality. The Lancet, January 24, 199-202.
Melrose, E.B. (1984). Maternal deaths at King Edward VIII Hospital, Durban: a review of 258 consecutive cases. South African Medical Journal, 65, 161-165.
Newell, K.W., Duenas Lehmann, A., Leblanc, D.R. & Garces Osorio, N. (1966). The use of toxoid for the prevention of tetanus neonatorum. Bulletin of the World Health Organization, 35, 863-871.
Newman, C., Jacobs, C. & Roberts, B. (1975). Postabortal tetanus. Connecticut Medicine, 39(12),773-774.
Okonofua, F.F., Esen, U.I. & Bamgbose, J.K. (1990). Fatal maternal tetanus following premature rupture of membranes and retained dead fetus. Tropical and Geographical Medicine, 42, 166-167.
Patel, J.C.(ed) (1963). Proceedings of the first international conference on tetanus, November 8-10 1963, Bombay. Bombay: The study group of tetanus, King Edward Memorial Hospital.
Patel, J.C., Metha, B.C., Dhirwani, M.K., Brandarkar, S. D. (1960). Puerperal tetanus. Journal of Obstetrics and Gynecology of India 11, 187-192.
Price, T.G. (1984). Preliminary report on maternal deaths in the Southern Highlands of Tanzania in 1981. Journal of Obstetrics and Gynecology of Eastern and Central Africa, 3, 103-110.
Ratna Budiarso, L. (1989). Maternal mortality in Indonesia: a review of recent evidence. Child Survival Research Notes, Australian National University, No. 22CS, 1-5.
REACH/MotherCare. (1990). Neonatal tetanus elimination: issues and future directions. Arlington: REACH/ MotherCare.
Rey, M. Diop-Mar, I. Robert, D. (1981). Treatment of tetanus. In Veronesi R. & Foccacia R. (Eds), Tetanus: Important new concepts.. Amsterdam, Excerpta Medica, pp 207-237.
Rey, M. & Tikhomirov, E. (1989). Non neonatal tetanus over the world. In G. Nistico, B. Bizzini,B. Bytchenko & R. Triau (Eds.), Eighth international conference on tetanus (pp. 506-518). Rome-Milan: Pythagora Press.
Rochat, R.W., Jabeen, S., Rosenberg, M.J., Measham, A.R., Khan, A.R., Obaidullah, M. & Gould, P. (1981). Maternal and abortion related deaths in Bangladesh, 1978-79. International Journal of Gynaecology and Obstetrics, 19, 155-164.
Rochat, R.W., Kramer, D., Senanayake, P. & Howell, C. (1980). Induced abortion and health problems in developing countries. The Lancet, August 30, 484-484.
18
Ross, D.A. (1986). Does training TBAs prevent neonatal tetanus?. Health Policy and Planning, 1(2), 89-98.
Schofield, F. (1986). Selective primary health care: strategies for control of disease in the developing world. XXII. Tetanus: a preventable problem. Reviews of Infectious Diseases, 8(1), 144-154.
Sepet, B. (1898) Tetanus puerperal. Congres de Gynecologie et Obstetrique, Marseille 1898.
Singleton, AR. & Witi, RW. (1956) Tetanus con. iicating pregnancy (report of a case). Obstetrics & Gynecology 7(5): 540-1.
Smucker, C., Simmons, G.B., Bernstein, S., Misra, B.D. (1980) Neonatal mortality in South Asia: The special role of tetanus. Population Studies 34: 321-35.
Stanfield, J.P. & Galazka, A. (1985). Neonatal tetanus: an underreported scourge. World Health Forum 6: 127-29.
Steinglass, R., Brenzel, L. & Percy, A. (1991). Tetanus. In: Jamison DT & Mosley WH, (Eds),Disease Control Priorities in Developing Countries. Oxford University Press for The World Bank, New York (in press).
Suleiman, 0. (1982) Mortality from tetanus neonatorum in Punjab, Pakistan. Pakistan Pediatric Journal 6(2-3), 152-183.
Suri, J.C. (1967). The problem of tetanus in India. In L. Eckmann (Ed.), Principles on tetanus: Proceedings of an international conference on tetanus, Bern, 15-19 July 1966 (pp. 61-70). Bern: Huber.
Tallo, V.L. (1980). Bohol Province MCH/FP Project. Reported causes of deaths by age: Bohol project and non-project areas, 1970-75 and 1976-79. Research Note No. 73. (Unpublished)
Tavares, W. (1980). Estudio epidemiologico de tetanos en el estado de Rio de Janeiro. In Curso Basico de Vigilancia Epidemiologica de Enfermedades Immunoprevenibles Quito, Ecuador: Ministerio de Salud Publica and UNICEF.
Tietze, C. (1983). Induced abortion. In S.L. Barron & A.M. Thomson (Eds.), Obstetrical Epidemiology (pp. 319-346). London: Acadcmic Press.
Vaishnava, H., Neogy, C.N., Dixit, N.S., Passey, M.N., Gupta, S.C. &Arora, N. (1964). Clinical study of tetanus in Delhi for a period of 32 months. Journal of the Association of Physicians of India, 42, 203-212.
Walker, G.J.A., McCaw-Binns, A., Ashley, D.E.C. &Bernard, G.W. (1990). Identifying maternal deaths in developing countries: experience in Jamaica. International Journal of Epidemiology, 19(3), 599-605.
Weinstein, B.B. & Beacham, W.D. (1941). Postabortal tetanus. American Journal of Obstetrics and Gynecology, 42, 1031-1040.
Wessler, S. & Avioli, L.A. (1969). Tetanus. Journal of American Medical Association, 207(l),123-127.
19
Weston, L. (1986). Reducing maternal deaths in developing countries. PHN Technical Note 86-19. Washington, DC: Population, Health and Nutrition Dept., World Bank.
Winikoff, B. (1990). Women's health in the developing countries. In H.M. Wallace & K. Giri (Eds.), Health care of women and children in developing countries (pp. 167-190). Oakland, California: Third Party Publishing Co..
World Health Organization. (1986). Maternal mortality rates: a tabulation of available data. 2nd edition, No. FHE/86.3. (UnPub)
Zohoun, T. (1975). Le tetanos chez la femme enceinte (a propos de 25 cas). Thse en M~decine, Dakar, No. 13.
20



























