Embed Size (px)
Citation preview
Rhythms of Daily Rhythms of Daily LivingLiving© Dining & ChoiceDining & ChoiceSTRATEGIC OBJECTIVES – TACTICAL STRATEGIC OBJECTIVES – TACTICAL
IMPLEMENTATIONIMPLEMENTATION Aligning Experiences – Expectations – Resources – Outcomes
June 9, 2004 VANHA 2
Why Do 65% Of NH Residents Eat Less Than 75% Of Most Meals* ? Primary Factors That Contribute To Malnutrition In
Nursing Homes 1. An Inappropriate Dining Experience For The Resident.
2. Meal Delivery Methodology and Systems Not Conducive To Eating.
3. Good Nutrition is of no value if it is not consumed
*Excerpted From Ch 14 Of Report To Congress “Appropriateness of Minimum Staffing Ratios In Nursing Homes” Authored By J. F. Schnelle et al, Borun Center For Gerontological Research
June 9, 2004 VANHA 3
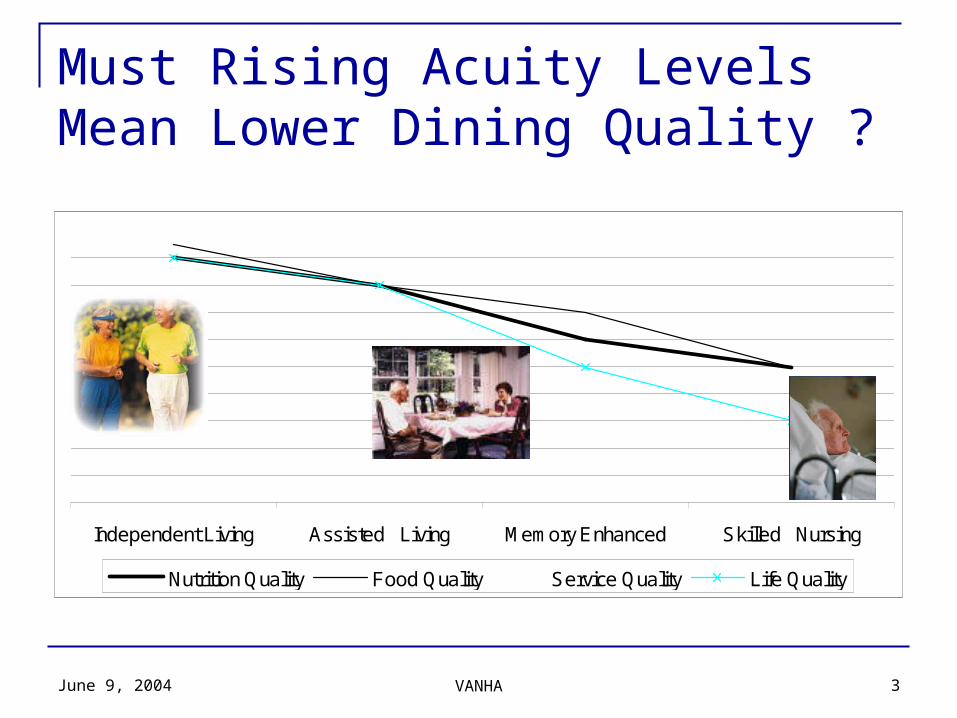
Must Rising Acuity Levels Mean Lower Dining Quality ?
©©
Independent Living Assisted Living Memory Enhanced Skilled Nursing
Nutrition Quality Food Quality Service Quality Life Quality
June 9, 2004 VANHA 4
What Are Factors of Rhythms Of Daily Living For Dining? service choice of where you eat Defined and met expectation Reputation – consistency Timeliness Presentation of meal Taste Do not rush me NeighborsAtmosphere, aroma cleanliness choice Residents eat when hungry friendliness Generational expectations Personal eating habits Choose to dine at a time of the resident’s choice
The Simple Answer Is NoNo!
June 9, 2004 VANHA 5
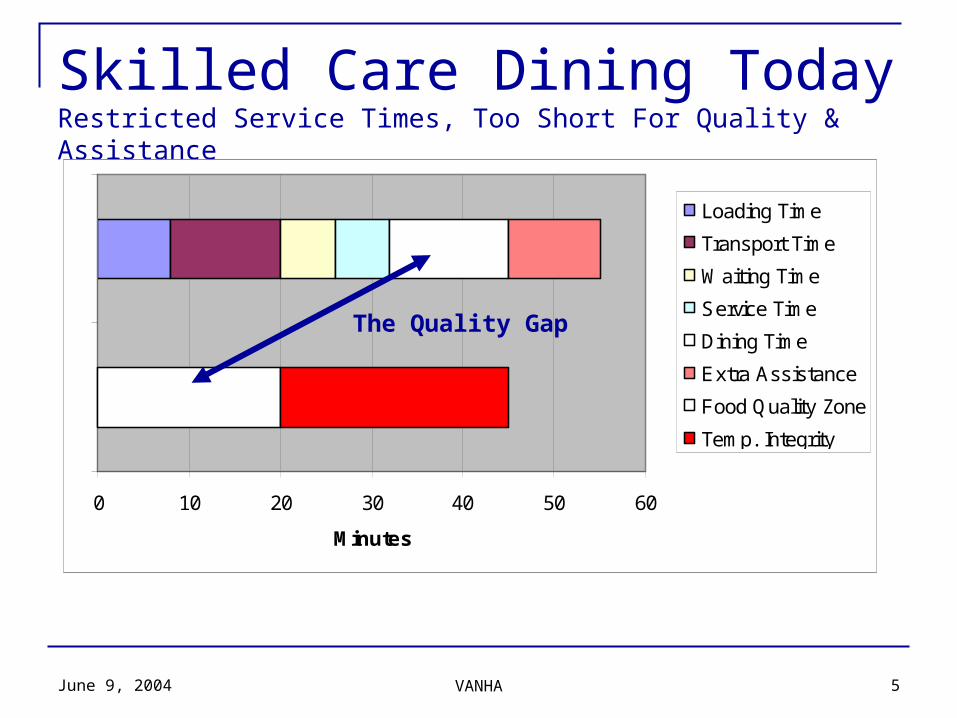
Skilled Care Dining TodayRestricted Service Times, Too Short For Quality & Assistance
< 20 MinutesFor Dining
0 10 20 30 40 50 60
Minutes
Loading Time
Transport Time
Waiting Time
Service Time
Dining Time
Extra Assistance
Food Quality Zone
Temp. Integrity
The Quality Gap
June 9, 2004 VANHA 6
Bridging The Quality GapServe The Resident, Not The System
The System – Individual Preparation, Bulk Service Prepare Individual Menu Items For Storage Place On A Tray For Transport To Feeding Area Transport and Leave In Cart Distribute and Unwrap At Scheduled Meal Time
The Alternative – Bulk Preparation, Individual Service Prepare Menu Items In Bulk Transport To Dining Room Servery Plate Individually and Serve Upon Request
June 9, 2004 VANHA 7
Balancing the Natural Rhythms of Resident Living and Care Work A “More Normal” Pattern of Living and Work
Residents Eat What And When They Want Over A Longer Meal Service Pre-Meal Medications, Bathing and Other Activities Are Less Pressured Staff Provides Assistance As Required
24 Minutes Is Average Optimal Feeding Assistance Time With A Range From 5 To 70 Minutes Depending On ADL Status*
48% Of Nursing Home Population Require Some Degree of Assistance* A Dining Experience, Not A Feeding Period
Shift Dining Service Focus From Trays To Residents and Quality Collaborative Service Support Aroma Therapy Course Presentation Minimal Distraction Environment
*Excerpts From Ch 14 Of Report To Congress “Appropriateness of Minimum Staffing Ratios In Nursing Homes” Authored By J. F. Schnelle et al, Borun Center For Gerontological Research
June 9, 2004 VANHA 8
Rhythms of Daily LivingRhythms of Daily LivingThe core of RDL is the opportunity to exercise choice –
residents’ for how they choose to live their day and staff choice for care delivery. This creates a collaborative coalition of residents and caregivers working together in a living environment. RDL facilitates the delivery of care, the experience of living and the dignity of self-determination.
RDL is a management principle that aligns the natural rhythms of residents and the support they need. The organizing principle of RDL is that people should be able to make meaningful choices in their daily lives – on their own or with assistance. RDL relies on caregivers to help define and achieve outcomes that balance individual choice and system efficiency.
June 9, 2004 VANHA 9
40% of Residents Gain Weight In The First Few Program Months
50% Reduction In The Number Of Residents Losing Weight. Consistent Improvement In Resident Satisfaction $0.18 – $0.21 Reduction In Food Cost Per Meal From Less
waste. 85% Decrease In Use of Supplements Higher Job Satisfaction Improved Hydration Outcomes Exceed Regulatory Requirements
RDL Is RealReported Results From Ten Communities That Have Implemented RDL
June 9, 2004 VANHA 10
Assessment Points for RDL ImplementationStages are defined against the requirements of: Administration: fiscal, management and leadership
considerations Regulatory: compliance criteria (grouped by clinical and
operational considerations) Systems: software programs, forms, policy & procedures,
protocols Personnel: staffing requirements, training, HR. The impact
on each care disciplines is identified by department PP&E: Property, Plant & Equipment necessary to perform
the tasks and functions
June 9, 2004 VANHA 11
STAGES of RDL Readiness GAP Analysis
Establish clear understanding among all constituents (residents, staff and administration) as to the program impact on 6 principle areas.
Culinary Capacity Establish a servery on the resident floor where all meals can be finished, plated and served.
Individualized Service Establish a service program without the tray system. Meals are plated in the servery when the resident is in the
dining room. Choice is based on pre-ordered menu items, however time of service is not flexible. Point of Service Menu Choice
Establish the opportunity for the resident to choose alternate items from a menu during meal service. Schedule Choice I[1]
Establish the opportunity for residents who are self-sufficient and independent to dine at a time of their choosing, within established service times.
Schedule Choice II Establish the opportunity for residents who require assistance with dining but are able to determine when they
would like to dine to do so within established service times. 7. Venue Choice (If Appropriate)
Establish the opportunity for residents to choose alternate places to dine.
[1] Schedule choice is the last and most difficult stage to implement because it affects the scheduling of all resident activities from bathing to medication and activities.
June 9, 2004 VANHA 12
How Do You Individualize Care?1. What Are Strategic Objectives?
Current Strengths Opportunities Identified For Improvement
2. What Is The Vision for Community Dining Experience? Choice
Menu, Time and Venue?3. What Is History of “Transformation” Projects?
What Were Expectations How Defined and Structured How was it trained & accepted?
What Are The Most Important Experiences? Resident Experiences Staff Experience Family & Other Stakeholders?
June 9, 2004 VANHA 13
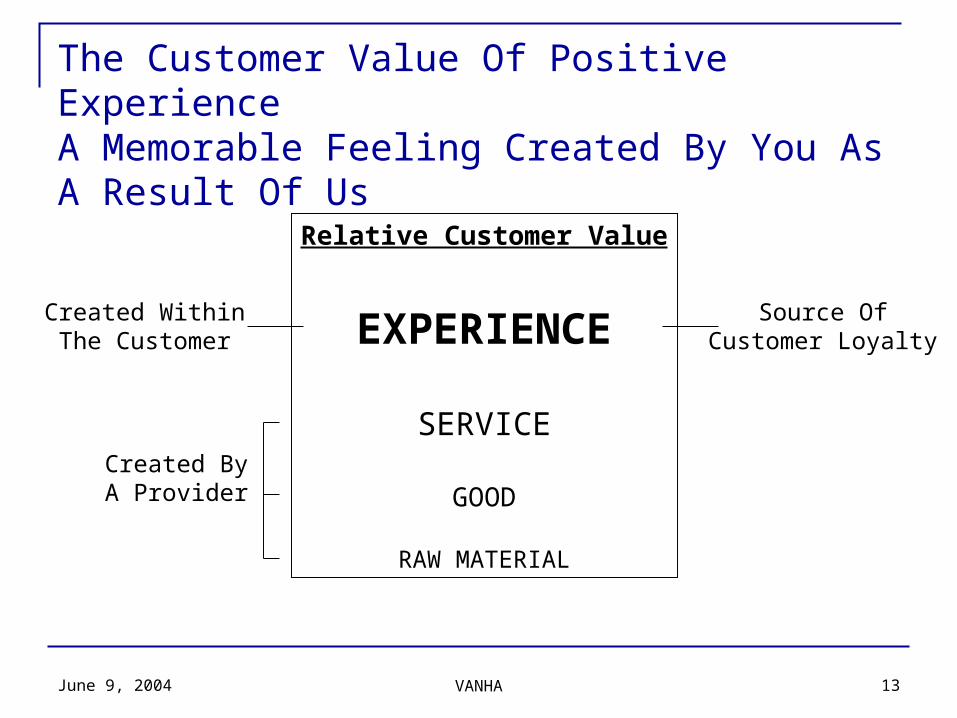
The Customer Value Of Positive ExperienceA Memorable Feeling Created By You As A Result Of Us
Relative Customer Value
EXPERIENCE
SERVICE
GOOD
RAW MATERIAL
Source OfCustomer Loyalty
Created WithinThe Customer
Created ByA Provider
June 9, 2004 VANHA 14
Strategy MappingAs dining options and service evolution and enhancements are
discussed, specific initiatives are defined and envisioned by community leadership, community constituencies, department management and staff. As these new “dining experiences" and expectations are defined, mapping aligns resources from vision to strategic objective to tactical implementation assuring effective implementation and benefits.
Drs. R. Kaplan and D. Norton present this process in Strategy Maps. The mapping process allows communities to:
Clarify strategies and communicate them to all constituents Identify key internal services that drive strategic success Align resources to a common objective Expose operational gaps and initiate appropriate corrective
response
June 9, 2004 VANHA 15
Mapping Process Tasks
Identify Service Initiatives Define Their Contribution to Strategic Objectives Define Appropriate Measurements of Successful
Experience Outcomes Identification of Resource and Operational Intersects Identification of Intersects and Roles of Collaborating
Departments Structure of the Process for Resource Allocation to
Develop the Defined Initiative Sequencing of The Tasks Implementation of the Initiative.
June 9, 2004 VANHA 16
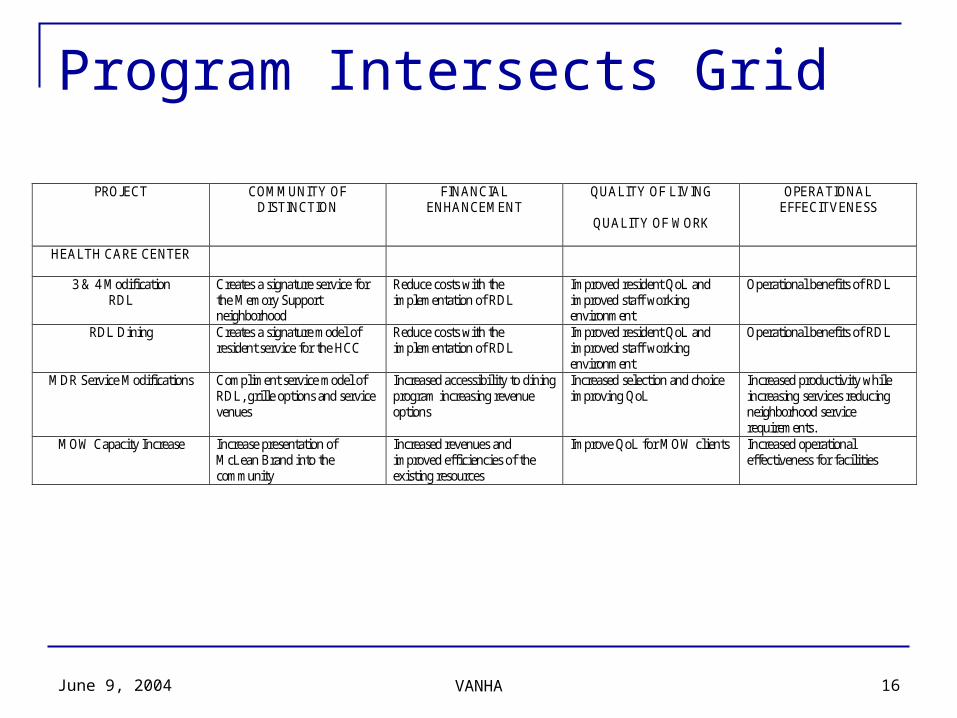
Program Intersects Grid
PROJECT COMMUNITY OF DISTINCTION
FINANCIAL ENHANCEMENT
QUALITY OF LIVING
QUALITY OF WORK
OPERATIONAL EFFECITVENESS
HEALTH CARE CENTER
3 & 4 Modification RDL
Creates a signature service for the Memory Support neighborhood
Reduce costs with the implementation of RDL
Improved resident QoL and improved staff working environment
Operational benefits of RDL
RDL Dining Creates a signature model of resident service for the HCC
Reduce costs with the implementation of RDL
Improved resident QoL and improved staff working environment
Operational benefits of RDL
MDR Service Modifications Compliment service model of RDL, grille options and service venues
Increased accessibility to dining program increasing revenue options
Increased selection and choice improving QoL
Increased productivity while increasing services reducing neighborhood service requirements.
MOW Capacity Increase Increase presentation of McLean Brand into the community
Increased revenues and improved efficiencies of the existing resources
Improve QoL for MOW clients Increased operational effectiveness for facilities
June 9, 2004 VANHA 17
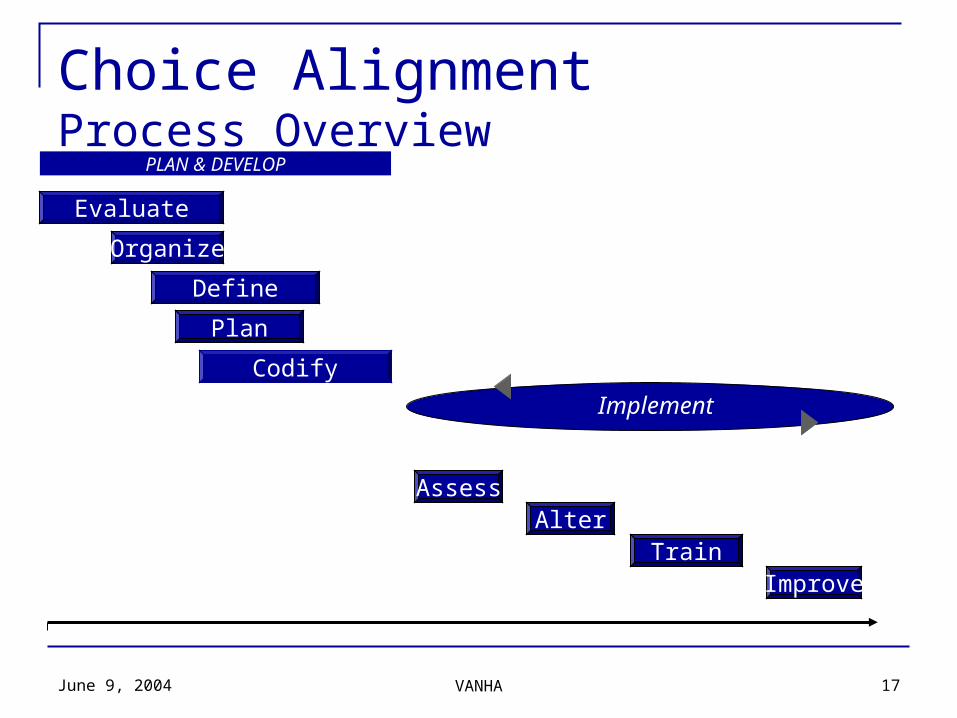
PLAN & DEVELOP
Organize
Alter
Codify
TrainImprove
Choice AlignmentProcess Overview
Plan
Evaluate
Define
Assess
Implement
June 9, 2004 VANHA 18
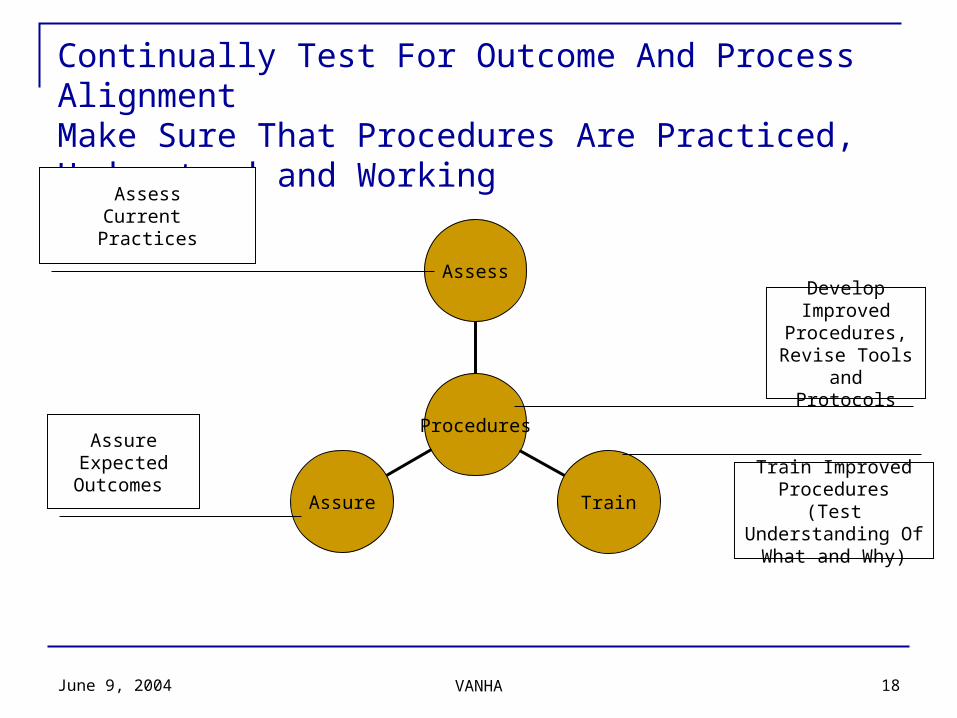
Continually Test For Outcome And Process AlignmentMake Sure That Procedures Are Practiced, Understood and Working
Procedures
Assure Train
Assess
AssessCurrent Practices
AssureExpected
Outcomes Train Improved Procedures
(Test Understanding Of What and Why)
Develop Improved
Procedures, Revise Tools and Protocols