Embed Size (px)
Citation preview

Rheumatoid arthritis: the importance of early diagnosis and
treatmentNovember 2011
Helen LinklaterConsultant Rheumatologist
Epsom and St Helier

The race to diagnosis...
• Common: 1% of adults worldwide
• Progressive: – joint pain– joint damage– increased mortality
• Estimated cost of sick leave/work-related disability for people with RA:
£1.8 billion a year!
DISABILITY

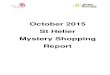
A new approach...Disease progression in RA
Emery P et al . Rheumatology 2008;47:392-398
© The Author 2007. Published by Oxford University Press on behalf of the British Society forRheumatology. All rights reserved. For Permissions, please email:[email protected]

Rheumatoid arthritis: progressivemetacarpophalangeal erosion


What is early RA?
• “Very early” = three months after disease onset (Hyrich, 2008)
– This may be a window of opportunity
• “Early” = 12 months into disease (Hyrich, 2008)
– Prompt introduction of DMARDs can lead to benefits up to 5 years after the drugs are introduced when compared with a delayed start (Raza, 2010)

Spotting a winner...
Early therapeutic intervention improves clinical outcomes
(van Dongen, 2007)
Undifferentiated inflammatory arthritis (anti-CCP positive) treated with 12/12 methotrexate - outcome at 18 months

Diagnosing early RA - before damage occurs
• Anti-CCP• Ultrasound• MRI imaging +/-
gadolinium

Anti-CCP
ACPA
• Anti-citrullinated peptide antibody (ACPA) - anti-cyclic citrullinated peptide (CCP)
Diagnosis
50% patients with RA have anti-CCP or IgM-RF several years before symptom onset (Nielen, 2004)
Strongly associated with genetic phenotypes associated with RA, and with smoking
Prognosis
Poorer response to therapy
Predicts erosions
(Aggarwal, 2009)
> 95% positive predictive value in early inflammatory arthritis

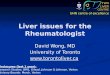
Ultrasound assessmentMCP joint
• Synovial hypertrophy• Synovial fluid Effusion
Synovial thickening
MC headPP head
MCP joint
• Erosion• Power Doppler
Erosion
Doppler signal
But operator dependent, non-standardised, variability...

ACR/EULAR criteria 2010
Target Population of theCriteria

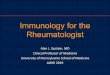
2010 ACR/EULARClassification Criteria for RA
JOINT DISTRIBUTION (0-5)1 large joint 0
2-10 large joints 1
1-3 small joints (large joints not counted) 2
4-10 small joints (large joints not counted) 3
>10 joints (at least one small joint) 5
SEROLOGY (0-3)Negative RF AND negative ACPA 0
Low positive RF OR low positive ACPA 2
High positive RF OR high positive ACPA 3
SYMPTOM DURATION (0-1)<6 weeks 0
=6 weeks 1
ACUTE PHASE REACTANTS (0-1)Normal CRP AND normal ESR 0
Abnormal CRP OR abnormal ESR 1
=6 = definiteRA
What if the score is <6?
Patient might fulfill thecriteria…
Prospectively over time(cumulatively)
Retrospectively if dataon all four domains havebeen adequately recordedin the past

A history of treatment in earlyRA
Steroids/DMARDs
NSAIDs
Conservative therapy
Newer biologics
Anti-TNF + DMARDs
Steroids/DMARDs
DMARD = Disease Modifying anti-Rheumatic drug
TNF = Tumour necrosis factor

Obstacles to treating early RA...
Services for people with rheumatoid arthritis 15 July 2009
- 50-75% people with RA delay seeking medical help from GP for 3 months following symptom onset
- 20% delay for 1 year
- Average length of time (symptom onset - Rx) 9 months
Subject of much research!

Combination therapy in early RA
“Despite …evidence infavour of intensive treatment strategies based on combinations of DMARDs with glucocorticoids... they are not often used in daily practice”
(Verschueren, 2011)
• Difficult to have complex treatment discussion at diagnosis
• Time limitations
• Lack of CNS support
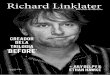
BeSt Study (2005)
2 DMARDs + steroid
DMARD + Infliximab
% without radiological progression

Summary
• New criteria explicitly designed to find early disease
• ACPA very specific
• USS/MRI imaging aids diagnosis
• Facilitates disease stratification and early treatment

Does this alter your practice?• Persistent joint swelling in
1 joint, or involvement of MCP or MTP joints = consider urgent referral (ideally within 6 wks of symptom onset)
• RhF and radiographs will probably be normal (NICE, 2009)

2010 ACR/EULARClassification Criteria for RA
JOINT DISTRIBUTION (0-5)1 large joint 0
2-10 large joints 1
1-3 small joints (large joints not counted) 2
4-10 small joints (large joints not counted) 3
>10 joints (at least one small joint) 5
SEROLOGY (0-3)Negative RF AND negative ACPA 0
Low positive RF OR low positive ACPA 2
High positive RF OR high positive ACPA 3
SYMPTOM DURATION (0-1)<6 weeks 0
=6 weeks 1
ACUTE PHASE REACTANTS (0-1)Normal CRP AND normal ESR 0
Abnormal CRP OR abnormal ESR 1
=6 = definiteRA
What if the score is <6?
Patient might fulfill thecriteria…
Prospectively over time(cumulatively)
Retrospectively if dataon all four domains havebeen adequately recordedin the past

References1. Hyrich, K Patients with suspected rheumatoid arthritis should be referred early to rheumatology BMJ 2008 336 : 215
2. Raza, K The Michael Mason prize: early rheumatoidarthritis—the window narrows Rheumatology 2010;49:406–410
3. Van Dongen H et al. Efficacy of Methotrexate Treatment in Patients With Probable Rheumatoid Arthritis Arthritis and Rheumatism 56, No. 5, May 2007, pp 1424–1432
4. Nielen M et al (2004) Specific Autoantibodies Precede the Symptoms of Rheumatoid Arthritis Arthritis and Rheumatism 50, (2) pp 380–386
5. Aggarwal, R et al (2009) Anti–Citrullinated Peptide Antibody Assays and Their Role in the Diagnosis of Rheumatoid Arthritis Arthritis & Rheumatism (Arthritis Care & Research) 61 (11) pp 1472–1483
5. ACR/EULAR Classification criteria for RA 2010
6. Verschueren P, Westhovens R Optimal care for early RA patients: the challenge of translating scientific data into clinical practice Rheumatology 2011;50:11941200
7. NICE guidance CG79 (Feb 2009) Rheumatoid arthritis: the management of rheumatoid arthritis in adults

Any Questions?