Embed Size (px)
Citation preview
717
RHEUMATOID ARTHRITIS IN A CHIPPEWA BAND
I. Pilot Screening Study of Disease Prevalence
JOAN HARVEY, MICHAEL LOTZE, and MARY BETTY STEVENS, with the assistance of GERTRUDE LAMBERT and DENNIS JACOBSON
The MiUe Lacs Band of Chippewa Indians in central Minnesota was screened for rheumatoid arthri- tis, with a 77% completion rate of the reservation cen- sus. Rheumatoid arthritis was found in marked excess, namely 6.8% of those evaluated or, minimally, 5.3% of the total band if all persons had been evaluated with no additional cases identified. This relatively closed popu- lation thus provides an opportunity to assess genetic and environmental factors of significance in this disease.
Rheumatoid arthritis has been detected world- wide and in diverse populations. The prevalence of defi- nite rheumatoid arthritis in these various groups has been surprisingly constant (1- 18) (Table l), ranging from 0. I % to 1.5% in 90% of the populations surveyed. Except for the finding of rheumatoid arthritis (RA) in 2.1% of a Jamaican population, the only report of higher disease prevalence concerned the Yakima In- dians in the State of Washington among whom 3.4% of the women studied had definite or classic rheumatoid arthritis according to the criteria of the American Rheu- matism Association (19).
From the Division of Rheumatology, The Johns Hopkins University School of Medicine and the National Institutes of Health.
Supported in part by the Arthritis Foundation Clinical Re- search Center and the Johns Hopkins NIAMDD Multipurpose Ar- thritis Center (P60 AM 20558).
Joan Harvey, MD: Postdoctoral Fellow; Michael Lotze, MD: Clinical Associate; Mary Betty Stevens, MD: Associate Professor of Medicine; Gertrude Lambert, RN. Dennis Jacobson, MD: Ne-la- Shing Clinic. Mille Lacs Reservation, Minnesota.
Address reprint requests to Dr. Stevens, Director, Rheuma- tology Division, Johns Hopkins University at Good Samaritan Hospi- tal, 5601 Loch Raven Blvd., Baltimore, Maryland 21239.
Submitted for publication August 1 I , 1980; accepted in re- vised form December 18, 1980.
While providing primary health care in rural Minnesota, we observed an apparent increase in rheu- matoid arthritis on a reservation of Chippewa native Americans. This prospective screening study was under- taken in the spring of 1978 to establish the prevalence of peripheral inflammatory joint disease, including RA, in this group. The data reported here not only establish an unusually high prevalence of rheumatoid arthritis in this Chippewa Band but also support the potential of this relatively closed population to provide added im- munogenetic insight into the disease.
METHODS Background. The Chippewa (or Ojibway) people are
thought to be part of the Algic group of American Indians. According to their tradition, the Chippewa had migrated from the Eastern seaboard to settle primarily in Canada, North Da- kota, Wisconsin, and Minnesota (20). As a hunting-and-gath- ering people, they participated in fur trade with the French and English during the eighteenth and nineteenth centuries, initially intermarrying with the French as well as other Indian tribes. However, since the eighteenth century, apparently there has been relatively little genetic mixing with whites.
Today, the majority of the Chippewa (approximately 15,000-20,000 persons) live in Minnesota and are divided into the Red Lake Band and the Minnesota Chippewa Tribe. The latter is composed of six geographic subdivisions, one of which is the Mille Lacs Band. The official voting roster of the Mille Lacs Band numbers 1,208 adults of whom 265 (22%) re- side at Vineland, a reservation established in 1855 on the western shore of Lake Mille Lacs in Central Minnesota. The Vineland population is a relatively stable and isolated one geographically and, by tradition, socially separate from other bands.
Study population selection. Mille Lacs Band members were selected for study only on the basis of their availability and willingness to participate. The January 1978 census of the Vineland Reservation which we obtained listed all adults aged
Arthritis and Rheumatism, Vol. 24, No. 5 (May 1981)
718 HARVEY ET AL
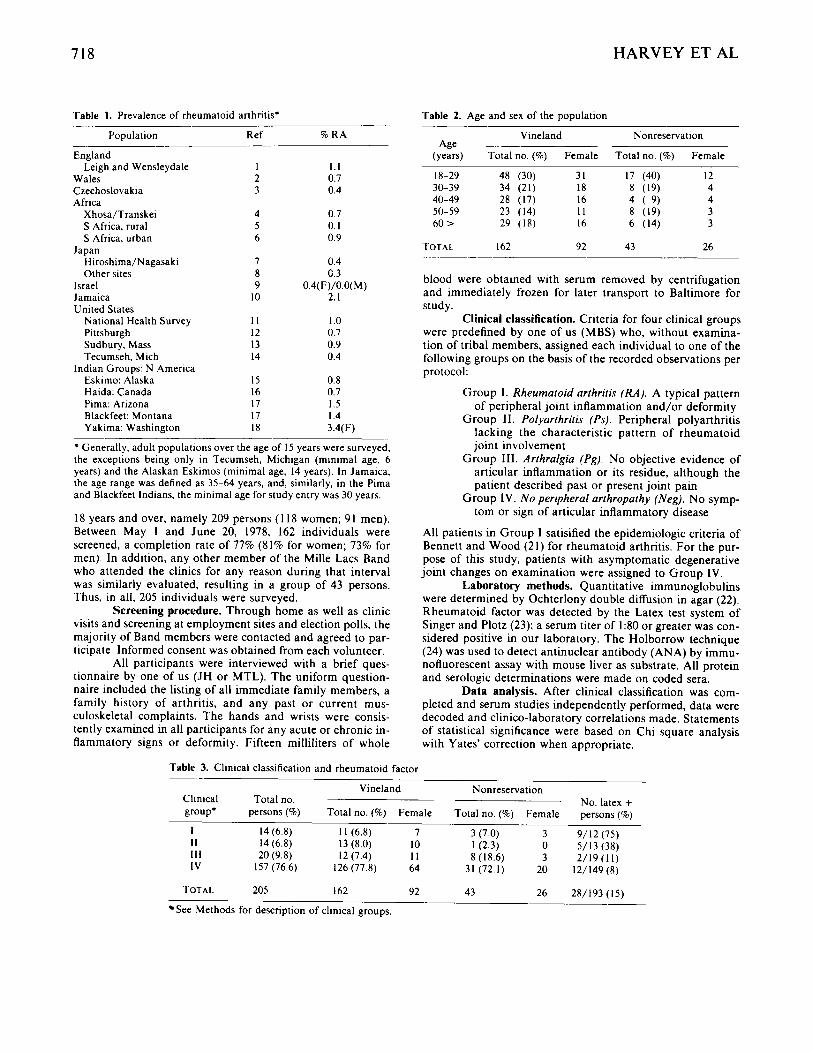
Table 1. Prevalence of rheumatoid arthritis’ .
Population Ref % RA -. - England
Wales 2 0.7 CLechoslovakia 3 0.4 Africa
Xhosa/Transkei 4 0.7 S Africa, rural 5 0. I S Africa, urban 6 0.9
iiiroshima/Nagasaki 7 0.4 Other sites 8 0.3
Israel 9 0.4( F)/O.O( M) Jamaica 10 2. I United States
National Health Survey I I I .o Pittsburgh 12 0.7 Sudbury, Mass 13 0.9 Tecumseh, Mich 14 0.4
Eskimo: Alaska 15 0.8 Haida: Canada 16 0.7 Pima: Arizona 17 1.5 Blackfeet: Montana 17 I .4 Yakima: Washington i n 3.4(F)
Leigh and Wensleydale I 1.1
Japan
Indian Groups: N America
* Generally, adult populations over the age of 15 years were surveyed, the exceptions being only in Tecumseh, Michigan (minimal age, 6 years) and the Alaskan Eskimos (minimal age, 14 years). In Jamaica. the age range was defined as 35-64 years, and, similarly, in the Pima and Blackfeet Indians, the minimal age for study entry was 30 years.
18 years and over, namely 209 persons ( 1 18 women; 91 men). Between May 1 and June 20, 1978. 162 individuals were screened, a completion rate of 77% (81% for women; 73% for men). In addition, any other member of the Mille Lacs Band who attended the clinics for any reason during that interval was similarly evaluated, resulting in a group of 43 persons. Thus, in all, 205 individuals were surveyed.
Screening procedure. Through home as well as clinic visits and screening at employment sites and election polls, the majority of Band members were contacted and agreed to par- ticipate. Informed consent was obtained from each volunteer.
All participants were interviewed with a brief ques- tionnaire by one of us (JH or MTL). The uniform question- naire included the listing of all immediate family members, a family history of arthritis, and any past or current mus- culoskeletal complaints. The hands and wrists were consis- tently examined in all participants for any acute or chronic in- flammatory signs or deformity. Fifteen milliliters of whole
Table 2. Age and sex of the population ____ Vineland Nonreservatioii
Age (years) Total no. (’70) Female Total no. (70) Female
18-29 48 (30) 31 17 (40) I2 30-39 34 (21) 18 8 (19) 4 40-49 28 (17) 16 4 ( 9) 4 50-59 23 (14) I 1 8 (19) 3 60 > 29 ( 1 8 ) 16 6 (14) 3
TOTAL I62 92 43 26
blood were obtained with serum removed by centrifugation and immediately frozen for later transport to Baltimore for study.
Clinical classification. Criteria for four clinical groups were predefined by one of us (MBS) who, without examina- tion of tribal members, assigned each individual to one of the following groups on the basis of the recorded observations per protocol:
Group I. Rheumatoid arthritis (RA). A typical pattern of peripheral joint inflammation and/or deformity
Group 11. Polyarthritis (Ps). Peripheral polyarthritis lacking the characteristic pattern of rheumatoid joint involvement
Group 111. Arthralgia (Pg). No objective evidence of articular inflammation or its residue, although the patient described past or present joint pain
Group IV. N o peripheral arthropathy (Neg). No symp- tom or sign of articular inflammatory disease
All patients in Group I satisified the epidemiologic criteria of Bennett and Wood (21) for rheumatoid arthritis. For the pur- pose of this study, patients with asymptomatic degenerative joint changes on examination were assigned to Group IV.
Laboratory methods. Quantitative immunoglobulins were determined by Ochterlony double diffusion in agar (22). Rheumatoid factor was detected by the Latex test system of Singer and Plotz (23); a serum titer of 1:80 or greater was con- sidered positive in our laboratory. The Holborrow technique (24) was used to detect antinuclear antibody (ANA) by immu- nofluorescent assay with mouse liver as substrate. All protein and serologic determinations were made on coded sera.
Data analysis. After clinical classification was com- pleted and serum studies independently performed, data were decoded and clinico-laboratory correlations made. Statements of statistical significance were based on Chi square analysis with Yates’ correction when appropriate.
Table 3. Clinical classification and rheumatoid factor ~-
Vineland Nonreservation Clinical Total no. No. latex + group* persons (‘76) Total no. (9’0) Female Total no. (76) Female persons (70)
I 14 (6.8) 1 1 (6.8) 7 3 (7.0) 3 9/12(75) I 1 14 (6.8) 13 (8.0) 10 I (2.3) 0 5/13(3X) 111 20 (9.8) 12 (7.4) I I 8 ( I 8.6) 3 2/19(11) IV 157 (76.6) 126(77.8) 64 31 (72.1) 20 12/149(8)
TOTAL 205 I62 92 43 26 28/193 (15)
See Methods for description of clinical groups.
RA IN THE CHIPPEWA 719
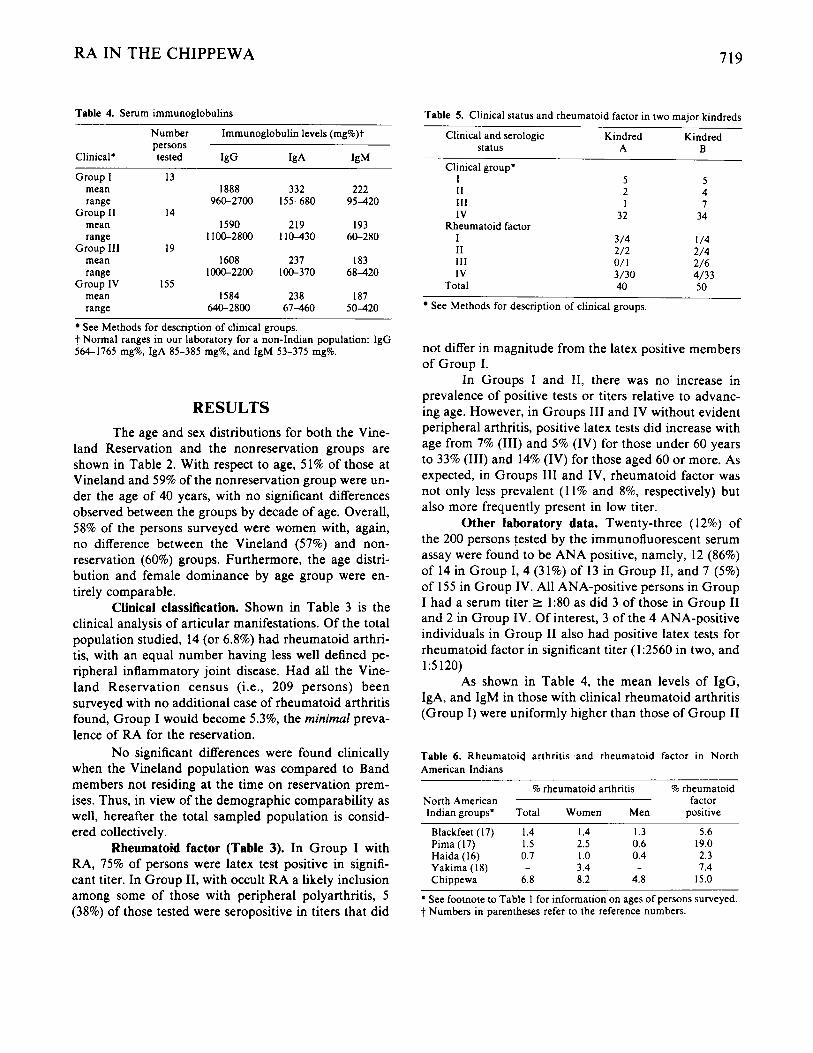
Table 4. Serum immunoglobulins
Number Immunoglobulin levels (mg%)t persons
Clinical* tested IgG IgA IgM Group I
mean range
Group I1 mean range
Group I l l mean range
Group IV mean range
13 1888
960-2700
I590 1100-2800
1608 1000-2200
I584 640-2800
14
19
155
332 155-680
219 1 1 0 4 3 0
237 100-370
238 6 7 4 6 0
222 95-420
193 60-280
183 68-420
187 5 0 4 2 0
See Methods for description of clinical groups. t Normal ranges in our laboratory for a non-hdian population: IgG 564-1765 mg%, IgA 85-385 mg%, and IgM 53-375 mg%.
RESULTS The age and sex distributions for both the Vine-
land Reservation and the nonreservation groups are shown in Table 2. With respect to age, 51% of those at Vineland and 59% of the nonreservation group were un- der the age of 40 years, with no significant differences observed between the groups by decade of age. Overall, 58% of the persons surveyed were women with, again, no difference between the Vineland (57%) and non- reservation (60%) groups. Furthermore, the age distri- bution and female dominance by age group were en- tirely comparable.
Clinical classification. Shown in Table 3 is the clinical analysis of articular manifestations. Of the total population studied, 14 (or 6.8%) had rheumatoid arthri- tis, with an equal number having less well defined pe- ripheral inflammatory joint disease. Had all the Vine- land Reservation census (i.e., 209 persons) been surveyed with no additional case of rheumatoid arthritis found, Group I would become 5.3%, the minimal preva- lence of RA for the reservation.
No significant differences were found clinically when the Vineland population was compared to Band members not residing at the time on reservation prem- ises. Thus, in view of the demographic comparability as well, hereafter the total sampled population is consid- ered collectively.
Rheumatoid factor (Table 3). In Group I with RA, 75% of persons were latex test positive in signifi- cant titer. In Group 11, with occult RA a likely inclusion among some of those with peripheral polyarthritis, 5 (38%) of those tested were seropositive in titers that did
Table 5. Clinical status and rheumatoid factor in two major kindreds
Clinical and serologic Kindred Kindred
Clinical group*
status A B
I 5 5 11 2 4 111 I 7 IV 32 34
I 3/4 1 /4 I1 2/2 2/4 111 o/ 1 2/6 IV 3/30 4/33
Total 40 50
Rheumatoid factor
See Methods for description of clinical groups.
not differ in magnitude from the latex positive members of Group I.
In Groups I and 11, there was no increase in prevalence of positive tests or titers relative to advanc- ing age. However, in Groups 111 and IV without evident peripheral arthritis, positive latex tests did increase with age from 7% (111) and 5% (IV) for those under 60 years to 33% (111) and 14% (IV) for those aged 60 or more. As expected, in Groups 111 and IV, rheumatoid factor was not only less prevalent (1 1% and 8%, respectively) but also more frequently present in low titer.
Other laboratory data. Twenty-three (12%) of the 200 persons tested by the immunofluorescent serum assay were found to be ANA positive, namely, 12 (86%) of 14 in Group I, 4 (31%) of 13 in Group 11, and 7 (5%) of 155 in Group IV. All ANA-positive persons in Group I had a serum titer 2 1:80 as did 3 of those in Group I1 and 2 in Group IV. Of interest, 3 of the 4 ANA-positive individuals in Group I1 also had positive latex tests for rheumatoid factor in significant titer (1:2560 in two, and 15120)
As shown in Table 4, the mean levels of IgG, IgA, and IgM in those with clinical rheumatoid arthritis (Group I) were uniformly higher than those of Group I1
Table 6. Rheumatoid arthritis and rheumatoid factor in North American Indians
~~ ~
% rheumatoid arthntis % rheumatoid North American factor Indian groups. Total Women Men positive
Blackfeet (17) 1.4 I .4 I .3 5.6 Pima ( 17) 1.5 2.5 0.6 19.0 Haida (16) 0.7 I .o 0.4 2.3
Chippewa 6.8 8.2 4.8 15.0 Yakima (18) - 3.4 - 7.4
* See footnote to Table 1 for information on ages of persons surveyed. t Numbers in parentheses refer to the reference numbers.
720 HARVEY ET AL
with undifferentiated arthritis and Groups I11 and IV without peripheral inflammatory joint disease. Of inter- est, no significant differences were found between Groups 11, 111, and IV.
The Chippewa kindreds. Family pedigrees de- rived from the screening questionnaire revealed a strik- ing degree of interrelationship. In fact, 90 (or 44%) of the 205 persons evaluated were identified with two large kindreds, emphasizing the closed nature of this Band’s membership.
Shown in Table 5 are the two major kinships of 40 and 50 members, respectively. Together they account for 10 (71%) of the 14 persons with rheumatoid arthritis in Group I and 6 (43%) of those with polyarthritis in Group 11.
Positive latex tests for rheumatoid factor were found in 8 members of Kindred A and 9 in Kindred B. Thus, of the 28 rheumatoid factor positive individuals in this Chippewa Band, 17 (61%) were clustered in these 2 families. Furthermore, of the Band members without peripheral arthritis in Groups I11 and IV, 9 (64%) of the 14 with rheumatoid factor were found in these kindreds. Advanced age did not satisfactorily explain this familial excess.
DISCUSSION These pilot data establish an unsually high prev-
alence of rheumatoid arthritis in the Mille Lacs Band of Chippewa Indians. Among Band members screened, RA was identified in 8.2% of women and 4.8% of men, with an overall disease prevalence of 6.8%. Had all Band members been available for study with no addi- tional cases found, the prevalence of rheumatoid arthri- tis in the group as a whole would become, minimally, 5.3% and, in women, 5.9%. Thus, as shown in Table 6, a prominent excess of this disease is present in this Chip- pewa Band compared to the larger Indian populations previously studied.
However, at this stage of population screening, our observations resist valid comparison with these other reported studies in view of different clinical screening and criteria and, most particularly, the intense familial interrelationships within the Chippewa Band.
Clinically, the population survey was accom- plished through hand and wrist examination after com- pletion of a standardized questionnaire focused on pres- ence and pattern of articular pain and swelling. Although the exclusion of serologic and radiographic data preclude application of the American Rheumatism Association’s (19) criteria, 13 persons (of 14) in Group I
would have nonetheless satisfied at least 5 of the revised Rome criteria (25) for active RA. Furthermore, 4 per- sons with polyarthritis (Group 11) would satisfy 5 cri- teria of the American Rheumatism Association for defi- nite RA if their latex test titers (15120 or greater) had entered our classification scheme. Thus, supported by the added excess of seropositivity in Group 11, our esti- mate by these pilot studies of the prevalence of RA al- most certainly represents under- rather than over- diagnosis. Such was predictable from our study design at the outset, namely, to identify as the first step only typical and unequivocal rheumatoid arthritis (i.e., Group 1).
Even more significant than the modified ap- proach to clinical categorization is the family structure of this group. Although the Mille Lacs Band was readily recognized as a small, geographically and socially iso- lated group, the degree of interrelationships among members became evident only on completion of the pi- lot screening. Few kindreds comprise the total popu- lation with, as noted earlier, two accounting for 71% of those with rheumatoid arthritis and 43% of those with less well defined polyarthritis. For the most part, the de- gree (if any) of familial clustering of RA or rheumatoid factor positivity has not been recorded in previously re- ported surveys. Whether the excess of rheumatoid ar- thritis in this Chippewa Band relates to genetic and/or environmental attributes is not apparent from these pi- lot observations but merits indepth study.
ACKNOWLEDGMENTS The understanding and cooperation of the Vineland
Reservation Business Committee and the Mille Lacs Band membership are gratefully acknowledged. Without their inter- est and support,, this study could not have been accomplished. Similarly, the support and endorsement of the National Health Service Corps and the Mille Lacs Family Health Cen- ter are appreciated.
REFERENCES 1. Lawrence JS: Prevalence of rheumatoid arthritis. AM
Rheum Dis 2011-17, 1961 2. Miall WE, Ball J, Kellgren JH: Prevalence of rheumatoid
arthritis in urban and rural populations in South Wales. Ann Rheum Dis 17:263-272, 1958
3. Sitaj S, Sebo M: Rheumatoid arthritis and ankylosing spondylitis in Czechoslovakia, Population Studies of the Rheumatic Diseases. Edited by PH Bennett, PHN Wood. Amsterdam, Excerpta Medica Foundation, 1968, pp 64- 66
4. Meyers OC, Daynes G, Beighton P: Rheumatoid arthritis

RA IN THE CHIPPEWA 72 1
5 .
6.
7.
8.
9.
10.
11.
12.
13.
14.
in a tribal Xhosa population in the Transkei, Southern Africa. Ann Rheum Dis 36:62-65, 1977 Beighton P, Solomon L, Valkenburg HA: Rheumatoid ar- thritis in a rural South African Negro population. Ann Rheum Dis 34:136-141, 1975 Solomon L, Robin G, Valkenburg HA: Rheumatoid ar- thritis in an urban South African population. Ann Rheum Dis 34:128-135, 1975 Wood JW, Kato H, Johnson KG, Uda Y, Russell WJ, Duff IF: Rheumatoid arthritis in Hiroshima and Naga- saki, Japan. Arthritis Rheum 10:21-31, 1967 Schichikawa K: Prevalence of rheumatic diseases in Ja- pan, Population Studies of the Rheumatic Diseases. Ed- ited by PH Bennett, PHN Wood. Amsterdam, Excerpta Medica Foundation, 1968, pp 55-59 Adler E, Abramson JH, Elkan Z, Hador SB, Goldberg R: Rheumatoid arthritis in a Jerusalem population. I. Epide- miology of the disease. Am J Epidemiol85:365-377, 1967 Lawrence JS, Brenner JM, Ball J, Burch TA: Rheumatoid arthritis in a subtropical population. Ann Rheum Dis
Engel A, Roberts J, Burch TA: Rheumatoid arthritis in adults, United States, 1960-1962. PHS Publication No. 1000, Series 11, No. 17. Washington, DC, U. S. Govern- ment Printing Office, 1966 Cobb S, Warren JE, Merchant WR, Thompson DJ: An estimate of the prevalence of rheumatoid arthritis. J Chron Dis 5:638-643, 1957 OSullivan JB, Cathcart ES: The prevalence of rheuma- toid arthritis. Ann Intern Med 76573-577, 1972 Mikkelson WM, Dodge HJ, Fuff IF, Kato H: Estimates of the prevalence of rheumatoid diseases in the population of Tecumseh, Michigan, 1959-60. J Chron Dis 20:251- 369. 1967
25~59-66, 1966
15. Beasley RP, Retaillia H, Healey LA: Prevalence of rheu- matoid arthritis in Alaskan Eskimos. Arthritis Rheum
16. Gofton JP, Rbbinson HS, Price GE: A study of rheumatic disease in a Canadian Indian population. 11. Rheumatoid arthritis. Ann Rheum Dis 23:364-371, 1964
17. OBrien WM, Bennett PH, Burch TA, Bunim JJ: A ge- netic study of rheumatoid arthritis and rheumatoid factor in Blackfeet and Pima Indians. Arthritis Rheum 10:163- 179, 1967
18. Beasley RP, Wilkins RF, Bennett PH: High prevalence of rheumatoid arthritis in Yakima Indians. Arthritis Rheum
19. Ropes MW, Bennett GA, Cobb MD, Jacox R, Jessar RA: 1958 revision of diagnostic criteria for rheumatoid arthri- tis. Bull Rheum Dis 9:175-176, 1958
20. Warren William W: History of the Ojibway Nation. Third edition. Minneapolis, Ress and Haines Inc., 1974
21. Bennett PH, Wood PHN: Population Studies of the Rheumatic Diseases. Amsterdam, Excerpta Medica Foun- dation, 1968, p 455
22. Fahey JL, Mckelvey EM: Quantitative determination of serum immune globulins in antibody-agar plates. J Im- munol94:84-90, 1965
23. Singer JM, Plotz CM: The latex fixation test: application to the serologic diagnosis of rheumatoid arthritis. Am J Med 21:888-892, 1956
24. Holborrow EJ, Weir DM, Johnson GD: A serum factor in lupus erythematosus with affinity for tissue nuclei. Br Med J 2:732-734, 1957
25. Kellgren JH: Diagnostic criteria for population studies. Bull Rheum Dis 13:291-292, 1962
16:737-742, 1973
16:743-748, 1973









