Embed Size (px)
Citation preview
Rheumatoid Arthritis, Brief Rheumatoid Arthritis, Brief Review of Differential Review of Differential Diagnosis and Initial Diagnosis and Initial
TreatmentTreatment
Jonathan S. Coblyn, M.D.Jonathan S. Coblyn, M.D.
Brigham and WomenBrigham and Women’’s Hospitals Hospital
DisclosuresDisclosures
CVSCVS
ConclusionConclusionA new era in the treatment of rheumatoid A new era in the treatment of rheumatoid
arthritisarthritis
•• Proof of principle has been established that Proof of principle has been established that selective targeting of pathogenic elements is selective targeting of pathogenic elements is therapeutically effective. therapeutically effective.
•• Early therapyEarly therapy--especially combination therapy especially combination therapy tied to improved outcomes.tied to improved outcomes.
•• The future is now! Less joint replacements and The future is now! Less joint replacements and improved morbidity and mortality now improved morbidity and mortality now evident.evident.
•• A plea. Refer to confirm diagnosis and initiate A plea. Refer to confirm diagnosis and initiate treatmenttreatment
The Rapid Pace of Drug The Rapid Pace of Drug ““DiscoveryDiscovery”” in Rheumatologyin Rheumatology
1995 2000 2006-2010
CsA leflunomide
celecoxibrofecoxib
etanercept
infliximabadalimumab
Rituximab/abataceptTocilizumab (2010)
Year Marketed for RA
The Characteristics of RAThe Characteristics of RA
Systemic chronic inflammatory diseaseSystemic chronic inflammatory disease•• Mainly affects synovial jointsMainly affects synovial joints
•• Variable expressionVariable expression•• Risk increased by both genetic and Risk increased by both genetic and
environmental factorsenvironmental factors•• Strongest genetic risk conferred by shared Strongest genetic risk conferred by shared
epitope in close association with class II epitope in close association with class II MHC gene, (HLA) DR4MHC gene, (HLA) DR4
•• Cigarette smoking clearly an environmental Cigarette smoking clearly an environmental triggertrigger
The Characteristics of RA, contThe Characteristics of RA, cont’’dd
•• Prevalence about 1%Prevalence about 1%
•• Worldwide distributionWorldwide distribution
•• Female: Male ratio 3:1Female: Male ratio 3:1
•• Peak age of onset 25 Peak age of onset 25 –– 50 years50 years•• Synovitis, but tends to spare the LS spineSynovitis, but tends to spare the LS spine
Joint Involvement on Presentation of RAJoint Involvement on Presentation of RA
PolyarticularPolyarticular 75%75%
Small joints of Small joints of hands and feethands and feet 60%60%
Large jointsLarge joints 30%30%
Large and Large and small jointssmall joints
10%10%
MonoarticularMonoarticular 25%25%
KneeKnee 50%50%
ShoulderShoulderWristWristHipHip 50%50%AnkleAnkleElbowElbow
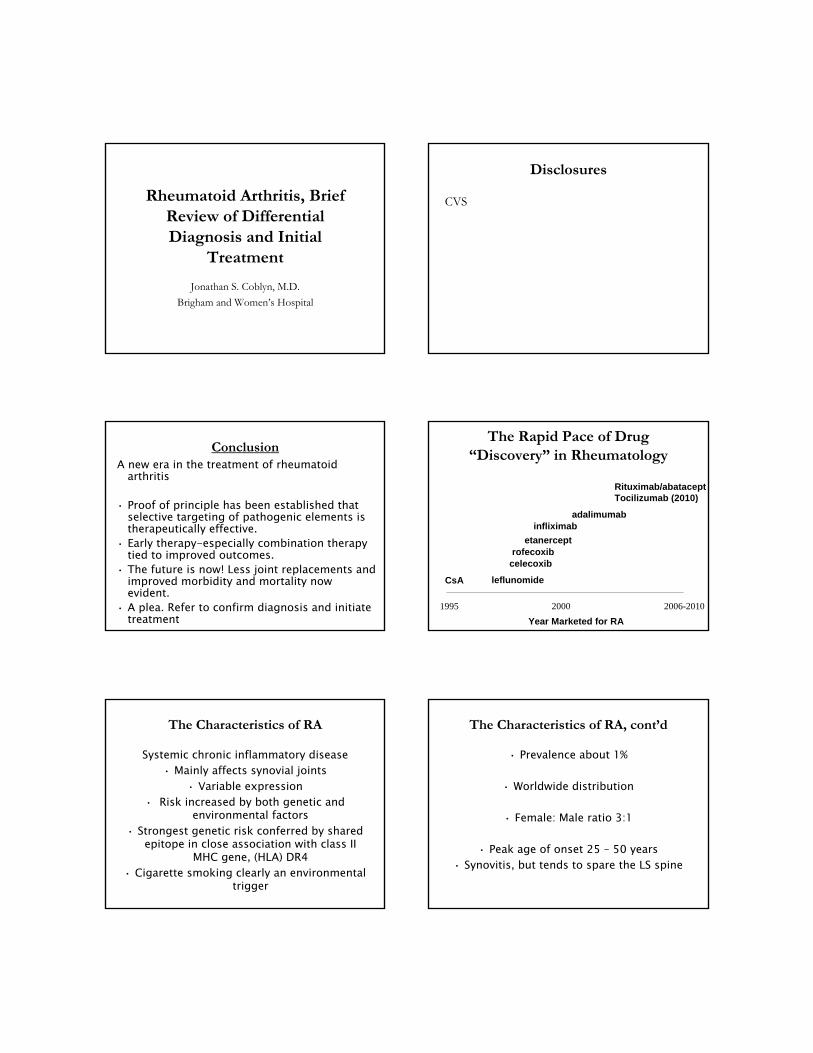
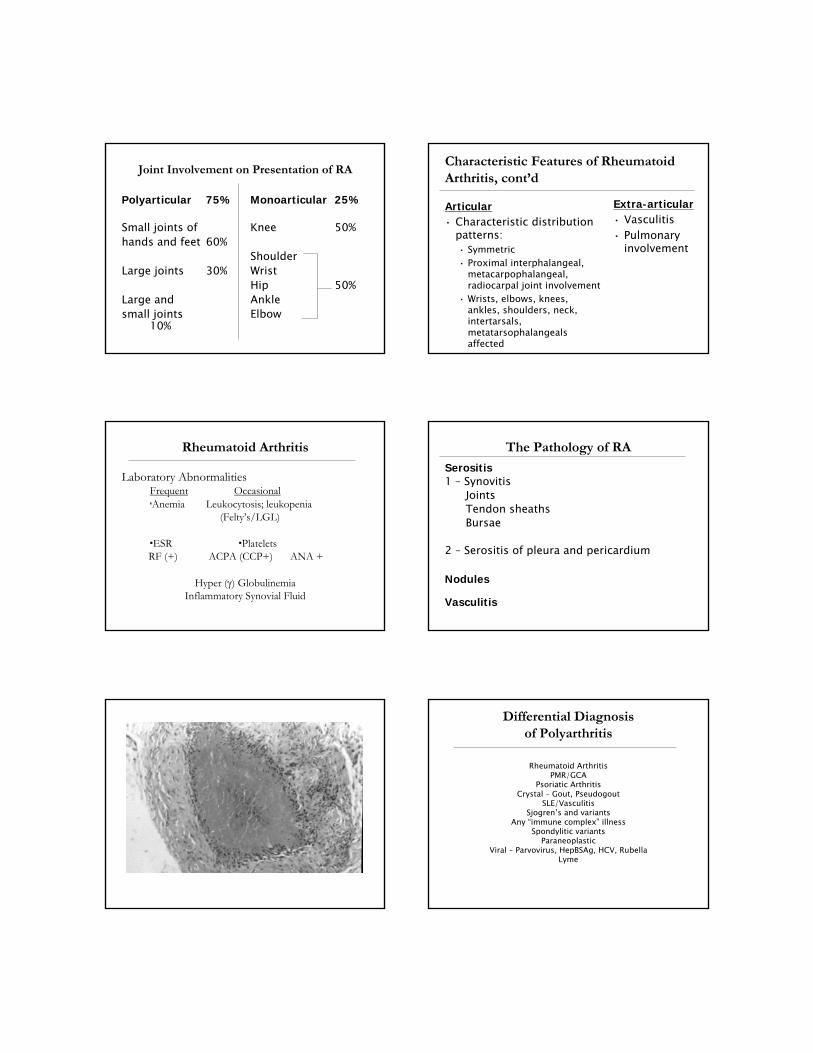
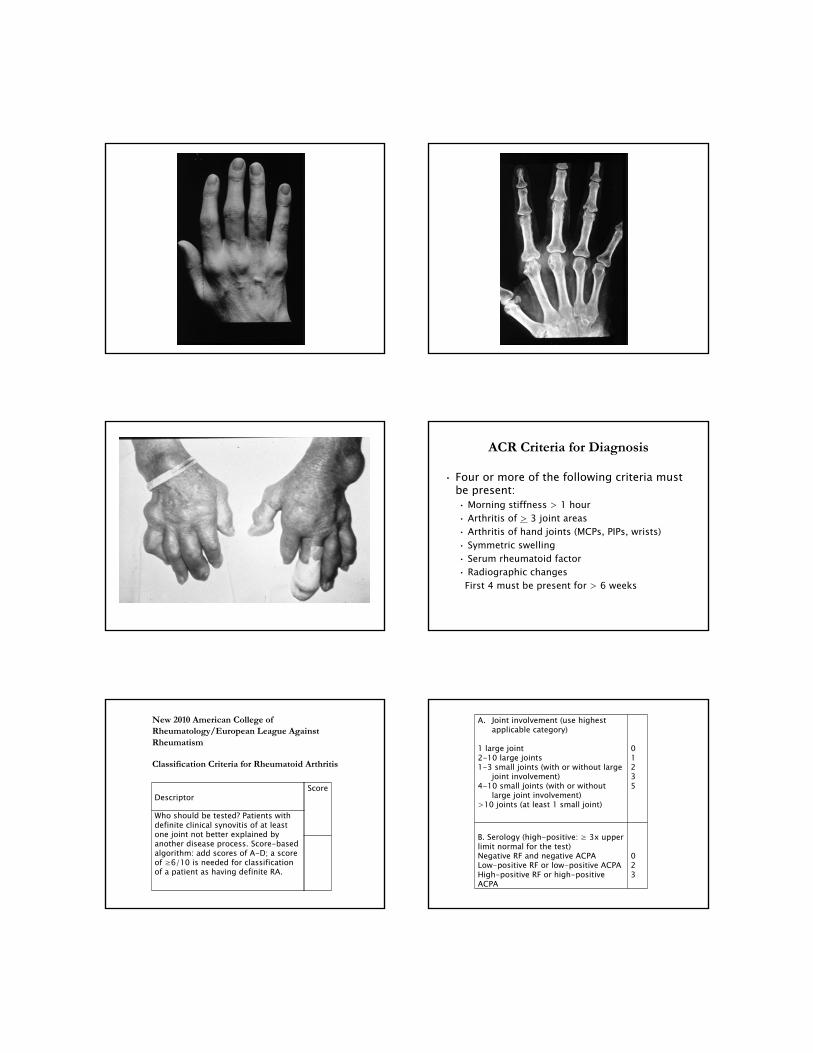
Characteristic Features of Rheumatoid Characteristic Features of Rheumatoid Arthritis, contArthritis, cont’’dd
ArticularArticular•• Characteristic distribution Characteristic distribution
patterns:patterns:•• SymmetricSymmetric•• Proximal interphalangeal, Proximal interphalangeal,
metacarpophalangeal, metacarpophalangeal, radiocarpal joint involvementradiocarpal joint involvement
•• Wrists, elbows, knees, Wrists, elbows, knees, ankles, shoulders, neck, ankles, shoulders, neck, intertarsals, intertarsals, metatarsophalangeals metatarsophalangeals affectedaffected
d
ExtraExtra--articulararticular•• VasculitisVasculitis•• Pulmonary Pulmonary
involvementinvolvement
Rheumatoid ArthritisRheumatoid Arthritis
Laboratory AbnormalitiesLaboratory AbnormalitiesFrequentFrequent OccasionalOccasionalAnemiaAnemia Leukocytosis; leukopenia Leukocytosis; leukopenia
(Felty(Felty’’s/LGL) s/LGL)
ESRESR PlateletsPlateletsRF (+)RF (+) ACPA (CCP+)ACPA (CCP+) ANA +ANA +
Hyper (Hyper () Globulinemia) GlobulinemiaInflammatory Synovial Fluid Inflammatory Synovial Fluid
The Pathology of RAThe Pathology of RA
SerositisSerositis1 1 –– SynovitisSynovitis
JointsJointsTendon sheathsTendon sheathsBursaeBursae
2 2 –– Serositis of pleura and pericardiumSerositis of pleura and pericardium
NodulesNodules
VasculitisVasculitis
Differential Diagnosis Differential Diagnosis of Polyarthritisof Polyarthritis
Rheumatoid ArthritisRheumatoid ArthritisPMR/GCAPMR/GCA
Psoriatic ArthritisPsoriatic ArthritisCrystal Crystal –– Gout, PseudogoutGout, Pseudogout
SLE/VasculitisSLE/VasculitisSjogrenSjogren’’s and variantss and variants
Any Any ““immune compleximmune complex”” illnessillnessSpondylitic variantsSpondylitic variants
ParaneoplasticParaneoplasticViral Viral –– Parvovirus, HepBSAg, HCV, RubellaParvovirus, HepBSAg, HCV, Rubella
LymeLyme
ACR Criteria for DiagnosisACR Criteria for Diagnosis
•• Four or more of the following criteria must Four or more of the following criteria must be present:be present:•• Morning stiffness > 1 hourMorning stiffness > 1 hour•• Arthritis of Arthritis of >> 3 joint areas3 joint areas•• Arthritis of hand joints (MCPs, PIPs, wrists)Arthritis of hand joints (MCPs, PIPs, wrists)•• Symmetric swellingSymmetric swelling•• Serum rheumatoid factorSerum rheumatoid factor•• Radiographic changesRadiographic changes
First 4 must be present for > 6 weeksFirst 4 must be present for > 6 weeks
Descriptor
Who should be tested? Patients with definite clinical synovitis of at least one joint not better explained by another disease process. Score-based algorithm: add scores of A-D; a score of ≥6/10 is needed for classification of a patient as having definite RA.
Score
New 2010 American College of Rheumatology/European League Against Rheumatism
Classification Criteria for Rheumatoid Arthritis
A. Joint involvement (use highest applicable category)
1 large joint2-10 large joints1-3 small joints (with or without large
joint involvement)4-10 small joints (with or without
large joint involvement)>10 joints (at least 1 small joint)
01235
B. Serology (high-positive: ≥ 3x upper limit normal for the test)Negative RF and negative ACPALow-positive RF or low-positive ACPAHigh-positive RF or high-positive ACPA
023
C. Acute phase reactantsNormal CRP and ESRAbnormally elevated CRP or ESR
01
D. Duration of symptoms<6 weeks≥6 weeks
01
ACPA: anti-citrullinated peptide antibodies; CRP: c-reactive protein; ESR: erythrocyte sedimentation rate; RA: rheumatoid arthritis
CAD in RACAD in RA
Risk of cardiovascular mortality in patients with Risk of cardiovascular mortality in patients with RA: a metaRA: a meta--analysis of observational studiesanalysis of observational studies
AvinaAvina--Zubieta et alZubieta et al
Arth Rheum 2008;59(12):1690Arth Rheum 2008;59(12):1690
24 studies/111,758 patients24 studies/111,758 patients——50% increased risk 50% increased risk of CVD deaths in RAof CVD deaths in RA
Systemic Disease AffectingSystemic Disease Affecting::
•• Heart and CADHeart and CAD
•• Lungs Lungs
•• Blood vesselsBlood vessels--vasculitisvasculitis
•• MusclesMuscles
•• EyesEyes
•• SkinSkin
•• Diarthrodial jointsDiarthrodial joints--““Unusual jointsUnusual joints””--cricoarytenoid and C cricoarytenoid and C --spinespine
•• Neurologic changesNeurologic changes
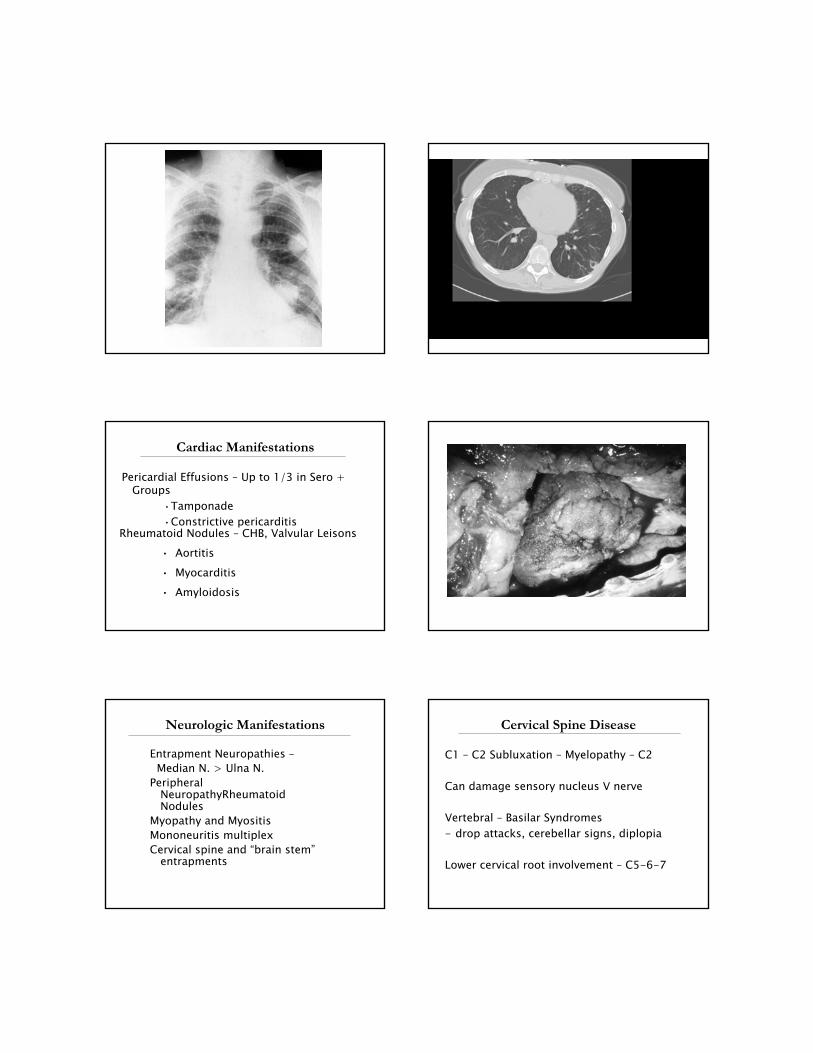
Pulmonary ManifestationsPulmonary Manifestations
Pleural EffusionsPleural Effusions•• Exudates > TransudatesExudates > Transudates•• Can have low PHCan have low PH•• Hallmark is low glucose Hallmark is low glucose –– Often < 30Often < 30
Rheumatoid nodulesRheumatoid nodules
Pulmonary ManifestationsPulmonary Manifestations
Interstitial FibrosisInterstitial Fibrosis
BrochiectasisBrochiectasis
Pulmonary HypertensionPulmonary Hypertension
VasculitisVasculitis
Bronchiolitis ObliteransBronchiolitis Obliterans
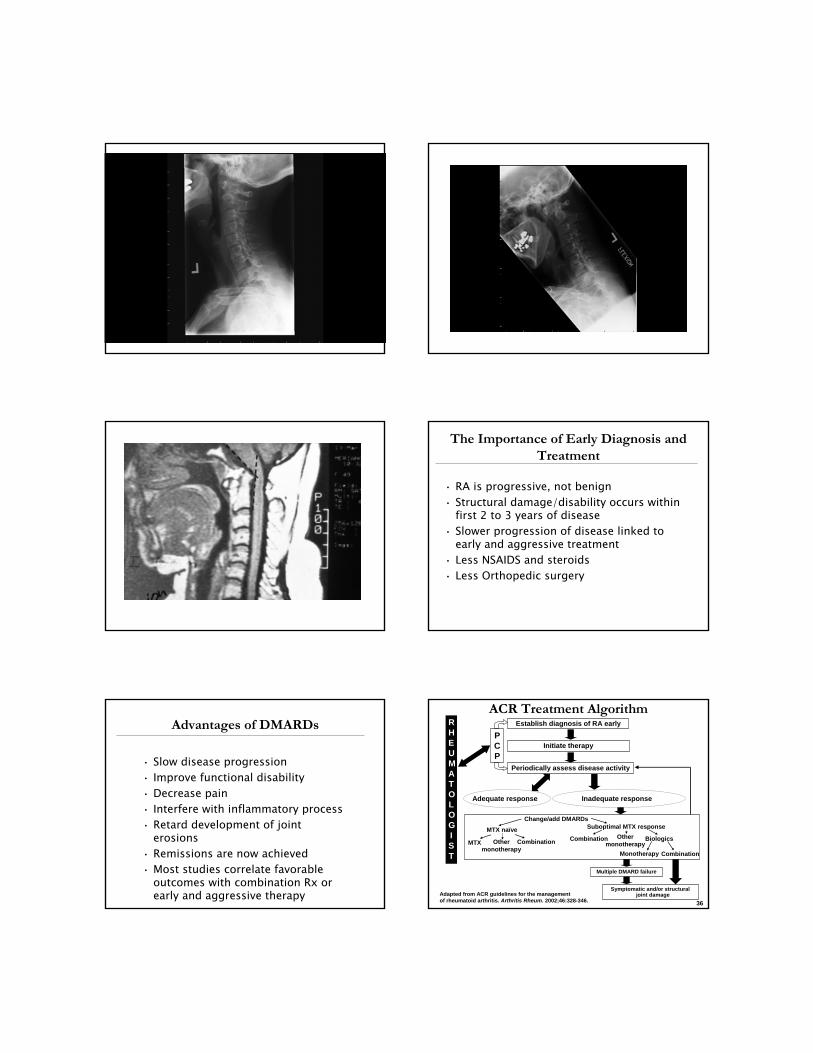
Cardiac ManifestationsCardiac Manifestations
Pericardial Effusions Pericardial Effusions –– Up to 1/3 in Sero + Up to 1/3 in Sero + GroupsGroups
••TamponadeTamponade••Constrictive pericarditisConstrictive pericarditis
Rheumatoid Nodules Rheumatoid Nodules –– CHB, Valvular LeisonsCHB, Valvular Leisons•• AortitisAortitis•• MyocarditisMyocarditis•• AmyloidosisAmyloidosis
Neurologic ManifestationsNeurologic Manifestations
Entrapment Neuropathies Entrapment Neuropathies ––Median N. > Ulna N.Median N. > Ulna N.
Peripheral Peripheral NeuropathyRheumatoid NeuropathyRheumatoid NodulesNodules
Myopathy and MyositisMyopathy and MyositisMononeuritis multiplexMononeuritis multiplexCervical spine and Cervical spine and ““brain stembrain stem””
entrapmentsentrapments
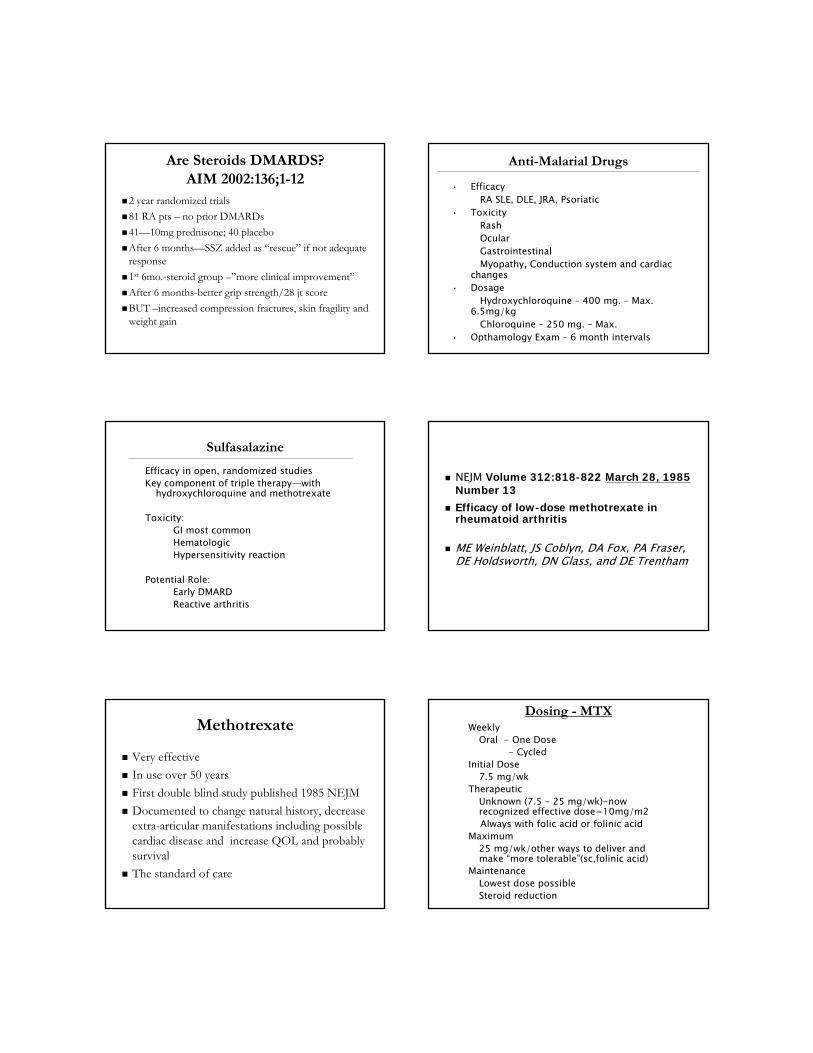
Cervical Spine DiseaseCervical Spine Disease
C1 C1 –– C2 Subluxation C2 Subluxation –– Myelopathy Myelopathy –– C2C2
Can damage sensory nucleus V nerveCan damage sensory nucleus V nerve
Vertebral Vertebral –– Basilar SyndromesBasilar Syndromes-- drop attacks, cerebellar signs, diplopiadrop attacks, cerebellar signs, diplopia
Lower cervical root involvement Lower cervical root involvement –– C5C5--66--77
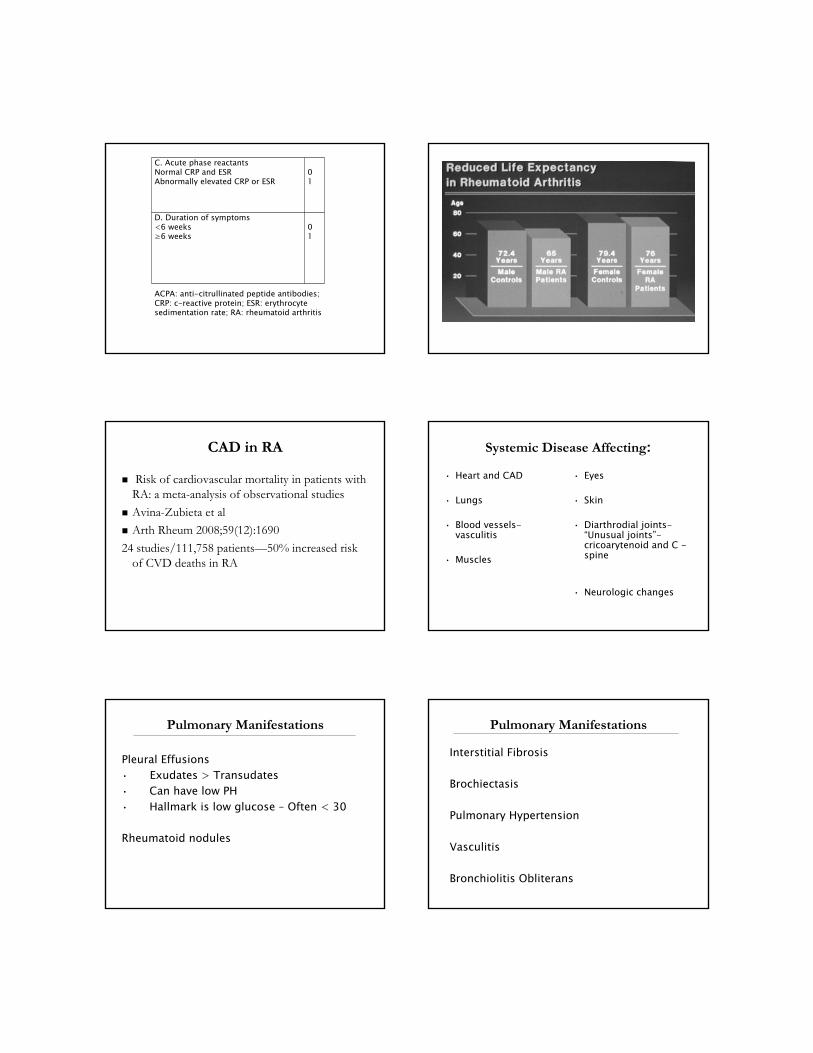
The Importance of Early Diagnosis and The Importance of Early Diagnosis and TreatmentTreatment
•• RA is progressive, not benignRA is progressive, not benign•• Structural damage/disability occurs within Structural damage/disability occurs within
first 2 to 3 years of diseasefirst 2 to 3 years of disease•• Slower progression of disease linked to Slower progression of disease linked to
early and aggressive treatmentearly and aggressive treatment•• Less NSAIDS and steroidsLess NSAIDS and steroids•• Less Orthopedic surgeryLess Orthopedic surgery
Advantages of DMARDsAdvantages of DMARDs
•• Slow disease progressionSlow disease progression•• Improve functional disabilityImprove functional disability•• Decrease painDecrease pain•• Interfere with inflammatory processInterfere with inflammatory process•• Retard development of joint Retard development of joint
erosionserosions•• Remissions are now achievedRemissions are now achieved•• Most studies correlate favorable Most studies correlate favorable
outcomes with combination Rx or outcomes with combination Rx or early and aggressive therapyearly and aggressive therapy
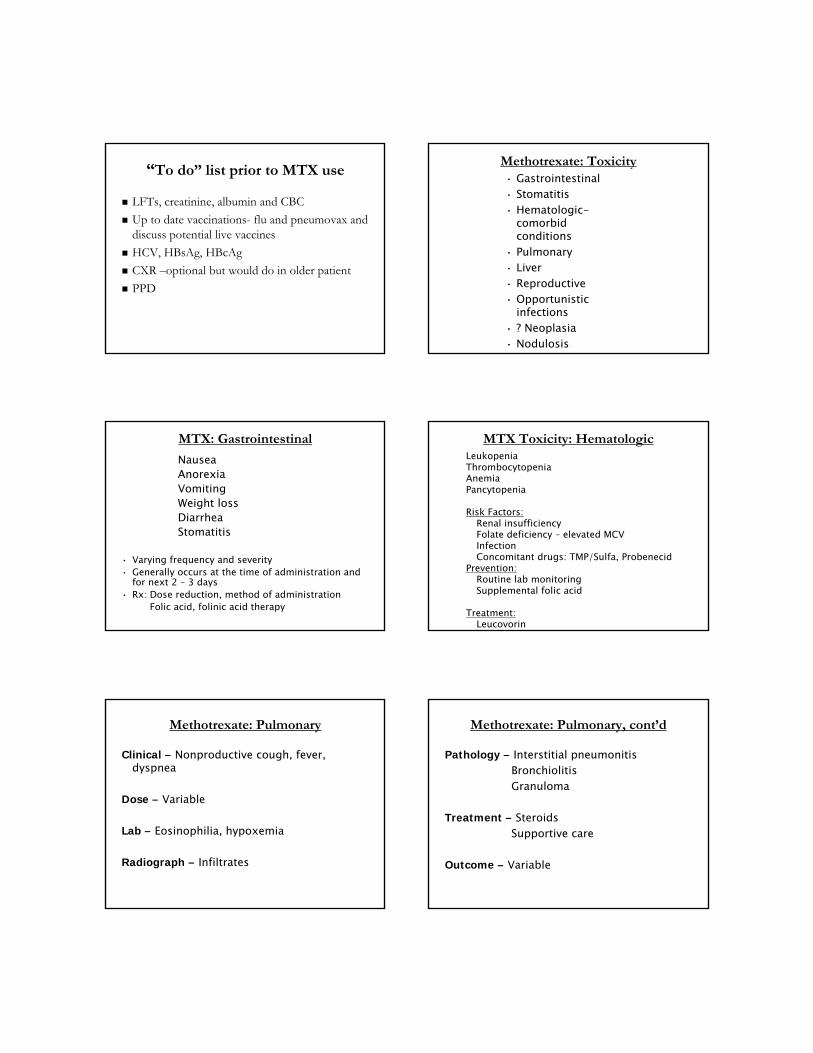
Establish diagnosis of RA early
Initiate therapyPCP
Periodically assess disease activity
RHEUMATOLOGIST
Adequate response Inadequate response
Change/add DMARDs
MTX naïve Suboptimal MTX response
MTX Othermonotherapy
Combination Combination Othermonotherapy
Biologics
Monotherapy Combination
Multiple DMARD failure
Symptomatic and/or structural joint damage
ACR Treatment AlgorithmACR Treatment Algorithm
Adapted from ACR guidelines for the management of rheumatoid arthritis. Arthritis Rheum. 2002;46:328-346. 36
Are Steroids DMARDS?Are Steroids DMARDS?AIM 2002:136;1AIM 2002:136;1--1212
2 year randomized trials 2 year randomized trials
81 RA pts 81 RA pts –– no prior DMARDsno prior DMARDs
4141——10mg prednisone; 40 placebo10mg prednisone; 40 placebo
After 6 monthsAfter 6 months——SSZ added as SSZ added as ““rescuerescue”” if not adequate if not adequate responseresponse
11stst 6mo.6mo.--steroid group steroid group ––””more clinical improvementmore clinical improvement””
After 6 monthsAfter 6 months--better grip strength/28 jt scorebetter grip strength/28 jt score
BUT BUT ––increased compression fractures, skin fragility and increased compression fractures, skin fragility and weight gainweight gain
AntiAnti--Malarial DrugsMalarial Drugs
•• EfficacyEfficacyRA SLE, DLE, JRA, PsoriaticRA SLE, DLE, JRA, Psoriatic
•• ToxicityToxicityRashRashOcularOcularGastrointestinalGastrointestinalMyopathy, Conduction system and cardiac Myopathy, Conduction system and cardiac
changeschanges•• DosageDosage
Hydroxychloroquine Hydroxychloroquine –– 400 mg. 400 mg. –– Max. Max. 6.5mg/kg6.5mg/kg
Chloroquine Chloroquine –– 250 mg. 250 mg. –– Max.Max.•• Opthamology Exam Opthamology Exam –– 6 month intervals6 month intervals
SulfasalazineSulfasalazine
Efficacy in open, randomized studiesEfficacy in open, randomized studiesKey component of triple therapyKey component of triple therapy——with with
hydroxychloroquine and methotrexatehydroxychloroquine and methotrexate
Toxicity:Toxicity:GI most commonGI most commonHematologicHematologicHypersensitivity reactionHypersensitivity reaction
Potential Role:Potential Role:Early DMARDEarly DMARDReactive arthritisReactive arthritis
NEJM NEJM Volume 312:818Volume 312:818--822822 March 28, 1985March 28, 1985Number 13Number 13
Efficacy of lowEfficacy of low--dose methotrexate in dose methotrexate in rheumatoid arthritisrheumatoid arthritis
ME Weinblatt, JS Coblyn, DA Fox, PA Fraser, ME Weinblatt, JS Coblyn, DA Fox, PA Fraser, DE Holdsworth, DN Glass, and DE TrenthamDE Holdsworth, DN Glass, and DE Trentham
Methotrexate Methotrexate
Very effectiveVery effective
In use over 50 yearsIn use over 50 years
First double blind study published 1985 NEJMFirst double blind study published 1985 NEJM
Documented to change natural history, decrease Documented to change natural history, decrease extraextra--articular manifestations including possible articular manifestations including possible cardiac disease and increase QOL and probably cardiac disease and increase QOL and probably survivalsurvival
The standard of careThe standard of care
Dosing Dosing -- MTXMTXWeeklyWeekly
Oral Oral -- One DoseOne Dose-- Cycled Cycled
Initial DoseInitial Dose7.5 mg/wk 7.5 mg/wk
TherapeuticTherapeuticUnknown (7.5 Unknown (7.5 –– 25 mg/wk)25 mg/wk)--now now recognized effective dose=10mg/m2recognized effective dose=10mg/m2Always with folic acid or folinic acidAlways with folic acid or folinic acid
MaximumMaximum25 mg/wk/other ways to deliver and 25 mg/wk/other ways to deliver and make make ““more tolerablemore tolerable””(sc,folinic acid)(sc,folinic acid)
MaintenanceMaintenanceLowest dose possibleLowest dose possibleSteroid reductionSteroid reduction
““To doTo do”” list prior to MTX uselist prior to MTX use
LFTs, creatinine, albumin and CBCLFTs, creatinine, albumin and CBC
Up to date vaccinationsUp to date vaccinations-- flu and pneumovax and flu and pneumovax and discuss potential live vaccinesdiscuss potential live vaccines
HCV, HBsAg, HBcAgHCV, HBsAg, HBcAg
CXR CXR ––optional but would do in older patientoptional but would do in older patient
PPDPPD
Methotrexate: ToxicityMethotrexate: Toxicity•• GastrointestinalGastrointestinal•• StomatitisStomatitis•• HematologicHematologic--
comorbid comorbid conditionsconditions
•• PulmonaryPulmonary•• LiverLiver•• ReproductiveReproductive•• Opportunistic Opportunistic
infectionsinfections•• ? Neoplasia? Neoplasia•• NodulosisNodulosis
MTX: GastrointestinalMTX: Gastrointestinal
NauseaNauseaAnorexiaAnorexiaVomitingVomitingWeight lossWeight lossDiarrheaDiarrheaStomatitisStomatitis
•• Varying frequency and severityVarying frequency and severity•• Generally occurs at the time of administration and Generally occurs at the time of administration and
for next 2 for next 2 –– 3 days3 days•• Rx: Dose reduction, method of administrationRx: Dose reduction, method of administration
Folic acid, folinic acid therapyFolic acid, folinic acid therapy
MTX Toxicity: HematologicMTX Toxicity: HematologicLeukopeniaLeukopeniaThrombocytopeniaThrombocytopeniaAnemiaAnemiaPancytopeniaPancytopenia
Risk Factors:Risk Factors:Renal insufficiencyRenal insufficiencyFolate deficiency Folate deficiency –– elevated MCVelevated MCVInfectionInfectionConcomitant drugs: TMP/Sulfa, ProbenecidConcomitant drugs: TMP/Sulfa, Probenecid
Prevention:Prevention:Routine lab monitoringRoutine lab monitoringSupplemental folic acidSupplemental folic acid
Treatment:Treatment:LeucovorinLeucovorin
Methotrexate: PulmonaryMethotrexate: Pulmonary
Clinical Clinical –– Nonproductive cough, fever, Nonproductive cough, fever, dyspneadyspnea
Dose Dose –– VariableVariable
Lab Lab –– Eosinophilia, hypoxemiaEosinophilia, hypoxemia
Radiograph Radiograph –– InfiltratesInfiltrates
Methotrexate: Pulmonary, contMethotrexate: Pulmonary, cont’’dd
Pathology Pathology –– Interstitial pneumonitisInterstitial pneumonitisBronchiolitisBronchiolitisGranulomaGranuloma
Treatment Treatment –– SteroidsSteroidsSupportive careSupportive care
Outcome Outcome –– Variable Variable
MTX: Opportunistic InfectionsMTX: Opportunistic Infections
•• Case Reports in Rheumatoid ArthritisCase Reports in Rheumatoid Arthritis•• Varying duration and dose of MTXVarying duration and dose of MTX•• OrganismsOrganisms
Herpes zosterHerpes zosterlocalizedlocalizeddisseminateddisseminated
PCPPCPNocardiaNocardiaCryptococcusCryptococcusHistoplasmosisHistoplasmosisAspergillusAspergillus
MTX: Opportunistic Infections, contMTX: Opportunistic Infections, cont’’dd
•• No concomitant steroids in several patientsNo concomitant steroids in several patients
•• Normal CBC/differentials observedNormal CBC/differentials observed
MTX: LiverMTX: Liver
Survey of Members of ACRSurvey of Members of ACR
58% responded58% responded
Identified 24 cases of serious liver diseaseIdentified 24 cases of serious liver diseaseCriteria: Clinical Criteria: Clinical –– 1717
Biopsy Biopsy –– 77
Mean age: 65 yearsMean age: 65 years
MTX: NodulesMTX: Nodules
•• Risk factors: UnknownRisk factors: Unknown
•• Dose and duration: VariableDose and duration: Variable
•• Location: Diffuse Location: Diffuse –– CutaneousCutaneous--FeetFeet–– VisceralVisceral
Treatment: UnknownTreatment: UnknownDose reductionDose reductionDrug cessationDrug cessationSteroids Steroids –– Systemic and injectionSystemic and injectionCombination Rx:Combination Rx:
Plaquenil, Sulfasalazine, CsAPlaquenil, Sulfasalazine, CsA
MTX Toxicity: LymphomaMTX Toxicity: Lymphoma
•• NHL NHL –– 3 patients3 patients•• Diffuse large cell, B cellDiffuse large cell, B cell•• Treatment duration > 2 yearsTreatment duration > 2 years•• No SjogrenNo Sjogren’’s symptomss symptoms
J Rheumatol 18: 1741J Rheumatol 18: 1741--1743, 19911743, 199119: 146219: 1462--1468, 19921468, 1992
Methotrexate Methotrexate
EfficacyEfficacy——Now established DMARDNow established DMARD Lancet 2002;359:1173 1240 Lancet 2002;359:1173 1240
consecutive pts with RAconsecutive pts with RA——treated with treated with mtx decreased mortality and c/v riskmtx decreased mortality and c/v risk——Other studies confirmed these Other studies confirmed these observationsobservations
Still unclear how much Still unclear how much ““betterbetter”” newer newer therapies aretherapies are
Established Gold StandardEstablished Gold Standard
Selection of an Initial DMARD: LeflunomideSelection of an Initial DMARD: Leflunomide
•• Early onset of Early onset of action (~ 4 weeks)action (~ 4 weeks)
•• Stabilized benefit Stabilized benefit for longfor long--term useterm use
•• Selectively targets Selectively targets autoimmune autoimmune lymphocytes to lymphocytes to reduce untoward reduce untoward AEsAEs
•• Toxicities: Toxicities: hepatotoxicity, hepatotoxicity, gastrointestinal,gastrointestinal,
•• HypertensionHypertension•• ?pulmonary?pulmonary•• neuropathyneuropathy
PROS CONSLeflunomideLeflunomide
•• Pyrimidine synthesis inhibitorPyrimidine synthesis inhibitor•• Selective for dihydroorotate dehydrogenaseSelective for dihydroorotate dehydrogenase•• Metabolized in liver to active metaboliteMetabolized in liver to active metabolite•• Well absorbed orallyWell absorbed orally•• Requires loading doseRequires loading dose•• Prolonged halfProlonged half--life (14 d)life (14 d)•• TeratogenicTeratogenic
Leflunomide DosingLeflunomide Dosing
•• Loading dose Loading dose ––variablevariable-- 100 mg x 3 days or 100 mg x 3 days or qodx3 or even weekly x3, but most often qodx3 or even weekly x3, but most often start daily dosing atstart daily dosing at
20 mg QD20 mg QD
•• Dose may be decreased to 10 mg QD if Dose may be decreased to 10 mg QD if tolerability issues arisetolerability issues arise
Adverse Events of Potential Clinical Adverse Events of Potential Clinical SignificanceSignificance
•• Gastrointestinal EventsGastrointestinal Events•• Allergic ReactionsAllergic Reactions•• InfectionsInfections•• Reversible AlopeciaReversible Alopecia•• HypertensionHypertension•• LFTs/Cirrhosis/?death if LFTs/Cirrhosis/?death if
unmonitoredunmonitored•• Potential teratogenesisPotential teratogenesis--
consider avoiding in child consider avoiding in child bearing age unless document bearing age unless document counselingcounseling
•• Cholestyramine use to decrease Cholestyramine use to decrease half life as decreases half life as decreases enterohepatic circulationenterohepatic circulation
Next Therapy After Methotrexate:Next Therapy After Methotrexate:How to Decide When and WhatHow to Decide When and What
Disease activityDisease activity——Use objective Use objective measurementsmeasurements——DAS, CDAIDAS, CDAI
Radiographic progressionRadiographic progression PatientPatient’’s appetite for risks appetite for risk Prior medical issues which may make Prior medical issues which may make
some therapies contraindicatedsome therapies contraindicated Economic review of systems!Economic review of systems! And how to decide next drug?And how to decide next drug?
Biologics in the Treatment Biologics in the Treatment of Rheumatoid Arthritisof Rheumatoid Arthritis
Biologic TherapiesBiologic Therapies
Changed the face of RAChanged the face of RA Induce remissionInduce remission Change the natural history even Change the natural history even
without a clinical improvement!without a clinical improvement! Adverse events but no Adverse events but no ““new signalsnew signals”” Early use in methotrexate Early use in methotrexate ““inadequate inadequate
respondersresponders”” But methotrexate is great in 20But methotrexate is great in 20--30% if 30% if
used correctlyused correctly
Cost of CareCost of Care--Risk and ExpenseRisk and Expense
Biologic Therapies as of 2012Biologic Therapies as of 2012
Five antiFive anti--tnf agentstnf agents--etanercept, etanercept, adalimumab, infliximab, golimumab adalimumab, infliximab, golimumab and certolizumab pegoland certolizumab pegol
IL1IL1--receptor antagonistreceptor antagonist——anakinraanakinra CoCo--stimulatory blocker abataceptstimulatory blocker abatacept B cell depletion rituximabB cell depletion rituximab IL6 receptor antagonist tocilizumabIL6 receptor antagonist tocilizumab
AntiAnti--Tnf TherapyTnf Therapy
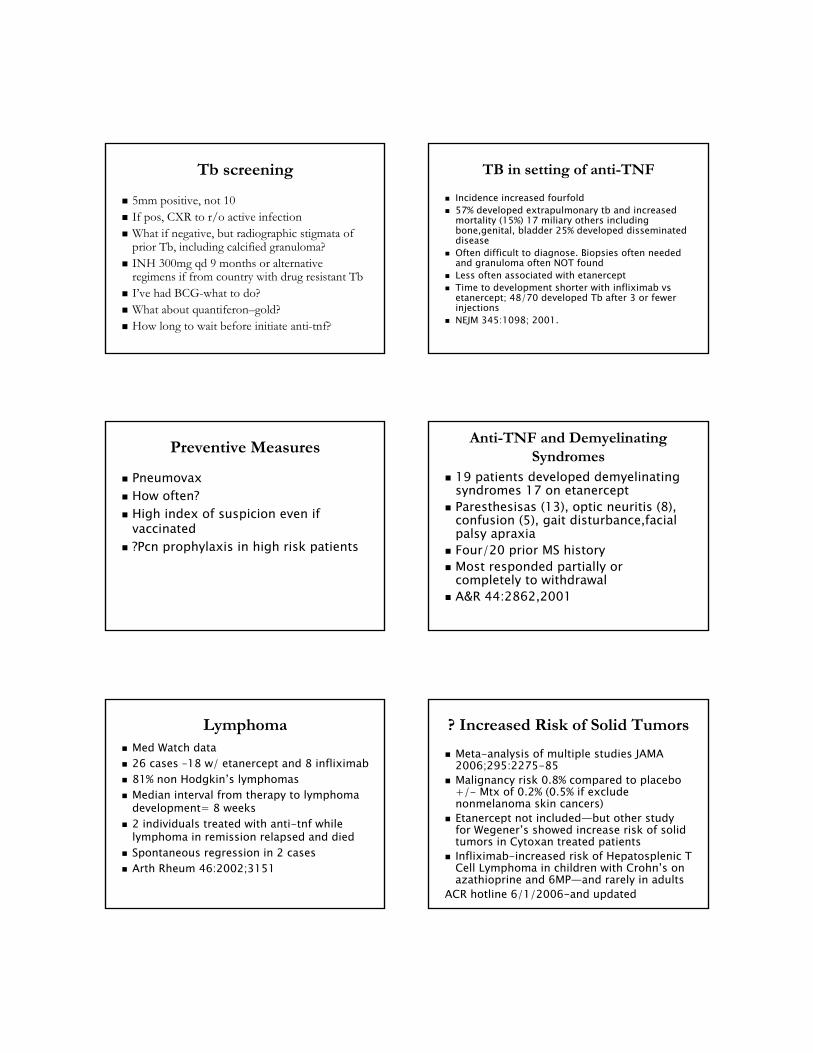
All have similar effectsAll have similar effects——with roughly a with roughly a response rate of 60response rate of 60--70%70%
Work in early disease and late Work in early disease and late diseasedisease——clinical outcomes better in clinical outcomes better in early diseaseearly disease
Stabilize Stabilize radiographicradiographic progressionprogression Decreased NSAIDS, steroids and mtx Decreased NSAIDS, steroids and mtx
dosesdoses Remission in some studies upon Remission in some studies upon
withdrawalwithdrawal
AntiAnti--TNF TherapiesTNF TherapiesAdverse EventsAdverse Events
Sepsis, Septic Joints,Pneumococci(Pneumovax)Sepsis, Septic Joints,Pneumococci(Pneumovax)Tuberculosis (PPD and treat prior)Tuberculosis (PPD and treat prior)
Injection site reactions/diffuse rashesInjection site reactions/diffuse rashesPulmonary symptomsPulmonary symptoms
? Increased risk lymphoma/solid tumors? Increased risk lymphoma/solid tumorsIncreased risk Class IIIIncreased risk Class III--IV CHFIV CHF
NeurologicNeurologic--demyelinationdemyelinationHematologicHematologic--pancytopeniapancytopeniaAutoimmune diseasesAutoimmune diseases--SLESLE
?LFT abnormalities?LFT abnormalities
Tb screeningTb screening
5mm positive, not 105mm positive, not 10 If pos, CXR to r/o active infectionIf pos, CXR to r/o active infection What if negative, but radiographic stigmata of What if negative, but radiographic stigmata of
prior Tb, including calcified granuloma?prior Tb, including calcified granuloma? INH 300mg qd 9 months or alternative INH 300mg qd 9 months or alternative
regimens if from country with drug resistant Tbregimens if from country with drug resistant Tb II’’ve had BCGve had BCG--what to do?what to do? What about quantiferonWhat about quantiferon––gold?gold? How long to wait before initiate antiHow long to wait before initiate anti--tnf?tnf?
TB in setting of antiTB in setting of anti--TNFTNF
Incidence increased fourfoldIncidence increased fourfold 57% developed extrapulmonary tb and increased 57% developed extrapulmonary tb and increased
mortality (15%) 17 miliary others including mortality (15%) 17 miliary others including bone,genital, bladder 25% developed disseminated bone,genital, bladder 25% developed disseminated diseasedisease
Often difficult to diagnose. Biopsies often needed Often difficult to diagnose. Biopsies often needed and granuloma often NOT foundand granuloma often NOT found
Less often associated with etanerceptLess often associated with etanercept Time to development shorter with infliximab vs Time to development shorter with infliximab vs
etanercept; 48/70 developed Tb after 3 or fewer etanercept; 48/70 developed Tb after 3 or fewer injectionsinjections
NEJM 345:1098; 2001.NEJM 345:1098; 2001.
Preventive MeasuresPreventive Measures
PneumovaxPneumovax How often?How often? High index of suspicion even if High index of suspicion even if
vaccinatedvaccinated ?Pcn prophylaxis in high risk patients?Pcn prophylaxis in high risk patients
AntiAnti--TNF and Demyelinating TNF and Demyelinating SyndromesSyndromes
19 patients developed demyelinating 19 patients developed demyelinating syndromes 17 on etanerceptsyndromes 17 on etanercept
Paresthesisas (13), optic neuritis (8), Paresthesisas (13), optic neuritis (8), confusion (5), gait disturbance,facial confusion (5), gait disturbance,facial palsy apraxiapalsy apraxia
Four/20 prior MS historyFour/20 prior MS history Most responded partially or Most responded partially or
completely to withdrawalcompletely to withdrawal A&R 44:2862,2001A&R 44:2862,2001
LymphomaLymphoma Med Watch dataMed Watch data 26 cases 26 cases ––18 w/ etanercept and 8 infliximab18 w/ etanercept and 8 infliximab 81% non Hodgkin81% non Hodgkin’’s lymphomass lymphomas Median interval from therapy to lymphoma Median interval from therapy to lymphoma
development= 8 weeksdevelopment= 8 weeks 2 individuals treated with anti2 individuals treated with anti--tnf while tnf while
lymphoma in remission relapsed and diedlymphoma in remission relapsed and died Spontaneous regression in 2 casesSpontaneous regression in 2 cases Arth Rheum 46:2002;3151Arth Rheum 46:2002;3151
? Increased Risk of Solid Tumors? Increased Risk of Solid Tumors
MetaMeta--analysis of multiple studies JAMA analysis of multiple studies JAMA 2006;295:22752006;295:2275--8585
Malignancy risk 0.8% compared to placebo Malignancy risk 0.8% compared to placebo +/+/-- Mtx of 0.2% (0.5% if exclude Mtx of 0.2% (0.5% if exclude nonmelanoma skin cancers)nonmelanoma skin cancers)
Etanercept not includedEtanercept not included——but other study but other study for Wegenerfor Wegener’’s showed increase risk of solid s showed increase risk of solid tumors in Cytoxan treated patientstumors in Cytoxan treated patients
InfliximabInfliximab--increased risk of Hepatosplenic T increased risk of Hepatosplenic T Cell Lymphoma in children with CrohnCell Lymphoma in children with Crohn’’s on s on azathioprine and 6MPazathioprine and 6MP——and rarely in adultsand rarely in adults
ACR hotline 6/1/2006ACR hotline 6/1/2006--and updatedand updated
AntiAnti--TNF and CHFTNF and CHF
Increased expression of tnf and response to Increased expression of tnf and response to treatment in animal modelstreatment in animal models
Human experience: Study using infliximab Human experience: Study using infliximab in 150 patients with Class IIIin 150 patients with Class III--IV CHF. IV CHF. Randomly Rx with placebo, 5, 10 mg/kg at Randomly Rx with placebo, 5, 10 mg/kg at 0,2, and 6 weeks0,2, and 6 weeks
No improvement despite modest increase in No improvement despite modest increase in ef at 5mg/kg dose, BUT increased hosp. ef at 5mg/kg dose, BUT increased hosp. and death in 10mg/kg group.and death in 10mg/kg group.
Role remains unclear as RA increases risk of Role remains unclear as RA increases risk of CHFCHF
Circulation 107: 3133,2003.Circulation 107: 3133,2003.
Case Report LevelCase Report Level
Pancytopenia and aplasiaPancytopenia and aplasia Granulomatous pulmonary diseaseGranulomatous pulmonary disease Vasculitis and common Injection site Vasculitis and common Injection site
reactionsreactions SLE type glomerulonephritisSLE type glomerulonephritis
Absolute Contraindications to Absolute Contraindications to TNFTNF--BlockersBlockers
CHF III/IVCHF III/IV Active/latent TbActive/latent Tb Active infectionActive infection Active or recent h/o malignancy (solid Active or recent h/o malignancy (solid
tumors)tumors) MS/optic neuritisMS/optic neuritis h/o lymphomah/o lymphoma Live vaccinesLive vaccines AnaphylaxisAnaphylaxis
Adapted Semin A&R 2005;34Adapted Semin A&R 2005;34
Newer Biologics in RANewer Biologics in RA
AbataceptAbatacept RituximabRituximab TocilizumabTocilizumab
How many antiHow many anti--TNFs should we try?TNFs should we try?Which one to select??? Use these first?Which one to select??? Use these first??Difference in side effects?Difference in side effects
ABATACEPTABATACEPT
Novel mechanism of actionNovel mechanism of actionBlocks cell coBlocks cell co--activation pathwayactivation pathwayApproved for use in RA and in evaluation in Approved for use in RA and in evaluation in
other rheumatic diseasesother rheumatic diseasesMonthly infusionsMonthly infusionsSimilar risks to anti tnf but less often TbSimilar risks to anti tnf but less often TbMay be used with or without mtxMay be used with or without mtxUsually after tnf Usually after tnf ““failurefailure””——response rate response rate
50%50%Onset 4Onset 4--16 weeks with improvement in 16 weeks with improvement in
fatigue and qol dramatic in some casesfatigue and qol dramatic in some cases
Interrupts Autoimmune Response Underlying RA
Abatacept (CTLA4Ig): Mechanism Abatacept (CTLA4Ig): Mechanism of Actionof Action
CTLA4Ig BlocksActivation
Normal Activation
Signal 1Signal 2
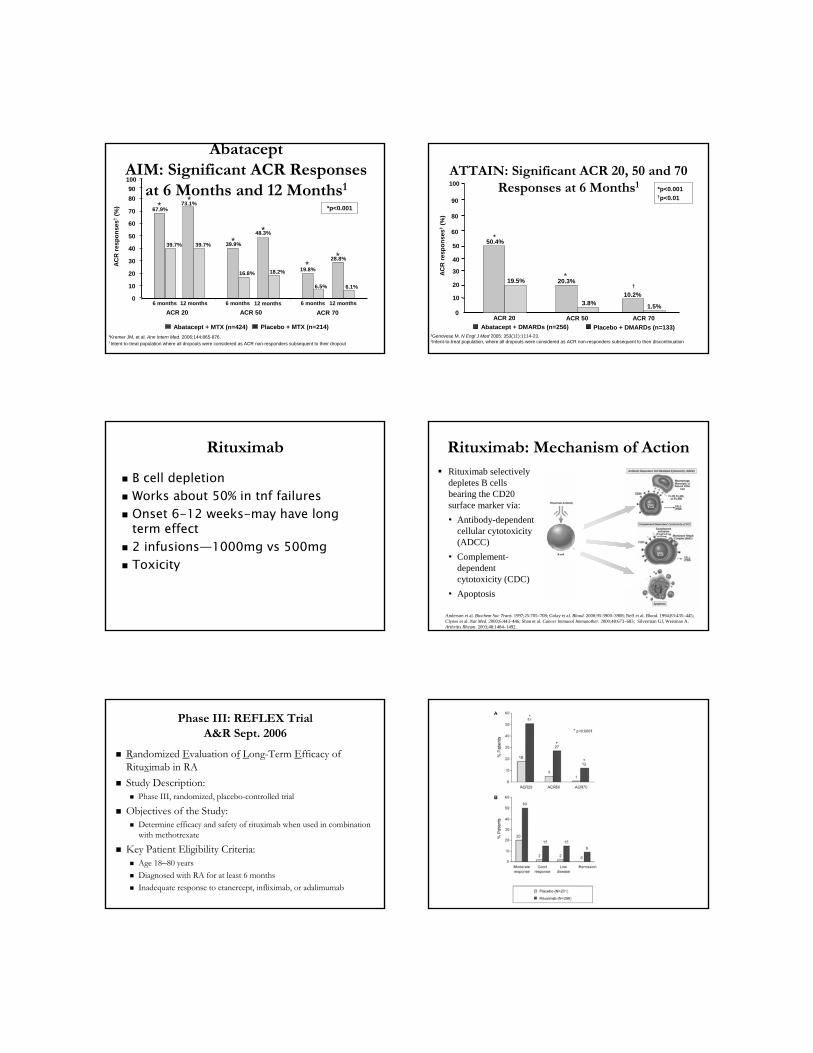
AbataceptAbataceptAIM: Significant ACR Responses AIM: Significant ACR Responses
at 6 Months and 12 Monthsat 6 Months and 12 Months11
AC
R r
esp
on
ses†
(%)
†Intent-to-treat population where all dropouts were considered as ACR non-responders subsequent to their dropout
0
10
20
30
40
50
60
70
80
ACR 20 ACR 50 ACR 70
67.9%
39.7%
*
39.9%
16.8%19.8%
6.5%
73.1%
39.7%
48.3%
18.2%
28.8%
6.1%
6 months 12 months6 months 6 months12 months12 months
*
**
**
Abatacept + MTX (n=424) Placebo + MTX (n=214)
*p<0.001
90
100
1Kremer JM, et al. Ann Intern Med. 2006;144:865-876.
ATTAIN: Significant ACR 20, 50 and 70 ATTAIN: Significant ACR 20, 50 and 70 Responses at 6 MonthsResponses at 6 Months11
1Genovese M. N Engl J Med 2005; 353(11):1114-23.‡Intent-to-treat population, where all dropouts were considered as ACR non-responders subsequent to their discontinuation
50.4%
AC
R r
esp
on
ses‡
(%)
ACR 50 ACR 70
10.2%3.8%
20.3%
1.5%0
10
20
Abatacept + DMARDs (n=256) Placebo + DMARDs (n=133)
*p<0.001 †p<0.01
30
40
50
19.5%
ACR 20
60
80
90
100
*
*†
RituximabRituximab
B cell depletionB cell depletion Works about 50% in tnf failuresWorks about 50% in tnf failures Onset 6Onset 6--12 weeks12 weeks--may have long may have long
term effectterm effect 2 infusions2 infusions——1000mg vs 500mg1000mg vs 500mg ToxicityToxicity
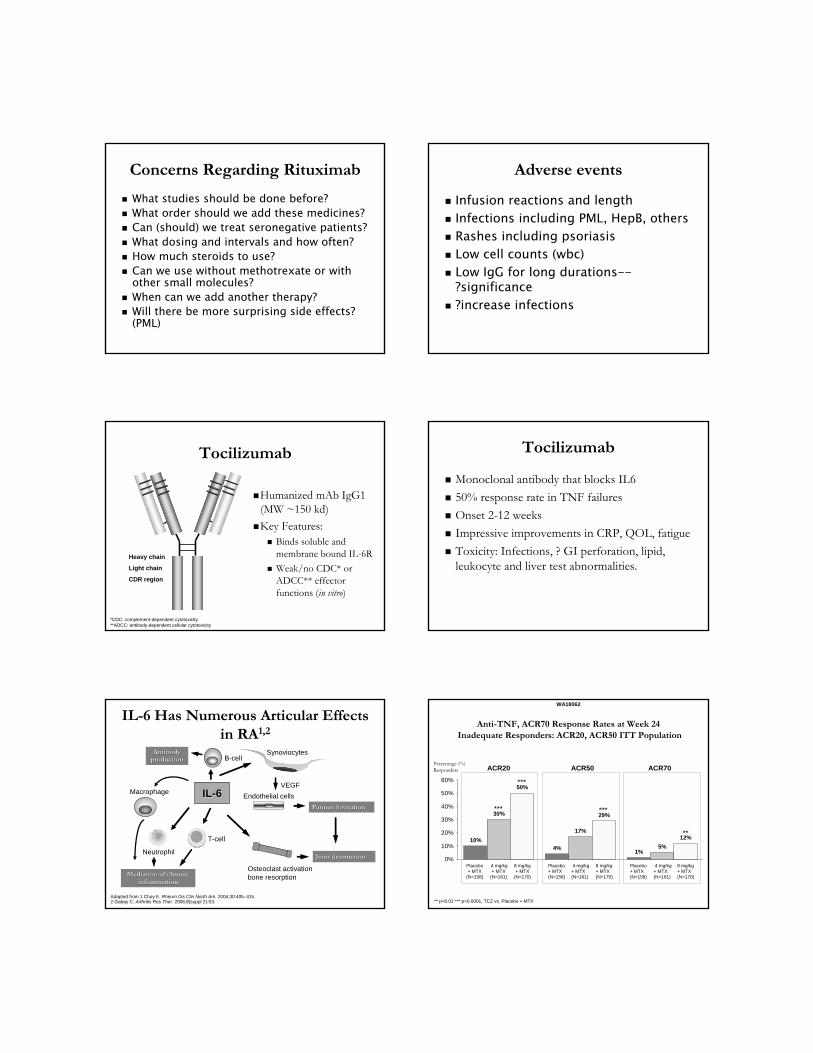
Rituximab: Mechanism of ActionRituximab: Mechanism of Action Rituximab selectively
depletes B cells bearing the CD20 surface marker via:
• Antibody-dependent cellular cytotoxicity (ADCC)
• Complement-dependent cytotoxicity (CDC)
• Apoptosis
Anderson et al. Biochem Soc Trans. 1997;25:705–708; Golay et al. Blood. 2000;95:3900–3908; Reff et al. Blood. 1994;83:435–445; Clynes et al. Nat Med. 2000;6:443–446; Shan et al. Cancer Immunol Immunother. 2000;48:673–683; Silverman GJ, Weisman A. Arthritis Rheum. 2003;48:1484–1492.
Phase III: REFLEX TrialPhase III: REFLEX TrialA&R Sept. 2006A&R Sept. 2006
RRandomized andomized EEvaluation ovaluation off LLongong--Term Term EEfficacy of fficacy of RituRituxximab in RA imab in RA
Study Description:Study Description: Phase III, randomized, placeboPhase III, randomized, placebo--controlled trialcontrolled trial
Objectives of the Study:Objectives of the Study: Determine efficacy and safety of rituximab when used in combinatDetermine efficacy and safety of rituximab when used in combination ion
with methotrexatewith methotrexate
Key Patient Eligibility Criteria:Key Patient Eligibility Criteria: Age 18Age 18––80 years80 years
Diagnosed with RA for at least 6 monthsDiagnosed with RA for at least 6 months
Inadequate response to etanercept, infliximab, or adalimumabInadequate response to etanercept, infliximab, or adalimumab
Concerns Regarding RituximabConcerns Regarding Rituximab
What studies should be done before?What studies should be done before? What order should we add these medicines?What order should we add these medicines? Can (should) we treat seronegative patients?Can (should) we treat seronegative patients? What dosing and intervals and how often?What dosing and intervals and how often? How much steroids to use?How much steroids to use? Can we use without methotrexate or with Can we use without methotrexate or with
other small molecules?other small molecules? When can we add another therapy?When can we add another therapy? Will there be more surprising side effects? Will there be more surprising side effects?
(PML)(PML)
Adverse eventsAdverse events
Infusion reactions and lengthInfusion reactions and length Infections including PML, HepB, othersInfections including PML, HepB, others Rashes including psoriasisRashes including psoriasis Low cell counts (wbc)Low cell counts (wbc) Low IgG for long durationsLow IgG for long durations----
?significance?significance ?increase infections?increase infections
TocilizumabTocilizumab
Humanized mAb IgG1 Humanized mAb IgG1 (MW ~150 kd)(MW ~150 kd)
Key Features:Key Features: Binds soluble and Binds soluble and
membrane bound ILmembrane bound IL--6R 6R
Weak/no CDC* or Weak/no CDC* or ADCC** effector ADCC** effector functions (functions (in vitroin vitro))
Heavy chain
Light chain
CDR region
*CDC: complement*CDC: complement--dependent cytotoxicitydependent cytotoxicity**ADCC: antibody**ADCC: antibody--dependent cellular cytotoxicitydependent cellular cytotoxicity
TocilizumabTocilizumab
Monoclonal antibody that blocks IL6Monoclonal antibody that blocks IL6
50% response rate in TNF failures50% response rate in TNF failures
Onset 2Onset 2--12 weeks12 weeks
Impressive improvements in CRP, QOL, fatigueImpressive improvements in CRP, QOL, fatigue
Toxicity: Infections, ? GI perforation, lipid, Toxicity: Infections, ? GI perforation, lipid, leukocyte and liver test abnormalities.leukocyte and liver test abnormalities.
ILIL--6 Has Numerous Articular Effects 6 Has Numerous Articular Effects in RAin RA1,21,2
Synoviocytes
Osteoclast activationbone resorption
Endothelial cells
VEGF
Pannus formationPannus formation
Joint destructionJoint destruction
Mediation of chronicMediation of chronicinflammationinflammation
ILIL--66Macrophage
T-cell
B-cell
Neutrophil
AntibodyAntibodyproductionproduction
Adapted from 1 Choy E. Adapted from 1 Choy E. Rheum Dis Clin North AmRheum Dis Clin North Am. 2004;30:405. 2004;30:405––415. 415. 2 Gabay C. 2 Gabay C. Arthritis Res Ther.Arthritis Res Ther. 2006;8(suppl 2):S3.2006;8(suppl 2):S3.
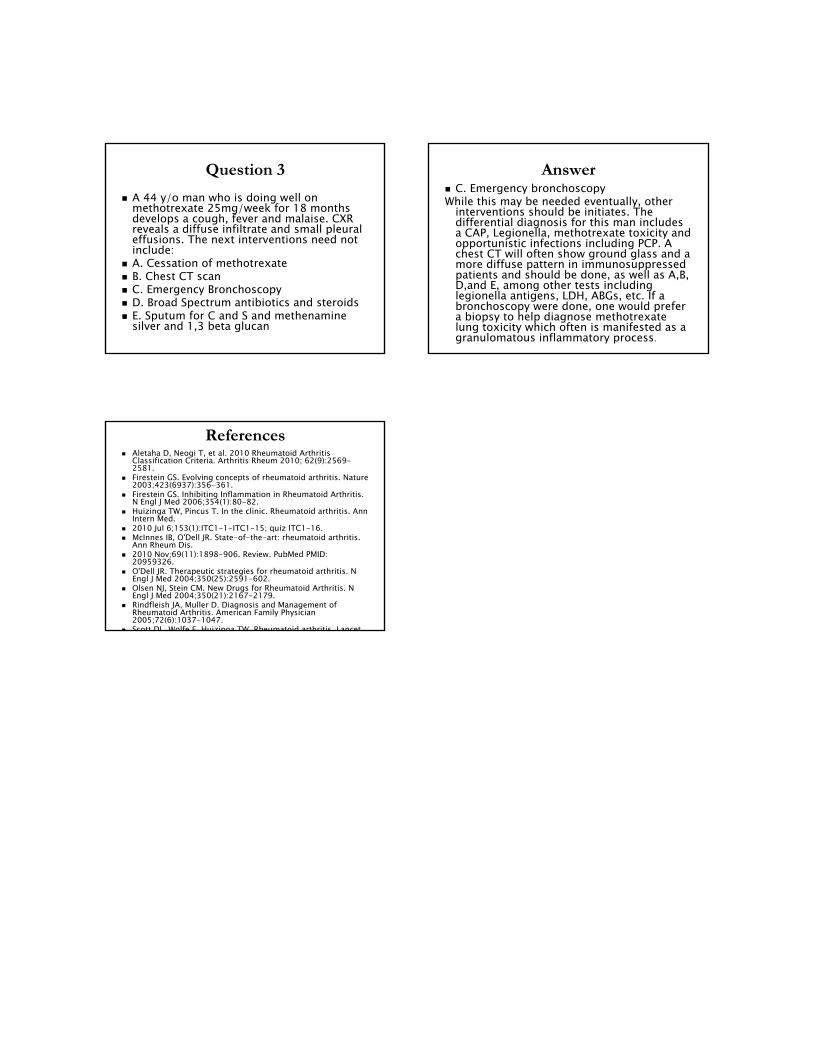
PlaceboPlacebo+ MTX+ MTX(N=158)(N=158)
4 mg/kg4 mg/kg+ MTX+ MTX(N=161)(N=161)
8 mg/kg8 mg/kg+ MTX+ MTX(N=170)(N=170)
****
PlaceboPlacebo+ MTX+ MTX(N=158)(N=158)
4 mg/kg4 mg/kg+ MTX+ MTX(N=161)(N=161)
8 mg/kg8 mg/kg+ MTX+ MTX(N=170)(N=170)
******
PlaceboPlacebo+ MTX+ MTX
(N=158)(N=158)
4 mg/kg4 mg/kg+ MTX+ MTX
(N=161)(N=161)
8 mg/kg8 mg/kg+ MTX+ MTX
(N=170)(N=170)
******
******
AntiAnti--TNF, ACR70 Response Rates at Week 24TNF, ACR70 Response Rates at Week 24Inadequate RespondersInadequate Responders: : ACR20, ACR50 ACR20, ACR50 ITT PopulationITT Population
** p<0.01 *** p<0.0001, TCZ vs. Placebo + MTX** p<0.01 *** p<0.0001, TCZ vs. Placebo + MTX
10%4%
1%
30%
17%
5%
50%
29%
12%
0%
10%
20%
30%
40%
50%
60%
WA18062WA18062
Percentage (%)Percentage (%)RespondersResponders ACR20ACR20 ACR50ACR50 ACR70ACR70

Newer Drugs in DevelopmentNewer Drugs in Development
Newer B cell and anti TNF agentsNewer B cell and anti TNF agents p38MAP kinase inhibitorsp38MAP kinase inhibitors Janus Kinase 3 inhibitorsJanus Kinase 3 inhibitors--tofacitinibtofacitinib--
FDA advisory board approvalFDA advisory board approval Spleen tyrosine kinase inhibitorsSpleen tyrosine kinase inhibitors CCR1 antagonistsCCR1 antagonists Gene therapyGene therapy
ConclusionConclusionA new era in the treatment of rheumatoid A new era in the treatment of rheumatoid
arthritisarthritis
•• Proof of principle has been established that Proof of principle has been established that selective targeting of pathogenic elements is selective targeting of pathogenic elements is therapeutically effective. therapeutically effective.
•• Early therapyEarly therapy--especially combination therapy especially combination therapy tied to improved outcomes.tied to improved outcomes.
•• The future is now! Less joint replacements and The future is now! Less joint replacements and improved morbidity and mortality now improved morbidity and mortality now evident.evident.
•• A plea. Refer to confirm diagnosis and initiate A plea. Refer to confirm diagnosis and initiate treatmenttreatment
Question 1Question 1
1. A 581. A 58--yearyear--old male patient presents with old male patient presents with polyarticular pain that has lasted for 6 weeks. He polyarticular pain that has lasted for 6 weeks. He has had fevers and weight loss, and has a history of has had fevers and weight loss, and has a history of traveling to the Cape and Vineyard. He has morning traveling to the Cape and Vineyard. He has morning stiffness, shoulder, hip and MCP pain on exam. stiffness, shoulder, hip and MCP pain on exam. After the usual complete history and physical After the usual complete history and physical performed that reveals a small knee effusion as performed that reveals a small knee effusion as well as above. The work need not include (not well as above. The work need not include (not maymay——we are cutting the CMS budget):we are cutting the CMS budget):
A. CXR and hand and feet filmsA. CXR and hand and feet films B. Lyme titer and ANA B. Lyme titer and ANA C. Rheumatoid factor and anti CCPC. Rheumatoid factor and anti CCP D. A diagnostic tap of the kneeD. A diagnostic tap of the knee E. ESR and CRPE. ESR and CRP
AnswerAnswer
A is correctA is correct The tap of the knee will establish whether this is The tap of the knee will establish whether this is
an inflammatory disease or not and is the single an inflammatory disease or not and is the single most important test outlined. Whether the patient most important test outlined. Whether the patient is seropositive or not, and/ or has elevated is seropositive or not, and/ or has elevated inflammatory markers is key to guiding future inflammatory markers is key to guiding future therapeutics. While it is not wrong to obtain a CXR therapeutics. While it is not wrong to obtain a CXR (and in fact may be done when deciding drug (and in fact may be done when deciding drug therapy) it is not essential at this time. Hand and therapy) it is not essential at this time. Hand and feet films are unlikely to reveal anything significant feet films are unlikely to reveal anything significant after only 6 weeks of symptoms. A lyme titer and is after only 6 weeks of symptoms. A lyme titer and is reasonable to obtain due to his travel in an reasonable to obtain due to his travel in an endemic area; the ANA is really gratuitous and endemic area; the ANA is really gratuitous and would not offer any diagnostic help, but I thought would not offer any diagnostic help, but I thought you should think about its role in the differential you should think about its role in the differential diagnosis of this patient.diagnosis of this patient.
Question 2Question 2
2. A 482. A 48--yearyear--old man presents with rheumatoid old man presents with rheumatoid arthritis. He is deciding what DMARDs to take. He arthritis. He is deciding what DMARDs to take. He has erosive disease, and has a history of travel to has erosive disease, and has a history of travel to Russia and Peru, and has a vague sulfa allergy. His Russia and Peru, and has a vague sulfa allergy. His labs are unremarkable, except for a creatinine of labs are unremarkable, except for a creatinine of 1.7 and an AST of 38. 1.7 and an AST of 38.
A. What further tests or interventions need not be A. What further tests or interventions need not be done?done?
Tests: Tests: a. CXRa. CXR b. PPDb. PPD c. Pneumovaxc. Pneumovax d. HCV and HBSAg and HBcAgd. HCV and HBSAg and HBcAg e. ACE level and SPEPe. ACE level and SPEP
AnswerAnswer
E is correctE is correct A, B, and C must be done prior to any A, B, and C must be done prior to any
immunosuppressive treatment in this patient. A immunosuppressive treatment in this patient. A CXR is not mandatory in many instances, but in this CXR is not mandatory in many instances, but in this man, with possible exposure to Tb, and with the man, with possible exposure to Tb, and with the additional consideration of adding methotrexate or additional consideration of adding methotrexate or an antian anti--TNF, it is imperative. Due to his travel TNF, it is imperative. Due to his travel history a PPD is imperative and hepatitis serologies history a PPD is imperative and hepatitis serologies are needed due to the abnormal liver blood tests, are needed due to the abnormal liver blood tests, as one may consider methotrexate or rituximab as one may consider methotrexate or rituximab (both associated with Hepatitis B reactivation (both associated with Hepatitis B reactivation syndromes). An ACE level is almost never helpful syndromes). An ACE level is almost never helpful for any reason and an SPEP, while always for any reason and an SPEP, while always interesting, is not needed at this juncture.interesting, is not needed at this juncture.
Question 3Question 3
A 44 y/o man who is doing well on A 44 y/o man who is doing well on methotrexate 25mg/week for 18 months methotrexate 25mg/week for 18 months develops a cough, fever and malaise. CXR develops a cough, fever and malaise. CXR reveals a diffuse infiltrate and small pleural reveals a diffuse infiltrate and small pleural effusions. The next interventions need not effusions. The next interventions need not include:include:
A. Cessation of methotrexateA. Cessation of methotrexate B. Chest CT scanB. Chest CT scan C. Emergency BronchoscopyC. Emergency Bronchoscopy D. Broad Spectrum antibiotics and steroidsD. Broad Spectrum antibiotics and steroids E. Sputum for C and S and methenamine E. Sputum for C and S and methenamine
silver and 1,3 beta glucansilver and 1,3 beta glucan
AnswerAnswer C. Emergency bronchoscopyC. Emergency bronchoscopyWhile this may be needed eventually, other While this may be needed eventually, other
interventions should be initiates. The interventions should be initiates. The differential diagnosis for this man includes differential diagnosis for this man includes a CAP, Legionella, methotrexate toxicity and a CAP, Legionella, methotrexate toxicity and opportunistic infections including PCP. A opportunistic infections including PCP. A chest CT will often show ground glass and a chest CT will often show ground glass and a more diffuse pattern in immunosuppressed more diffuse pattern in immunosuppressed patients and should be done, as well as A,B, patients and should be done, as well as A,B, D,and E, among other tests including D,and E, among other tests including legionella antigens, LDH, ABGs, etc. If a legionella antigens, LDH, ABGs, etc. If a bronchoscopy were done, one would prefer bronchoscopy were done, one would prefer a biopsy to help diagnose methotrexate a biopsy to help diagnose methotrexate lung toxicity which often is manifested as a lung toxicity which often is manifested as a granulomatous inflammatory processgranulomatous inflammatory process. .
ReferencesReferences Aletaha D, Neogi T, et al. 2010 Rheumatoid Arthritis Aletaha D, Neogi T, et al. 2010 Rheumatoid Arthritis
Classification Criteria. Arthritis Rheum 2010; 62(9):2569Classification Criteria. Arthritis Rheum 2010; 62(9):2569--2581.2581.
Firestein GS. Evolving concepts of rheumatoid arthritis. Nature Firestein GS. Evolving concepts of rheumatoid arthritis. Nature 2003;423(6937):3562003;423(6937):356--361.361.
Firestein GS. Inhibiting Inflammation in Rheumatoid Arthritis. Firestein GS. Inhibiting Inflammation in Rheumatoid Arthritis. N Engl J Med 2006;354(1):80N Engl J Med 2006;354(1):80--82.82.
Huizinga TW, Pincus T. In the clinic. Rheumatoid arthritis. Ann Huizinga TW, Pincus T. In the clinic. Rheumatoid arthritis. Ann Intern Med.Intern Med.
2010 Jul 6;153(1):ITC12010 Jul 6;153(1):ITC1--11--ITC1ITC1--15; quiz ITC115; quiz ITC1--16.16. McInnes IB, O'Dell JR. StateMcInnes IB, O'Dell JR. State--ofof--thethe--art: rheumatoid arthritis. art: rheumatoid arthritis.
Ann Rheum Dis. Ann Rheum Dis. 2010 Nov;69(11):18982010 Nov;69(11):1898--906. Review. PubMed PMID: 906. Review. PubMed PMID:
20959326.20959326. O'Dell JR. Therapeutic strategies for rheumatoid arthritis. N O'Dell JR. Therapeutic strategies for rheumatoid arthritis. N
Engl J Med 2004;350(25):2591Engl J Med 2004;350(25):2591--602.602. Olsen NJ, Stein CM. New Drugs for Rheumatoid Arthritis. N Olsen NJ, Stein CM. New Drugs for Rheumatoid Arthritis. N
Engl J Med 2004;350(21):2167Engl J Med 2004;350(21):2167--2179.2179. Rindfleish JA, Muller D. Diagnosis and Management of Rindfleish JA, Muller D. Diagnosis and Management of
Rheumatoid Arthritis. American Family Physician Rheumatoid Arthritis. American Family Physician 2005;72(6):10372005;72(6):1037--1047.1047.
Scott DL, Wolfe F, Huizinga TW. Rheumatoid arthritis. Lancet.Scott DL, Wolfe F, Huizinga TW. Rheumatoid arthritis. Lancet.










