Embed Size (px)
Citation preview
7/27/2019 Rheumatoid Arth
http://slidepdf.com/reader/full/rheumatoid-arth 1/33
Rheumatoid arthritis
From Wikipedia, the free encyclopedia
Rheumatoid arthritis
Classification and external resources
Rheumatoid Arthritis.JPG
A hand affected by rheumatoid arthritis
C!"#$ %$&"%$'
C!"( )#*
+%% #$-$$
!iseases! ##&$'
%edlinePlus $$$*-#
e%edicine article/--#)#& article/#0''#(& article/-$&*#) article/*$#0)#
article/--&#' article/$*#(
%e12 !$$##)0
Rheumatoid arthritis 3RA4 is an autoimmune disease that results in a chronic, systemic
inflammatory disorder that may affect many tissues and or5ans, but principally attacks
flexible 3syno6ial4 7oints. t can be a disablin5 and painful condition, 8hich can lead to
substantial loss of functionin5 and mobility if not ade9uately treated.
:he process in6ol6es an inflammatory response of the capsule around the 7oints
3syno6ium4 secondary to s8ellin5 3tur5escence4 of syno6ial cells, excess syno6ial fluid,
and the de6elopment of fibrous tissue 3pannus4 in the syno6ium. :he patholo5y of the
disease process often leads to the destruction of articular cartila5e and ankylosis
3fusion4 of the 7oints. RA can also produce diffuse inflammation in the lun5s, themembrane around the heart 3pericardium4, the membranes of the lun5 3pleura4, and
8hite of the eye 3sclera4, and also nodular lesions, most common in subcutaneous
tissue. Althou5h the cause of RA is unkno8n, autoimmunity plays a bi5 part, and RA is a
systemic autoimmune disease. t is a clinical dia5nosis made on the basis of symptoms,
physical exam, radio5raphs 3;"rays4 and labs.<#=
7/27/2019 Rheumatoid Arth
http://slidepdf.com/reader/full/rheumatoid-arth 2/33
:reatments are pharmacolo5ical and non"pharmacolo5ical. >on"pharmacolo5ical
treatment includes physical therapy, orthoses, occupational therapy and nutritional
therapy but these don?t stop the pro5ression of 7oint destruction. Anal5esics 3painkillers4
and anti"inflammatory dru5s, includin5 steroids, suppress symptoms, but don?t stop the
pro5ression of 7oint destruction either. !isease"modifyin5 antirheumatic dru5s
3!%AR!s4 slo8 or halt the pro5ress of the disease. :he ne8er biolo5ics are !%AR!s.<#= :he e6idence for complementary and alternati6e medicine 3CA%4 treatments for RA
related pain is 8eak,<0= 8ith the lack of hi5h 9uality e6idence leadin5 to the conclusions
that their use is currently not supported by the e6idence.<-= Patients should inform their
health care pro6ider of any CA% treatments and continue takin5 traditional treatments.
<*=
About $.'@ of the nited 1tates adult population has RA, 8omen t8o to three times as
often as men.<&= +nset is most fre9uent durin5 middle a5e, but people of any a5e can be
affected.<'=
:he name is based on the term Brheumatic fe6erB, an illness 8hich includes 7oint pain
and is deri6ed from the Greek 8ord DE"rheuma 3nom.4, DEHI"rheumatos 35en.4ῥ ῥ
3Bflo8, currentB4. :he suffix "oid 3Bresemblin5B4 5i6es the translation as 7oint inflammation
that resembles rheumatic fe6er. :he first reco5nied description of RA 8as made in #$$
by !r. Au5ustin Jacob KandrL"eau6ais 3#))0M#*$4 of Paris.<)=
Contents
# 1i5ns and symptoms
#.# Joints
#.0 1kin
#.- Kun5s
#.* Nidneys
#.& 2eart and blood 6essels
#.' +ther
0 Causes
- Pathophysiolo5y
-.# Abnormal immune response
7/27/2019 Rheumatoid Arth
http://slidepdf.com/reader/full/rheumatoid-arth 3/33
* !ia5nosis
*.# ma5in5
*.0 lood tests
*.- Criteria
*.* !ifferential dia5noses
*.& %onitorin5 pro5ression
& %ana5ement
&.# Kifestyle
&.0 !isease modifyin5 a5ents
&.- Anti"inflammatory a5ents
&.* 1ur5ery
&.& Alternati6e medicine
' Pre6ention
) Pro5nosis
).# Pro5nostic factors
).0 %ortality
Opidemiolo5y
( 2istory
#$ References
## Oxternal links
1i5ns and symptoms
RA primarily affects 7oints, ho8e6er it also affects other or5ans in #&M0&@ of indi6iduals.
<= t can be difficult to determine 8hether disease manifestations are directly caused by
the rheumatoid process itself, or from side effects of the medications used to treat it M for
example, lun5 fibrosis from methotrexate or osteoporosis from corticosteroids.
Joints

7/27/2019 Rheumatoid Arth
http://slidepdf.com/reader/full/rheumatoid-arth 4/33
A dia5ram sho8in5 ho8 rheumatoid arthritis affects a 7oint
Arthritis of 7oints in6ol6es inflammation of the syno6ial membrane. Joints become
s8ollen, tender and 8arm, and stiffness limits their mo6ement. With time, multiple 7oints
are affected 3it is a polyarthritis4. %ost commonly in6ol6ed are the small 7oints of the
hands, feet and cer6ical spine, but lar5er 7oints like the shoulder and knee can also be
in6ol6ed.<(= #$( 1yno6itis can lead to tetherin5 of tissue 8ith loss of mo6ement and
erosion of the 7oint surface causin5 deformity and loss of function.<#=
RA typically manifests 8ith si5ns of inflammation, 8ith the affected 7oints bein5 s8ollen,
8arm, painful and stiff, particularly early in the mornin5 on 8akin5 or follo8in5 prolon5ed
inacti6ity. ncreased stiffness early in the mornin5 is often a prominent feature of the
disease and typically lasts for more than an hour. Gentle mo6ements may relie6e
symptoms in early sta5es of the disease. :hese si5ns help distin5uish rheumatoid fromnon"inflammatory problems of the 7oints, often referred to as osteoarthritis or B8ear"and"
tearB arthritis. n arthritis of non"inflammatory causes, si5ns of inflammation and early
mornin5 stiffness are less prominent 8ith stiffness typically less than # hour, and
mo6ements induce pain caused by mechanical arthritis.<#$= :he pain associated 8ith RA
is induced at the site of inflammation and classified as nocicepti6e as opposed to
neuropathic.<##= :he 7oints are often affected in a fairly symmetrical fashion, althou5h
this is not specific, and the initial presentation may be asymmetrical.<(= #$(
As the patholo5y pro5resses the inflammatory acti6ity leads to tendon tetherin5 anderosion and destruction of the 7oint surface, 8hich impairs ran5e of mo6ement and leads
to deformity. :he fin5ers may suffer from almost any deformity dependin5 on 8hich 7oints
are most in6ol6ed. 1pecific deformities, 8hich also occur in osteoarthritis, include ulnar
de6iation, boutonniere deformity, s8an neck deformity and BQ"thumb.B BQ"thumbB or BQ"
deformityB consists of hyperextension of the interphalan5eal 7oint, fixed flexion and
subluxation of the metacarpophalan5eal 7oint and 5i6es a BQB appearance to the thumb.
<(= #$( :he hammer toe deformity may be seen. n the 8orst case, 7oints are kno8n as
arthritis mutilans due to the mutilatin5 nature of the deformities.<citation needed=
1kin
:he rheumatoid nodule, 8hich is sometimes cutaneous, is the feature most
characteristic of RA. t is a type of inflammatory reaction kno8n to patholo5ists as a
Bnecrotiin5 5ranulomaB. :he initial patholo5ic process in nodule formation is unkno8n
but may be essentially the same as the syno6itis, since similar structural features occur
in both. :he nodule has a central area of fibrinoid necrosis that may be fissured and
7/27/2019 Rheumatoid Arth
http://slidepdf.com/reader/full/rheumatoid-arth 5/33
8hich corresponds to the fibrin"rich necrotic material found in and around an affected
syno6ial space. 1urroundin5 the necrosis is a layer of palisadin5 macropha5es and
fibroblasts, correspondin5 to the intimal layer in syno6ium and a cuff of connecti6e tissue
containin5 clusters of lymphocytes and plasma cells, correspondin5 to the subintimal
one in syno6itis. :he typical rheumatoid nodule may be a fe8 millimetres to a fe8
centimetres in diameter and is usually found o6er bony prominences, such as theolecranon, the calcaneal tuberosity, the metacarpophalan5eal 7oint, or other areas that
sustain repeated mechanical stress. >odules are associated 8ith a positi6e RF
3rheumatoid factor4 titer and se6ere erosi6e arthritis. Rarely, these can occur in internal
or5ans or at di6erse sites on the body.
1e6eral forms of 6asculitis occur in RA. A beni5n form occurs as microinfarcts around
the nailfolds. %ore se6ere forms include li6edo reticularis, 8hich is a net8ork 3reticulum4
of erythematous to purplish discoloration of the skin caused by the presence of an
obliterati6e cutaneous capillaropathy.
+ther, rather rare, skin associated symptoms include pyoderma 5an5renosum, 18eet?s
syndrome, dru5 reactions, erythema nodosum, lobe panniculitis, atrophy of fin5er skin,
palmar erythema, diffuse thinnin5 3rice paper skin4, and skin fra5ility 3often 8orsened by
corticosteroid use4.
Kun5s
Fibrosis of the lun5s is a reco5nied response to rheumatoid disease. t is also a rare but
8ell reco5nied conse9uence of therapy 3for example 8ith methotrexate and
leflunomide4. Caplan?s syndrome describes lun5 nodules in indi6iduals 8ith RA and
additional exposure to coal dust. Pleural effusions are also associated 8ith RA. Another
complication of RA is Rheumatoid Kun5 !isease. t is estimated that about one 9uarter
of Americans 8ith RA de6elop Rheumatoid Kun5 !isease.<#0=
Nidneys
Renal amyloidosis can occur as a conse9uence of chronic inflammation.<#-= RA may
affect the kidney 5lomerulus directly throu5h a 6asculopathy or a mesan5ial infiltrate but
this is less 8ell documented 3thou5h this is not surprisin5, considerin5 immune complex"
mediated hypersensiti6ities are kno8n for patho5enic deposition of immune complexes
in or5ans 8here blood is filtered at hi5h pressure to form other fluids, such as urine and
syno6ial fluid<#*=4. :reatment 8ith Penicillamine and 5old salts are reco5nied causes of
membranous nephropathy.
7/27/2019 Rheumatoid Arth
http://slidepdf.com/reader/full/rheumatoid-arth 6/33
2eart and blood 6essels
People 8ith RA are more prone to atherosclerosis, and risk of myocardial infarction
3heart attack4 and stroke is markedly increased.<#&=<#'= +ther possible complications
that may arise include pericarditis, endocarditis, left 6entricular failure, 6al6ulitis and
fibrosis.<#)= %any people 8ith RA do not experience the same chest pain that others feel
8hen they ha6e an5ina or myocardial infarction. :o reduce cardio6ascular risk, it is
crucial to maintain optimal control of the inflammation caused by RA 38hich may be
in6ol6ed in causin5 the cardio6ascular risk4, and to use exercise and medications
appropriately to reduce other cardio6ascular risk factors such as blood lipids and blood
pressure. !octors 8ho treat RA patients should be sensiti6e to cardio6ascular risk 8hen
prescribin5 anti"inflammatory medications, and may 8ant to consider prescribin5 routine
use of lo8 doses of aspirin if the 5astrointestinal effects are tolerable.<#)=
+ther
+cular
:he eye is directly affected in the form of episcleritis 8hich 8hen se6ere can 6ery
rarely pro5ress to perforatin5 scleromalacia. Rather more common is the indirect effect
of keratocon7uncti6itis sicca, 8hich is a dryness of eyes and mouth caused by
lymphocyte infiltration of lacrimal and sali6ary 5lands. When se6ere, dryness of the
cornea can lead to keratitis and loss of 6ision. Pre6enti6e treatment of se6ere dryness
8ith measures such as nasolacrimal duct blocka5e is important.
2epatic
Cytokine production in 7oints and/or hepatic 3li6er4 Nupffer cells leads to increased
acti6ity of hepatocytes 8ith increased production of acute"phase proteins, such as C"
reacti6e protein, and increased release of enymes such as alkaline phosphatase into
the blood. n Felty?s syndrome, Nupffer cell acti6ation is so marked that the resultin5
increase in hepatocyte acti6ity is associated 8ith nodular hyperplasia of the li6er, 8hich
may be palpably enlar5ed. Althou5h Nupffer cells are 8ithin the hepatic parenchyma,
they are separate from hepatocytes. As a result there is little or no microscopic e6idenceof hepatitis 3immune"mediated destruction of hepatocytes4. 2epatic in6ol6ement in RA is
essentially asymptomatic.
2ematolo5ical
Anemia is by far the most common abnormality of the blood cells 8hich can be
7/27/2019 Rheumatoid Arth
http://slidepdf.com/reader/full/rheumatoid-arth 7/33
caused by a 6ariety of mechanisms. :he chronic inflammation caused by RA leads to
raised hepcidin le6els, leadin5 to anemia of chronic disease 8here iron is poorly
absorbed and also se9uestered into macropha5es. RA may also cause a 8arm
autoimmune hemolytic anemia.<#= :he red cells are of normal sie and colour
3normocytic and normochromic4. A lo8 8hite blood cell count 3neutropenia4 usually only
occurs in patients 8ith Felty?s syndrome 8ith an enlar5ed li6er and spleen. :hemechanism of neutropenia is complex. An increased platelet count 3thrombocytosis4
occurs 8hen inflammation is uncontrolled.
>eurolo5ical
Peripheral neuropathy and mononeuritis multiplex may occur. :he most common
problem is carpal tunnel syndrome caused by compression of the median ner6e by
s8ellin5 around the 8rist. Atlanto"axial subluxation can occur, o8in5 to erosion of the
odontoid process and/or trans6erse li5aments in the cer6ical spine?s connection to the
skull. 1uch an erosion 3-mm4 can 5i6e rise to 6ertebrae slippin5 o6er one another and
compressin5 the spinal cord. Clumsiness is initially experienced, but 8ithout due care
this can pro5ress to 9uadriple5ia.
Constitutional symptoms
Constitutional symptoms includin5 fati5ue, lo8 5rade fe6er, malaise, mornin5 stiffness,
loss of appetite and loss of 8ei5ht are common systemic manifestations seen in patients
8ith acti6e RA.
+steoporosis
Kocal osteoporosis occurs in RA around inflamed 7oints. t is postulated to be partially
caused by inflammatory cytokines. %ore 5eneral osteoporosis is probably contributed to
by immobility, systemic cytokine effects, local cytokine release in bone marro8 and
corticosteroid therapy.
Kymphoma
:he incidence of lymphoma is increased in RA, althou5h it is still uncommon.<#(=<0$=
Causes

7/27/2019 Rheumatoid Arth
http://slidepdf.com/reader/full/rheumatoid-arth 8/33
RA is a form of autoimmunity, the causes of 8hich are still not completely kno8n. t is a
systemic 38hole body4 disorder principally affectin5 syno6ial tissues. :here is no
e6idence that physical and emotional effects or stress could be a tri55er for the disease.
:he many ne5ati6e findin5s su55est that either the tri55er 6aries, or that it mi5ht in factbe a chance e6ent inherent 8ith the immune response<0#=
2alf of the risk for RA is belie6ed to be 5enetic.<00= t is stron5ly associated 8ith the
inherited tissue type ma7or histocompatibility complex 3%2C4 anti5en 2KA"!R* 3most
specifically !R$*$# and $*$*4, and the 5enes P:P>00 and PA!*Shence family
history is an important risk factor.<0-=<0*= nheritin5 the P:P>00 5ene has been sho8n to
double a person?s susceptibility to RA. PA!* has been identified as a ma7or risk factor in
people of Asian descent, but not in those of Ouropean descent.<0&= First"de5ree relati6es
pre6alence rate is 0M-@ and disease 5enetic concordance in monoy5otic t8ins isapproximately #&M0$@.<0'=<0)=
1mokin5 is the most si5nificant non"5enetic risk<00= 8ith RA bein5 up to three times
more common in smokers than non"smokers, particularly in men, hea6y smokers, and
those 8ho are rheumatoid factor positi6e.<0= %odest alcohol consumption may be
protecti6e.<0(=
Opidemiolo5ical studies ha6e confirmed a potential association bet8een RA and t8oherpes6irus infectionsOpstein"arr 6irus 3OT4 and 2uman 2erpes Tirus ' 322T"'4.<-$=
ndi6iduals 8ith RA are more likely to exhibit an abnormal immune response to OT and
ha6e hi5h le6els of anti"OT antibodies.<-#=
Titamin ! deficiency is common in those 8ith RA and may be causally associated.<-0=
1ome trials ha6e found a decreased risk for RA 8ith 6itamin ! supplementation 8hile
others ha6e not.<-0=
Pathophysiolo5y
:he key pieces of e6idence relatin5 to patho5enesis are
A 5enetic link 8ith 2KA"!R* and related allotypes of %2C Class and the : cell"
7/27/2019 Rheumatoid Arth
http://slidepdf.com/reader/full/rheumatoid-arth 9/33
associated protein P:P>00.
An undeniable link to the patho5enesis of 6ascular disease of many types, includin5
the possibility of a stron5 causal connection to rheumatoid 6asculitis, a typical feature of
this condition.<--=
A remarkable deceleration of disease pro5ression in many cases by blockade of thecytokine :>F 3alpha4.
A similar dramatic response in many cases to depletion of lymphocytes, but no
comparable response to depletion of : lymphocytes.
A more or less random pattern of 8hether and 8hen predisposed indi6iduals are
affected.
:he presence of autoantibodies to 5GFc, kno8n as rheumatoid factors 3RF4, and
antibodies to citrullinated peptides 3ACPA4.
:hese data su55est that the disease in6ol6es abnormal cellM: cell interaction, 8ith
presentation of anti5ens by cells to : cells 6ia 2KA"!R elicitin5 : cell help and
conse9uent production of RF and ACPA. nflammation is then dri6en either by cell or :
cell products stimulatin5 release of :>F and other cytokines. :he process may be
facilitated by an effect of smokin5 on citrullination but the stochastic 3random4
epidemiolo5y su55ests that the rate limitin5 step in 5enesis of disease in predisposed
indi6iduals may be an inherent stochastic process 8ithin the immune response such as
immuno5lobulin or : cell receptor 5ene recombination and mutation. 31ee entry under
autoimmunity for 5eneral mechanisms.4
f :>F release is stimulated by cell products in the form of RF or ACPA "containin5
immune complexes, throu5h acti6ation of immuno5lobulin Fc receptors, then RA can be
seen as a form of :ype hypersensiti6ity.<-*=<-&= f :>F release is stimulated by : cell
products such as interleukin"#) it mi5ht be considered closer to type T hypersensiti6ity
althou5h this terminolo5y may be 5ettin5 some8hat dated and unhelpful.<-'= :he debate
on the relati6e roles of immune complexes and : cell products in inflammation in RA has
continued for -$ years. :here is little doubt that both and : cells are essential to the
disease. 2o8e6er, there is 5ood e6idence for neither cell bein5 necessary at the site ofinflammation. :his tends to fa6our immune complexes 3based on antibody synthesised
else8here4 as the initiators, e6en if not the sole perpetuators of inflammation. %oreo6er,
8ork by :hurlin5s and others in Paul"Peter :ak?s 5roup and also by Arthur Na6ana5h?s
5roup su55est that if any immune cells are rele6ant locally they are the plasma cells,
8hich deri6e from cells and produce in bulk the antibodies selected at the cell sta5e.
<citation needed=

7/27/2019 Rheumatoid Arth
http://slidepdf.com/reader/full/rheumatoid-arth 10/33
Althou5h :>F appears to be the dominant, other cytokines 3chemical mediators4 are
likely to be in6ol6ed in inflammation in RA. lockade of :>F does not benefit all patients
or all tissues 3lun5 disease and nodules may 5et 8orse4. lockade of K"#, K"#& and K"'
also ha6e beneficial effects and K"#) may be important. Constitutional symptoms suchas fe6er, malaise, loss of appetite and 8ei5ht loss are also caused by cytokines released
into the blood stream.
As 8ith most autoimmune diseases, it is important to distin5uish bet8een the cause3s4
that tri55er the process, and those that may permit it to persist and pro5ress.
Abnormal immune response
:he factors that allo8 an abnormal immune response, once initiated, to become
permanent and chronic, are becomin5 more clearly understood. :he 5enetic association
8ith 2KA"!R*, as 8ell as the ne8ly disco6ered associations 8ith the 5ene P:P>00 and
8ith t8o additional 5enes,<-)= all implicate altered thresholds in re5ulation of the
adapti6e immune response. t has also become clear from recent studies that these
5enetic factors may interact 8ith the most clearly defined en6ironmental risk factor for
RA, namely ci5arette smokin5<0=<-= +ther en6ironmental factors also appear to
modulate the risk of ac9uirin5 RA, and hormonal factors in the indi6idual may explain
some features of the disease, such as the hi5her occurrence in 8omen, the not"
infre9uent onset after child"birth, and the 3sli5ht4 modulation of disease risk by hormonal
medications. Oxactly ho8 altered re5ulatory thresholds allo8 the tri55erin5 of a specificautoimmune response remains uncertain. 2o8e6er, one possibility is that ne5ati6e
feedback mechanisms that normally maintain tolerance of self are o6ertaken by aberrant
positi6e feedback mechanisms for certain anti5ens such as 5G Fc 3bound by RF4 and
citrullinated fibrino5en 3bound by ACPA4 3see entry on autoimmunity4.
+nce the abnormal immune response has become established 38hich may take se6eral
years before any symptoms occur4, plasma cells deri6ed from lymphocytes produce
rheumatoid factors and ACPA of the 5G and 5% classes in lar5e 9uantities. :hese are
not deposited in the 8ay that they are in systemic lupus. Rather, they acti6atemacropha5es throu5h Fc receptor and complement bindin5, 8hich seems to play an
important role in the intense inflammatory response present in RA.<-(= :his contributes
to inflammation of the syno6ium, in terms of edema, 6asodilation and infiltration by
acti6ated :"cells 3mainly C!* in nodular a55re5ates and C! in diffuse infiltrates4.
1yno6ial macropha5es and dendritic cells further function as anti5en presentin5 cells by
expressin5 %2C class molecules, leadin5 to an established local immune reaction in
7/27/2019 Rheumatoid Arth
http://slidepdf.com/reader/full/rheumatoid-arth 11/33
the tissue. :he disease pro5resses in concert 8ith formation of 5ranulation tissue at the
ed5es of the syno6ial linin5 3pannus4 8ith extensi6e an5io5enesis and production of
enymes that cause tissue dama5e. %odern pharmacolo5ical treatments of RA tar5et
these mediators. +nce the inflammatory reaction is established, the syno6ium thickens,
the cartila5e and the underlyin5 bone be5ins to disinte5rate and e6idence of 7oint
destruction accrues.
!ia5nosis
ma5in5
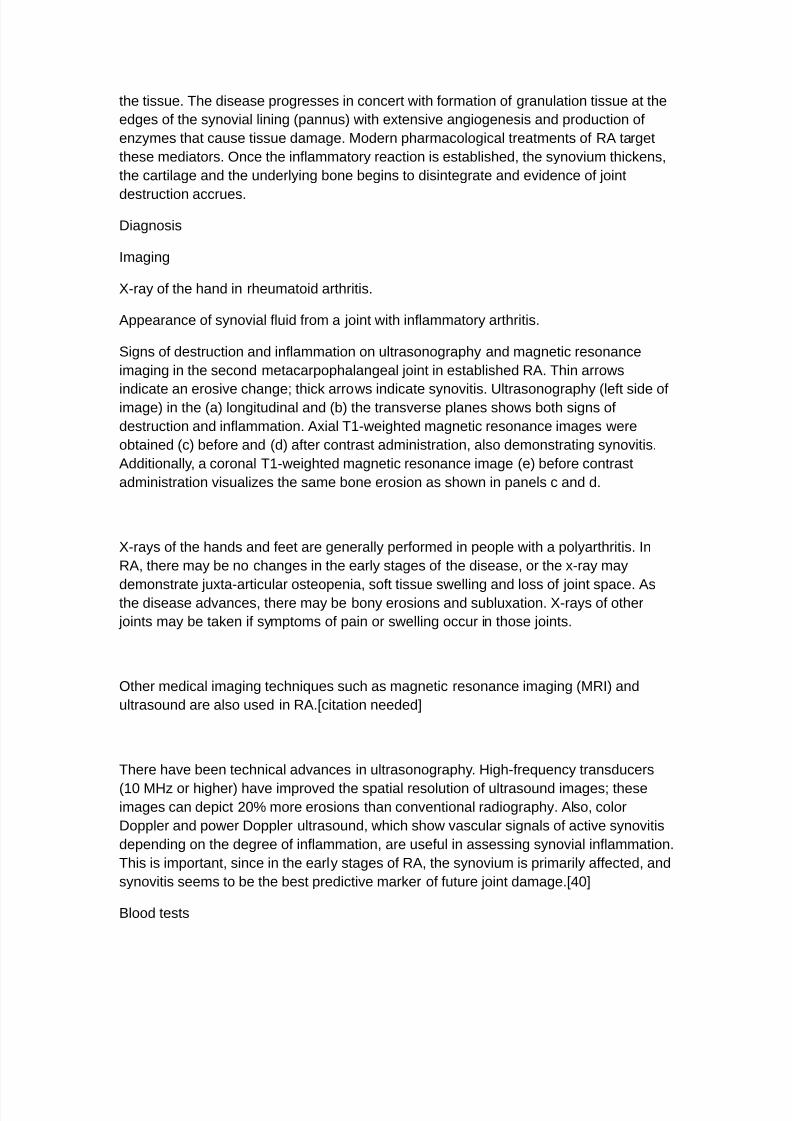
;"ray of the hand in rheumatoid arthritis.
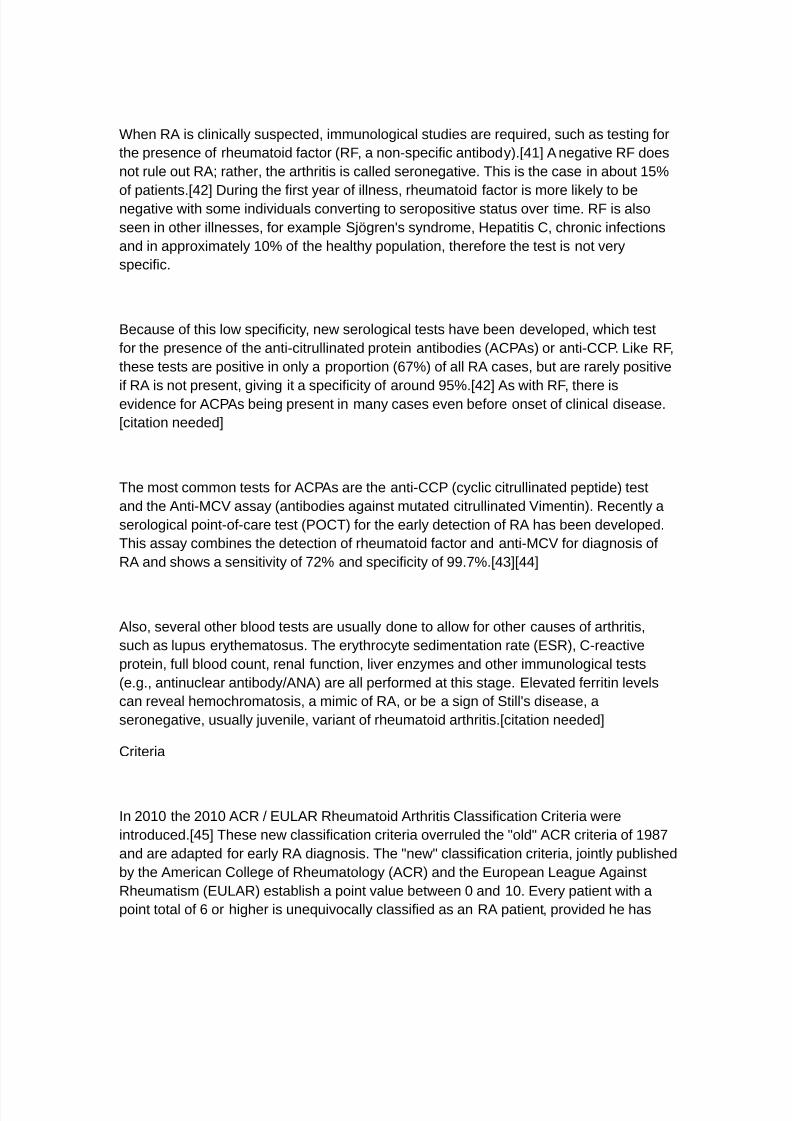
Appearance of syno6ial fluid from a 7oint 8ith inflammatory arthritis.
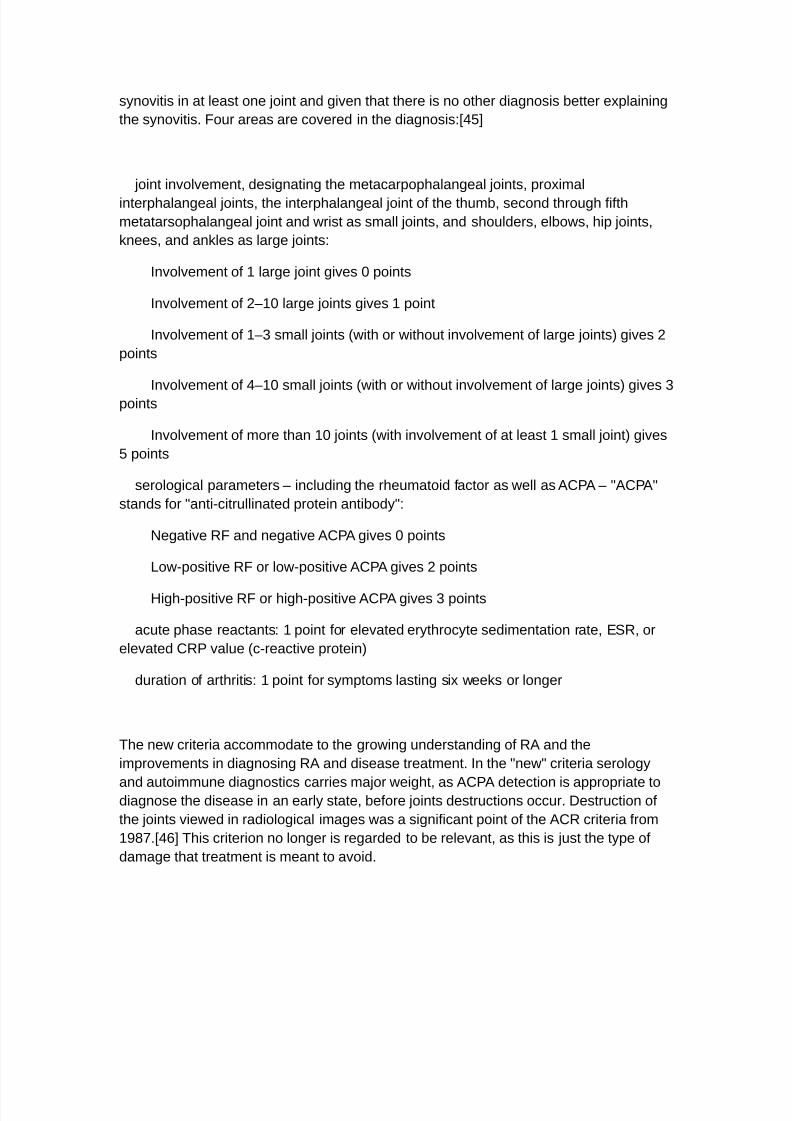
1i5ns of destruction and inflammation on ultrasono5raphy and ma5netic resonance
ima5in5 in the second metacarpophalan5eal 7oint in established RA. :hin arro8s
indicate an erosi6e chan5eU thick arro8s indicate syno6itis. ltrasono5raphy 3left side ofima5e4 in the 3a4 lon5itudinal and 3b4 the trans6erse planes sho8s both si5ns of
destruction and inflammation. Axial :#"8ei5hted ma5netic resonance ima5es 8ere
obtained 3c4 before and 3d4 after contrast administration, also demonstratin5 syno6itis.
Additionally, a coronal :#"8ei5hted ma5netic resonance ima5e 3e4 before contrast
administration 6isualies the same bone erosion as sho8n in panels c and d.
;"rays of the hands and feet are 5enerally performed in people 8ith a polyarthritis. n
RA, there may be no chan5es in the early sta5es of the disease, or the x"ray may
demonstrate 7uxta"articular osteopenia, soft tissue s8ellin5 and loss of 7oint space. Asthe disease ad6ances, there may be bony erosions and subluxation. ;"rays of other
7oints may be taken if symptoms of pain or s8ellin5 occur in those 7oints.
+ther medical ima5in5 techni9ues such as ma5netic resonance ima5in5 3%R4 and
ultrasound are also used in RA.<citation needed=
:here ha6e been technical ad6ances in ultrasono5raphy. 2i5h"fre9uency transducers
3#$ %2 or hi5her4 ha6e impro6ed the spatial resolution of ultrasound ima5esU theseima5es can depict 0$@ more erosions than con6entional radio5raphy. Also, color
!oppler and po8er !oppler ultrasound, 8hich sho8 6ascular si5nals of acti6e syno6itis
dependin5 on the de5ree of inflammation, are useful in assessin5 syno6ial inflammation.
:his is important, since in the early sta5es of RA, the syno6ium is primarily affected, and
syno6itis seems to be the best predicti6e marker of future 7oint dama5e.<*$=
lood tests
7/27/2019 Rheumatoid Arth
http://slidepdf.com/reader/full/rheumatoid-arth 12/33
When RA is clinically suspected, immunolo5ical studies are re9uired, such as testin5 for
the presence of rheumatoid factor 3RF, a non"specific antibody4.<*#= A ne5ati6e RF does
not rule out RAU rather, the arthritis is called serone5ati6e. :his is the case in about #&@
of patients.<*0= !urin5 the first year of illness, rheumatoid factor is more likely to bene5ati6e 8ith some indi6iduals con6ertin5 to seropositi6e status o6er time. RF is also
seen in other illnesses, for example 17V5ren?s syndrome, 2epatitis C, chronic infections
and in approximately #$@ of the healthy population, therefore the test is not 6ery
specific.
ecause of this lo8 specificity, ne8 serolo5ical tests ha6e been de6eloped, 8hich test
for the presence of the anti"citrullinated protein antibodies 3ACPAs4 or anti"CCP. Kike RF,
these tests are positi6e in only a proportion 3')@4 of all RA cases, but are rarely positi6e
if RA is not present, 5i6in5 it a specificity of around (&@.<*0= As 8ith RF, there ise6idence for ACPAs bein5 present in many cases e6en before onset of clinical disease.
<citation needed=
:he most common tests for ACPAs are the anti"CCP 3cyclic citrullinated peptide4 test
and the Anti"%CT assay 3antibodies a5ainst mutated citrullinated Timentin4. Recently a
serolo5ical point"of"care test 3P+C:4 for the early detection of RA has been de6eloped.
:his assay combines the detection of rheumatoid factor and anti"%CT for dia5nosis of
RA and sho8s a sensiti6ity of )0@ and specificity of ((.)@.<*-=<**=
Also, se6eral other blood tests are usually done to allo8 for other causes of arthritis,
such as lupus erythematosus. :he erythrocyte sedimentation rate 3O1R4, C"reacti6e
protein, full blood count, renal function, li6er enymes and other immunolo5ical tests
3e.5., antinuclear antibody/A>A4 are all performed at this sta5e. Ole6ated ferritin le6els
can re6eal hemochromatosis, a mimic of RA, or be a si5n of 1till?s disease, a
serone5ati6e, usually 7u6enile, 6ariant of rheumatoid arthritis.<citation needed=
Criteria
n 0$#$ the 0$#$ ACR / OKAR Rheumatoid Arthritis Classification Criteria 8ere
introduced.<*&= :hese ne8 classification criteria o6erruled the BoldB ACR criteria of #()
and are adapted for early RA dia5nosis. :he Bne8B classification criteria, 7ointly published
by the American Colle5e of Rheumatolo5y 3ACR4 and the Ouropean Kea5ue A5ainst
Rheumatism 3OKAR4 establish a point 6alue bet8een $ and #$. O6ery patient 8ith a
point total of ' or hi5her is une9ui6ocally classified as an RA patient, pro6ided he has
7/27/2019 Rheumatoid Arth
http://slidepdf.com/reader/full/rheumatoid-arth 13/33
syno6itis in at least one 7oint and 5i6en that there is no other dia5nosis better explainin5
the syno6itis. Four areas are co6ered in the dia5nosis<*&=
7oint in6ol6ement, desi5natin5 the metacarpophalan5eal 7oints, proximal
interphalan5eal 7oints, the interphalan5eal 7oint of the thumb, second throu5h fifth
metatarsophalan5eal 7oint and 8rist as small 7oints, and shoulders, elbo8s, hip 7oints,
knees, and ankles as lar5e 7oints
n6ol6ement of # lar5e 7oint 5i6es $ points
n6ol6ement of 0M#$ lar5e 7oints 5i6es # point
n6ol6ement of #M- small 7oints 38ith or 8ithout in6ol6ement of lar5e 7oints4 5i6es 0
points
n6ol6ement of *M#$ small 7oints 38ith or 8ithout in6ol6ement of lar5e 7oints4 5i6es -
points
n6ol6ement of more than #$ 7oints 38ith in6ol6ement of at least # small 7oint4 5i6es
& points
serolo5ical parameters M includin5 the rheumatoid factor as 8ell as ACPA M BACPAB
stands for Banti"citrullinated protein antibodyB
>e5ati6e RF and ne5ati6e ACPA 5i6es $ points
Ko8"positi6e RF or lo8"positi6e ACPA 5i6es 0 points
2i5h"positi6e RF or hi5h"positi6e ACPA 5i6es - points
acute phase reactants # point for ele6ated erythrocyte sedimentation rate, O1R, or
ele6ated CRP 6alue 3c"reacti6e protein4
duration of arthritis # point for symptoms lastin5 six 8eeks or lon5er
:he ne8 criteria accommodate to the 5ro8in5 understandin5 of RA and the
impro6ements in dia5nosin5 RA and disease treatment. n the Bne8B criteria serolo5y
and autoimmune dia5nostics carries ma7or 8ei5ht, as ACPA detection is appropriate todia5nose the disease in an early state, before 7oints destructions occur. !estruction of
the 7oints 6ie8ed in radiolo5ical ima5es 8as a si5nificant point of the ACR criteria from
#().<*'= :his criterion no lon5er is re5arded to be rele6ant, as this is 7ust the type of
dama5e that treatment is meant to a6oid.
7/27/2019 Rheumatoid Arth
http://slidepdf.com/reader/full/rheumatoid-arth 14/33
:he criteria are not intended for the dia5nosis for routine clinical careU they 8ere
primarily intended to cate5orie research 3classification criteria4. n clinical practice, the
follo8in5 criteria apply<citation needed=
t8o or more s8ollen 7oints
mornin5 stiffness lastin5 more than one hour for at least six 8eeks
the detection of rheumatoid factors or autoantibodies a5ainst ACPA such as
autoantibodies to mutated citrullinated 6imentin can confirm the suspicion of RA. A
ne5ati6e autoantibody result does not exclude a dia5nosis of RA.
!ifferential dia5noses
1e6eral other medical conditions can resemble RA, and usually need to be distin5uished
from it at the time of dia5nosis<*)=<*=
Crystal induced arthritis 35out, and pseudo5out4 M usually in6ol6es particular 7oints
3knee, %:P#, heels4 and can be distin5uished 8ith aspiration of 7oint fluid if in doubt.
Redness, asymmetric distribution of affected 7oints, pain occurs at ni5ht and the startin5
pain is less than an hour 8ith 5out.
+steoarthritis M distin5uished 8ith ;"rays of the affected 7oints and blood tests, a5e
3mostly older patients4, startin5 pain less than an hour, a"symmetric distribution of
affected 7oints and pain 8orsens 8hen usin5 7oint for lon5er periods.
1ystemic lupus erythematosus 31KO4 M distin5uished by specific clinical symptoms
and blood tests 3antibodies a5ainst double"stranded !>A4
+ne of the se6eral types of psoriatic arthritis resembles RA M nail chan5es and skin
symptoms distin5uish bet8een them
Kyme disease causes erosi6e arthritis and may closely resemble RA M it may be
distin5uished by blood test in endemic areas
Reacti6e arthritis 3pre6iously Reiter?s disease4 M asymmetrically in6ol6es heel,
sacroiliac 7oints, and lar5e 7oints of the le5. t is usually associated 8ith urethritis,
con7uncti6itis, iritis, painless buccal ulcers, and keratoderma blennorrha5ica.
Ankylosin5 spondylitis M this in6ol6es the spine, althou5h a RA"like symmetrical small"
7oint polyarthritis may occur in the context of this condition.
7/27/2019 Rheumatoid Arth
http://slidepdf.com/reader/full/rheumatoid-arth 15/33
2epatitis C M RA"like symmetrical small"7oint polyarthritis may occur in the context of
this condition. 2epatitis C may also induce Rheumatoid Factor auto"antibodies
Rarer causes that usually beha6e differently but may cause 7oint pains<*)=
1arcoidosis, amyloidosis, and Whipple?s disease can also resemble RA.
2emochromatosis may cause hand 7oint arthritis.
Acute rheumatic fe6er can be differentiated from RA by a mi5ratory pattern of 7oint
in6ol6ement and e6idence of antecedent streptococcal infection. acterial arthritis 3such
as streptococcus4 is usually asymmetric, 8hile RA usually in6ol6es both sides of the
body symmetrically.
Gonococcal arthritis 3another bacterial arthritis4 is also initially mi5ratory and can
in6ol6e tendons around the 8rists and ankles.
%onitorin5 pro5ression
:he pro5ression of RA can be follo8ed usin5 scores such as !isease Acti6ity 1core of
0 7oints 3!A104. t is 8idely used as an indicator of RA disease acti6ity and response
to treatment, but is not al8ays a reliable indicator of treatment effect.<*(= :he 7ointsincluded in !A10 are 3bilaterally4 proximal interphalan5eal 7oints 3#$ 7oints4,
metacarpophalan5eal 7oints 3#$4, 8rists 304, elbo8s 304, shoulders 304 and knees 304.
When lookin5 at these 7oints, both the number of 7oints 8ith tenderness upon touchin5
3:O>04 and s8ellin5 31W04 are counted. n addition, the erythrocyte sedimentation
rate 3O1R4 is measured. Also, the patient makes a sub7ecti6e assessment 31A4 of
disease acti6ity durin5 the precedin5 ) days on a scale bet8een $ and #$$, 8here $ is
Bno acti6ityB and #$$ is Bhi5hest acti6ity possibleB. With these parameters, !A10 is
calculated as<&$= !A10$.&'Xtimes YXs9rt Y:O>0ZZ[$.0Xtimes YXs9rt Y1W0ZZ
[$.)$Xtimes Xln3O1R4[$.$#*Xtimes 1A
From this, the disease acti6ity of the patient can be classified as follo8s<&$=
Current
!A10 !A10 decrease from initial 6alue
#.0 $.' but \ #.0 \ $.'
7/27/2019 Rheumatoid Arth
http://slidepdf.com/reader/full/rheumatoid-arth 16/33
\ -.0 nacti6e Good impro6ement %oderate impro6ement >o
impro6ement
-.0 but \ &.# %oderate %oderate impro6ement %oderate
impro6ement >o impro6ement
&.# Tery acti6e %oderate impro6ement >o impro6ement >oimpro6ement
%ana5ement
:here is no cure for RA, but treatments can impro6e symptoms and slo8 the pro5ress of
the disease. !isease"modifyin5 treatment has the best results 8hen it is started early
and a55ressi6ely.<&#=
:he 5oals of treatment are to minimie symptoms such as pain and s8ellin5, to pre6ent
bone deformity 3for example, bone erosions 6isible in ;"rays4, and to maintain day"to"
day functionin5.<&0= :his can often be achie6ed usin5 t8o main classes of medications
anal5esics such as >1A!s, and disease"modifyin5 antirheumatic dru5s 3!%AR!s4.<&-=
RA should 5enerally be treated 8ith at least one specific anti"rheumatic medication.<&#=
:he use of benodiaepines 3such as diaepam4 to treat the pain is not recommended
as it does not appear to help and is associated 8ith risks.<&*= Anal5esics, other than
>1A!s, offer lesser, but some benefit 8ith respect to pain.<00= 8hilst not causin5 the
same le6el of 5astrointestinal irritation.
Kifestyle
Re5ular exercise is recommended as both safe and useful to maintain muscles stren5th
and o6erall physical function.<&&= t is uncertain if specific dietary measures ha6e an
effect.<&'=
!isease modifyin5 a5ents
!isease"modifyin5 antirheumatic dru5s 3!%AR!4 are the primary treatment for RA.<00=
:hey are a di6erse collection of dru5s, 5rouped by use and con6ention. :hey ha6e been
found to impro6e symptoms, decrease 7oint dama5e, and impro6e o6erall functional
abilities.<00= :hey should be started 6ery early in the disease as 8hen they result in
disease remission in approximately half of people and impro6ed outcomes o6erall.<&)=
7/27/2019 Rheumatoid Arth
http://slidepdf.com/reader/full/rheumatoid-arth 17/33
:he most commonly used a5ent is methotrexate 8ith other fre9uently used a5ents
includin5 sulfasalaine and leflunomide. 1odium aurothiomalate 3Gold4 and cyclosporin
are less commonly used due to more common ad6erse effects. A5ents may be used in
combinations.<00=
%ethotrexate is the most important and useful !%AR! and is usually the first treatment.
<&0=<&-=<&= Ad6erse effects should be monitored re5ularly 8ith toxicity includin5
5astrointestinal, hematolo5ic, pulmonary, and hepatic.<&= 1ide effects such as nausea,
6omitin5 or abdominal pain can be reduced by takin5 folic acid.<&(= :he most common
undesirable affect is that it increases li6er enymes in almost #&@ of people.<&= t is
thus recommended that those 8ho consistently demonstrate abnormal le6els of li6er
enymes or ha6e a history of li6er disease or alcohol use under5o li6er biopsies.<'$=
%ethotrexate is also considered a terato5enic and as such, it is recommended 8omen of
childbearin5 a5e should use contracepti6es to a6oid pre5nancy and to discontinue its
use if pre5nancy is planned.<&0=<&=
iolo5ical a5ents should 5enerally only be used if methotrexate and other con6entional
a5ents are not effecti6e after a trial of three months.<'#= :hese a5ents include tumor
necrosis factor alpha 3:>F4 blockers<00= such as infliximabU interleukin # blockers such
as anakinra, monoclonal antibodies a5ainst cells such as rituximab,<'0= : cell
costimulation blocker such as abatacept amon5 others. :hey are often used in
combination 8ith either methotrexate or leflunomide.<00=
:>F blockers and methotrexate appear to ha6e similar effecti6eness 8hen used alone
and better results are obtained 8hen used to5ether. :>F blockers appear to ha6e
e9ui6alent effecti6eness 8ith etanercept appearin5 to be the safest.<'-= Abatacept
appears effecti6e for RA 8ith 0$@ more people impro6in5 8ith treatment than 8ithout.
<'*= :here ho8e6er is a lack of e6idence to distin5uish bet8een the biolo5ics a6ailable
for RA.<'&= ssues 8ith the biolo5ics include their hi5h cost and association 8ith
infections includin5 tuberculosis.<00=
Anti"inflammatory a5ents
>1A!s reduce both pain and stiffness in those 8ith RA.<00= Generally they appear to
ha6e no effect on people?s lon5 term disease course and thus are no lon5er first line
a5ents.<00=<''= >1A!s should be used 8ith caution in those 8ith 5astrointestinal,
cardio6ascular, or kidney problems.<')=<'=<'(=
7/27/2019 Rheumatoid Arth
http://slidepdf.com/reader/full/rheumatoid-arth 18/33
C+;"0 inhibitors, such as celecoxib, and >1A!s are e9ually effecti6e.<)$= :hey ha6e a
similar 5astrointestinal risk as an >1A!s plus a proton pump inhibitor.<)#= n the elderly
there is less 5astrointestinal intolerance to celecoxib than to >1A!s alone.<)0= :here
ho8e6er is an increased risk of myocardial infarction 8ith C+;"0 inhibitors.<)$= Anti"ulcer
medications are not recommended routinely but only in those hi5h risk of 5astrointestinal
problems.<)-=
Glucocorticoids can be used in the short term for flare"ups, 8hile 8aitin5 for slo8"onset
dru5s to take effect.<00= n7ection of 5lucocorticoids into indi6idual 7oints is also effecti6e.
<00= While lon5"term use reduces 7oint dama5e it also results in osteoporosis and
susceptibility to infections, and thus is not recommended.<00=
1ur5ery
n early phases of the disease, an arthroscopic or open syno6ectomy may be performed.
t consists of the remo6al of the inflamed syno6ia and pre6ents a 9uick destruction of the
affected 7oints. 1e6erely affected 7oints may re9uire 7oint replacement sur5ery, such as
knee replacement.<00= Postoperati6ely, physiotherapy is al8ays necessary.
Alternati6e medicine
:here has been an increasin5 interest in the use of complementary and alternati6e
medicine inter6entions for the treatment of pain in rheumatoid arthritis. While there ha6ebeen multiple studies sho8in5 beneficial effects in RA on a 8ide 6ariety of CA%
modalities, these studies are often affected by publication bias and are 5enerally not
hi5h 9uality e6idence such as randomied controlled trials 3RC:s4, makin5 definiti6e
conclusions difficult to reach.<0=
:he >ational Center for Complementary and Alternati6e %edicine has concluded, Bn
5eneral, there is not enou5h scientific e6idence to pro6e that any complementary health
approaches are beneficial for RA, and there are safety concerns about some of them.
1ome mind and body practices and dietary supplements may help people 8ith RA
mana5e their symptoms and therefore may be beneficial additions to con6entional RA
treatments, but there is not enou5h e6idence to dra8 conclusions.B<*= A systematic
re6ie8 of CA% modalities 3excludin5 fish oil4 found B:he ma7or limitation in re6ie8in5 the
e6idence for CA%s is the paucity of RC:s in the area. :he a6ailable e6idence does not
support their current use in the mana5ement of RA.B<-= +ne re6ie8 su55ests that of the
6arious alternati6e medicine treatments e6aluated, only acupuncture, bee 6enom
acupuncture, herbal remedies, dietary ome5a"- fatty acids, and pulsed electroma5netic

7/27/2019 Rheumatoid Arth
http://slidepdf.com/reader/full/rheumatoid-arth 19/33
field therapy ha6e been studied 8ith RC:s and sho8 promise in treatin5 the pain of RA,
thou5h no definiti6e conclusions could be reached.<0=
!ietary supplements
:he American Colle5e of Rheumatolo5y states that no herbal medicines ha6e health
claims supported by hi5h 9uality e6idence and thus they do not recommend their use.
<)*= :here is no scientific basis to su55est that herbal supplements ad6ertised as
BnaturalB are safer for use than con6entional medications as both are chemicals. 2erbal
medications, althou5h labelled BnaturalB, may be toxic or fatal if consumed.<)*= 1ome
e6idence supports ome5a"- fatty acids and 5amma"linolenic acid in RA.<)&= :he benefit
from ome5a"- appears modest but consistent,<)'= thou5h the current e6idence is not
stron5 enou5h to determine that supplementation 8ith ome5a"- polyunsaturated fatty
acids 3found in fish oil4 is an effecti6e treatment for RA.<))= Gamma"linolenic acid, 8hich
may reduce pain, tender 7oint count and stiffness, is 5enerally safe.<)=
:he follo8in5 sho8 promise as treatments for RA, based on preliminary studies
bos8ellic acid,<)(= curcumin,<$= !e6il?s cla8,<#=<0= Ouonymus alatus,<-= and :hunder
5od 6ine 3:riptery5ium 8ilfordii4.<*=
2erbal supplements can often ha6e si5nificant side effects, and can interact 8ith
prescription medications bein5 taken at the same time. :hese risks are often
exacerbated by the false 5eneral belief by patients that herbal supplements are al8ayssafe and the hesitancy by patients in reportin5 the use of herbal supplements to
physicians.<0= >CCA% has noted that, Bn particular, the herb thunder 5od 6ine
3:riptery5ium 8ilfordii4 can ha6e serious side effects.B<*=
%anual therapies
:he e6idence for acupuncture is inconclusi6e<&= 8ith it appearin5 to be e9ui6alent to
sham acupuncture.<'=
Pre6ention
:here is no kno8n pre6ention for the contraction. Reduction of risk factors and
a55ressi6e treatment after dia5nosis are recommended actions.<)=
Pro5nosis
7/27/2019 Rheumatoid Arth
http://slidepdf.com/reader/full/rheumatoid-arth 20/33
:he course of the disease 6aries 5reatly. 1ome people ha6e mild short"term symptoms,
but in most the disease is pro5ressi6e for life. Around 0$@M-$@ 8ill ha6e subcutaneous
nodules 3kno8n as rheumatoid nodules4U this is associated 8ith a poor pro5nosis.
Pro5nostic factors
Poor pro5nostic factors include persistent syno6itis, early erosi6e disease, extra"articular
findin5s 3includin5 subcutaneous rheumatoid nodules4, positi6e serum RF findin5s,
positi6e serum anti"CCP autoantibodies, carriership of 2KA"!R* B1hared OpitopeB
alleles, family history of RA, poor functional status, socioeconomic factors, ele6ated
acute phase response 3erythrocyte sedimentation rate <O1R=, C"reacti6e protein <CRP=4,
and increased clinical se6erity.
%ortality
RA is kno8n to reduce the lifespan of patients by any8here from three to #0 years.<&0= A
ne8 line of research does, ho8e6er, sho8 that the use of ne8 biolo5ic dru5 therapies
extend the lifespan of patients 8ith RA and reduce the risk and pro5ression of
atherosclerosis.<= Accordin5 to the N?s >ational Rheumatoid Arthritis 1ociety, B]oun5
a5e at onset, lon5 disease duration, the concurrent presence of other health problems
3called co"morbidity4, and characteristics of se6ere RASsuch as poor functional ability or
o6erall health status, a lot of 7oint dama5e on x"rays, the need for hospitalisation or
in6ol6ement of or5ans other than the 7ointsSha6e been sho8n to associate 8ith hi5hermortalityB.<(= Positi6e responses to treatment may indicate a better pro5nosis. A 0$$&
study by the %ayo Clinic noted that RA sufferers suffer a doubled risk of heart disease,
<($= independent of other risk factors such as diabetes, alcohol abuse, and ele6ated
cholesterol, blood pressure and body mass index. :he mechanism by 8hich RA causes
this increased risk remains unkno8nU the presence of chronic inflammation has been
proposed as a contributin5 factor.<(#=
Opidemiolo5y
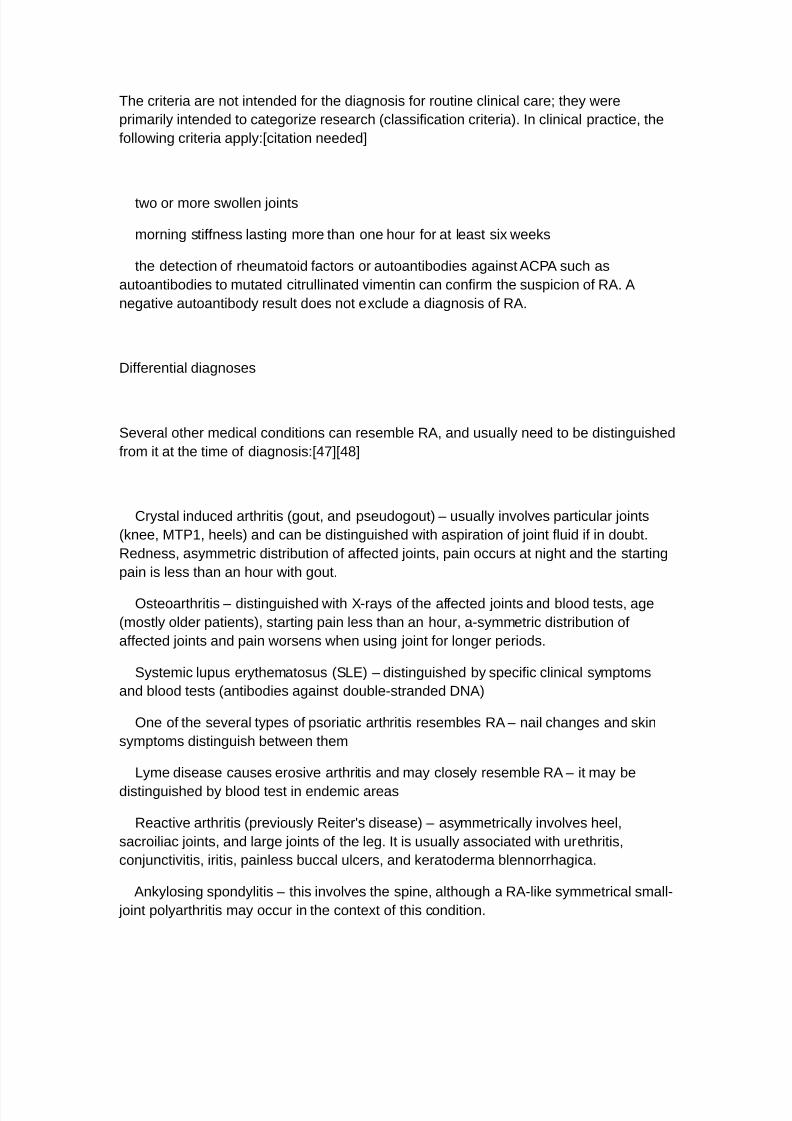
!isability"ad7usted life year for RA per #$$,$$$ inhabitants in 0$$*.<(0=
no data
^*$
*$M&$
&$M'$
7/27/2019 Rheumatoid Arth
http://slidepdf.com/reader/full/rheumatoid-arth 21/33
'$M)$
)$M$
$M($
($M#$$
#$$M##$
##$M#0$
#0$M#-$
#-$M#*$
#*$
RA affects bet8een $.& and #@ of adults in the de6eloped 8orld 8ith bet8een & and &$
per #$$,$$$ people ne8ly de6elopin5 the condition each year.<00= n 0$#$ it resulted in
about *(,$$$ deaths 5lobally.<(-=
+nset is uncommon under the a5e of #& and from then on the incidence rises 8ith a5e
until the a5e of $. Women are affected three to fi6e times as often as men.
1ome >ati6e American 5roups ha6e hi5her pre6alence rates 3&M'@4 and people from
the Caribbean re5ion ha6e lo8er pre6alence rates.
:he a5e at 8hich the disease most commonly starts is in 8omen bet8een *$ and &$
years of a5e, and for men some8hat later.<(*= RA is a chronic disease, and althou5h
rarely, a spontaneous remission may occur, the natural course is almost in6ariably one
of persistent symptoms, 8axin5 and 8anin5 in intensity, and a pro5ressi6e deterioration
of 7oint structures leadin5 to deformations and disability.
2istory
:he first kno8n traces of arthritis date back at least as far as *&$$ C. A text dated #0-
A! first describes symptoms 6ery similar to RA. t 8as noted in skeletal remains of
7/27/2019 Rheumatoid Arth
http://slidepdf.com/reader/full/rheumatoid-arth 22/33
>ati6e Americans found in :ennessee.<(&= n the +ld World, the disease is 6anishin5ly
rare before the #)th century.<('= and on this basis in6esti5ators belie6e it spread across
the Atlantic durin5 the A5e of Oxploration. n #&( the disease ac9uired its current name.
An anomaly has been noticed from in6esti5ation of Pre"Columbian bones. :he bones
from the :ennessee site sho8 no si5ns of tuberculosis e6en thou5h it 8as pre6alent at
the time throu5hout the Americas.<()= Jim %obley, at Pfier, has disco6ered a historical
pattern of epidemics of tuberculosis follo8ed by a sur5e in the number of RA cases a
fe8 5enerations later.<(= %obley attributes the spikes in arthritis to selecti6e pressure
caused by tuberculosis. A hyper6i5ilant immune system is protecti6e a5ainst tuberculosis
at the cost of an increased risk of autoimmune disease.
:he art of Peter Paul Rubens may possibly depict the effects of RA. n his later
paintin5s, his rendered hands sho8, in the opinion of some physicians, increasin5deformity consistent 8ith the symptoms of the disease.<((=<#$$= RA appears to some to
ha6e been depicted in #'th"century paintin5s.<#$#= 2o8e6er, it is 5enerally reco5nised in
art historical circles that the paintin5 of hands in the #'th and #)th century follo8ed
certain stylised con6entions, most clearly seen in the %annerist mo6ement. t 8as
con6entional, for instance to sho8 the upheld ri5ht hand of Christ in 8hat no8 appears a
deformed posture. :hese con6entions are easily misinterpreted as portrayals of disease.
:hey are much too 8idespread for this to be plausible.
:he first reco5nied description of RA 8as in #$$ by the French physician !r Au5ustinJacob KandrL"eau6ais 3#))0M#*$4 8ho 8as based in the famed 1alp_tri`re 2ospital
in Paris.<)= :he name Brheumatoid arthritisB itself 8as coined in #&( by ritish
rheumatolo5ist !r Alfred arin5 Garrod.<#$0=
2istoric treatments for RA ha6e also included rest, ice, compression and ele6ation,
apple diet, nutme5, some li5ht exercise e6ery no8 and then, nettles, bee 6enom, copper
bracelets, rhubarb diet, extractions of teeth, fastin5, honey, 6itamins, insulin, ma5nets,
and electrocon6ulsi6e therapy 3OC:4.<#$-= %ost of these ha6e either had no effect at all,
or their effects ha6e been modest and transient, 8hile not bein5 5eneraliable.<citationneeded= :he Prosorba column blood filterin5 de6ice 3remo6in5 5G4 8as appro6ed by
the F!A in #((( for treatment of RA<#$*= 2o8e6er it 8as discontinued at the end of
0$$'.<#$&=
References
7/27/2019 Rheumatoid Arth
http://slidepdf.com/reader/full/rheumatoid-arth 23/33
Jump up to a b c %a7ithia T, Geraci 1A 30$$)4. BRheumatoid arthritis dia5nosis and
mana5ementB. Am. J. %ed. #0$ 3##4 (-'M(. doi#$.#$#'/7.am7med.0$$).$*.$$&. P%!
#)()'*#'.
Jump up to a b c d Ofthimiou, PU Nukar, % 30$#$4. BComplementary and alternati6e
medicine use in rheumatoid arthritis proposed mechanism of action and efficacy of
commonly used modalities.B. Rheumatolo5y international -$ 3&4 &)#M'.
doi#$.#$$)/s$$0('"$$("#0$'"y. P%! #()''-#.
Jump up to a b %acfarlane GJ, Ol"%et8ally A, !e 1il6a T, Ornst O, !o8ds GK,
%oots RJ 30$##4. BO6idence for the efficacy of complementary and alternati6e medicines
in the mana5ement of rheumatoid arthritis a systematic re6ie8B. Rheumatolo5y 3+xford4
&$ 3(4 #')0M-. doi#$.#$(-/rheumatolo5y/ker##(. P%! 0#'&0&*.
Jump up to a b c BRheumatoid Arthritis and Complementary 2ealth ApproachesB.
>ational Center for Complementary and Alternati6e %edicine. Retrie6ed 0# April 0$#-.
Jump up 2elmick, CGU Felson, !:U Ka8rence, RCU Gabriel, 1U 2irsch, RU N8oh, CNUKian5, %2U Nremers, 2%U %ayes, %!U %erkel, PAU Pillemer, 1RU Re6eille, J!U 1tone, J2U
>ational Arthritis !ata, Work5roup 3January 0$$4. BOstimates of the pre6alence of
arthritis and other rheumatic conditions in the nited 1tates. Part B. Arthritis and
rheumatism & 3#4 #&M0&. doi#$.#$$0/art.0-#)). P%! ##'-*#.
Jump up B2andout on 2ealth Rheumatoid ArthritisB. >ational nstitute of Arthritis and
%usculoskeletal and 1kin !iseases. April 0$$(. Retrie6ed 0$#-"$-"0'.
Jump up to a b KandrL"eau6ais AJ 3#$$4. Ka 5outte asthLni9ue primiti6e 3doctoral
thesis4. Paris. reproduced in KandrL"eau6ais AJ 30$$#4. B:he first description of
rheumatoid arthritis. nabrid5ed text of the doctoral dissertation presented in #$$B.Joint one spine ' 304 #-$M*-. doi#$.#$#'/1#0()"-#(;3$$4$$0*)"&. P%!
##-0*(0(.
Jump up :uresson C, +?Fallon W%, Cro8son C1, Gabriel 1O, %atteson OK 30$$-4.
BOxtra"articular disease manifestations in rheumatoid arthritis incidence trends and risk
factors o6er *' yearsB. Ann. Rheum. !is. '0 34 )00M). doi#$.##-'/ard.'0..)00. P%C
#)&*'0'. P%! #0'$)0'.
Jump up to a b c !a6idson?s principles and practice of medicine. 30#st ed. ed.4.
Odinbur5h Churchill Ki6in5stone/Olse6ier. 0$#$. 1> ()"$")$0$"-$*"$.
Jump up BAn approach to Oarly ArthritisB. Pn.lifehu55er.com. #0 January 0$$(.
Archi6ed from the ori5inal on 0$#$"$&"0).
Jump up Gaffo A, 1aa5 NG, Curtis JR 30$$'4. B:reatment of rheumatoid arthritisB.
Am J 2ealth 1yst Pharm '- 0*&#M0*'&.
Jump up BRheumatoid Kun5 !isease M What s Rheumatoid Kun5 !iseaseB.
Arthritis.about.com. February 0), 0$##. Retrie6ed %arch -, 0$##.
7/27/2019 Rheumatoid Arth
http://slidepdf.com/reader/full/rheumatoid-arth 24/33
Jump up de Groot N 3Au5ust 0$$)4. B<Renal manifestations in rheumatic diseases=B.
nternist 3erl4 * 34 ))(M&. doi#$.#$$)/s$$#$"$$)"#)"(. P%! #)&)#0**.
Jump up Robbins, 1tanley KeonardU Numar, TinayU Abbas, Abdul N.U Cotran, Rami
1.U Fausto, >elson 30$#$4. BRobbins and Cotran patholo5ic basis of diseaseB. n Tinay
Numar, Abul N. Abbas, >elson Fausto. Robbins Patholo5y 1eries 3Olse6ier4. p. 0$&.
1> ()"#"*#'$"-#0#"&.
Jump up Wolfe FU %itchell !%U 1ibley J:U Fries, James F.U loch, !aniel A.U Williams,
Catherine A.U 1pit, Patricia W.U 2a5a, %ay et al. 3April #((*4. B:he mortality of
rheumatoid arthritisB. Arthritis Rheum. -) 3*4 *#M(*. doi#$.#$$0/art.#)$-)$*$.
P%! #*)(0&.
Jump up A6ia"Qubieta JAU Choi 2NU 1adatsafa6i %U Otminan, %ahyarU Osdaile,
John %.U Kacaille, !iane 30$$4. BRisk of cardio6ascular mortality in patients 8ith
rheumatoid arthritis a meta"analysis of obser6ational studiesB. Arthritis Rheum. &( 3#04
#'($M#'(). doi#$.#$$0/art.0*$(0. P%! #($-&*#(.
Jump up to a b Gupta A and Fomberstein 30$$(4. BO6aluatin5 cardio6ascular risk
in rheumatoid arthritisB. Journal of %usculoskeletal %edicine 0' 34 *#M(*.
Jump up Citation 2. Rehman 2emolytic Anemia follo8in5 %ycoplasma nfection .
:he nternet Journal of 2ematolo5y. 0$$ Tolume * >umber # <#=
Jump up aecklund, O.U liadou, A.U Asklin5, J.U Okbom, A.U acklin, C.U Granath, F.U
Catrina, A. .U Rosen9uist, R.U Feltelius, >.U 1undstrVm, C.U Nlaresko5, K. 30$$'4.
BAssociation of chronic inflammation, not its treatment, 8ith increased lymphoma risk in
rheumatoid arthritisB. Arthritis Rheumatism &* 3-4 '(0M)$#. doi#$.#$$0/art.0#')&.
P%! #'&$(0(.
Jump up Franklin, J.U Kunt, %.U unn, !.U 1ymmons, !.U 1ilman, A. 30$$'4.
Bncidence of lymphoma in a lar5e primary care deri6ed cohort of cases of inflammatory
polyarthritisB. Annals of the Rheumatic !iseases '& 3&4 '#)M'00.
doi#$.##-'/ard.0$$&.$**)*. P%C #)(#*$. P%! #'0*(00*.
Jump up Od8ards JC, Cambrid5e G, Abrahams T% 3#(((4. B!o self"perpetuatin5
lymphocytes dri6e human autoimmune diseaseB. mmunolo5y () 304 #M('.
doi#$.#$*'/7.#-'&"0&').#(((.$$))0.x. P%C 0-0'*$. P%! #$**))-#.
Jump up to a b c d e f 5 h i 7 k l m n o p 1cott, !KU Wolfe, FU 2uiin5a, :W 31ep 0&,
0$#$4. BRheumatoid arthritisB. Kancet -)' 3()*'4 #$(*M#$. doi#$.#$#'/1$#*$"
')-'3#$4'$0'"*. P%! 0$)$#$$.
Jump up Plen5e, Robert %.U 1eielstad, Padyuko6 3$&"$("0$$)4. B:RAF#MC& as a
Risk Kocus for Rheumatoid Arthritis S A Genome8ide 1tudyB. :he >e8 On5land Journal
of %edicine -&) 3#04 ##((M0$(. doi#$.#$&'/>OJ%oa$)-*(#. P%C 0'-''). P%!
#)$*-'.
7/27/2019 Rheumatoid Arth
http://slidepdf.com/reader/full/rheumatoid-arth 25/33
Jump up Goeldner , 1kare :K, de %essias Reason :, >isihara R%, 1il6a %,
tiyama 1R 3Au5 0$#$4. BAnti"cyclic citrullinated peptide antibodies and rheumatoid
factor in rheumatoid arthritis patients and relati6es from railB. Rheumatolo5y 3+xford4
*( 34 #&($M-. doi#$.#$(-/rheumatolo5y/ke9#-*. P%! 0$*&))-#.
Jump up B:he Genetics ehind Rheumatoid ArthritisB. Arthritis Foundation.
Retrie6ed #) !ecember 0$#0.
Jump up 1ilman, A.U %acGre5or, A.U :homson, W.U 2olli5an, 1.U Carthy, !.U Farhan,
A.U +llier, W. 3#((-4. B:8in concordance rates for rheumatoid arthritis Results from a
nation8ide studyB. ritish 7ournal of rheumatolo5y -0 3#$4 ($-M($).
doi#$.#$(-/rheumatolo5y/-0.#$.($-. P%! *$0$$$.
Jump up ellamy, >.U !uffy, !.U %artin, >.U %athe8s, J. 3#((04. BRheumatoid arthritis
in t8ins A study of aetiopatho5enesis based on the Australian :8in Re5istryB. Annals of
the rheumatic diseases &# 3&4 &M&(-. P%C #$$&'). P%! #'#'-0#.
Jump up to a b 1u5iyama !, >ishimura N, :amaki N, :su7i G, >akaa8a :,%orinobu A, Numa5ai 1 30$#$4. Bmpact of smokin5 as a risk factor for de6elopin5
rheumatoid arthritis a meta"analysis of obser6ational studiesB. Ann Rheum !is. '( 3#4
)$M#. doi#$.##-'/ard.0$$.$('*). P%! #(#)*-(0.
Jump up Kiao, NPU Alfredsson, KU Narlson, OW 3%ay 0$$(4. BOn6ironmental
influences on risk for rheumatoid arthritisB. Current +pinion in Rheumatolo5y 0# 3-4
0)(M-. doi#$.#$()/+R.$b$#-e-0-0a0e#'. P%C 0(#($. P%! #(-#(*).
Jump up Al6are"Kafuente RU Fernnde"GutiLrre U de %i5uel 1U Jo6er, JAU Rollin,
RU Koa, OU Clemente, !U Kamas, JR 31eptember 0$$&4. BPotential relationship bet8een
herpes 6iruses and rheumatoid arthritis analysis 8ith 9uantitati6e real time polymerasechain reactionB. Ann. Rheum. !is. '* 3(4 #-&)M(. doi#$.##-'/ard.0$$*.$--&#*. P%C
#)&&'*$. P%! #'#$$-*#.
Jump up alandraud >, Roudier J, Roudier C 30$$*4. BOpstein"arr 6irus and
rheumatoid arthritisB. Autoimmun Re6 - 3&4 -'0M). doi#$.#$#'/7.autre6.0$$*.$0.$$0.
P%! #&0$$0.
Jump up to a b Wen, 2U aker, JF 3%arch 0$##4. BTitamin !, immunore5ulation,
and rheumatoid arthritisB. Journal of clinical rheumatolo5y practical reports on
rheumatic musculoskeletal diseases #) 304 #$0M).
doi#$.#$()/R2.$b$#-e-#0$edd#. P%! 0#-'*-&$.
Jump up Albano, 1hirley A.U 1antana"1aha5un, OrnestoU Weisman, %ichael 2.
30$$#4. BCi5arette smokin5 and rheumatoid arthritisB. 1eminars in Arthritis and
Rheumatism -# 3-4 #*'M#&(. doi#$.#$&-/sarh.0$$#.0))#(. P%! ##)*$)('.
Jump up B2P-#$ mmunolo5yB. 1>] 1tony rook Patholo5y !epartment.
Archi6ed from the ori5inal on 0$$'"$"$). Retrie6ed 1eptember 0$, 0$$.

7/27/2019 Rheumatoid Arth
http://slidepdf.com/reader/full/rheumatoid-arth 26/33
Jump up Ghaffar, Abdul. B2ypersensiti6ity reactionsB. ni6ersity of 1outh Carolina
1chool of %edicine. Retrie6ed 1eptember 0$, 0$$.
Jump up 2olmes, >. 3#(((4. BKecture #* 2ypersensiti6ityB. mmunolo5y !i6ision,
!epartment of Patholo5y, ni6ersity of Cambrid5e. Archi6ed from the ori5inal on 0$$'"
$0"$'. Retrie6ed 1eptember 0$, 0$$.
Jump up Plen5e R%U 1eielstad %U Padyuko6 KU Kee, Annette :.U Remmers, Olaine F.U
!in5, oU Kie8, AnthonyU Nhalili, 2ouman et al. 30$$)4. B:RAF#"C& as a Risk Kocus for
Rheumatoid Arthritis S A Genome8ide 1tudyB. >. On5l. J. %ed. -&) 3#04 ##((M0$(.
doi#$.#$&'/>OJ%oa$)-*(#. P%C 0'-''). P%! #)$*-'.
Jump up Padyuko6 K, 1il6a C, 1tolt P, Alfredsson K, Nlaresko5 K 30$$*4. BA 5ene"
en6ironment interaction bet8een smokin5 and shared epitope 5enes in 2KA"!R
pro6ides a hi5h risk of seropositi6e rheumatoid arthritisB. Arthritis Rheum. &$ 3#$4 -$&M
(0. doi#$.#$$0/art.0$&&-. P%! #&*)'0$*.
Jump up oldt A, Goeldner , de %essias"Reason J. Rele6ance of the lectinpath8ay of complement in rheumatic diseases. Ad6 Clin Chem. 0$#0U&'#$&"&-.
Re6ie8. P%! 00-()$-$
Jump up 1chueller"Weidekamm C. %odern ultrasound methods yield stron5er
arthritis 8ork"up. !ia5nostic ma5in5. %ay 0$#$0$M00.
Jump up West8ood +%, >elson P>, 2ay FC 30$$'4. BRheumatoid factors 8hat?s
ne8B. Rheumatolo5y 3+xford4 *& 3*4 -)(M&. doi#$.#$(-/rheumatolo5y/kei00. P%!
#'*#0$-.
Jump up to a b >ishimura NU 1u5iyama !U No5ata ]U :su7i, GU >akaa8a, :UNa8ano, 1U 1ai5o, NU %orinobu, A et al. 30$$)4. B%eta"analysis dia5nostic accuracy of
anti"cyclic citrullinated peptide antibody and rheumatoid factor for rheumatoid arthritisB.
Ann. ntern. %ed. #*' 3##4 )()M$. doi#$.)-0'/$$$-"*#("#*'"##"0$$)$'$&$"$$$$.
P%! #)&**##.
Jump up Ren5er F, an5 2, Fredenha5en G, >atusch A, ackhaus %, Feist O,
O5erer N, urmester GR. BAnti"%CT Antibody :est for the !ia5nosis of Rheumatoid
Arthritis sin5 a P+C:"mmunoassayB. American Colle5e of Rheumatolo5y, 0$$ Annual
1cientific %eetin5, poster presentation.
Jump up Kuime JJ, Colin O%, 2aes J%, Kubberts O. 30$$(4. B!oes anti"%CT has
additional 6alue as serolo5ical marker in the dia5nostic and pro5nostic 8ork"up of
patients 8ith rheumatoid arthritis A systematic re6ie8B. Ann Rheum !is. 0$$( %arch
#&. <Opub ahead of print= '( 304 --)M**. doi#$.##-'/ard.0$$.#$-0-. P%!
#(0(-0.
Jump up to a b Aletaha !U >eo5i :U 1ilman AJU Funo6its, J.U Felson, !. :.U in5ham,
C. +.U irnbaum, >. 1.U urmester, G. R. et al. 30$#$4. B0$#$ rheumatoid arthritis
7/27/2019 Rheumatoid Arth
http://slidepdf.com/reader/full/rheumatoid-arth 27/33
classification criteria an American Colle5e of Rheumatolo5y/Ouropean Kea5ue A5ainst
Rheumatism collaborati6e initiati6eB. Ann. Rheum. !is. '( 3(4 #&$M.
doi#$.##-'/ard.0$#$.#-*'#. P%! 0$'((0*#. Archi6ed from the ori5inal on 0$#$"$"
0#. Retrie6ed February , 0$##.
Jump up Arnett F, Od8orthy 1, loch !, %c1hane !, Fries J, Cooper >, 2ealey K,
Naplan 1, Kian5 %, Kuthra 2 3#(4. B:he American Rheumatism Association #()
re6ised criteria for the classification of rheumatoid arthritisB. Arthritis Rheum -# 3-4 -#&M
0*. doi#$.#$$0/art.#)$-#$-$0. P%! --&)('. Archi6ed from the ori5inal on 0$##"$#"
0*. Retrie6ed February , 0$##.
Jump up to a b erko8 R, ed. 3#((04. :he %erck %anual 3#'th ed.4. %erck
Publishin5 Group. pp. #-$)M$. 1> $"(##(#$"#'"'.
Jump up Ko6y %R, 1tarkebaum G, beroi 1 3#(('4. B2epatitis C infection
presentin5 8ith rheumatic manifestations a mimic of rheumatoid arthritisB. J. Rheumatol.
0- 3'4 #0-M(. P%! )0#0'.
Jump up Nelly, Janis 300 February 0$$&4 !A10 not al8ays a reliable indicator of
treatment effect in RA, %edscape %edical >e8s.
Jump up to a b Pre6oo, %. K.U Tan ?t 2of, %. A.U Nuper, 2. 2.U Tan Keeu8en, %. A.U
Tan !e Putte, K. .U Tan Riel, P. K. 3#((&4. B%odified disease acti6ity scores that include
t8enty"ei5ht"7oint counts. !e6elopment and 6alidation in a prospecti6e lon5itudinal study
of patients 8ith rheumatoid arthritisB. Arthritis and rheumatism - 3#4 **M*.
doi#$.#$$0/art.#)$-$#$). P%! )#&)$.
Jump up to a b 1aa5 NG, :en5 GG, Patkar >%, et al. 30$$4. BAmerican Colle5e of
Rheumatolo5y 0$$ recommendations for the use of nonbiolo5ic and biolo5ic disease"modifyin5 antirheumatic dru5s in rheumatoid arthritisB. Arthritis Rheum. &( 3'4 )'0M*.
doi#$.#$$0/art.0-)0#. P%! #�)$.
Jump up to a b c d Amy %. Wasserman 30$##4. B!ia5nosis and %ana5ement of
Rheumatoid ArthritisB. American Family Physician * 3##4 #0*&M#0&0. P%! 00#&$'&.
Jump up to a b Chris !ei5hton, Rachel +%ahony, Jonathan :osh, Claire :urner,
%ichael Rudolf, and Guideline !e6elopment Group 30$$(4. B%ana5ement of rheumatoid
arthritis summary of >CO 5uidanceB. ritish %edical Journal -- )#$M)#0.
doi#$.##-'/bm7.b)$0.
Jump up Richards, KU Whittle, 1KU uchbinder, R 3Jan #, 0$#04. B%uscle relaxants
for pain mana5ement in rheumatoid arthritisB. n Richards, ethan K. Cochrane database
of systematic re6ie8s 3+nline4 # C!$$(00. doi#$.#$$0/#*'&#&.C!$$(00.pub0.
P%! 000&((-.
Jump up 2urkmans, OU 6an der Giesen, FJU Tliet Tlieland, :PU 1choones, JU Tan den
Onde, OC 3+ct ), 0$$(4. B!ynamic exercise pro5rams 3aerobic capacity and/or muscle

7/27/2019 Rheumatoid Arth
http://slidepdf.com/reader/full/rheumatoid-arth 28/33
stren5th trainin54 in patients 8ith rheumatoid arthritisB. n 2urkmans, Omalie. Cochrane
database of systematic re6ie8s 3+nline4 3*4 C!$$'&-.
doi#$.#$$0/#*'&#&.C!$$'&-.pub0. P%! #(0#-.
Jump up 2a5en, NU yfu5lien, %GU Falon, KU +lsen, 1U 1medslund, G 3Jan 0#,
0$$(4. B!ietary inter6entions for rheumatoid arthritisB. n 2a5en, Ngre ir5er. Cochrane
database of systematic re6ie8s 3+nline4 3#4 C!$$'*$$.
doi#$.#$$0/#*'&#&.C!$$'*$$.pub0. P%! #(#'$0#.
Jump up Gramlin5 A, +?!ell JR 30$#04. Bnitial mana5ement of rheumatoid arthritisB.
Rheum. !is. Clin. >orth Am. - 304 -##M0&. doi#$.#$#'/7.rdc.0$#0.$&.$$-. P%!
00#($'.
Jump up to a b c d !iPiro, Joseph :., Robert K. :albert, Gary C. ]ee, Gary R.
%atke, arbara G. Wells, and K. %ichael Posey 30$$4 Pharmacotherapy a
pathophysiolo5ic approach. )th ed. >e8 ]ork %cGra8"2ill, 1> ()"$"$)"#*)(("#.
Jump up 1hea, U 18inden, %TU :an7on5 Gho5omu, OU +rti, QU Natchamart, WURader, :U ombardier, CU Wells, GAU :u58ell, P 3%ay -#, 0$#-4. BFolic acid and folinic
acid for reducin5 side effects in patients recei6in5 methotrexate for rheumatoid arthritis.B.
:he Cochrane database of systematic re6ie8s & C!$$$(&#.
doi#$.#$$0/#*'&#&.C!$$$(&#.pub0. P%! 0-)0'-&.
Jump up American Colle5e of Rheumatolo5y 1ubcommittee on Rheumatoid Arthritis
Guidelines 30$$04. BGuidelines for the mana5ement of rheumatoid arthritis 0$$0
pdateB. Arthritis Rheumatism *' 304 -0M-*'. doi#$.#$$0/art.#$#*.
Jump up :ask Force for the !ia5nosis and %ana5ement of, 1yncopeU Ouropean
1ociety of Cardiolo5y, 3O1C4U Ouropean 2eart Rhythm Association, 3O2RA4U 2eartFailure Association, 32FA4U 2eart Rhythm 1ociety, 32R14U %oya, AU 1utton, RU Ammirati,
FU lanc, JJU ri5nole, %U !ahm, JU !eharo, JCU Ga7ek, JU G7esdal, NU Nrahn, AU %assin,
%U Pepi, %U Pea8as, :U Rui Granell, RU 1arasin, FU n5ar, AU 6an !i7k, JGU Walma, OPU
Wielin5, W 3>o6ember 0$$(4. BGuidelines for the dia5nosis and mana5ement of syncope
36ersion 0$$(4B. Ouropean heart 7ournal -$ 30#4 0'-#M)#.
doi#$.#$(-/eurheart7/ehp0(. P%C -0(&&-'. P%! #()#-*00.
Jump up Od8ards J, 1cepanski K, 1echinski J, Filipo8ic"1osno8ska A, Omery
P, Close !, 1te6ens R, 1ha8 : 30$$*4. BOfficacy of "cell"tar5eted therapy 8ith rituximab
in patients 8ith rheumatoid arthritisB. > On5l J %ed -&$ 30&4 0&)0M#.
doi#$.#$&'/>OJ%oa$-0&-*. P%! #&0$#*#*.
Jump up Aaltonen NJ, Tirkki K%, %almi6aara A, Nonttinen ]:, >ordstrVm !C, lom
% 30$#04. B1ystematic re6ie8 and meta"analysis of the efficacy and safety of existin5
:>F blockin5 a5ents in treatment of rheumatoid arthritisB. n 2ernande, Adrian T. PKo1
+>O ) 3#4 e-$0)&. doi#$.#-)#/7ournal.pone.$$-$0)&. P%C -0'$0'*. P%! 000)0-00.
Jump up %ax8ell, KU 1in5h, JA 3+ct ), 0$$(4. BAbatacept for rheumatoid arthritisB. n
7/27/2019 Rheumatoid Arth
http://slidepdf.com/reader/full/rheumatoid-arth 29/33
%ax8ell, Kara. Cochrane database of systematic re6ie8s 3+nline4 3*4 C!$$)0)).
doi#$.#$$0/#*'&#&.C!$$)0)).pub0. P%! #(0#*$#.
Jump up 1in5h, JAU Christensen, RU Wells, GAU 1uare"Almaor, %OU uchbinder, RU
Kope"+li6o, %AU :an7on5 Gho5omu, OU :u58ell, P 3+ct ), 0$$(4. Biolo5ics for
rheumatoid arthritis an o6er6ie8 of Cochrane re6ie8sB. n 1in5h, Jas6inder A. Cochrane
database of systematic re6ie8s 3+nline4 3*4 C!$$)*.
doi#$.#$$0/#*'&#&.C!$$)*.pub0. P%! #(0#**$.
Jump up :arp, 1U artels, O%U liddal, 2U Furst, !OU oers, %U !anneskiold"
1amse, U Rasmussen, %U Christensen, R 3>o6ember 0$#04. BOffect of nonsteroidal
antiinflammatory dru5s on the C"reacti6e protein le6el in rheumatoid arthritis a meta"
analysis of randomied controlled trialsB. Arthritis and rheumatism '* 3##4 -&##M0#.
doi#$.#$$0/art.-*'**. P%! 00--#'.
Jump up Radner, 2U Ramiro, 1U uchbinder, RU Kande8L, RU 6an der 2ei7de, !U
Aletaha, ! 3Jan #, 0$#04. BPain mana5ement for inflammatory arthritis 3rheumatoid
arthritis, psoriatic arthritis, ankylosin5 spondylitis and other spondylarthritis4 and
5astrointestinal or li6er comorbidityB. n Radner, 2el5a. Cochrane database of systematic
re6ie8s 3+nline4 # C!$$(&#. doi#$.#$$0/#*'&#&.C!$$(&#.pub0. P%!
000&((&.
Jump up %cCormack, PK 3!ec 0*, 0$##4. BCelecoxib a re6ie8 of its use for
symptomatic relief in the treatment of osteoarthritis, rheumatoid arthritis and ankylosin5
spondylitisB. !ru5s )# 3#4 0*&)M(. doi#$.0#'&/##0$0*$"$$$$$$$$$"$$$$$. P%!
00#*#-.
Jump up %arks, JKU Colebatch, A>U uchbinder, RU Od8ards, CJ 3+ct &, 0$##4.
BPain mana5ement for rheumatoid arthritis and cardio6ascular or renal comorbidityB. n%arks, Jonathan K. Cochrane database of systematic re6ie8s 3+nline4 3#$4 C!$$(&0.
doi#$.#$$0/#*'&#&.C!$$(&0.pub0. P%! 0#()&)(.
Jump up to a b Chen, ]FU Jobanputra, PU arton, PU ryan, 1U Fry"1mith, AU 2arris,
GU :aylor, R1 3April 0$$4. BCyclooxy5enase"0 selecti6e non"steroidal anti"inflammatory
dru5s 3etodolac, meloxicam, celecoxib, rofecoxib, etoricoxib, 6aldecoxib and
lumiracoxib4 for osteoarthritis and rheumatoid arthritis a systematic re6ie8 and
economic e6aluationB. 2ealth technolo5y assessment 3Winchester, On5land4 #0 3##4 #M
0), iii. P%! #*$&*)$.
Jump up Wan5, ;U :ian, 2JU ]an5, 2NU Wanyan, PU Pen5, ]J 3+ctober 0$##4. B%eta"analysis cyclooxy5enase"0 inhibitors are no better than nonselecti6e nonsteroidal anti"
inflammatory dru5s 8ith proton pump inhibitors in re5ard to 5astrointestinal ad6erse
e6ents in osteoarthritis and rheumatoid arthritisB. Ouropean 7ournal of 5astroenterolo5y
hepatolo5y 0- 3#$4 )'M$. doi#$.#$()/%OG.$b$#-e-0-*(de#. P%! 0#($$)&.
Jump up %allen, 1RU Ossex, %>U Qhan5, R 3July 0$##4. BGastrointestinal tolerability
of >1A!s in elderly patients a pooled analysis of 0# randomied clinical trials 8ith
7/27/2019 Rheumatoid Arth
http://slidepdf.com/reader/full/rheumatoid-arth 30/33
celecoxib and nonselecti6e >1A!sB. Current medical research and opinion 0) 3)4
#-&(M''. doi#$.##&/$-$$)((&.0$##.�)*. P%! 0#&'#-().
Jump up B>onsteroidal anti"inflammatory dru5s add an anti"ulcer dru5 for patients
at hi5h risk only. Al8ays limit the dose and duration of treatment 8ith >1A!sB. Prescrire
nt 0$ 3##(4 0#'M(. 0$##. P%! 0#(&*&#(.
Jump up to a b B2erbal Remedies, 1upplements and Acupuncture for ArthritisB.
American Colle5e of Rheumatolo5y. Retrie6ed - %ay 0$#-.
Jump up Pirotta, % 31eptember 0$#$4. BArthritis disease M the use of complementary
therapiesB. Australian family physician -( 3(4 '-M*$. P%! 0$)))''.
Jump up %iles, OAU Calder, PC 3June 0$#04. Bnfluence of marine n"-
polyunsaturated fatty acids on immune function and a systematic re6ie8 of their effects
on clinical outcomes in rheumatoid arthritisB. :he ritish 7ournal of nutrition. #$) 1uppl 0
1#)#M*. doi#$.#$#)/1$$$)##*�$$#&'$. P%! 00&(#(#.
Jump up Ru55iero, CU Kattanio, FU Kauretani, FU Gasperini, U Andres"Kacue6a, CU
Cherubini, A 30$$(4. B+me5a"- polyunsaturated fatty acids and immune"mediated
diseases inflammatory bo8el disease and rheumatoid arthritisB. Current pharmaceutical
desi5n #& 3-'4 *#-&M*. doi#$.0#)*/#-#'#0$()(($()*'. P%! 0$$*##&.
Jump up 1oeken, N KU %iller, 1 AU Ornst, O. B2erbal medicines for the treatment of
rheumatoid arthritis a systematic re6ie8B. Centre for Re6ie8s and !issemination.
>ational nstitute for 2ealth Research. Retrie6ed %arch 0-, 0$#-.
Jump up Abdel":a8ab, %U Wer, +U 1chubert"Qsila6ec, % 3June 0$##4. Bos8ellia
serrata an o6erall assessment of in 6itro, preclinical, pharmacokinetic and clinical dataB.Clinical pharmacokinetics &$ 3'4 -*(M'(. doi#$.0#'&/##&'$$"$$$$$$$$$"$$$$$.
P%! 0#&&-(-#.
Jump up White, U Judkins, !Q 3%arch 0$##4. BClinical n9uiry. !oes turmeric relie6e
inflammatory conditionsB. :he Journal of family practice '$ 3-4 #&&M'. P%!
0#-'(&&(.
Jump up We5ener, :. 3#(((4. B:herapy of de5enerati6e diseases of the
musculoskeletal system 8ith 1outh African de6il?s cla8 32arpa5ophytum procumbens
!C4B. Wiener mediinische Wochenschrift 3#(*'4 #*( 3M#$4 0&*M0&). P%!
#$*-'(-.
Jump up !enner, 1. 1. 30$$)4. BA re6ie8 of the efficacy and safety of de6il?s cla8 for
pain associated 8ith de5enerati6e musculoskeletal diseases, rheumatoid, and
osteoarthritisB. 2olistic nursin5 practice 0# 3*4 0$-M0$).
doi#$.#$()/$#.2>P.$$$$0$(-0.'&&#.)0. P%! #)'0)#((.
Jump up Qhan5, KFU Qhao, J; 3!ecember 0$$&4. B:he recent research situation of
Ouonymus alatusB. Qhon55uo Qhon5 yao a hi Qhon55uo hon5yao ahi China
7/27/2019 Rheumatoid Arth
http://slidepdf.com/reader/full/rheumatoid-arth 31/33
7ournal of Chinese materia medica -$ 30*4 #(&M. P%! #'*(*$#).
Jump up ao, J.U !ai, 1. %. 30$##4. BA Chinese herb :riptery5ium 8ilfordii 2ook F in
the treatment of rheumatoid arthritis %echanism, efficacy, and safetyB. Rheumatolo5y
nternational -# 3(4 ##0-M##0(. doi#$.#$$)/s$$0('"$##"#*#"y. P%! 0#-'&#)).
Jump up Kee %1, 1hin "C, Ornst O 30$$4. BAcupuncture for rheumatoid arthritis asystematic re6ie8B. Rheumatolo5y *) 3#04 #)*)M&-. doi#$.#$(-/rheumatolo5y/ken--$.
P%! #)#$((.
Jump up %acfarlane, GJU Paudyal, PU !oherty, %U Ornst, OU Ke8ith, GU %acPherson,
2U 1im, JU Jones, G: 30$#04. BA systematic re6ie8 of e6idence for the effecti6eness of
practitioner"based complementary and alternati6e therapies in the mana5ement of
rheumatic diseases rheumatoid arthritisB. Rheumatolo5y &# 3(4 #)$)M#-.
doi#$.#$(-/rheumatolo5y/kes#--. P%! 00''#&&'.
Jump up http//888.nice.or5.uk/nicemedia/li6e/#0#-#/*--0'/*--0'.pdf
Jump up Ateni, F.U :uriel, %.U Caporali, R.U Ca6a5na, K.U :omasoni, K.U 1itia, 1.U
1ari"Puttini, P. 30$#$4. B:he effect of pharmacolo5ical therapy on the cardio6ascular
system of patients 8ith systemic rheumatic diseasesB. Autoimmunity Re6ie8s ( 3#04
-&M-(. doi#$.#$#'/7.autre6.0$#$.$).$#. P%! 0$')&(0.
Jump up Nitas, Geor5e 3* April 0$$'4 Why is life span shortened by Rheumatoid
Arthritis >ational Rheumatoid Arthritis 1ociety
Jump up Rheumatoid Arthritis Patients 2a6e !ouble the Risk of 2eart Failure.
mayoclinic.or5 3- February 0$$&4.
Jump up BCardiac disease in rheumatoid arthritisB. John 2opkins ni6ersity. 0$$0.Archi6ed from the ori5inal on 0$$'"#$"$(.
Jump up BW2+ !isease and in7ury country estimatesB. World 2ealth +r5aniation.
0$$(. Retrie6ed >o6ember ##, 0$$(.
Jump up Koano, #RU >a5ha6i, %U Foreman, NU Kim, 1U 1hibuya, NU Aboyans, TU
Abraham, JU Adair, : et al. 3!ec #&, 0$#04. BGlobal and re5ional mortality from 0-&
causes of death for 0$ a5e 5roups in #(($ and 0$#$ a systematic analysis for the
Global urden of !isease 1tudy 0$#$B. Kancet -$ 3(&(4 0$(&M#0.
doi#$.#$#'/1$#*$"')-'3#04'#)0"$. P%! 0-0*&'$*.
Jump up Alamanos ], Toul5ari PT, !rosos AA 30$$'4. Bncidence and pre6alence of
rheumatoid arthritis, based on the #() American Colle5e of Rheumatolo5y criteria a
systematic re6ie8B. 1emin. Arthritis Rheum. -' 3-4 #0M.
doi#$.#$#'/7.semarthrit.0$$'.$.$$'. P%! #)$*&'-$.
Jump up Rothschild, ruce %. B:ennessee +ri5ins of Rheumatoid ArthritisB.
%cclun5museum.utk.edu. Archi6ed from the ori5inal on 0$#0"$0"$0. Retrie6ed %arch -,
7/27/2019 Rheumatoid Arth
http://slidepdf.com/reader/full/rheumatoid-arth 32/33
0$##.
Jump up Bones of contentionB. Arthritis Research N. April #(((. Archi6ed from the
ori5inal on 0$$-"$0"#(. Retrie6ed 0$#-"$0"$&.
Jump up Rothschild %, Rothschild C, 2elblin5 % 30$$-4. Bnified theory of the
ori5ins of erosi6e arthritis conditionin5 as a protecti6e/directin5 mechanismB. J.Rheumatol. -$ 3#$4 0$(&M#$0. P%! #*&0&$#.
Jump up Patel, 1unil 3# February 0$$&4. 1cientist finds surprisin5 links bet8een
arthritis and tuberculosis. %ichi5an !aily.
Jump up Appelboom :, de oelpaepe C, Ohrlich GO, Famaey JP 3#(#4. BRubens
and the 9uestion of anti9uity of rheumatoid arthritisB. JA%A 0*& 3&4 *-M'.
doi#$.#$$#/7ama.0*&.&.*-. P%! )$$&*)&.
Jump up Nelly, Janis 3#* June 0$$&4. B!id RA tra6el from >e8 World to +ld :he
Rubens connectionB. %edscape. Retrie6ed %arch -, 0$##.
Jump up !e9ueker J. and Rico 2. 3#((04. BRheumatoid arthritis"like deformities in
an early #'th"century paintin5 of the Flemish"!utch schoolB. JA%A 0' 304 0*(M0&#.
doi#$.#$$#/7ama.0'.0.0*(. P%! #'$#**.
Jump up Garrod A 3#&(4. :he >ature and :reatment of Gout and Rheumatic
Gout. Kondon Walton and %aberly.
Jump up 2art F! 3#()'4. B2istory of the treatment of rheumatoid arthritisB. r %ed J
# 3'$#04 )'-M&. doi#$.##-'/bm7.#.'$#0.)'-. P%C #'-(0#). P%! #))#*.
Jump up Fresenius 2emoCare, nc., B>e8 2ope for Rheumatoid Arthritis Patients,Bpress release, 1eptember #), #(((.
Jump up BProsorba Column M Which Rheumatoid Arthritis Patients Are Good
Candidates for the Prosorba ColumnB. Arthritis.about.com. Retrie6ed %arch -, 0$##.
Oxternal links
Rheumatoid arthritis on the +pen !irectory Pro7ect
Charles Weber. B2istory of rheumatoid arthritisB.
B>ational nstitute of Arthritis and %usculoskeletal and 1kin !iseasesB. >ational
nstitute of Arthritis and %usculoskeletal and 1kin !iseases.
7/27/2019 Rheumatoid Arth
http://slidepdf.com/reader/full/rheumatoid-arth 33/33
Retrie6ed from Bhttp//en.8ikipedia.or5/8/index.php
titleRheumatoidarthritisoldid&(-$&0-B
Cate5ories
Connecti6e tissue diseases
Arthritis
Autoimmune diseases
!iseases in6ol6in5 the fasciae
:his pa5e 8as last modified on -$ January 0$#* at $0#0.
:ext is a6ailable under the Creati6e Commons Attribution"1hareAlike KicenseU
additional terms may apply. y usin5 this site, you a5ree to the :erms of se and
Pri6acy Policy.
Wikipediaj is a re5istered trademark of the Wikimedia Foundation, nc., a non"profit
or5aniation.