Embed Size (px)
Citation preview

10/23/2015
1
EXCELLENCE EXPERTISE INNOVATION
CollaborationforSuccessfulContactInvestigations
RexPryor,ShannonMeyer,&LaurenGiftOctober20,2015
Comprehensive Care of Patients with Tuberculosis and Their Contacts
October 19‐22, 2015Wichita, KS
• No conflict of interests
• No relevant financial relationships with any commercial companies pertaining to this educational activity
RexPryor,ShannonMeyer,&LaurenGifthavethefollowingdisclosuresto
make:

10/23/2015
2
Comprehensive Care of Patients with TB and Their Contacts
October 20, 2015
Presenters
Rex Pryor, Warden, Lansing Correctional Facility
Shannon Meyer, Deputy Warden, Lansing Correctional Facility
Lauren Gift, Health Services Administrator, Lansing Correctional Facility
Phil Griffin, Kansas Tuberculosis Controller
COLLABORATING FOR SUCCESSFUL CONTACT INVESTIGATIONS
OUTLINE OF PRESENTATION
• Background of building the Public Health and Department of Corrections relationship
• The Warden’s perspective of why this worked
• Medical events related to this investigation
• Timeline of events leading to the investigation
• The investigation process
• Keys to success

10/23/2015
3
BUILDING THE RELATIONSHIP
• May 2002 – I became TB Controller
• September 2002 – 4+ Smear Positive delayed diagnosis identified in a correctional facility
• No relationship with KDOC – believed what I was told
• Investigated 3 county jails and KDOC intake unit – 450 contacts total but only 30 – 50 in KDOC
BUILDING THE RELATIONSHIP
• 2003 – Contracted with an expert to deliver first training
• 2004 – Three courses and building stronger relationship
• 2005 – New offender diagnosed with TB – had been 2 cells away from offender in 2002, but not on contact list
• 1800+ staff and offenders put on watch list and investigated histories
• Total of 6 offenders and staff not identified in original investigation eventually have TB

10/23/2015
4
BUILDING THE RELATIONSHIP
• 2008 – Total rewrite of all TB protocols
• All TB related protocols and policies that point forward must be reviewed and approved by TB Program
• All convertors notified to TB program for review
• All isolations to evaluate for TB notified to TB program immediately
• All isolation releases cleared through TB program
• Full access to audit TB activities at each facility
• Audit points used to assist in writing the 2013 RFP for healthcare contract for KDOC
USING IGRA IN CORRECTIONAL SETTINGS
• Use of the IGRA in corrections is becoming more common
• Partnership between Public Health Department and Corrections is KEY to best outcomes
• Staff education on proper technique for obtaining the blood and preparing the specimen for transport is essential

10/23/2015
5
ADVANTAGES AND CHALLENGES OF THE IGRA
• Advantages to using the IGRA
• Results can be obtained after a single patient visit
• Variability of interpretation reduced from TST since interpretation performed by a qualified laboratory
• Not affected by previous BCG vaccination (eliminates false positives)
• Do not affect results of future IGRA tests
ADVANTAGES AND CHALLENGES OF THE IGRA
• Challenges to use of the IGRA
• Blood sample is required (possible increase in bloodbornepathogen exposures to staff)
• Blood specimens need to be processed within 12-16 hours after collection or with special onsite storage
• Perceived cost of testing may be a barrier with use on large populations

10/23/2015
6
BUILDING THE RELATIONSHIP
• Kansas Department of Health and Environment (KDHE) offered QFT to all state correctional facilities at no charge for use in particular circumstances
• Follow up any positive TST with a QFT (offender or staff)
• Use in all contact investigations
• Request use in special circumstances when high suspicion of TB and poor confidence in TST
• KDHE provided onsite training for all sites
• All QFT tubes supplied to sites by KDHE and tests processed at KDHE laboratory
BUILDING THE RELATIONSHIPTHE DATA IS SPEAKING
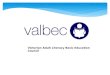
• In the first 10 months of the IGRA use, 65.9% of offenders with positive TST were found to be negative by QFT
• Only 2 refusals by offenders
• These significant results have influenced how we look at policy together
• This project has further strengthened the relationship
130
253
0
50
100
150
200
250
300
Positive Negative
Quantiferon Results10/2014 ‐ 7/2015(N= 384 positive TST)*
* 1 result was indeterminate and retested as negative

10/23/2015
7
ESTIMATED IGRA IMPACT TO DATE
• Collection of QFT prior to CXR in asymptomatic individuals in Kansas Correctional Facilities has resulted in multiple savings of financial as well as human resources.
• 253 offenders did not have CXR expense or exposure
• 253 offenders did not have to go onto chronic care
• 253 offenders did not have to be followed and counseled for treatment for TB infection or treated without need of treatment
• 3,800 to 20,240 offender movements for treatment eliminated (treatment for 9 months of INH or 12 Weeks of INH/Rifapentine)
IMPORTANCE OF COLLABORATION
• Coordination through the Warden’s office
• Communication between KDHE, central office, Corizon & contract monitor
• All actions processed/approved by Warden
• Cooperation between agencies
• Developed a detailed plan of action
• Consistent message from everyone
• Constantly kept staff informed

10/23/2015
8
MEDICAL HISTORY
• In & out of Kansas system since 2009
• Paroled & Absconded:
• Traveling carnival worker – Wake County, North Carolina
• Positive skin tests for 30 years; refused treatment
• Monitored in our system for LTBI
• No symptoms; all chest x-rays negative
• Returned to KDOC on PV (90 day sentence) in November of 2014
• Reported intentional violation to get hernia repair
PAROLE VIOLATION
• Intake:
• Weight 142
• BP 110/78
• Temp 99.1
• BMI 22.57
• Daily Alcohol, Amphetamine, and Marijuana Abuse
• No Cough, weight loss, appetite loss, fever, fatigue, chest pain, or night sweats.

10/23/2015
9
TB SCREENING & REFERRAL
• TB screening was negative
• Skin test not completed due to past positive
• Added to chronic care list for monitoring:
• LTBI
• Hep C
• Hx of prostate enlargement
• Current complaints of hernia
• Referred to HCP for follow-up
HERNIA
• Presented to HCP
• DP2 and VDRL ordered
• Left hernia, first noticed 2 yrs ago, pain 5/10
• Denied any other medical symptoms
• Stated he violated to get his hernia repaired, a pair of new glasses and some dentures.
• Exam revealed large hernia in left groin, full, hard, discolored.

10/23/2015
10
HERNIA REPAIR
• HCP placed referral for urgent hernia repair
• Admitted to infirmary, Tylenol #3 for pain management
• Surgical Consult – Hernia Repair Recommended
• Temp 98.9
• BP 109/72
• First Available Surgical Date Scheduled
POST-OP
• Returned to infirmary after surgical hernia repair at hospital
• Monitored closely and administered pain medication
• Within a few days, ambulating with no signs of distress
• Eating, drinking, managing all ADL’s
• Normal bowel movements
• No respiratory problems or cough

10/23/2015
11
RECOVERY
• Pain decreased, managed with Tylenol
• Post-surgical follow-up with surgeon: No concerns
• Healing well
• Had less than 60 days left to serve
• Looking forward to release
• Wanted new glasses, seen by optical
• No other complaints or symptoms UNTIL……
THEN WHAT?
• He presented 3 days before release at 6:44PM with the following symptoms:
• Weight loss
• Bilateral wheezing
• 100.6 temp
• Loose stool
• Tachycardia
• UA: Dark yellow, SG 1.010

10/23/2015
12
ADMITTED IMMEDIATELY
• Placed in Infirmary
• CXR ordered
• Isolation Precautions
• IV fluids started
• Monitor overnight, HCP follow-up AM
• Sent to outside hospital next day (2 days prior to sentence release date)
HOSPITALIZATION
• TB Precautions
• HIV Test Ordered
• Sputum Collected at Hospital
• CT of Chest Obtained
• Collaboration with Health Department
• Collaboration with Department of Corrections
• Precautionary investigation initiated

10/23/2015
13
PENDING RESULTS
• Why KDHE?
• Guidance for preliminary investigation
• Implications:
• At least 2 states (Kansas and North Carolina)
• Commercial Airplane Transportation
• Outside medical appointment and Surgery
• Infirmary Housing with immune compromised patients
RESULTS
• Small pulmonary nodules
• Small to moderate left pleural effusion
• Active disseminated TB disease could not be excluded
• Patient transferred to ICU
• Pneumonia vs TB vs pulmonary malignancy
• Plan: Confirm dx with induction of sputum
• Obtain HIV Test

10/23/2015
14
DIAGNOSIS & TREATMENT
• Sputum confirmed dx of active TB Disease
• Diagnosed with AIDS
• Remained in ICU
• Paroled (reached max date), remained in hospital receiving treatment
• Health department monitored patient closely
• Coordinated with parole to ensure continuity of care
• Facility conducted full contact investigation working collaboratively with KDHE
TB CONTROLLER RECEIVED THE CALL
• TB Controller scheduled to be in Atlanta for CDC consultation two days after the confirmation of disease
• Conference call set to get all on the same page
• Following call, TB Controller ordered expedited testing of specimen using NAAT, confirmed within 48 hours of suspicion
• New conference call to set action plan to prepare for site investigation and communication plan
• Warden sends first communications to staff and TB Controller leaves the state

10/23/2015
15
TIMELINE OF EVENTS
Broad list of details for KDHE to start with
• Housing
• List of Staff
- Security - Unit Team - Food Service
- Medical/Mental Health - Maintenance - Chaplain
• List of Offenders
• List of Outside Trips
INITIAL INFORMATION
• Security – 148
• Transport Officers - 10
• Unit Team – 10
• Medical/Mental Health - 39
• Offenders - 544
• Other Staff - 10

10/23/2015
16
CHALLENGES
• Confidentiality
• Assure staff that KDHE is leading the investigation & all test results would be confidential
• Scheduling in a 24/7 environment
• Different shifts
• Planned leave
• Days off
• Resignations
THE INVESTIGATION
• TB Controller returned to state and went directly from airport to Lansing Correctional Facility
• On site face to face meeting
• Regional Corizon Health Administration
• National Corizon Leaders on Phone
• KDOC Central Office Health Care Monitors
• Warden’s Senior Staff
• TB Controller

10/23/2015
17
THE INVESTIGATION
• TB Controller was presented with preliminary materials
• Detailed timeline of all movement
• Detailed list of all security staff who may have ever worked in the presence of the index case broken down by shifts
• Detailed list of all medical and mental health staff by contact
• Detailed list of all offenders who ever shared the cell house
• Facility diagrams and blue prints of air flow systems
• Full movement list of the index case
• And a bottle of water
THE INVESTIGATION
• Discussed the details of the index case and the immediate concerns of staff present
• Developed an education plan for staff and inmates
• Physical tour of facility
• All cell assignments
• Infirmary assignments
• Ventilation system
• Offices for discharge planning and mental health

10/23/2015
18
THE INVESTIGATION
• Staff Education
• Presentation to sergeants and leadership
• What is TB and how is it spread
• Likelihood of infection
• Process for selection of contact risks
• Process for conducting screenings
• Importance of compliance of officers
• Questions and answers
THE INVESTIGATION
• Contact priority assignment
• Reviewed all possible staff exposures
• Initial transport officers
• First and second shift – 5 shifts
• Third shift – 10 shifts
• Review of offender possible exposures
• One cell to the right or left
• One cell up or down
• Cellmates when in multi-man cells

10/23/2015
19
THE INVESTIGATION
• Contact priority assignment
• Required extensive assistance from DOC central office information technology to sort offender lists to be analyzed by public health
• Required extensive assistance from Deputy Warden to sort staff lists to be analyzed by public health
• Required extensive assistance from HSA to pull offender medical information to be analyzed by public health
THE INVESTIGATION
• Contact priority assignment
• Review medical staff possible exposures
• While in infirmary – 5 shifts
• Night of most symptoms
• Consideration of others
• Self identified staff with compromised immune systems
• Other offenders with comprised immune systems
• Referred “Worried Wells” to their own providers

10/23/2015
20
THE INVESTIGATION
• Baseline on record for everyone, so only tested 8 week post exposure
• Final screening numbers
• Round one
• Staff – 9
• Offenders – 32
• Round two
• Staff – 30
• Offenders - 6
THE INVESTIGATION
• With prioritizing exposures of contacts through Public Health best practice and CDC guidelines, the pool of contacts was narrowed from 761 to 77
• Over testing leads to many poor outcomes
• False beliefs about transmission likelihood
• Poor ability to evaluate instigation for completeness when transmission is found
• Poor follow through in future investigations

10/23/2015
21
THE INVESTIGATION
• The screening activities
• Used Quantiferon Gold In Tube on all contacts
• Only one encounter required
• Less subjective testing method
• Less likelihood of refusal
• More specific and sensitive test
• No BCG concerns
THE INVESTIGATION• TB Controller present for all individual screenings
• Staff
• Conducted testing starting at 10:00 PM for third shift coming on duty and second shift going off duty
• Conducted testing starting at 5:30 AM for first shift coming on duty
• Conducted testing between Noon and 2:00 PM for staff off duty, paid overtime for call in to test
• Warden required 100% compliance to continue work
• Each person was screened for signs and symptoms by TB Controller and offered one on one counsel to address any personal concerns
• Corizon Health staff drew the blood
• TB Controller took possession of the specimens immediately

10/23/2015
22
THE INVESTIGATION
• TB Controller present for all individual screenings
• Offenders
• Conducted testing starting at 7:00 AM
• Each offender was called out as in a sick call, mandated call
• Each person was screened for signs and symptoms by TB Controller and offered one on one counsel to address any personal concerns
• Corizon Health staff drew the blood
• TB Controller took possession of the specimens immediately
THE INVESTIGATION
• Specimens were transported to state public health lab for processing
• Priority processing
• All results reported directly to TB Controller only
• TB Controller provided results to Corizon Health for offenders and Corizon Health staff
• TB Controller provided results to Human Resources for DOC staff
• Contacts were provided results and given opportunity to discuss results with TB Controller if there were questions

10/23/2015
23
THE INVESTIGATION
• 76 negative results
• 1 positive result
• Officer, retested to assure accuracy
• Met with TB Controller for interview
• Not considered transmission from this case, likely other exposure to a family member
• Provided full health evaluation through Workers Compensation
• Provided full treatment for TB Infection through local health department
KEYS TO SUCCESS
• Mutual trust and respect of roles between Corrections, Healthcare Contractor and Public Health
• Complete transparency throughout process
• Open communication
• Unrestricted access as needed
• Warden supported and enforced all Public Health decisions and recommendations
• Public Health understood and respected security needs as well as confidentiality concerns of staff and offenders

10/23/2015
24
KEYS TO SUCCESS
• Use of QFT greatly reduced offender movement as only one encounter was required
• Use of QFT greatly reduced cost of overtime and rescheduling of staff as only one encounter was required
• 100% compliance in screening and testing because of Warden’s mandate
• No media attention or family complaint calls because education of risk was provided throughout the process and all questions that were posed were answered directly
ACKNOWLEDGEMENTS
• Lansing Correctional Facility Warden’s office and leadership team
• Corizon Health Kansas Regional Office
• Corizon Health Lansing Correctional Facility staff
• Kansas Department of Corrections Medical Monitoring staff
• Kansas Department of Corrections Classification staff
• Qiagen TBOSS Program
• Kansas Department of Health and Environment Laboratories
• Kansas Department of Health and Environment TB Program

10/23/2015
25