Embed Size (px)
Citation preview
EditorialNervous system and COVID-19 80Bertha Torres-Oliva, Karina Vélez-Jiménez, Idelfonso Rodríguez-Leyva, and Lorena Guerrero-Torres
Original Articles Preventive treatment in migraine. Used drugs and related variables. Results of the European work and migraine survey 82Ma. Teófila Vicente-Herrero, Ma. Victoria Ramírez-Iñiguez de la Torre, Elena Ruíz-de la Torre, and Luis Reinoso-Barbero
Executive dysfunction in middle-aged hypertensive adults 90Edwin J. Palma-Díaz, Damaris F. Estrella-Castillo, Rita E. Zapata-Vázquez, Edgar García-Santamaría, and Héctor A. Rubio Zapata
Clinical considerations on the introduction of ocrelizumab in Mexico 97Laura Ordoñez-Boschetti, Merced Velázquez-Quintana, Eli Skromne-Eisenberg, Irene Treviño-Frenk, Verónica Rivas-Alonso, Brenda Bertado-Cortes, Manuel De la Maza-Flores, Sandra Quiñones-Aguilar, Luis Amaya-Sánchez, Leonardo Llamas-López, and Victor Gonzalez-Amezquita
Cranial electrical stimulation for the treatment of insomnia, anxiety, and depression symptoms in adults 104Jesús A. Moo-Estrella, and María F. Pérez-Pichardo
Review ArticleSynapses and neural communication in neuropathological conditions 111Alejandro Sánchez, Dora L. Flores, Eugenio Leyva, and Carlos Castro
PERMANYERwww.permanyer.com
VOLUME 21 - NUMBER 3 / May-June 2020 – ISSN: 1665-5044
eISSN: 2604-6180
www.revmexneurociencia.com
Revista Mexicana de
NeurocienciaPublicación oficial de la Academia Mexicana de Neurología A.C.
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020
80
Nervous system and COVID-19Bertha Torres-Oliva1, Karina Vélez-Jiménez2, Idelfonso Rodríguez-Leyva3, and Lorena Guerrero-Torres4*1University of Guanajuato, Guanajuato; 2Hospital Ángeles Lomas, Mexico City; 3Neurology Service, Universidad Autónoma de San Luis Potosí, San Luis Potosí; 4Department of Infectious Diseases, Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán, Mexico City. Mexico
Revista Mexicana de Neurociencia
EDITORIAL
Correspondence: *Lorena Guerrero-Torres
Department of Infectious Diseases
Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán
Vasco de Quiroga 15, Tlalpan
C.P. 14080, Mexico City, Mexico
E-mail: [email protected]
Available online: 18-05-2020
Mex Neuroci. 2020;21(3):80-81
www.revmexneurociencia.com
Date of reception: 19-04-2020
Date of acceptance: 22-04-2020
DOI: 10.24875/RMN.M20000079
A new disease has been reported recently: COVID-19, caused by a novel virus which was named SARS-CoV-2 coronavirus1. COVID-19 started in Wuhan, China, in late December 2019 at a seafood market. Due to its high rate contagion, 59 suspected patients were transferred to a des-ignated hospital in Wuhan, China. The predominant symp-toms were fever, dry cough, myalgia, fatigue, and, less frequently, headache, hemoptysis, and diarrhea. More than half of the patients developed dyspnea during the 2nd week of the onset of symptoms and all presented pneumonia with abnormal chest CT, as well as lymphopenia. A significant elevation in inflammatory markers was found in patients admitted to the intensive care unit (ICU). In 41 of the 59 cas-es, nCoV 2019 infection was confirmed by next-generation sequencing or real-time RT-PCR methods1.
In this case series, a third of the patients had under-lying diseases such as diabetes, hypertension, and cardiovascular disease. Furthermore, it was more com-mon in males (73%), with a median age of 49 years. Other studies have confirmed that age and comorbidi-ties are associated with higher rates of hospitalization for COVID-192,3.
Regarding the neurological manifestations of COVID-19 infection, in the retrospective study published by Mao et al., the presence of neurological symptoms was sought inten-tionally in 214 hospitalized patients with confirmed SARS-CoV-2 disease. They were classified into three categories: (1) signs and symptoms of affection to the central nervous system (CNS) such as headache, dizziness, alteration of
consciousness, ataxia, acute cerebrovascular disease, and epilepsy, (2) signs and symptoms of affection to the cranial and peripheral nerves, such as taste impairment, smell impairment, vision impairment, or neuralgia, and (3) skele-tal and muscular injury manifestations. Neurological mani-festations were found in 78 (36.4%) of patients. CNS symp-toms were the main form of neurological injury, present in 53 (24.8%) of the cases. The most common symptoms were dizziness (16%) and headache (13%). Cranial nerve involvement was infrequent, with hypogeusia in 12 (5.6%), hyposmia in 11 (5.1%), and vision problems in 3 (2.3%). There were 23 (10.7%) patients with muscle injury2.
This study also showed differences between the characteristics of patients with severe infection (41%) and nonsevere infection (58.9%). Patients with severe infection were significantly older (58.2 ± 15.0 vs. 48.9 ± 14.7; p < 0.001), had more comorbidities (47.7% vs. 32.5%; p < 0.05), especially hypertension (36.4% vs. 15.1%; p < 0.001), and had fewer typical symptoms compared to patients with nonsevere infection. Further-more, neurological disease was more common in pa-tients with severe infection compared with nonsevere infection (45.5% vs. 30.2%; p < 0.02), particularly acute cerebrovascular disease (5.7% vs. 0.8%; p < 0.001), altered consciousness (14.8% vs. 2.4%; p < 0.001), and skeletal muscle damage (19.3 % vs. 4.8%; p < 0.001)2.
Although neurological manifestations of COVID-19 seemed uncommon, the self-reported olfactory and taste disorders (OTD) questionnaire carried out by Giacomelli
1665-5044/© 2020 Academia Mexicana de Neurología A.C. Published by Permanyer. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

81
B. Torres-Oliva, et al.: Nervous System and COVID 19
et al. in 59 hospitalized patients with COVID-19 in Milan, Italy, revealed the necessity to expand the study of these manifestations in nonhospitalized infected patients with COVID-19. These investigators reported an alteration in taste or smell in 20 (33.9%) of patients and the presence of both symptoms in 11 (18.6%) of the patients. Further-more, 20.3% of the patients experienced the symptoms before hospital admission and 13.5% after hospital ad-mission. Changes in taste were frequently (91%) identi-fied before hospitalization. Moreover, OTDs were more common in women and younger people4.
In a recent report of 58 patients hospitalized for SARS-CoV-2 acute respiratory distress syndrome, neu-rological abnormalities were detected in 49 (84%) of them; 40 (69%) presented agitation and confusion, and 39 (67%) a corticospinal tract injury. Magnetic reso-nance image of the brain performed in 13 patients revealed meningeal reinforcement in 8 (62%), cerebro-vascular disease in 3 (23%), and perfusion abnormali-ties in 11 (100%) patients who underwent this sequence. In the cerebrospinal fluid (CSF) examination of seven patients who underwent lumbar puncture, the presence of oligoclonal bands was found in 2 (29%), high proteins and IgG in 1 (14%), and low albumin in 4 (57%). All CSF samples were negative for SARS-CoV-25.
Other manifestations caused by SARS-CoV-2 have emerged. As reported by Italian researchers, five patients with COVID-19 among their 1000 to 12,000 patients pre-sented a typical Guillain-Barré syndrome (GBS), with an interval from 5 to 10 days between the onset of COVID-19 symptoms and the first Guillain-Barré symptom. Three of these patients had ageusia or anosmia 5-7 days before the start of GBS. The CSF analysis reported an average protein level in two of them and a normal leukocyte count in all patients. Antiganglioside antibodies were tested in three patients and found normal. All RT-PCR of the CSF was negative for SARS-CoV-2. The electrophysiological studies reported an axonal variant in three patients and a demyelination variant in two patients. Gadolinium-based MRI showed an enhancement of the caudal nerve roots in two patients, enhancement of the facial nerve in one patient, and no signal change in nerves in two of them6.
Angiotensin-converting enzyme 2 (ACE-2) receptors have recently been identified as the site of entry into the cell by the SARS-CoV-2 virus7. These receptors are pres-ent in multiple organs such as the lung, the nervous sys-tem, and skeletal muscle, such that SARS-CoV-2 can cause neurological symptoms by direct or indirect mecha-nisms7-9. These receptors have been detected in glial cells and neurons, making it a potential target for SARS-CoV-28. The pathogenic mechanism for invading the central
nervous system of SARS-CoV-2 is suspected to be hema-togenous or the retrograde neuronal pathway2,7,8.
The proximity of the cribriform plate to the olfactory bulb could enable the SARS-CoV-2 virus to reach and inflict cerebral damage8. Therefore, changes in smell (hyposmia) could appear as an early symptom in the uncomplicated stage of COVID-194,8. Similarly, ACE-2 receptors are used by the SARS-Cov2 virus to pene-trate the epithelial cells of the mucosa of the oral cavity and on the tongue. These findings could explain the pathogenic mechanism in the alterations of taste and odor in SARS-CoV-2 infection10.
On March 11, 2020, the World Health Organization (WHO) declared the COVID-19 as a pandemic due to the exponential increase in cases outside of China, the number of countries affected, and the high mortality. To date, 2,319,066 confirmed cases had been reported in 213 countries, with 157,970 deaths worldwide11.
Humanity faces the most significant challenge in 100 years: the appearance of this new COVID-19 caused by a novel virus capable of affecting all the organs and systems, especially the lungs. Increasing evidence shows that SARS-CoV-2 may also invade the CNS and cause neurological manifestations. Damage to the nervous sys-tem can come in different forms and severity. Sudden loss of smell and taste as a symptom of infection should be further studied, as it could be a screening tool that con-tributes to early diagnosis and timely isolation. Innovating and learning about this disease is one of the critical areas to prevent infections, save lives, and hinder its effects.
References 1. Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, et al. Clinical features of
patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395:497-506.
2. Mao L, Wang M, Chen S, Jin H, Hu Y, He Q, et al. Neurologic manifes-tations of hospitalized patients with coronavirus disease 2019 in Wuhan, China. JAMA Neurol. 2020 [Epub ahead of print].
3. Guan W, Ni Z, Hu Y, Liang W, Ou C, He J, et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. 2020;382:1708-20.
4. Giacomelli A, Pezzati L, Conti F, Bernacchia D, Siano M, Oreni L, et al. Self-reported olfactory and taste disorders in SARS-CoV-2 patients: a cross-sectional study. Clin Infect Dis. 2020 [Epub ahead of print].
5. Helms J, Kremer S, Merdji H, Clere-Jehl R, Schenck M, Kummerlen C, et al. Neurologic features in severe SARS-CoV-2 infection. N Engl J Med. 2020 [Epub ahead of print].
6. Toscano G, Palmerini F, Ravaglia S, Ruiz L, Invernizzi P, Cuzzoni MG, et al. Guillain-Barré syndrome associated with SARS-CoV-2. N Engl J Med. 2020 [Epub ahead of print].
7. Wu Y, Xu X, Chen Z, Duan J, Hashimoto K, Yang L, et al. Nervous system involvement after infection with COVID-19 and other coronaviru-ses. Brain Behav Immun. 2020 [Epub ahead of print].
8. Baig AM, Khaleeq A, Ali U, Syeda H. Evidence of the COVID-19 virus targeting the CNS: tissue distribution, host-virus interaction, and propo-sed neurotropic mechanisms. ACS Chem Neurosci. 2020;11:995-8.
9. Li YC, Bai WZ, Hashikawa T. The neuroinvasive potential of SARS-CoV2 may play a role in the respiratory failure of COVID-19 patients. J Med Virol. 2020;92:552-5.
10. Xu H, Zhong L, Deng J, Peng J, Dan H, Zeng X, et al. High expression of ACE2 receptor of 2019-nCoV on the epithelial cells of oral mucosa. Int J Oral Sci. 2020;12:8.
11. Available from: https://www.who.int/emergencies/diseases/novel-corona-virus-2019 [Accessed Apr 22, 2020]..
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020
82
Preventive treatment in migraine. Used drugs and related variables. Results of the European work and migraine survey Ma. Teófila Vicente-Herrero1*, Ma. Victoria Ramírez-Iñiguez de la Torre1, Elena Ruíz-de la Torre2, and Luis Reinoso-Barbero3
1Occupational Medicine, Work Group for Guidelines and Protocols, Spanish Association of Specialists in Occupational Medicine, Madrid, Spain; 2Chairmanship, European Migraine and Headache Alliance, Brussels, Belgium; 3Occupational Medicine, Chairmanship, Spanish Association of Specialists in Occupational Medicine, Madrid, Spain
Revista Mexicana de Neurociencia
ORIGINAL ARTICLE
Correspondence: *Ma. Teófila Vicente-Herrero
E-mail: [email protected]
Available online: 18-05-2020
Rev Mex Neuroci. 2020;21(3):82-89
www.revmexneurociencia.com
Date of reception: 24-05-2019
Date of acceptance: 09-01-2020
DOI: 10.24875/RMN.20000089
1665-5044/ © 2020. Academia Mexicana de Neurología A.C. Published by Permanyer. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Abstract
Background: Migraine is a chronic debilitating and costly illness, the etiology of which is not yet fully known. Treatment is based on the control of acute attacks and the prophylactic management of chronic forms. Objective: The objective of this study is to find out the migraine preventive treatments which are used by patients in different countries in Europe, as well as observing the differences according to their social and demographic conditions. Methods: A cross-sectional observational study performed by means of an anonymous web-based survey of 3342 patients from Spain, Italy, France, Portugal, Ireland, United Kingdom, Germany, and other European Union (EU) countries. Study variables: Age, gender, country, type of town/city, level of studies completed, and rural or urban area have been dismissed. The different uses of preventive treatments are defined as: i always take preventive treatments, I take seasonal preventive treatments, I do not take preventive treat-ments, I do not know what a preventive treatment is. Results: The regular use of preventive treatments increases with age, their use is greater in patients over the age of 40 years (p < 0.0001), and they are most commonly used in Spain, Germany, United Kingdom, Italy, and in the rest of the countries in the EU (p < 0.0001). Out of all of the countries included in this sur-vey, Spain has the highest use of seasonal preventive medication (p < 0.0001). The lowest use of preventive treatments is in patients under the age of 40 years (p = 0.002) and in female patients (p = 0.028). The highest percentages of patients who do not use preventive treatments (p < 0.0001) are from Spain, Germany, and the rest of the countries in the EU. Young patients under the age of 40 years (p < 0.0001), patients in Spain, Germany, and the rest of the countries in the EU that were not included in the initial design (p < 0.0001) have the greatest lack of knowledge with regard to preventive treatments. Conclusions: The use of preventive pharmacological therapies in migraine remains low despite the fact that these therapies are scientifically backed. It is important to further develop the training of physicians and reinforce patient information, asses-sing patient preferences to improve their adherence to treatment.
Key words: Migraine. Preventive treatment. Public health.N
o p
art
of
this
pu
blic
atio
n m
ay b
e re
pro
du
ced
or
ph
oto
cop
yin
g w
ith
ou
t th
e p
rio
r w
ritt
en p
erm
issi
on
of
the
pu
blis
her
.
© P
erm
anye
r 20
20

83
M.T. Vicente-Herrero, et al.: Preventive treatment in migraine
In the last decade, migraine research has identified novel pharmacologic targets and therapies that represent great progress3. However, preventive treatments contin-ue to be underused, and this is due to significant factors, including adherence to treatment and patient preferenc-es. Adherence to therapy, though a key factor for suc-cessful treatment, is low among patients with chronic conditions such as migraines. Dose frequency plays a major role in adherence, as is having flexible dosing op-tions which allow for greater and better acceptance and adherence to treatment among adults with migraine4.
The objective of this study is to find out whether pre-ventive treatments are used by patients with migraine in different countries in Europe, as well as observing the differences according to their social and demo-graphic conditions, as by doing so it will be possible to contemplate more effective and targeted actions based on the results obtained.
Methods
A cross-sectional observational study performed by means of an anonymous web-based multiple-choice questionnaire with 32 questions, not validated, located on the European Migraine and Headache Alliance (EMHA)’s website, and scientifically backed by the Spanish Association of Specialists in Occupational
Introduction
Migraine is a debilitating and costly chronic illness, the etiology of which is not yet fully known; however, it is understood that it is partly attributable to genetically determined factors that play a relevant role. It is esti-mated that migraines affect 18% of women and 6% of men1.
Treatment is based on the control of acute attacks and the prophylactic management of chronic forms. This includes the use of different categories of medi-cation, although it has been demonstrated that not all subjects have the same clinical response to these forms of medication. The general picture is further ex-acerbated by the need for the frequent use of polyther-apy to treat comorbidities, which may interfere with the pharmacologic action of migraine medications, includ-ing both symptomatic and preventative treatments. The main objective of personalized medicine is to set opti-mal therapies in the light of the functional biochemical active substance and of the comorbidities of each in-dividual patient, to obtain the best clinical response. There are now novel therapeutic perspectives that have provided options for managing this pathology; nonethe-less, the pharmacologic interactions and their metabol-ic destiny must always be studied by the application of pharmacogenomics2.
Tratamiento preventivo en migraña. Fármacos usados y variables relacionadas. Resultados de la encuesta europea sobre trabajo y migraña
Resumen
Antecedentes: La migraña es un trastorno crónico incapacitante y costoso, cuya etiología aún no se conoce completamen-te; el tratamiento se basa en el control de los ataques agudos y el manejo profiláctico de las formas crónicas. Objetivo: El objetivo de este trabajo es descubrir el uso de tratamientos preventivos en pacientes con migraña de países europeos y las diferencias observadas según sus condiciones sociales y demográficas. Método: Estudio observacional transversal mediante encuesta web anónima a 3342 pacientes de España, Italia, Francia, Portugal, Irlanda, Reino Unido, Alemania y otros países de la Unión Europea (UE). Variables de estudio: edad, sexo, país, tipo de ubicación, nivel de estudios y área rural o urbana. Las opciones de uso de los tratamientos preventivos recopilados son: tratamientos preventivos siempre, tratamientos preventivos en temporadas, «no tomo tratamiento preventivo» y «no sé qué es un tratamiento preventivo». Resultados: El uso de tratamientos preventivos es superior en los mayores de 40 años (p < 0.0001), con la mayor utilización en España, Alemania, Reino Unido, Italia y el resto de los países de la UE no incluidos en el diseño inicial (p < 0.0001). España es el país con mayor uso de preventivos en temporadas (estacional) (p < 0.0001). El uso más bajo de tratamientos preventivos ocurre en personas menores de 40 años (p = 0.002) y en mujeres (p = 0.028). España, Alemania y el resto de los países de la UE tienen el mayor porcentaje de pacientes sin tratamiento preventivo (p < 0.0001). La mayor falta de conocimiento sobre los preventivos ocurre en pacientes con menos de 40 años de edad (p < 0.0001), en España, Alemania y el resto de los países de la UE no incluidos en el diseño inicial (p < 0.0001). Conclusiones: El uso de terapias farmacológicas preven-tivas en la migraña sigue siendo bajo a pesar de contar con respaldo científico. Es importante reforzar la capacitación del médico y la información al paciente, evaluando las preferencias del paciente para mejorar su adherencia al tratamiento.
Palabras clave: Migraña. Tratamiento preventivo. Salud pública.
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020
84
Rev Mex Neuroci. 2020;21(3)
Medicine (AEEMT). 3352 patients participated from Spain, Italy, France, Portugal, Ireland, United Kingdom, Germany, and other European Union (EU) countries which were not included in the initial study design and who responded to it. The inclusion criteria were that the patients must have been previously diagnosed with migraines, be working at the time of the questionnaire, or have been working in the previous year, and the patients had to participate voluntarily. The data were collected from September 2018 to January 2019.
Based on the initial description, the responses cor-responding to the management of the migraines were analyzed according to sociodemographic variables: age up to 20 years, between 21 and 40, between 41 and 60, more than 61; gender: man, and woman; place of residence: Spain, Italy, France, Portugal, Ireland, United Kingdom, Germany, and other country in the EU; type of town/city where they live: up to 500 inhab-itants, 501-10,000 inhabitants, 10,001-250,000 inhabi-tants, 250,001-1 million inhabitants, and more than a million inhabitants; level of studies completed: elemen-tary, intermediate, and higher; and environment in which they live: rural (town) and urban (capital).
The options for preventive treatment were defined by question 12 of the survey: i always take preventive treat-ment, I take seasonal preventive treatment, I always take several preventive treatments, I take several seasonal preventive treatments, I do not take preventive treat-ments, I do not know what a preventive treatment is.
Bivariate analysis was performed for each of the pro-posed options, as well as in relation to the different sociodemographic parameters.
Contingency tables were presented, which showed the absolute frequency (n) and the percentage (%) for each cross tab. Depending on the nature of the vari-ables in the survey (categorical variables), the Chi-squared test or Fisher’s exact test was used to analyze the possible relationship between the characteristics of the migraine and the sociodemographic variables.
The data for each of the possible answers were an-alyzed separately.
Results
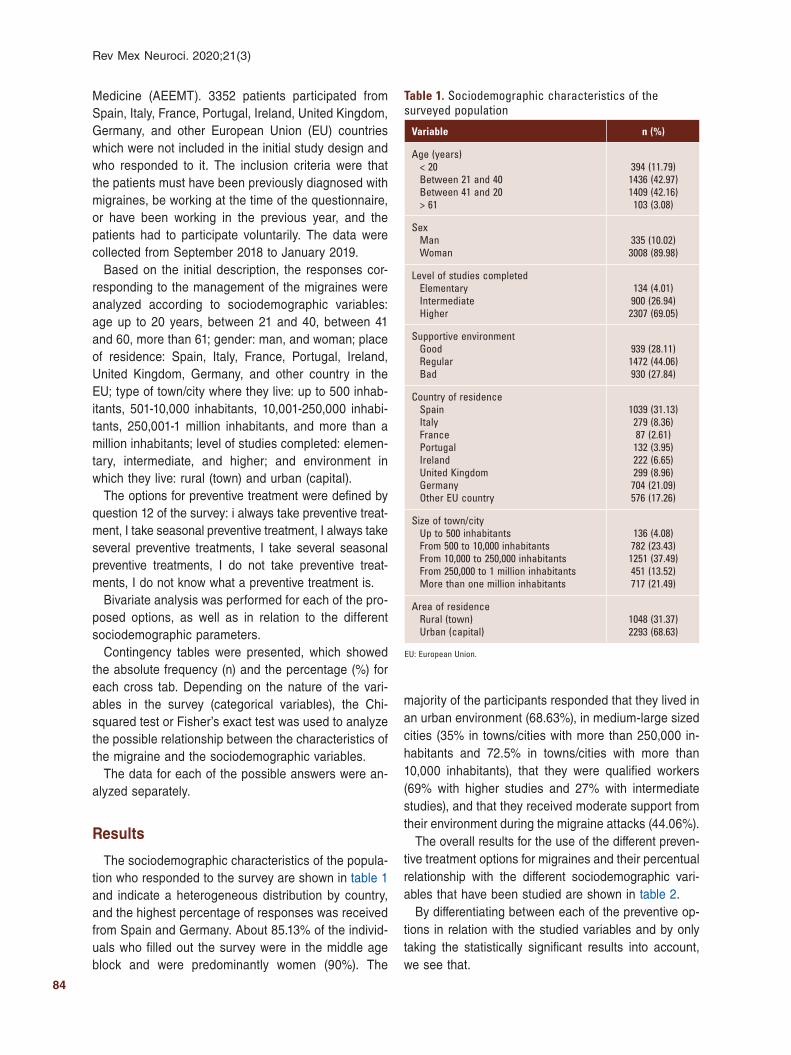
The sociodemographic characteristics of the popula-tion who responded to the survey are shown in table 1 and indicate a heterogeneous distribution by country, and the highest percentage of responses was received from Spain and Germany. About 85.13% of the individ-uals who filled out the survey were in the middle age block and were predominantly women (90%). The
majority of the participants responded that they lived in an urban environment (68.63%), in medium-large sized cities (35% in towns/cities with more than 250,000 in-habitants and 72.5% in towns/cities with more than 10,000 inhabitants), that they were qualified workers (69% with higher studies and 27% with intermediate studies), and that they received moderate support from their environment during the migraine attacks (44.06%).
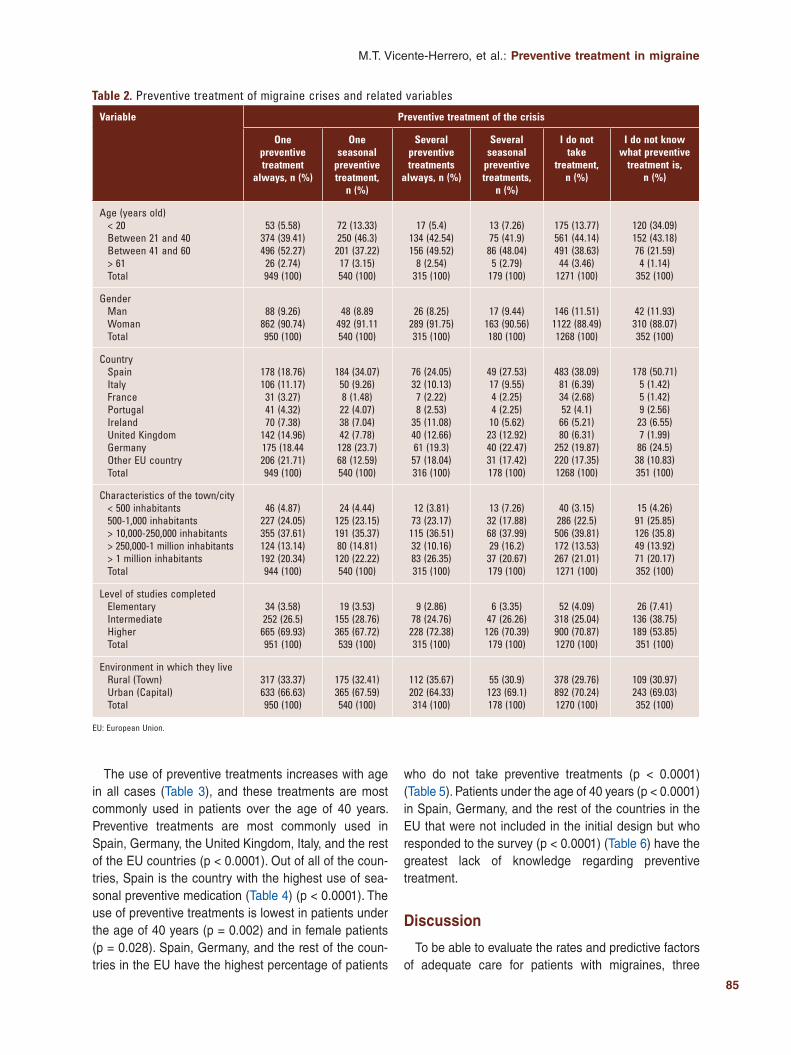
The overall results for the use of the different preven-tive treatment options for migraines and their percentual relationship with the different sociodemographic vari-ables that have been studied are shown in table 2.
By differentiating between each of the preventive op-tions in relation with the studied variables and by only taking the statistically significant results into account, we see that.
Table 1. Sociodemographic characteristics of the surveyed population
Variable n (%)
Age (years)< 20Between 21 and 40Between 41 and 20> 61
394 (11.79)1436 (42.97)1409 (42.16)
103 (3.08)
SexManWoman
335 (10.02)3008 (89.98)
Level of studies completedElementaryIntermediateHigher
134 (4.01)900 (26.94)
2307 (69.05)
Supportive environmentGoodRegularBad
939 (28.11)1472 (44.06)930 (27.84)
Country of residenceSpainItalyFrancePortugalIrelandUnited KingdomGermanyOther EU country
1039 (31.13)279 (8.36)87 (2.61)
132 (3.95)222 (6.65)299 (8.96)
704 (21.09)576 (17.26)
Size of town/cityUp to 500 inhabitantsFrom 500 to 10,000 inhabitantsFrom 10,000 to 250,000 inhabitantsFrom 250,000 to 1 million inhabitantsMore than one million inhabitants
136 (4.08)782 (23.43)
1251 (37.49)451 (13.52)717 (21.49)
Area of residenceRural (town)Urban (capital)
1048 (31.37)2293 (68.63)
EU: European Union.
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020
85
M.T. Vicente-Herrero, et al.: Preventive treatment in migraine
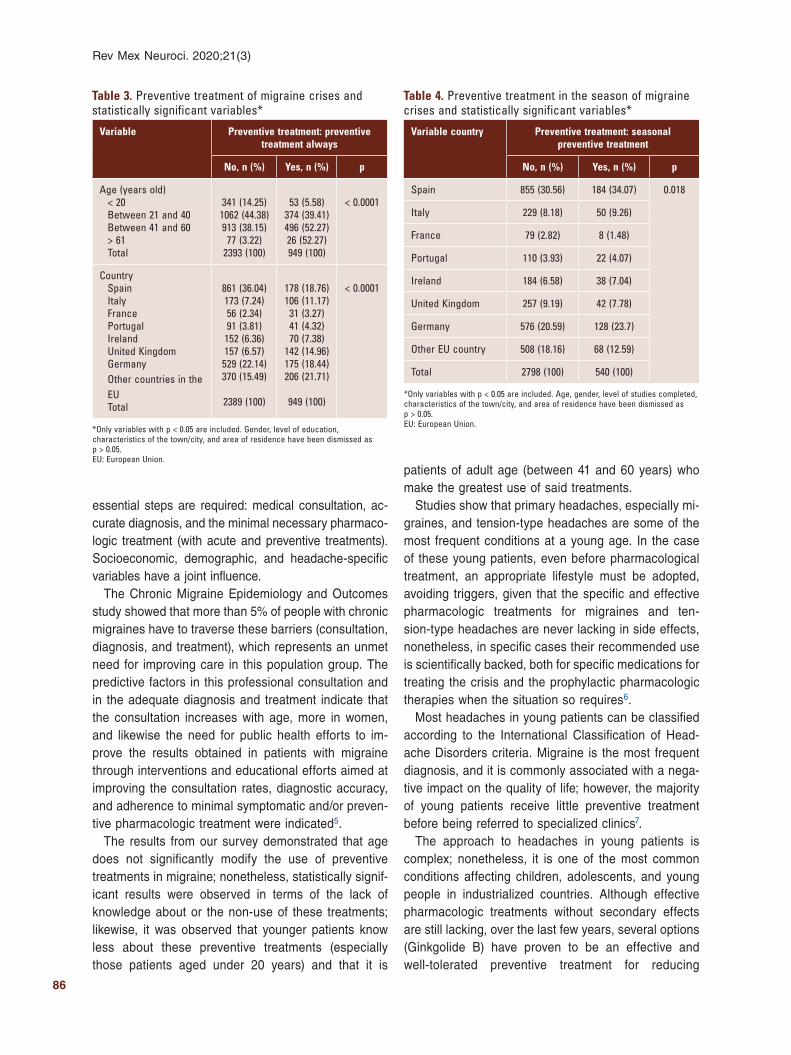
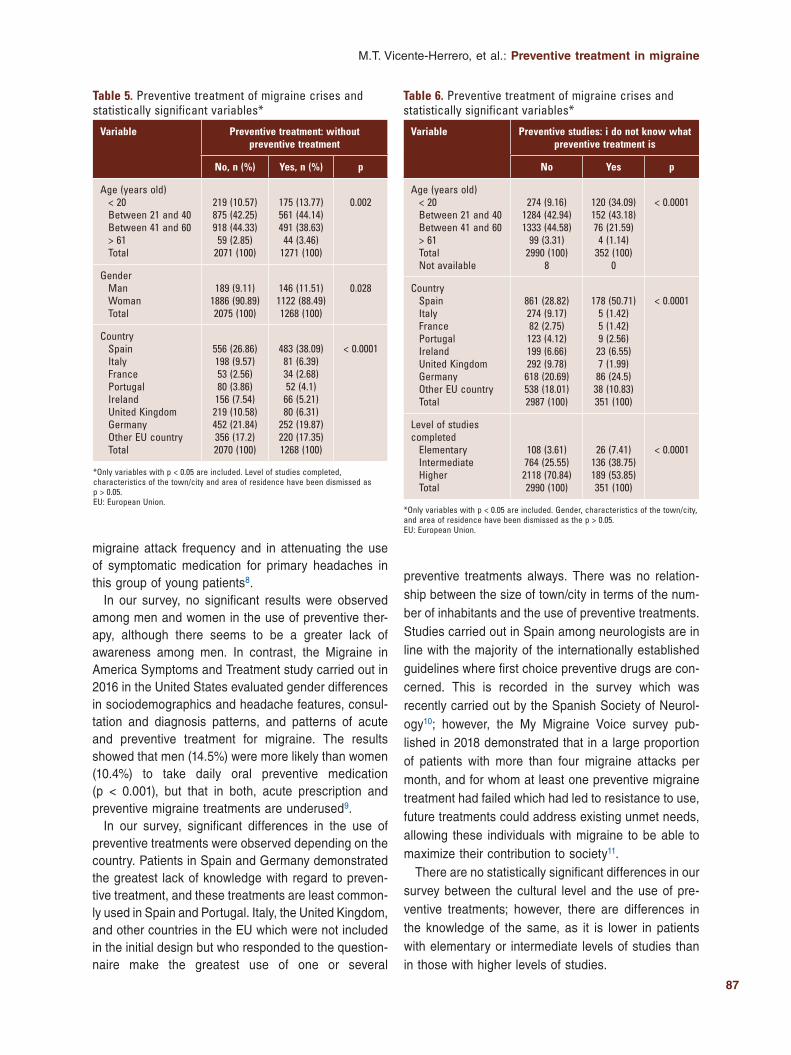
The use of preventive treatments increases with age in all cases (Table 3), and these treatments are most commonly used in patients over the age of 40 years. Preventive treatments are most commonly used in Spain, Germany, the United Kingdom, Italy, and the rest of the EU countries (p < 0.0001). Out of all of the coun-tries, Spain is the country with the highest use of sea-sonal preventive medication (Table 4) (p < 0.0001). The use of preventive treatments is lowest in patients under the age of 40 years (p = 0.002) and in female patients (p = 0.028). Spain, Germany, and the rest of the coun-tries in the EU have the highest percentage of patients
who do not take preventive treatments (p < 0.0001) (Table 5). Patients under the age of 40 years (p < 0.0001) in Spain, Germany, and the rest of the countries in the EU that were not included in the initial design but who responded to the survey (p < 0.0001) (Table 6) have the greatest lack of knowledge regarding preventive treatment.
Discussion
To be able to evaluate the rates and predictive factors of adequate care for patients with migraines, three
Table 2. Preventive treatment of migraine crises and related variables
Variable Preventive treatment of the crisis
One preventive treatment
always, n (%)
One seasonal
preventive treatment,
n (%)
Several preventive treatments
always, n (%)
Several seasonal
preventive treatments,
n (%)
I do not take
treatment, n (%)
I do not know what preventive
treatment is, n (%)
Age (years old)< 20Between 21 and 40Between 41 and 60> 61Total
53 (5.58)374 (39.41)496 (52.27)
26 (2.74)949 (100)
72 (13.33)250 (46.3)
201 (37.22)17 (3.15)540 (100)
17 (5.4)134 (42.54)156 (49.52)
8 (2.54)315 (100)
13 (7.26)75 (41.9)
86 (48.04)5 (2.79)
179 (100)
175 (13.77)561 (44.14)491 (38.63)
44 (3.46)1271 (100)
120 (34.09)152 (43.18)76 (21.59)
4 (1.14)352 (100)
GenderManWomanTotal
88 (9.26)862 (90.74)950 (100)
48 (8.89492 (91.11540 (100)
26 (8.25)289 (91.75)315 (100)
17 (9.44)163 (90.56)180 (100)
146 (11.51)1122 (88.49)1268 (100)
42 (11.93)310 (88.07)352 (100)
CountrySpainItalyFrancePortugalIrelandUnited KingdomGermanyOther EU countryTotal
178 (18.76)106 (11.17)
31 (3.27)41 (4.32)70 (7.38)
142 (14.96)175 (18.44206 (21.71)949 (100)
184 (34.07)50 (9.26)8 (1.48)
22 (4.07)38 (7.04)42 (7.78)
128 (23.7)68 (12.59)540 (100)
76 (24.05)32 (10.13)
7 (2.22)8 (2.53)
35 (11.08)40 (12.66)61 (19.3)
57 (18.04)316 (100)
49 (27.53)17 (9.55)4 (2.25)4 (2.25)
10 (5.62)23 (12.92)40 (22.47)31 (17.42)178 (100)
483 (38.09)81 (6.39)34 (2.68)52 (4.1)
66 (5.21)80 (6.31)
252 (19.87)220 (17.35)1268 (100)
178 (50.71)5 (1.42)5 (1.42)9 (2.56)
23 (6.55)7 (1.99)
86 (24.5)38 (10.83)351 (100)
Characteristics of the town/city< 500 inhabitants500-1,000 inhabitants > 10,000-250,000 inhabitants> 250,000-1 million inhabitants> 1 million inhabitantsTotal
46 (4.87)227 (24.05)355 (37.61)124 (13.14)192 (20.34)944 (100)
24 (4.44)125 (23.15)191 (35.37)80 (14.81)
120 (22.22)540 (100)
12 (3.81)73 (23.17)
115 (36.51)32 (10.16)83 (26.35)315 (100)
13 (7.26)32 (17.88)68 (37.99)29 (16.2)
37 (20.67)179 (100)
40 (3.15)286 (22.5)
506 (39.81)172 (13.53)267 (21.01)1271 (100)
15 (4.26)91 (25.85)126 (35.8)49 (13.92)71 (20.17)352 (100)
Level of studies completedElementaryIntermediateHigherTotal
34 (3.58)252 (26.5)
665 (69.93)951 (100)
19 (3.53)155 (28.76)365 (67.72)539 (100)
9 (2.86)78 (24.76)
228 (72.38)315 (100)
6 (3.35)47 (26.26)
126 (70.39)179 (100)
52 (4.09)318 (25.04)900 (70.87)1270 (100)
26 (7.41)136 (38.75)189 (53.85)351 (100)
Environment in which they liveRural (Town)Urban (Capital)Total
317 (33.37)633 (66.63)950 (100)
175 (32.41)365 (67.59)540 (100)
112 (35.67)202 (64.33)314 (100)
55 (30.9)123 (69.1)178 (100)
378 (29.76)892 (70.24)1270 (100)
109 (30.97)243 (69.03)352 (100)
EU: European Union.
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020
86
Rev Mex Neuroci. 2020;21(3)
essential steps are required: medical consultation, ac-curate diagnosis, and the minimal necessary pharmaco-logic treatment (with acute and preventive treatments). Socioeconomic, demographic, and headache-specific variables have a joint influence.
The Chronic Migraine Epidemiology and Outcomes study showed that more than 5% of people with chronic migraines have to traverse these barriers (consultation, diagnosis, and treatment), which represents an unmet need for improving care in this population group. The predictive factors in this professional consultation and in the adequate diagnosis and treatment indicate that the consultation increases with age, more in women, and likewise the need for public health efforts to im-prove the results obtained in patients with migraine through interventions and educational efforts aimed at improving the consultation rates, diagnostic accuracy, and adherence to minimal symptomatic and/or preven-tive pharmacologic treatment were indicated5.
The results from our survey demonstrated that age does not significantly modify the use of preventive treatments in migraine; nonetheless, statistically signif-icant results were observed in terms of the lack of knowledge about or the non-use of these treatments; likewise, it was observed that younger patients know less about these preventive treatments (especially those patients aged under 20 years) and that it is
patients of adult age (between 41 and 60 years) who make the greatest use of said treatments.
Studies show that primary headaches, especially mi-graines, and tension-type headaches are some of the most frequent conditions at a young age. In the case of these young patients, even before pharmacological treatment, an appropriate lifestyle must be adopted, avoiding triggers, given that the specific and effective pharmacologic treatments for migraines and ten-sion-type headaches are never lacking in side effects, nonetheless, in specific cases their recommended use is scientifically backed, both for specific medications for treating the crisis and the prophylactic pharmacologic therapies when the situation so requires6.
Most headaches in young patients can be classified according to the International Classification of Head-ache Disorders criteria. Migraine is the most frequent diagnosis, and it is commonly associated with a nega-tive impact on the quality of life; however, the majority of young patients receive little preventive treatment before being referred to specialized clinics7.
The approach to headaches in young patients is complex; nonetheless, it is one of the most common conditions affecting children, adolescents, and young people in industrialized countries. Although effective pharmacologic treatments without secondary effects are still lacking, over the last few years, several options (Ginkgolide B) have proven to be an effective and well-tolerated preventive treatment for reducing
Table 3. Preventive treatment of migraine crises and statistically significant variables*
Variable Preventive treatment: preventive treatment always
No, n (%) Yes, n (%) p
Age (years old)< 20Between 21 and 40Between 41 and 60> 61Total
341 (14.25)1062 (44.38)913 (38.15)
77 (3.22)2393 (100)
53 (5.58)374 (39.41)496 (52.27)26 (52.27)949 (100)
< 0.0001
CountrySpainItalyFrancePortugalIrelandUnited KingdomGermanyOther countries in the EUTotal
861 (36.04)173 (7.24)56 (2.34)91 (3.81)
152 (6.36)157 (6.57)
529 (22.14)370 (15.49)
2389 (100)
178 (18.76)106 (11.17)
31 (3.27)41 (4.32)70 (7.38)
142 (14.96)175 (18.44)206 (21.71)
949 (100)
< 0.0001
*Only variables with p < 0.05 are included. Gender, level of education, characteristics of the town/city, and area of residence have been dismissed as p > 0.05.EU: European Union.
Table 4. Preventive treatment in the season of migraine crises and statistically significant variables*
Variable country Preventive treatment: seasonal preventive treatment
No, n (%) Yes, n (%) p
Spain 855 (30.56) 184 (34.07) 0.018
Italy 229 (8.18) 50 (9.26)
France 79 (2.82) 8 (1.48)
Portugal 110 (3.93) 22 (4.07)
Ireland 184 (6.58) 38 (7.04)
United Kingdom 257 (9.19) 42 (7.78)
Germany 576 (20.59) 128 (23.7)
Other EU country 508 (18.16) 68 (12.59)
Total 2798 (100) 540 (100)
*Only variables with p < 0.05 are included. Age, gender, level of studies completed, characteristics of the town/city, and area of residence have been dismissed as p > 0.05.EU: European Union.
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020
87
M.T. Vicente-Herrero, et al.: Preventive treatment in migraine
migraine attack frequency and in attenuating the use of symptomatic medication for primary headaches in this group of young patients8.
In our survey, no significant results were observed among men and women in the use of preventive ther-apy, although there seems to be a greater lack of awareness among men. In contrast, the Migraine in America Symptoms and Treatment study carried out in 2016 in the United States evaluated gender differences in sociodemographics and headache features, consul-tation and diagnosis patterns, and patterns of acute and preventive treatment for migraine. The results showed that men (14.5%) were more likely than women (10.4%) to take daily oral preventive medication (p < 0.001), but that in both, acute prescription and preventive migraine treatments are underused9.
In our survey, significant differences in the use of preventive treatments were observed depending on the country. Patients in Spain and Germany demonstrated the greatest lack of knowledge with regard to preven-tive treatment, and these treatments are least common-ly used in Spain and Portugal. Italy, the United Kingdom, and other countries in the EU which were not included in the initial design but who responded to the question-naire make the greatest use of one or several
preventive treatments always. There was no relation-ship between the size of town/city in terms of the num-ber of inhabitants and the use of preventive treatments. Studies carried out in Spain among neurologists are in line with the majority of the internationally established guidelines where first choice preventive drugs are con-cerned. This is recorded in the survey which was recently carried out by the Spanish Society of Neurol-ogy10; however, the My Migraine Voice survey pub-lished in 2018 demonstrated that in a large proportion of patients with more than four migraine attacks per month, and for whom at least one preventive migraine treatment had failed which had led to resistance to use, future treatments could address existing unmet needs, allowing these individuals with migraine to be able to maximize their contribution to society11.
There are no statistically significant differences in our survey between the cultural level and the use of pre-ventive treatments; however, there are differences in the knowledge of the same, as it is lower in patients with elementary or intermediate levels of studies than in those with higher levels of studies.
Table 5. Preventive treatment of migraine crises and statistically significant variables*
Variable Preventive treatment: without preventive treatment
No, n (%) Yes, n (%) p
Age (years old)< 20Between 21 and 40Between 41 and 60> 61Total
219 (10.57)875 (42.25)918 (44.33)
59 (2.85)2071 (100)
175 (13.77)561 (44.14)491 (38.63)
44 (3.46)1271 (100)
0.002
GenderManWomanTotal
189 (9.11)1886 (90.89)2075 (100)
146 (11.51)1122 (88.49)1268 (100)
0.028
CountrySpainItalyFrancePortugalIrelandUnited KingdomGermanyOther EU countryTotal
556 (26.86)198 (9.57)53 (2.56)80 (3.86)
156 (7.54)219 (10.58)452 (21.84)356 (17.2)2070 (100)
483 (38.09)81 (6.39)34 (2.68)52 (4.1)
66 (5.21)80 (6.31)
252 (19.87)220 (17.35)1268 (100)
< 0.0001
*Only variables with p < 0.05 are included. Level of studies completed, characteristics of the town/city and area of residence have been dismissed as p > 0.05.EU: European Union.
Table 6. Preventive treatment of migraine crises and statistically significant variables*
Variable Preventive studies: i do not know what preventive treatment is
No Yes p
Age (years old)< 20Between 21 and 40Between 41 and 60> 61TotalNot available
274 (9.16)1284 (42.94)1333 (44.58)
99 (3.31)2990 (100)
8
120 (34.09)152 (43.18)76 (21.59)
4 (1.14)352 (100)
0
< 0.0001
CountrySpainItalyFrancePortugalIrelandUnited KingdomGermanyOther EU countryTotal
861 (28.82)274 (9.17)82 (2.75)
123 (4.12)199 (6.66)292 (9.78)
618 (20.69)538 (18.01)2987 (100)
178 (50.71)5 (1.42)5 (1.42)9 (2.56)
23 (6.55)7 (1.99)
86 (24.5)38 (10.83)351 (100)
< 0.0001
Level of studies completed
ElementaryIntermediateHigherTotal
108 (3.61)764 (25.55)
2118 (70.84)2990 (100)
26 (7.41)136 (38.75)189 (53.85)351 (100)
< 0.0001
*Only variables with p < 0.05 are included. Gender, characteristics of the town/city, and area of residence have been dismissed as the p > 0.05.EU: European Union.
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

88
Rev Mex Neuroci. 2020;21(3)
With regard to the environment in which they live, our results do not show any relationship between this and the use or knowledge of these preventive treatments; however, prior systematic reviews of the global preva-lence of migraine at the community level (302 studies which included 6,216,995 participants) showed that mi-graine affects one in ten people worldwide, with higher prevalence among women, among young people, and among urban residents in comparison with those living in a rural environments (11.2% among urban residents and 8.4% among rural residents)12.
The results of our survey confirm the scarce use and knowledge of preventive treatments in migraine as con-firmed by prior studies despite the scientific evidence that supports their use adjusted to international criteria. The American Academy of Neurology and the Canadian Headache Society have published evidence-based guidelines for preventive pharmacologic treatments for migraines that provide valuable guidance for clinicians; however, these pharmacologic therapies continue to be underused in clinical practice. The primary objective of these guidelines is to assist the practitioner in choosing an appropriate prophylactic medication for a person with migraine, based on current evidence in the medical lit-erature and expert consensus. These guidelines are focused on patients with episodic migraine (headache on ≤ 14 days a month) and there is good evidence from randomized controlled trials for the use of a number of different prophylactic medications in patients with migraines.
Medication choice for an individual patient requires careful consideration of patient clinical features13.
The principles of preventive treatment are important to improve compliance, minimize side effects, and im-prove patient outcomes. The choice of treatment should be based on the presence of comorbid and coexistent illness, patient preference, reproductive potential, and best available evidence14. The route of administration and preventive treatment-related adverse events has an impact on patient preference and their adherence to treatment15,16. Current treatment options for migraine prophylaxis are associated with poor tolerability and low adhesion and persistence, with an irregular course, frequent gaps, and discontinued prophylaxis by the end of the 1st year17. Persistence to oral preventive treat-ments is poor at 6 months and declines further by 12 months. Switching between treatments is common, but persistence worsens as patients cycle through var-ious preventive treatments18.
Scientific evidence supports the fact that preventive treatment is an important part of migraine therapy.
When prescribing medications, physicians should un-derstand patient’s preferences and select drugs that most closely meet their needs. Understanding the fac-tors that influence these preferences increases physi-cians’ ability to select appropriate migraine therapy. The results of patient surveys indicate that patients rated efficacy as the most important aspect of preventive therapy of migraine19. In addition to the functional im-pact of migraine, the decision to start prophylaxis is based on a complex of considerations from the patient’s perspective (e.g., perceived burden of migraine, expect-ed benefits or disadvantages, interaction with relatives, colleagues, and physician), therefore, when advising migraine patients about prophylaxis, their opinions should be taken into account. Patients need to be open to advice and information and intervention have to be offered at an appropriate moment in the course of migraine20.
The biases of this study include the use of a non-val-idated survey, the subjectivity of the responses, the greater participation by women, the non-uniform distri-bution of participants by countries, with greater partic-ipation from Spain and Germany, and the inclusion of respondent patients from countries that were not con-templated in the initial design.
The sample size and the comparative study by Eu-ropean countries are considered the strengths of this study, as well as the social and demographic variables that have been incorporated.
Conclusions
The use of preventive treatments increases with age, and the use of these treatments is greater in patients over the age of 40 years. The greatest lack of knowl-edge was observed among patients under the age of 40 years.
No relationship has been observed between the use of preventive treatments in migraine and the size of their place of residence or whether they live in a rural or urban area.
Knowledge of preventive treatments is lower in indi-viduals with elementary or intermediate studies than in those with higher studies.
The greatest use of regular preventive treatments is in Spain, Germany, the United Kingdom, and Italy.
Spain and Germany have the greatest percentage of patients who do not take treatment or who do not know about preventive treatments.
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020
89
M.T. Vicente-Herrero, et al.: Preventive treatment in migraine
The use of preventive pharmacologic therapies in migraine remains low despite the fact that it is scientif-ically backed.
It is important to further develop the training of physi-cians and reinforce patient information, assessing patient preferences to improve their adherence to treatment.
Acknowledgments
We are grateful to the European Migraine and Head-ache Alliance (EMHA) patients for their voluntary col-laboration in this survey, to the Spanish Association of Specialists in Occupational Medicine for its scientific support and backing, and to Silvia Lladosa for the sta-tistical study of the data.
Funding
This work has been funded by the EMHA.
Conflicts of interest
There are no conflicts of interest in this work.
Ethical disclosures
Protection of human and animal subjects. The authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of data. The authors declare that no patient data appear in this article.
Right to privacy and informed consent. The au-thors declare that no patient data appear in this article.
References 1. Harmon TP. Diagnosis and management of migraines and migraine va-
riants. Prim Care. 2015;42:233-41. 2. Pomes LM, Guglielmetti M, Bertamino E, Simmaco M, Borro M, Marte-
lletti P. Optimising migraine treatment: from drug-drug interactions to personalized medicine. J Headache Pain. 2019;20:56.
3. Do TP, Guo S, Ashina M. Therapeutic novelties in migraine: new drugs, new hope? J Headache Pain. 2019;20:37.
4. Cowan R, Cohen JM, Rosenman E, Iyer R. Physician and patient preferen-ces for dosing options in migraine prevention. J Headache Pain. 2019;20:50.
5. Dodick DW, Loder EW, Manack Adams A, Buse DC, Fanning KM, Reed ML, et al. Assessing barriers to chronic migraine consultation, diagnosis, and treatment: results from the chronic migraine epidemiology and outcomes (CaMEO) study. Headache. 2016;56:821-34.
6. Usai S, Grazzi L, Bussone G. Gingkolide B as migraine preventive treat-ment in young age: results at 1-year follow-up. Neurol Sci. 2011;32 Su-ppl 1:S197-9.
7. Pedraza Hueso MI, Ruíz Piñero M, Martínez Velasco E, Juanatey Gar-cía A, Guerrero Peral AL. Headache in young patients: clinical charac-teristics of a series of 651 cases. Neurologia. 2019;34:22-6.
8. Usai S, Grazzi L, Andrasik F, Bussone G. An innovative approach for migraine prevention in young age: a preliminary study. Neurol Sci. 2010;31 Suppl 1:S181-3.
9. Lipton RB, Munjal S, Alam A, Buse DC, Fanning KM, Reed ML, et al. Migraine in America symptoms and treatment (MAST) study: baseline study methods, treatment patterns, and gender differences. Headache. 2018;58:1408-26.
10. García-Azorin D, Santos-Lasaosa S, Gago-Veiga AB, Romero JV, Gue-rrero-Peral AL. Real world preventative drug management of migraine among Spanish neurologists. J Headache Pain. 2019;20:19.
11. Martelletti P, Schwedt TJ, Lanteri-Minet M, Quintana R, Carboni V, Die-ner HC, et al. My migraine voice survey: a global study of disease burden among individuals with migraine for whom preventive treatments have failed. J Headache Pain. 2018;19:115.
12. Woldeamanuel YW, Cowan RP. Migraine affects 1 in 10 people worldwide featuring recent rise: a systematic review and meta-analysis of community-ba-sed studies involving 6 million participants. J Neurol Sci. 2017;372:307-15.
13. Pringsheim T, Davenport W, Mackie G, Worthington I, Aubé M, Chris-tie SN, et al. Canadian headache society guideline for migraine pro-phylaxis. Can J Neurol Sci. 2012;39:S1-59.
14. Silberstein SD. Preventive migraine treatment. Continuum (Minneap Minn). 2015;21:973-89.
15. Matza LS, Deger KA, Vo P, Maniyar F, Goadsby PJ. Health state utilities associated with attributes of migraine preventive treatments based on pa-tient and general population preferences. Qual Life Res. 2019;28:2359-72.
16. Seng EK, Rains JA, Nicholson RA, Lipton RB. Improving medication adherence in migraine treatment. Curr Pain Headache Rep. 2015;19:24.
17. Woolley JM, Bonafede MM, Maiese BA, Lenz RA. Migraine prophylaxis and acute treatment patterns among commercially insured patients in the United States. Headache. 2017;57:1399-408.
18. Hepp Z, Dodick DW, Varon SF, Chia J, Matthew N, Gillard P, et al. Persistence and switching patterns of oral migraine prophylactic medica-tions among patients with chronic migraine: a retrospective claims analy-sis. Cephalalgia. 2017;37:470-85.
19. Peres MF, Silberstein S, Moreira F, Corchs F, Vieira DS, Abraham N, et al. Patients’ preference for migraine preventive therapy. Headache. 2007;47:540-5.
20. Dekker F, Knuistingh Neven A, Andriesse B, Kernick D, Reis R, Ferra-ri MD, et al. Prophylactic treatment of migraine; the patient’s view, a qualitative study. BMC Fam Pract. 2012;13:13.
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020
90
Executive dysfunction in middle-aged hypertensive adultsEdwin J. Palma-Díaz1, Damaris F. Estrella-Castillo2, Rita E. Zapata-Vázquez3, Edgar García-Santamaría4, and Héctor A. Rubio Zapata3*1Social Insertion Unit; 2University Rehabilitation Unit; 3Clinical and Epidemiological Research Unit; 4Physiological Science Department. School of Medicine, Autonomous University of Yucatán, Yucatán, Mexico
Revista Mexicana de Neurociencia
ORIGINAL ARTICLE
Abstract
Objective: The objective was to compare the executive functions between hypertensive and non-hypertensive middle-aged Mexican adults. Methods: An observational and analytic study was designed. Participants were men and women residents of Southeastern Mexico, aged between 40 and 60 years, with at least 5 years of hypertension diagnosis. The control group was people without hypertension. All participants completed a digit symbol substitution test (DSST), clinical and epidemio-logical data. Statistical analysis unpaired Student’s t-test, p < 0.05. Results: DSST score in control men was 37.78 ± 11.94, control women: 42.96 ± 11.19, hypertensive men: 16.81 ± 9.82, and hypertensive women: 26.88 ± 12.04. Significant differen-ces were found between hypertensive and non-hypertensive groups. Men had worse scores than women. No difference between normotensive men and women. Inverse correlation was found between DSST score and age, values of systolic and diastolic blood tension in the hypertension group. Conclusion: Hypertension decreases the executive function in middle-aged people, mainly in men. This dysfunction could be an early indicator of brain deterioration.
Key words: Hypertension. Executive cognitive function. Mature age. Brain dysfunction.
Disfunción ejecutiva en adultos hipertensos de edad madura
Resumen
Objetivo: comparar la función ejecutiva entre adultos mexicanos de mediana edad, hipertensos y no hipertensos. Métodos: se diseñó un estudio observacional y analítico. Los participantes eran hombres y mujeres residentes del sureste de México, con edades comprendidas entre 40 y 60 años y al menos cinco años de diagnóstico de hipertensión. Los con-troles fueron personas sin hipertensión. Todos los participantes completaron la prueba de Sustitución de Símbolo y Dígitos (DSST), datos clínicos y epidemiológicos. Análisis estadístico t-Student no pareada, p < 0.05. Resultados: la puntuación DSST en los hombres control fue de 37.78 ± 11.94 y las mujeres control: 42.96 ± 11.19, los hombres hipertensos: 16.81 ± 9.82 y las mujeres hipertensas: 26.88 ± 12.04. Se encontraron diferencias significativas entre el grupo hipertenso y no hipertenso. Los hombres tuvieron peores puntajes que las mujeres. No hay diferencia entre hombres y mujeres normotensos. Se encontró correlación inversa entre la puntuación DSST y la edad, los valores de tensión arterial sistólica y diastólica en el grupo con
Correspondence: *Héctor Armando Rubio Zapata
Clinical and Epidemiological Research Unit
School of Medicine, Autonomous University of
Yucatán Yucatán, Mexico
E-mail: [email protected]
Available online: 18-05-2020
Rev Mex Neuroci. 2020;21(3):90-96
www.revmexneurociencia.com
Date of reception: 10-09-2019
Date of acceptance: 16-01-2020
DOI: 10.24875/RMN.20000126
1665-5044/ © 2020. Academia Mexicana de Neurología A.C. Published by Permanyer. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

91
E.J. Palma-Díaz, et al.: Executive dysfunction in hypertensive adults
Introduction
According to the National Health Survey (ENSANUT MC) 2016, 25.5% of Mexican adults have hyperten-sion1,2. Hypertension causes functional and structural alterations in blood vessels, especially affecting arter-ies of medium and small caliber, which predominate in some organs like brain3. Several studies have estab-lished a causal relationship between hypertension and brain diseases such as stroke, vascular dementia, and recently Alzheimer’s disease4. Due to factors that are not yet completely clear, vascular damage induced by hypertension seems to be more aggressive in the fron-tal lobe, which could lead to executive dysfunction5.
Executive functions refer to a collection of cognitive abilities that enable and drive adaptive, goal-oriented behavior. These include the ability to generate thought and think flexibly, to update and manipulate information mentally, to inhibit what is irrelevant to current goals, to self-monitor, and to plan and adjust behavior as appropriate to the present context. Executive dysfunc-tion impairs efficient performing of daily activities and increases the risk of morbidity and mortality by acci-dents inside and outside the home, increases depen-dence on caregivers, limits productive activities, and reduces quality of life6,7. Chronicity and aging can worsen brain damage caused by hypertension8. Exec-utive dysfunction may be one of the first manifestations of brain damage9, especially in patients who do not achieve control despite consuming pharmacological treatment10.
In most cases, brain damage is irreversible6, so it is an important early diagnosis. Young and middle-aged hypertensive people usually have not symptoms of a cognitive impairment, however, there are standardized tools to evaluate the executive function11. The aim of this study was to compare the executive cognitive func-tion in middle-aged hypertensive and no hypertensive Mexican adults and related with some epidemiological data.
Methods
It is an observational and analytical study.Patients were recruited at the Unit of Social Insertion
(UUIS) of University of Yucatán, México. This institution
provides medical care to approximately 1179 users annually. The sample size was non-probabilistic and included all patients with and without hypertension, men and women from 41 to 60 years, with and without diagnosis of hypertension, and with minimum second-ary schooling who attended the external consultation from October 2018 to December 2018. All selected patients with hypertension had at least 5 years of diag-nosis to ensure chronicity period. To avoid biases on interpretation of cognitive function, results were exclud-ed patients with a history of cerebral vascular event, known brain diseases, with obesity (body mass index [BMI] > 30), dyslipidemias, and hypo or hyperthyroid-ism. Motor, visual or auditory dysfunction, or under neurological or psychiatric treatment were not included in the study. Ninety-two people agreed to participate and met the selection criteria.
We eliminated patients who at the time of the evalu-ation had mild cognitive deterioration and/or depressive symptomatology. Seven people were eliminated due to symptoms of depression and/or cognitive impairment.Forty-one hypertensive and 44 normotensive patients were included in final analysis.
Procedures
A physician in a clinic room evaluated patients, during the morning (8-10 am). A brief clinical history was com-plete emphasizing aspects related to hypertension, time of hypertension evolution, type of treatment it car-ries, drugs, doses, and achievement of therapeutic goal. All participants in fasting were weighed and mea-sured, without shoes, trousers or skirts, and shirt or blouse. The patients were weighed and measured with Detecto® brand stadiometer and scale; with these val-ues, the BMI was determined, according to the follow-ing formula: weight (Kg)/Size (M2).
Blood pressure (BP) was determined with a Check-ATeK® Baumanometer calibrated according to the official Mexican standard NOM-009-SCFI-1993 with the technique and specifications indicated by NOM-030-SSA2-201712. It was considerate as therapeutic goal if patient at time of measurement systolic BP (SBP) < 140 mmHg and diastolic < 90 mmHg. If in the past 3 months, average arterial BP would not
hipertensión. Conclusión: la hipertensión disminuye la función ejecutiva en personas de mediana edad, principalmente en hombres. Esta disfunción podría ser un indicador temprano de deterioro cerebral.
Palabras clave: Hipertensión. Función cognitiva ejecutiva. Edad madura. Disfunción cerebral.
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

92
Rev Mex Neuroci. 2020;21(3)
have exceeded reference values (taken from the clin-ical record), patients were considerate controlled.
Questionnaires
1. Digit symbol substitution test (DSST) evaluates the working memory, organization of perceived stimuli, visomotor coordination, and selective attention, which are executive cognitive functions. DSST was validated in Europe and the United States, mainly in the older adult population. Due to its iconographic nature, no linguistic translation is required, and the test has been used and validated in multiple contexts, regions, and languages, including Spanish and Mexican popula-tion13-15. All participants were explained how to re-spond and used as an example the first 10 boxes with their respective symbols to ensure that patient under-stood how to perform the test. Participant had to match numbers with their respective symbol in order and without skipping any box, as fast as possible and without any kind of external help. Test had a total duration of 90 s (in triplicate). The number of binomi-als number-symbol paired correctly constituted score of the participant in the DSST. Blank space between two completed items does not invalidate the test; how-ever, two or more consecutive blank spaces point to the end of the test. Paired symbols after two or more blank spaces are not considered in total score. DSST has no cutting points, score constitutes a continuous variable and has no individual value; it takes utility at population level when different groups are compared and is also useful when applied in the same individual overtime. Score reflects the speed of information pro-cessing as an executive function, and in comparison with other cognitive tests, DSST performance is strongly correlated with the volume of the prefrontal cortex16.
2. Mini-mental state examination (MMSE): this is widely validated tool, values in < 10 min cognitive state ex-amining functions such as the ability to record, atten-tion, calculus, memory, language, ability to follow simple instructions, and guidance. MMSE is used primarily to detect patients with mild cognitive impair-ment and other more severe forms of cognitive deterioration. Cutting point < 25 was an elimination criterion17.
3. Beck-II depression inventory (BDI-II): BDI-II requires 5-10 min to be completed and it explores data of major depression in the past 2 weeks, consistent with DSM-5 criteria. Depression has significant repercussions on global cognitive function and can
affect test results such as DSST, so score > 19 (of a maximum of 63) was an elimination criterion18.The procedures were the same for the control group
(not hypertensive), only the interrogation on arterial hypertension was excluded from the study.
Ethical considerations
The study was carried out in accordance with the provisions of the General Law on Health in the field of research, Mexican Secretariat of Health 1987. Ethical principles of the Helsinki World Medical Assembly and The International Code of Medical Ethics, as well as the provisions and Guidelines of the National Bioethics Commission (Conbioetica) 2016, were attended too. The project was evaluated and approved by the Ethics and Research Committee of the UUIS of the Autono-mous University of Yucatán.
Statistical analysis
It was carried out with the statistical program Graph-Pad Prism 7®. The normality of the data was deter-mined with the Shapiro-Wilk test. We compared the values of the scores of DSST with values of BP, age, duration of hypertension, using Student’s t-test for un-related samples. For variables: sex, therapeutic status, and Chi-square test were used. Linear correlation was performed with hypertension length, age, SBP, and diastolic blood pressure (DBP) related to the DSST score. The statistical significance was 95%, p < 0.05.
Results
The results presented below correspond to 85 adults. Table 1 describes its main characteristics, grouped as a control group (not hypertensive) and hypertension group.
We found similar distribution of sex, age and BMI in both groups.
There were no differences in BP between men and women, neither in the hypertension group nor in the control group. DSST values in the hypertension group were lower than the control group. Hypertensive men performed less than women did (p = 0.007). In the control group, there was no sex difference (p = 0.15).
Diagnostic average duration in the hypertension group was 11.9 ± 5 years, on men was 11.31 ± 5.5 years and woman 12.28 ± 4.7 (p = 0.55). Most hypertensive patients (82.9%) were receiving some form of pharma-cological treatment, 17% of patients had abandoned
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020
93
E.J. Palma-Díaz, et al.: Executive dysfunction in hypertensive adults
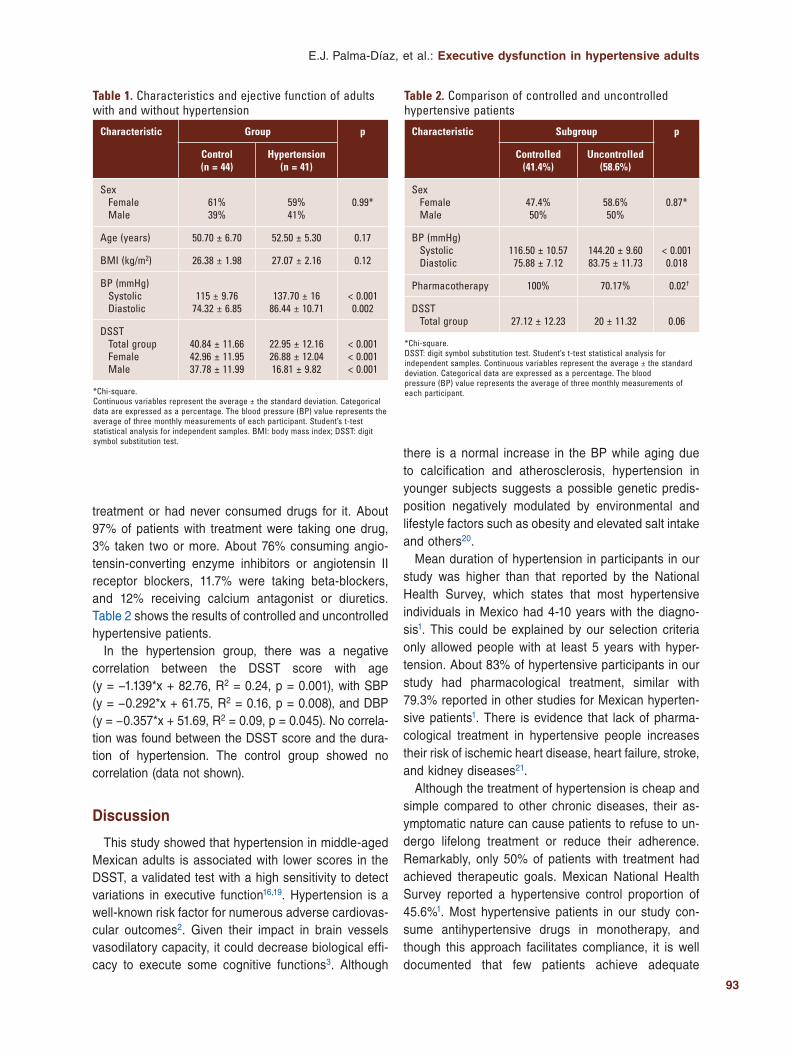
treatment or had never consumed drugs for it. About 97% of patients with treatment were taking one drug, 3% taken two or more. About 76% consuming angio-tensin-converting enzyme inhibitors or angiotensin II receptor blockers, 11.7% were taking beta-blockers, and 12% receiving calcium antagonist or diuretics. Table 2 shows the results of controlled and uncontrolled hypertensive patients.
In the hypertension group, there was a negative correlation between the DSST score with age (y = −1.139*x + 82.76, R2 = 0.24, p = 0.001), with SBP (y = −0.292*x + 61.75, R2 = 0.16, p = 0.008), and DBP (y = −0.357*x + 51.69, R2 = 0.09, p = 0.045). No correla-tion was found between the DSST score and the dura-tion of hypertension. The control group showed no correlation (data not shown).
Discussion
This study showed that hypertension in middle-aged Mexican adults is associated with lower scores in the DSST, a validated test with a high sensitivity to detect variations in executive function16,19. Hypertension is a well-known risk factor for numerous adverse cardiovas-cular outcomes2. Given their impact in brain vessels vasodilatory capacity, it could decrease biological effi-cacy to execute some cognitive functions3. Although
there is a normal increase in the BP while aging due to calcification and atherosclerosis, hypertension in younger subjects suggests a possible genetic predis-position negatively modulated by environmental and lifestyle factors such as obesity and elevated salt intake and others20.
Mean duration of hypertension in participants in our study was higher than that reported by the National Health Survey, which states that most hypertensive individuals in Mexico had 4-10 years with the diagno-sis1. This could be explained by our selection criteria only allowed people with at least 5 years with hyper-tension. About 83% of hypertensive participants in our study had pharmacological treatment, similar with 79.3% reported in other studies for Mexican hyperten-sive patients1. There is evidence that lack of pharma-cological treatment in hypertensive people increases their risk of ischemic heart disease, heart failure, stroke, and kidney diseases21.
Although the treatment of hypertension is cheap and simple compared to other chronic diseases, their as-ymptomatic nature can cause patients to refuse to un-dergo lifelong treatment or reduce their adherence. Remarkably, only 50% of patients with treatment had achieved therapeutic goals. Mexican National Health Survey reported a hypertensive control proportion of 45.6%1. Most hypertensive patients in our study con-sume antihypertensive drugs in monotherapy, and though this approach facilitates compliance, it is well documented that few patients achieve adequate
Table 1. Characteristics and ejective function of adults with and without hypertension
Characteristic Group p
Control (n = 44)
Hypertension (n = 41)
SexFemaleMale
61%39%
59%41%
0.99*
Age (years) 50.70 ± 6.70 52.50 ± 5.30 0.17
BMI (kg/m2) 26.38 ± 1.98 27.07 ± 2.16 0.12
BP (mmHg)Systolic Diastolic
115 ± 9.7674.32 ± 6.85
137.70 ± 1686.44 ± 10.71
< 0.0010.002
DSSTTotal groupFemaleMale
40.84 ± 11.6642.96 ± 11.9537.78 ± 11.99
22.95 ± 12.1626.88 ± 12.0416.81 ± 9.82
< 0.001< 0.001< 0.001
*Chi-square.Continuous variables represent the average ± the standard deviation. Categorical data are expressed as a percentage. The blood pressure (BP) value represents the average of three monthly measurements of each participant. Student’s t-test statistical analysis for independent samples. BMI: body mass index; DSST: digit symbol substitution test.
Table 2. Comparison of controlled and uncontrolled hypertensive patients
Characteristic Subgroup p
Controlled (41.4%)
Uncontrolled (58.6%)
SexFemaleMale
47.4%50%
58.6%50%
0.87*
BP (mmHg)Systolic Diastolic
116.50 ± 10.5775.88 ± 7.12
144.20 ± 9.6083.75 ± 11.73
< 0.0010.018
Pharmacotherapy 100% 70.17% 0.02†
DSSTTotal group 27.12 ± 12.23 20 ± 11.32 0.06
*Chi-square.DSST: digit symbol substitution test. Student’s t-test statistical analysis for independent samples. Continuous variables represent the average ± the standard deviation. Categorical data are expressed as a percentage. The blood pressure (BP) value represents the average of three monthly measurements of each participant.
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

94
Rev Mex Neuroci. 2020;21(3)
hypertensive control without two or more drugs22,23. We observed an important number of patients receiving beta-blockers, which, according to recent guidelines should not be used as first choice antihypertensive drugs because they promote the development of dys-lipidemias, impair glucose tolerance and hinder weight reduction23,24. It is important to analyze individual pa-tient conditions to offer the best treatment in each case and achieve therapeutic goals.
Our findings show that hypertensive patients have a worse performance in the DSST compared with normotensive people. Cognitive impairment is a grad-ual process and having hypertension could accelerate this process. Controversial results of the effect of hypertension on cognitive function have been found24,25. In our study, SBP was responsible for 16% of the variance in DSST scores in the hypertensive patients.
Some studies have found a better executive perfor-mance in men26; however, we found that men hyper-tensive obtained lower scores in DSST compared with woman hypertensive or normotensive people. There is evidence that in women, prenatal exposition to different hormonal concentrations promotes the overdevelop-ment of specific neuronal pathways and the neurotroph-ic effects of estrogens are well described27. The patients in this study were around 50 years old, so the women were in the menopausal period; consequently, it is likely that they maintained some degree of neuro-trophic estrogenic stimulation and better cerebral blood flow compared to man28.
The mechanisms that regulate arterial BP are similar in men and women; however, there are phys-iological differences at the molecular, cellular, and tissue levels between the sexes that contribute to differences in disease onset, susceptibility, preva-lence, and treatment responses. The sympathetic nervous system, the renin-angiotensin-aldosterone system, and the immune system are differentially activated in males and females. Sex hormones such as estrogens or testosterone as well as sex chromo-some complement likely contribute to sex differences in BP and cardiovascular disease. At the cellular level, differences in cell senescence pathways may contribute to increased longevity in women and may limit brain damage caused by hypertension29. There-fore, this may be an explanation because the women in our study were less affected in their executive function. In addition, many lifestyles and environmen-tal factors such as smoking, alcohol consumption, and diet, they are usually different in men and
women, as well as their possible effect on BP and brain function, were not evaluated in the present study.
SBP and DBP were higher than those reported in the previous studies in Mexico1, and higher BP readings were correlated with lower DSST scores. Uncontrolled hypertension increases vascular stiffness which rises pulse pressure. Increased BP is a risk factor for white matter lesions and subclinical hemorrhages that can cause cognitive alterations30. In concordance with other authors31, we could not find differences in executive function between controlled or uncontrolled hyperten-sive patients, maybe due to the small sample size. Several studies have reported that an elevated BP during middle age predicts cognitive impairment 20-30 years later32,33 and SBP control since middle age reduces this risk27,34.
Many studies have reported intense prefrontal acti-vation during DSST resolution using functional MRI and electroencephalography35,36, these areas are par-ticularly vulnerable to subclinical ischemia because they depend on distal blood supply. Vasomotor dys-function characteristic of hypertension impairs their capacity for compensatory redistribution of blood flow in response to cognitive challenge9. DSST is a power-ful tool to explore the executive cognitive domain asso-ciated with brain regions most affected by hypertensive vasculopathy. On the hypertensive group, we found an inverse correlation between age and DSST perfor-mance, which is consistent with the previous re-ports21,37. Motor dexterity decline through aging may contribute to this consistent finding and hypertension could accelerate this process. Although we guarantee a minimum level of education in our inclusion criteria, we did not specifically explore the influence of the ed-ucational level on DSST performance. However, the previous reports state that there is no relationship be-tween education and DSST performance probably due to their iconographic nature, making it useful in poor educated populations like ours8. As opposed to most studies revised, we could not observe a significant correlation between DSST scores and duration of dis-ease. The duration of hypertension is relevant because there is evidence that their neurodegenerative effects are accumulative38.
Effective hypertension management requires a sub-stantial amount of self-planning and adherence to phar-macological and non-pharmacological treatment. Thus, we propose that executive dysfunction may worsen self-care on hypertensive patients. Assessing executive function since middle age with easy administrated tests
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

95
E.J. Palma-Díaz, et al.: Executive dysfunction in hypertensive adults
like the DSST in primary health-care settings could promote early interventions that preserve the functional independence of hypertensive patients.
Conclusion
In conclusion, mature adults with hypertension had less efficiency in the executive function test. Men showed worse test performance compared to women. In this population the control of hypertension and the duration of the disease did not affect the performance of the executive function.
Funding
The present investigation has not received specific aid from public sector agencies, commercial sector, or non-profit entities.
Conflicts of interest
The authors declare no conflicts of interest.
Ethical disclosures
Protection of human and animal subjects. The authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of data. The authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consent. The au-thors have obtained the written informed consent of the patients or subjects mentioned in the article. The cor-responding author is in possession of this document.
References 1. Campos-Nonato I, Hernández-Barrera L, Pedroza-Tobías A, Medina C,
Barquera S. Hipertensión arterial en adultos mexicanos: prevalencia, diagnóstico y tipo de tratamiento. Ensanut MC 2016. Salud Pública Méx. 2018;60:233-43.
2. Lim SS, Vos T, Flaxman AD, Danaei G, Shibuya K, Adair-Rohani H, et al. A comparative risk assessment of burden of disease and injury attribu-table to 67 risk factors and risk factor clusters in 21 regions, 1990-2010: a systematic analysis for the global burden of disease study 2010. Lan-cet. 2012;380:2224-60.
3. Ibrahim MM, Damasceno A. Hypertension in developing countries. Lan-cet. 2012;380:611-9.
4. Novak V, Hajjar I. The relationship between blood pressure and cogniti-ve function. Nat Rev Cardiol. 2010;7:686-98.
5. Vicario A, Martinez CD, Baretto D, Diaz Casale A, Nicolosi L. Hyperten-sion and cognitive decline: impact on executive function. J Clin Hypertens (Greenwich). 2005;7:598-604.
6. Iadecola C, Yaffe K, Biller J, Bratzke LC, Faraci FM, Gorelick PB, et al. Impact of hypertension on cognitive function: a scientific statement from the American heart association. Hypertension. 2016;68:e67-e94.
7. Royall DR, Lauterbach EC, Cummings JL, Reeve A, Rummans TA, Kaufer DI, et al. Executive control function: a review of its promise and challenges for clinical research. A report from the committee on research of the American neuropsychiatric association. J Neuropsychiatry Clin Neurosci. 2002;14:377-405.
8. Abell JG, Kivimäki M, Dugravot A, Tabak AG, Fayosse A, Shipley M, et al. Association between systolic blood pressure and dementia in the Whitehall II cohort study: role of age, duration, and threshold used to define hypertension. Eur Heart J. 2018;39:3119-25.
9. Raz N, Rodrigue KM, Acker JD. Hypertension and the brain: vulnerabili-ty of the prefrontal regions and executive functions. Behav Neurosci. 2003;117:1169-80.
10. Iyer AS, Ahmed MI, Filippatos GS, Ekundayo OJ, Aban IB, Love TE, et al. Uncontrolled hypertension and increased risk for incident heart failure in older adults with hypertension: findings from a propensity-matched pros-pective population study. J Am Soc Hypertens. 2010;4:22-31.
11. Gaertner B, Wagner M, Luck T, Buttery AK, Fuchs J, Busch MA. Norma-tive data for the digit symbol substitution test in a population-based sample aged 65-79 years: results from the German health interview and examination survey for adults (DEGS1). Clin Neuropsychol. 2018; 32:114-32.
12. Secretaría de Salud. Para la Prevención, Detección, Diagnóstico, Trata-miento y Control de la Hipertensión Arterial Sistémica. NOM-030-SSA2-2017. Mexico: Diario Oficial de la Federación; 2017.
13. Vanotti S, Smerbeck A, Benedict RH, Caceres F. A new assessment tool for patients with multiple sclerosis from Spanish-speaking countries: va-lidation of the brief international cognitive assessment for MS (BICAMS) in Argentina. Clin Neuropsychol. 2016;30:1023-31.
14. Díaz-López LF, Haro-García LC, Juárez-Pérez CA, Aguilar-Madrid G. Alteraciones neuropsicológicas por exposición crónica a concentraciones bajas de monóxido de carbono en trabajadores de autopista de peaje de México. Salud Ment. 2015;38:353-9.
15. Tarraf W, Rodríguez CJ, Daviglus ML, Lamar M, Schneiderman N, Gallo L, et al. Blood pressure and hispanic/latino cognitive function: hispanic community health study/study of latinos results. J Alzheimers Dis. 2017;59:31-42.
16. Rosano C, Studenski SA, Aizenstein HJ, Boudreau RM, Longstreth WT Jr., Newman AB. Slower gait, slower information processing and smaller prefron-tal area in older adults. Age Ageing. 2012;41:58-64.
17. Crum RM, Anthony JC, Bassett SS, Folstein MF. Population-based nor-ms for the mini-mental state examination by age and educational level. JAMA. 1993;269:2386-91.
18. Aranda BD, Álvarez CD, Hernández RL, Ramírez MT. Propiedades psi-cométricas del modelo bifactorial del BDI-II (versión española) en mues-tras mexicanas de población general y estudiantes universitarios. Univ Psychol. 2015;14:15-26.
19. Lafont S, Marin-Lamellet C, Paire-Ficout L, Thomas-Anterion C, Laurent B, Fabrigoule C. The wechsler digit symbol substitution test as the best indicator of the risk of impaired driving in Alzheimer disease and normal aging. Dement Geriatr Cogn Disord. 2010;29:154-63.
20. Pinto E. Blood pressure and ageing. Postgrad Med J. 2007;83:109-14. 21. James PA, Oparil S, Carter BL, Cushman WC, Dennison-Himmelfarb C,
Handler J, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the eighth joint national committee (JNC 8). JAMA. 2014;311:507-20.
22. Whelton PK, Carey RM, Aronow WS, Casey DE Jr., Collins KJ, Dennison Himmelfarb C, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: executive summary: a report of the American college of cardiology/American heart association task force on clinical practice guidelines. Hypertension. 2018;71:1269-324.
23. Owen JG, Reisin E. Anti-hypertensive drug treatment of patients with and the metabolic syndrome and obesity: a review of evidence, meta-analysis, post hoc and guidelines publications. Curr Hypertens Rep. 2015;17:558.
24. Vasilopoulos T, Kremen WS, Kim K, Panizzon MS, Stein PK, Xian H, et al. Untreated hypertension decreases heritability of cognition in late middle age. Behav Genet. 2012;42:107-20.
25. Knecht S, Wersching H, Lohmann H, Berger K, Ringelstein EB. How much does hypertension affect cognition? Explained variance in cross-sectional analysis of non-demented community-dwelling individuals in the SEARCH study. J Neurol Sci. 2009;283:149-52.
26. Singh-Manoux A, Marmot M. High blood pressure was associated with cognitive function in middle-age in the Whitehall II study. J Clin Epidemiol. 2005;58:1308-15.
27. Sherwin BB, Henry JF. Brain aging modulates the neuroprotective effects of estrogen on selective aspects of cognition in women: a critical review. Front Neuroendocrinol. 2008;29:88-113.
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

96
Rev Mex Neuroci. 2020;21(3)
28. Memon A, McCullough L. Cerebral circulation in men and women. In: Kerkhof PL, Miller VM, editors. Sex-specific Analysis of Cardiovascular Function. Switzerland: Springer International Publishing AG, part of Sprin-ger Nature; 2018. p. 279-91.
29. Colafella KMM, Denton KM. Sex-specific differences in hypertension and associated cardiovascular disease. Nat Rev Nephrol. 2018; 14:185-201.
30. Mitchell GF. Effects of central arterial aging on the structure and function of the peripheral vasculature: implications for end-organ damage. J Appl Physiol (1985). 2008;105:1652-60.
31. Wei J, Yin X, Liu Q, Tan L, Jia C. Association between hypertension and cognitive function: a cross-sectional study in people over 45 years old in China. J Clin Hypertens (Greenwich). 2018;20:1575-83.
32. Kilander L, Nyman H, Boberg M, Hansson L, Lithell H. Hypertension is related to cognitive impairment: a 20-year follow-up of 999 men. Hyper-tension. 1998;31:780-6.
33. Launer LJ, Masaki K, Petrovitch H, Foley D, Havlik RJ. The association between midlife blood pressure levels and late-life cognitive function. The Honolulu-Asia aging study. JAMA. 1995;274:1846-51.
34. Gottesman RF, Schneider AL, Albert M, Alonso A, Bandeen-Roche K, Coker L, et al. Midlife hypertension and 20-year cognitive change: the atherosclerosis risk in communities neurocognitive study. JAMA Neurol. 2014;71:1218-27.
35. Usui N, Haji T, Maruyama M, Katsuyama N, Uchida S, Hozawa A, et al. Cortical areas related to performance of WAIS digit symbol test: a func-tional imaging study. Neurosci Lett. 2009;463:1-5.
36. Thornton KE, Carmody DP. Symbol digit and the quantitative EEG. Neurotherapy. 2012;16:210–222.
37. Smith EE, O’Donnell M, Dagenais G, Lear SA, Wielgosz A, Sharma M, et al. Early cerebral small vessel disease and brain volume, cognition, and gait. Ann Neurol. 2015;77:251-61.
38. Walker KA, Power MC, Gottesman RF. Defining the relationship between hypertension, cognitive decline, and dementia: a review. Curr Hypertens Rep. 2017;19:24.
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020
97
Clinical considerations on the introduction of ocrelizumab in MexicoLaura Ordoñez-Boschetti1*, Merced Velázquez-Quintana2, Eli Skromne-Eisenberg3, Irene Treviño-Frenk4, Verónica Rivas-Alonso5, Brenda Bertado-Cortes6, Manuel De la Maza-Flores7, Sandra Quiñones-Aguilar8, Luis Amaya-Sánchez9, Leonardo Llamas-López10, and Victor Gonzalez-Amezquita11
1Department of Neurology, Hospital Español de México, Mexico City; 2Department of Neurology, Unidad de Investigación en Salud de Chihuahua, Chihuahua; 3Mexican Neuroscience Institute, Hospital Ángeles Interlomas, Mexico City; 4Multiple Sclerosis Clinic, Department of Neurology, Instituto Nacional de Nutrición Salvador Zubirán (INNSZ), Mexico City; 5Multiple Sclerosis Clinic, Department of Neurology, Instituto Nacional de Neurología y Neurocirugía Doctor Manuel Velasco Suárez (INNNMVS), Mexico City; 6Multiple Sclerosis Clinic, Department of Neurology, Centro Médico Nacional Siglo XXI, Instituto Mexicano del Seguro Social (IMSS), Mexico City; 7Department of Neurology, Hospital San José, Instituto Tecnológico de Estudios Superiores de Monterrey (ITESM), Neurology and Neurosurgery Institute, Hospital Zambrano Hellion, Monterrey, Nuevo León; 8Demyelinating Diseases Clinic, Department of Neurology, Centro Médico Nacional Siglo XXI, Instituto Mexicano del Seguro Social (IMSS), Mexico City; 9Department of Neurology, Centro Médico Nacional Siglo XXI, Instituto Mexicano del Seguro Social (IMSS), Mexico City; 10Department of Neurology, Hospital Valentín Gómez Farías, Instituto de Seguridad y Servicios Sociales de los Trabajadores del Estado (ISSSTE), Guadalajara, Jalisco; 11Department of Neurology, Instituto de Seguridad Social del Estado de México y Municipios (ISSEMyM), Toluca, State of Mexico, Mexico
Revista Mexicana de Neurociencia
ORIGINAL ARTICLE
Abstract
Multiple sclerosis (MS) is the leading cause of neurological disability among young adults. The disease-modifying treatments (DMTs) have been a breakthrough in the care of this patients, becoming a treatable disease. Today, we face a broad spectrum of treatment possibilities, which should be used rationally to provide the maximum benefit for the patients. In the context of the introduction of ocrelizumab as a treatment option in the Mexican MS DMT portfolio, a group of neurologists was conve-ned to analyze the potential transition among DMT from their experience, through a desk research and expert opinion. As a result, here we describe the different considerations suggested for switching from different DMT to ocrelizumab that includes profiling studies, washout periods, and follow-up considerations. We concluded that the switch from other DMT previously used to ocrelizumab could be convenient and safe, as long as there is an adequate selection and profiling of the patients.
Key words: Drug switching. Expert opinion. Mexico. Multiple sclerosis. Ocrelizumab. Disease-modifying treatment.
Consideraciones clínicas sobre la introducción del ocrelizumab en México
Resumen
La esclerosis múltiple (EM) es la principal causa neurológica de discapacidad en adultos jóvenes. Los tratamientos modifi-cadores de la enfermedad (TME) han representado un enorme avance en su atención y han convertido a la EM en una enfermedad tratable. Hoy día nos enfrentamos a un amplio espectro de posibilidades de tratamientos, que deben ser utilizados de forma racional para brindar el mayor beneficio a los pacientes. En el contexto de la introducción del ocrelizu-mab al mercado mexicano se convocó a un grupo de neurólogos con el fin de analizar la transición terapéutica desde
Correspondence: *Laura Ordoñez-Boschetti
E-mail: [email protected]
Available online: 18-05-2020
Rev Mex Neuroci. 2020;21(3):97-103
www.revmexneurociencia.com
Date of reception: 14-11-2019
Date of acceptance: 18-01-2020
DOI: 10.24875/RMN.20000153
1665-5044/ © 2020 Academia Mexicana de Neurología A.C. Published by Permanyer. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

98
Rev Mex Neuroci. 2020;21(3)
Introduction
Multiple sclerosis (MS) is the main neurological cause of disability in young adults around the world. The diagnosis of MS has increased substantially in the past few decades, with a prevalence of 1.6/100,000 habitants in 19721,2. According to the previous studies, it has been estimated that there are at least 15,000 people in Mexico who suffer from MS, with a preva-lence of 7.5-30/100,000 habitants2,3.
Treatment aimed at modifying the natural history of MS has progressed considerably. The first disease-mod-ifying treatment (DMT) approved was interferon beta-1b in 19931, since then, we have had major changes in the understanding of the disease and now much more is known about environmental risk factors and genetic susceptibly, and the specific pathogenesis of MS may be explained in more detail. That is why there is now a wide range of treatment options available that should be used rationally to better benefit patients3.
This work was carried out in the context of the introduc-tion of ocrelizumab (Ocrevus®) to the Mexican market. Ocrelizumab is an IgG1 humanized monoclonal antibody that depletes B lymphocytes that express the CD20+ surface protein in their membrane. This limits immunolog-ical events linked to autoimmune conditions, specifically, MS4. Having a new DMT available, make it possible to debate over its use, which is why Roche has brought together a group of Mexican neurologists to examine the therapeutic transition from different points of view, based on their experience. The opinions given herein are the responsibility of the physicians who gave them and are independent from the unrestricted support given.
This work was carried out before ocrelizumab was available in Mexico; the health authorities have given the authorization to commercialize it.
Materials and methods
This analysis was carried out in the second half of 2017. Eleven neurologists considered as opinion
leaders in MS, highly experienced in DMT and its mechanism of action (MoA), who understood the impli-cations of changing treatment and were asked to give their point of view.
The group was made up of 11 neurologists who worked at some of the major public and private health institutions and hospitals in Mexico (INNN, IMSS, Hos-pital Español, Hospital Ángeles Lomas, INCNSZ, ISSSTE, ISSEMyM, etc.)
The work was carried out in two hands-on sessions, each lasting 2 days. Points to be considered included: (a) defining the guidelines for the proper use of ocreli-zumab; (b) establishing the medical reasons for why a switch in treatment could be considered and its impli-cations; (c) suggested paraclinical studies according to the treatment from which they are switching; (d) sug-gested washout period to migrate each DMT to ocreli-zumab; and (e) suggested paraclinical control studies.
The work has been carried out for academic purposes, design as a non-experimental and documentary re-search that involved open discussion in teams and reflections as a group.
The work was divided into two sessions: in the first, the group was divided into teams to discuss in depth of rationale behind each subject and reach a consen-sus; in the second, all proposals were discussed ex-tensively followed by an open discussion on what was learned and final comments and consensus.
Results
Placing ourselves in the MS treatment algorithm context, in Mexico, we have beta-1b interferon, beta-1a interferon, glatiramer acetate, teriflunomide, dimethyl fumarate, fingolimod, natalizumab, and alemtuzumab. Ocrelizumab is now one of the many drugs available.
Treatment guidelines around the world say that the choice of DMT depends on the characteristics of patients, comorbidities, activity/severity of the dis-ease, safety profile, access to treatment, and other aspects5-7.
diferentes ópticas, con base en la experiencia del grupo convocado con el uso de TME, realizando una investigación docu-mental y de opinión de expertos. Como resultado se describen los diferentes aspectos para considerar el cambio de diferentes moléculas previamente usadas a ocrelizumab, así como los estudios de perfilamiento sugeridos, el tiempo de eliminación para cada molécula, los tiempos de lavado necesarios para cada molécula y los estudios de seguimiento ne-cesarios. Se concluye que el cambio de las TME presentes a ocrelizumab puede resultar conveniente y seguro, siempre y cuando exista una adecuada selección y perfilamiento de los pacientes.
Palabras clave: Cambio de tratamiento. Esclerosis múltiple. México. Ocrelizumab. Opinión de expertos. Tratamiento modifi-cador de la enfermedad.
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020
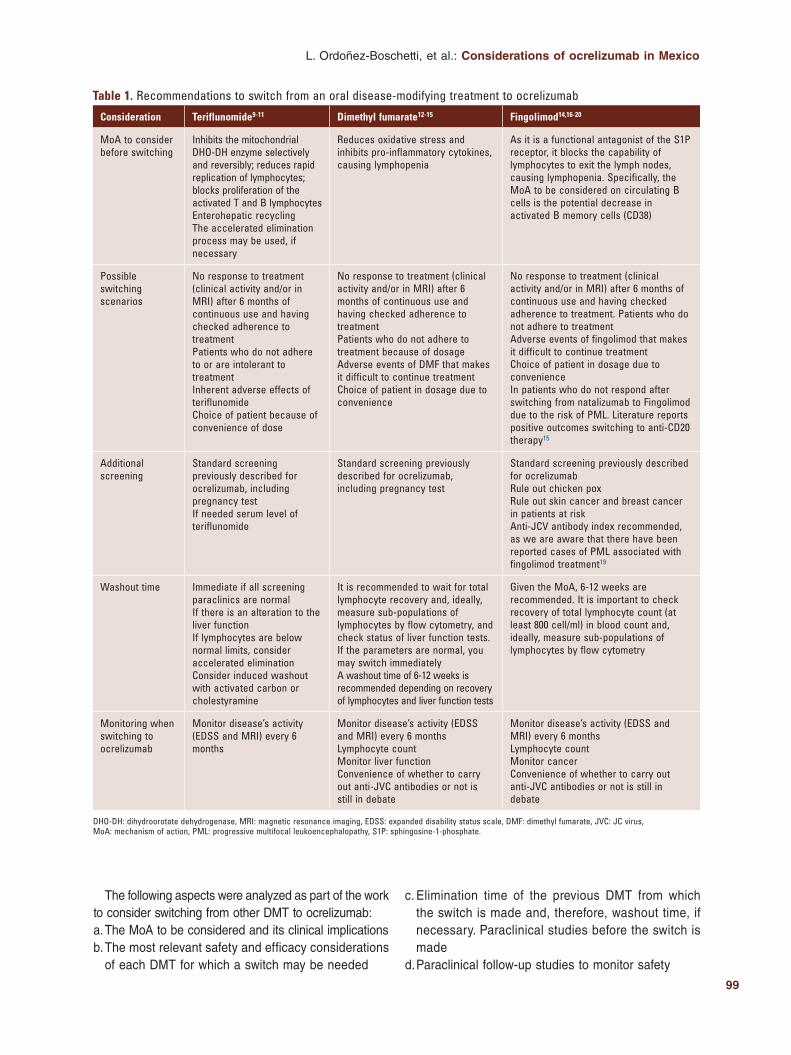
99
L. Ordoñez-Boschetti, et al.: Considerations of ocrelizumab in Mexico
Table 1. Recommendations to switch from an oral disease-modifying treatment to ocrelizumab
Consideration Teriflunomide9-11 Dimethyl fumarate12-15 Fingolimod14,16-20
MoA to consider before switching
Inhibits the mitochondrial DHO-DH enzyme selectively and reversibly; reduces rapid replication of lymphocytes; blocks proliferation of the activated T and B lymphocytesEnterohepatic recyclingThe accelerated elimination process may be used, if necessary
Reduces oxidative stress and inhibits pro-inflammatory cytokines, causing lymphopenia
As it is a functional antagonist of the S1P receptor, it blocks the capability of lymphocytes to exit the lymph nodes, causing lymphopenia. Specifically, the MoA to be considered on circulating B cells is the potential decrease in activated B memory cells (CD38)
Possible switching scenarios
No response to treatment (clinical activity and/or in MRI) after 6 months of continuous use and having checked adherence to treatmentPatients who do not adhere to or are intolerant to treatmentInherent adverse effects of teriflunomideChoice of patient because of convenience of dose
No response to treatment (clinical activity and/or in MRI) after 6 months of continuous use and having checked adherence to treatmentPatients who do not adhere to treatment because of dosageAdverse events of DMF that makes it difficult to continue treatmentChoice of patient in dosage due to convenience
No response to treatment (clinical activity and/or in MRI) after 6 months of continuous use and having checked adherence to treatment. Patients who do not adhere to treatmentAdverse events of fingolimod that makes it difficult to continue treatmentChoice of patient in dosage due to convenienceIn patients who do not respond after switching from natalizumab to Fingolimod due to the risk of PML. Literature reports positive outcomes switching to anti-CD20 therapy15
Additional screening
Standard screening previously described for ocrelizumab, including pregnancy testIf needed serum level of teriflunomide
Standard screening previously described for ocrelizumab, including pregnancy test
Standard screening previously described for ocrelizumabRule out chicken poxRule out skin cancer and breast cancer in patients at riskAnti-JCV antibody index recommended, as we are aware that there have been reported cases of PML associated with fingolimod treatment19
Washout time Immediate if all screening paraclinics are normalIf there is an alteration to the liver functionIf lymphocytes are below normal limits, consider accelerated eliminationConsider induced washout with activated carbon or cholestyramine
It is recommended to wait for total lymphocyte recovery and, ideally, measure sub-populations of lymphocytes by flow cytometry, and check status of liver function tests. If the parameters are normal, you may switch immediatelyA washout time of 6-12 weeks is recommended depending on recovery of lymphocytes and liver function tests
Given the MoA, 6-12 weeks are recommended. It is important to check recovery of total lymphocyte count (at least 800 cell/ml) in blood count and, ideally, measure sub-populations of lymphocytes by flow cytometry
Monitoring when switching to ocrelizumab
Monitor disease’s activity (EDSS and MRI) every 6 months
Monitor disease’s activity (EDSS and MRI) every 6 monthsLymphocyte countMonitor liver functionConvenience of whether to carry out anti-JVC antibodies or not is still in debate
Monitor disease’s activity (EDSS and MRI) every 6 monthsLymphocyte countMonitor cancerConvenience of whether to carry out anti-JVC antibodies or not is still in debate
DHO-DH: dihydroorotate dehydrogenase, MRI: magnetic resonance imaging, EDSS: expanded disability status scale, DMF: dimethyl fumarate, JVC: JC virus, MoA: mechanism of action, PML: progressive multifocal leukoencephalopathy, S1P: sphingosine-1-phosphate.
The following aspects were analyzed as part of the work to consider switching from other DMT to ocrelizumab:a. The MoA to be considered and its clinical implicationsb. The most relevant safety and efficacy considerations
of each DMT for which a switch may be needed
c. Elimination time of the previous DMT from which the switch is made and, therefore, washout time, if necessary. Paraclinical studies before the switch is made
d. Paraclinical follow-up studies to monitor safety
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020
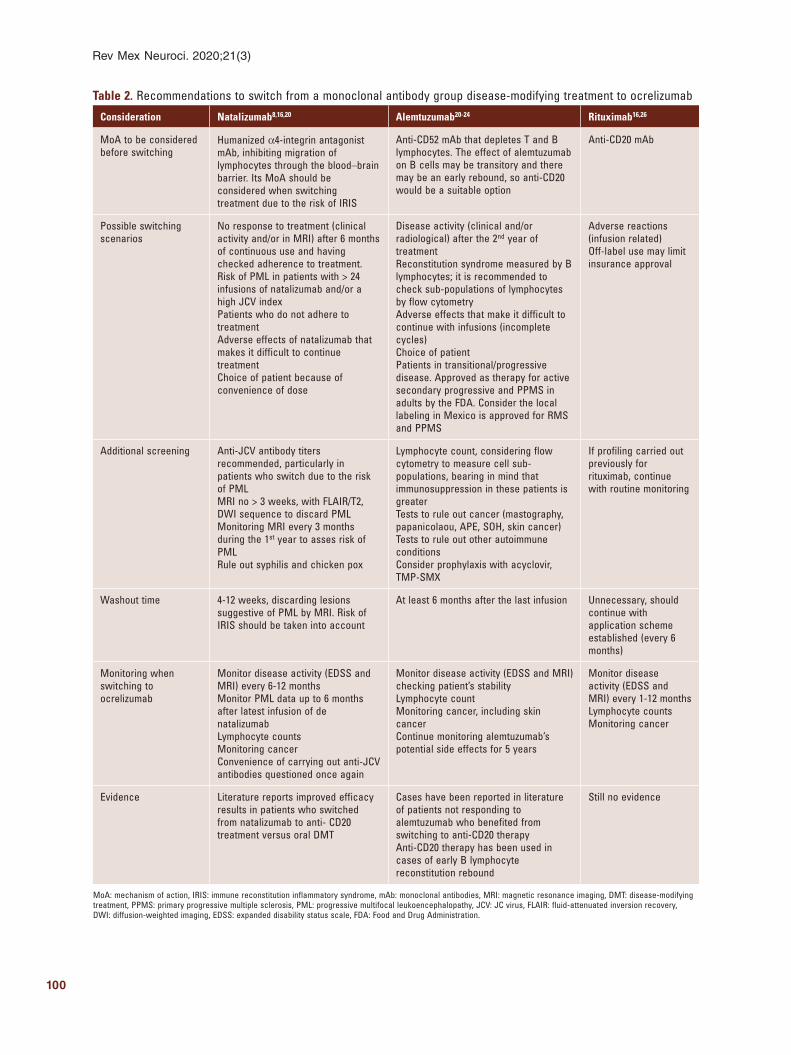
100
Rev Mex Neuroci. 2020;21(3)
Table 2. Recommendations to switch from a monoclonal antibody group disease-modifying treatment to ocrelizumab
Consideration Natalizumab8,16,20 Alemtuzumab20-24 Rituximab16,26
MoA to be considered before switching
Humanized α4-integrin antagonist mAb, inhibiting migration of lymphocytes through the blood–brain barrier. Its MoA should be considered when switching treatment due to the risk of IRIS
Anti-CD52 mAb that depletes T and B lymphocytes. The effect of alemtuzumab on B cells may be transitory and there may be an early rebound, so anti-CD20 would be a suitable option
Anti-CD20 mAb
Possible switching scenarios
No response to treatment (clinical activity and/or in MRI) after 6 months of continuous use and having checked adherence to treatment. Risk of PML in patients with > 24 infusions of natalizumab and/or a high JCV indexPatients who do not adhere to treatmentAdverse effects of natalizumab that makes it difficult to continue treatmentChoice of patient because of convenience of dose
Disease activity (clinical and/or radiological) after the 2nd year of treatmentReconstitution syndrome measured by B lymphocytes; it is recommended to check sub-populations of lymphocytes by flow cytometryAdverse effects that make it difficult to continue with infusions (incomplete cycles)Choice of patientPatients in transitional/progressive disease. Approved as therapy for active secondary progressive and PPMS in adults by the FDA. Consider the local labeling in Mexico is approved for RMS and PPMS
Adverse reactions (infusion related)Off-label use may limit insurance approval
Additional screening Anti-JCV antibody titers recommended, particularly in patients who switch due to the risk of PMLMRI no > 3 weeks, with FLAIR/T2, DWI sequence to discard PMLMonitoring MRI every 3 months during the 1st year to asses risk of PMLRule out syphilis and chicken pox
Lymphocyte count, considering flow cytometry to measure cell sub-populations, bearing in mind that immunosuppression in these patients is greaterTests to rule out cancer (mastography, papanicolaou, APE, SOH, skin cancer)Tests to rule out other autoimmune conditionsConsider prophylaxis with acyclovir, TMP-SMX
If profiling carried out previously for rituximab, continue with routine monitoring
Washout time 4-12 weeks, discarding lesions suggestive of PML by MRI. Risk of IRIS should be taken into account
At least 6 months after the last infusion Unnecessary, should continue with application scheme established (every 6 months)
Monitoring when switching to ocrelizumab
Monitor disease activity (EDSS and MRI) every 6-12 monthsMonitor PML data up to 6 months after latest infusion of de natalizumabLymphocyte countsMonitoring cancerConvenience of carrying out anti-JCV antibodies questioned once again
Monitor disease activity (EDSS and MRI) checking patient’s stabilityLymphocyte countMonitoring cancer, including skin cancerContinue monitoring alemtuzumab’s potential side effects for 5 years
Monitor disease activity (EDSS and MRI) every 1-12 monthsLymphocyte countsMonitoring cancer
Evidence Literature reports improved efficacy results in patients who switched from natalizumab to anti- CD20 treatment versus oral DMT
Cases have been reported in literature of patients not responding to alemtuzumab who benefited from switching to anti-CD20 therapyAnti-CD20 therapy has been used in cases of early B lymphocyte reconstitution rebound
Still no evidence
MoA: mechanism of action, IRIS: immune reconstitution inflammatory syndrome, mAb: monoclonal antibodies, MRI: magnetic resonance imaging, DMT: disease-modifying treatment, PPMS: primary progressive multiple sclerosis, PML: progressive multifocal leukoencephalopathy, JCV: JC virus, FLAIR: fluid-attenuated inversion recovery, DWI: diffusion-weighted imaging, EDSS: expanded disability status scale, FDA: Food and Drug Administration. N
o p
art
of
this
pu
blic
atio
n m
ay b
e re
pro
du
ced
or
ph
oto
cop
yin
g w
ith
ou
t th
e p
rio
r w
ritt
en p
erm
issi
on
of
the
pu
blis
her
.
© P
erm
anye
r 20
20

101
L. Ordoñez-Boschetti, et al.: Considerations of ocrelizumab in Mexico
In every case, the suggested paraclinical studies for patients to start treatment with ocrelizumab include the following:– Blood count– Blood chemistry– Liver function tests– Hepatitis testing – surface antigen and anti-core an-
tibodies of the virus (AgHBVs and anti-HBVc).– Rule out tuberculosis – recommend for the popula-
tion exposed.– Rule out HIV– recommend for the population
exposed.– Magnetic resonance imaging (MRI) – it is recom-
mended to have a baseline MRI of no more than 3 weeks8, ruling out any suspected progressive mul-tifocal leukoencephalopathy. The following sequenc-es must be taken into consideration: T1, T1 with gadolinium, T2, and fluid-attenuated inversion recov-ery, according to the international standard recom-mended by the MAGNIMS group8. The frequency and make-up of each follow-up is determined by the needs of the individual patient8.If switching from other DMT, specific recommended
studies may be added based on what is known about the MoA, as shown in tables 1 and 2. Therapies were divided into two large DMT groups: (a) oral DMT and (b) monoclonal antibodies (mAb). The tables below sum-marize the considerations made in the discussion groups.
We should point out that there is currently not enough evidence to draw final conclusions, so in this study, we will look at recommendations based on evidence avail-able of the MoA and the recommendations to switch from each DMT. The vast experience of clinical neurologists in using innovative DMT for MS was taken into account.
Conclusions
Some 25 years after the introduction of the first interferon for treating MS, we have witnessed how DMT has evolved, aiming to adjust the pathological process-es of this disease that we understand better than be-fore. We are well aware that there is no single treatment algorithm and decisions should be made based on the knowledge of the MoA and the experience gained with these therapies.
When discussing DMT, we may classify its development in three eras: (i) from 1993 to 2003, when the first inter-ferons were introduced and drugs were developed to better understand the immune physiopathological pro-cess of MS; (ii) the second was from 2003 to 2009 with
the advent of more efficacious DMT, such as natalizum-ab, the first monoclonal antibody, and fingolimod, the first oral DMT; and (iii) the third from 2009 to date, in which not only were biological therapies developed but also small molecules, such as dimethyl fumarate. The range of MoA from the DMT has been expanded during this time, the results are encouraging27.
Bearing this in mind, it is of particular interest to reflect on the experience and opinions of clinical neu-rologists about the potential switching from other DMT to those recently approved, such as ocrelizumab.
The group concludes that the switch of current DMT to ocrelizumab may be convenient and safe, as long as the patients are selected and evaluated correctly. We should bear in mind that the patients should be moni-tored closely during the first 24 h after the switch.
Real-life evidence is needed by means of several cas-es and evidence of safety in the medium and long term.
Ethical declaration
This work was carried out with the unrestricted support of Roche de México, including transport, travel expenses, and the fees of each person attending meetings.
Acknowledgments
The authors would like to thank Drs. Maria Pia Roque, Mariana Arzate, Roxana Flores, Carlos Pla, and As-drubal Huerta of Roche México for assisting in the lo-gistics of the activities carried out and Dr. Jose de Jesus Flores Rivera for his support.
Conflicts of interest
Dr. Ordoñez reports personal fees and non-financial support from Roche Servicios de Mexico, during the con-duct of the study, personal fees and non-financial support from Novartis, personal fees and non-financial support from Stendhal, personal fees and non-financial support from Teva, personal fees and non-financial support from Sanofi, personal fees and non-financial support from Mer-ck, grants and personal fees from Biogen, and grants and personal fees from Synthon, outside the submitted work; Dr. Velazquez Quintana reports personal fees and non-fi-nancial support from Roche Servicios de Mexico, during the conduct of the study; Dr. Skromne Eisenberg reports personal fees and non-financial support from Roche Ser-vicios de Mexico, during the conduct of the study, person-al fees and non-financial support from Merck, personal
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

102
Rev Mex Neuroci. 2020;21(3)
fees and non-financial support from Sanofi, personal fees and non-financial support from Stendhal, personal fees and non-financial support from Teva, and personal fees and non-financial support from Biogen, outside the submitted work; Dr. Treviño Frenk reports personal fees and non-financial support from Roche Servicios de Mex-ico, during the conduct of the study, personal fees and non-financial support from Teva, personal fees and non-fi-nancial support from Novartis, personal fees and non-fi-nancial support from Stendhal, personal fees and non-fi-nancial support from Merck, and personal fees and non-financial support from Sanofi, outside the submitted work; Dr. Rivas Alonso reports personal fees and non-fi-nancial support from Roche Servicios de Mexico, during the conduct of the study, personal fees and non-financial support from Stendhal, personal fees and non-financial support from Novartis, personal fees and non-financial support from Sanofi, personal fees and non-financial sup-port from Biogen, personal fees and non-financial support from Allegran, personal fees and non-financial support from Merck, personal fees and non-financial support from Psicofarma, personal fees and non-financial support from Allegran, and personal fees and non-financial support from Actellion, outside the submitted work; Dr. Bertado Cortes reports personal fees and non-financial support from Roche Servicios de Mexico, during the conduct of the study, personal fees and non-financial support from Novartis, personal fees and non-financial support from Teva, personal fees and non-financial support from Stend-hal, personal fees and non-financial support from Sanofi, personal fees and non-financial support from Merck, and personal fees and non-financial support from Biogen, out-side the submitted work; Dr. De La Maza Flores reports personal fees and non-financial support from Roche Ser-vicios de Mexico, during the conduct of the study, person-al fees and non-financial support from Novartis, personal fees and non-financial support from Sanofi, and personal fees and non-financial support from Merck, outside the submitted work; Dr. Quiñones Aguilar reports personal fees and non-financial support from Roche Servicios de Mexico, during the conduct of the study, personal fees and non-financial support from Novartis, personal fees and non-financial support from Sanofi, personal fees and non-financial support from Biogen, personal fees and non-financial support from Merck, personal fees and non-financial support from Teva, personal fees and non-fi-nancial support from Allegran, and personal fees and non-financial support from Dysport, outside the submitted work; Dr. Amaya Sanchez reports personal fees and non-financial support from Roche Servicios de Mexico, during the conduct of the study, personal fees and
non-financial support from Novartis, personal fees and non-financial support from Sanofi, and personal fees and non-financial support from Bayer, outside the submitted work; Dr. Llamas Lopez reports personal fees and non-fi-nancial support from Roche Servicios de Mexico, during the conduct of the study, personal fees and non-financial support from Biogen, personal fees and non-financial support from Merck, personal fees and non-financial sup-port from Novartis, personal fees and non-financial sup-port from Teva, personal fees and non-financial support from Stendhal, and grants from Probiomedic, outside the submitted work; and Dr. Gonzalez Amezquita reports per-sonal fees and non-financial support from Roche Servicios de Mexico, during the conduct of the study, personal fees and non-financial support from Bayer, personal fees and non-financial support from Merck, personal fees and non-financial support from Sanofi, personal fees and non-financial support from Stendhal, personal fees and non-financial support from UCB, personal fees and non-fi-nancial support from Probiomedic, personal fees and non-financial support from Armstron, personal fees and non-financial support from Allegran, and personal fees and non-financial support from Merz, outside the submit-ted work.
Ethical disclosures
Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of data. The authors declare that no patient data appear in this article.
Right to privacy and informed consent. The authors declare that no patient data appear in this article.
References 1. Tillery EE, Clements JN, Howard Z. What’s new in multiple sclerosis?
Ment Health Clin. 2017;7:213-20. 2. Velazquez M, Lopez P, Rivera C. Características epidemiológicas de la
esclerosis múltiple en un estado fronterizo con los Estados Unidos de Norteamérica. Arch Neurocie. 2002;3:147-50.
3. Correa E, Paredes V, Martínez B. Prevalence of multiple sclerosis in Latin America and its relationship with European migration. Mult Scler J Exp Transl Clin. 2016;2:1-10.
4. Frau J, Coghe G, Lorefice L, Fenu G, Cocco E. New horizons for multi-ple sclerosis therapeutics: milestones in the development of ocrelizumab. Neuropsychiatr Dis. Treat 2018;14:1093-9.
5. Soelberg Sorensen P. Safety concerns and risk management of multiple sclerosis therapies. Acta Neurol Scand. 2017;136:168-86.
6. Rae-Grant A, Day GS, Marrie RA, Rabinstein A, Cree BAC, Gronseth GS, et al. Practice guideline recommendations summary: disease-modifying therapies for adults with multiple sclerosis: report of the Guideline Deve-lopment, Dissemination, and Implementation Subcommittee of the Ame-rican Academy of Neurology. Neurology. 2018;90:777-88.
7. Wattjes MP, Rovira À, Miller D, Yousry TA, Sormani MP, de Stefano MP, et al. Evidence-based guidelines: MAGNIMS consensus guidelines on the use of MRI in multiple sclerosis--establishing disease prognosis and monitoring patients. Nat Rev Neurol. 2015;11:597-606.
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

103
L. Ordoñez-Boschetti, et al.: Considerations of ocrelizumab in Mexico
8. Montalban X, Gold R, Thompson AJ, Otero-Romero S, Amato MP, Chandraratna D, et al. ECTRIMS/EAN guideline on the pharmacolo-gical treatment of people with multiple sclerosis. Eur J Neurol. 2018; 25:215-37.
9. Miller AE. Oral teriflunomide in the treatment of relapsing forms of mul-tiple sclerosis: clinical evidence and long-term experience. Ther Adv Neurol Disord. 2017;10:381-96.
10. O’Connor P, Comi G, Freedman MS, Miller AE, Kappos L, Bouchard JP, et al. Long-term safety and efficacy of teriflunomide: nine-year follow-up of the randomized TEMSO study. Neurology. 2016;86:920-30.
11. Gandoglia I, Ivaldi F, Laroni A, Benvenuto F, Solaro C, Mancardi G, et al. Teriflunomide treatment reduces B cells in patients with MS. Neurol Neuroimmunol Neuroinflamm. 2017;4:e403.
12. Zhovtis Ryerson L, Green R, Confident G, Pandey K, Richter B, Bacon T, et al. Efficacy and tolerability of dimethyl fumarate in White-, African- and Hispanic- Americans with multiple sclerosis. Ther Adv Neurol Disord. 2016;9:454-61.
13. Chen H, Assmann JC, Krenz A, Rahman M, Grimm M, Karsten CM, et al. Hydroxycarboxylic acid receptor 2 mediates dimethyl Fumarate’s protec-tive effect in EAE. J Clin Invest 2014;124:2188-92.
14. Hersh CM, Love TE, Cohn S, Hara-Cleaver C, Bermel RA, Fox RJ, et al. Comparative efficacy and discontinuation of dimethyl fumarate and fingo-limod in clinical practice at 12-month follow-up. Mult Scler Relat Disord. 2016;10:44-52.
15. Fox RJ, Kita M, Cohan SL, Henson LJ, Zambrano J, Scannevin RH, et al. BG-12 (dimethyl fumarate): a review of mechanism of action, efficacy, and safety. Curr Med Res Opin. 2014;30:251-62.
16. Alping P, Frisell T, Novakova L, Islam-Jakobsson P, Salzer J, Björck A, et al. Rituximab versus fingolimod after natalizumab in multiple sclerosis patients. Ann Neurol. 2016;79:950-8.
17. Angerer IC, Hecker M, Koczan D, Roch L, Friess J, Rüge A, et al. Trans-criptome profiling of peripheral blood immune cell populations in multiple sclerosis patients before and during treatment with a sphingosine-1-phos-phate receptor modulator. CNS Neurosci Ther 2018;24:193-201.
18. Nakamura M, Morris M, Cerghet M, Schultz L, Elias S. Longitudinal fo-llow-up of a cohort of patients with incidental abnormal magnetic reso-nance imaging findings at presentation and their risk of developing mul-tiple sclerosis. Int J MS Care. 2014;16:111-5.
19. Ingwersen J, Aktas O, Kuery P, Kieseier B, Boyko A, Hartung HP. Fin-golimod in multiple sclerosis: mechanisms of action and clinical efficacy. Clin Immunol. 2012;142:15-24.
20. Berger JR. Classifying PML risk with disease modifying therapies. Mult Scler Relat Disord. 2017;12:59-63.
21. Baker D, Herrod SS, Alvarez-Gonzalez C, Giovannoni G, Schmierer K. Interpreting lymphocyte reconstitution data from the pivotal phase 3 trials of alemtuzumab. JAMA Neurol. 2017;74:961-9.
22. Haghikia A, Dendrou CA, Schneider R, Grüter T, Postert T, Matzke M, et al. Severe B-cell-mediated CNS disease secondary to alemtuzumab therapy. Lancet Neurol. 2017;16:104-6.
23. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/la-bel/2019/761053s018lbl.pdf. [Last accessed on 2020 Jan 15].
24. Kappos L, Wolinsky JS, Giovannoni G, Arnold DL, Lublin F, Wang Q, et al. Ocrelizumab reduces disability progression independent of relapse activity in patients with relapsing multiple sclerosis. Mult Scler J. 2017;23:309-10.
25. Wehrum T, Beume LA, Stich O, Mader I, Mäurer M, Czaplinski A, et al. Activation of disease during therapy with alemtuzumab in 3 patients with multiple sclerosis. Neurology. 2018;90:e601-5.
26. Hauser SL. The Charcot lecture beating MS: a story of B cells, with twists and turns. Mult Scler. 2015;21:8-21.
27. Ransohoff RM, Hafler DA, Lucchinetti CF. Multiple sclerosis-a quiet re-volution. Nat Rev Neurol. 2015;11:134-42.
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020
104
Cranial electrical stimulation for the treatment of insomnia, anxiety, and depression symptoms in adultsJesús A. Moo-Estrella*, and María F. Pérez-PichardoSleep Laboratory, School of Psychology, Universidad Autónoma de Yucatán, Mérida, Yucatán, Mexico
Revista Mexicana de Neurociencia
ORIGINAL ARTICLE
Abstract
Background: Clinical advantages of the cranial electrical stimulation (CES) are not yet clear. Objective: The objective of the study was to know the effects as a result of the CES intervention for the treatment of insomnia symptoms, anxiety, and depression. Method: Twenty-four individuals agreed to participate in the study, all of them with initial insomnia diagnosis (ISDC-2), with an average age of 32.10 (± 14.24) years old (58% women), distributed in control (n = 11) and experimental group (n = 13). The intruments used were Beck’s depression inventory, State-Trait Anxiety Inventory, the Insomnia Severity Index, and the Insomnia Symptoms Questionnaire. A CES device (Fisher Wallace-100) was given to each participant for its use at nights and mornings (20 min each session) for 10 days. Results: Insomnia symptoms decreased significantly in both the control and experimental groups (p < 0.01), but only in the experimental group there was a significant reduction in the severity of insomnia (p < 0.05). According to the effect size (Cohen’s d), the experimental group had a larger effect in the insomnia severity and a moderated effect for anxiety and depression. The placebo group had a small effect in anxiety and a medium in insomnia and depression. Conclusions: The CES effect is superior to placebo to reduce the insomnia severity, but it is no different from placebo for anxiety and depression symptoms.
Key words: Anxiety. Cranial electrical stimulation. Depression. Insomnia.
Estimulación eléctrica craneal para el tratamiento de los síntomas de insomnio, ansiedad y depresión en adultos
Resumen
Introducción: La estimulación eléctrica craneal (EEC) es una técnica neurofisiológica que consiste en enviar pulsos de corriente eléctrica (< 4 mA) al cerebro a través de electrodos colocados en el cuero cabelludo. Sin embargo, los alcances clínicos de la EEC como tratamiento para las alteraciones afectivas y del sueño aún no están claros. Objetivo: Conocer los efectos del uso de la intervención EEC para el tratamiento sobre los síntomas de insomnio, ansiedad y depresión. Método: Participaron 24 sujetos que cumplieron los criterios de insomnio de acuerdo con el ISDC-2, con una edad promedio de 32.10 (± 14.24) años (58% mujeres), divididos en grupo control (n = 11) y grupo experimental (n = 13). Los instrumentos utilizados fueron el inventario de depresión de Beck, el cuestionario de ansiedad-estado (Spielberger), el Índice de Severi-dad de Insomnio y un cuestionario de síntomas de insomnio. Cada participante recibió un dispositivo de EEC (FW-100) para
Correspondence: *Jesús A. Moo-Estrella
E-mail: [email protected]
Available online: 18-05-2020
Rev Mex Neuroci. 2020;21(3):104-110
www.revmexneurociencia.com
Date of reception: 09-05-2019
Date of acceptance: 18-01-2020
DOI: 10.24875/RMN.20000083
1665-5044/ © 2020. Academia Mexicana de Neurología A.C. Published by Permanyer. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

105
J.A. Moo-Estrella, M.F. Pérez-Pichardo: CES for insomnia, anxiety, and depression
Introduction
Anxiety, depression, and insomnia are considered to be among the alterations that generate disturbance in people who suffer them1,2. It is estimated that these changes may be present even in one-third of the world’s population3-5, and in Mexico, they can reach similar numbers6-8. These disorders are associated with the pathophysiology of the brain. Insomnia and anxiety include an increase of emo-tional, cognitive, somatic, and cortical excitability9,10 while depression is associated with the decrease of cortical activity in prefrontal areas and the anterior cingulate gy-rus11. Many interventions focus on drug treatments12-14, but they often have certain limitations, such as cost, side effects, and a decrease of its efficiency and the quality of patient’s lifestyles15-17. The non-pharmacological ap-proaches for the treatment of these disorders are diverse and its effectiveness is still in research18,19. Non-invasive brain stimulation techniques are used as an alternative to pharmacological treatment and they have shown a notable upturn in recent decades20.
Cranial electrical stimulation (CES) is a non-invasive neurophysiological technique that works through low-in-tensity pulses of electric current of ≤ 4 milliamperes (mA) in frequencies from 0.5 to 15,000 Hz, through two electrodes placed on the scalp21. The CES is safe22 and it has been employed on different disorders such as major depression, anxiety, post-traumatic stress disor-der, and insomnia23. Brain stimulation with alternating current (AC) such as CES has important approaches in the treatment of anxiety, depression, and insomnia24, however, it requires greater attention on its mechanism of action, especially in clinical research.
The mechanism of the CES on clinical symptoms has been explained at different levels on the nervous system. On the one hand, it is believed that the CES affects subcortical structures such as the reticular acti-vating system, the thalamus, hypothalamus, and limbic system16,21. Brain imaging studies suggest a cortical
deactivation in the prefrontal and parietal midline of the brain after 20 min of CES25. In addition, it is proposed that the effects of CES include both cortical and sub-cortical areas producing changes similar to the use of anti-anxiety medications26. At the electrophysiological level, it is observed an increase in alpha activity and a decrease in delta and beta activity27. At a biochemical level, it is suggested an increase in endorphins, adre-nocorticotropic hormone, serotonin, melatonin, norepi-nephrine, cholinesterase, and reduction of cortisol21.
Given that the electrodes are placed over the scalp, this technique is considered a form of peripheral nerve stimulation. Although the positive effects of the CES have been observed in different levels of the nervous system, its efficacy on clinical symptoms is not yet conclusive. However, the use of the CES in the clinical practice has increased steadily in recent decades, so it is required the application of empirical studies which can be distinguished from the placebo effect.
Method
Participants
Twenty-six cases that covered the insomnia symptoms based on the International Classification of Sleep Disor-ders (ICSD) were considered initially2. The inclusion cri-teria were to be over 18 years old and the exclusion criteria were having antecedents of epilepsy, receive treatment for insomnia or drug use with effects on the central nervous system or metallic implants and/or pace-makers. Of the 26 cases, two were eliminated from the control group, for failing to comply with the age of major-ity and the second report of phosphenes as a side effect in the first session of the treatment of CES (Fig. 1 shows the eligibility diagram). The final sample included 24 subjects with an average age of 32.10 (± 14. 24) years old (58% women), with a diagnosis of insomnia. Participants were randomized between the control
su uso en la noche y en la mañana (20 minutos cada sesión), durante 10 días, empleado durante 20 minutos cada noche antes de dormir y 20 minutos al despertar. Los cuestionarios fueron aplicados antes y después del tratamiento. Resultados: Los síntomas de insomnio disminuyeron significativamente tanto en el grupo control como el experimental (p < 0.01), pero solo en el grupo experimental hubo una reducción significativa de la gravedad del insomnio (p < 0.05). Con base en el tamaño del efecto (d de Cohen), el grupo experimental tuvo un efecto mayor en la reducción de la gravedad del insomnio y un efecto moderado para la ansiedad y la depresión. En el grupo de placebo (control) la magnitud del efecto fue leve para la ansiedad y moderada tanto para el insomnio como para la depresión. Conclusiones: El efecto EEC fue superior al placebo para reducir la gravedad en el tratamiento del insomnio, pero no fue diferente al placebo y tuvo efectos similares en la disminución de los síntomas de ansiedad y depresión.
Palabras clave: Ansiedad. Estimulación eléctrica craneal. Depresión. Insomnio.
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020
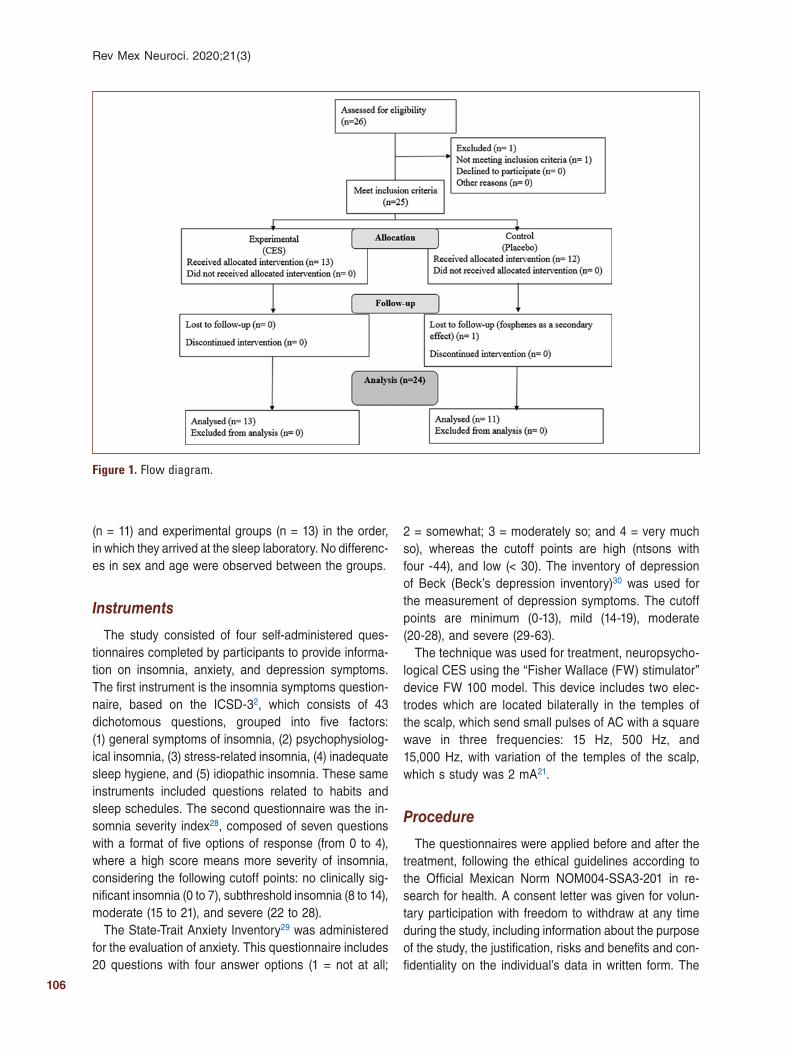
106
Rev Mex Neuroci. 2020;21(3)
(n = 11) and experimental groups (n = 13) in the order, in which they arrived at the sleep laboratory. No differenc-es in sex and age were observed between the groups.
Instruments
The study consisted of four self-administered ques-tionnaires completed by participants to provide informa-tion on insomnia, anxiety, and depression symptoms. The first instrument is the insomnia symptoms question-naire, based on the ICSD-32, which consists of 43 dichotomous questions, grouped into five factors: (1) general symptoms of insomnia, (2) psychophysiolog-ical insomnia, (3) stress-related insomnia, (4) inadequate sleep hygiene, and (5) idiopathic insomnia. These same instruments included questions related to habits and sleep schedules. The second questionnaire was the in-somnia severity index28, composed of seven questions with a format of five options of response (from 0 to 4), where a high score means more severity of insomnia, considering the following cutoff points: no clinically sig-nificant insomnia (0 to 7), subthreshold insomnia (8 to 14), moderate (15 to 21), and severe (22 to 28).
The State-Trait Anxiety Inventory29 was administered for the evaluation of anxiety. This questionnaire includes 20 questions with four answer options (1 = not at all;
2 = somewhat; 3 = moderately so; and 4 = very much so), whereas the cutoff points are high (ntsons with four -44), and low (< 30). The inventory of depression of Beck (Beck’s depression inventory)30 was used for the measurement of depression symptoms. The cutoff points are minimum (0-13), mild (14-19), moderate (20-28), and severe (29-63).
The technique was used for treatment, neuropsycho-logical CES using the “Fisher Wallace (FW) stimulator” device FW 100 model. This device includes two elec-trodes which are located bilaterally in the temples of the scalp, which send small pulses of AC with a square wave in three frequencies: 15 Hz, 500 Hz, and 15,000 Hz, with variation of the temples of the scalp, which s study was 2 mA21.
Procedure
The questionnaires were applied before and after the treatment, following the ethical guidelines according to the Official Mexican Norm NOM004-SSA3-201 in re-search for health. A consent letter was given for volun-tary participation with freedom to withdraw at any time during the study, including information about the purpose of the study, the justification, risks and benefits and con-fidentiality on the individual’s data in written form. The
Figure 1. Flow diagram.
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

107
J.A. Moo-Estrella, M.F. Pérez-Pichardo: CES for insomnia, anxiety, and depression
device was delivered to each subject for home use for 10 days. Previously held a training session in the sleep laboratory (Faculty of Psychology, Universidad Autóno-ma de Yucatán) indicating the use of the device for 20 min every night before bedtime and 20 min in the morning. For the control group, it was indicated that the therapeutic level was zero (placebo). It is worth men-tioning that a brochure on sleep hygiene was provided for the two groups. During the study, participants did not receive additional treatment. At the end of the pro-tocol, control was provided to participants in the group the device 10 days more in active mode (level 2).
The statistical test was used for data analysis Stu-dent’s t-test for related samples whereas alpha mini-mum of 0.05. Similarly, the effect size was analyzed to assess the relevance of the effects of intervention among groups within the practical context of research. For the effect size, following cutoff points were consid-ered: no effect al0.20, small = 0.21-0.49, medium effect = 0.50-0.79, and large effect =0.8031.
Results
A difference was found in relation to the sleep habits (p < 0.01) in the experimental group, which reported one more hour of sleep after the intervention (Table 1). There was a significant reduction of four symptoms of insomnia in both groups. In addition, the psychophysi-ological insomnia symptoms decreased in the control group (p = 0.026) and severity of insomnia in the ex-perimental group (p = 0.002).
In the report of anxiety symptoms, there were no differences between groups, but in depression symp-toms, there was a reduction of four points in the control group (p = 0.018) and five points in the experimental (p = 0.016), as shown in table 2.
Based on the analysis of the effect size (Cohen’s d), both CES and placebo had a positive effect in reducing the symptoms, but at different levels. For the insomnia index the effect was strong in the CES group (d = 0.88) and moderated in the placebo group (d = 0.52). For symptoms of anxiety, the effect was modest with the CES (d = 0.54) and moderated with placebo (d = 0.35). In both groups the effect size of depression was mod-erated (d = 0.69, and d = 0.58, respectively).
Discussion
It is suggested that the CES can have positive effects over the symptoms of anxiety, insomnia, and depression due to its influence on the limbic system
and the autonomic nervous system, interconnected with the hypothalamic-pituitary-adrenal-immune axis32. However, our results, after low-voltage CES, suggest a variety on the effects on the symptoms of anxiety, de-pression, and insomnia. In this sense, the increase of an hour of sleep and decrease the severity of insomnia as a result of the CES are observed, but psychophys-iological insomnia symptoms reduced as the result of a placebo effect. Symptoms of anxiety and depression decreased in CES group, but they were not superior to placebo group.
The increase in the time dedicated to sleep during the week supports the hypothesis that the CES changed the perception of sleep. However, there are no changes in bedtime schedules and get up to match this in-crease. Reporting sleeping an extra hour as the effect of the CES was consistent with the results previously obtained16. It is noteworthy that even with an increase of an hour of sleep (from 5 to 6 h), they are below rec-ommended hours of sleep time33. Possibly, these re-sults can increase by extending the number of sessions of CES. In addition, it is proposed to consider that the application of the CES should be accompanied by strat-egies such as hygiene of sleep and therapy cognitive behavior to improve the effectiveness of the CES and maintain longer the positive effects on sleep34.
In relation with insomnia, our results are similar to the results of a meta-analysis study that suggests that the CES is effective for the treatment of insomnia se-verity35. However, we recommend to obtain objective sleep measurements to establish the physiological mechanism associated with clinical changes. Our re-sults indicate that some types of insomnia such as the psychophysiological may improve as a result of the placebo effect. Psychophysiological insomnia is char-acterized by concerns over not being able to sleep, occurring particularly at the time of going to bed2. Fur-thermore, it is possible that placebo shifted the focus of attention: the concern to the concentration in the sense of the device, providing relaxation to fall asleep.
In relation to anxiety, some authors have suggested that the CES technique should not be used in the treat-ment of their symptoms unless that is used for its value as placebo36. In our study, the effect of CES improved the symptoms of anxiety, as it has been reported in the previous studies, but the effect was similar to the pla-cebo’s when analyzed the results considering the statistical significance, no statistical differences were observed. Similar results in different studies are dis-cussed based on statistical significance, however, anal-ysis with an alternative statistic as the d Cohen31 may
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020
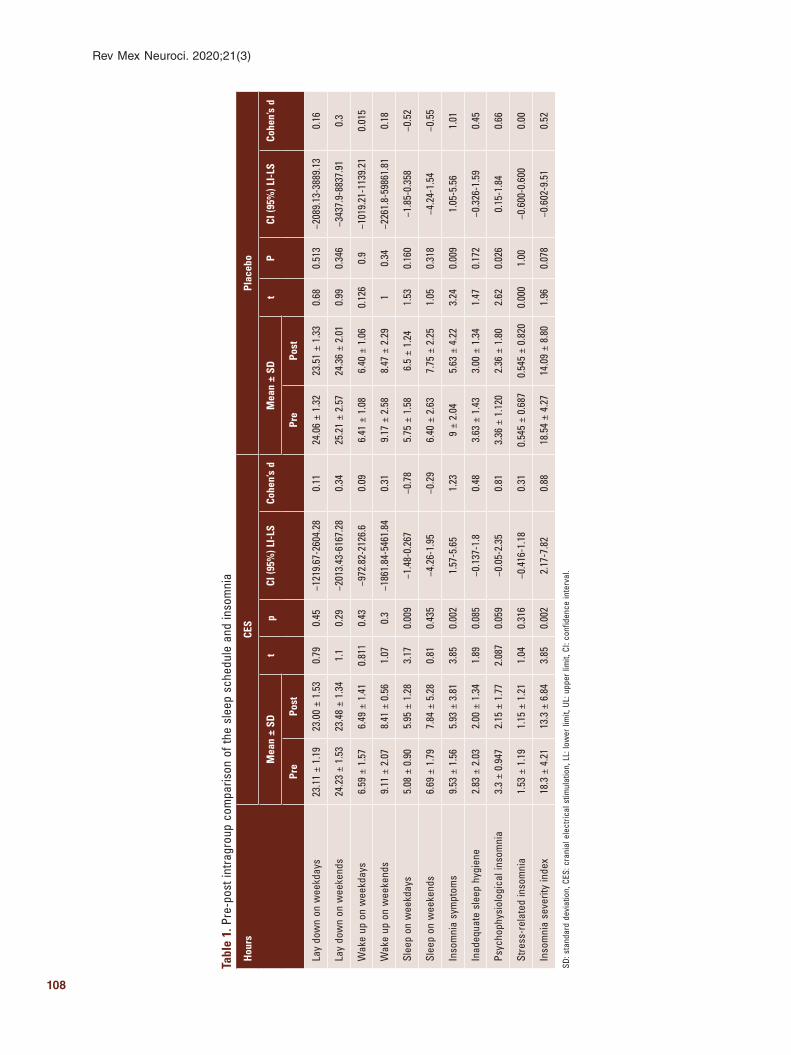
108
Rev Mex Neuroci. 2020;21(3)
Tabl
e 1.
Pre
-pos
t int
ragr
oup
com
paris
on o
f the
sle
ep s
ched
ule
and
inso
mni
a
Hou
rsCE
SPl
aceb
o
Mea
n ±
SDt
pCI
(95%
) LI-
LSCo
hen’
s d
Mea
n ±
SDt
PCI
(95%
) LI-
LSCo
hen’
s d
Pre
Post
Pre
Post
Lay
dow
n on
wee
kday
s23
.11
± 1.
1923
.00
± 1.
530.
790.
45−1
219.
67-2
604.
280.
1124
.06
± 1.
3223
.51
± 1.
330.
680.
513
−208
9.13
-388
9.13
0.16
Lay
dow
n on
wee
kend
s24
.23
± 1.
5323
.48
± 1.
341.
10.
29−2
013.
43-6
167.
280.
3425
.21
± 2.
5724
.36
± 2.
010.
990.
346
−343
7.9-
8837
.91
0.3
Wak
e up
on
wee
kday
s6.
59 ±
1.5
76.
49 ±
1.4
10.
811
0.43
−972
.82-
2126
.60.
096.
41 ±
1.0
86.
40 ±
1.0
60.
126
0.9
−101
9.21
-113
9.21
0.01
5
Wak
e up
on
wee
kend
s9.
11 ±
2.0
78.
41 ±
0.5
61.
070.
3−1
861.
84-5
461.
840.
319.
17 ±
2.5
88.
47 ±
2.2
91
0.34
−226
1.8-
5986
1.81
0.18
Slee
p on
wee
kday
s5.
08 ±
0.9
05.
95 ±
1.2
83.
170.
009
−1.4
8-0.
267
−0.7
85.
75 ±
1.5
86.
5 ±
1.24
1.53
0.16
0−1
.85-
0.35
8−0
.52
Slee
p on
wee
kend
s6.
69 ±
1.7
97.
84 ±
5.2
80.
810.
435
−4.2
6-1.
95−0
.29
6.40
± 2
.63
7.75
± 2
.25
1.05
0.31
8−4
.24-
1.54
−0.5
5
Inso
mni
a sy
mpt
oms
9.53
± 1
.56
5.93
± 3
.81
3.85
0.00
21.
57-5
.65
1.23
9 ±
2.04
5.63
± 4
.22
3.24
0.00
91.
05-5
.56
1.01
Inad
equa
te s
leep
hyg
iene
2.83
± 2
.03
2.00
± 1
.34
1.89
0.08
5−0
.137
-1.8
0.48
3.63
± 1
.43
3.00
± 1
.34
1.47
0.17
2−0
.326
-1.5
90.
45
Psyc
hoph
ysio
logi
cal i
nsom
nia
3.3
± 0.
947
2.15
± 1
.77
2.08
70.
059
−0.0
5-2.
350.
813.
36 ±
1.1
202.
36 ±
1.8
02.
620.
026
0.15
-1.8
40.
66
Stre
ss-r
elat
ed in
som
nia
1.53
± 1
.19
1.15
± 1
.21
1.04
0.31
6−0
.416
-1.1
80.
310.
545
± 0.
687
0.54
5 ±
0.82
00.
000
1.00
−0.6
00-0
.600
0.00
Inso
mni
a se
verit
y in
dex
18.3
± 4
.21
13.3
± 6
.84
3.85
0.00
22.
17-7
.82
0.88
18.5
4 ±
4.27
14.0
9 ±
8.80
1.96
0.07
8−0
.602
-9.5
10.
52
SD: s
tand
ard
devi
atio
n, C
ES: c
rani
al e
lect
rical
stim
ulat
ion,
LL:
low
er li
mit,
UL:
upp
er li
mit,
CI:
conf
iden
ce in
terv
al.
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020
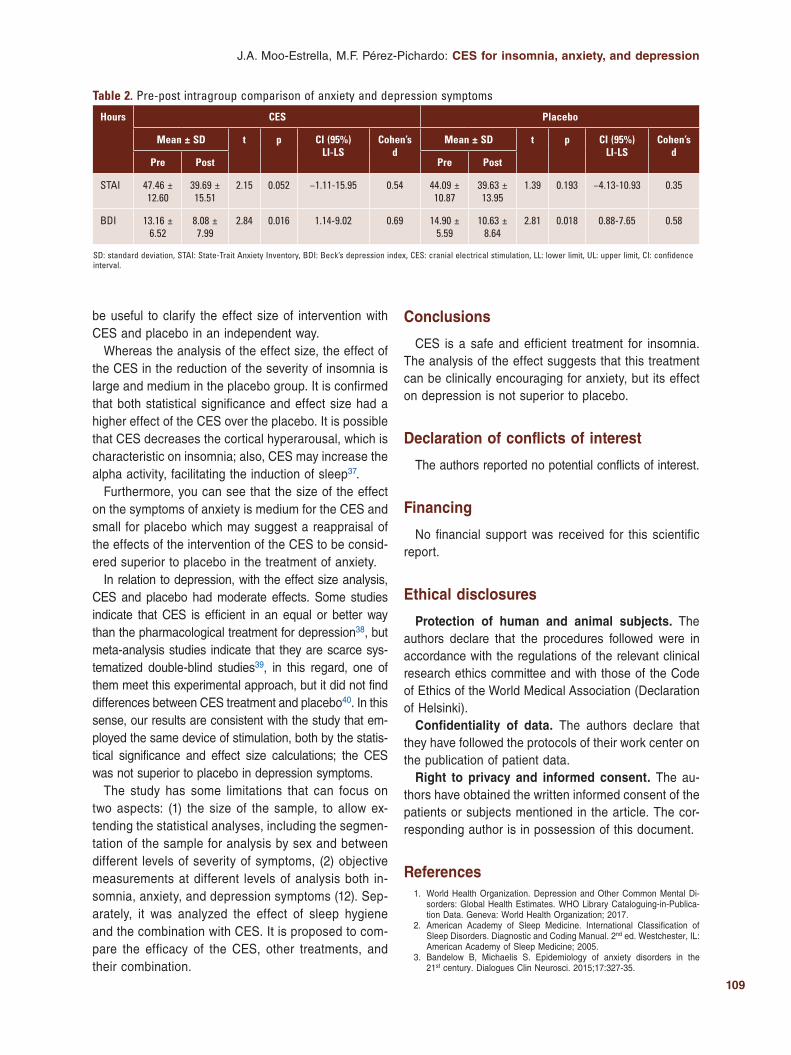
109
J.A. Moo-Estrella, M.F. Pérez-Pichardo: CES for insomnia, anxiety, and depression
Conclusions
CES is a safe and efficient treatment for insomnia. The analysis of the effect suggests that this treatment can be clinically encouraging for anxiety, but its effect on depression is not superior to placebo.
Declaration of conflicts of interest
The authors reported no potential conflicts of interest.
Financing
No financial support was received for this scientific report.
Ethical disclosures
Protection of human and animal subjects. The authors declare that the procedures followed were in accordance with the regulations of the relevant clinical research ethics committee and with those of the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Confidentiality of data. The authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consent. The au-thors have obtained the written informed consent of the patients or subjects mentioned in the article. The cor-responding author is in possession of this document.
References 1. World Health Organization. Depression and Other Common Mental Di-
sorders: Global Health Estimates. WHO Library Cataloguing-in-Publica-tion Data. Geneva: World Health Organization; 2017.
2. American Academy of Sleep Medicine. International Classification of Sleep Disorders. Diagnostic and Coding Manual. 2nd ed. Westchester, IL: American Academy of Sleep Medicine; 2005.
3. Bandelow B, Michaelis S. Epidemiology of anxiety disorders in the 21st century. Dialogues Clin Neurosci. 2015;17:327-35.
be useful to clarify the effect size of intervention with CES and placebo in an independent way.
Whereas the analysis of the effect size, the effect of the CES in the reduction of the severity of insomnia is large and medium in the placebo group. It is confirmed that both statistical significance and effect size had a higher effect of the CES over the placebo. It is possible that CES decreases the cortical hyperarousal, which is characteristic on insomnia; also, CES may increase the alpha activity, facilitating the induction of sleep37.
Furthermore, you can see that the size of the effect on the symptoms of anxiety is medium for the CES and small for placebo which may suggest a reappraisal of the effects of the intervention of the CES to be consid-ered superior to placebo in the treatment of anxiety.
In relation to depression, with the effect size analysis, CES and placebo had moderate effects. Some studies indicate that CES is efficient in an equal or better way than the pharmacological treatment for depression38, but meta-analysis studies indicate that they are scarce sys-tematized double-blind studies39, in this regard, one of them meet this experimental approach, but it did not find differences between CES treatment and placebo40. In this sense, our results are consistent with the study that em-ployed the same device of stimulation, both by the statis-tical significance and effect size calculations; the CES was not superior to placebo in depression symptoms.
The study has some limitations that can focus on two aspects: (1) the size of the sample, to allow ex-tending the statistical analyses, including the segmen-tation of the sample for analysis by sex and between different levels of severity of symptoms, (2) objective measurements at different levels of analysis both in-somnia, anxiety, and depression symptoms (12). Sep-arately, it was analyzed the effect of sleep hygiene and the combination with CES. It is proposed to com-pare the efficacy of the CES, other treatments, and their combination.
Table 2. Pre-post intragroup comparison of anxiety and depression symptoms
Hours CES Placebo
Mean ± SD t p CI (95%) LI-LS
Cohen’s d
Mean ± SD t p CI (95%) LI-LS
Cohen’s d
Pre Post Pre Post
STAI 47.46 ± 12.60
39.69 ± 15.51
2.15 0.052 −1.11-15.95 0.54 44.09 ± 10.87
39.63 ± 13.95
1.39 0.193 −4.13-10.93 0.35
BDI 13.16 ± 6.52
8.08 ± 7.99
2.84 0.016 1.14-9.02 0.69 14.90 ± 5.59
10.63 ± 8.64
2.81 0.018 0.88-7.65 0.58
SD: standard deviation, STAI: State-Trait Anxiety Inventory, BDI: Beck’s depression index, CES: cranial electrical stimulation, LL: lower limit, UL: upper limit, CI: confidence interval.
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

110
Rev Mex Neuroci. 2020;21(3)
4. Lim GY, Tam WW, Lu Y, Ho CS, Zhang MW, Ho RC. Prevalence of depression in the community from 30 countries between 1994 and 2014. Sci Rep. 2018;8:2861.
5. Morin CM, Benca R. Chronic insomnia. Lancet. 2012;379:1129-41. 6. Craske MG, Stein MB. Anxiety. Lancet. 2016;388:3048-59. 7. Moo-Estrella J, Pérez-Benítez H, Solís-Rodríguez F, Arankowsky-San-
doval G. Evaluation of depressive symptoms and sleep alterations in college students. Arch Med Res. 2005;36:393-8.
8. Bouscoulet LT, Vázquez-García JC, Muiño A, Márquez M, López MV, de Oca MM, et al. Prevalence of sleep related symptoms in four Latin Ame-rican cities. J Clin Sleep Med. 2008;4:579-85.
9. Bonnet MH, Arand DL. Hyperarousal and insomnia: state of the science. Sleep Med Rev. 2010;14:9-15.
10. Levenson JC, Kay DB, Buysse DJ. The pathophysiology of insomnia. Chest. 2015;147:1179-92.
11. Huang YJ, Lane HY, Lin CH. New treatment strategies of depression: based on mechanisms related to neuroplasticity. Neural Plast. 2017;2017:4605971.
12. Farach FJ, Pruitt LD, Jun JJ, Jerud AB, Zoellner LA, Roy-Byrne PP. Pharmacological treatment of anxiety disorders: current treatments and future directions. J Anxiety Disord. 2012;26:833-43.
13. Paris J. The mistreatment of major depressive disorder. Can J Psychia-try. 2014;59:148-51.
14. Schweitzer PK, Feren SD. Pharmacological treatment of insomnia. In: Clinical Handbook of Insomnia. Berlin, Germany: Springer Science and Business Media; 2017.
15. Rose KM, Taylor AG, Bourguignon C. Effects of cranial electrical stimu-lation on sleep disturbances, depressive symptoms, and caregiving appraisal in spousal caregivers of persons with Alzheimer’s disease. Appl Nurs Res. 2009;22:119-25.
16. Lande RG, Gragnani C. Efficacy of cranial electric stimulation for the treatment of insomnia: a randomized pilot study. Complement Ther Med. 2013;21:8-13.
17. Camposo M, Oliva JC, Granero A, Palao DJ. Efectividad y coste-efecti-vidad de la terapia electroconvulsiva de mantenimiento: un análisis na-turalístico en espejo. Actas Esp Psiquiatr. 2017;45:257-67.
18. Goyatá SL, Avelino CC, Santos SV, Souza Junior DI, Gurgel MD, Terra Fde S. Effects from acupuncture in treating anxiety: integrative review. Rev Bras Enferm. 2016;69:602-9.
19. Farah WH, Alsawas M, Mainou M, Alahdab F, Farah MH, Ahmed AT, et al. Non-pharmacological treatment of depression: a systematic review and evidence map. Evid Based Med. 2016;21:214-21.
20. Liu S, Sheng J, Li B, Zhang X. Recent advances in non-invasive brain sti-mulation for major depressive disorder. Front Hum Neurosci. 2017;11:526.
21. Kirsch DL, Nichols F. Cranial electrotherapy stimulation for treatment of anxiety, depression, and insomnia. Psychiatr Clin North Am. 2013;36:169-76.
22. Antal A, Alekseichuk I, Bikson M, Brockmöller J, Brunoni AR, Chen R, et al. Low intensity transcranial electric stimulation: safety, ethical, legal regu-latory and application guidelines. Clin Neurophysiol. 2017;128:1774-809.
23. Shekelle PG, Shekelle P, Cook I, Miake-Lye IM, Mak S, Booth MS, et al. The Effectiveness and Risks of Cranial Electrical Stimulation for the Treatment of Pain, Depression, Anxiety, PTSD, and Insomnia: a Syste-matic Review. VA Evidence-based Synth Progr Reports. Washington, DC: Department of Veterans Affairs (US); 2018.
24. Food and Drug Administration. Summary of Basis of Approval, Neurolo-gical Devices. Vol. 21. Silver Spring, Maryland: food and Drug Adminis-tration; 1979. Available from: https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/cfrsearch.cfm?fr=882.5800 .
25. Feusner JD, Madsen S, Moody TD, Bohon C, Hembacher E, Bookheimer SY, et al. Effects of cranial electrotherapy stimulation on resting state brain activity. Brain Behav. 2012;2:211-20.
26. Kennerly R. QEEG analysis of cranial electrotherapy: a pilot study. J Neu-rother. 2004;8:112-3.
27. Morin CM, LeBlanc M, Bélanger L, Ivers H, Mérette C, Savard J. Preva-lence of insomnia and its treatment in Canada. Can J Psychiatry. 2011;56:540-8.
28. Spielberger CD, Gorsuch RL, Lushene RE. State-Trait Anxiety Inventory. Madrid: TEA; 1982.
29. Beck AT, Steer RA, Brown GK. Beck Depression Inventory. 2nd ed. Buenos Aires: Paidós; 2006.
30. Cohen J. A power primer. Psychol Bull. 1992;112:155-9. 31. Yennurajalingam S, Kang DH, Hwu WJ, Padhye NS, Masino C, Dibaj
SS, et al. Cranial electrotherapy stimulation for the management of depression, anxiety, sleep disturbance, and pain in patients with ad-vanced cancer: a preliminary study. J Pain Symptom Manage. 2018; 55:198-206.
32. Hirshkowitz M, Whiton K, Albert SM, Alessi C, Bruni O, DonCarlos L, et al. National Sleep Foundation’s updated sleep duration recommenda-tions: final report. Sleep Health. 2015;1:233-43.
33. Murawski B, Wade L, Plotnikoff RC, Lubans DR, Duncan MJ. A systema-tic review and meta-analysis of cognitive and behavioral interventions to improve sleep health in adults without sleep disorders. Sleep Med Rev. 2018;40:160-9.
34. Kirsch DL, Gilula MF. CES in the treatment of insomnia: a review and meta-analysis. Pract Pain Manage. 2007;7:30-43.
35. Passini FG, Watson CG, Herder J. The effects of cerebral electric thera-py (electrosleep) on anxiety, depression, and hostility in psychiatric pa-tients. J Nerv Ment Dis. 1976;163:263-6.
36. Kalmbach DA, Cuamatzi-Castelan AS, Tonnu CV, Tran KM, Anderson JR, Roth T, et al. Hyperarousal and sleep reactivity in insomnia: current in-sights. Nat Sci Sleep. 2018;10:193-201.
37. Gilula MF, Kirsch DL. Cranial electrotherapy stimulation review: a safer alternative to psychopharmaceuticals in the treatment of depression. J Neurother. 2005;9:7-26.
38. Kavirajan HC, Lueck K, Chuang K. Alternating current cranial electrothe-rapy stimulation (CES) for depression. Cochrane Database Syst Rev. 2014;7:CD010521.
39. Mischoulon D, De Jong MF, Vitolo OV, Cusin C, Dording CM, Yeung AS, et al. Efficacy and safety of a form of cranial electrical stimulation (CES) as an add-on intervention for treatment-resistant major depressive di-sorder: a three week double blind pilot study. J Psychiatr Res. 2015; 70:98-105.
40. Bhardwaj M, Arumugam N, Gambhir S. Efficacy of cranial electrical sti-mulation and rational emotive behavior therapy in improving psychologi-cal illness among chronic stroke survivors: a pilot randomized controlled trial. Ann Indian Acad Neurol. 2018;21:188-92.
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020
111
Synapses and neural communication in neuropathological conditionsAlejandro Sánchez1*, Dora L. Flores2,3, Eugenio Leyva1, and Carlos Castro2
1Faculty of Sciences; 2Faculty of Engineering, Architecture and Design. Universidad Autónoma de Baja California, Ensenada, Baja California, Mexico; 3Department of Computer Science, Institute for Genomics and Bioinformatics and Center for Machine Learning and Intelligent Systems, University of California, Irvine, California, USA
Revista Mexicana de Neurociencia
REVIEW ARTICLE
Correspondence: *Alejandro Sánchez
E-mail: [email protected]
Date of reception: 10-10-2019
Date of acceptance: 31-01-2020
DOI: 10.24875/RMN.20000136
1665-5044/ © 2020. Academia Mexicana de Neurología A.C. Published by Permanyer. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/).
Available online: 18-05-2020
Rev Mex Neuroci. 2020;21(3):111-121
www.revmexneurociencia.com
Abstract
The central nervous system (CNS) is an extraordinary and complex communication network that receives voluminous amounts of information simultaneously but is vulnerable to disease and injury. This research emphasizes on the importance of gap junctions in neuropathological conditions and neurodegenerative diseases. Namely, we explore the degree of participation of chemical and electrical synapses within an updated panorama of integrative molecular techniques used for their study. The number of electrical and chemical synapses that coexist in the human brain is unknown, yet they are present in almost all types of cells. Frequently, electrical and chemical synapses are found separately, yet sometimes mixed electrical-chemical synapses are found coupled or together. Unfortunately, synaptic dysfunction has adverse effects on organs and vital structu-res. In this review, we discuss the most common diseases derived from synaptic dysfunction, as well as their occurrence in Mexico. Similarly, we discuss current treatments for diseases involving human connexins. Studies on the CNS are important to understand how this system works and explain current action mechanisms used as treatments of neuropathologies.
Key words: Gap junctions. Nervous system. Neuropathologies.
Sinapsis y comunicación neuronal en afecciones neuropatológicas
Resumen
El sistema nervioso central (SNC) es una red de comunicación extraordinaria y compleja que recibe cantidades voluminosas de información simultáneamente, pero es vulnerable a enfermedades y lesiones. Esta investigación enfatiza la importancia de las uniones gap en condiciones neuropatológicas y enfermedades neurodegenerativas. A saber, exploramos el grado de participación de las sinapsis químicas y eléctricas dentro de un panorama actualizado de las técnicas moleculares integra-tivas utilizadas para su estudio. Se desconoce la cantidad de sinapsis eléctricas y químicas que coexisten en el cerebro humano, pero están presentes en casi todos los tipos de células. Con frecuencia, las sinapsis eléctricas y químicas se en-cuentran por separado, aunque a veces las sinapsis mixtas quimicoeléctricas se encuentran acopladas. Desafortunadamen-te, la disfunción sináptica tiene efectos adversos en los órganos y las estructuras vitales. En esta revisión discutimos las enfermedades más comunes derivadas de la disfunción sináptica, así como su ocurrencia en México. Del mismo modo, discutimos los tratamientos actuales para padecimientos neurológicos que involucran conexinas humanas. Los estudios
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

112
Rev Mex Neuroci. 2020;21(3)
Introduction
The nervous system has five forms of communication: mechanical signaling, electrical signaling, short-range signaling, local signaling, and long-range signaling. Me-chanical signaling involves adhesion and recognition, whereas electrical signaling is triggered by electrical synapses and gap junctions (GJs). Short-range signaling occurs thanks to chemical synapses and neurotransmit-ters, local signaling is triggered by hemichannels, and finally, long-range signaling involves neurohormones1,2.
In most animal cells, except isolated moving cells, intracellular channels are formed between the cyto-plasm of adjacent cells. These channels ensure the exchange of ions, metabolites, and other messenger molecules, but they also mediate electrical coupling among connected cells3,4. Similarly, specific intracellu-lar channels are formed by multi-protein complexes, commonly known as GJs. Pathologies affecting GJs have adverse effects on vital organs, senses, and bones.
There are three families of unrelated proteins that are involved in electric synapses connexins, pannexins, and innexins (Fig. 1). The family of connexins comprises 20 members which are found only in chordates4, and some of them are expressed in the central nervous system (CNS)5. On the other hand, pannexins are found in ver-tebrates, and innexins exist only in invertebrates.
A GJ channel is formed by two hemichannels, each from one of two neighboring cells, leaving a narrow 2-4 nm gap between them. Furthermore, some hemi-channels only serve as a backdoor to important metab-olites. Studies on the functional role of innexins in the nervous system of invertebrates generate results that are applicable to all animal species, particularly mam-mals. Therefore, in this review, we emphasize on the importance of invertebrate animal models, namely, Hirudo medicinalis, to study synaptic function and thus respond to complex questions in neuroscience. Simi-larly, we present a panorama of neurological disorders, in which synaptic dysfunction is a characteristic. Then, we compare this information to that reported in the lit-erature about human connexins and current treatments of human neurological diseases.
Hirudo development of the nervous system
It is well-known that molecular interactions influence the development of virtually all types of cells, including nerve cells, during embryogenesis6,7. GJs are consid-ered as important mediators of cell communication8. In fact, research has demonstrated that GJs play a key role in the development and preservation of nerve cells: GJ inhibition causes progenitor cells to cease prolifera-tion, thus leading to cell differentiation, or even death9. Cells can affect one another and promote growth. Elec-trical synapses work both during the development of the nervous system and in adulthood. If an innexin is ecto-pically expressed, it creates new connections with ad-jacent neurons, thus forming new communication chan-nels. However, if some innexins are blocked, new channels cannot be formed (Fig 2)9.
H. medicinalis is a well-known species of the genus Hirudo and the family of Hirudinidae; however, it is usually confused with another leech species, Hirudo verbana, mainly due to their physical resemblance and similar behavior (Fig 1). Due to the size of its neurons and the structure of its nervous system, H. medicinalis is a popular model in biology. It is used to study neu-ron-to-neuron communication, specifically GJs. The nervous system of H. medicinalis comprises 32 gan-glia, which is considered as motor brains and contains 400 neurons of approximately 10-50 μ in diameter. These characteristics make H. medicinalis neurons more accessible to neuroscience studies. Furthermore, ganglia six and seven contain the male and female sexual organs of this species, respectively9.
Important cells of the nervous system
GJs take part in electrical coupling and contribute to synapse regeneration after neuronal injury. There is an average of ten glial cells or neuroglia per neuron, which makes them the most abundant cell types in the CNS. Glial cells comprise macroglia (astrocytes and oligo-dendrocytes), microglia, and ependymal cells. Astro-cytes are associated with the majority of neurological disorders and diseases, such as brain ischemia, Alz-heimer’s disease (AD), and epilepsy. Similarly, GJs can be related to the malignant degree and metastasis of
sobre el SNC son importantes para comprender cómo funciona este sistema y explicar los mecanismos de acción actuales utilizados como tratamientos de neuropatologías.
Palabras clave: Uniones de hendidura. Sistema nervioso. Neuropatologías.
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020
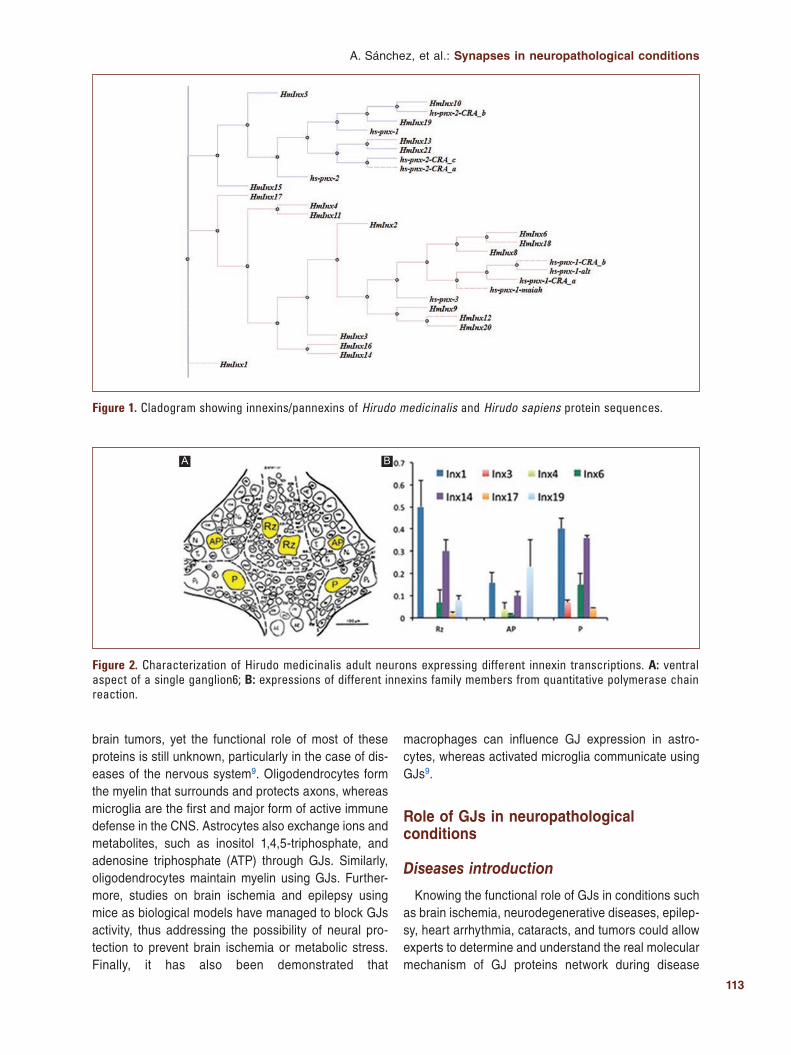
113
A. Sánchez, et al.: Synapses in neuropathological conditions
brain tumors, yet the functional role of most of these proteins is still unknown, particularly in the case of dis-eases of the nervous system9. Oligodendrocytes form the myelin that surrounds and protects axons, whereas microglia are the first and major form of active immune defense in the CNS. Astrocytes also exchange ions and metabolites, such as inositol 1,4,5-triphosphate, and adenosine triphosphate (ATP) through GJs. Similarly, oligodendrocytes maintain myelin using GJs. Further-more, studies on brain ischemia and epilepsy using mice as biological models have managed to block GJs activity, thus addressing the possibility of neural pro-tection to prevent brain ischemia or metabolic stress. Finally, it has also been demonstrated that
macrophages can influence GJ expression in astro-cytes, whereas activated microglia communicate using GJs9.
Role of GJs in neuropathological conditions
Diseases introduction
Knowing the functional role of GJs in conditions such as brain ischemia, neurodegenerative diseases, epilep-sy, heart arrhythmia, cataracts, and tumors could allow experts to determine and understand the real molecular mechanism of GJ proteins network during disease
Figure 1. Cladogram showing innexins/pannexins of Hirudo medicinalis and Hirudo sapiens protein sequences.
Figure 2. Characterization of Hirudo medicinalis adult neurons expressing different innexin transcriptions. A: ventral aspect of a single ganglion6; B: expressions of different innexins family members from quantitative polymerase chain reaction.
A B
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

114
Rev Mex Neuroci. 2020;21(3)
processes, a practical separation of diseases based on the type of synapse involved, to simplify their study. Consequently, it could also help design treatments to successfully eliminate these conditions. Connexins and pannexins are key proteins to the bone and skeletal muscle development, maintenance, and regeneration. Research has found that connexin channels are pres-ent in the bone among osteoblasts, osteoclasts, and osteocytes. Similarly, connexins are important for bone growth and adaptation10.
The permeability of GJ channels is increased by multiple factors, including low pH levels, high cytosolic free calcium levels, and voltage gradient across the GJ. In vertebrate species, embryonic tissues are easily dis-sociated by treating them with low concentrations of a proteolytic enzyme, such as trypsin, along with a diva-lent-cation chelator, such as ethylenediaminetetraacetic acid, to disrupt the protein-protein interactions that hold the cells together.
The connection between cancer development and GJs was first reported by Loewenstein and Kanno when they studied liver cancer using electrophysiology techniques in 196611. Twenty-four years later, it was already estab-lished that GJ mutations were linked to multiple human genetic diseases12. Nowadays, connexins are known to be related to the development of conditions such as hearing loss, skin disorders, congenital cataracts and other vision disorders, heart arrhythmia, demyelinating diseases, and oculodentodigital dysplasia13.
Although the exact percentage of electrical, chemi-cal, or combined synapse participation is currently un-known, a simplification would help unravel the workings of opening neuronal communication channels during different conditions and would allow progress in these areas. At the molecular level, cellular communication plays a decisive role in the development or treatment of these diseases, and of course, the channels through which these signal molecules travel (Fig 3).
Brain ischemia
Cerebrovascular ischemia, or brain ischemia, oc-curs when there is insufficient blood flow to the brain. It leads to limited oxygen supply and can cause the death of brain cells. The side of the ischemic lesion has the same physiopathological mechanism and lo-cal consequences with different clinical manifesta-tions, its severity, and its duration, yet sufferers can risk death. When a person presents symptoms of brain ischemia, they must receive emergency treat-ment. Even a temporary deficit in oxygen supply can impair the brain, when the brain is damaged as a result of ischemia, the consequences are severe (i.e., physical or mental disability or death). In fact, cerebrovascular diseases such as brain ischemia are a leading cause of death in the USA. Cerebral vascu-lar disease is ranked as the second leading cause of death (9.7%) in Mexico.
Figure 3. A: internal view of Hirudo medicinalis ganglion through epifluorescence using Lucifer yellow injection, neuropil is illuminated, B: internal view of H. medicinalis ganglion through epifluorescence using Neurobiotin, entire ganglion is illuminated, C: superposition of previous images, showing neuropil location in ganglion, D: ventral view of H. medicinalis ganglion – upper side corresponds to the organism’s anterior connective tissue, E: control ganglion, red: TMR-dextran, green: Neurobiotin, F: visualization of the structure of a touch-sensitive neuron (T neuron) in ganglion using Neurobiotin.
A
D E F
B C
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

115
A. Sánchez, et al.: Synapses in neuropathological conditions
The functional role of astrocytes and GJs in brain ischemia is still unclear, yet the two are known to fulfill a potentially neuroprotective function that involves isch-emic tolerance and remodeling of neuronal networks by phagocytosis14. Experiments using cell culture tech-niques have demonstrated that blocking GJs in astro-cytes make the cells more vulnerable to glutamate cy-totoxicity15. Likewise, using hippocampal slice cultures, it was found that blocking GJs cause neuronal damage in ischemic conditions, such as oxygen and glucose deprivation16. GJs channels are known to remain open during these conditions17.
The most promising strategy for evaluating the func-tional role of connexins involves blocking them using interfering RNA, drugs such as carbenoxolone (CBX), and mimetic peptides, including Gap 19 and Gap 1617. Yet any state of overregulation can lead to microglial activation and neuroinflammation18. This strategy can help experts identify which connexins are implicated in apoptosis and inflammation. Consequently, it would be possible for scientists to develop new treatment options for brain ischemia. To date, Connexin 43 (Cx43) is the most promising connexin19. Cx43 expression is sensitive to neuronal injury and can be detected as early as 2 h post permanent middle cerebral artery occlusion (pM-CAO). These findings underscore Cx43 GJ as a poten-tial early target for therapeutic intervention in ischemic stroke. Cx43 is potentially a useful early marker to de-lineate and investigate the ischemia progression19.
Epilepsy
Leading causes of epilepsy include infectious diseas-es and abnormal brain development. Epilepsy is a neu-rological disorder that develops as a result of abnormal brain function, neural communication anomalies, or im-balanced neurotransmitters – which are responsible for neurotransmission (i.e., communication between neu-rons). Hence, epilepsy occurs when neurons occasion-ally send abnormal signals in the brain20.
After a head injury, brain stroke, or any other acci-dent, the brain might try to self-repair; however, this process can accidentally lead to abnormal brain con-nections, and thus epilepsy. During the epileptic crisis, many neurons send signals at the same time – as many as 500 times/s. This event causes changes in a per-son’s behavior, movements, feelings, and levels of con-sciousness. Nowadays, epilepsy is referred to as a spectrum of disorders with a myriad of causes, sever-ities, and effects. Some people may experience con-vulsions or lose consciousness, whereas others may
simply stop what they are doing, have a short lapse of awareness, and stare into space for a moment without knowing what is happening around them20.
In general, a person is considered to have epilepsy after two unprovoked seizures; a “seizure” is a parox-ysmal alteration of neurologic function caused by the excessive, hypersynchronous discharge of neurons in the brain, separated by at least 24 h. Provoked seizures are caused by known precipitating factors, such as high fever, nervous system infections, acute traumatic brain injury, or fluctuations in blood sugar, or electrolyte lev-els. To date, nearly 2.3 million adults and 450,000 chil-dren and adolescents in the US suffer from epilepsy. In Mexico, there are about 2 million people with epilep-sy, according to the Ministry of Health. Anyone can have epilepsy, men and women, regardless of their race, ethnicity, or age.
There are also severe cases of epilepsy, such as Dravet syndrome. This is a rare but lifelong dysfunction of the brain characterized by medically refractory sei-zures and causing serious learning disabilities. Current medications can control epilepsy in 60% of sufferers, whereas the remaining 40% experience what is com-monly known as drug-resistant epilepsy. Nowadays, treatment options for epilepsy include about 20 differ-ent types of drugs, special diets, and surgical techniques, and medical specialty like neurosurgery. Common tests for epilepsy diagnosis include imaging and monitoring techniques (e.g., electroencephalogra-phy and magnetoencephalography), patient medical history, blood tests, behavioral tests, and neurological exams. Cx43 is related to cryptogenic epilepsy that is defined as a group of focal or generalized epilepsy, which are believed to be symptomatic of a histopatho-logical or cellular occult alteration, but not of a genetic nature21.
Research has found that Cx43 in GJs21 and hemi-channels22 adversely affects astrocyte function, there-by causing epileptic seizures, which in turn induce Cx43 expression23. On the other hand, changes in Con-nexin 36 (Cx36) expression cause cell death24 and neural communication anomalies, thus resulting in ep-ilepsy25. Furthermore, GJs in astrocytes play a crucial role in ionic regulation; particularly, they can change the concentration of potassium ions. Changes in the strength of GJ coupling can cause neuronal hyperex-citability, and consequently, spontaneous epileptic ac-tivity26, which ultimately leads to astrocyte uncoupling. Finally, there is evidence that pannexin 1 (Panx1) con-tributes to the maintenance of epileptic seizures by releasing ATP. The absence of Panx1 in astrocytes
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

116
Rev Mex Neuroci. 2020;21(3)
potentiates seizure manifestation due to low levels of adenosine kinase, whereas the absence of Panx1 in neurons reduces seizure manifestation27.
GJ blockers to treat epilepsy
In a recent research Scemes et al.28, they studied 13 GJ blockers as treatment options for epilepsy: CBX, quinine, mefloquine, quinidine, anandamide, oleamide, heptanol, octanol, meclofenamic acid, niflumic acid, flufenamic acid, glycyrrhetinic acid, and retinoic acid. In the in vitro experiments, all these compounds demonstrated to have anticonvulsant effects in brain slices. The blockers modified the behavioral parame-ters related to seizures induced by 4-aminopyridine, pentylenetetrazol, pilocarpine, penicillin, and maximal electroshock. Similar research works suggest that GJ blockers are a future alternative for the treatment of epilepsy. Nevertheless, most of these compounds have been discontinued as treatments due to their side ef-fects, thus implying that further research must be con-ducted to identify the action mechanisms for neuro-logical disorders such as epilepsy (Table 1).
Multiple studies on connexins have been conducted with the aim of understanding and reporting the devas-tating effects of connexin dysfunctions (Table 2). Connexins are important, since they form synapses. Moreover, GJs are present in all biological cells, except spermatozoids, and some types of blood cells.
Neurodegenerative diseases
AD
AD is the most common degenerative disease, in México, approximately 800,000 people have AD. Clini-cally, AD is caused by cerebral atrophy of the frontal cortex, along with neurofibrillary tangle and large num-bers of senile plaques. The ApoE4 allele is usually seen as a risk factor for AD, yet health experts also look for other indicators. That is, not everybody carrying the ApoE4 gene variant will go onto develop AD as they grow old, although the probabilities are significantly higher. Moreover, some experts state that knowing that a person carries the ApoE4 allele does not benefit at all since none of the current treatment options cures the disease. ApoE gene polymorphic form ApoE4 (ε4) allele is the most commonly associated genetic risk factor linked with the late onset of the AD. In response to injury or neuroinflammation, Apoε4 undergoes neuron-specif-ic proteolysis. Even if it is not clear the relationship
between this allele and Cx43, it will be interesting to focus on Cx43 function under this condition28. Thus far, the relationship between AD and GJs remains unclear, yet glial cells are thought to contribute to the aggressive propagation of this disease by inhibiting cell communi-cation and promoting neuroinflammatory responses29. Moreover, scientific evidence suggests a relationship
between neurotoxicity of Aβ42 deposits in AD and up-regulation of Cx43 as a result of released neurotoxic molecules that cause oxidative stress30.
That said, researchers have found that Cx43 pre-vents, to some extent, the brain from deteriorating; however, Cx43 overexpression identified in experi-ments on AD-like pathologies30 seems to severely af-fect intercellular communication, thus relating Cx43 overexpression with neuroinflammation.
Cx43 also seems to be involved in glutamate excito-toxicity induced by manganese exposure, thus promot-ing neurodegenerative diseases, such as AD and Parkinson’s disease (PD). Moreover, in the relationship between GJ activity in glial cells and glutamate excito-toxicity, the latter is linked to excessive NMDAR activity and neurodegeneration31. That said, two promising treatments of AD include blocking specific GJs for Cx4332 and the Metabolic Enhancement for Neurode-generation (MEND) approach. MEND is a 36-point ther-apeutic personalized program including aspects such as medication, comprehensive dietary changes, vita-mins, brain stimulation, and exercise, to name but a few. There is a revision that mentions the importance of GJ in AD, their positive and negative role in neurons and other cell types, expressing that there is a need for further investigation in a GJ oriented treatment for AD33.
PD
PD is characterized by the loss of dopaminergic neu-rons in the part of the brain known as the substantia nigra (SN). There are no exact numbers of Parkinson’s patients in Mexico. However, the National Institute of Neurology and Neurosurgery estimates a prevalence of 50 new cases per 100,000 inhabitants/year. Clinical symptoms include shaking, rigidity or tremor, and motor disorders such as bradykinesia which means slowness of movement, and it is one of the cardinal symptoms of Parkinson’s (i.e., difficulty with walking). The 1-meth-yl-4-fenyl-1,2,3,6-tetrahydropyridine (MPTP) chemical model is used to represent the conditions of PD, and it causes permanent symptoms. MPTP is extensively modeled in mice and is characterized by overexpression of Cx43 in both the striatum and the astrocytic
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020
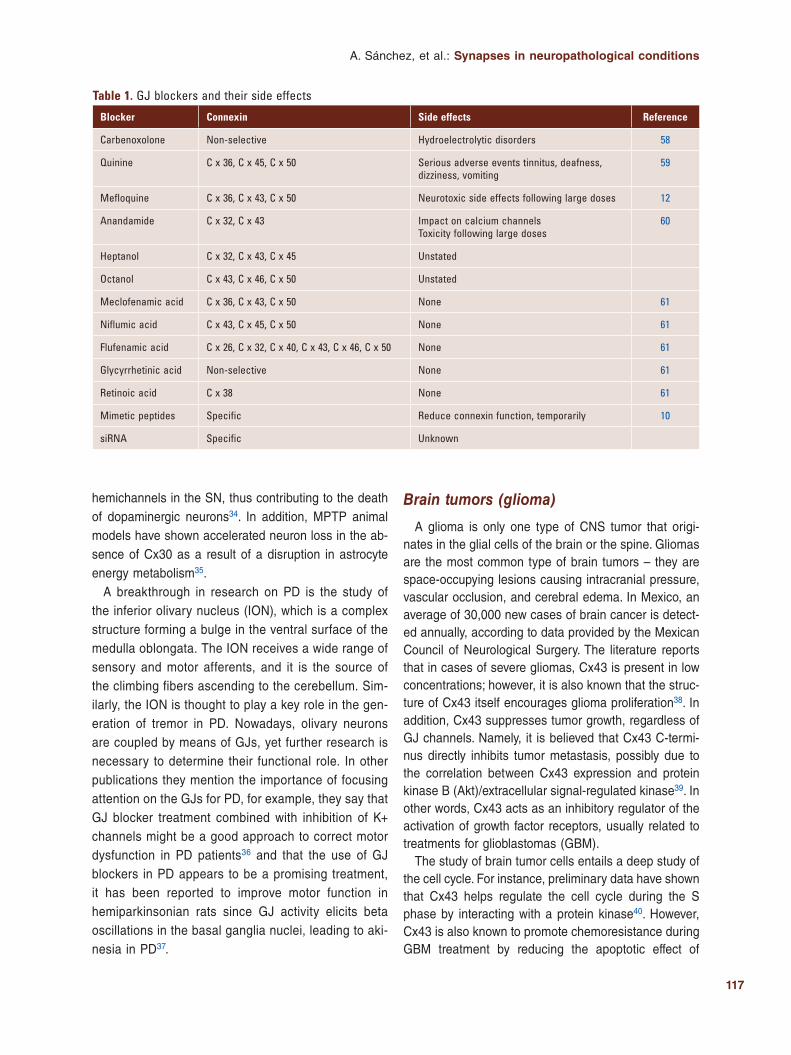
117
A. Sánchez, et al.: Synapses in neuropathological conditions
hemichannels in the SN, thus contributing to the death of dopaminergic neurons34. In addition, MPTP animal models have shown accelerated neuron loss in the ab-sence of Cx30 as a result of a disruption in astrocyte energy metabolism35.
A breakthrough in research on PD is the study of the inferior olivary nucleus (ION), which is a complex structure forming a bulge in the ventral surface of the medulla oblongata. The ION receives a wide range of sensory and motor afferents, and it is the source of the climbing fibers ascending to the cerebellum. Sim-ilarly, the ION is thought to play a key role in the gen-eration of tremor in PD. Nowadays, olivary neurons are coupled by means of GJs, yet further research is necessary to determine their functional role. In other publications they mention the importance of focusing attention on the GJs for PD, for example, they say that GJ blocker treatment combined with inhibition of K+ channels might be a good approach to correct motor dysfunction in PD patients36 and that the use of GJ blockers in PD appears to be a promising treatment, it has been reported to improve motor function in hemiparkinsonian rats since GJ activity elicits beta oscillations in the basal ganglia nuclei, leading to aki-nesia in PD37.
Brain tumors (glioma)
A glioma is only one type of CNS tumor that origi-nates in the glial cells of the brain or the spine. Gliomas are the most common type of brain tumors – they are space-occupying lesions causing intracranial pressure, vascular occlusion, and cerebral edema. In Mexico, an average of 30,000 new cases of brain cancer is detect-ed annually, according to data provided by the Mexican Council of Neurological Surgery. The literature reports that in cases of severe gliomas, Cx43 is present in low concentrations; however, it is also known that the struc-ture of Cx43 itself encourages glioma proliferation38. In addition, Cx43 suppresses tumor growth, regardless of GJ channels. Namely, it is believed that Cx43 C-termi-nus directly inhibits tumor metastasis, possibly due to the correlation between Cx43 expression and protein kinase B (Akt)/extracellular signal-regulated kinase39. In other words, Cx43 acts as an inhibitory regulator of the activation of growth factor receptors, usually related to treatments for glioblastomas (GBM).
The study of brain tumor cells entails a deep study of the cell cycle. For instance, preliminary data have shown that Cx43 helps regulate the cell cycle during the S phase by interacting with a protein kinase40. However, Cx43 is also known to promote chemoresistance during GBM treatment by reducing the apoptotic effect of
Table 1. GJ blockers and their side effects
Blocker Connexin Side effects Reference
Carbenoxolone Non-selective Hydroelectrolytic disorders 58
Quinine C x 36, C x 45, C x 50 Serious adverse events tinnitus, deafness, dizziness, vomiting
59
Mefloquine C x 36, C x 43, C x 50 Neurotoxic side effects following large doses 12
Anandamide C x 32, C x 43 Impact on calcium channelsToxicity following large doses
60
Heptanol C x 32, C x 43, C x 45 Unstated
Octanol C x 43, C x 46, C x 50 Unstated
Meclofenamic acid C x 36, C x 43, C x 50 None 61
Niflumic acid C x 43, C x 45, C x 50 None 61
Flufenamic acid C x 26, C x 32, C x 40, C x 43, C x 46, C x 50 None 61
Glycyrrhetinic acid Non-selective None 61
Retinoic acid C x 38 None 61
Mimetic peptides Specific Reduce connexin function, temporarily 10
siRNA Specific Unknown
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020
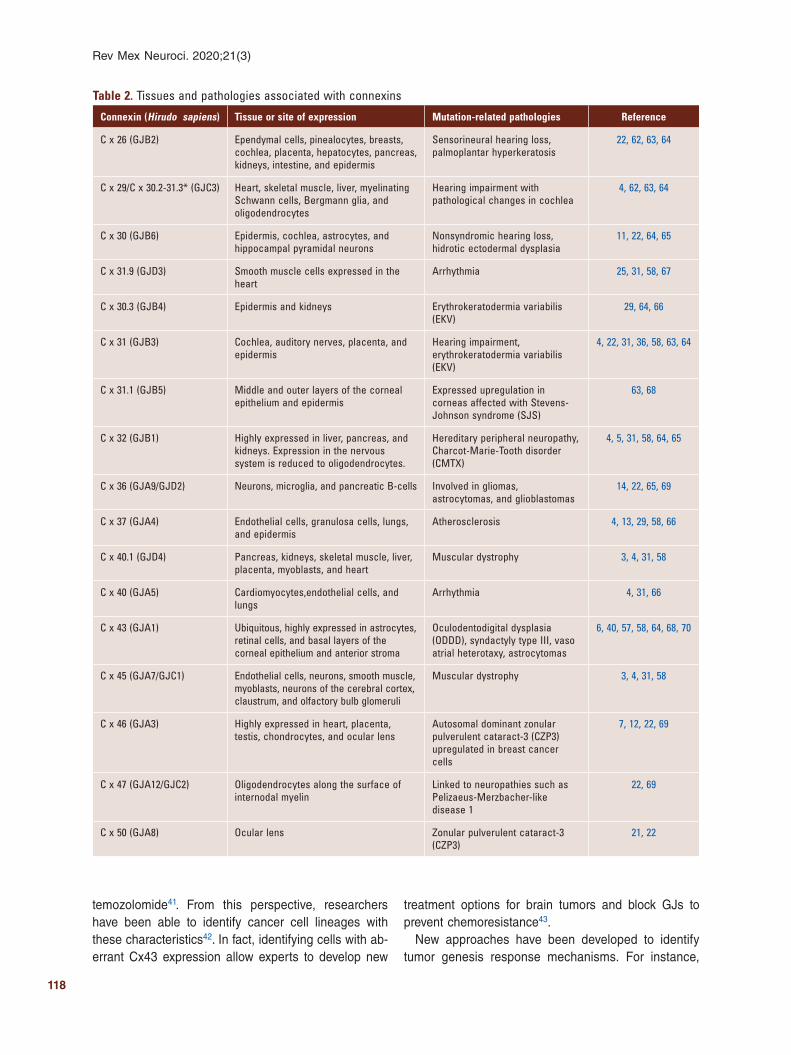
118
Rev Mex Neuroci. 2020;21(3)
temozolomide41. From this perspective, researchers have been able to identify cancer cell lineages with these characteristics42. In fact, identifying cells with ab-errant Cx43 expression allow experts to develop new
treatment options for brain tumors and block GJs to prevent chemoresistance43.
New approaches have been developed to identify tumor genesis response mechanisms. For instance,
Table 2. Tissues and pathologies associated with connexins
Connexin (Hirudo sapiens) Tissue or site of expression Mutation-related pathologies Reference
C x 26 (GJB2) Ependymal cells, pinealocytes, breasts, cochlea, placenta, hepatocytes, pancreas, kidneys, intestine, and epidermis
Sensorineural hearing loss, palmoplantar hyperkeratosis
22, 62, 63, 64
C x 29/C x 30.2-31.3* (GJC3) Heart, skeletal muscle, liver, myelinating Schwann cells, Bergmann glia, and oligodendrocytes
Hearing impairment with pathological changes in cochlea
4, 62, 63, 64
C x 30 (GJB6) Epidermis, cochlea, astrocytes, and hippocampal pyramidal neurons
Nonsyndromic hearing loss, hidrotic ectodermal dysplasia
11, 22, 64, 65
C x 31.9 (GJD3) Smooth muscle cells expressed in the heart
Arrhythmia 25, 31, 58, 67
C x 30.3 (GJB4) Epidermis and kidneys Erythrokeratodermia variabilis (EKV)
29, 64, 66
C x 31 (GJB3) Cochlea, auditory nerves, placenta, and epidermis
Hearing impairment, erythrokeratodermia variabilis (EKV)
4, 22, 31, 36, 58, 63, 64
C x 31.1 (GJB5) Middle and outer layers of the corneal epithelium and epidermis
Expressed upregulation in corneas affected with Stevens-Johnson syndrome (SJS)
63, 68
C x 32 (GJB1) Highly expressed in liver, pancreas, and kidneys. Expression in the nervous system is reduced to oligodendrocytes.
Hereditary peripheral neuropathy, Charcot-Marie-Tooth disorder (CMTX)
4, 5, 31, 58, 64, 65
C x 36 (GJA9/GJD2) Neurons, microglia, and pancreatic B-cells Involved in gliomas, astrocytomas, and glioblastomas
14, 22, 65, 69
C x 37 (GJA4) Endothelial cells, granulosa cells, lungs, and epidermis
Atherosclerosis 4, 13, 29, 58, 66
C x 40.1 (GJD4) Pancreas, kidneys, skeletal muscle, liver, placenta, myoblasts, and heart
Muscular dystrophy 3, 4, 31, 58
C x 40 (GJA5) Cardiomyocytes,endothelial cells, and lungs
Arrhythmia 4, 31, 66
C x 43 (GJA1) Ubiquitous, highly expressed in astrocytes, retinal cells, and basal layers of the corneal epithelium and anterior stroma
Oculodentodigital dysplasia (ODDD), syndactyly type III, vaso atrial heterotaxy, astrocytomas
6, 40, 57, 58, 64, 68, 70
C x 45 (GJA7/GJC1) Endothelial cells, neurons, smooth muscle, myoblasts, neurons of the cerebral cortex, claustrum, and olfactory bulb glomeruli
Muscular dystrophy 3, 4, 31, 58
C x 46 (GJA3) Highly expressed in heart, placenta, testis, chondrocytes, and ocular lens
Autosomal dominant zonular pulverulent cataract-3 (CZP3) upregulated in breast cancer cells
7, 12, 22, 69
C x 47 (GJA12/GJC2) Oligodendrocytes along the surface of internodal myelin
Linked to neuropathies such as Pelizaeus-Merzbacher-like disease 1
22, 69
C x 50 (GJA8) Ocular lens Zonular pulverulent cataract-3 (CZP3)
21, 22
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

119
A. Sánchez, et al.: Synapses in neuropathological conditions
laser scanning microscopy (confocal laser scanning microscopy) and simple molecule localization micros-copy are employed for the spatial localization of Cx43 in tumor genesis and the formation of metastasis44. Moreover, the literature reports epigenetic approaches for Cx26, Cx30, and Cx4345. In fact, cell homeostasis can help suppress gliomas, yet it is also theorized that tumor cells affect neighbor cells through GJs46,47, whereas increased GJ regulation decreases the prolif-eration of glioma cells48.
Autism
Autism spectrum disorder (ASD) is a developmental disorder whose causes are usually unknown. It is influ-enced by multiple factors across race, ethnicity, and socioeconomic status aspects. According to the litera-ture, in the USA, over 100 million families are affected by ASD. In 2017, around 1% of all children in Mexico, about 400,000 have autism. Recent evidence suggests that alterations of gut microbial-associated epitopes, including GJ alpha 1, can adversely affect the function of Cx4349. Such results associate gastrointestinal prob-lems in ASD with GJs and neuronal loss. In addition, research has found an increase in astrocytic Cx43 expression in a part of the brain’s frontal cortex (i.e. Brodmann area 9) of subjects with autism, thus suggesting abnormal glial-neuronal communication in brains of ASD sufferers. Finally, studies on brain con-nectivity relying on electrophysiological techniques have used H. medicinalis as a key model to reduce the expression of specific connexins. In humans, this could help find a way to reduce overconnectivity in the brains of subjects with autism50.
New studies have emerged to diagnose neuropathol-ogies with different novel approaches. Histochemistry was used to proper identify neurons, neuritic processes and axons, myelin sheaths, neuroglial cells, and con-nective tissue in the nervous system50. New strategies have been developed to predict ASD. One approach can be using genetic information contained in the Au-tism Genetic Resource Exchange; this database was used to predict the diagnostic of ASD in combination with an instrument of behavioral evaluation51. The other approach is the use of neuroimaging information which can be useful in the evaluation of psychiatric disorders. For ASD computational techniques were used to pro-cess magnetic resonance images of subjects with ASD and control groups52,53. There is no relationship be-tween neuroimaging and GJs. Neuroimaging can be used as alternative information to try to evaluate the
condition of a patient. Magnetic resonance procedures can be helpful to see the brain activity of patients with ASD. Moreover, computational techniques can be use-ful to process that information.
Symptom onset, genetic, and neuropathological data were examined from patients with Lewy body proteins to determine the relationship between those proteins and AD54. In addition, postmortem magnetic resonance was used to examine serial coronal sections, horizontal sections of brainstem, and cerebellum to find neuro-pathological lesions54,55.
Discussion
The study of both the nervous system and neuropa-thologies through integrative molecular neuroscience requires not only fully-equipped laboratories and key biological models – such as H. medicinalis – but also extensive training on techniques such as injection of individual neurons, nanoballistics, and confocal micros-copy, not to mention neuroimmunology and advanced histological techniques (Fig. 3).
Data show that connexin mimetic peptides can be used as GJ function blockers56,57 to disrupt innexin functions and to analyze the specific function and ac-tion of each member of the innexin family in H. me-dicinalis. In this sense, results from research on the nervous system of H. medicinalis can be extrapolated to understand the functional role of GJs in the nervous systems of other species, including vertebrates.
Conclusion
According to the World Health Organization (OMS), disability is a complex phenomenon that reflects a close and borderline relationship between the charac-teristics of the human being and the characteristics of the environment where he lives. It is a broad term that contains and encompasses deficiencies, limitations to perform certain activities, and restrictions on participa-tion. According to the National Human Rights Commis-sion (CNDH) in Mexico, disabilities are divided into motor, sensory, cognitive-intellectual, and psychosocial disabilities. If we analyze these disabilities at the cel-lular-molecular level, we can see a clear lack of cellular communication or defective communication between the neurons of the central and/or peripheral nervous system, a disconnection between different regions of the body.
The CNS plays a central role in the control of our bodily functions, yet failures in this system can cause multiple
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

120
Rev Mex Neuroci. 2020;21(3)
diseases and disabilities. Any CNS problem diagnosis is devastating. Studying GJs is important when trying to understand neuron-to-neuron communication. In fact, knowing and understanding the functional role of GJs in certain neuropathologies could allow experts to develop new treatment options to tackle such pathologies from the root cause. In this sense, H. medicinalis is a well-known model used in in vivo experiments on neurons, innexins, and neurotransmitters.
Our work demonstrates that cell communication through GJs and electrical/chemical synapses is close-ly related to neurological conditions. However, evidence suggests that turning off connexins causes collateral damage or side effects that do not benefit humans. Additional and deeper in vivo studies are needed for a medical breakthrough and to find treatment options to cure neurological diseases.
Funding
None.
Conflicts of interest
None.
Ethical disclosures
Protection of human and animal subjects. The authors declare that no experiments were performed on humans or animals for this study.
Confidentiality of data. The authors declare that they have followed the protocols of their work center on the publication of patient data.
Right to privacy and informed consent. The au-thors declare that no patient data appear in this article.
References 1. Bruzzone R, White TW, Paul DL. Connections with connexins: the mo-
lecular basis of direct intercellular signaling. Eur J Biochem. 1996; 238:1-27.
2. Chailakhyan LM. Ligand-receptor and junction-mediated cell-cell interac-tions: comparison of the two principles. Differentiation. 1990;45:1-6.
3. Chernet BT, Fields C, Levin M. Long-range gap junctional signaling controls oncogene-mediated tumorigenesis in Xenopus laevis embryos. Front Physiol. 2014;5:519.
4. Slivko-Koltchik GA, Kuznetsov VP, Panchin YV. Are there gap junctions without connexins or pannexins? BMC Evol Biol. 2019;19:46.
5. Esseltine JL, Laird DW. Next-generation connexin and pannexin cell biology. Trends Cell Biol. 2016;26:944-55.
6. Pereda AE. Electrical synapses and their functional interactions with chemical synapses. Nat Rev Neurosci. 2014;15:250-63.
7. Baranes K, Hibsh D, Cohen S, Yamin T, Efroni S, Sharoni A, et al. Comparing transcriptome profiles of neurons interfacing adjacent cells and nanopatterned substrates reveals fundamental neuronal interactions. Nano Lett. 2019;19:1451-9.
8. Mathews J, Levin M. Gap junctional signaling in pattern regulation: phy-siological network connectivity instructs growth and form. Dev Neurobiol. 2017;77:643-73.
9. Swayne LA, Bennett SA. Connexins and pannexins in neuronal develo-pment and adult neurogenesis. BMC Cell Biol. 2016;17 Suppl 1:10.
10. Plotkin LI, Davis HM, Cisterna BA, Sáez JC. Connexins and pannexins in bone and skeletal muscle. Curr Osteoporos Rep. 2017;15:326-34.
11. Loewenstein WR, Kanno Y. Intercellular communication and the control of tissue growth: lack of communication between cancer cells. Nature. 1966;209:1248-9.
12. Mesnil M, Aasen T, Boucher J, Chépied A, Cronier L, Defamie N, et al. An update on minding the gap in cancer. Biochim Biophys Acta Biomem-br. 2018;1860:237-43.
13. Laird DW, Naus CC, Lampe PD. SnapShot: connexins and disease. Cell. 2017;170:1260-0.
14. Koizumi S, Hirayama Y, Morizawa YM. New roles of reactive astrocytes in the brain; an organizer of cerebral ischemia. Neurochem Int. 2018;119:107-14.
15. Ozog MA, Bechberger JF, Naus CC. Ciliary neurotrophic factor (CNTF) in com-bination with its soluble receptor (CNTFRalpha) increases connexin43 expression and suppresses growth of C6 glioma cells. Cancer Res. 2002;62:3544-8.
16. Liu Z, Chopp M. Astrocytes, therapeutic targets for neuroprotection and neurorestoration in ischemic stroke. Prog Neurobiol. 2016;144:103-20.
17. Chen Y, Wang L, Zhang L, Chen B, Yang L, Li X, et al. Inhibition of connexin 43 hemichannels alleviates cerebral ischemia/reperfusion injury via the TLR4 signaling pathway. Front Cell Neurosci. 2018;12:372.
18. Yin X, Feng L, Ma D, Yin P, Wang X, Hou S, et al. Roles of astrocytic connexin-43, hemichannels, and gap junctions in oxygen-glucose depri-vation/reperfusion injury induced neuroinflammation and the possible regulatory mechanisms of salvianolic acid B and carbenoxolone. J Neu-roinflammation. 2018;15:97.
19. Freitas-Andrade M, She J, Bechberger J, Naus CC, Sin WC. Acute connexin43 temporal and spatial expression in response to ischemic stroke. J Cell Commun Signal. 2018;12:193-204.
20. National Institutes of Health. National Institute of Neurological Disorders and Stroke. Bethesda, MD: National Institutes of Health; 2019.
21. Shandra O, Winemiller AR, Heithoff BP, Munoz-Ballester C, George KK, Benko MJ, et al. Repetitive diffuse mild traumatic brain injury causes an atypical astrocyte response and spontaneous recurrent seizures. J Neu-rosci. 2019;39:1944-63.
22. Walrave L, Pierre A, Albertini G, Aourz N, De Bundel D, Van Eeckhaut A, et al. Inhibition of astroglial connexin43 hemichannels with TAT-Gap19 exerts anticonvulsant effects in rodents. Glia. 2018;66:1788-804.
23. Ran X, Xiang J, Song PP, Jiang L, Liu BK, Hu Y. Effects of gap junctions blockers on fast ripples and connexin in rat hippocampi after status epilepticus. Epilepsy Res. 2018;146:28-35.
24. Belousov AB, Nishimune H, Denisova JV, Fontes JD. A potential role for neuronal connexin 36 in the pathogenesis of amyotrophic lateral sclero-sis. Neurosci Lett. 2018;666:1-4.
25. Wu XL, Ma DM, Zhang W, Zhou JS, Huo YW, Lu M, et al. Cx36 in the mouse hippocampus during and after pilocarpine-induced status epilep-ticus. Epilepsy Res. 2018;141:64-72.
26. Du M, Li J, Chen L, Yu Y, Wu Y. Astrocytic Kir4.1 channels and gap junctions account for spontaneous epileptic seizure. PLoS Comput Biol. 2018;14:e1005877.
27. Plata A, Lebedeva A, Denisov P, Nosova O, Postnikova TY, Pimashkin A, et al. Astrocytic atrophy following status epilepticus parallels reduced Ca2+ activity and impaired synaptic plasticity in the rat hippocampus. Front Mol Neurosci. 2018;11:215.
28. Scemes E, Velíšek L, Velíšková J. Astrocyte and neuronal pannexin1 contribute distinctly to seizures. ASN Neuro. 2019;11:1759091419833502.
29. Manjarrez-Marmolejo J, Franco-Pérez J. Gap junction blockers: an over-view of their effects on induced seizures in animal models. Curr Neuro-pharmacol. 2016;14:759-71.
30. Biswas J, Gupta S, Verma DK, Gupta P, Singh A, Tiwari S, et al. Invol-vement of glucose related energy crisis and endoplasmic reticulum stress: insinuation of streptozotocin induced Alzheimer’s like pathology. Cell Signal. 2018;42:211-26.
31. Sharma P, Srivastava P, Seth A, Tripathi PN, Banerjee AG, Shrivast va SK. Comprehensive review of mechanisms of pathogenesis involved in Alzheimer’s disease and potential therapeutic strategies. Prog Neurobiol. 2019;174:53-89.
32. Wang M, Zhou J, He F, Cai C, Wang H, Wang Y, et al. Alteration of gut microbiota-associated epitopes in children with autism spectrum disor-ders. Brain Behav Immun. 2019;75:192-9.
33. Giaume C, Sáez JC, Song W, Leybaert L, Naus CC. Connexins and pannexins in Alzheimer’s disease. Neurosci Lett. 2019;695:100-5.
34. Lu C, Meng Z, He Y, Xiao D, Cai H, Xu Y, et al. Involvement of gap junctions in astrocyte impairment induced by manganese exposure. Bra-in Res Bull. 2018;140:107-13.
35. Kasap M, Bonnett K, Aamodt EJ, Dwyer DS. Akinesia and freezing caused by Na+ leak-current channel (NALCN) deficiency corrected by pharmacological inhibition of K+ channels and gap junctions. J Comp Neurol. 2017;525:1109-21.
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020

121
A. Sánchez, et al.: Synapses in neuropathological conditions
36. Phookan S, Sutton AC, Walling I, Smith A, O’Connor KA, Campbell JC, et al. Gap junction blockers attenuate beta oscillations and improve fo-relimb function in hemiparkinsonian rats. Exp Neurol. 2015;265:160-70.
37. Maatouk L, Yi C, Carrillo-de Sauvage MA, Compagnion AC, Hunot S, Ezan P, et al. Glucocorticoid receptor in astrocytes regulates midbrain dopamine neurodegeneration through connexin hemichannel activity. Cell Death Differ. 2019;26:580-96.
38. Fujita A, Yamaguchi H, Yamasaki R, Cui Y, Matsuoka Y, Yamada KI, et al. Connexin 30 deficiency attenuates A2 astrocyte responses and induces severe neurodegeneration in a 1-methyl-4-phenyl-1,2,3,6-tetra-hydropyridine hydrochloride Parkinson’s disease animal model. J Neuro-inflammation. 2018;15:227.
39. Zhang YW, Kaneda M, Morita I. The gap junction-independent tumor-su-ppressing effect of connexin 43. J Biol Chem. 2003;278:44852-6.
40. Gielen PR, Aftab Q, Ma N, Chen VC, Hong X, Lozinsky S, et al. Conne-xin43 confers temozolomide resistance in human glioma cells by modu-lating the mitochondrial apoptosis pathway. Neuropharmacology. 2013;75:539-48.
41. Lai SW, Huang BR, Liu YS, Lin HY, Chen CC, Tsai CF, et al. Differential characterization of temozolomide-resistant human glioma cells. Int J Mol Sci. 2018;19:e127.
42. Mettang M, Meyer-Pannwitt V, Karpel-Massler G, Zhou S, Carragher NO, Föhr KJ, et al. Blocking distinct interactions between glioblastoma cells and their tissue microenvironment: a novel multi-targeted therapeutic approach. Sci Rep. 2018;8:5527.
43. Pilarczyk G, Papenfuß F, Bestvater F, Hausmann M. Spatial arrange-ments of connexin43 in cancer related cells and re-arrangements under treatment conditions: investigations on the nano-scale by super-resolu-tion localization light microscopy. Cancers (Basel). 2019;11:e301.
44. Jayalakshmi J, Vanisree AJ, Ravisankar S, Rama K. Site specific hyper-methylation of CpGs in Connexin genes 30, 26 and 43 in different grades of glioma and attenuated levels of their mRNAs. Int J Neurosci. 2019;129:273-82.
45. Zhang W, Couldwell WT, Simard MF, Song H, Lin JH, Nedergaard M. Direct gap junction communication between malignant glioma cells and astrocytes. Cancer Res. 1999;59:1994-2003.
46. Chen D, Liu Y, Yang H, Chen D, Zhang X, Fermandes JC, et al. Conne-xin 43 promotes ossification of the posterior longitudinal ligament through activation of the ERK1/2 and p38 MAPK pathways. Cell Tissue Res. 2016;363:765-73.
47. Ozog MA, Siushansian R, Naus CC. Blocked gap junctional coupling increases glutamate-induced neurotoxicity in neuron-astrocyte co-cultu-res. J Neuropathol Exp Neurol. 2002;61:132-41.
48. Wang J, Yang ZY, Guo YF, Kuang JY, Bian XW, Yu SC. Targeting diffe-rent domains of gap junction protein to control malignant glioma. Neuro Oncol. 2018;20:885-96.
49. Machado C, Rodríguez R, Estévez M, Leisman G, Chinchilla M, Portela L, et al. Trastorno del espectro autista: un reto para las neurociencias. Rev Mex Neuroci. 2017;18:30-45.
50. Irwin DJ, Grossman M, Weintraub D, Hurtig HI, Duda JE, Xie SX, et al. Neuropathological and genetic correlates of survival and dementia onset in synucleinopathies: a retrospective analysis. Lancet Neurol. 2017;16:55-65.
51. Fenouil T, Fourier A, Quadrio I, Streichenberger N, Bernardini S, Zima T, et al. The standardization of cerebrospinal fluid markers and neuropatho-logical diagnoses brings to light the frequent complexity of concomitant pathology in Alzheimer’s disease: the next challenge for biochemical markers? Clin Biochem. 2019;72:15-23.
52. De Reuck JL. Post-mortem magnetic resonance imaging as an additional tool of the neuropathological examination of neurodegenerative and ce-rebrovascular diseases. Eur Neurol Rev. 2016;11:22-5.
53. Wall DP, Kosmicki J, Deluca TF, Harstad E, Fusaro VA. Use of machine learning to shorten observation-based screening and diagnosis of autism. Transl Psychiatry. 2012;2:e100.
54. Sato JR, Hoexter MQ, Oliveira PP Jr., Brammer MJ, MRC AIMS Consor-tium, Murphy D, et al. Inter-regional cortical thickness correlations are associated with autistic symptoms: a machine-learning approach. J Psy-chiatr Res. 2013;47:453-9.
55. Heinsfeld AS, Franco AR, Craddock RC, Buchweitz A, Meneguzzi F. Identification of autism spectrum disorder using deep learning and the ABIDE dataset. Neuroimage Clin. 2018;17:16-23.
56. Wang J, Ma M, Locovei S, Keane RW, Dahl G. Modulation of membrane channel currents by gap junction protein mimetic peptides: size matters. Am J Physiol Cell Physiol. 2007;293:C1112-9.
57. Glass BJ, Hu RG, Phillips AR, Becker DL. The action of mimetic peptides on connexins protects fibroblasts from the negative effects of ischemia reperfusion. Biol Open. 2015;4:1473-80.
58. Shiels A, Mackay D, Ionides A, Berry V, Moore A, Bhattacharya S. A mis-sense mutation in the human connexin50 gene (GJA8) underlies autoso-mal dominant “zonular pulverulent” cataract, on chromosome 1q. Am J Hum Genet. 1998;62:526-32.
59. Muller KJ, Scott SA. Transmission at a ‘direct’ electrical connexion me-diated by an interneurone in the leech. J Physiol. 1981;311:565-83.
60. Lo YK, Tang KY, Chang WN, Lu CH, Cheng JS, Lee KC, et al. Effect of oleamide on Ca(2+) signaling in human bladder cancer cells. Biochem Pharmacol. 2001;62:1363-9.
61. Söhl G, Nielsen PA, Eiberger J, Willecke K. Expression profiles of the novel human connexin genes hCx30.2, hCx40.1, and hCx62 differ from their putative mouse orthologues. Cell Commun Adhes. 2003;10:27-36.
62. Altevogt BM, Kleopa KA, Postma FR, Scherer SS, Paul DL. Connexin29 is uniquely distributed within myelinating glial cells of the central and peripheral nervous systems. J Neurosci. 2002;22:6458-70.
63. Fagerberg L, Hallström BM, Oksvold P, Kampf C, Djureinovic D, Ode-berg J, et al. Analysis of the human tissue-specific expression by geno-me-wide integration of transcriptomics and antibody-based proteomics. Mol Cell Proteomics. 2014;13:397-406.
64. Wallenstein MC, Mauss EA. Effect of prostaglandin synthetase inhibitors on experimentally induced convulsions in rats. Pharmacology. 1984;29:85-93.
65. Abrams C, Rash J. Connexins in the nervous system. In: Connexins: a Guide. Part I: fundamentals of Connexin Biology. Totowa, New Jersey: Humana Press; 2009. p. 43-59.
66. Oyamada M, Oyamada Y, Takamatsu T. Regulation of connexin expres-sion. Biochim Biophys Acta. 2005;1719:6-23.
67. Nielsen PA, Beahm DL, Giepmans BN, Baruch A, Hall JE, Kumar NM. Molecular cloning, functional expression, and tissue distribution of a novel human gap junction-forming protein, connexin-31.9. Interaction with zona occludens protein-1. J Biol Chem. 2002;277:38272-83.
68. Wingard JC, Zhao HB. Cellular and deafness mechanisms underlying connexin mutation-induced hearing loss a common hereditary deafness. Front Cell Neurosci. 2015;9:202.
69. Beyer E, Berthoud V. The family of connexin genes. In: Connexins: A Gui-de. Part I: fundamentals of Connexin Biology. Totowa, New Jersey: Hu-mana Press; 2009. p. 3-27.
70. Söhl G, Willecke K. Gap junctions and the connexin protein family. Car-diovasc Res. 2004;62:228-32.
No
par
t o
f th
is p
ub
licat
ion
may
be
rep
rod
uce
d o
r p
ho
toco
pyi
ng
wit
ho
ut
the
pri
or
wri
tten
per
mis
sio
n o
f th
e p
ub
lish
er.
©
Per
man
yer
2020













![Digital Signal Processing for Optical Coherent ... · [1]Xu Zhang, Darko Zibar, Idelfonso Tafur Monroy, Richard Younce. \Engineering rules for chromatic dispersion compensation in](https://img.pdfslide.us/doc/110x75/5f610c4284952b38e0754b98/digital-signal-processing-for-optical-coherent-1xu-zhang-darko-zibar-idelfonso.jpg)














