Upload
jotapintor
View
53
Download
1
Tags:
Embed Size (px)
DESCRIPTION
publicaciones implantología zimmer
Citation preview
QU
INTE
SSE
NZ
A IN
TE
RN
AZ
ION
ALE
& J
OM
I 2
bis
/2014
Qe
I&Jla rivista internazionale di implantologia
chirurgia orale e maxillo-facciale
Vo
lum
e 3
0 .
Nu
mb
er 2
bis
. 2
01
4Qu
intes
senz
a Ediz
ioni S
.r.l. -
Via C
iro M
enot
ti 65
- 20
017
Rho (
MI) -
Pos
te It
alian
e Spa
- Sp
ed. in
A.P.
D.L.
353
/200
3 (co
nv. in
L. 2
7/02
/04
n. 46
) art.
1 co
mm
a 1, D
CB -
Mila
no
QuintessenzaInternazionale
&JOMI
Implant & Regenerative Therapy with Digital Dentistry
Publication Supported by Zimmer Dental
2013 Zimmer Dental Inc. All rights reserved for content and images. ZD1208, Rev. 6/13.1. Rosenlicht JL. SwissPluss Implant System, part 1: surgical aspects and intersystem comparisons. Implant Dent. 2002;11:144-153.- Rosentlich JL. SwissPLus Implant System, part 2 : prostodontic aspects and intersystem comparisons. Implant Dent. 2002;11:249-257. - Gunaseelan R, Rajan M. Overwiew of the SwissPlus Implant System. J Oral Implantol. -2005;31:121-128. - Sunitha R, Ramakrishnan T, Kumar S, Emmadi P. Soft tissue preservation and crestal bone loss around single-tooth implants. J Oral Implantol. - 2008;34:223-229. - Ormanier Z, Palti A, Shifman A. Survival of immediately loaded dental implants in deficient alveolar bone sites augmented with -Tricalcium Phosphate. Implant Dent. 2006;15:395-402.
Visit www.zimmerdental.com to learnmore about SwissPlus Dental Implant.
I am the Tapered SwissPlus Dental Implant, I am designed to achieve excellent primary stability and my performance has been the subject of many studies1 based on 12 years of clinical experience.
My all-in-one simplifies the different procedures. Smart and affordable, I have a multi-functional fixture
mount managing most of clinical cases. Performance, simplicity and economy I am Zimmer.
THE IMPLANT
FOR MORE
AFFORDABLE Q
UALITY CARE
www.zimmerdental.com
ZD1208_SwissPluss_Implant Ad_210x280.indd 1 04.03.14 16:54
2012 Zimmer Dental Inc. All rights reserved. 6547, Rev. 8/12
I am building on the tradition of the tried-and-true Tapered Screw-Vent Implant with more than a decade of experience and over 2 million units sold, I offer a variety of crestal
configurations for optimum flexibility and choice to conveniently meet your clinical needs. Leveraging the
proprietary Platform Plus Technology to optimize your connection, and provide the highest torque values
on the market I strive for primary stability and immediate function. Versatility, clinical choice, quality,
and innovation I am Zimmer.
Visit www.zimmerdental.com to learn more about
the Tapered Screw-Vent Implant Family.
www.zimmerdental.com
VerSaTIlITy
redefIned
6547_TSV_Implant_210x280.indd 1 04.03.14 16:55
ed
ito
ria
l
VOLUME 30 NUMBER 2bis 2014
Dear Colleagues,I want to thank Quintessence, dr. Horst -Wolfgang Haase and Lauro Dusetti, for an invitation to make a welcome to the readers of this Special Edition of Quintessence International & JOMI.Implant & Regenerative Therapy with Digital Dentistry immediately gives the idea of the topics covered, their multidisciplinary nature, than are current and as such further investigation of which they need it.As always, the use of new medical devices or new therapies need to clinical pio-neers with devoted skills have the ability to identify the most appropriate proto-cols, and then implement them, making them more predictable.I do not want to enter the single item, but the entire article collection confirms that the effort continues in the dental industry, through the development of products, and will allow us to give patients treatments more effective.From our side, we clinicians could have, increasingly, procedures that will allow us to obtain a more repeatable quality in the therapy itself.
I wish you all a good read
Prof. Mariano Sanz
2 VOLUME 30 NUMBER 2bis 2014
ISSN 1723-7793
Scientific Director
Tiziano Testori
Gianfranco Carnevale
Raffaele Cavalcanti
Matteo Chiapasco
Ugo Consolo
Gianpiero Cordioli
Matteo Deflorian
Sergio De Paoli
Danilo Di Stefano
Giuseppe Ferronato
Luca Fumagalli
Giovanni Lodi
Salvatore Longoni
Massimiliano Martignoni
Marco Morra
Andrea Parenti
Stefano Parma Benfenati
Roberto Pontoriero
Loris Prosper
Antonio Rocci
Eugenio Romeo
Massimo Simion
Giovanni Zucchelli
Reading Committee
Scientific CommitteeLilia Bortolotti
Antonio Carrassi
Enrico Conserva
Ugo Covani
Massimo De Sanctis
Fabio Galli
Mauro Fradeani
Luca Francetti
Luigi Galasso
Enrico Gherlone
Stefano Gracis
Domenico Massironi
Pierfrancesco Nocini
Adriano Piattelli
Giovan Paolo Pini Prato
Giacomo Urbani
Francesco Zuffetti
Roberto Weinstein
PublisherQuintessenza EdizioniHorst-Wolfgang Haase
Director of Quintessenza EdizioniLauro Dusetti
Director in chargeCristina Reina
Marketing & PR OfficeLauro Dusetti (Management) Mob. 338 9312741 [email protected] Fassetti [email protected]
EditorBarbara Rossi [email protected] Reina [email protected]
SubscriptionsMaria Calabrese [email protected] Vergani [email protected]
AdministrationMaria Calabrese [email protected]
CongressesLauro Dusetti [email protected] Fassetti [email protected] Marta Vergani [email protected]
QUiNTESSENZA iNTERNAZiONALE is an Italian-language quarterly, published by Quintessenza Edizioni s.r.l., Via Ciro Menotti 65 - 20017 Rho, Milan.COPyRiGhT 2014 Literary ownership and all rights reserved to Quintessence Publishing Co. Inc. No part of the content of this publication may be reproduced or transferred in any form or on any elec-tronic or mechanical support, photocopy, disk or piracy system without the express written authorisa-tion of the Editor. The Editor declines all responsibil-ity for manuscripts submitted without having been expressly requested by the publishers. The opinions published are those of the authors.
Termination of subscriptions must be received by registered post, 3 months ahead of the expiry date.
Quintessenza Edizioni is not responsible for missed deliveries of the publication due to rea-sons beyond its control.
Printing: Reggiani S.P.A.Via Dante Alighieri, 5021010 Brezzo di Bedero (VA) - Italy
Registered with the Court of Milan at no. 511 on 16-09-03Registered for transmission by post: Decree law 353/2003 (converted into law no. 46 of 27/02/04)Art. 1(1) Commercial Business Division - Milan
SUBSCRiPTiONSSubscriptions for 2013:Quintessenza Internazionale & JOMI + JOMI online English versionFull = print + online 110.00Online = online version only, 70.00Subscription rates include packaging and delivery costs.
FORM OF PAyMENT By bank cheque or postal order, to:Quintessenza Edizioni s.r.l.Via Ciro Menotti 6520017 - Rho, Milan -Tel. 02.93.18.08.21
This publication is af fil iated to the Italian Union of Periodicals (Unione Stampa Periodica Italiana)
05
13
23
31
41
51
57
63
79
69
91
Z i m m e r
97
VOLUME 30 NUMBER 2bis 2014
su
mm
ar
y
RevitaliZe Patient Solutions: preliminary results from a single cohort prospective study using Screw-Vent TSVT implantsA. Agnini, M. A Salama, A. Mastrorosa Agnini, H. Salama, C. FJ Stappert, D. Romeo
Lateral bone augmentation with a block allograft (Puros, Zimmer dental) combined with GBR and followed by implant placement in a staged approach: A case report O. Argibay Lorenzo, C. Carral Freire, J. Blanco Carrin
Digital Dentistry meets Implantology The Munich Implant Concept - A case report F. Beuer, J. Schweiger, J. F. Gth
Surgical recommendations for allograft block grafting O. Blume, O. Richter, M. Back, T. Mller-Hotop
Trabecular Metal Dental Implants: Overview of design and developmental research M. Collins, J. Bassett, H. Bo Wen, C. Gervais, M. Lomicka, S. Papanicolaou
Implant therapy with an innovative surface (trabecular metal) and CAD/CAM restorations a clinical case K. Fischer, S. Fickl
Immediate post-extraction provizionalisation: aesthetic and functional stability after 13 yearsB. Fissore
Simultaneous TM implant placement and horizontal ridge augmentation with IngeniOs HA: A Case Report R. Gmez Meda
The ortho-perio-prosthodontic team-approach for successful management of the single-tooth implant in the esthetic zoneG. Pellitteri, U. Schneider-Moser, L. Moser
High resolution histologic and histomorphometric analysis of block allografts in humans: Report of three casesW. Gutwerk
Preliminary outcome in consecutively treated case series with Trabecular Metal implants C. M. Soardi, H-L Wang, E. Clozza, D. Zaffe, L. Checchi
Surgery All at Once: Socket preservation and immediate placement of an implant in an infected site in the anterior region a Case Report W.P. van der Schoor, A.R.M. van der Schoor
5VOLUME 30 NUMBER 2bis 2014
Purpose: The aim of this paper was to report preliminary results from a cohort of subjects treated with the
RevitaliZe Patient Solutions approach. Clinical and radiographic results of axial and tilted implants up to
fourteen months of loading are presented. Material and Methods: From September 2011 to May 2012, 7
patients were recruited and treated with a metal reinforced fixed full-arch prosthesis screw-retained over
two axial and two tiled implants within 24 hours from the surgery. Final restorations were placed 6 months
later. Follow-up visits were scheduled every 6 months and radiographic evaluation of peri-implant bone level
changes was conducted. Results: Seven patients (5 females and 2 males) were followed up for an average
of 11,88 months (range 8-16 months). Five subjects received implant treatment in both arches, resulting in
12 restorations. A total of 48 fixtures (Zimmer Screw-Vent TSVT) were placed and no failure was reported
during the follow-up period, leading to 100% implant and prosthetic survival rates. Radiographic analysis after
6 months of loading was conducted for all prostheses. No significant difference in marginal bone loss was
found between tilted and axial implants in both jaws. Conclusions: The present preliminary data suggests that
immediate loading with RevitaliZe Patient Solutions could be considered a predictable and cost- and time-
effective approach for the treatment of total edentulism.
Keywords: Dental implants, Fixed implant restoration, Immediate loading, Tilted implants.
Alessandro Agnini*, Maurice A Salama**, Andrea Mastrorosa Agnini***, Henry Salama****, Christian FJ Stappert*****, Davide Romeo******
RevitaliZe Patient Solutions: preliminary results from a single cohort prospective study using Screw-Vent TSVT
implants
INTRODUCTION
According to the most recent review of the den-tal literature, immediate loading procedures for total edentulism have reported high percentages of clinical success1,2, therefore an increasing number of clinicians have adopted these protocols in their daily practice. The reduction of total treatment time and the possi-bility to deliver a functional implant prosthesis a few hours after the surgery represents notable advantages for patients, specially for individuals with a failing denti-tion because they can avoid the psychological trauma and discomfort of a transitional removable prosthesis3.
An essential condition for immediate loading proto-cols is a minimum amount of fixtures primary stability, quantifiable in 35 Ncm4. Implant design, bone quality and quantity and a proper surgical technique strongly contribute to a fixed implant at the time of placement4-6 and the rigid splinting effect of provisional restoration directs the healing process towards osseointegration7,8.
* DDS, Private Practice Modena and Sassuolo - Assistant Professor Modena University.
** DMD, Private Practice Atlanta, GA. Asst Clinical Professor of Periodontology Medical College of Georgia, Augusta, GA - USA.
*** DDS, Private Practice Modena and Sassuolo, Italy.**** DDM, Private Practice, Atlanta, GA, Asst. Clinical Professor of
Periodontology, Medical College of Georgia, Augusta.***** DDS, M.S., PhD, Professor and director of Implant Periodontal
Prosthodontics, Department of Periodontics, University of Maryland schoolf of dentistry, Professor, department of Prosthodontics, Albert Ludwigs University, Freiburg, Germany.
****** DDS, PhD, Research Associate, department of Periodontics, University of Maryland School fo Dentistry, Baltimore, MD, Usa.
Correspondence: Andrea Mastrorosa AgniniStudio Agnini OdontoiatriaCorso Canal Grande 3 - 41126 Modena, ItalyE-mail: [email protected]
A g n i n i A , S A l A m A mA, m A S t r o r o S A A g n i n i A , S A l A m A H, S tA p p e r t CFJ, r o m e o D
6 VOLUME 30 NUMBER 2bis 2014
In the last years, different clinical studies assessed tilted implants as a feasible treatment option, bringing surgical and prosthetic advantages9. The rehabilitation of complete arches with only four implants (two ante-rior axial and two posterior tilted), supporting a fixed prosthesis with limited distal cantilever was analyzed in recent studies10,11. Encouraging clinical outcomes have been reported in the medium term12 and no difference in implant survival rate and marginal bone loss have been registered between axial and tilted fixtures13.
The aim of this paper was to report preliminary re-sults of RevitaliZe Patient Solutions, a new treatment modality that allows clinicians to immediately restore complete arches with a full-arch bridge screw-retained over two straight anterior and two posterior angled fixtures.
MATERIALS AND METHODS
Study protocolThe study was designed as a prospective single-
cohort clinical trial conducted according to the prin-ciples of the Helsinki Declaration of 1975, as revised in 2000. Consecutively treated patients were included and scheduled to be followed for up to 10 years after loading. Subjects were explained all potential adverse effects and complications of treatment and they signed an informed consent to be included in the study. Surgi-cal interventions and prosthetic phases were done in two clinical centers by one operator (AA) with experi-ence in immediate loading rehabilitations.
Selection CriteriaPatients were enrolled if they were older than 18
years as well as physically and psychologically able to undergo conventional implant surgery and restorative procedures (American Society of Anesthesiologist (ASA) class I or II)14.
Further inclusion criteria were: edentulous arch or presence of teeth with unfavorable long-term prog-nosis; adequate bone volume in the anterior maxilla and anterior mandible for implant placement (10 mm height and 3.7 mm wide), based on the pre-operative CT scan measurements; patients who preferred fixed implant-supported rehabilitation without recurring to any bone grafting procedure. All implants had to reach a minimum insertion torque of 30 Ncm. If one or two implants failed to reach that level but the other fixtures have adequate primary stability, immediate loading was still performed.
Main exclusion criteria were: presence of active in-fection or inflammation in the planned implant area; untreated periodontitis; serious problems of coagula-tion, disease of the immune system, uncontrolled di-abetes and metabolic disease affecting bone; severe bruxism or clenching, heavy smoking (more than 25 cigarettes/day), radiation therapy to the head or neck region in the previous 5 years, alcoholism or use of drugs, pregnancy or lactation at the time of surgery, poor oral hygiene and motivation, and unavailability to attend regular follow-up visits.
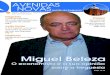
Fig 157 year old patient presenting metal crowns from up-per canine to contralateral and a partial removable denture to replace posterior teeth. Opposing dentition is composed by metallic crowns. Smile line can be considered average, exposing 10 teeth during maximum smile, while the incisal superior plane is distant from the inferior lip.
Fig 2Plaque and calculus were observed, as well as gin-gival recessions on some teeth in both arches. Mismatch in dental midlines is observed as well as disharmony in dental proportion.
A g n i n i A , S A l A m A mA, m A S t r o r o S A A g n i n i A , S A l A m A H, S tA p p e r t CFJ, r o m e o D
7VOLUME 30 NUMBER 2bis 2014
Pre-surgical assessment and treatment planning
Arch size, bone volume, inter-arch relation and dis-tance were evaluated pre-operatively by means of a clinical examination (Figure 1 and 2) and analysis of pan-oramic radiographs, periapical radiographs (Figure 3), computerized tomography scans, radiograph of the skull in lateral view and study models mounted in articulator.
Before the surgery, a resin transfer plate was made duplicating the patients denture or based on a wax-up for partially edentulous patients, with a secure stop on the palate vault or on the retromolar triangle. Subse-quently, an opening approximately at the level of the occlusal surface was made to use the plate as a surgical guide, as described by Biscaro15.
Surgical techniqueAll surgical procedures were performed under intra-
venous sedation and local anesthesia (Figure 4). If some remaining teeth were present, they were extracted and their sockets were debrided with sterile saline solution. A mid-crestal incision was made, always excluding the retromolar triangle or the maxillary tuberosity, and a full thickness flap was reflected. Direct visualization of the mental nerve was made and the anterior loop was estimated with an atraumatic periodontal probe gently placed into the canal. Where necessary, regularization of the crest was performed with bony forceps and ro-tary instruments before stabilizing the resin transfer plate using the palatal vault or the retromolar area.
Bone quality was evaluated based on Lekholm and Zarb classification16 and Tapered Screw-Vent implants (Zimmer Dental Inc., Carlsbad, California) were placed
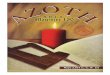
Fig 3Peri-apical x-rays show severe bone loss and a sce-nario of failing dentition, with horizontal resorption and ver-tical defects around natural teeth and maxillary implants. Pneumatization of maxillary sinuses prevents implants placement without recurring to sinus lift augmentations.
Fig 4After two sessions of scaling and root planning ne-cessary to reduce the marginal inflammation, some failing roots on the lower jaw were extracted, while the remaining pillars with a minimal stability were maintained to support a provisional acrylic bridge. A soft diet was suggested until the day of the surgery.
Fig 5A 3.7 mm wide Tapered Screw-Vent implant (TSVT) is inserted with a 30 degreed inclination according to the protocol. Anterior straight fixture is already placed.
Fig 6Tooth extraction and immediate implant placement in the mandible. Post extraction gaps were filled with a mixture of autogenous bone and xenograft.
A g n i n i A , S A l A m A mA, m A S t r o r o S A A g n i n i A , S A l A m A H, S tA p p e r t CFJ, r o m e o D
8 VOLUME 30 NUMBER 2bis 2014
according to RevitaliZe Patient Solutions protocol (Figure 5 and 6). Tapered Screw-Vent abutments (Fig-ure 7) and Spectra-Angle abutments (Zimmer Dental Inc., Carlsbad, California, USA) were screw retained to straight and tilted implants, respectively.
Immediate provisional restorationCopings for open tray impression were positioned
over the abutments and isolated with a sterile piece of rubber dam. Copings were connected to each other by orthodontic wire and acrylic resin (Pattern Resin, GC America) or composite Protemp 4 (3M ESPE, Pioltello, Milan, Italy) and then fixed to the surgical guide with the same material 17. After 5 minutes, the complex of im-pression copings and guide was removed, healing abut-ments were placed and flaps were sutured with Gore-Tex 5/0 (WL Gore & Associates, Flagstaff, Arizona, USA).
Implant analogs were screwed on the impression copings and the stone was removed from the study
model in the area corresponding to implant placement. The entire complex made by surgical guide, impression copings and analogs were positioned again over the study model. New stone was placed to secure implant analogs, converting the study model in the final master cast 17 (Figure 8). A screw retained metal reinforced provisional was made (Figure 9 and 10) and positioned in the patients mouth the same day or within 24 hours after surgery (Figure 11). The immediate restoration contained no more than 12 teeth and distal cantilevers were usually avoided. Full occlusal contacts in centric occlusion were maintained for all teeth, while lateral interferences were removed.
Final restoration protocolIn absence of pain and inflammatory signs (Figure
12), the final restoration based on a CAD/CAM frame-work was delivered 6 months after loading. Five pa-tients for a total of 10 arches were treated with a mono-
Fig 7 Spectra-Angle abutments were posi-tioned over posterior implants to correct their inclination and get a fa-vorable access for the prosthetic screw.
Fig 8The complex made by surgical guide, impression co-pings and analogs rigidly connected with composite resin were positioned again over the study model to create the master model for the fabrication of the provisional bridge.
Fig 9A metal framework is glued over 4 titanium cylinders to provide rigidity at the provisional prosthesis.
Fig 10Provisional restoration contains 12 teeth, with pink gingiva if necessary.
A g n i n i A , S A l A m A mA, m A S t r o r o S A A g n i n i A , S A l A m A H, S tA p p e r t CFJ, r o m e o D
9VOLUME 30 NUMBER 2bis 2014
lithic zirconium-oxide bridge, where just an external layer of 0.6 mm thickness from first premolar to the contralateral was modeled by dental technician to get a natural esthetic appearance (Figure 13-16). The mor-phology of the occlusal surfaces was entirely created from the monolithic block of zirconia. Two subjects were rehabilitated with titanium frameworks and ve-neering composite according to their desires.8
Outcome MeasuresThe main outcome measures for the present study
were: 1. Prosthesis success: when the prosthesis was in func-
tion, without mobility or pain, even in face of the loss of one or more implants. Prosthesis stability was tested at each follow-up visit by means of two op-posing instruments pressure.
Fig 11 Immediate restorations are delivered within 24 hours from the surgery. Contacts in centric occlusion are maintain for all the 12 teeth while distal cantilevers, if present, are under the occlusal plane. Interferences in lateral excursion are removed.
Fig 12After six months necessary for osseointegration, hard and soft tissues are stable for the final restorations.
Fig 13 Final bridge consists of a monolithic zirconium-oxided framework with a layer of 0.6 mm of veneering porcelain at the vestibular side of frontal teeth and first premolars.
Fig 14Frontal intra-oral view of final bridges.
Fig 15A natural smile was obtained thanks to the ma-terials used for the restorations and to the work of the dental technician.
Fig 16Final panoramic x-ray showing implant distribution and bone level around implants after 1 year of loading.
A g n i n i A , S A l A m A mA, m A S t r o r o S A A g n i n i A , S A l A m A H, S tA p p e r t CFJ, r o m e o D
10 VOLUME 30 NUMBER 2bis 2014
Secondary outcomes were:1. Implant survival: when the implant was in function
and stable with no evidence of peri-implant radiolu-cency, no suppuration or pain at the implant site or ongoing pathologic processes18.
2. Biological and prosthetic complications, such as peri-implantitis, fistula or abscess, mechanical or prosthet-ic complications like fracture of the implant or any prosthetic component19,20.
3. Plaque and Bleeding Indexes at implant level. Each implant was examined on four aspects (mesial, dis-tal, vestibular, palatal/lingual). The percentage of sites in which plaque could be found, regardless of its amount, was recorded. A total of 16 sites per patient were examined, as previously described11. Briefly, any site in which plaque could be detected by naked eye or with a probe accounted for 6.25% (1/16) of the total score (100%). The same was made for bleeding index, considering positive any site that showed bleeding on probing11.
4. Patient satisfaction in term of aesthetics, phonetics and masticatory function was recorded by means of a questionnaire at baseline (before the treatment), at 7 months (after delivering the final prosthesis) and then at the 1-year and 2-year follow-ups21. The an-swers were based on a 5-point Likert-type scale, with scores ranging from poor to excellent (1 = poor, 2 = sufficient, 3 = good, 4 = very good, 5 = excellent). Da-ta were statistically analyzed by means of the Fishers exact test.
5. Marginal bone level change: Periapical radiographs were performed using a long-cone paralleling tech-nique and an individual x-ray holder at baseline, at 6 and 12 months, and yearly thereafter. Marginal bone level was assessed with an image analysis soft-ware (UTHSCSA Image Tool version 3.00 for Win-dows, University of Texas Health Science Center in San Antonio, TX, USA) by two experienced blinded evaluators. Mesial and distal values were averaged so as to have a single value for each implant. Bone loss around tilted and axial implants was compared by using paired Students t-test. Analysis of variance (ANOVA) was used to analyze bone level changes over time and P = 0.05 was considered as the level of significance.
RESULTS
From September 2011 to the same month of 2012, 7 healthy patients (5 women and 2 men; mean age 58 years; range 46-74 years) have been rehabilitated ac-cording to the RevitaliZe Patient Solutions. Five sub-jects were treated in both arches (4 of them during the same day) for a total of 12 immediately loaded fixed prosthesis (7 maxillae and 5 mandibles) supported by four implants. Four patients were smokers with a daily consumption of 4.7 cigarettes.
Forty-eight Tapered Screw-Vent TSVT (Zimmer Dental Inc., Carlsbad, California, USA) implants with MTXsurface were placed and all of them were imme-diately loaded. Forty-four fixtures had a diameter of 3.7 mm, while length ranged from 10 to 16 mm. Pos-terior implants had a mesio-distal inclination ranging between 20 and 40 degrees according to anatomical limitation and local condition.
No complication occurred during surgical or pros-thetic phases and no fracture of the final prostheses or any screw loosening have been reported.
The mean follow-up duration was 11.88 2.38 months (range 9-16 months) and no implant or pros-thetic failure occurred, resulting in 100% survival rates.
Peri-implant bone loss after 1-year follow-up could be evaluated for 7 arches (n = 14 implants per group) and this parameter averaged 1.02 0.10 mm and 1.02 0.08 mm for axial and tilted implants, respec-tively. Such difference was not statistically significant (p > .05).
Plaque and bleeding scores were recorded after 6 months of loading for all prosthesis and they were 12.08 5.33 and 9.58 5.03, respectively.
All patients completed the questionnaire for satis-faction. Aesthetic, phonetics and masticatory function were judged as excellent or very good by all of them.
DISCUSSION
The purpose of this paper was to report prelimi-nary outcomes of immediate implant-supported fixed bridges for edentulous patients or for subjects who will become edentulous due to a failing dentition. Seven patients for a total of 15 arches were treated accord-ing to the RevitaliZe Patient Solutions, consisting on a functional screw-retained metal reinforced provisional restoration delivered within 24 hours from the place-ment of two axial and two tilted fixtures.
A g n i n i A , S A l A m A mA, m A S t r o r o S A A g n i n i A , S A l A m A H, S tA p p e r t CFJ, r o m e o D
11VOLUME 30 NUMBER 2bis 2014
The results of 100% implant and prosthetic sur-vival rates after a mean follow-up of 12 months are in line with similar studies with immediate loading pro-tocols9-12,22. Agnini and coworkers17 reported 98.02% implant survival rate for 202 fixtures followed for an average of 44 months.
In this study, 1-year marginal bone loss of 1.02 0.10 mm and 1.02 0.08 mm was registered for 14 axial and 14 tilted implants, respectively. These results are similar to the data of a recent study from the same authors where the same implant morphology was used but a variation of the implant collar exists. Tapered Screw-Vent TSV fixtures placed in that study differ from the Tapered Screw-Vent TSVT version used in this inves-tigation for the presence of a 0.5 mm MTX Microtex-tured Surface followed by 1.8 mm of Textured Micro-grooves. The full textured neck placed in sub-crestal position should increased the amount and stability of the fibrin clot, leading to a major bone formation, while the role of the six microgrooves is to augment fixture primary stability in the most coronal area, specially in soft bone, and to provide more surface for new bone formation. However, a larger number of patients with a longer follow-up is necessary to draw conclusions about a possible role of TSVT implants in marginal bone level maintenance.
In this protocol posterior implants are tilted with an inclination ranging between 20 to 40 degrees. A 15 and 30 degrees tapered angulated abutments can correct up to 30 and 45 degrees implants inclination, respec-tively, thanks to the 15 degrees conical shape of their platform. The use of this abutments results in a most favorable orientation of the prosthetic screw.
Great results in terms of esthetics and function were registered from all patients, especially in case of zir-conia frameworks. The vestibular part of frontal teeth were left open to dental technician veneering ability for the characterization of every single element. The fact that the occlusal surface was part of the monolith-ic block decrease the working time for the technician, with a reduction of economic cost.
CONCLUSION
The preliminary results of the present prospective study are positive and in agreement with similar stud-ies. No incidence of surgical or prosthetic complica-tions, high implant and prosthesis survival rates and improved hygienic level throughout the study reveal
that RevitaliZe Patient Solutions is a predictable tech-nique for the rehabilitation of complete arches. How-ever, long-term clinical data are necessary to confirm this statement.
REFERENCES 1. Esposito M, Grusovin MG, Achille H, Coulthard P, Worthington HV.
Interventions for replacing missing teeth: different times for loading dental implants. Cochrane Database of Systematic Reviews 2009 Jan 21 CD003878. Chichester, UK: John Wiley & Sons Ltd.
2. Papaspyridakos P, Mokti M, Chen GJ, Benic GI, Gallucci GO, Chro-nopoulos V. Implant and prosthodontic survival rates with implant fixed complete dental prostheses in the edentulous mandible after at least 5 years: a systematic review. Clin Implant Dent Relat Res 2013, Jan 11. doi:10.1111/cid.12036
3. Gallucci GO, Morton D, Weber H-P. Loading protocols for dental implants in edentulous patients. Int J Oral Maxillofac Implants 2009;24:132-146.
4. Javed F, Romanos GE. The role of primary stability for successful immediate loading of dental implants. A literature review. Journal of Dentistry 2010;38:612-620.
5. Marquezan M, Osrio A, SantAnna E, Souza MM, Maia L. Does bone mineral density influence the primary stability of dental implants ? A systematic review. Clin Oral Implants Res 2012;23:767-774.
6. Bahat O, Sullivan RM. Parameters for successful implant integration revisited part I: immediate loading considered in light of the original prerequisites for osseointegration. Clin Implant Dent Relat Res 2010;12(Suppl 1):e2-12.
7. Ghoul WE, Chidiac JJ. Prosthetic requirements for immediate implant loading: a review. J Prosthodont 2012;21(2):141-154.
8. Strub JR, Jurdzik BA, Tuna T. Prognosis of immediately loaded implants and their restorations: a systematic literature review. J Oral Rahabilita-tion 2012;39:704-717.
9. Del Fabbro M, Bellini CM, Romeo D, Francetti L. Tilted implants for the rehabilitation of edentulous jaws. A systematic review. Clin Implant Dent Relat Res 2010, May 13 doi: 10.1111/j.1708-8208.2010.00288.x.
10. Agliardi E, Panigatti S, Cleric M, Villa C, Mal P. Immediate rehabilita-tion of the edentulous jaws with full prostheses supported by four implants: interim results of a single cohort prospective study. Clinical Oral Implant Research 2010;21:459-465.
11. Weinstein R, Agliardi E, Del Fabbro M, Romeo D, Francetti L. Immediate rehabilitation of the extremely mandible with fixed full-prosthesis supported by four implants. Clin Implant Dent Relat Res 2012;14:434-441.
12. Mal P, de Arajo Nobre M, Lopes A, Moss SM, Molina GJ. A Longitudi-nal study of the survival of All-on-Four implants in the mandible with up to 10 years of follow-up. Journal of American Dental Association 2011;142:310-320.
13. Francetti L, Romeo D, Corbella S, Taschieri S, Del Fabbro M. Bone level changes around axial and tilted implants in full arch fixed immediate restorations. A 5-year prospective study. Clin Implant Dent Relat Res 2012;14:646-654.
14. Keats AS. The ASA classification of physical status A Recapitulation. Anestesiology 1978;4:233-236.
15. Biscaro L, Becattelli A, Poggio PM, Soattin M, Rossini F. The one-model technique: a new method for immediate loading with fixed prostheses in edentulous or potentially edentulous jaws. Int J Periodontics Restor-ative Dent 2009; 29: 307-313.
16. Lekholm U, Zarb GA. Patient selection and preparation. In: Brnemark P-I, Zarb GA, Albrektsson T, eds. Tissue-integrated prostheses: osseon-tegration in clinical dentistry. Chicago, IL:Quintessence,1985:199-209.
17. Agnini A, Agnini AM, Romeo D, Chiesi M, PAriente L, Stappert CF. Clini-cal investigation on axial versus tilted implants for immediate fixed rehabilitation of edentulous arches: preliminary results of a single cohort study. Clinical Implant Detn Relat Res 2012, Nov 21 doi:10.1111/cid.12020
A g n i n i A , S A l A m A mA, m A S t r o r o S A A g n i n i A , S A l A m A H, S tA p p e r t CFJ, r o m e o D
12 VOLUME 30 NUMBER 2bis 2014
18. Sacca S, Coulthard P. Implant failure: etiology and complications. Med Oral Patol Oral Cir Bucal 2011;16:42-44.
19. Esposito M, Hirsch JM, Lekholm U, Thomsen P. Biological factors con-tributing to failures of osseointegrated oral implants. (II). Etiopatho-genesis. Eur J Oral Sci 1998;106:721-764.
20. Zurdo J, Romo C, Wennstrm JL. Survival and complication rates of implant-supported fixed partial dentures with cantilevers: a system-atic review. Clin Oral Implants Res 2009;20:59-66.
21. Dierens M, Collaert B, Deschepper E, Browaeys H, Klinge B, De Bruyn H (2009). Patient-centered outcome of immediately loaded implants in the rehabilitation of fully edentulous jaws. Clin Oral Implants Res 2009;20:1070-7.
22. Agliardi E, Pozzi A, Stappert CFJ, Benzi R, Romeo D, Gherlone E. Im-mediate fixed rehabilitation of the edentulous maxilla: a prospective clinical and radiological study after 3 years of loading. Clinical Implant Dent Relat Res 2012, Aug 9. Doi:10.1111/j.1708-8208.2012.00482.x.
13VOLUME 30 NUMRO 2 bis 2014
* Master en Parodontologie. Universit de Saint-Jacques-de-Compostelle.
** Master en Parodontologie. Universit de Saint-Jacques-de-Compostelle.
*** MD, DDS, PhD, Professeur. Universit de Saint-Jacques-de-Compostelle.
Objectif : illustrer, dun point de vue clinique et radiographique, deux cas cliniques daugmentation de crte
latrale laide dun nouveau matriau de greffe osseuse, Puros(Zimmer Dental, Inc, Carlsbad, CA). Ce matriau
a t pralablement prpar par un nouveau procd de traitement et de strilisation, Tutoplast (Tutogen
Medical, Inc, Alachua, Fl), laugmentation tant suivie de la pose dimplants selon une approche tage. Matriels
et mthodes : Deux patients ont t traits. Les procdures daugmentation de crte latrale alvolaire ont
t ralises dans une zone dente au moyen dun nouveau matriau de greffe osseuse, Puros(Zimmer
Dental, Inc, Carlsbad, CA). Les implants ont t poss en position prothtiquement idale au bout de 6 mois
de cicatrisation. 3 mois plus tard, les restaurations dfinitives ont t poses. Des clichs radiographiques ont
t obtenus immdiatement avant la chirurgie, puis 6 mois et 1 an aprs celle-ci. Rsultats : aprs six mois de
cicatrisation, le matriau greff tait parfaitement intgr dans le site receveur, aussi bien dun point de vue
clinique que radiographique. Les implants ont t poss sans complications, en position prothtiquement idale.
Au bout dun an de cicatrisation, et 6 mois aprs la pose des implants et de la prothse, les rsultats taient
stables. Aucun signe de changements structurels ou de rsorption osseuse ntait constat. Conclusions : 6
mois aprs la mise en charge, les rsultats esthtiques et fonctionnels de ces cas cliniques o les implants
avaient t poss aprs rgnration de crte latrale par le matriau dallogreffe Puros (Zimmer Dental, Inc,
Carlsbad, CA) et la membrane en pricarde CopiOs taient excellents, ce qui tait par ailleurs confirm par les
rsultats cliniques et radiologiques. Nempche que lvidence scientifique est encore insuffisante pour valider
cette technique. Ds lors, il faudra raliser des essais cliniques randomiss.
Mots-cls : Augmentation osseuse latrale, Allogreffe, Rgnration osseuse, Implants dentaires, Substituts osseux.
Argibay Lorenzo Olalla*, Carral Freire Cristina**, Blanco Carrin Juan***
Augmentation osseuse latrale laide dun bloc cortico-spongieux allognique (Puros, Zimmer dental) et rgnration osseuse guide (ROG) suivie de la pose dun
implant selon une approche tage: cas cliniques
INTRODUCTION
Les implants en titane sont considrs comme un traitement efficace et prvisible de ldentement partiel et total1.
En implantologie, il est dsormais pratique courante de poser les implants selon les besoins anticips de la restauration plutt quen fonction de los disponible.
Pour que limplant soit pos en position prothti-quement idale, il faut aussi que le site receveur dis-pose dune largeur de la crte et dune hauteur osseuse rpondant des exigences minimales.
Il existe de nombreuses techniques qui permettent dobtenir une augmentation osseuse latrale, soit en mme temps que la pose dimplants, soit avant celle-ci, au bout dune priode de cicatrisation.
Ces procdures impliquaient le recours la greffe osseuse avec diffrents types de greffons (autogreffes, allogreffes, xnogreffes ou substituts osseux), seuls ou en combinaison avec des procdures de rgnration osseuse guide (ROG) et des techniques dexpansion crestale.
Coordonnes de lauteur : Argibay Lorenzo, OlallaC/Entrerrios sn 15702 Santiago de Compostela, A Corua, Espagne. Tl. 0034 981 571 826
A r g i b Ay L o r e n z o o, C A r r A L F r e i r e C , b L A n C o C A r r i n J
14
a b
VOLUME 30 NUMRO 2 bis 2014
Los allognique a des caractristiques ostoconduc-trices semblables celles des greffons autologues. Ds lors, il a t utilis comme alternative los autologue dans les greffes osseuses2.
Les particules spongieuses allogniques minrali-ses (MCBA) ont t utilises comme matriau de greffe dans le traitement des dfauts de los parodontal, mais galement en chirurgie bucco-dentaire pour les sites post-extractionnels et pour les procdures daugmen-tation de crte, avant la pose dimplants ou simultan-ment celle-ci. Le MCBA est produit osseux dorigine humaine prlev sur donneur dcd, puis trait et strilis.
Cet article vise illustrer, dun point de vue clinique et radiographique, deux cas cliniques daugmentation de crte latrale laide dune nouvelle forme de ce matriau de greffe osseuse, Puros(Zimmer Dental, Inc, Carlsbad, CA). Ce matriau a t pralablement prpar par un nouveau procd de traitement et de strilisation, Tutoplast (Tutogen Medical, Inc, Alachua, Fl), laugmentation tant suivie de la pose secondaire dimplants dentaires.
MATRIELS ET MTHODES
1er CASPatient : une femme de 56 ans, non fumeuse, en
bonne sant systmique, prsentant lexamen de nombreux lments manquants perdus essentiel-lement pour des raisons parodontales, au dbut de ladolescence. Lexamen clinique et les radiographies ont montr une perte osseuse svre dans les zones dentes (Fig.1). Toutes les diffrentes alternatives de traitement ont t discutes de faon approfondie.
Un guide chirurgical a t ralis pour pouvoir poser les implants en position prothtiquement idale. Lors de la premire procdure chirurgicale, cce guide a t utilis pour identifier les zones qui devaient tre rg-nres, alors que dans le deuxime temps chirurgical il a servi la pose des implants.
La greffe osseuse tant ncessaire pour dvelopper un volume osseux suffisant pour la pose dimplants, la patiente a prfr une allogreffe, pour spargner un
Fig. 1Vue clinique intrabuccale. Zones dentes.
Figg. 2a,bVue clinique intrabuccale. Zones dentes, vue occlusale. Evaluation radiographique initiale.
15
A r g i b Ay L o r e n z o o, C A r r A L F r e i r e C , b L A n C o C A r r i n J
VOLUME 30 NUMRO 2 bis 2014
deuxime acte chirurgical pour le prlvement dun greffon dos autogne.
Procdure chirurgicale: aprs avoir anesthsi la pa-tiente par des infiltrations locales, il a t pratiqu une incision mdio-crestale. Un lambeau mucopriost a t soulev pour exposer la crte alvolaire rsiduelle, qui mesurait 3mm de large (Fig.3).
Lallogreffe strile (Puros Block Allograft, Zimmer Dental, Inc, Carlsbad, CA) a t hydrate. Elle a t reti-re de son emballage et place dans le cylindre dune seringue sans embout. Aprs avoir extrait le piston, la seringue a t remplie de solution strile jusqu couvrir entirement le greffon. Lair excdentaire a t vacu, en bouchant lembout du cylindre. Puis, par un mouve-ment de retrait du piston, lhydratation par la solution strile du greffon allognique a t optimise. Lair exc-dentaire a t vacu encore une fois, et cette opration a t rpte pendant 3 5 minutes avant de passer la phase de prparation (Fig. 4).
Lallogreffe a t modele sous irrigation, avec une pice main haute vitesse (Ti-Max Z, NSK) et une fraise, de faon assurer la stabilit du greffon et maximiser
le contact avec los. Les angles corticaux tranchants du greffon ont t arrondis pour minimiser le traumatisme des tissus mous. La couche de particules spongieuses a t adapte au site receveur (Fig. 5).
Nous avons essay de prserver la surface de la corti-cale autant que possible, afin de pouvoir disposer dune surface dense pour la fixation du greffon.
Des micro-perforations ont t ralises dans la corti-cale du site receveur, afin de provoquer un saignement. Ce saignement pourrait contribuer la prolifration des facteurs de croissance et des plaquettes, qui jouent un rle essentiel dans la cicatrisation et dans la revasculari-sation (Fig. 6).
Des trous daccs ont t prpars au travers du gref-fon par un foret de 1,5 mm de diamtre (Straumann AG, Ble, Suisse), jusqu los receveur sous-jacent, afin dy loger les vis de fixation.
Ceci fait, le bloc a t plac dans le site chirurgical, o il a t stabilis laide de deux mini-vis de 12 mm (Straumann AG, Ble, Suisse) pour prvenir la rotation du greffon (Fig. 7).
Fig. 5Lallogreffe a t modele de faon assurer la stabilit du greffon et maximiser le contact osseux.
Fig. 6Des trous sont transpercs dans los cortical recev-eur afin de provoquer un saignement.
Fig. 3La crte alvolaire rsiduelle. Fig. 4Le bloc dallogreffe Puros dans le cylindre de la seringue avec la solution.
A r g i b Ay L o r e n z o o, C A r r A L F r e i r e C , b L A n C o C A r r i n J
16
a b
c d
a b
VOLUME 30 NUMRO 2 bis 2014
Figg. 7a-dLe bloc prpar est plac dans le site chirurgical et stabilis par des mini-vis.
Fig. 8Le site greff est entirement couvert dune mem-brane en pricarde (CopiOs).
Figg. 9a,bDissection du prioste et suture des lambeaux.
17
A r g i b Ay L o r e n z o o, C A r r A L F r e i r e C , b L A n C o C A r r i n J
VOLUME 30 NUMRO 2 bis 2014
Le greffon a t ensuite soigneusement dtour dans la cavit buccale, afin dliminer tous les bords ou les angles tranchants qui pourraient contribuer aux compli-cations des tissus mous. Autour du bloc, les espaces vides ont t remplis avec des particules osseuses (particules
corticales Puros, Zimmer Dental, Inc, Carlsbad, CA). Le site greff a t entirement recouvert dune membrane en pricarde (membrane CopiOs Pericardium, Zimmer Dental, Inc, Carlsbad, CA.) (Fig. 8).
Nous avons ralis une fermeture sans tension des tissus mous (Fig. 9).
En post-opratoire, la patiente a reu des antibio-tiques, des bains de bouche antimicrobiens et un traite-ment antalgique.
La cicatrisation post-opratoire sest droule sans histoire et sans signes cliniques dinfection, dhiscence ou problmes cliniques.
La sance de pose dimplants a t prvue 6 mois plus tard. Avant dexposer le site, une radiographie a t ralise afin dvaluer lincorporation du bloc cortico-spongieux (I-CAT, systme dimagerie dentaire Cone Beam en 3-D) (Fig. 10).
Le site a t expos sous anesthsie locale, ce qui a permis de dcouvrir un bloc bien intgr, dsormais in-corpor dans los environnant. Les vis de fixation ont t retires. Aprs la procdure daugmentation, la largeur de la crte avait atteint les 9 mm. Le site implantaire a t prpar par un forage squentiel sous irrigation selon le
Fig. 10valuation radiologique du greffon 6 mois.
Fig. 11Deuxime chirurgie. Pose de limplant.
Fig. 12Sutures.
A r g i b Ay L o r e n z o o, C A r r A L F r e i r e C , b L A n C o C A r r i n J
18
b
a
VOLUME 30 NUMRO 2 bis 2014
osseuse tait ncessaire pour pouvoir placer correcte-ment les implants (sur la base de considrations pro-thtiques) (Fig. 13).
Nous avons dcid de raliser une greffe dos au-togne sur le ct droit, et une allogreffe sur le ct gauche (Puros Block Allograft, Zimmer Dental, Inc, Carlsbad, CA).
Procdure chirurgicale : aprs avoir anesthsi la patiente par des infiltrations locales, il a t pratiqu une incision mdio-crestale. Un lambeau mucopriost a t soulev pour exposer la crte alvolaire rsiduelle, qui mesurait de 2 3mm de large (Fig. 14).
Lallogreffe strile (Puros Block Allograft, Zimmer Dental, Inc, Carlsbad, CA) a t hydrate selon la proc-dure dcrite dans le cas prcdent.
Des trous daccs ont t prpars au travers du gref-fon par un foret de 1,5 mm de diamtre (Straumann AG, Ble, Suisse), jusqu los receveur sous-jacent, afin dy loger les vis de fixation.
Ceci fait, le bloc a t plac dans le site chirurgical, o il a t stabilis laide de deux mini-vis (Straumann AG, Ble, Suisse) pour prvenir la rotation du greffon (Fig. 7).
Du ct controlatral, nous avons utilis la zone postrieure de la mandibule comme deuxime site chirurgical, afin dy prlever un greffon dos autogne. Ce greffon a t dabord prpar, puis fix, galement avec des mini-vis (Fig.16).
Le modelage final du greffon a t ralis dans la cavit buccale. Autour du bloc, les espaces vides ont t remplis avec des particules osseuses (particules corti-
Figg. 13a,bExamen clinique et radiologique initial.
protocole standard (Straumann Dental Implant System, Ble, Suisse) (Fig. 11).
2e CASPatient: dans ce cas, nous avons trait une femme
de 55 ans, en bonne sant systmique et totalement dente. Lexamen clinique et les radiographies ont montr une perte osseuse svre dans les zones den-tes. Toutes les diffrentes alternatives de traitement ont t discutes de faon approfondie. Une greffe
Fig. 14 Crte alvolaire rsiduelle.
Fig. 15 Stabilisation du greffon et contact osseux.
19
A r g i b Ay L o r e n z o o, C A r r A L F r e i r e C , b L A n C o C A r r i n J
a b
VOLUME 30 NUMRO 2 bis 2014
Figg. 16a,bGreffon autologue provenant de la mandibule.
Fig. 17Particules osseuses dans les espaces autour du matriau greff et du greffon autologue.
Fig. 18Sutures.
Fig. 19Examen radiologique 6 mois (greffon autologue). Fig. 20Examen radiologique 6 mois (Allogreffe).
A r g i b Ay L o r e n z o o, C A r r A L F r e i r e C , b L A n C o C A r r i n J
20 VOLUME 30 NUMRO 2 bis 2014
cales Puros, Zimmer Dental, Inc, Carlsbad, CA) (Fig.17). Le tout a t couvert dune membrane en pricarde (membrane CopiOs Pericardium Zimmer Dental, Inc, Carlsbad, CA.)
Aprs la fermeture des tissus mous sans tension, nous avons enfin sutur les lambeaux (Fig. 18).
En post-opratoire, la patiente a reu des antibio-tiques, des bains de bouche antimicrobiens et un trai-tement antalgique.
La cicatrisation post-opratoire sest droule sans histoire et sans signes cliniques dinfection, dhiscence ou problmes cliniques.
La sance de pose dimplants a t prvue 6 mois plus tard. Avant dexposer le site, des radiographies ont t ralises afin dvaluer lincorporation des greffons (I-CAT, systme dimagerie dentaire Cone Beam en 3-D) (Fig. 19-20).
Le site a t expos sous anesthsie locale, ce qui a permis de dcouvrir un bloc bien intgr, dsormais incorpor dans los environnant. Aprs avoir retir les vis de fixation, ltape suivante a t la pose guide dimplants, laide du guide chirurgical (Straumann Dental Implant System, Ble, Suisse) (Fig. 21)
Pendant la pose des implants, il ny a pas eu de com-plications chirurgicales au niveau de los rgnr. Ceci fait, les lambeaux ont t suturs (Fig. 22)
Quatre semaines plus tard, la patiente a reu son provisoire, et 10 mois plus tard la prothse dfinitive, qui a pu tre pose de faon optimale (Fig. 23).
RSULTATS
Ces cas dcrivent la rponse de cicatrisation aprs une procdure daugmentation de crte latrale par les particules dos spongieux minralis Puros(Zimmer Dental, Inc, Carlsbad, CA), suivie par la pose secondaire dimplants et par la pose dune prothse.
Aprs six mois de cicatrisation, le matriau greff tait parfaitement intgr dans le site receveur, aussi bien dun point de vue clinique que radiographique. Les implants ont t poss sans complications, en position prothtiquement idale.
Au bout dun an de cicatrisation, et 6 mois aprs la pose des implants et de la prothse, les rsultats taient
Fig. 21Pose des implants (deuxime chirurgie).
Fig. 22Sutures.
Fig. 23Rsultat final. Fig. 24Restauration finale (vue clinique).
21
A r g i b Ay L o r e n z o o, C A r r A L F r e i r e C , b L A n C o C A r r i n J
VOLUME 30 NUMRO 2 bis 2014
stables. Aucun signe de changements structurels ou de rsorption osseuse ntait constat.
DISCUSSION
6 mois aprs la mise en charge, les rsultats esth-tiques et fonctionnels de ces cas cliniques o les im-plants ont t poss aprs rgnration de crte lat-rale par le matriau dallogreffe Puros (Zimmer Dental, Inc, Carlsbad, CA) et la membrane en pricarde CopiOs taient excellents, ce qui tait par ailleurs confirm par les rsultats cliniques et radiologiques.
Une greffe russie implique un processus de revascu-larisation concomitante et le remplacement du greffon par los de lhte, sans pertes significatives en termes de force et de volume. Le volume osseux est important pour de nombreux facteurs lis la sant buccale et au traitement de restauration potentiel, y compris la posi-tion et la localisation des implants poss, leur succs ou leur chec, et lesthtique des restaurations dfinitives.
Lutilisation des allogreffes a des avantages, dont notamment labsence de limites quant au nombre de greffons disponibles, llimination du deuxime site chirurgical pour le prlvement dos autologue et la possibilit dviter la morbidit du site donneur.
Los des donneurs dcds utilis dans Puros est fourni par une banque des tissus certifie (selon lgis-lation en vigueur du pays).
Le matriau allognique, qui consiste en de los corti-cal provenant de donneurs humains, a t soumis un procd brevet en 5 tapes (Tutoplast) afin dassurer sa scurit biologique. Les phases de ce procd sont les suivantes : dlipidation (limination des graisses), traitement osmotique, oxydation au proxyde dhy-drogne, dshydratation par solvant et irradiation par rayonnement gamma faible dose. Ce traitement inac-tive le virus du VIH et lagent responsable de la maladie
de Creutzfeldt-Jakob. Dans une tude exprimentale des tissus prlevs chez des sujets dcds de SIDA et dhpatite C, ne prsentaient plus aucun signe infec-tieux lissue du traitement5.
Le site greff a t entirement recouvert dune membrane en pricarde (membrane CopiOs Pericar-dium, Zimmer Dental, Inc, Carlsbad, CA.)
La membrane en pricarde CopiOs assure une bar-rire long terme. Selon une tude animale de Rotha-mel et ses coll.6, le temps de rsorption de la membrane est 20 24 semaines. Selon ces Auteurs, la membrane en pricarde favorise ladhsion et la prolifration des fibroblastes du ligament parodontal humain, ainsi que celles des ostoblastes humains. La membrane en pri-carde CopiOs est galement traite selon les diffrentes tapes du procd brevet Tutoplast.
Nanmoins les critres scientifiques sont encore insuffisants pour valider cette technique. Ds lors, il faudra raliser des essais cliniques randomiss.
BIBLIOgRApHIE 1. Alberktsson T, Zarb G, Whortington P &Ericsson A R. the long term
efficacy of currently use dental implants: a review and proposed crite-ria of success. International Journal of Oral and Maxillofacial Implants. 1986; 1:11-25.
2. Becker W, Urist M, Becker BE. Clinical and histological observations of the sites implanted with intraoral autologous bone grafts or allografts. 15 human case reports. J Periodontol 1996; 67: 1025-33.
3. Keith DJ, Petrungaro SS, ELwell CW, Caputo C, Scopf C. Clinical and his-tological evaluation of a mineralized block allograft: results from the development period (2001-2004). Int J Periodontics and Restorative Dent 2006; 26: 321-27.
4. Froum SJ, Tarnow DP, Wallace SS. The use of a mineralized allograft for sinus augmentation: an interim histological case report from a prospective clinical study. Compend Contin Educ Dent 2005; 26:81-86.
5. Schopf C, Diaber W, Tadiz D. Tutoplast poocessed allografts and xeno-grafts. 3D Block technique from image diagnostics to block graft bone regeneration. Milano, Italy: RC Libri SRL 2005; 53-75.
6. Rothamel D, Schwarz F, Sager M, Herten M, Sculean A, Becker J. Biodegradation of differently cross linked collagen membranes. An experimental study in the rat. Clin Oral Impl Res 2005; 16: 369-78.
23VOLUME 30 NUMBER 2bis 2014
* Dental School of the Ludwig-Maximilian University of Munich. Department of Prosthodontics - Goethestr 70 - 80336 Munich, Germany.
The digital fabrication of dental restorations has become a standard procedure during the last decade.
Intraoral scanning devices are about to be established in general dental offices. However, up until now,
digital fabrication has solely concerned the replacing of analogue workflows without further benefits. The
presented concept for implant-supported single crowns describes a digital approach without a physical
model from implant placement to delivery of the final restoration in 2 appointments. Here, the benefits of
digital fabrication and the unique way to scan the implant right after placement give an additional value that
would not be achieved by analogue techniques. In addition to financial benefits, it represents the biologically
advantageous, one-abutment, on-time approach with customized screw-retained, full-contour crowns made
from lithium-disilicate.
Key Words: Dental implant, Digital dentistry, One-abutment one-time, Biological.
Florian Beuer*, Josef Schweiger*, Jan-Frederik Gth*
Digital Dentistry meets Implantology The Munich Implant Concept - A case report
IntroductIon
During the last decades, implant supported restora-tions have significantly changed prosthetic treatment concepts and their reliability could be proved scien-tifically.1-4 In particular, single implants help to avoid sacrificing natural tooth structure when fixed dental prostheses (FDPs) supported from adjacent teeth can be avoided. However, to achieve a functional, esthetic, and biological long-term success, several clinical con-siderations have to be taken into account, of which the soft tissue conditions around the implant can be con-sidered as one of the most important factors.5
The interface, which is established during soft tis-sue healing between the peri-implant mucosa and the
implant/abutment, consists of an epithelium and a con-nective tissue component.6 Berglundh et al. reported a length of approximately 2 mm for the junctional epithe-lium and a height of 1-2 mm for the connective tissue zone, resulting in a total transmucosal attachment of 3-4 mm.7 Several technical factors might possibly influ-ence the condition of this critical peri-implant mucosa, such as the material of the abutment, the veneering material, the fit of the abutment or a platform-switch.8,9
For example, different abutment materials lead to dif-ferent histological findings of the peri-implant mucosa. Thus, titanium and zirconia were reported to show fa-vorable quality of the attachment between implant and mucosa compared to gold-alloys. In particular, an apical shift of the mucosal barrier and the marginal bone was shown for gold-alloy abutments after 5 months in an animal study.10 On the other hand, veneering porcelain failed to establish a stable barrier resulting in recessions of the mucosa and bone resorption.11 Unfortunately, the influence of the match of the implant and the abutment on soft tissue stability and bone remodeling remains unclear at the moment. However, no negative effects of platform switching have been published. Furthermore, the clinical impact of the implant abutment connection cannot be stated clearly.12
Correspondence: Priv. Doz. Dr. Florian BeuerDental School of the Ludwig-Maximilian University of MunichDepartment of ProsthodonticsGoethestr 70 - 80336 MunichTel. +49 89 5160 9558 - Fax +49 89 5160 9502E-mail: [email protected]
B e u e r F, S c h w e i g e r J , g t h J F
24 VOLUME 30 NUMBER 2bis 2014
In contrast, some clinical procedures are known to influence the soft tissue around dental implants. For ex-ample, frequent probing at dental implants was shown to increase the pocket probing depths and markedly disrupted the epithelial and connective tissue attach-ment.13 Additionally, an elevation of a full flap (perios-teum) leads to a substantial loss of hard tissues and therefore influences the soft tissue behavior.14 Further-more, the prosthetic treatment concept was reported to influence the stability of the soft tissues. Repeated abutment change was associated with a disruption of the mucosal seal and an increase of the dimension of the transmucosal barrier in an animal study. If zirconia was used as abutment material, the effect was even stronger. As such, from a histological point of view, abutments should not be changed after once they have been placed.15 In this context, interesting concepts e.g., the one abutment-one time concept have been already described. Against a control group using provi-sional abutments, the one abutment-one time group showed significantly less bone loss at the 18 months and 3 years recall after implant placement.16
Today, the computer-aided design (CAD)/computer aided manufacturing (CAM) of implant abutments has become a new standard for customized abutments. However, using digital technology for fabrication of dental restorations requires the digitalization of the oral situation. This can be done either by direct digi-talization, using an intraoral scanning device, or by in-direct digitalization of a plaster model in the dental laboratory.17 Because of the multiple potential sources of error during the conventional way, including con-ventional impression, plaster model, and indirect digi-
talization, the direct digitalization using an intraoral scanner seems to be the most logical way to access the digital workflow and CAD/CAM.18-20 As a whole, the digital workflow offers the possibility to facilitate the daily procedures and offers new, innovative treatment strategies that provide advantages for dentists, dental technicians, and patients.
Against this background, this report introduces the Munich Implant concept (MIC) that describes the treatment of a patient with an implant-supported, full-contour crown within two appointments without any physical model, using intraoral scanning and CAD/CAM technology.
cASE rEPort
Anamnesis and Preoperative ProcedureA 44-year old male patient was referred to the De-
partment of Prosthodontics with a periapical ostitis after endodontical treatment of his mandibulary right first molar (FDI 46, Fig. 1). The severe destruction and heavy inflammation made the extraction of the tooth necessary. After discussing the alternative treatments, the patient decided to have a single-tooth implant and gave his informed consent.
Ten weeks after extraction, the soft tissue was healed (Fig. 2) and a cone-beam computer tomography (CT) of the site was made to receive three-dimensional in-formation about the soft and hard tissues (CS 9300, Carestream Dental, Rochester, NY, USA) at the desired implant position.
Fig 1X-ray of the preoperative findings: Apical ostitis at tooth 46 after root canal treatment and severe coronal destruction lead to the extraction of tooth.
Fig 2Pre-operative situation 10 weeks after extraction of tooth FDI 46.
B e u e r F, S c h w e i g e r J , g t h J F
25VOLUME 30 NUMBER 2bis 2014
Appointment 1: Implant Surgery and ScanningThe intraoral situation was digitized using an intra-
oral scanning device (Intrascan, Zfx, Dachau, Germany) to receive a dataset of the clinical situation (Fig. 3). This scan involved the mandible (gap and adjacent teeth), the maxilla, and a vestibular scan for bite-registration.
The patient was instructed to take antibiotics (Amoxicillin, 1.000 mg t.i.d.) and 400 mg of Ibuprofen one hour before surgery to prevent inflammation and swelling. Ibuprofen was continued for 2 days. Right be-fore surgery, the patient rinsed his mouth with a 0.2% chlorhexidine solution for 3 minutes21. A crestal incision in region 46 was followed by a sulcular incision at tooth 45 and tooth 47. A full-thickness flap was elevated, and all inflammatory and granulation tissue was debrided with a curette. For a tension-free wound closure, the periosteum was slitted at the basal of the flap, right at beginning of the surgery, to prevent bleeding by the time of the membrane placement at the end of the pro-
cedure. An implant (length 10 mm, diameter 4.7 mm, Trabecular Metal, Zimmer Dental, Freiburg, Germany) was placed at the planned position (Fig. 4).
After placement, a scan-body (experimental design, Zfx) was screwed to the primary stable implant to en-able the direct digitalization of the implant position (Fig. 5). The precise fit of the scan-body could be con-trolled easily, and the scan was conducted within the gingiva-extra scan-mode. During scanning, it was of paramount importance to also scan the adjacent teeth to enable a superimposition of the scan-body-dataset with the situation scan, which was conducted prior to surgery (Fig. 6).
After scanning, the scan body was removed, a covering screw was placed, and the wound was closed with a deep horizontal mattress and interrupted sutures (Prolene 6.0; Ethicon, Johnson & Johnson Medical, Norderstedt, Ger-many). A control x-ray was made (Fig. 7), and the patient was instructed on adequate behavior for the next days.
Fig 3Datasets (maxilla, mandible and bite-registration) of the preoperative situation after intraoral scanning using the Zfx Intrascan.
Fig 4Insertion of the implant during the first appointment (Trabecular Metal Implant, Zimmer Dental, Freiburg).
Fig 5Scan body placed on the implant immediately after insertion. The Scan body and adjacent teeth were scanned by a powder-free Intraoral-Scanner (Zfx Intrascan, Zfx, Dachau) to register the implant position.
Fig 6Dataset of the Scan body and adjacent teeth, that is to be superimposed with the preoperative scan-dataset.
B e u e r F, S c h w e i g e r J , g t h J F
26 VOLUME 30 NUMBER 2bis 2014
Wound healing was uneventful; the sutures were removed 8 days after implant placement. Subsequently, the scan-data was transferred online to the dental laboratory of the Department of Prosthodontics of the LMU Munich, where the crown was manufactured during the healing period.
LaboratoryThe scan data were imported into a CAD-Software
(Zfx-CAD-Software, Zfx) to design the final restoration (Fig. 8, 9). For the final restoration, the restorative team decided to deliver a full-contour crown made from lith-ium-disilicate (IPS e.max CAD, Ivoclar Vivadent, Schaan, FL), which was stained and glazed.22 The finalized crown was adhesively bonded (Multilink Implant, Ivoclar Viva-dent, Schaan, FL) to a titanium insert (Fig. 10) in ac-cordance to the manufacturers recommendations.23,24
Appointment 2: Re-entry and DeliveryAfter 12 weeks of healing, the reentry of the implant
took place, and the final crown was inserted. There-fore, only a mucosal flap was necessary, and the peri-
osteum could remain on the bone. The covering screw was removed; the implant was rinsed with isotonic so-dium chloride solution and dried. The screw-retained crown was tried in, occlusal and proximal contacts were checked and adapted. The crown was polished in the dental laboratory according to the manufacturers rec-ommendations and was cleaned in an ultrasonic bath. Before placing, the restoration was disinfected in 0.2% chlorhexidine solution. The crown was placed, and the screw was fixed with a torque moment of 20 Ncm. The soft-tissue was adapted to the crown with 2 papilla su-tures (Prolene 6.0, Ethicon, Johnson & Johnson Medi-cal, Norderstedt, Germany). Sutures were removed after uneventful healing after 6 days (Fig. 11).
18-month RecallAt the 18-month follow-up, stable soft and hard tis-
sue-conditions were found (Fig. 12, 13). The treatment outcome was met with full satisfaction of the patient. Unfortunately, the replacement of the adjacent crowns had to be postponed due to financial reasons.
Fig 7Post-surgery x-ray.
Fig 8Dataset after online-transfer to the dental laboratory and import to the dental CAD-Software (Zfx CAD Software, Zfx Dachau).
Fig 9CAD of the full-contour crown.
Fig 10 Milled full-contour crown from Lithium-Disilicate (IPS e.max CAD) in a pre-crystallized stage. After staining and glazing, the crown was adhesively bonded to the tita-nium insert, before delivery to the dental office.
B e u e r F, S c h w e i g e r J , g t h J F
27VOLUME 30 NUMBER 2bis 2014
dIScuSSIon
Today, the CAD/CAM-supported fabrication of abut-ments and implant-supported restorations can be considered as the new standard.25,26 In consideration of the industrial quality of the applied materials and the almost unlimited design-opportunities regarding the emergence profile, the dimensions and angula-tion of the restorations have to be mentioned as the major advantage of this digital procedure. In addition to higher mechanical stability that can be achieved by CAD/CAM-fabricated restorations22, concepts that offer additional value to patients and practitioners mean further advantages of digital implant-supported prosthodontics.
Regarding the MIC, the fabrication of the restora-tion during the (closed) healing-phase of the implant rationalizes the treatment-procedure. The accuracy of the transfer of the implant position by an intraoral scan seems to be sufficient for single tooth implants.27 Also, the adjacent teeth and antagonists are directly digi-tized, which facilitates the transfer of the situation to the dental laboratory. Based on the authors experience, physical models are not necessary for that kind of single tooth-restoration. When using a transfer-post after the healing-period, the correct fit is often controlled by an x-ray. When optical scanning is carried out immediately after surgery, before the wound is closed, the fit of the scan-body can be easily controlled visually without ra-diation exposure.
After placement of the restoration at the time of uncovering the implant, the healing of the soft-tissue takes place at the definitive restoration instead of at a healing abutment. Consequently, the emergence profile heals immediately toward an optimal shape. In contrast, standard healing abutments exhibit a round profile, which means that the cross section of the emer-gence profile has to be modified from round-shaped toward root-shaped before placement of the defini-tive restoration. This is achieved by repeated change of provisional restorations or continuously individual-ized healing-abutments to apply gentle pressure on the emergence profile.28 However, too much high pressure might cause a change of the mucosa that can lead to a loss of attached gingiva and recessions.29
Additionally, the immediate placement of the defini-tive restoration enables the formation of a long junc-tional epithelium between the restoration and soft-tissues that should not be separated again6,10,15,30. This sealing between the oral environment and the alveolar
Fig 11 Inserted crown one week in situ before suture-removal.
Fig 1218 month recall: The x-ray shows stable conditions of the bone around the implant and adjacent teeth.
Fig 1318 month recall: Stable conditions of the soft-tissue around the implant-supported crown could be observed.
B e u e r F, S c h w e i g e r J , g t h J F
28 VOLUME 30 NUMBER 2bis 2014
bone is an important factor for the long-term success of implant-supported restorations.9,30,31 In consideration of these findings less peri-implant inflammation can be expected when the junctional epithelium is not de-tached and injured. However, this has to be proven in animal experiments and clinical studies.
Observed from Seen from the economic standpoint, the concept offers clear advantages for dentists and patients. On the one hand, the concept saves treatment time, yet the healing period does not have to be ab-breviated. On the other hand, the MIC-concept offers saving-potential regarding additional implant parts, as there is no need for transfer posts and healing-abut-ments.
A screw-retained full contour crown from lithium-disilicate on a titanium insert seems to be the perfect restorative approach for the presented concept. Even in cases where the soft-tissue-level might heal more apical from the planned level, there will be no aestheti-cal or functional disadvantages due to the continuous color and form of the restoration. However, the concept is also possible for cemented restorations with an abut-ment and a cemented crown.9
Overall, the Munich Implant Concept represents a concept with economical and biological advantages for practitioners and patients, and the ongoing integration of the digital workflow offers the potential of further enhancements and simplifications.
rEFErEncES 1. Akca K, Uysal S, Cehreli MC. Implant-tooth-supported fixed partial
prostheses: correlations between in vivo occlusal bite forces and marginal bone reactions. Clin Oral Implants Res 2006; 17: 331-336.
2. Buser D, Mericske-Stern R, Bernard JP, et al. Long-term evaluation of non-submerged ITI implants. Part 1: 8-year life table analysis of a prospective multi-center study with 2359 implants. Clin Oral Implants Res 1997; 8: 161-172.
3. Kopp KC, Koslow AH, Abdo OS. Predictable implant placement with a diagnostic/surgical template and advanced radiographic imag-ing. J Prosthet Dent 2003; 89: 611-615.
4. Krennmair G, Krainhofner M, Waldenberger O, Piehslinger E. Dental implants as strategic supplementary abutments for implant-tooth-supported telescopic crown-retained maxillary dentures: a retrospective follow-up study for up to 9 years. Int J Prosthodont 2007; 20: 617-622.
5. Happe A, Stimmelmayr M, Schlee M, Rothamel D. Surgical manage-ment of peri-implant soft tissue color mismatch caused by shine-through effects of restorative materials: one-year follow-up. Int J Periodontics Restorative Dent 2013; 33: 81-88.
6. Zucchelli G, Mazzotti C, Mounssif I, Mele M, Stefanini M, Monte-bugnoli L. A novel surgical-prosthetic approach for soft tissue dehiscence coverage around single implant. Clin Oral Implants Res 2013; 24: 957-962.
7. Berglundh T, Lindhe J, Ericsson I, Marinello CP, Liljenberg B, Thomsen P. The soft tissue barrier at implants and teeth. Clin Oral Implants Res 1991; 2: 81-90.
8. Rodriguez AM, Rosenstiel SF. Esthetic considerations related to bone and soft tissue maintenance and development around dental implants: report of the Committee on Research in Fixed Prosth-odontics of the American Academy of Fixed Prosthodontics. J Prosthet Dent 2012; 108: 259-267.
9. Esposito M, Maghaireh H, Grusovin MG, Ziounas I, Worthington HV. Soft tissue management for dental implants: what are the most effective techniques? A Cochrane systematic review. Eur J Oral Implantol 2012; 5: 221-238.
10. Welander M, Abrahamsson I, Berglundh T. The mucosal barrier at implant abutments of different materials. Clin Oral Implants Res 2008; 19: 635-641.
11. Abrahamsson I, Berglundh T, Glantz PO, Lindhe J. The mucosal at-tachment at different abutments. An experimental study in dogs. J Clin Periodontol 1998; 25: 721-727.
12. Schwarz F, Alcoforado G, Nelson K, et al. Impact of implant-abut-ment connection, positioning of the machined collar/MICrogap, and platform switching on crestal bone level changes. Camlog Foundation Consensus Report. Clin Oral Implants Res 2013.
13. Schwarz F, Mihatovic I, Ferrari D, Wieland M, Becker J. Influence of frequent clinical probing during the healing phase on healthy peri-implant soft tissue formed at different titanium implant surfaces: a histomorphometrical study in dogs. J Clin Periodontol 2010; 37: 551-562.
14. Araujo MG, Lindhe J. Ridge alterations following tooth extraction with and without flap elevation: an experimental study in the dog. Clin Oral Implants Res 2009; 20: 545-549.
15. Becker K, Mihatovic I, Golubovic V, Schwarz F. Impact of abutment material and dis-/re-connection on soft and hard tissue changes at implants with platform-switching. J Clin Periodontol 2012; 39: 774-780.
16. Canullo L, Bignozzi I, Cocchetto R, Cristalli MP, Iannello G. Immedi-ate positioning of a definitive abutment versus repeated abutment replacements in post-extractive implants: 3-year follow-up of a randomised multicentre clinical trial. Eur J Oral Implantol 2010; 3: 285-296.
17. DIN13995:2010-02. Dentistry - Terminology of process chain for CAD/CAM-systems. 2010.
18. Christensen GJ. The challenge to conventional impressions. J Am Dent Assoc 2008; 139: 347-349.
19. Christensen GJ. The state of fixed prosthodontic impressions: room for improvement. J Am Dent Assoc 2005; 136: 343-346.
20. Christensen GJ. Laboratories want better impressions. J Am Dent Assoc 2007; 138: 527-529.
21. Stimmelmayr M, Stangl M, Edelhoff D, Beuer F. Clinical prospective study of a modified technique to extend the keratinized gingiva around implants in combination with ridge augmentation: one-year results. Int J Oral Maxillofac Implants 2011; 26: 1094-1101.
22. Guess PC, Zavanelli RA, Silva NR, Bonfante EA, Coelho PG, Thomp-son VP. Monolithic CAD/CAM lithium disilicate versus veneered Y-TZP crowns: comparison of failure modes and reliability after fatigue. Int J Prosthodont 2010; 23: 434-442.
23. Stimmelmayr M, Edelhoff D, Guth JF, Erdelt K, Happe A, Beuer F. Wear at the titanium-titanium and the titanium-zirconia implant-abutment interface: a comparative in vitro study. Dent Mater 2012; 28: 1215-1220.
24. Stimmelmayr M, Sagerer S, Erdelt K, Beuer F. In vitro fatigue and fracture strength testing of one-piece zirconia implant abutments and zirconia implant abutments connected to titanium cores. Int J Oral Maxillofac Implants 2013; 28: 488-493.
25. Beuer F, Schweiger J, Edelhoff D, Sorensen JA. Reconstruction of esthetics with a digital approach. Int J Periodontics Restorative Dent 2011; 31: 185-193.
26. Beuer F, Schweiger J, Edelhoff D. Digital dentistry: an overview of recent developments for CAD/CAM generated restorations. Br Dent J 2008; 204: 505-511.
27. Syrek A, Reich G, Ranftl D, Klein C, Cerny B, Brodesser J. Clinical evaluation of all-ceraMIC crowns fabricated from intraoral digital impressions based on the principle of active wavefront sampling. J Dent 2010; 38: 553-559.
B e u e r F, S c h w e i g e r J , g t h J F
29VOLUME 30 NUMBER 2bis 2014
28. Khoury F, Happe A. Soft tissue management in oral implantology: a review of surgical techniques for shaping an esthetic and func-tional peri-implant soft tissue structure. Quintessence Int 2000; 31: 483-499.
29. Stimmelmayr M, Allen EP, Reichert TE, Iglhaut G. Use of a combina-tion epithelized-subepithelial connective tissue graft for closure and soft tissue augmentation of an extraction site following ridge preservation or implant placement: description of a technique. Int J Periodontics Restorative Dent 2010; 30: 375-381.
30. Cochran DL, Mau LP, Higginbottom FL, et al. Soft and hard tissue histologic dimensions around dental implants in the canine re-stored with smaller-diameter abutments: a paradigm shift in peri-implant biology. Int J Oral Maxillofac Implants 2013; 28: 494-502.
31. Cutrim ES, Peruzzo DC, Benatti B. Evaluation of soft tissues around single tooth implants in the anterior maxilla restored with cement-ed and screw-retained crowns. J Oral Implantol 2012; 38: 700-705.
30
31VOLUME 30 NUMBER 2bis 2014
* Private practice, Tal 13, D 80331 Munich, Germany.** Private practice, Johannisbollwerk 20, D 20459 Hamburg,
Germany.
Aim: Severe alveolar ridge deficiencies i.e. as a result of trauma and edentulism require bone augmentation
before implant placement. Many different techniques and materials are available and have been investigated
in the last 3 decades. One promising material group are block grafts for onlay block augmentation to
reconstruct larger deficiencies of the jaw. Besides this, allogeneic block grafting becomes more and
more attractive since allogeneic materials offers some advantages compared to autogenous bone blocks.
However, there was still no surgical guide described in the literature to achieve predictable results with
allograft blocks. This article discusses material properties, surgical recommendations and the influence of
different treatment steps on the outcome of allogeneic block grafting.
Key Words: Bone allograft, Block augmentation, Puros, Augmentations recommendations.
Oliver Blume*, Ole Richter**, Michael Back*, Thomas Mller-Hotop*
Surgical recommendations for allograft block grafting
IntroductIon
Dental implants are widely used in oral reconstruc-tion for the replacement of missing teeth. In many cases pre-implant augmentative surgeries are neces-sary due to loss of bone volume followed by second stage implant placement. Bone regeneration of minor defects can be done according the the guided bone regeneration procedure with different bone graft mate-rials in combination with resorbable or non-resorbable membranes1,2. For vertical and lateral augmentations of the jaw autogenous bone block have been harvested from different intra and extra-oral origins i.e. chin, ra-mus or iliac crest to reconstruct the ridge3-5. Despite autogenous bone is considered as the gold standard, harvesting of autogenous bone brings with several drawbacks. Clinical concerns are donor site morbidity,
pain, swelling, bone quality and quantity depending on the donor site as well as graft resorption during heal-ing and increased chair time6-9. For this reasons block grafts of synthetic10,11, xenogenic12,13 and allogeneic14-17
origin have been investigated. The most successful re-sults have been obtained by choosing allogeneic bone blocks since allogeneic bone is similar to autogenous bone and possess a great biological quality18,19. It was shown earlier that performance of autogenous and al-logeneic onlay grafts for ridge augmentation is com-parable20. Today allogeneic block grafts have the ad-vantages of unlimited supply and can be ordered in different packagings and compositions (cancellous or cortico-cancellous blocks). Different kinds of allogeneic materials are available depending on the harvesting and processing of the donor material. Going through this fresh-frozen21,22, freeze-dried23,24, mineralized25, de-mineralized 26 and solvent-preserved, gamma steril-ized15,17,27 allogeneic materials have been investigated for their use in clinical dentistry. From a safety point of view allogeneic materials are sometimes considered as highly risky since reports were published describ-ing disease transmissions28-30. Looking deeper in these articles shows that in the cases of disease transmissions non-purified, non-tested donor material was used.
Correspondence: Oliver Blume Tal 13, D 80331 Munich, GermanyE-mail: [email protected]
B lu m e O, R i c h t e R O, B a c k m, m l l e R -h O tO p t
32 VOLUME 30 NUMBER 2bis 2014
Today, harvesting and processing of allogeneic bone blocks is regulated by different government and indus-try entities depending of the national law31-33 and are considered as safe.
Different surgeons chose different treatments steps while using autogenous or allogeneic blocks to rebuild defects of the jaw. Up to know no surgical protocol has been published dealing with the needs and risks of al-lograft block grafting in dental surgery to obtain pre-dictable results. The aim of this article is to review and discuss different surgical steps reg. to their impact of the surgical outcome of block grafting with Puros Al-lograft blocks.
MaterIals and Methods
Puros Allograft Block Puros Allograft blocks are processed by the Tutoplast
process. The process gently removes unwanted material such as fats, cells, antigens and inactivates pathogens, while preserving the bone mineral and collagen matrix34. The processing consists of six consecutive steps as shown in Fig 1. and was described in detail previously34. A key benefit of the Tutoplast process is the preservation of the natural composition of the collagen and bone mineral. Since the donated tissue is handled during processing at max. 37 C there are no structural and chemical changes in the collagen and bone mineral structure as well as composition. Further the gentle solvent dehydration and the low dose gamma irradiation (dose < 25 kGy) ensure
that the natural cross links of the collagen fibers will be maintained 35-37 resulting in a sterile allograft with great biological and mechanical performances. The mechani-cal properties of the processed tissue are comparable with the non-processed raw material allowing an easy handling and shaping of the bone blocks38,39. Moreover the preserved collagen/mineral structure will be remod-eled and revascularized into new, vital bone within 612 month by osteoclastic and osteoblastic activities17, 40.
Block grafting surgical procedure 1. Allograft block preparation
During processing the bone blocks have been de-hydrated resulting in a white, brittle bone block which could fracture during shaping. Based on this the bone blocks have to re-wetted prior shaping in sterile sa-line or water. An easy and effective way doing this is to place the bone block into a syringe and draw sterile saline into the syringe until the block graft is complete-ly covered. By pulling on the plunger of the syringe a negative pressure will be applied and air trapped in the trabecular structure of the graft begins to expel. This procedure has to be repeated several times till all bubbles have been removed (Fig 2). The block should be placed in saline solution for additional 10 15 min to get fully saturated. The fully wetted block is hydro-philic allowing easy penetration of blood if placed at the recipient site.
2. Preparation of recipient site and block shapingThe recipient site has to be evaluated for hard and
soft tissue deficiencies, aesthetic concerns and health
Fig 1Tutoplast processing of Puros Al-lografts.
B lu m e O, R i c h t e R O, B a c k m, m l l e R -h O tO p t
33VOLUME 30 NUMBER 2bis 2014
status of the adjacent teeth - if there are any. An ad-equate incision design should be chosen to raise a flap allowing access to the surgical field and to ensure a tension-free closure after grafting. In fact flap design is a critical aspect in the entire grafting procedure since esthetic aspects play a decisive role, especially in the anterior maxilla. The surgeon should know biotype, soft tissue thickness, soft tissue amount and consider that larger hard tissue volumes have to be covered after bone grafting to decide which incision technique en-sures a complete covering. Several types of incisions are known to raise either full thickness or split-flaps such as midcrestal, lingual, vestibular incisions with/without vertical releasing incisions41,42. By choosing a midcrestal incision extension of the incision at least one tooth mesial and distal of the recipient site is recom-mended (Fig 3).
If scoring of the periosteum is considered to ensure a tension-free adaption of the flap some colleagues
incise periosteum immediately after raising the flap to allow time for hemostasis enabling good visibility of the surgical field, easier placement of particulate graft material and a membrane. However, since incision and flap design can impact the vascularization of the flap an appropriate technique is recommended to avoid flap necrosis if blood supply becomes diminished43. Both the recipient site and the block graft should be shaped to achieve close approximation of their surfaces since intimidate contact is mandatory for incorporation of the graft and success of the entire grafting procedure. (1) The wetted allograft block can be shaped with differ-
ent rotating or cutting instruments with minimum risk of fracture. Care has to be taken that shaping will be done under saline solution to avoid heating of the block and denaturation of the collagen matrix (Fig 4).
(2) At the recipient sites preparation includes decorti-cation and perforation of the host bone to promote blood supply to the graft. If sufficient host bone is pres-
Fig 2Rehydration of an allograft block in saline.
Fig 3Midcrestal inscision with one vertical releasing