Embed Size (px)
Citation preview
The Spine Journal 9 (2009) 735–743
Technical Report
Revision strategies for single- and two-level total disc arthroplastyprocedures: a biomechanical perspective
Bryan W. Cunningham, MSca,b,*, Nianbin Hu, MDa,b, Helen J. Beatson, BSa,b,Hassan Serhan, PhDc, John C. Sefter, DOa,b, Paul C. McAfee, MDa,b
aOrthopaedic Spinal Research Laboratory, St. Joseph Medical Center, Towson, MD 21204, USAbScoliosis and Spine Center, St. Joseph Medical Center, Towson, MD 21204, USA
cDePuy Spine, Inc., Raynham, MA, USA
Received 2 August 2007; received in revised form 13 March 2009; accepted 28 March 2009
Abstract BACKGROUND CONTEXT: The utilization
FDA device/drug s
Disc; ISOLA Pedicle
Author disclosures
foundation).
1529-9430/09/$ – see
doi:10.1016/j.spinee.2
of motion-preserving implants versus conventional in-strumentation systems, which stabilize the operative segments, necessitates improved understanding oftheir comparative biomechanical properties and optimal biomechanical method for surgical revision.PURPOSE: Using an in vitro human cadaveric model, the primary objective was to comparethe multidirectional flexibility properties of single- versus two-level total disc arthroplasty proce-dures and determine the acute in vitro biomechanical characteristics of two methods of surgicalrevision—posterior transpedicular instrumentation alone or circumferential spinal arthrodesis.STUDY DESIGN: This in vitro biomechanical study was undertaken to compare the multidirec-tional flexibility kinematics of single- versus two-level lumbar total disc arthroplasty reconstruc-tions using an in vitro model.METHODS: A total of seven human cadaveric lumbosacral spines (L1-sacrum) were biomechani-cally evaluated under the following L4–L5 reconstruction conditions: intact spine; discectomy alone;Charite total disc replacement; Charite with pedicle screws; two-level Charite (L4–S1); two-levelCharite with pedicle screws (L4–S1); Charite L4–L5 with pedicle screws and femoral ring allograft(FRA) (L5–S1); and pedicle screws with FRA (L4–S1). Multidirectional flexibility testing used thePanjabi Hybrid Testing protocol, which includes pure moments for the intact condition with the overallspinal motion replicated under displacement control for subsequent reconstructions. Hence, changesin adjacent level kinematics can be obtained compared with pure moment testing strategies. Uncon-strained intact moments of 67.5 Nm were used for axial rotation, flexion-extension, and lateral bend-ing testing with quantification of the operative- and adjacent-level range of motion (ROM). All datawere normalized to the intact spine condition (intact5100%).RESULTS: In axial rotation, single- and two-level Charite reconstructions produced significantlymore motion than pedicle screw constructs combined with the Charite or FRA (p!.05). There wereno differences between the Charite augmented with pedicle screws or pedicle screws with FRA(pO.05). The two-level annulus lumbar resection required for multilevel Charite implantationhad an added destabilizing effect, resulting in a 140% to 160% ROM increase over the intact con-dition. Under two-level reconstructions, rotational motion at the L4–L5 level increased from160626% to 263665% with the implantation of the second Charite at L5–S1. Flexion-extensionand lateral bending conditions with the Charite reconstructions in this group of seven spines dem-onstrated no significant differences compared with the intact spine (pO.05). The Charite combinedwith pedicle screws or pedicle screws with FRA significantly reduced motion at the operative levelcompared with the Charite reconstruction (p!.05). The most pronounced changes in adjacent levelkinematics and intradiscal pressures were observed under flexion-extension loading. The addition ofpedicle screw fixation increased segmental motion and intradiscal pressures at the proximal anddistal adjacent levels compared with the intact and Charite reconstruction groups (p!.05).
tatus: approved for this indication (Charite Artificial
Screw Spinal System).
: BWC, NH, HJB, HS, JCS, PCM (funding, nonprofit
* Corresponding author. Orthopaedic Spinal Research Laboratory, St.
Joseph Medical Center, 7601 Osler Drive, Jordan Center, Suite 167, Tow-
son, MD 21204, USA. Tel.: (410) 337-1274; fax: (410) 427-2140.
E-mail address: [email protected] (B.W. Cunningham)
front matter � 2009 Elsevier Inc. All rights reserved.
009.03.011

736 B.W. Cunningham et al. / The Spine Journal 9 (2009) 735–743
CONCLUSIONS: The findings highlight a variety of important trends at the operative and adja-cent levels. In terms of revision strategies, posterior pedicle screw reconstruction combined with anexisting Charite was not found acutely to be statistically different from pedicle screws combinedwith FRA. � 2009 Elsevier Inc. All rights reserved.
Keywords: Multilevel total disc arthroplasty; Revision strategies; Motion preservation.
Introduction
Total disc arthroplasty is increasingly being used as analternative to interbody spinal arthrodesis in the treatmentof degenerative disc disease. This new technology offersa variety of clinical and research challenges, includingthe need for surgical revision. When used as an alternativeto interbody arthrodesis, an artificial disc serves to replacethe symptomatic degenerated disc, and may restore somefunctional biomechanical properties of the motion segment,protect neurovascular structures, and preserve certain kine-matic properties of the functional spinal unit.
From a basic scientific perspective, the long-term suc-cessful performance of total disc arthroplasty is based firstand foremost in the biomechanical motion-preserving prop-erties of the device. Assuming that proper surgical tech-nique and implant positioning are achieved, the initialbiomechanical stability and kinematics are of primary con-cern. To address these issues, previous in vitro biomechan-ical studies have investigated the motion-preservingproperties after total disc arthroplasty [1–4], quantifiedthe operative- and adjacent-level facet loads based on finiteelement modeling [5] and reported on pertinent clinical andbiomechanical objectives in lumbar disc arthroplasty[6–13]. However, no studies to date have defined the mul-tidirectional flexibility properties after surgical revision.Specifically, in cases requiring revision for a nondisplacedand nonfragmented prosthesis, is it biomechanically justi-fied to attempt to reconstruct the operative motion segmentusing a posterior pedicle screw–based system augmentedwith posterolateral arthrodesis, or is a combined anteropos-terior reconstruction procedure indicated? Moreover, arethere inherent differences in the flexibility properties ofsingle- versus multilevel arthroplasty procedures and howdo these differences influence the revision technique?
Using an in vitro human cadaveric model, the primaryobjective of this study was to compare the multi-directionalflexibility properties of single- versus two-level total discarthroplasty and revision constructs:posterior transpedicularinstrumentation alone or circumferential spinal arthrodesis.
Materials and methods
Specimen preparation
A total of seven fresh-frozen human cadaveric lumbosa-cral spines (age range 55–75 yr, mean 62 yr) were har-vested en-bloc and used in this investigation. Before
biomechanical analysis, standard anteroposterior and lateralplain films were obtained to exclude specimens demonstrat-ing intervertebral disc or osseous pathology. In preparationfor biomechanical testing, the lumbosacral spine wasthawed to room temperature and cleaned of all residualmusculature, with care taken to preserve all ligamentous at-tachments and facet joint capsules. The proximal (T12–L2)and distal (sacroiliac) ends of the specimen were secured inrectangular steel tubing foundations using eight compres-sion screws for fixation. Four Plexiglas motion detectionmarkers were placed on the anterior aspects of L3, L4,L5, and S1, and each marker was equipped with threenon-co-linear light emitting diodes designed for detectionby an optoelectronic motion measurement system.
Three-dimensional flexibility testing
Testing was performed using a custom designed six-degree-of-freedom spine simulator (six-degree-of-freedom-spine simulator) configured with an OptoTrak 3020 motionanalysis system (Northern Digital Corp., Ontario, Canada)The six-degree-of-freedom-spine simulator gimbal apparatusis configured with three independent stepper motors, har-monic drives, and electromagnetic clutches that are capableof applying pure, unconstrained rotational moments aboutthree axes (X, Y, and Z). Unconstrained translations (millime-ters) are permitted using linear bearing guide rails (X and Z)and MTS actuator (Y-axis) (Fig. 1). To determine the multidi-rectional flexibility, nondestructive, unconstrained loading pa-rameters included six pure moments:flexion and extension(6X-axis), lateral bending (6Z-axis), and axial rotation(6Y-axis) applied to the superior end (L2) of the verticallyoriented specimen, whereas the caudal portion of the speci-men (sacrum) remained fixed to a testing platform. The intactlumbar spinal segments were evaluated under axial rotation(Y-axis, 67.5 Nm), flexion-extension (X-axis, 67.5 Nm),and lateral bending (Z-axis, 67.5 Nm) testing modes usinga pure moment loading system operating in torque control.
After the intact specimen analysis, the hybrid testingprotocol proposed by Panjabi [14] was used such that thesystem was reprogrammed to operate in displacement con-trol with the intact segment’s full range of motion (ROM)serving as the angle limit in each loading direction. Eachtest was repeated for three loading and unloading cyclesat a rate of 3 degrees/second, with data from the third cycleused for computational analysis. To prevent desiccationduring assessment, specimens were moistened with 0.9%NaCl sterile irrigation solution.
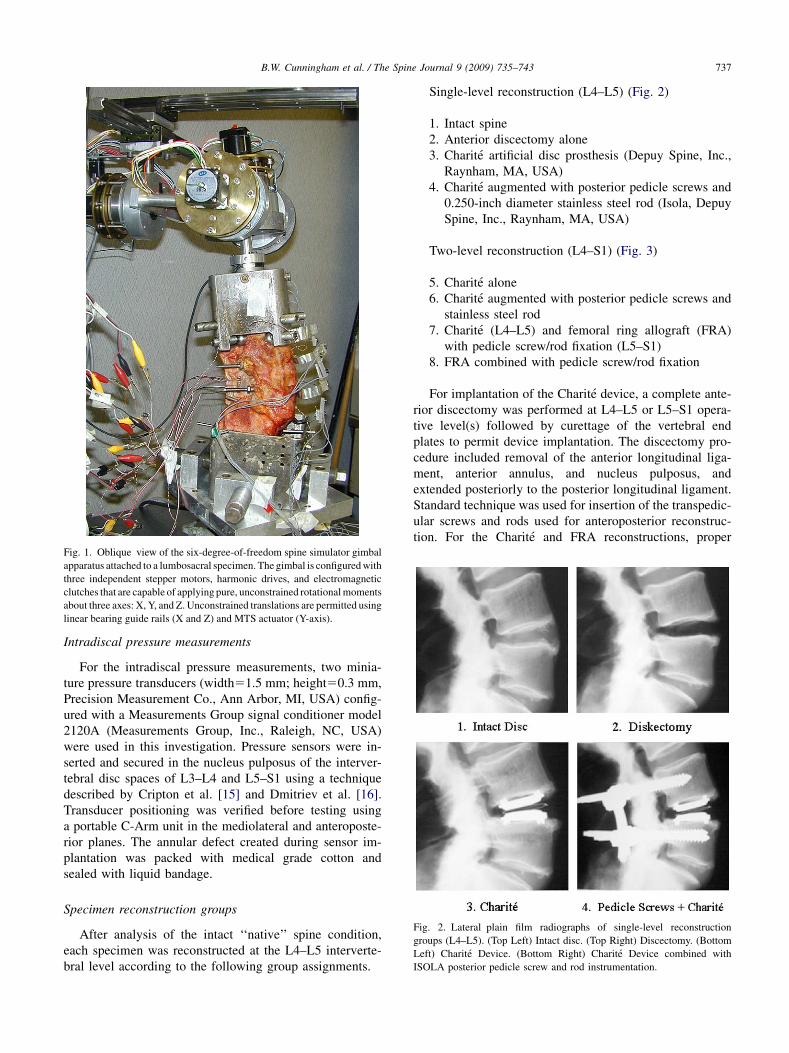
Fig. 2. Lateral plain film radiographs of single-level reconstruction
groups (L4–L5). (Top Left) Intact disc. (Top Right) Discectomy. (Bottom
Left) Charite Device. (Bottom Right) Charite Device combined with
ISOLA posterior pedicle screw and rod instrumentation.
Fig. 1. Oblique view of the six-degree-of-freedom spine simulator gimbal
apparatus attached to a lumbosacral specimen. The gimbal is configured with
three independent stepper motors, harmonic drives, and electromagnetic
clutches that are capable of applying pure, unconstrained rotational moments
about three axes: X, Y, and Z. Unconstrained translations are permitted using
linear bearing guide rails (X and Z) and MTS actuator (Y-axis).
737B.W. Cunningham et al. / The Spine Journal 9 (2009) 735–743
Intradiscal pressure measurements
For the intradiscal pressure measurements, two minia-ture pressure transducers (width51.5 mm; height50.3 mm,Precision Measurement Co., Ann Arbor, MI, USA) config-ured with a Measurements Group signal conditioner model2120A (Measurements Group, Inc., Raleigh, NC, USA)were used in this investigation. Pressure sensors were in-serted and secured in the nucleus pulposus of the interver-tebral disc spaces of L3–L4 and L5–S1 using a techniquedescribed by Cripton et al. [15] and Dmitriev et al. [16].Transducer positioning was verified before testing usinga portable C-Arm unit in the mediolateral and anteroposte-rior planes. The annular defect created during sensor im-plantation was packed with medical grade cotton andsealed with liquid bandage.
Specimen reconstruction groups
After analysis of the intact ‘‘native’’ spine condition,each specimen was reconstructed at the L4–L5 interverte-bral level according to the following group assignments.
Single-level reconstruction (L4–L5) (Fig. 2)
1. Intact spine2. Anterior discectomy alone3. Charite artificial disc prosthesis (Depuy Spine, Inc.,
Raynham, MA, USA)4. Charite augmented with posterior pedicle screws and
0.250-inch diameter stainless steel rod (Isola, DepuySpine, Inc., Raynham, MA, USA)
Two-level reconstruction (L4–S1) (Fig. 3)
5. Charite alone6. Charite augmented with posterior pedicle screws and
stainless steel rod7. Charite (L4–L5) and femoral ring allograft (FRA)
with pedicle screw/rod fixation (L5–S1)8. FRA combined with pedicle screw/rod fixation
For implantation of the Charite device, a complete ante-rior discectomy was performed at L4–L5 or L5–S1 opera-tive level(s) followed by curettage of the vertebral endplates to permit device implantation. The discectomy pro-cedure included removal of the anterior longitudinal liga-ment, anterior annulus, and nucleus pulposus, andextended posteriorly to the posterior longitudinal ligament.Standard technique was used for insertion of the transpedic-ular screws and rods used for anteroposterior reconstruc-tion. For the Charite and FRA reconstructions, proper

Fig. 3. Lateral plain film radiographs of two-level reconstruction groups
(L4–S1). (Top Left) Charite device. (Top Right) Charite device combined
with pedicle screw and rod instrumentation. (Bottom Left) Charite device
combined with pedicle screws and femoral ring allograft (FRA) spacer.
(Bottom Right) FRA spacers and pedicle screw/rod instrumentation.
738 B.W. Cunningham et al. / The Spine Journal 9 (2009) 735–743
intersegmental distraction and ligamentotaxis was achievedusing the David Spreader (Depuy-Spine, Raynham, MA,USA). The Charite implant was carefully removed andreplaced with an appropriately sized FRA spacer at theoperative L4–L5 and L5–S1 levels. All reconstructionsstrictly adhered to the manufacturer’s recommendations.
Data and statistical analysis
The intervertebral ROM at each intervertebral level (L3–L4,L4–L5, and L5–S1) was calculated as the sum of the neutraland elastic zones (neutral zone [NZ]þelastic zone [EZ]5ROM) and represents the peak total ROM (Euler angles rota-tion) at the third loading cycle. The expressed degrees of rota-tion (axial rotation6Y-axis, flexion-extension6X-axis, andlateral bending6Z-axis) for multi-directional flexibilityanalyses are according to the three-dimensional conceptualframework of Panjabi [17]. For the six main motions, corre-sponding to the peak angular displacement applied, theoperative- and adjacent-level vertebral rotations (degrees) werequantified in terms of peak ROM at maximum load. Intradiscalpressures recorded in pounds per square inch (psi) were quan-tified under peak lateral bending and flexion-extension loadingconditions. The non-destructive ROM data were normalized tothe intact spine condition (100%) for each loading mode,whereas intradiscal pressures are reported as absolute values(per square inch). Statistical analysis included descriptivesand a repeated measures analysis of variance with Student-Newman-Keuls test for group-to-group comparisons. Compar-isons with values of p!.05 were considered statisticallysignificant.
Results
Operative and adjacent level kinematics
Axial rotation (6Y-axis)Axial rotation loading produced the greatest differences
in segmental ROM at the operative and adjacent levels,particularly after two-level reconstructions. There were nodifferences observed at the L3–L4 level for any treatmentgroup—single- or two-level (pO.05). The motion producedat L4–L5 after a single-level discectomy, single-level Char-ite or two-level Charite (L4–S1) was significantly greaterthan the intact, Charite combined with pedicle screws andFRA combined with pedicle screws (single and two levels)(p!.05). The most pronounced changes in L4–L5 segmen-tal motion were observed for the two-level Charite recon-struction and hybrid reconstruction—Charite (L4–L5)combined with pedicle screws and FRA (L5–S1). Whencompared with the intact condition, segmental motion atthe L4–L5 level markedly increased from 160626% to263665% with the implantation of the second Charite atL5–S1. Moreover, the addition of pedicle screws andFRA at L5–S1 further increased the motion at L4–L5 to292671%, which was significantly greater than all othergroups except the two-level Charite (p!.05). As expected,segmental motion at the inferior L5–S1 level was signifi-cantly greater after single-level (L4–L5) discectomy, Char-ite alone, and Charite combined with pedicle screws incomparison with the two-level Charite and FRA augmentedwith pedicle screws (p!.05). The most interesting findingunder this loading modality was that observed with theaddition of a second Charite implant at L5–S1. Rotationalmotion about L4–L5 and L5–S1 significantly increasedcompared with the intact condition, which was differentfrom all other treatments (p!.05). There were no differ-ences between the Charite augmented with pedicle screwsor pedicle screws with FRA (pO.05) (Fig. 4).
Flexion-extension (6X-axis)Under flexion-extension loading, the L3–L4 level dem-
onstrated no differences in segmental motion except forthe two-level FRA treatment combined with pediclescrews, which resulted in statistically greater motion thanthe intact, discectomy, single- or two-level Charite(p!.05). As expected, the discectomy condition at L4–L5 produced significantly more motion at this level versusall other treatments (p!.05). Moreover, the intact condi-tion, single-level Charite, two-level Charite, and Charitecombined with FRA and pedicle screws at L5–S1 ex-hibited significantly more motion than any of the single-or two-level pedicle screw reconstructions—Charite orFRA spacer (p!.05). Segmental motion at the inferiorL5–S1 level was significantly greater for the intact, dis-cectomy, Charite alone, Charite combined with pediclescrews, and two-level Charite versus all other treatments(p!.05). There were no differences between the Charite
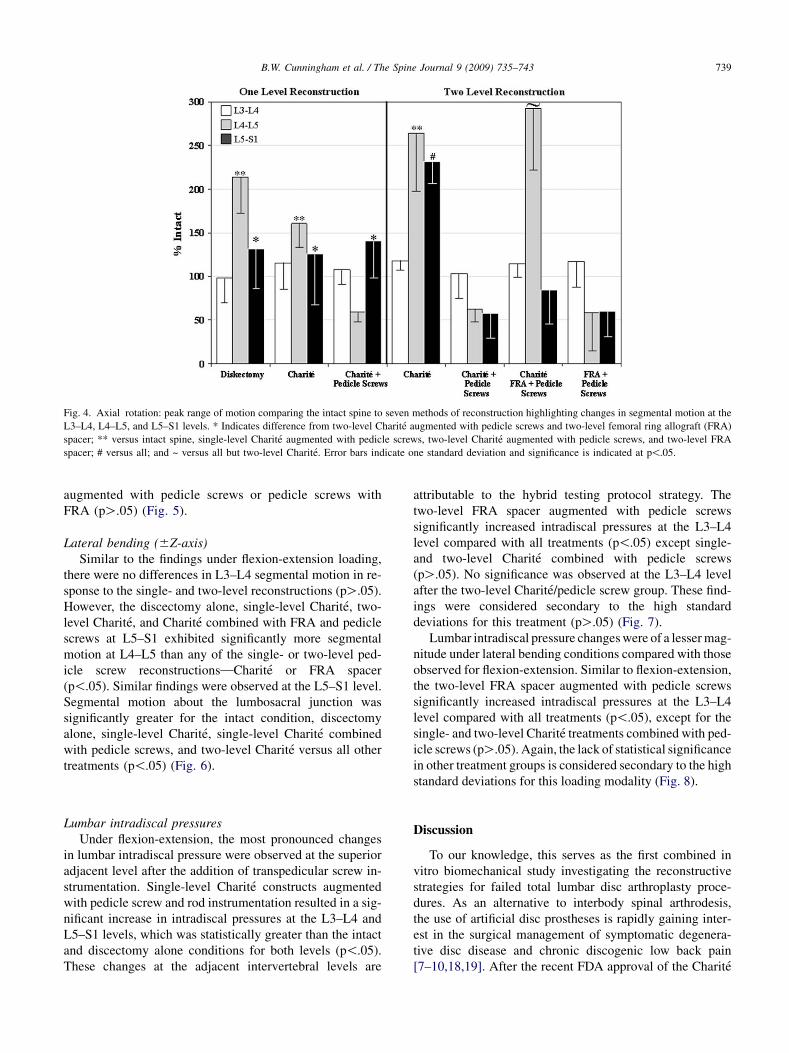
Fig. 4. Axial rotation: peak range of motion comparing the intact spine to seven methods of reconstruction highlighting changes in segmental motion at the
L3–L4, L4–L5, and L5–S1 levels. * Indicates difference from two-level Charite augmented with pedicle screws and two-level femoral ring allograft (FRA)
spacer; ** versus intact spine, single-level Charite augmented with pedicle screws, two-level Charite augmented with pedicle screws, and two-level FRA
spacer; # versus all; and ~ versus all but two-level Charite. Error bars indicate one standard deviation and significance is indicated at p!.05.
739B.W. Cunningham et al. / The Spine Journal 9 (2009) 735–743
augmented with pedicle screws or pedicle screws withFRA (pO.05) (Fig. 5).
Lateral bending (6Z-axis)Similar to the findings under flexion-extension loading,
there were no differences in L3–L4 segmental motion in re-sponse to the single- and two-level reconstructions (pO.05).However, the discectomy alone, single-level Charite, two-level Charite, and Charite combined with FRA and pediclescrews at L5–S1 exhibited significantly more segmentalmotion at L4–L5 than any of the single- or two-level ped-icle screw reconstructions—Charite or FRA spacer(p!.05). Similar findings were observed at the L5–S1 level.Segmental motion about the lumbosacral junction wassignificantly greater for the intact condition, discectomyalone, single-level Charite, single-level Charite combinedwith pedicle screws, and two-level Charite versus all othertreatments (p!.05) (Fig. 6).
Lumbar intradiscal pressuresUnder flexion-extension, the most pronounced changes
in lumbar intradiscal pressure were observed at the superioradjacent level after the addition of transpedicular screw in-strumentation. Single-level Charite constructs augmentedwith pedicle screw and rod instrumentation resulted in a sig-nificant increase in intradiscal pressures at the L3–L4 andL5–S1 levels, which was statistically greater than the intactand discectomy alone conditions for both levels (p!.05).These changes at the adjacent intervertebral levels are
attributable to the hybrid testing protocol strategy. Thetwo-level FRA spacer augmented with pedicle screwssignificantly increased intradiscal pressures at the L3–L4level compared with all treatments (p!.05) except single-and two-level Charite combined with pedicle screws(pO.05). No significance was observed at the L3–L4 levelafter the two-level Charite/pedicle screw group. These find-ings were considered secondary to the high standarddeviations for this treatment (pO.05) (Fig. 7).
Lumbar intradiscal pressure changes were of a lesser mag-nitude under lateral bending conditions compared with thoseobserved for flexion-extension. Similar to flexion-extension,the two-level FRA spacer augmented with pedicle screwssignificantly increased intradiscal pressures at the L3–L4level compared with all treatments (p!.05), except for thesingle- and two-level Charite treatments combined with ped-icle screws (pO.05). Again, the lack of statistical significancein other treatment groups is considered secondary to the highstandard deviations for this loading modality (Fig. 8).
Discussion
To our knowledge, this serves as the first combined invitro biomechanical study investigating the reconstructivestrategies for failed total lumbar disc arthroplasty proce-dures. As an alternative to interbody spinal arthrodesis,the use of artificial disc prostheses is rapidly gaining inter-est in the surgical management of symptomatic degenera-tive disc disease and chronic discogenic low back pain[7–10,18,19]. After the recent FDA approval of the Charite
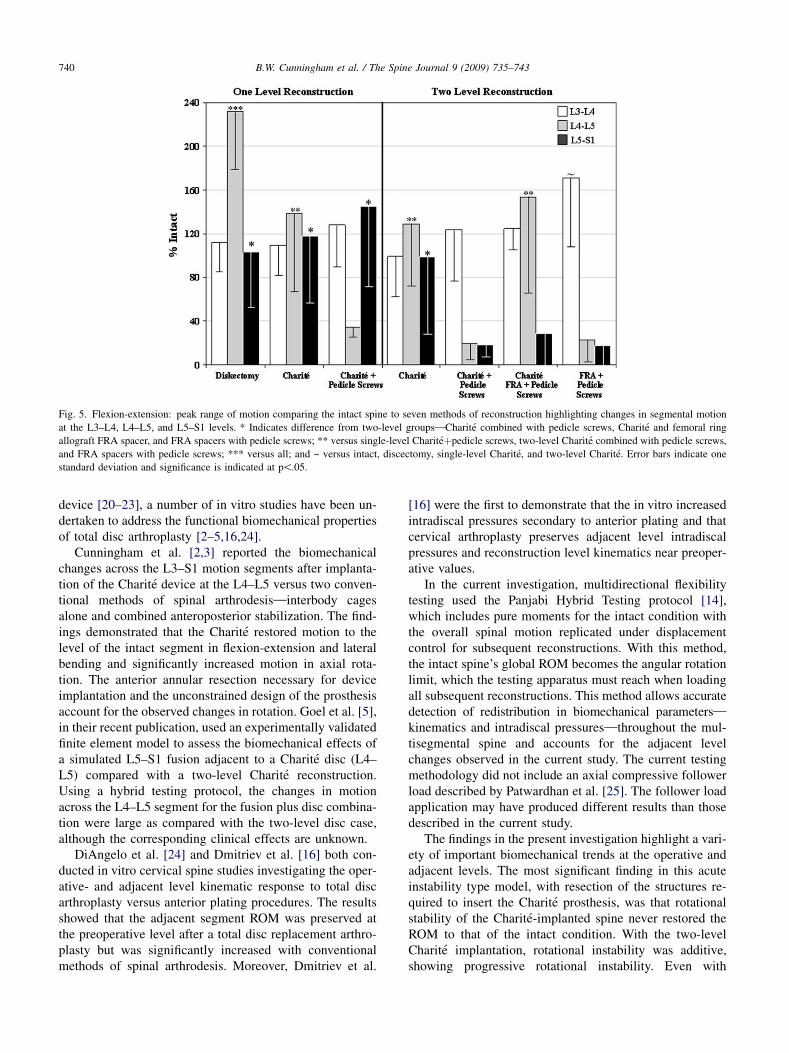
Fig. 5. Flexion-extension: peak range of motion comparing the intact spine to seven methods of reconstruction highlighting changes in segmental motion
at the L3–L4, L4–L5, and L5–S1 levels. * Indicates difference from two-level groups—Charite combined with pedicle screws, Charite and femoral ring
allograft FRA spacer, and FRA spacers with pedicle screws; ** versus single-level Chariteþpedicle screws, two-level Charite combined with pedicle screws,
and FRA spacers with pedicle screws; *** versus all; and ~ versus intact, discectomy, single-level Charite, and two-level Charite. Error bars indicate one
standard deviation and significance is indicated at p!.05.
740 B.W. Cunningham et al. / The Spine Journal 9 (2009) 735–743
device [20–23], a number of in vitro studies have been un-dertaken to address the functional biomechanical propertiesof total disc arthroplasty [2–5,16,24].
Cunningham et al. [2,3] reported the biomechanicalchanges across the L3–S1 motion segments after implanta-tion of the Charite device at the L4–L5 versus two conven-tional methods of spinal arthrodesis—interbody cagesalone and combined anteroposterior stabilization. The find-ings demonstrated that the Charite restored motion to thelevel of the intact segment in flexion-extension and lateralbending and significantly increased motion in axial rota-tion. The anterior annular resection necessary for deviceimplantation and the unconstrained design of the prosthesisaccount for the observed changes in rotation. Goel et al. [5],in their recent publication, used an experimentally validatedfinite element model to assess the biomechanical effects ofa simulated L5–S1 fusion adjacent to a Charite disc (L4–L5) compared with a two-level Charite reconstruction.Using a hybrid testing protocol, the changes in motionacross the L4–L5 segment for the fusion plus disc combina-tion were large as compared with the two-level disc case,although the corresponding clinical effects are unknown.
DiAngelo et al. [24] and Dmitriev et al. [16] both con-ducted in vitro cervical spine studies investigating the oper-ative- and adjacent level kinematic response to total discarthroplasty versus anterior plating procedures. The resultsshowed that the adjacent segment ROM was preserved atthe preoperative level after a total disc replacement arthro-plasty but was significantly increased with conventionalmethods of spinal arthrodesis. Moreover, Dmitriev et al.
[16] were the first to demonstrate that the in vitro increasedintradiscal pressures secondary to anterior plating and thatcervical arthroplasty preserves adjacent level intradiscalpressures and reconstruction level kinematics near preoper-ative values.
In the current investigation, multidirectional flexibilitytesting used the Panjabi Hybrid Testing protocol [14],which includes pure moments for the intact condition withthe overall spinal motion replicated under displacementcontrol for subsequent reconstructions. With this method,the intact spine’s global ROM becomes the angular rotationlimit, which the testing apparatus must reach when loadingall subsequent reconstructions. This method allows accuratedetection of redistribution in biomechanical parameters—
kinematics and intradiscal pressures—throughout the mul-tisegmental spine and accounts for the adjacent levelchanges observed in the current study. The current testingmethodology did not include an axial compressive followerload described by Patwardhan et al. [25]. The follower loadapplication may have produced different results than thosedescribed in the current study.
The findings in the present investigation highlight a vari-ety of important biomechanical trends at the operative andadjacent levels. The most significant finding in this acuteinstability type model, with resection of the structures re-quired to insert the Charite prosthesis, was that rotationalstability of the Charite-implanted spine never restored theROM to that of the intact condition. With the two-levelCharite implantation, rotational instability was additive,showing progressive rotational instability. Even with
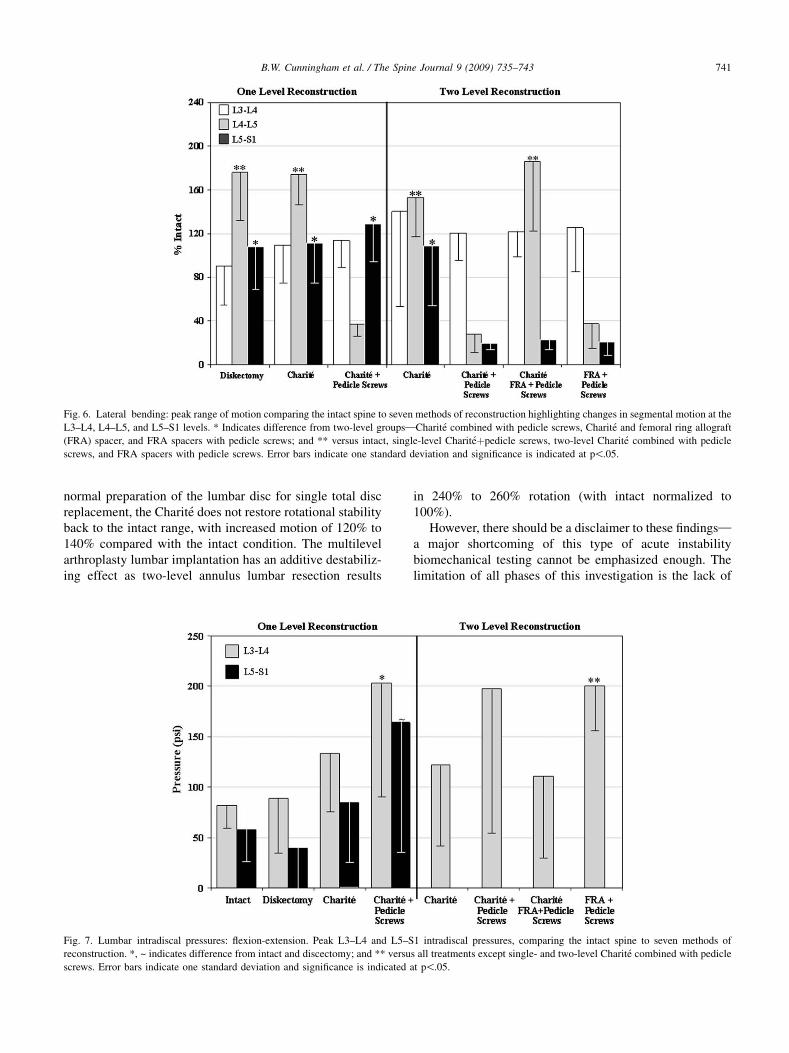
Fig. 6. Lateral bending: peak range of motion comparing the intact spine to seven methods of reconstruction highlighting changes in segmental motion at the
L3–L4, L4–L5, and L5–S1 levels. * Indicates difference from two-level groups—Charite combined with pedicle screws, Charite and femoral ring allograft
(FRA) spacer, and FRA spacers with pedicle screws; and ** versus intact, single-level Chariteþpedicle screws, two-level Charite combined with pedicle
screws, and FRA spacers with pedicle screws. Error bars indicate one standard deviation and significance is indicated at p!.05.
741B.W. Cunningham et al. / The Spine Journal 9 (2009) 735–743
normal preparation of the lumbar disc for single total discreplacement, the Charite does not restore rotational stabilityback to the intact range, with increased motion of 120% to140% compared with the intact condition. The multilevelarthroplasty lumbar implantation has an additive destabiliz-ing effect as two-level annulus lumbar resection results
Fig. 7. Lumbar intradiscal pressures: flexion-extension. Peak L3–L4 and L5–S
reconstruction. *, ~ indicates difference from intact and discectomy; and ** versu
screws. Error bars indicate one standard deviation and significance is indicated
in 240% to 260% rotation (with intact normalized to100%).
However, there should be a disclaimer to these findings—
a major shortcoming of this type of acute instabilitybiomechanical testing cannot be emphasized enough. Thelimitation of all phases of this investigation is the lack of
1 intradiscal pressures, comparing the intact spine to seven methods of
s all treatments except single- and two-level Charite combined with pedicle
at p!.05.
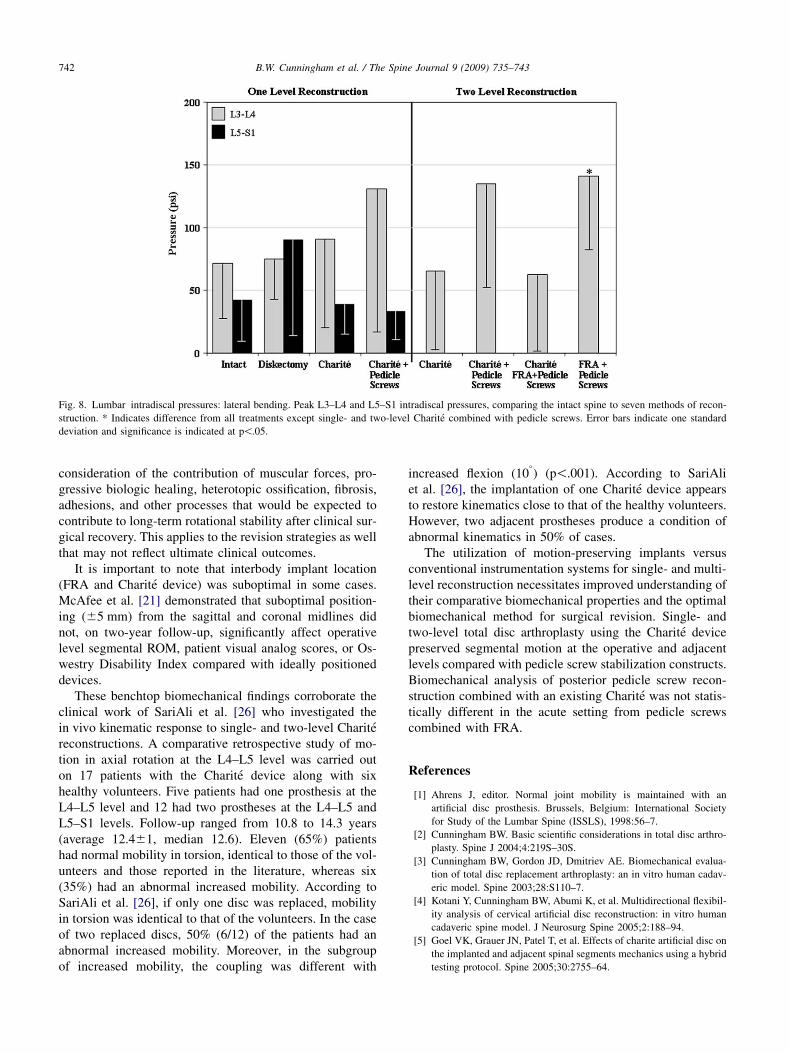
Fig. 8. Lumbar intradiscal pressures: lateral bending. Peak L3–L4 and L5–S1 intradiscal pressures, comparing the intact spine to seven methods of recon-
struction. * Indicates difference from all treatments except single- and two-level Charite combined with pedicle screws. Error bars indicate one standard
deviation and significance is indicated at p!.05.
742 B.W. Cunningham et al. / The Spine Journal 9 (2009) 735–743
consideration of the contribution of muscular forces, pro-gressive biologic healing, heterotopic ossification, fibrosis,adhesions, and other processes that would be expected tocontribute to long-term rotational stability after clinical sur-gical recovery. This applies to the revision strategies as wellthat may not reflect ultimate clinical outcomes.
It is important to note that interbody implant location(FRA and Charite device) was suboptimal in some cases.McAfee et al. [21] demonstrated that suboptimal position-ing (65 mm) from the sagittal and coronal midlines didnot, on two-year follow-up, significantly affect operativelevel segmental ROM, patient visual analog scores, or Os-westry Disability Index compared with ideally positioneddevices.
These benchtop biomechanical findings corroborate theclinical work of SariAli et al. [26] who investigated thein vivo kinematic response to single- and two-level Charitereconstructions. A comparative retrospective study of mo-tion in axial rotation at the L4–L5 level was carried outon 17 patients with the Charite device along with sixhealthy volunteers. Five patients had one prosthesis at theL4–L5 level and 12 had two prostheses at the L4–L5 andL5–S1 levels. Follow-up ranged from 10.8 to 14.3 years(average 12.461, median 12.6). Eleven (65%) patientshad normal mobility in torsion, identical to those of the vol-unteers and those reported in the literature, whereas six(35%) had an abnormal increased mobility. According toSariAli et al. [26], if only one disc was replaced, mobilityin torsion was identical to that of the volunteers. In the caseof two replaced discs, 50% (6/12) of the patients had anabnormal increased mobility. Moreover, in the subgroupof increased mobility, the coupling was different with
increased flexion (10�) (p!.001). According to SariAli
et al. [26], the implantation of one Charite device appearsto restore kinematics close to that of the healthy volunteers.However, two adjacent prostheses produce a condition ofabnormal kinematics in 50% of cases.
The utilization of motion-preserving implants versusconventional instrumentation systems for single- and multi-level reconstruction necessitates improved understanding oftheir comparative biomechanical properties and the optimalbiomechanical method for surgical revision. Single- andtwo-level total disc arthroplasty using the Charite devicepreserved segmental motion at the operative and adjacentlevels compared with pedicle screw stabilization constructs.Biomechanical analysis of posterior pedicle screw recon-struction combined with an existing Charite was not statis-tically different in the acute setting from pedicle screwscombined with FRA.
References
[1] Ahrens J, editor. Normal joint mobility is maintained with an
artificial disc prosthesis. Brussels, Belgium: International Society
for Study of the Lumbar Spine (ISSLS), 1998:56–7.
[2] Cunningham BW. Basic scientific considerations in total disc arthro-
plasty. Spine J 2004;4:219S–30S.
[3] Cunningham BW, Gordon JD, Dmitriev AE. Biomechanical evalua-
tion of total disc replacement arthroplasty: an in vitro human cadav-
eric model. Spine 2003;28:S110–7.
[4] Kotani Y, Cunningham BW, Abumi K, et al. Multidirectional flexibil-
ity analysis of cervical artificial disc reconstruction: in vitro human
cadaveric spine model. J Neurosurg Spine 2005;2:188–94.
[5] Goel VK, Grauer JN, Patel T, et al. Effects of charite artificial disc on
the implanted and adjacent spinal segments mechanics using a hybrid
testing protocol. Spine 2005;30:2755–64.
743B.W. Cunningham et al. / The Spine Journal 9 (2009) 735–743
[6] Crawford NR. Biomechanics of lumbar arthroplasty. Neurosurg Clin
N Am 2005;16:595–602.
[7] Lee CK, Goel VK. Artificial disc prosthesis: design concepts and
criteria. Spine J 2004;4:209S–18S.
[8] Lee CK, Langrana NA, Parsons JR, Zimmerman MC. Development
of a prosthetic intervertebral disc. Spine 1991;16:S253–5.
[9] Lemaire JP, Skalli W, Lavaste F, et al. Intervertebral disc prosthesis.
Results and prospects for the year 2000. Clin Orthop Relat Res
1997;337:64–76.
[10] Lemaire JP, Carrier H, Sariali el H, et al. Clinical and radiological
outcomes with the Charite artificial disc: a 10-year minimum fol-
low-up. J Spinal Disord Tech. 2005;18:353–9.
[11] Schlegel JD, Smith JA, Schleusener RL. Lumbar motion segment
pathology adjacent to thoracolumbar, lumbar, and lumbosacral
fusions. Spine 1996;21:970–81.
[12] Wigfield C, Gill S, Nelson R, et al. Influence of an artificial cervical
joint compared with fusion on adjacent-level motion in the treat-
ment of degenerative cervical disc disease. J Neurosurg 2002;96:
17–21.
[13] Zeegers WS, Bohnen LM, Laaper M, Verhaegen MJ. Artificial disc
replacement with the modular type SB Charite III: 2-year results in
50 prospectively studied patients. Eur Spine J 1999;8:210–7.
[14] Panjabi MM. Biomechanical testing to identify adjacent-level effects.
Calgary, Canada: World Congress of Biomechanics, 2002.
[15] Cripton PA, Dumas GA, Nolte LP. A minimally disruptive technique
for measuring intervertebral disc pressure in vitro: application to the
cervical spine. J Biomech 2001;34:545–9.
[16] Dmitriev AE, Cunningham BW, Hu N, et al. Adjacent level intradis-
cal pressure and segmental kinematics following a cervical total disc
arthroplasty: an in vitro human cadaveric model. Spine 2005;30:
1165–72.
[17] Panjabi MM. Biomechanical evaluation of spinal fixation devices:
I. A conceptual framework. Spine 1988;13:1129–34.
[18] Bao QB, McCullen GM, Higham PA, Dumbleton JH, Yuan HA. The
artificial disc: theory, design and materials. Biomaterials 1996;17:
1157–67.
[19] Griffith SL, Shelokov AP, Buttner-Janz K, et al. A multicenter retro-
spective study of the clinical results of the LINK SB Charite interver-
tebral prosthesis. The initial European experience. Spine 1994;19:
1842–9.
[20] Guyer RD, McAfee PC, Hochschuler SH, et al. Prospective random-
ized study of the Charite artificial disc: data from two investigational
centers. Spine J 2004;4:252S–9S.
[21] McAfee PC, Cunningham B, Holsapple G, et al. A prospective,
randomized, multicenter Food and Drug Administration investiga-
tional device exemption study of lumbar total disc replacement with
the CHARITE artificial disc versus lumbar fusion: part II: evaluation
of radiographic outcomes and correlation of surgical technique
accuracy with clinical outcomes. Spine 2005;30:1576–83; discussion
E1388–1590.
[22] McAfee PC, Fedder IL, Saiedy S, Shucosky EM, Cunningham BW.
SB Charite disc replacement: report of 60 prospective randomized
cases in a US center. J Spinal Disord Tech 2003;16:424–33.
[23] McAfee PC, Geisler FH, Saiedy SS, et al. Revisability of the CHARITE
artificial disc replacement: analysis of 688 patients enrolled in the U.S.
IDE study of the CHARITE Artificial Disc. Spine 2006;31:1217–26.
[24] DiAngelo DJ, Roberston JT, Metcalf NH, et al. Biomechanical
testing of an artificial cervical joint and an anterior cervical plate.
J Spinal Disord Tech 2003;16:314–23.
[25] Patwardhan AG, Havey RM, Meade KP, et al. A follower load
increases the load-carrying capacity of the lumbar spine in compres-
sion. Spine 1999;24:1003–9.
[26] SariAli el H, Lemaire JP, Pascal-Mousselard H, et al. In vivo study
of the kinematics in axial rotation of the lumbar spine after total
intervertebral disc replacement: long-term results: a 10–14 years
follow up evaluation. Eur Spine J 2006;15:1501–10.




![Biomechanical Evaluation of AxiaLIF as Supplemental Hardware … · treating degenerative disc disease, instability and adult degenerative scoliosis [2]. The AxiaLIF¨ hardware, consisting](https://img.pdfslide.us/doc/110x75/600570bcfdb4a53ba20badc5/biomechanical-evaluation-of-axialif-as-supplemental-hardware-treating-degenerative.jpg)









![NSI EDUCATIONAL COURSE TRAVELLING FELLOWSHIPS - NSI · Discussants : Ramakrishna E / R Satish Lumbar Disc Arthroplasty : Review - DV Rajakumar [ Banglore] Against Arthroplasty : K](https://img.pdfslide.us/doc/110x75/6009a5686314955a4c128dfb/nsi-educational-course-travelling-fellowships-nsi-discussants-ramakrishna-e.jpg)














