-
8/10/2019 Revised Gi 1 Esophagus
1/46
The GI System, Part 1:
The Esophagus
Mark Galan, MD
October 2, 2014
-
8/10/2019 Revised Gi 1 Esophagus
2/46
Esophageal Disorders
Congenital
Inflammatory (Esophagitis)
Vascular Neoplastic
But first.
-
8/10/2019 Revised Gi 1 Esophagus
3/46
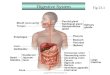
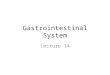
First Things FirstWhat Is Normal?
Epithelium (squamous)
Lamina propria
Muscularis mucosa
Submucosa
Muscularis propria(inner circumferential)
Muscularis propria
(outer longitudinal)
Layers of the esophagus: Mucosa, Submucosa, Muscularis
Propria
-
8/10/2019 Revised Gi 1 Esophagus
4/46
More Normal
The Squamous epithelium of the
esophagus gives way to the
glandular epithelium of the
stomach at the gastroesophageal
junction at the Z-line.
The GE junction is where a lot of
important pathology occurs
-
8/10/2019 Revised Gi 1 Esophagus
5/46
Tracheo-Esophageal Fistula
Most common congenital anomaly
Associated with esophageal atresia in
90% of cases (usually the middle 3rd)
Presents in neonatal period
Can lead to death due to aspiration
pneumonia To help understand the concept, a little
embryology is useful.
-
8/10/2019 Revised Gi 1 Esophagus
6/46
Development of the Foregut
-
8/10/2019 Revised Gi 1 Esophagus
7/46
-
8/10/2019 Revised Gi 1 Esophagus
8/46
Hernias
Two major types:
Hiatal (sliding). The
entire proximal
stomach protrudes intothe mediastinum
Paraesophageal
(rolling). Only part of
the fundus protrudes
into the mediastinum
-
8/10/2019 Revised Gi 1 Esophagus
9/46
Esophagitis
Reflux: most important cause: distal 1/3
Certain foods or drugs (NSAIDs, Fe)
Hypersensitivity reaction
N/G tubes Infections: e.g. Herpes, Candida, CMV (in
immunosuppressed individuals)
Caustic bases (NaOH) or acids
Complications: Erosions, ulcers, perforation,Barretts metaplasia
(reflux), strictures (lye)
-
8/10/2019 Revised Gi 1 Esophagus
10/46
-
8/10/2019 Revised Gi 1 Esophagus
11/46
Reflux Esophagitis
Most common cause of esophagitis
Passage of gastric/duodenal contents
back up through the lower esophageal
sphincter
Incidence in the US is ~30-40%
More common in adults >40; also commonin babies
-
8/10/2019 Revised Gi 1 Esophagus
12/46
Classic elements of
reflux esophagitis:
Elongation of rete
Basal cell
hyperplasia
Intraepithelialeosinophils (which
are also seen in
hypersensitivity
esophagitis)
-
8/10/2019 Revised Gi 1 Esophagus
13/46
Endoscopically, an esophagus with
eosinophilic esophagitis is described as
feline esophagusalso known astrachealization. Compare to normal
(right)
-
8/10/2019 Revised Gi 1 Esophagus
14/46
Now Lets Take a Brief Detour to Talk about
What Can Happen As A Result of Reflux
Esophagitis
Repeated injury to the esophagus will cause the
glandular-type epithelium of the stomach to
move into the esophagus.
This glandular epithelium can then become
intestinalizeda condition known as Barretts
Esophagus
Barretts Esophagus is the background fromwhich esophageal
adenocarcinoma can arise
(more about that shortly.)
-
8/10/2019 Revised Gi 1 Esophagus
15/46
Review: Normal gastroesophageal junction (Z-line)
-
8/10/2019 Revised Gi 1 Esophagus
16/46
On the left is normal esophagus, with the Z-line right where it
is
supposed to be. But in Barretts esophagus, the glandular
epitheliummoves up into the esophagus
-
8/10/2019 Revised Gi 1 Esophagus
17/46
Barretts EsophagusGross Pathology
Barrettsred,
velvety, salmon-
colored mucosa
Normal esophaguspale
pink mucosa (normal
squamous)
-
8/10/2019 Revised Gi 1 Esophagus
18/46
In addition to the glandular, gastric-type epithelium
moving upward, Barretts esophagus is
characterized by intestinalization of the glandular
epithelium (goblet cells)
OK, now back to the discussion of esophagitis.
-
8/10/2019 Revised Gi 1 Esophagus
19/46
Candida
Most common cause of infectious esophagitis
Usually C. albicans or C. tropicalis
Associations/risk factors:
Immunosuppression
HIV, BMT, immunosuppressive tx, bone marrow disorders
Acid-suppression tx
Diabetes
Esophageal motility disorders
Rheumatic diseases
Presentation:
Dysphagia
Treatment:
Antifungals (like fluconazole)
The characteristic white
-
8/10/2019 Revised Gi 1 Esophagus
20/46
The characteristic white
plaques of candidal
esophagitis, seen on
endoscopy
NASPGHN
-
8/10/2019 Revised Gi 1 Esophagus
21/46
PAS stain
-
8/10/2019 Revised Gi 1 Esophagus
22/46
Herpes Simplex Virus (HSV)
2ndmost common cause of
infectious esophagitis after
Candida
Usually affects
immunosuppressed people, but
can also be a problem withimmunocompetent children
You may also see superinfection
with bacteria and fungi
Causes esophageal ulcers, which
can turn into perforations; the
infection can also become
disseminated
Treat with antivirals (like acyclovir)
-
8/10/2019 Revised Gi 1 Esophagus
23/46
An HSV ulcer. Note the large cells.
-
8/10/2019 Revised Gi 1 Esophagus
24/46
HSV esophagitis. Note the Multinucleation, Margination, and
Molding
Dr. D. Wiedbrauk, Warde Medical Laboratory
-
8/10/2019 Revised Gi 1 Esophagus
25/46
Cytomegalovirus (CMV)
Infection Virtually always in
immunocompromised patients
Up to ~30% of HIV patients
not on HAART have CMV,
HSV, or Candida
esophagitis
Can cause ulcers that grossly
resemble HSV ulcers
Therapy:
Antivirals
Modulation of immunosuppression
Treat the underlying cause (as
with HAART in HIV patients)
Indian J Pathol Microbiol 2011;54:852-3
-
8/10/2019 Revised Gi 1 Esophagus
26/46
-
8/10/2019 Revised Gi 1 Esophagus
27/46
Mallory-Weiss Syndrome
Longitudinal tears in the lower esophagus,
possibly extending into the upper stomach
hematemesis
Complication of violent vomiting
Most commonly seen in alcoholics
Tears are usually superficial and do notlead to perforation
A transmural perforation due to violent
vomiting is known as Boerhaave Syndrome
-
8/10/2019 Revised Gi 1 Esophagus
28/46
Mallory-Weiss tear
-
8/10/2019 Revised Gi 1 Esophagus
29/46
Esophageal Varices
Complication of portal hypertension, occurs in90% of cirrhotic
patients
Results from an increase in pressure in theportal vein, which
shunts blood into associatedveinswhich are not built to withstand
theincreased pressure.
Alcohol is #1 cause
Can result in massive hematemesisand deathifnot treated
immediately (#1 cause of death incirrhotics)
Anatomy of the portal venous
-
8/10/2019 Revised Gi 1 Esophagus
30/46
Anatomy of the portal venous
system, which shows how
esophageal varices can form. A
major player in this process is the
left gastric vein, aka the cardiac
vein.
-
8/10/2019 Revised Gi 1 Esophagus
31/46
Esophageal varix
-
8/10/2019 Revised Gi 1 Esophagus
32/46
Esophageal Carcinoma
Two Main Types:
Squamous cell carcinoma
Adenocarcinoma
The interesting epidemiologic differences worldwide
between the two:
While SCC accounts for about 90% of esophageal cancers
worldwide, here in America the incidences of SCC and
adenocarcinoma are roughly comparable. Environmental and genetic
factors are believed to be the
reasons
-
8/10/2019 Revised Gi 1 Esophagus
33/46
Squamous Cell Carcinoma of the
Esophagus
Obligatory epidemiology slide
M>F (About 4:1)
In America, the main causes are EtOH and tobacco(which work
synergistically)
Other factors Environmental
Food
HPV
Corrosives and thermal injury
RTX for other mediastinal tumors
Celiac disease
-
8/10/2019 Revised Gi 1 Esophagus
34/46
High-grade dysplasia
-
8/10/2019 Revised Gi 1 Esophagus
35/46
High grade dysplasia,
or carcinoma in-situ
(CIS)
Compare the CIS to
normal squamous
epithelium
-
8/10/2019 Revised Gi 1 Esophagus
36/46
-
8/10/2019 Revised Gi 1 Esophagus
37/46
Another image of squamous cell carcinoma that has invaded
Gross photograph of
-
8/10/2019 Revised Gi 1 Esophagus
38/46
p g p
squamous cell
carcinoma, showing an
ulcerated plaque
-
8/10/2019 Revised Gi 1 Esophagus
39/46
-
8/10/2019 Revised Gi 1 Esophagus
40/46
-
8/10/2019 Revised Gi 1 Esophagus
41/46
The Road to Adenocarcinoma
Over time, repeated injury to an esophagus
that has already undergone intestinal
metaplasia (Barretts) will generate mutations
that will lead to dysplasia (carcinoma in-situ),and eventually
carcinoma in-situ.
-
8/10/2019 Revised Gi 1 Esophagus
42/46
The Road to Adenocarcinoma
High-grade glandular
-
8/10/2019 Revised Gi 1 Esophagus
43/46
dysplasia, compared
to a simple case of
Barretts esophagus.
S13-796
-
8/10/2019 Revised Gi 1 Esophagus
44/46
Esophageal Adenocarcinoma
Eventually, the dysplastic cells will start to
invade and become invasive adenocarcinoma
Invasive
-
8/10/2019 Revised Gi 1 Esophagus
45/46
adenocarcinoma of
the esophagus
-
8/10/2019 Revised Gi 1 Esophagus
46/46
Another example of invasive adenocarcinoma arising in a
background of
Barretts