Embed Size (px)
DESCRIPTION
Electrical Impedance Tomography
Citation preview

C
Electrical impedance tomograph
yEduardo L.V. Costaa, Raul Gonzalez Limab and Marcelo B.P. AmatoaaRespiratory Intensive Care Unit, University of SaoPaulo School of Medicine and bDepartment ofMechanical Engineering, Escola Politecnica, Universityof Sao Paulo, Sao Paulo, Brazil
Correspondence to Marcelo B.P. Amato, MD, PhD,Respiratory Intensive Care Unit, University of SaoPaulo School of Medicine, Av Dr Arnaldo 455, Room2206 (2nd floor), 01246-903 Sao Paulo, BrazilTel: +55 11 3061 7361; fax: +55 11 3061 2492;e-mail: [email protected]
Current Opinion in Critical Care 2009,15:18–24
Purpose of review
Electrical impedance tomography (EIT) is a noninvasive, radiation-free monitoring tool
that allows real-time imaging of ventilation. The purpose of this article is to discuss the
fundamentals of EIT and to review the use of EIT in critical care patients.
Recent findings
In addition to its established role in describing the distribution of alveolar ventilation, EIT
has been shown to be a useful tool to detect lung collapse and monitor lung recruitment,
both regionally and on a global basis. EIT has also been used to diagnose with high
sensitivity incident pneumothoraces during mechanical ventilation. Additionally, with
injection of hypertonic saline as a contrast agent, it is possible to estimate ventilation/
perfusion distributions.
Summary
EIT is cheap, noninvasive and allows continuous monitoring of ventilation. It is gaining
acceptance as a valuable monitoring tool for the care of critical patients.
Keywords
electrical impedance tomography, imaging, lungs, monitoring
Curr Opin Crit Care 15:18–24� 2009 Wolters Kluwer Health | Lippincott Williams & Wilkins1070-5295
IntroductionElectrical impedance tomography (EIT) is a noninvasive,
radiation-free monitoring tool that allows real-time ima-
ging of ventilation [1–3]. EIT is the only bedside method
that allows repeated, noninvasive measurements of
regional changes in lung volumes [4,5]. For this reason,
EIT has been used as a monitoring tool in a variety of
applications in critical care medicine, including monitor-
ing of ventilation distribution [3,6], assessment of lung
hyperdistension [7] and collapse [8�,9�], detection of
pneumothorax [10�,11], among others. In this article,
we will discuss the fundamentals of EIT and review
the use of EIT in critical care patients in the light of
recent literature.
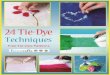
How electrical impedance tomography worksEIT uses injection of high frequency and low amplitude
electrical currents, typically through 16 or 32 electrodes
around the thorax, to obtain images of a cross section of
the lungs (Fig. 1) [1,10�]. These currents travel through
the thorax following pathways that vary according to
chest wall shape and thoracic distribution of impedi-
tivities. The resulting electric potentials on the surface
of the chest wall are measured and used to obtain the
electric impedance distribution within the thorax using a
reconstruction algorithm that solves an ill-posed non-
linear problem. Ill-posedness means that the solution
opyright © Lippincott Williams & Wilkins. Unautho
1070-5295 � 2009 Wolters Kluwer Health | Lippincott Williams & Wilkins
for intrathoracic impedances may not be unique or
may be unstable: small errors in voltage measurements
may lead to fairly different solutions. This problem is
aggravated by the small number of measurements made
at the body surface, because of the present technological
limitation on minimum electrode size (and thus maximal
electrode number). In order to overcome the ill-posed
nature of impedance estimation, most EIT imaging
algorithms make use of additional assumptions, known
as regularizations, such as smoothness of the intrathoracic
impedance distribution [12,13]. These regularizations
help the estimation algorithm to decide between com-
peting solutions, producing an image that is a reasonable
estimation of the true impedance distribution within the
thorax, at the expense of degraded spatial resolution or
attenuation of maximum perturbations.
Absolute versus difference imagesThoracic shape can contribute as much as internal thor-
acic impedances to the measured voltages at the chest
wall surface [13]. Consequently, the reconstruction of the
absolute impedance distribution, albeit feasible, requires
knowledge of the shape of the thorax. Difference images,
described by Brown [13], can be generated without
precise knowledge of the thoracic geometry. Their recon-
struction is based on relative changes in impedance in
relation to a reference, assuming that the shape of the
thorax is nearly rounded and did not change in between.
rized reproduction of this article is prohibited.
DOI:10.1097/MCC.0b013e3283220e8c

C
Electrical impedance tomography Costa et al. 19
Figure 1 Disposition of electrodes around the thorax and elec-
trical current injection
Computerized tomography (CT) of the thorax of a patient with schema-tically drawn electrodes and electrical current pathways through thethorax. One pair of electrodes injects electrical current at a time whereasthe remaining electrodes read the voltages produced as a result ofelectrical current passing through the thorax. The injecting pair isalternated sequentially so that after a full cycle, all possible adjacentelectrodes serve as injectors. Each full cycle results in an image and 50images are produced each second.
This relative or differential approach cancels out most
errors related to wrong assumptions about the true thor-
acic shape (the same error is equally present in both
images) and has proven its validity in the last years.
The use of normalized voltage measurements further
improves the robustness of such solution, which ignores
the absolute values of impedance at the beginning of the
measurements. Typically, at a frequency of 10 kHz, the
electrical impedance of the chest tissues is in the order of
2–4 Vm, and the average impedance of the lung is around
10 Vm [14]. During respiration, whereas lung impedance
changes up to 300% (from 7.2 to 23.6 Vm in one report)
[14], chest wall impedance remains relatively constant.
Most currently available EIT devices in clinical practice
and most publications in the field use the relative
approach and thus calculate difference impedance
images in relation to a reference. The output image of
such algorithms is usually a 32� 32 or a 64� 64 array
(which might be later interpolated) from which each
element corresponds to a pixel on the image and contains
the change in impedance in relation to a reference frame,
expressed as a percentage. The baseline impedance
cannot be recovered. Thus, breaths producing a change
in lung impedance from 5 to 10 Vm, or from 10 to 20 Vm
will produce exactly the same relative image. As we will
see later, this limitation is not worrisome as far as clinical
applications are concerned, because there is a well
described and linear relationship between the amount
opyright © Lippincott Williams & Wilkins. Unauth
of air entering the voxel and the percentage change in
lung impedance [15,16].
One drawback of the use of difference images is that only
regions of the thorax that change their impedance over
time are represented in EIT images. Consequently,
preexisting consolidated areas of the lung (e.g., pneumo-
nia or atelectasis), pleural effusions or large bullae are not
represented in difference EIT images. For this reason,
absolute images have the potential to bring additional
and important information and there is continuing
research to improve the quality of absolute images.
Although some progress has been made, with promising
results presented by Hahn et al. [11], the quality of the
images is still not good enough for meaningful clinical
use. Further development in this area, using estimations
of electrode position and taking thoracic shape into
account will enable precise absolute image reconstruc-
tion.
Spatial and temporal resolutionSpatial resolution of EIT depends on the accuracy and
noise of the measurements, the number of electrodes,
and the regularization used. For this reason, spatial resol-
ution varies from one EIT device to another, and even
within a single device depending on the settings
employed. In bench tests, the resolution is usually
optimized because less regularization is required. At
the bedside, however, noise and wrong assumptions
about thoracic shape require stronger regularizations
and resolution is compromised. On average, in 16-elec-
trode systems, resolution is 12% of the thoracic diameter
for regions in the periphery of the lung and 20% for
central regions. In 32-electrode systems, this resolution
can be improved to 6–10% of the thoracic diameter
(Turri F, personal communication). In a typical adult
patient, this resolution corresponds to approximately
1.5–3 cm in the cross-sectional plane. The spatial resol-
ution in the craniocaudal direction is lower, the slice
thickness amounting to approximately 7–10 cm. Such
thick slices can be useful for studying the lung behavior
during mechanical ventilation, when the detection of
heterogeneities along the gravity axis is the main target
[17,18].
Although it is possible to improve spatial resolution, for
example, by increasing the number of electrodes or by
improving hardware performance, it is unlikely that EIT
will ever reach the resolution of CT or MRI [19]. On the
contrary, modern EIT devices are characterized by high
temporal resolution, with some generating 50 images/s. It
is thus possible to follow closely the time pattern of
regional inflation and deflation of the lung. For example,
it is possible to show that some areas start to inflate after
others, reflecting either tidal recruitment [20�] or local
orized reproduction of this article is prohibited.

C
20 Respiratory system
auto-PEEP. Additionally, by use of brief periods of apnea
or by filtering out ventilation [21�], high temporal resol-
ution allows for monitoring of changes in intrathoracic
impedance caused by perfusion.
Clinical applicationsInitial EIT applications on critical care medicine focused
mainly on ventilation and its distribution; now other
applications are being studied such as detection of pneu-
mothorax, assessment of lung recruitment and collapse,
and lung perfusion.
Assessment of lung recruitment and lung collapse
Careful titration of PEEP is of utmost importance for the
success of ventilatory strategies based on the open lung
approach. Global lung parameters, such as pressure-
volume curves [22,23] or respiratory system compliance
[24] fail to represent what is happening to the lung on a
regional basis [25]. Collapsed and overdistended lung
compartments commonly coexist, and a method capable
of assessing both, simultaneously, would be invaluable as
a tool to titrate PEEP. Our group described an EIT-based
method for estimating alveolar collapse at the bedside,
pointing out its regional distribution. On an experimental
model in pigs, we found a good correlation between EIT
and CT estimates of lung collapse during decremental
opyright © Lippincott Williams & Wilkins. Unautho
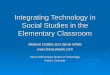
Figure 2 Estimation of collapse and overdistension
Computerized tomography (CT) of the thorax of a patient with right inferiohyperdistension (left) and lung collapse (right) in a patient with ARDS. The lright, at a PEEP of 3 cmH2O. In these images, CT slice thickness was 1 cm
PEEP trials after a maximal lung recruitment maneuver
[26]. Combining data obtained from EIT and respiratory
mechanics, it is also possible to estimate the amount of
overdistension during a PEEP trial, although validation
of such estimates represents a challenge due to the lack of
a gold standard to compare with (Fig. 2) [27]. Meier et al.[9�] recently used EIT to monitor regional tidal volume
during a PEEP titration maneuver in a model of surfac-
tant depletion in pigs. Looking at changes in regional
tidal volumes that occurred with changes in PEEP, they
were able to detect the initiation of regional lung collapse
and of regional lung recruitment before global changes
occurred in lung mechanics. Additionally, they showed
good correlation of ventilation estimated by EIT and CT,
confirming the results of Victorino et al. [3]. Together,
these results bring an exciting possibility of bedside
titration of PEEP based on regional lung mechanics.
In a similar report, Luepschen et al. [28�] showed that the
center of gravity of ventilation images moves dorsally
during lung recruitment and ventrally during lung col-
lapse. This EIT-based parameter brought additional
information to a fuzzy controller of ventilation that opti-
mized lung recruitment based on oxygenation, venti-
latory parameters and hemodynamics. Other authors also
used the center of gravity of ventilation to assess lung
recruitment [29]. In 16 newborn piglets with acute lung
rized reproduction of this article is prohibited.
r lobe pneumonia (top figures) and EIT maps (bottom figures) of lungeft-hand images were obtained at PEEP of 23 cmH2O and those on the
, and EIT slice thickness was approximately 7 cm.

C
Electrical impedance tomography Costa et al. 21
injury induced by whole lung lavage, Frerichs et al.showed that EIT allows visualization of the effects of
acute lung injury, lung recruitment, surfactant adminis-
tration, and mechanical ventilation strategy. They found
that lung injury displaces the ventilation ventrally, and
lung recruitment restores the center of ventilation to the
normal position. After surfactant administration, venti-
lation shifts ventrally over 10–60 min, but remains in the
preinjury position if surfactant administration is followed
by a recruitment maneuver.
Other methods to estimate lung recruitment using EIT
have been proposed. In a recent report [20�], the authors
compared EIT measures to dynamic CT in 18 pigs
divided into three groups (control, direct, and indirect
lung injury). EIT allowed real-time monitoring of
regional ventilation distribution. During an interposed
slow inflation, regional recruitment was detected by using
the time delay between start of inspiration and start of
regional inflation (ventilation delay index). Hinz et al.[30�] monitored 20 mechanically ventilated patients
during with acute lung injury/acute respiratory distress
syndrome (ARDS) during tidal breathing and showed
that the behavior of regional impedance over time was
heterogeneous and significantly different from that of the
whole lung. The findings suggested the occurrence of
hyperdistension and tidal recruitment in different regions
of the lung (Fig. 2).
Although a careful titration of PEEP is important, lung
conditions frequently change, and a selected PEEP
might not suffice to keep the lung open at all times,
especially if transient depressurization of the lung occurs.
Depressurization is particularly common when suction-
ing of the airways is required for clearance of secretions.
To assess the derecruitment caused by closed-system
suctioning, Wolf et al. [31�] studied six children with
ARDS, on pressure controlled ventilation and continu-
ously monitored with EIT. They showed that lung
volumes decreased on average by 5.3 ml/kg after three
suctioning maneuvers. Unexpectedly, they showed that
the most dorsal regions of the lung were the least affected
by derecruitment; as the authors used difference EIT
images, they could only speculate that this region was
atelectatic even before the suctioning maneuver. Another
possibility might be suggested in this context, which is
the presence of air trapping in dependent lung regions. In
pigs monitored with EIT after surfactant depletion,
Lindgren et al. [8�] found different results. They showed
that endotracheal suctioning induced collapse of the lung
and decreased regional lung compliance during open-
system suctioning but not during closed-system suction-
ing. The collapse was predominantly in the dorsal
regions, but recruitment was reestablished in less than
10 min by simple reconnection to the ventilator. Never-
theless, it is important to bear in mind that the model of
opyright © Lippincott Williams & Wilkins. Unauth
surfactant depletion using whole lung lavage leads to
lungs prone to collapse, but highly recruitable. There-
fore, these results need careful scrutiny before being
extrapolated to inflamed, edematous lungs of ARDS
patients, on whom depressurization can cause long-term
effects and should be avoided.
On a different report, the same authors used EIT to
assess lung collapse during bronchoscopic suctioning
in patients mechanically ventilated with acute lung
injury [32�]. They elegantly showed that bronchoscopy
initially leads to localized auto-PEEP due to the reduced
transverse area available for airflow, and that suctioning
leads to a decrease in lung aeration and compliance even
when a closed suctioning system is used. They obtained
similar findings both in volume-controlled and pressure-
controlled ventilation. In mechanically ventilated
patients being submitted to bronchoscopic procedures,
EIT might prove to be a useful tool to quantify the
amount of collapse and guide postsuctioning recruit-
ment.
Detection of pneumothorax and pleural effusion
Pneumothorax is a relatively common complication in
critical care patients under mechanical ventilation or
submitted to invasive procedures such as central venous
line placement or thoracocentesis. Costa et al. [10�]
created an algorithm for the detection of pneumotho-
races using EIT. The algorithm was created in a first
set of 10 pigs, and subsequently tested in 29 pigs. EIT
showed a sensitivity of 100% (CI 93–100%) to detect
pneumothoraces as small as 20 ml (Fig. 3). The major
limitation of this study was the need for a baseline
measurement before the occurrence of the pneumo-
thorax, limiting the application to monitoring of situa-
tions with high risk of developing pneumothorax, such
as central venous line placements or mechanical ventila-
tion with high alveolar pressures.
Another group of investigators [11] studied the combined
use of dynamic and absolute images for the diagnosis of
pneumothorax and pleural effusion. They studied five
pigs and showed reproducible results with the develop-
ment of pneumothorax consisting of regional increase in
absolute impedance and decreased ventilation. Pleural
effusions, being more conductive than the lung, pro-
duced a regional decrease in impedance associated with
decreased ventilation. They further acquired images in
four patients and showed that EIT absolute images were
compatible with CT images.
The use of EIT as a sensitive monitoring tool for the
detection of pneumothorax and pleural effusions
[10�,11,33] is appealing but probably will not be applied
in clinical practice until systematic studies in patients
are performed.
orized reproduction of this article is prohibited.

C
22 Respiratory system
Figure 3 Detection of pneumothorax
Computerized tomography (CT), ventilationmap, and aeration change map obtained atbaseline and after the induction of a 100 mlpneumothorax in a pig with partial atelectasisof the lungs.
Correct placement of endotracheal tube
Steinmann et al. [34�] studied 40 patients requiring one-
lung ventilation for surgical procedures. EIT monitoring
started before intubation and continued throughout the
protocol. All clinical decisions were based on fiberoptic
bronchoscopy and EIT investigators were blinded to
bronchoscopy findings. EIT correctly identified left
and right one-lung ventilation, but could not identify
misplacement of the endobronchial cuff, suggesting that
EIT cannot fully replace bronchoscopy as a guide to one-
lung ventilation. Although not designed to address this
question, this study suggests that EIT can be used to
diagnose selective intubation or endotracheal tube dis-
placement during conventional two-lung ventilation.
Perfusion and ventilation/perfusion ratios
The relationship between ventilation and perfusion
(VA/Q) is important in the pathophysiology of a number
of clinical conditions, such as pulmonary thromboembol-
ism, advanced chronic obstructive pulmonary disease and
ARDS. Additionally, in the ICU, VA/Q relationships
can change quite fast following changes that occur in
cardiac output and alveolar ventilation [35�]. Better
understanding of the VA/Q relationships could potentially
help guide treatment decisions and optimize gas
exchange. It is possible to use EIT to study lung per-
fusion through intravenous injection of hypertonic saline,
which serves as a contrast agent for EIT images (because
of its extremely low impeditivity), together with a breath
opyright © Lippincott Williams & Wilkins. Unautho
hold maneuver [36�,37]. Using this technique, we con-
ducted a study (Borges JB, unpublished data) to compute
regional VA/Q ratios in a pig model of ARDS and com-
pared them to VA/Q ratios computed with single photon
emission tomography. Ventilation was calculated using
the concept of functional images, as previously described
[2]. Regional perfusion estimations were based on the
time-signal intensity curve (or first-pass contrast curve)
observed in each pixel after the bolus of hypertonic
saline. A gamma curve, which models the indicator
washin, was fitted to sequential impedance measure-
ments of each pixel during the passage of the ‘contrast’.
We found that it is possible to derive meaningful VA/Q
maps from EIT data (Fig. 4) (Borges JB, unpublished
data).
Recently Deibele et al. [21�] used a combination of
techniques including signal filtering and principal com-
ponents analysis to separate the respiratory from the
cardiac signal in real time without the need for breath
holding. The authors were able to decompose the EIT
signal and to produce images from the cardiac oscillations.
This technique has the advantage over the hypertonic
saline technique in that it allows continuous monitoring
of cardiac-related oscillations. The amplitude of cardiac
related oscillations seen in the EIT signals, however, has
not been shown to correspond to the amount of local
perfusion, and further studies are necessary to explore its
precise physiological meaning [38].
rized reproduction of this article is prohibited.

C
Electrical impedance tomography Costa et al. 23
Figure 4 Ventilation/perfusion maps
Computed tomography, ventilation/perfusion (VA/Q) map and distribution of ventilation and blood flow derived from electrical impedance tomographydata. On the color scale for the VA/Q maps, red indicates shunt, green indicates VA/Q¼1, and white indicates dead space ventilation. Shunt is shownby the closed circle at VA/Q¼0. Panels a, b and c are from a mechanically ventilated pig with normal lungs and panels d, e and f are from the sameanimal after induction of atelectasis of the left lung. CT, computed tomography. Adapted with permission from (Borges JB, unpublished data).
ConclusionEIT is gradually gaining acceptance as a valuable
monitoring tool for the care of critical patients. It is cheap,
noninvasive and, up to now, has been shown to reliably
track changes in regional ventilation, describe regional
ventilation distribution and regional lung mechanics,
detect pneumothoraces, and monitor lung recruitment
and derecruitment. Other applications such as monitoring
of lung perfusion and of ventilation/perfusion distri-
bution are feasible but still require further studies.
AcknowledgementsFinancial support by grants from ‘Fundacao de Amparo a Pesquisa doEstado de Sao Paulo (FAPESP)’ – Sao Paulo State Research SupportFoundation and ‘Financiadora de Estudos e Projetos (FINEP)’ –Studies and Projects Financial Support Provider.
References and recommended readingPapers of particular interest, published within the annual period of review, havebeen highlighted as:� of special interest�� of outstanding interest
Additional references related to this topic can also be found in the CurrentWorld Literature section in this issue (p. 71).
1 Barber DC, Brown BH. Applied potential tomography. Journal of Physics E:Scientific Instruments 1984; 17:723–733.
2 Frerichs I, Hahn G, Schiffmann H, et al. Monitoring regional lung ventilation byfunctional electrical impedance tomography during assisted ventilation. Ann NY Acad Sci 1999; 873:493–505.
3 Victorino JA, Borges JB, Okamoto VN, et al. Imbalances in regional lungventilation: a validation study on electrical impedance tomography. Am JRespir Crit Care Med 2004; 169:791–800.
opyright © Lippincott Williams & Wilkins. Unauth
4 Frerichs I, Hinz J, Herrmann P, et al. Detection of local lung air content byelectrical impedance tomography compared with electron beam CT. J ApplPhysiol 2002; 93:660–666.
5 Wolf GK, Arnold JH. Noninvasive assessment of lung volume: respiratoryinductance plethysmography and electrical impedance tomography. Crit CareMed 2005; 33:S163–S169.
6 Frerichs I, Dargaville PA, Dudykevych T, Rimensberger PC. Electrical im-pedance tomography: a method for monitoring regional lung aeration and tidalvolume distribution? Intensive Care Med 2003; 29:2312–2316.
7 Adler A, Shinozuka N, Berthiaume Y, et al. Electrical impedance tomographycan monitor dynamic hyperinflation in dogs. J Appl Physiol 1998; 84:726–732.
8
�Lindgren S, Odenstedt H, Olegard C, et al. Regional lung derecruitment afterendotracheal suction during volume- or pressure-controlled ventilation: astudy using electric impedance tomography. Intensive Care Med 2007;33:172–180.
This study demonstrates that lung derecruitment occurs after open-system en-dotracheal suctioning.
9
�Meier T, Luepschen H, Karsten J, et al. Assessment of regional lung recruit-ment and derecruitment during a PEEP trial based on electrical impedancetomography. Intensive Care Med 2008; 34:543–550.
During a PEEP titration maneuver, the authors were able to identify the start of lungcollapse using electrical impedance tomography to image regional changes in thelungs.
10
�Costa ELV, Chaves CN, Gomes S, et al. Real-time detection of pneumothoraxusing electrical impedance tomography. Crit Care Med 2008; 36:1230–1238.
This study shows that it is possible to detect small volumes of pneumothorax usingelectrical impedance tomography.
11 Hahn G, Just A, Dudykevych T, et al. Imaging pathologic pulmonary air andfluid accumulation by functional and absolute EIT. Physiol Meas 2006;27:S187–S198.
12 Bayford RH. Bioimpedance tomography (electrical impedance tomography).Annu Rev Biomed Eng 2006; 8:63–91.
13 Brown BH. Electrical impedance tomography (EIT): a review. J Med EngTechnol 2003; 27:97–108.
14 Harris ND, Suggett AJ, Barber DC, Brown BH. Applications of appliedpotential tomography (APT) in respiratory medicine. Clin Phys Physiol Meas1987; 8 (Suppl A):155–165.
orized reproduction of this article is prohibited.

C
24 Respiratory system
15 Nopp P, Harris ND, Zhao TX, Brown BH. Model for the dielectric properties ofhuman lung tissue against frequency and air content. Med Biol Eng Comput1997; 35:695–702.
16 Adler A, Amyot R, Guardo R, et al. Monitoring changes in lung air and liquidvolumes with electrical impedance tomography. J Appl Physiol 1997;83:1762–1767.
17 Gattinoni L, Pelosi P, Vitale G, et al. Body position changes redistribute lungcomputed-tomographic density in patients with acute respiratory failure.Anesthesiology 1991; 74:15–23.
18 Borges JB, Okamoto VN, Matos GFJ, et al. Reversibility of lung collapse andhypoxemia in early acute respiratory distress syndrome. Am J Respir Crit CareMed 2006; 174:268–278.
19 Seagar AD, Barber DC, Brown BH. Theoretical limits to sensitivity andresolution in impedance imaging. Clin Phys Physiol Meas 1987; 8 (Suppl A):13–31.
20
�Wrigge H, Zinserling J, Muders T, et al. Electrical impedance tomographycompared with thoracic computed tomography during a slow inflation man-euver in experimental models of lung injury. Crit Care Med 2008; 36:903–909.
This study shows that an index of regional ventilation delay based on electricalimpedance tomography can be used to monitor lung recruitment.
21
�Deibele JM, Luepschen H, Leonhardt S. Dynamic separation of pulmonary andcardiac changes in electrical impedance tomography. Physiol Meas 2008;29:S1–S14.
This study describes technical aspects of a method capable of separatingpulmonary and cardiac changes in the electrical impedance signal, and appliesthe method to two healthy volunteers.
22 Villar J, Kacmarek RM, Perez-Mendez L, Aguirre-Jaime A. A high positive end-expiratory pressure, low tidal volume ventilatory strategy improves outcome inpersistent acute respiratory distress syndrome: a randomized, controlled trial.Crit Care Med 2006; 34:1311–1318.
23 Amato MB, Barbas CS, Medeiros DM, et al. Effect of a protective-ventilationstrategy on mortality in the acute respiratory distress syndrome. N Engl J Med1998; 338:347–354.
24 Suarez-Sipmann F, Bohm SH, Tusman G, et al. Use of dynamic compliancefor open lung positive end-expiratory pressure titration in an experimentalstudy. Crit Care Med 2007; 35:214–221.
25 Hinz J, Moerer O, Neumann P, et al. Regional pulmonary pressure volumecurves in mechanically ventilated patients with acute respiratory failuremeasured by electrical impedance tomography. Acta Anaesthesiol Scand2006; 50:331–339.
26 Beraldo MA, Reske A, Borges JB, et al. PEEP titration by EIT (electricimpedance tomography): correlation with multislice CT. Am J Respir CritCare Med 2006; 173:A64.
opyright © Lippincott Williams & Wilkins. Unautho
27 Borges JB, Costa ELV, Beraldo MA, et al. A bedside real-time monitor todetect airspace collapse in patients with ALI/ARDS. Am J Respir Crit CareMed 2006; 173:A377.
28
�Luepschen H, Meier T, Grossherr M, et al. Protective ventilation usingelectrical impedance tomography. Physiol Meas 2007; 28:S247–S260.
This study describes the integration of the center of gravity of ventilation imagesinto a fuzzy controller of mechanical ventilation.
29 Frerichs I, Dargaville PA, van Genderingen H, et al. Lung volume recruitmentafter surfactant administration modifies spatial distribution of ventilation. Am JRespir Crit Care Med 2006; 174:772–779.
30
�Hinz J, Gehoff A, Moerer O, et al. Regional filling characteristics of the lungs inmechanically ventilated patients with acute lung injury. Eur J Anaesthesiol2007; 24:414–424.
This study analyzes regional lung mechanics and shows that tidal recruitment andoverdistension coexist during mechanically patients.
31
�Wolf GK, Grychtol B, Frerichs I, et al. Regional lung volume changes inchildren with acute respiratory distress syndrome during a derecruitmentmaneuver. Crit Care Med 2007; 35:1972–1978.
This study identified lung derecruitment after endotracheal suctioning in children.
32
�Lindgren S, Odenstedt H, Erlandsson K, et al. Bronchoscopic suctioning maycause lung collapse: a lung model and clinical evaluation. Acta AnaesthesiolScand 2008; 52:209–218.
Study demonstrating lung collapse during bronchoscopy.
33 Beraldo MA, Costa ELV, Gomes S, et al. Detection of pleural effusion at thebedside by EIT. Am J Respir Crit Care Med 2007; 173:A791.
34
�Steinmann D, Stahl CA, Minner J, et al. Electrical impedance tomography toconfirm correct placement of double-lumen tube: a feasibility study. Br JAnaesth 2008; 101:411–418.
This study shows that electrical impedance tomography allows for detection ofmainstem bronchus intubation, but cannot fully replace bronchoscopy as a guideto one lung ventilation.
35
�Wagner PD. The multiple inert gas elimination technique (MIGET). IntensiveCare Med 2008; 34:994–1001.
Excellent review of the MIGET technique.
36
�Tanaka H, Ortega NRS, Galizia MS, et al. Fuzzy modeling of electricalimpedance tomography images of the lungs. Clinics 2008; 63:363–370.
Study describing a fuzzy modeling technique for heart and lung segmentationusing electrical impedance tomography.
37 Frerichs I, Hinz J, Herrmann P, et al. Regional lung perfusion as determined byelectrical impedance tomography in comparison with electron beam CTimaging. IEEE Trans Med Imaging 2002; 21:646–652.
38 Smit HJ, Vonk Noordegraaf A, Marcus JT, et al. Determinants of pulmonaryperfusion measured by electrical impedance tomography. Eur J Appl Physiol2004; 92:45–49.
rized reproduction of this article is prohibited.