Embed Size (px)
Citation preview

Education of the Educators
Education of the patient has always been considered to be an important aspect of management of Diabetes mellitus. In practice, meaningful education has played little part in most diabetic services throughout the country and, indeed, very few centres have established a formal plan of diabetes education for a11 patients. It is therefore gratifying to note the formation of an autonomous Education Section of the British Diabetic Association; it is expected that this will lead to vigorous activity in the field of diabetes education and make the subject relevant and important enough to attract some of the best minds amongst us.
Whilst it is quite appropriate for the Professions to consider the different media of education and its methods of delivery, it is equally important to consider who is best equipped to impart knowledge to patients. Teachers in schools and colleges have to undergo a period of training in the art and skills of teaching. With rare exceptions, the vast majority of senior nurses and doctors have received no such formal training; most of the best teachers amongst them have learnt their skills by trial and error, aided by innate talent. It is therefore not unreasonable to question the efficiency of doctors and nurses as educators.
In addition to the art and science of teaching, a basic requirement of a teacher is the possession of an adequate knowledge of his subject. Although there has been no formal assessment of the standard of teaching about diabetes in medical schools, it is nevertheless a common “clinical impression” that there is considerable room for improvement; this observation applies equally to the coverage of the subject in a doctor’s general professional training. In this issue, Knight et a1 report findings which
general impression. The implications lend support to this are most disturbing.’
Education of the Educators must be taken seriously and undertaken with urgency because, without suitably trained doctors and nurses, plans for patient education simply cannot be implemented. It is also pertinent to ask why a relatively small number of general practitioners are motivated to look after the diabetic patients in their practices. Efforts to interest more doctors in general practice in the responsibility of caring for diabetics must clearly continue but improvements in the teaching of diabetes amongst undergraduates would probably be an even more rewarding measure.
There is a steady rise in the number of nurses involved in the care of diabetes, together with an almost equal increase in the number of “labels” to their posts. How does one discern the subtle differences between Diabetes Liaison Sister, Nurse Specialist in Diabetes, Nurse Consultant and Nurse Technician? How, indeed, are these different grades trained and assessed? The simple truth is that there is no defined training and no assessment.
If the establishments involved in the training of doctors and nurses disagree with any of these observations, they should have no objection to the carrying out of a formal assessment of training programmes, for they will presumably have nothing to fear from such scrutiny. The need for an assessment can hardly be denied, for it is the only firm basis upon which t o attempt to bring about relevant and significant changes.
The immediate question is: “Who should initiate this move?“ The matter of the education of the educator cannot be allowed to be pushed aside by the current surge of enthusiasm for education of the patient. AKB
Reviewing What We Do and What We Fail to Do
Do you work, as I do, in a diabetic clinic where the service which you provide leaves rather a lot to be desired? Towards the end of a busy clinic, and with the waiting room still uncomfortably full, are you tempted to scan the fundi rather too quickly, or do you write in the notes “Examine feet next time”, knowing that you will probably be just as hard-pressed on this patient’s next visit? I suspect that most of us do these things, feeling a little guilty as we do them, but consoling ourselves with the thought that we can do no better with the time and resources which are available to us. This is an understandable attitude but one which inevitably engenders a degree of complacency. Perhaps we ought to look more objectively at just how often we are departing from acceptable medical practice.
Practical DIABETES November 1984 Vol 1 No 2
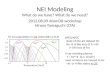
Some of the components which I regard as essential to good diabetic management are listed in the Table. We might argue about how frequently these investigations should be done but would surely agree that they should be carried out at regular intervals. I have reviewed the notes of 44 patients who attended my diabetic clinic on one day. 17 patients were excluded from the survey because they had been attending the clinic for less than four years. 19 of the remaining 27 patients were treated with insulin and 8 with oral hypoglycaemic drugs. The results are shown in the Table. I suspect that these results are no worse than those to be found in many diabetic clinics, but by the standards applied to other areas of medical practice they are poor. What would be our reaction if half the samples which we
3

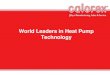
TABLE. Frequency of some examinations and investigations in 27 patients attending a diabetic clinic.
Examination/ Investigation
Fundi
Feet
Blood pressure
Dietary review
Proteinuria
Blood , &as:‘,
Serum cholesterol
H bA, ( i f o n insulin)
% Patients Examined in: Last 1 Year List 3 Year
85 100
33 56
78 93
41 67
100 100
89 100
48 74
89 100
sent for laboratory investigation came back with the report: “Insufficient time and staff to deal with this request”?
It is clear that we do some things better than others. Among the areas which we consistently neglect are the examination of the feet and dietary review. I am particul- arly disappointed by the poor record of examining the feet because I am impressed by the evidence suggesting thar much of the morbidity and mortality which result from diabetic iuo; 2isease can be prevented by intensive education and early treatment in high risk groups. (Refs I, 2, 3). Further analysis of the data shows that the propor- tion of my patients who have their feet examined in any one year has not improved over the last four years: 1984,33%; 1983,30%; 1982,22% and 1981,33%. Many of the patients whose feet are examined are already known to have foot problems, so the number of newly discovered “at risk” patients in any year is small.
How does it help me to have the information from this study? I must of course recognise that the figures tell only part of the story. Not every patient who is recorded as having had his eyes examined has necessarily had an adequate examination of the fundi, and not every newly detected hypertensive may have had his blood pressure satisfactorily controlled. Nevertheless, I think the results do provide potentially useful information. First, I may be able to make some small improvements without additional resources. For example, the format of the notes used for follow-up visits makes it difficult to see at a glance what has been done and what has been omitted in preceding years. Redesigning the notes to include a separate column for examination of the feet should help to identify those pat-nts whose feet have not been examined for some years.
Another separate column for the blood pressure might eliminate unnecessarily frequent recordings in those patienis whose blood pressure has been recorded as normal in each of the last five years. A notice in the clinic which encourages patients to refer themselves directly to
4
Reviewing what we do and what we fail to do
the dietitian might improve the rate of dietary review. If it generated more work than the dietitian could manage then complaints from patients that they were unable to see a dietitian would have a greater effect on administrators than any pleas that I could make for additional dietetic expertise.
I shall of course use the information from this survey to add substance to my case when pressing both unit and district management teams for additional resources. Our management teams have a difficult task in the present financial climate and are more likely to be impressed by documented fact than by unsubstantiated opinion and grumbling. In this respect, it would help to have more substantial evidence than is currently available about the costs and benefits of adequate diabetic care (Ref 4).
It would add weight to efforts made at district level if more information were collected on a national basis. We have much to learn from the obstetricians who have for many years contributed to the triennial Reports on Confidential Enquiries into Maternal Deaths, which are published under the aegis of the DHSS. These reports have consistently emphasised the importance of a high standard of antenatal care with a consequent improvement in the facilities required to provide such care. In his preface to one report, the Chief Medical Officer “hoped that other comparable exercises will become part of the Health Service in future” (Ref 5).
The identification of avoidable factors in the causation of premature deaths due to diabetes might be more difficult than the comparable exercise for maternal deaths, but it could and should be attempted on a national basis. Meanwhile, much might be achieved at district level if we followed Osler’s injunction (Ref 6).
“Zf you have the good fortune to command a large clinic, remember that one of y o y chief duties is the tabulation and anaIysi; of the carefully recorded experience.”
Only by demonstrating the true extent of our patient’s need can we expect to meet that need.
H Connor
References (1) Davidson J K, Alogna M, Goldsmith M, Borden J.
Assessment of program effectiveness at Grady Memorial Hospital - Atlanta. In Steiner G, Lawrence P A (Eds). Educating diabetic patients. New York, Springer Publishing Co, 1981; 329-48.
(2) Assal J-P, Gfeller R, Ekoe J-M. Patient education in diabetes. In Recent trends in diabetic research. Stockholm, Almqvist & Wiksell International, 1982; 276-89.
Prevention and amputation level of lower limbs in diabetics. Abstract submitted to IV World Congress International Society for Prosthetics and Orthotics, London, 5-9 September 1983.
Diabetic management and education: costs and benefits. In Baksi A K , Hide D W, Giles G (Eds). Diabetes Education. Chichester, John Wiley & Sons Ltd, 1984; 3-10.
Preface to report Ojr confidential enquiries into maternal deaths in England and Wales. 1967-1969. London, Her Majesty’s Stationery Office, 1972.
Sir William Osler - Aphorisms. Springfield, Illinois, Charles C Thomas, 1961; 76.
(3) Vaucher J, Assal J-P, Ekoe J-M, Kreinhofer M.
(4) Connor H.
(5) Godber G.
(6) Bean W B (Ed).
Practical DIABETES November 1984 Vol 1 No 2