Neuropathology and Applied Neurobiology (2011), 37, 118134
doi: 10.1111/j.1365-2990.2010.01131.x
Review: The neuropathology of drug abuseA. Bttner Institute of
Forensic Medicine, University of Rostock, Rostock, Germany
_
118..134
A. Bttner (2011) Neuropathology and Applied Neurobiology 37,
118134 The neuropathology of drug abuseDrug abuse represents a
signicant health issue. The major substances abused include
cannabis, opiates, cocaine, amphetamine, methamphetamine and
ecstasy. Alterations of intracellular messenger pathways,
transcription factors and immediate early genes within the brain
reward system seem to be fundamentally important for the
development of addiction and chronic drug abuse. Genetic risk
factors and changes in gene expression associated with drug abuse
are still poorly understood. Besides cardiovascular complications,
psychiatric and neurologic symptoms are the most common
manifestations of drug toxicity. A broad spectrum of changes
affecting the central nervous system is seen in drug abusers. The
major ndings result from the consequences of ischaemia and
cerebrovascular diseases. Except for a few observations of
vasculitis, the aetiology of these cerebrovascular accidents is not
fully understood. The abuse of amphetamine, methamphetamine and
MDMA has been related to neurotoxicity in human long-term abusers
and to the risk of developing Parkinsons disease. However, whether
such neurotoxicity occurs remain to be established. Systematic
histological, immunohistochemical and morphometric investigations
have shown profound morphological alterations in the brains of
polydrug abusers. The major ndings comprise neuronal loss,
neurodegenerative alterations, a reduction of glial brillary acidic
proteinimmunopositive astrocytes, widespread axonal damage with
concomitant microglial activation as well as reactive and
degenerative changes of the cerebral microvasculature. These
observations demonstrate that drugs of abuse initiate a cascade of
interacting toxic, vascular and hypoxic factors, which nally result
in widespread disturbances within the complex network of central
nervous system cell-to-cell interactions.
Keywords: astrocytes, cerebral microvasculature, drug abuse,
microglia, neurodegeneration
IntroductionDrug abuse represents a serious health issue
worldwide. Drugs of abuse can be grouped as stimulants, analgesics
and narcotics, hypnotics as well as antidepressants, nicotine and
alcohol [13]. Besides the latter two substances, the predominant
substances abused include cannabis, opiates, cocaine, amphetamine,
methamphetamine and designer drugs [1,2]. Although individuals with
a drug habit may favour one or other class of drug, depending
in
Correspondence: Andreas Bttner, Institute of Forensic Medicine,
University of Rostock, St.-Georg-Strasse 108, 18055 Rostock,
Germany. Tel: +49 381 494 9900; Fax: +49 381 494 9902; E-mail:
[email protected]
part on what is available, most perform polysubstance abuse
[48]. The methodological problems in investigating the effects of
drugs of abuse on the central nervous system (CNS) consist of
distinguishing between substancespecic effects related to the
properties of the drug itself, the inuence of adulterants, and of
secondary effects related to the lifestyle of drug abusers, for
example, malnutrition, infections and systemic diseases. Because
polysubstance abuse is seen in the majority of cases, it is difcult
to relate the observed ndings to a single substance. Therefore, in
most cases the exact aetiology of the various CNS alterations
remains unclear. Injecting drug abuse is also a risk factor for the
acquisition of HIV-1 infection and there is evidence that
118
2011 The Author Neuropathology and Applied Neurobiology 2011
British Neuropathological Society
The neuropathology of drug abuse
119
HIV-1-associated CNS disorders are accentuated in drug abusers
[9,10]. Infection of the brain with hepatitis viruses, especially
with hepatitis C virus (HCV) is another potential confounding
factor in the neuropathological appearances of the observed brain
changes. Injection drug abusers are the largest group of persons
infected with HCV, with a prevalence of 5090% [11]. The
transmission of HCV is not the effect of the drug injected but of
sharing contaminated equipment [11]. In contrast to HIV, HCV is
detectable in high concentrations in other utensils for heroin
injection, such as lters, spoons and rinsing liquids. Besides
hepatic encephalopathy, there is also emerging evidence of
neurocognitive impairment in HCV infection independently of drug
abuse or HIV-1 infection [1215]. Research on the neurobiology of
addiction has shown that the reinforcing properties of most drugs
of abuse are mediated by activation of the mesolimbic dopaminergic
system, the orbitofrontal cortex and the extended amygdala [1619].
Alterations of the intracellular messenger pathways, transcription
factors and immediate early gene expression in these reward
circuits are believed to be important for the development of
addiction and chronic drug abuse [1620]. Possible genetic risk
factors for drug addiction and changes in gene expression,
associated with drug abuse, are still poorly understood [21,22].
Although a broad spectrum of alterations affecting the CNS has been
described in drug abusers [1,2,23], there is no specic change that
is characteristic and little is known about the fundamental
neuropathological alterations of the cellular elements of the human
brain. Therefore, despite a large body of literature on animal
models, the following review will focus on the relevant human CNS
ndings. The pharmacology and CNS alterations in alcohol and
nicotine abuse are reviewed elsewhere [3,2427].
tions and hyperintense lesions have been demonstrated in the
white matter, which were attributed to ischaemic lesion [34,3840].
Single photon emission computed tomography showed focal perfusions
decits in various brain regions [4145]. On positron emission
tomography a reduction of the global glucose metabolism has been
demonstrated [46,47]. Studies using proton magnetic resonance
spectroscopy have identied several biochemical changes in the brain
that may underlie the neuropathology that subsequently gives rise
to the cognitive and behavioural impairments associated with drug
addiction [48]. Some neurochemical abnormalities have been
attributed to alterations in nonneuronal brain tissue [48].
Diffusion tensor imaging revealed microstructural abnormalities in
the white matter and the corpus callosum, suggestive of axonal
injury [4954]. Despite these numerous neuroimaging studies, the
cause or possible morphological correlates of these alterations are
still not fully resolved.
CNS effects of the major drugs of abuseDepending of the
frequency and types of drugs abused, the predominant
neurologic-psychiatric complications of drug abuse include a high
prevalence of depression, memory loss and cognitive decline, and
the possible predisposition to schizophrenia.
CannabisCannabis is the most commonly used illicit drug
worldwide [2,5559]. Cannabis preparations (marihuana, hashish) are
usually mixed with tobacco and smoked. Oral ingestion as tea or
addition to pastries is also widespread. Cannabis is unsuitable for
intravenous use as it is relatively waterinsoluble. The
concentration of the major psychoactive component of cannabis,
D9-tetrahydrocannabinol (THC), varies according to the preparation
and the origin of the plant from 1% to 7% in marihuana, 2% to 10%
in hashish and 10% to 60% in hash oil [55,57]. Cannabis combines
many of the properties of alcohol, tranquillizers, opiates and
hallucinogens; it is anxiolytic, sedative, analgesic and
psychedelic [55]. The psychotropic action of cannabis starts after
several minutes reaches a maximum by 2030 min and persists for 24
h. However,
Neuroimaging ndingsNeuroimaging studies revealed widespread
alterations in the brains of drug abusers [28]: Computed tomography
studies have shown diffuse brain atrophy [2931]. On magnetic
resonance imaging decreased grey and white matter volume has been
demonstrated in particular areas of the brain [3237]. Moreover,
focal demyelina-
2011 The Author Neuropathology and Applied Neurobiology 2011
British Neuropathological Society, 37, 118134
120
A. Bttner
the action of cannabis is of highly individual variability.
Furthermore, there is a dose-related impairment of cognitive and
psychomotor performance. Acute effects include euphoria and
relaxation with perceptual changes. However, dysphoric reactions,
including anxiety and panic, depression, paranoia and psychosis can
also occur. Systemic effects include a dose-related tachycardia,
vasodilation and postural hypotension [5559]. THC is a
lipid-soluble substance that is distributed heterogeneously within
the brain, with its highest concentrations in neocortical, limbic,
sensory and motor areas [5558]. THC and other cannabinoids exert
their effects by the interaction with specic cannabinoid receptors,
which are distributed heterogeneously within the brain [5964]. Two
cannabinoid receptors, CB1 and CB2, have been pharmacologically
characterized and anatomically localized. CB1 receptors are found
predominantly in the central and peripheral nervous system, where
they have been implicated in presynaptic inhibition of
neurotransmitter release. CB2 receptors are present on immune
cells, where they may be involved in cytokine release [5965]. The
highest density of CB1 receptors is found in the substantia nigra,
the basal ganglia, the hippocampus and the cerebellum [63,66,67].
Within the neocortex they are present with the highest density in
the frontal cortex, the dentate gyrus, the mesolimbic dopaminergic
system and the temporal lobe [63,66,67]. This specic distribution
of CB1 receptors correlates well with the effects of cannabinoids
on memory, perception and movement control. The very low density of
CB1 receptors in the brain stem and medulla oblongata explains the
low acute toxicity and lack of lethality of cannabis [55,59,66].
Nevertheless, the CNS toxicity of cannabis seems to have been
underestimated for a long time [68], as recent ndings revealed
THC-induced neuronal death in cultured rat neurones [6971]. The
discovery of specic endogenous cannabinoid receptor ligands
(endocannabinoids), and the distribution of their receptors,
strongly suggests that these lipid neurotransmitter systems play an
important role in higher cortical-emotional functions, memory
storage, movement coordination and several pathological conditions
[59,6265,72,73]. Despite its widespread abuse, cannabis-related
cerebrovascular events are infrequently reported. They are believed
to be due to a cannabis-induced vasospasm or a
cannabis-induced hypotension [7478]. However, due to the
widespread use of this drug, it is difcult and often impossible to
establish whether these strokes are truly associated with cannabis,
other ingested drugs, or purely coincidental. The important
question whether cannabis can cause irreversible brain damage,
particularly to adolescents, or lead to increased risk for
schizophrenia, persisting beyond transient intoxication, is still a
matter of debate [79,80].
Opioids and derivativesOpioids, especially heroin, are the
leading substances that cause death in drug abusers. Derivatives
include morphine, hydrocodone, oxycodone, hydromorphine, codeine
and other narcotics such as fentanyl, meperidene, methadone and
opium [2,3]. Heroin is made from opium and crosses the bloodbrain
barrier (BBB) faster than morphine [81]. Heroin is usually
administered intravenously. Intranasal and subcutaneous
administration is also possible. Heroin alkaloid may be prepared
for inhalation by heating on metallic foil (chasing the dragon)
that results in a higher bioavailability of heroin compared with
smoking in a cigarette [3]. Intravenous heroin induces an extreme
euphoria lasting for several minutes. Subsequently, there is a
pleasant dream-like state with drowsiness and analgesia [81].
However, marked tolerance develops to euphoria. Opiate overdose
produces the triad of coma, respiratory depression and miosis [81].
Between 50% and 70% of intravenous heroin abusers have experienced
a non-fatal overdose at some time in their lives [4]. Medical
complications of long-term heroin abuse include thrombophlebitis,
endocarditis, hepatitis, pneumonia, nephropathy and
immunodepression [2,81]. Due to the practise of needlesharing,
there is a high risk for infections [11]. Risk factors for
opioid-induced deaths include overdose, concomitant use of other
CNS depressants and loss of tolerance after a period of abstinence
[48]. At necropsy, up to 90% of all cases of persons dying of
heroin overdose show brain oedema with prominent tonsillar
herniation and uncal grooving. However, rapid death after heroin
intake will not lead to any morphological evidence of neuronal cell
injury. In cases of delayed death after a survival period of 5 h or
longer, hypoxicischaemic leukoencephalopathy with loss of neurones
in
2011 The Author Neuropathology and Applied Neurobiology 2011
British Neuropathological Society, 37, 118134
The neuropathology of drug abuse
121
the hippocampal formation, the Purkinje cell layer and/or the
olivary nucleus, as well as vascular congestion, will become
apparent [8286]. In the globus pallidus, neuronal loss and
bilateral, symmetrical ischaemic lesions/ necrosis have been
described in 510% of cases [85,87]. All the above mentioned
alterations are assumed to be caused rather by recurrent episodes
of hypoxia during the intoxicated state than to be related to
direct neurotoxic effects of the opioid drugs [8287]. Stroke in
heroin abusers, occurring in the absence of endocarditis or mycotic
aneurysms, has rarely been observed [84,8893]. Within the
hippocampus of heroin deaths, enhanced expression of glial brillary
acidic protein (GFAP) by astrocytes and/or a proliferation of
microglia have been found [84]. However, an increased GFAP
expression could not be conrmed by other authors [23]. An increase
in polysialic acid neural cell adhesion molecule positive
hippocampal neurones and astrocytes is assumed to reect an attempt
to repair cell damage [94]. Perivascular pigment-laden macrophages
and pigment depositions are sometimes observed and are attributed
to repeated intravenous injections of impure heroin [95], or to BBB
breakdown [23,96]. Infections in heroin abusers result from
unsterile injection techniques and from immunosuppression, caused
by chronic opiate abuse [1,2,11,85,97]. Endocarditis might lead to
septic foci in the brain or to intracranial mycotic aneurysms
[1,2,85,97]. Transverse myelitis/myelopathy is an exceptionally
rare lesion described in heroin abusers [1,2,85,98,99]. The
aetiology is still unclear and neither the clinical picture nor the
pathological changes correspond to any particular pattern. A
distinct entity, spongiform leukoencephalopathy, has been reported
to occur almost exclusively after inhalation of heroin pyrolysate
vapours (chasing the dragon) [1,2,100102]. The most characteristic
nding is the selective involvement of the posterior limb of the
internal capsule and sparing of subcortical U-bres.
Neuropathological examination reveals spongiform degeneration of
the deep white matter with vacuolation of the myelin sheath, loss
of oligodendrocytes, axonal reduction and astrogliosis. The grey
matter is usually unremarkable and the brainstem, spinal cord and
peripheral nerves are spared [100102]. A lipophilic toxin-induced
process was considered to be due to contaminants, but a denite
toxin could not yet be identied.
Alterations of neurotransmitters and receptorsLong-term heroin
abuse seems not to be related with a reduced density of CNS m- and
d-opioid receptors [103 106]. Instead, the molecular mechanisms
underlying opiate addiction seem to involve the second messenger
signalling system [16,18,19,104,107114]. Necropsy studies revealed
that long-term heroin abuse causes an increase in certain G
proteins in different regions of the brain [105,107,110]. Others
have shown a decreased level of Ca2+-dependent protein kinase C-a
[104] and an increased level of a membrane-associated G
proteincoupled receptor kinase [113]. Further ndings include the
downregulation of the adenylyl-cyclase subtype I [109,111], a
decrease in the density of alpha 2-adrenoreceptors [103], a
decrease in the immunoreactivity of protein kinase C-ab [114], and
decreased levels of neurolament proteins [115]. Within the
dopaminergic system the levels of tyrosine hydroxylase protein and
those of the dopamine (DA) metabolite homovanillic acid were
reduced in the nucleus accumbens [116]. Striatal levels of
serotonin (5-hydroxytryptamine or 5-HT) were either normal or
elevated, whereas the concentration of the 5-HT metabolite
5-hydroxyindoleacetic acid was decreased [116]. According to the
authors, chronic heroin abuse might produce a modest reduction in
dopaminergic and serotonergic activity that could affect
motivational state and impulse control. Maintenance therapy for
heroin addiction includes codeine, dihydrocodeine, methadone and
buprenorphine [117120]. In the majority of deaths related to these
substances, additional CNS depressant drugs, mainly alcohol and
benzodiazepines, can be detected. The neuropathological ndings are
similar to those encountered in heroin deaths.
CocaineCocaine is derived from the leaves of the coca plant.
Cocaine hydrochloride is a water-soluble white salt and the most
frequent preparation of the drug that is available in form of
cystals, granules or a white powder. It can be administered
intranasally (snorting) or injected [2,3]. The free alkaloid form
(free base) that had been extracted with volatile solvents is
usually smoked. Crack cocaine is produced by rst dissolving the
hydrochloride salt in water, then mixing with baking soda and
heating. The
2011 The Author Neuropathology and Applied Neurobiology 2011
British Neuropathological Society, 37, 118134
122
A. Bttner
cracking sound made by the crystals when they are heated
provides the name [2]. Cocaine initially induces profound
subjective well-being together with alertness and increased
self-condence. Subsequently, there is a mild euphoria followed by
fatigue. Acute psychiatric disturbances include dysphoria,
agitation, aggressive behaviour, depression, paranoia, psychosis
and hallucinations. Medical complications include vasoconstriction,
tachycardia, hypertension and sudden cardiac death [3,25,31].
Cocaine is a potent CNS stimulant. It crosses the BBB rapidly due
to its highly lipophilic properties [121,122]. Throughout the
brain, cocaine and its major metabolites are widely distributed and
receptors with varying afnities are found [123,124]. Cocaine acts
by binding to specic receptors at presynaptic sites preventing the
reuptake of neurotransmitters [2,3,122]. The major synaptic effect
of cocaine is the release of dopamine (DA) from the synaptic
vesicles and the blocking of DA reuptake resulting in an enhanced
dopaminergic neurotransmission [2,3,122]. Cocaine is the most
frequent drug of abuse associated with fatal and non-fatal
cerebrovascular events, with either haemorrhagic or ischaemic
strokes [89,91 93,125135]. In contrast to the non-drug-using
population, cocaine-related stroke occurs primarily in young adults
[1,125128]. Cocaine-related ischaemic infarctions can occur in
every brain region [2,128,130]. The underlying cause is attributed
to cerebral vasospasm either by cocaine or its metabolites
[92,128,131,136138]. Other mechanisms include cocaine-induced
cardiac arrhythmia with secondary cerebral ischaemia, or the direct
effects of cocaine on haemostasis with increased platelet
aggregation [89,128,131,135,139,140]. In cocaine-related
intracerebral (ICH) and subarachnoidal (SAH) haemorrhage,
underlying arteriovenous malformations or aneurysms are frequently
observed [93,125,127130,132,141,142]. Cocaine abuse has been shown
to predispose to aneurysmal rupture at a signicantly earlier age,
and in much smaller aneurysms, compared with non-drug-using persons
[125,143]. Cocaine-related ICH is associated more frequently with
subcortical locations, a higher risk of intraventricular
haemorrhage, and poor prognosis compared with nondrug-abusing
patients with spontaneous ICH [144]. Rupture of an arteriovenous
malformation, or aneurysm, are most likely related to the sudden
elevation of blood
pressure and heart rate from the sympathomimetic effect of the
drug [92,128130,132,141,145]. A cocaine-induced cerebral vasculitis
as a cause for cerebrovascular events could only be demonstrated in
rare cases [89,146,147]. In experimental models, cocaine enhances
leucocyte migration across the cerebral vessel wall and opens the
BBB to HIV-1 invasion by a direct effect on brain endothelial cells
and by the induction of pro-inammatory cytokines and chemokines
[148,149].
Alterations of neurotransmitters and receptorsIn the striatum of
cocaine-related deaths, reductions in the levels of enkephalin
mRNA, m-opioid receptor binding and DA uptake site binding, along
with elevation in levels of dynorphin mRNA and k-opioid receptor
binding have been described [150]. In chronic cocaine abusers, a
decreased level of DA was identied in the caudate nucleus and
frontal cortex, but not in the putamen, nucleus accumbens and
cerebral cortex [151155]. This decrease was not paralleled by an
increase of DA D1 and D2 gene expression [156]. Simultaneously,
there was an increase of cocaine binding sites on the DA
transporter with a decrease of the DA D1 receptor density in the
striatum and of DA D1 and DA D3 receptor density in the nucleus
accumbens [152154,157159]. A marked reduction in immunoreactivity
of the vesicular monoamine transporter-2 [151] and of the
transcription factor NURR1 [160] in necropsy samples of human
cocaine abusers might reect damage to the dopaminergic system. An
overexpression of a-synuclein in midbrain DA neurones in chronic
cocaine abusers may occur as a protective response to changes in DA
turnover and increased oxidative stress resulting from cocaine
abuse [161]. This accumulation of a-synuclein protein in long-term
cocaine abuse might increase the risk of developing Parkinsonism
[161]. Further necropsy ndings include an upregulation of k2-opioid
receptors in the limbic system [162] and of cAMP response
element-binding protein in the ventral tegmental area [163]. In the
serotonergic system an increase of the 5-HT transporter in the
striatum, substantia nigra and limbic system has been demonstrated
[164]. In the putamen, a DA-rich brain area, the activity of
phospholipase A2 and phosphocholine cytidylyltransferase was
selectively decreased [165].
2011 The Author Neuropathology and Applied Neurobiology 2011
British Neuropathological Society, 37, 118134
The neuropathology of drug abuse
123
Amphetamines and methamphetamineAmphetamines and methamphetamine
are widely used psychostimulants that act on monoamine transporters
[2,3]. These substances are available as powder, capsules, tablets
or uids. Therefore, they can be swallowed, snorted, injected
intravenously or smoked. The composition, purity and dose are
highly variable [2]. Their potent sympathomimetic effects include
an elevation of pulse rate, blood pressure and an increased level
of alertness. Adverse effects include insomnia, excitability,
seizures, panic attacks, psychosis and aggressive behaviour
[2,3,25]. Throughout the brain, methamphetamine is heterogeneously
distributed [166]. Amphetamines and methamphetamine are the second
most common cause (after cocaine) of strokes occurring largely in
persons younger than 45 years [127]. Furthermore, SAH and ICH have
been described [2,3,91,92,125,126,129,167172]. Similar to cocaine,
a sudden elevation in blood pressure [167,169,171] is postulated as
a major mechanism. The vasoconstrictive effect of both substances
may also lead to the development of ischaemic infarction [167,171].
Methamphetamine has been shown to induce inammatory genes in human
brain endothelial cells [173].
dopaminergic system markers [181,184], the evidence is
inconclusive in regard to dopaminergic system degeneration. To dene
methamphetamine abuse as a risk factor in Parkinson disease, it
would be important to know whether these alterations represent
neurodegenerative changes or a drug-induced compensatory response
to the disruption of neurochemical homeostasis [182,183]. The
mechanisms of methamphetamine-induced neurotoxicity are thought to
be mediated by multiple mechanisms including the generation of free
radicals and nitric oxide, excitotoxicity, mitochondrial
dysfunction, and the induction of immediate early genes as well as
transcription factors [175177,182185]. However, whether
neurotoxicity occurs in human methamphetamine and amphetamine
abusers remains to be established.
Amphetamine and methamphetamine derivativesAmphetamine and
methamphetamine derivatives (designer drugs) comprise a broad
spectrum of substances [2,186]. The street name ecstasy subsumes
different hallucinogenic amphetamine derivatives with MDMA
(3,4-methylenedioxymethamphetamine) and MDE
(3,4-methylenedioxyethylamphetamine) being the main components
[187]. These drugs are taken orally in form of tablets that are
usually embossed with a logo [2]. The effects of MDMA and MDEA last
about 35 h and include relaxation, euphoria, sensual enhancement,
reduction of anxiety and emotional closeness to others. This
psychological prole has been called entactogenic and has the
connotation of inducing a feeling of touch with the world within.
In addition, these substances also have stimulant-like and
hallucinogenic effects [2,188 191]. The effects of MDMA vary
according to the dose and the frequency and duration of use [190].
Adverse effects include headache, nausea, tooth grinding (bruxism),
tachycardia and an increase in body temperature. Furthermore,
hyperactivity, ight of ideas, depersonalization, panic attacks,
anxiety, depression, agitation, delirium, and insomnia may occur
[190]. MDMA interacts with various neurotransmitter circuits but
predominantly affects the dopaminergic and serotonergic system
[186,188191]. In human post mortem tissue, a distinct
immunopositive reaction for MDMA and MDA was observed in the white
matter in all cortical regions and in neurones of the basal
ganglia, the hypo-
Alterations of neurotransmitters and receptorsThe neurotoxic
effects of amphetamines and methamphetamine on the dopaminergic
system have been described in various animal species and in humans.
These effects are characterized by desensitization of DA receptor
function, marked reduction of DA transporters and of DA levels as
well as other dopaminergic axonal markers [174 181]. Similar
alterations have been observed in the serotonergic system [175].
However, the irreversibility of these changes has not been
established [175]. Although these alterations have been attributed
to neurodegeneration, direct evidence for the loss of nerve
terminals and/or their corresponding substantia nigra cell bodies
have not been provided unequivocally [175,177]. Nevertheless, based
on animal studies, there is concern that the alterations in the
dopaminergic system may predispose methamphetamine abusers to
develop Parkinsonism as they age [175,182,183]. Because
neuroimaging and necropsy studies of human methamphetamine abusers
suggest changes in only some
2011 The Author Neuropathology and Applied Neurobiology 2011
British Neuropathological Society, 37, 118134
124
A. Bttner
thalamus, the hippocampus and the cerebellar vermis, but
relatively weak staining of neurones in the brainstem was seen
[192]. In reports on human fatalities following MDMA consumption,
detailed neuropathological examinations were mostly not performed
[193196]. Cerebrovascular complications after ecstasy consumption
have been described only occasionally [197203]. In the globus
pallidus bilateral hyperintense lesions have been found [204,205].
On neuropathological examination necrosis of the globus pallidus,
diffuse astrogliosis and spongiform changes of the white matter
have been described [205]. Other neuropathological ndings in deaths
after ecstasy abuse were mainly due to the complications of
hyperthermia with disseminated intravascular coagulopathy and
consisted of cerebral oedema, focal haemorrhages and nerve cell
loss [196].
ations have been attributed to drug-induced respiratory failure
and were therefore considered to be non-specic [84,220]. However,
in most of these studies, there was no control group and systematic
data on frequency or topography of the lesions are lacking.
Subsequent systematic neuropathological studies of polydrug abusers
revealed ischaemia-independent widespread neuronal loss, a
reduction of GFAP-positive astrocytes, an axonal damage with
concomitant microglia activation as well as reactive and
degenerative vascular changes [23].
NeuronesThe neuronal loss has been ascribed to be due to a
direct impairment of neurones by drugs of abuse and, indirectly, to
drug-induced damage of astrocytes, axons and the cerebral
vasculature [23]. In support of this nding is the observation in
animal models that drugs of abuse can induce apoptotic neuronal
cell death [69,175,221225]. In human studies drug-induced
alterations of neurolament proteins [115,226,227], of neuronal
TUNEL positivity [96] or of transcription factors, for example,
cAMP response element-binding protein [112] and c-fos [20] is
thought to be an alternative pathway for neuronal loss. In young
opiate abusers an increase in the number and distribution of
hyperphosphorylated tau-positive neurobrillary pretangles, fully
formed tangles and neuritic threads has been reported [228]. This,
together with reports of occasional ubiquitin-positive inclusions
in neurones of drug abusers [96], indicates drug-related
neurodegeneration. Whether these changes are potentially reversible
is still unclear. Within the substantia nigra there was a decrease
of the numerical density of the pigmented neurones, whereas the
density of the non-pigmented neurones was unchanged [23]. The
presence of eosinophilic ubiquitinated cytoplasmic inclusions,
which did not resemble classic Lewy bodies, and which are negative
for a-synuclein, indicates abnormal cytoplasmic protein
sequestration [96]. To date it is not clear whether this nding
represents a transient neuronal abnormality or commitment to an
irreversible neurodegenerative pathway [96].
Alterations of neurotransmitters and receptorsIn the brains of
laboratory animals, including nonhuman primates, exposure to MDMA
has been associated with dopaminergic and especially serotonergic
neurotoxicity [176,188191,206209]. There is strong evidence for
neurodegeneration and axonal loss, although the exact mechanism is
still unclear [189191,206209]. Current hypotheses include the
formation of toxic MDMA metabolites with generation of free
radicals as well as oxidative stress, excitotoxicity, apoptosis and
mitochondrial dysfunction [176,209212]. Although in recent years,
the question of ecstasyinduced neurotoxicity and possible
functional sequelae has been addressed in several studies, the
extent to which these animal and non-human primate data are
applicable to humans and whether persistent neurotoxicity occurs in
humans is still controversial [42,207209,213219]. To date, the most
consistent ndings associate subtle cognitive, particularly memory,
impairments with heavy ecstasy abuse [213,218,219].
Neuropathological studiesThe consequences of drugs of abuse on
the cellular elements of the human brain have not been studied
systematically. There are only few reports on histopathological
alterations in the brains of human drug abusers describing oedema,
vascular congestion, ischaemic nerve cell damage and neuronal loss
[8385,96,220]. These alter-
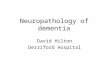
White matterIn the white matter of polydrug abusers a widespread
axonal damage has been demonstrated by using b-APP
2011 The Author Neuropathology and Applied Neurobiology 2011
British Neuropathological Society, 37, 118134
The neuropathology of drug abuse
125
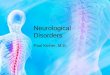
Figure 1. Immunohistochemistry demonstrating
b-APP-immunopositive bundles and b-APP-immunopositive globular
deposits in the pons of polydrug abusers, counterstained with
haematoxylin, original magnication 100.
negative drug abusers and non-drug using controls there was no
statistical difference between these groups in relation to
astrocytes [231,234]. In the brains of polydrug abusers the
numerical density of GFAP-positive astrocytes has been shown to be
reduced [23]. This reduction of GFAP-positive astrocytes is
believed to be due to the interference of drugs with the GFAP gene
transcription, inducing an altered GFAP phosphorylation [235], as
well as the generation of free radicals by induction of a
cytochrome P450 isoform [236]. I2-imidazoline receptors are
involved in the regulation of the GFAP expression [226]. In the
frontal cortex of heroin deaths the density of I2-imidazoline
receptors and the immunoreactivity of the related imidazoline
receptor protein were decreased [237].
immunohistochemistry [23,229]. The alterations consisted of
b-APP-immunopositive bundles and globular depositions (Figure 1),
but they never showed the extensive pattern seen in traumatic brain
injury [23,229]. Furthermore, there is a concomitant activation of
microglia predominantly in the white matter and in most subcortical
regions [23,83,220,229]. This upregulation of microglia has also
been shown in drug abusers with and without pre-symptomatic HIV-1
infection [230,231]. Activated microglial cells are a source of
proinammatory cytokines, which are linked to neuronal damage and
loss [10]. The axonal injury suggests a toxicmetabolic drug effect,
as there were no sufcient ndings for a secondary phenomenon in
these cases, neither due to a generalized hypoxic-ischaemic
condition, nor to a brain oedema and the concomitant activation of
microglia is indicative of a long-standing progressive process
[23,229]. These alterations might be the morphological correlate of
the observed demyelination and hyperintense areas seen on magnetic
resonance imaging.
Vascular changesIn AIDS patients concentric small-vessel wall
thickening, perivascular space dilatation, pigment deposition,
vessel wall mineralization and perivascular inammatory cell
inltrates were seen in 50% of the former drug abusers [238].
Similar vascular alterations can be observed in HIV-1-negative
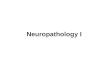
polydrug abusers (Figure 2A) [23,96]. The presence of acute and
chronic BBB breakdown in drug abusers, suggests that the brain
parenchyma is exposed to unusual quantities of serum proteins,
including immunoglobulins, as well as other blood-borne factors,
including HIV [96]. It may further be the stimulus for the
occasional perivascular lymphocytic aggregates that are seen in the
brains of HIV-1-negative drug abusers (Figure 2B) [10].
Furthermore, reactive endothelial cell proliferation, degenerative
hyalinotic thickening, marked endothelial swelling and endothelial
cell hyperplasia are present in the brains of polydrug abusers
(Figure 2C,D) [23]. In addition, a decrease of the collagen type IV
content of the vascular basal lamina [239] and a disruption of the
BBB tight junctions [10] have been observed. This non-inammatory
vasculopathy has been interpreted as the morphological substrate of
a disturbed BBB and might be the morphological substrate of the
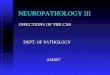
alterations seen on neuroimaging [23,240]. In conclusion, drugs of
abuse initiate a cascade of interacting toxic, vascular and hypoxic
factors that nally result in widespread disturbances within the
complex network of CNS cell interactions (Figure 3). However, much
work will need to be done to clarify the yet
AstrocytesAlthough astrocytes play an essential role, for
example, in the maintenance of BBB, regulation of glutamatergic
neurotransmission and neurotransmitter metabolism, little is known
about alterations of these cells in human drug abusers [232,233].
In an older study widespread fragmentation and a numerical
depletion of astrocytes in the white matter have been reported in
the brains of drug deaths [85]. In HIV-1-positive opiate abusers,
HIV-1-
2011 The Author Neuropathology and Applied Neurobiology 2011
British Neuropathological Society, 37, 118134
126
A. Bttner
A
B
C
D
Figure 2. Photomicrographs illustrating the spectrum of cerebral
vascular changes in polydrug abusers. (A) Small artery in occipital
white matter showing concentric wall thickening. The surrounding
perivascular space contains occasional macrophages and pigment
deposition. H&E, original magnication 200. (B) Small vessel in
the orbital white matter with perivascular lymphocytic aggregates.
H&E, original magnication 200. (C) Endothelial proliferation in
the dentate nucleus, H&E, original magnication 200. (D)
Endothelial hyperplasia in the parietal white matter, H&E,
original magnication 200.
unresolved questions of the disastrous role of drugs of abuse on
the CNS.
AcknowledgementsThe help of Claire Delbridge in correcting the
manuscript is highly appreciated. I thank Jeanne Bell, Institute of
Neuropathology, University of Edinburgh for critical discussions
and Serge Weis, Laboratory of Neuropathology, Neuropsychiatric
Hospital Wagner-Jauregg, Linz, Austria for his long-standing
support and friendship.
ReferencesFigure 3. The consequences of drugs of abuse on the
cellular elements of the CNS.
1 Bttner A, Weis S. Central nervous system alterations in drug
abuse. In Forensic Pathology Reviews, Vol. 1. Ed. M Tsokos. Totowa,
NJ: Humana Press, 2004; 79136
2011 The Author Neuropathology and Applied Neurobiology 2011
British Neuropathological Society, 37, 118134
The neuropathology of drug abuse
127
2 Karch SB. Karchs Pathology of Drug Abuse 4th edn. Boca Raton:
CRC Press, 2008 3 Quinn DI, Wodak A, Day RO. Pharmacokinetic and
pharmacodynamic principles of illicit drug use and treatment of
illicit drug users. Clin Pharmacokinet 1997; 33: 344400 4 Cofn PO,
Galea S, Ahern J, Leon AC, Vlahov D, Tardiff K. Opiates, cocaine
and alcohol combinations in accidental drug overdose deaths in New
York City, 19901998. Addiction 2003; 98: 73947 5 Darke S. Polydrug
use and overdose: overthrowing old myths. Addiction 2003; 98: 711 6
Gerostamoulos J, Staikos V, Drummer OH. Heroinrelated deaths in
Victoria: a review of cases for 1997 and 1998. Drug Alcohol Depend
2001; 61: 1237 7 Preti A, Miotto P, De Coppi M. Deaths by
unintentional illicit drug overdose in Italy, 1984-2000. Drug
Alcohol Depend 2002; 66: 27582 8 Steentoft A, Teige B, Holmgren P,
Vuori E, Kristinsson J, Hansen AC, Ceder G, Wethe G, Rollmann D.
Fatal poisoning in Nordic drug addicts in 2002. Forensic Sci Int
2006; 160: 14856 9 Anthony IC, Arango JC, Stephens B, Simmonds P,
Bell JE. The effects of illicit drugs on the HIV infected brain.
Front Biosci 2008; 13: 1294307 10 Bell JE, Arango JC, Anthony IC.
Neurobiology of multiple insults: HIV-1-associated brain disorders
in those who use illicit drugs. J NeuroImmune Pharmacol 2006; 1:
18291 11 Backmund M, Reimer J, Meyer K, Gerlach JT, Zachoval R.
Hepatitis C virus infection and injection drug users: prevention,
risk factors, and treatment. Clin Infect Dis 2005; 40 (Suppl. 5):
S3305 12 Cherner M, Letendre SL, Heaton RK, Durelle J, MarquieBeck
J, Gragg B, Grant I. Hepatitis C augments cognitive decits
associated with HIV infection and methamphetamine. Neurology 2005;
64: 13437 13 Forton DM, Taylor-Robinson SD, Thomas HC. Central
nervous system changes in hepatitis C virus infection. Eur J
Gastroenterol Hepatol 2006; 18: 3338 14 Martin-Thormeyer EM, Paul
RH. Drug abuse and hepatitis C infection as comorbid features of
HIV associated neurocognitive disorder: neurocognitive and
neuroimaging features. Neuropsychol Rev 2009; 19: 215 21 15
Morgello S. The nervous system and hepatitis C virus. Semin Liver
Dis 2005; 25: 11821 16 Cunha-Oliveira T, Rego AC, Oliveira CR.
Cellular and molecular mechanisms involved in the neurotoxicity of
opioid and psychostimulant drugs. Brain Res Brain Res Rev 2008; 58:
192208 17 Hyman SE, Malenka RC, Nestler EJ. Neural mechanisms of
addiction: the role of reward-related learning and memory. Annu Rev
Neurosci 2006; 29: 56598 18 Koob GF, Volkow ND. Neurocircuitry of
addiction. Neuropsychopharmacology 2010; 35: 21738
19 Nestler EJ. Molecular mechanisms of drug addiction.
Neuropharmacology 2004; 47: 2432 20 Harlan RE, Garcia MM. Drugs of
abuse and immediateearly genes in the forebrain. Mol Neurobiol
1998; 16: 22167 21 Kuhar MJ, Joyce A, Dominguez G. Genes in drug
abuse. Drug Alcohol Depend 2001; 62: 15762 22 Nestler EJ, Landsman
D. Learning about addiction from the genome. Nature 2001; 409: 8345
23 Bttner A, Weis S. Neuropathological alterations in drug abusers:
the involvement of neurons, glial, and vascular systems. Forensic
Sci Med Pathol 2006; 2: 11526 24 Bttner A, Weis S. Central nervous
system alterations in alcohol abuse. In Forensic Pathology Reviews,
Vol. 5. Ed. M Tsokos. Totowa, NJ: Humana Press, 2008; 6989. 25
Trelles L, Jeri R. Central nervous system stimulants: cocaine,
amphetamine, nicotine. In Handbook of Clinical Neurology, Vol. 65:
Intoxications of the Nervous System, Part II. Eds PJ Vinkens, GW
Bruyn, FA de Wolff. Amsterdam: Elsevier, 1995; 25172. 26 Harper C.
The neuropathology of alcohol-related brain damage. Alcohol Alcohol
2009; 44: 13640 27 Yildiz D. Nicotine, its metabolism and an
overview of its biological effects. Toxicon 2004; 43: 61932 28
Kaufman MJ. Brain Imaging in Substance Abuse: Research, Clinical,
and Forensic Applications. Totowa, NJ: Humana Press, 2001 29
Pascual-Leone A, Dhuna A, Anderson DC. Cerebral atrophy in habitual
cocaine users. A planimetric CT study. Neurology 1991; 41: 348 30
Pezawas LM, Fischer G, Diamant K, Schneider C, Schindler SD,
Thurnher M, Ploechl W, Eder H, Kasper S. Cerebral CT ndings in male
opioid-dependent patients: stereological, planimetric and linear
measurements. Psychiatry Res Neuroimag 1998; 83: 13947 31 Strang J,
Gurling H. Computerized tomography and neuropsychological
assessment in long-term high-dose heroin addicts. Br J Addict 1989;
84: 101119 32 Bartzokis G, Beckson M, Lu PH, Edwards N, Rapoport R,
Wiseman E, Bridge P. Age-related brain volume reductions in
amphetamine and cocaine addicts and normal controls: implications
for addiction research. Psychiatry Res 2000; 98: 93102 33 Berman S,
ONeill J, Fears S, Bartzokis G, London ED. Abuse of amphetamines
and structural abnormalities in the brain. Ann N Y Acad Sci 2008;
1141: 195220 34 Lim KO, Wozniak JR, Mueller BA, Franc DT, Specker
SM, Rodriguez CP, Silverman AB, Rotrosen JP. Brain macrostructural
and microstructural abnormalities in cocaine dependence. Drug
Alcohol Depend 2008; 92: 16472 35 Lyoo IK, Pollack MH, Silveri MM,
Ahn KH, Diaz CI, Hwang J, Kim SJ, Yurgelun-Todd D, Kaufman MJ,
Renshaw PF. Prefrontal and temporal gray matter density decreases
in opiate dependence. Psychopharmacology (Berl) 2006; 184:
13944
2011 The Author Neuropathology and Applied Neurobiology 2011
British Neuropathological Society, 37, 118134
128
A. Bttner
36 Schlaepfer TE, Lancaster E, Heidbreder R, Strain EC, Kosel M,
Fisch H-U, Pearlson GD. Decreased frontal white-matter volume in
chronic substance abuse. Int J Neuropsychopharmacol 2007; 9: 14753
37 Ycel M, Solowij N, Respondek C, Whittle S, Fornito A, Pantelis
C, Lubman DI. Regional brain abnormalities associated with
long-term heavy cannabis use. Arch Gen Psychiatry 2008; 65: 694701
38 Bae SC, Lyoo IK, Sung YH, Yoo J, Chung A, Yoon S-J, Kim D-J,
Hwang J, Kim SJ, Renshaw PF. Increased white matter
hyperintensities in male methamphetamine abusers. Drug Alcohol
Depend 2006; 81: 838 39 Bartzokis G, Goldstein IB, Hance DB,
Beckson M, Shapiro D, Lu PH, Edwards N, Mintz J, Bridge P. The
incidence of T2-weighted MR imaging signal abnormalities in the
brain of cocaine-dependent patients is age-related and
region-specic. AJNR Am J Neuroradiol 1999; 20: 162835 40 Lyoo IK,
Streeter CC, Ahn KH, Lee HK, Pollack MH, Silveri MM, Nassar LE,
Levin JM, Sarid-Segal O, Ciraulo DA, Renshaw PF, Kaufman MJ. White
matter hyperintensities in subjects with cocaine and opiate
dependence and healthy comparison subjects. Psychiatry Res
Neuroimag 2004; 131: 13545 41 Botelho MF, Relvas JS, Abrantes M,
Cunha MJ, Marques TR, Rovira E, Fontes Ribeiro CA, Macedo T. Brain
blood ow SPET imaging in heroin abusers. Ann N Y Acad Sci 2006;
1074: 46677 42 Chang L, Grob CS, Ernst T, Itti L, Mishkin FS,
JoseMelchor R, Poland RE. Effect of ecstasy
[3,4methylenedioxymethamphetamine (MDMA)] on cerebral blood ow: a
co-registered SPECT and MRI study. Psychiatry Res 2000; 98: 1528 43
Ernst T, Chang L, Oropilla G, Gustavson A, Speck O. Cerebral
perfusion abnormalities in abstinent cocaine abusers: a perfusion
MRI and SPECT study. Psychiatry Res 2000; 99: 6374 44 Gottschalk
PC, Kosten TR. Cerebral perfusion defects in combined cocaine and
alcohol dependence. Drug Alcohol Depend 2002; 68: 95104 45 OLeary
DS, Block RI, Koeppel JA, Flaum M, Schultz SK, Andreasen NC, Boles
Ponto LL, Watkins GL, Hurtig RR, Hichwa RD. Effects of smoking
marijuana on brain perfusion and cognition. Neuropsychopharmacology
2002; 26: 80216 46 London ED, Cascella NG, Wong DF, Phillips RL,
Dannals RF, Links JM, Herning R, Grayson R, Jaffe JH, Wagner HN Jr.
Cocaine-induced reduction of glucose utilization in human brain.
Arch Gen Psychiatry 1990; 47: 567 74 47 Volkow ND, Fowler JS, Wolf
AP, Hitzemann R, Dewey S, Bendriem B, Alpert R, Hoff A. Changes in
brain glucose metabolism in cocaine dependence and withdrawal. Am J
Psychiatry 1991; 148: 6216 48 Licata SC, Renshaw PF. Neurochemistry
of drug action: insights from proton magnetic resonance
spectroscopic
49
50
51
52
53
54
55 56 57 58
59 60
61 62
63
imaging and their relevance to addiction. Ann N Y Acad Sci 2010;
1187: 14871 Alicata D, Chang L, Cloak C, Abe K, Ernst T. Higher
diffusion in striatum and lower fractional anisotropy in white
matter of methamphetamine users. Psychiatry Res Neuroimag 2009;
174: 18 Arnone D, Barrick TR, Chengappa S, Mackay CE, Clark CA,
Abou-Saleh MT. Corpus callosum damage in heavy marijuana use:
preliminary evidence from diffusion tensor tractography and
tract-based spatial statistics. Neuroimage 2008; 41: 106774 Liu H,
Li L, Hao Y, Cao D, Xu L, Rohrbaugh R, Xue Z, Hao W, Shan B, Liu Z.
Disrupted white matter integrity in heroin dependence: a controlled
study utilizing diffusion tensor imaging. Am J Drug Alcohol Abuse
2008; 34: 56274 Ma L, Hasan KM, Steinberg JL, Narayana PA, Lane SD,
Zuniga EA, Kramer LA, Moeller FG. Diffusion tensor imaging in
cocaine dependence: regional effects of cocaine on corpus callosum
and effect of cocaine administration route. Drug Alcohol Depend
2009; 104: 2627 Romero MJ, Asensio S, Palau C, Sanchez A, Romero
FJ. Cocaine addiction: diffusion tensor imaging study of the
inferior frontal and anterior cingulate white matter. Psychiatry
Res Neuroimag 2010; 181: 5763 Tobias MC, ONeill J, Hudkins M,
Bartzokis G, Dean AC, London ED. White-matter abnormalities in
brain during early abstinence from methamphetamine abuse.
Psychopharmacology (Berl) 2010; 209: 1324 Ashton CH. Pharmacology
and effects of cannabis: a brief review. Br J Psychiatry 2001; 178:
1016 Iversen L. Cannabis and the brain. Brain 2003; 126: 125279
Johns A. Psychiatric effects of cannabis. Br J Psychiatry 2001;
178: 11622 Nahas GG. The pharmacokinetics of THC in fat and brain:
resulting functional responses to marihuana smoking. Hum
Psychopharmacol Clin Exp 2001; 16: 24755 Ameri A. The effects of
cannabinoids on the brain. Prog Neurobiol 1999; 58: 31548 Howlett
AC, Barth F, Bonner TI, Cabral G, Casellas P, Devane WA, Felder CC,
Herkenham M, Mackie K, Martin BR, Mechoulam R, Pertwee RG.
Classication of cannabinoid receptors. Pharmacol Rev 2002; 54:
161202 Pertwee RG. Pharmacology of cannabinoid CB1 and CB2
receptors. Pharmacol Ther 1997; 74: 12980 Fride E. Endocannabinoids
in the central nervous system - an overview. Prostaglandins Leukot
Essent Fatty Acids 2002; 66: 22133 Glass M, Dragunow M, Faull RLM.
Cannabinoid receptors in the human brain: a detailed anatomical and
quantitative autoradiographic study in the fetal neonatal and adult
human brain. Neuroscience 1997; 77: 299318
2011 The Author Neuropathology and Applied Neurobiology 2011
British Neuropathological Society, 37, 118134
The neuropathology of drug abuse
129
64 Childers SR, Breivogel CS. Cannabis and endogenous
cannabinoid systems. Drug Alcohol Depend 1998; 51: 17387 65 Wilson
RI, Nicoll RA. Endocannabinoid signaling in the brain. Science
2002; 296: 67882 66 Herkenham M. Cannabinoid receptor localization
in brain: relationship to motor and reward systems. Ann N Y Acad
Sci 1992; 654: 1932 67 Mailleux P, Parmentier M, Vanderhaeghen J-J.
Distribution of cannabinoid receptor messenger RNA in the human
brain: an in situ hybridization histochemistry with
oligonucleotides. Neurosci Lett 1992; 143: 2004 68 Scallet AC.
Neurotoxicology of cannabis and THC: a review of chronic exposure
studies in animals. Pharmacol Biochem Behav 1991; 40: 6716 69
Campbell VA. Tetrahydrocannabinol-induced apoptosis of cultured
cortical neurones is associated with cytochrome c release and
caspase-3 activation. Neuropharmacology 2001; 40: 7029 70 Chan GCK,
Hinds TR, Impey S, Storm DR. Hippocampal neurotoxicity of
delta9-tetrahydrocannabinol. J Neurosci 1998; 18: 532232 71 Guzmn
M, Snchez C, Galve-Roperh I. Control of the cell survival/death
decision by cannabinoids. J Mol Med 2001; 78: 61325 72 Di Marzo V.
Regulation of endocannabinoid levels under physiological and
pathological conditions. A mini-review. Pharm Pharmacol Commun
2000; 6: 23541 73 Tanda G, Goldberg SR. Cannabinoids: reward,
dependence, and underlying neurochemical mechanisms - a review of
recent preclinical data. Psychopharmacology (Berl) 2003; 169: 11534
74 Barnes D, Palace J, OBrien MD. Stroke following marijuana
smoking. Stroke 1992; 23: 1381 75 Mateo I, Pinedo A,
Gomez-Beldarrain M, Basterretxea JM, Garcia-Monco JC. Recurrent
stroke associated with cannabis use. J Neurol Neurosurg Psychiatry
2005; 76: 4357 76 Mouzak A, Agathos P, Kerezoudi E, Mantas A,
VourdeliYiannakoura E. Transient ischemic attack in heavy cannabis
smokers - how safe is it? Eur Neurol 2000; 44: 424 77 Thanvi BR,
Treadwell SD. Cannabis and stroke: is there a link? Postgrad Med J
2009; 85: 803 78 Zachariah SB. Stroke after heavy marijuana
smoking. Stroke 1991; 22: 4069 79 DeLisi LE. The effect of cannabis
on the brain: can it cause brain anomalies that lead to increased
risk for schizophrenia? Curr Opin Psychiatry 2008; 21: 14050 80
Moore THM, Zammit S, Lingford-Hughes A, Barnes TRE, Jones PB, Burke
M, Lewis G. Cannabis use and risk of psychotic or affective mental
health outcomes: a systematic review. Lancet 2007; 370: 31928 81
Brust JCM. Opiate addiction and toxicity. In Handbook of Clinical
Neurology, Vol. 65: Intoxications of the Nervous
82
83
84
85
86 87
88
89
90
91
92
93
94
95
96
System, Part II. Eds PJ Vinkens, GW Bruyn, FA de Wolff.
Amsterdam: Elsevier, 1995; 34961 Ginsberg MD, Hedley-Whyte ET,
Richardson EP Jr. Hypoxic-ischemic leukoencephalopathy in man. Arch
Neurol 1976; 33: 514 Gosztonyi G, Schmidt V, Nickel R, Rothschild
MA, Camacho S, Siegel G, Zill E, Pauli G, Schneider V.
Neuropathologic analysis of postmortal brain samples of
HIV-seropositive and -seronegative i.v. drug addicts. Forensic Sci
Int 1993; 62: 1015 Oehmichen M, Meiner C, Reiter A, Birkholz M.
Neuropathology in non-human immunodeciency virus-infected drug
addicts: hypoxic brain damage after chronic intravenous drug abuse.
Acta Neuropathol 1996; 91: 6426 Pearson J, Richter RW. Addiction to
opiates: neurologic aspects. In Handbook of Clinical Neurology.
Intoxications of the Nervous System, Part II. Eds PJ Vinken, GW
Bruyn. Amsterdam: North-Holland Publishing Company, 1979; 365400
Protass LM. Delayed postanoxic encephalopathy after heroin use. Ann
Intern Med 1971; 74: 7389 Andersen SN, Skullerud K.
Hypoxic/ischaemic brain damage, especially pallidal lesions, in
heroin addicts. Forensic Sci Int 1999; 102: 519 Adle-Biassette H,
Marc B, Benhaiem-Sigaux N, Durigon M, Gray F. Infarctus crbraux
chez un toxicomane inhalant lhroine. Arch Anat Cytol Pathol 1996;
44: 1217 Brust JCM. Clinical, radiological, and pathological
aspects of cerebrovascular disease associated with drug abuse.
Stroke 1993; 24 (Suppl. I): I-129-33 Brust JCM, Richter RW. Stroke
associated with addiction to heroin. J Neurol Neurosurg Psychiatry
1976; 39: 1949 Caplan LR, Hier DB, Banks G. Current concepts of
cerebrovascular disease - stroke: stroke and drug abuse. Stroke
1982; 13: 86972 Kelly MA, Gorelick PB, Mirza D. The role of drugs
in the etiology of stroke. Clin Neuropharmacol 1992; 15: 24975
Sloan MA, Kittner SJ, Rigamonti D, Price TR. Occurrence of stroke
associated with use/abuse of drugs. Neurology 1991; 41: 135864
Weber M, Modemann S, Schipper P, Trauer H, Franke H, Illes P,
Geiger KD, Hengstler JG, Kleemann WJ. Increased polysialic acid
neural cell adhesion molecule expression in human hippocampus of
heroin addicts. Neuroscience 2006; 138: 121523 Gray F, Lescs MC,
Keohane C, Paraire F, Marc B, Durigon M, Gherardi R. Early brain
changes in HIV infection: neuropathological study of 11
seropositive, non-AIDS cases. J Neuropathol Exp Neurol 1992; 51:
177 85 Bell JE, Arango JC, Robertson R, Brettle RP, Leen C,
Simmonds P. HIV and drug misuse in the Edinburgh
2011 The Author Neuropathology and Applied Neurobiology 2011
British Neuropathological Society, 37, 118134
130
A. Bttner
97
98
99
100
101
102
103
104
105
106
107
108
109
110
cohort. J Acquir Immune Dec Syndr 2002; 31 (Suppl. 2): S3542
Adelman LS, Aronson SM. The neuropathologic complications of
narcotic drug addiction. Bull N Y Acad Med 1969; 45: 22534 McCreary
M, Emerman C, Hanna J, Simon J. Acute myelopathy following
intranasal insufation of heroin: a case report. Neurology 2000; 55:
31617 Pearson J, Richter RW, Baden MM, Challenor YB, Bruun B.
Transverse myelopathy as an illustration of the neurologic and
neuropathologic features of heroin addiction. Hum Pathol 1972; 3:
10713 Kriegstein AR, Armitage BA, Kim PY. Heroin inhalation and
progressive spongiform leukoencephalopathy. N Engl J Med 1997; 336:
58990 Rizzuto N, Morbin M, Ferrari S, Cavallaro T, Sparaco M, Boso
G, Gaetti L. Delayed spongiform leukoencephalopathy after heroin
abuse. Acta Neuropathol 1997; 94: 8790 Wolters EC, Stam FC,
Lousberg RJ, van Wijngaarden GK, Rengelink H, Schipper MEI,
Verbeeten B. Leucoencephalopathy after inhalating heroin
pyrolysate. Lancet 1982; 320: 12337 Gabilondo AM, Meana JJ,
Barturen F, Sastre M, GarcaSevilla JA. m-opioid receptor and
a2-adrenoreceptor agonist binding sites in the postmortem brain of
heroin addicts. Psychopharmacology (Berl) 1994; 115: 13540
Garca-Sevilla JA, Ventayol P, Busquets X, La Harpe R, Walzer C,
Guimn J. Regulation of immunolabelled mu-opioid receptors and
protein kinase C-alpha and zeta isoforms in the frontal cortex of
human opiate addicts. Neurosci Lett 1997; 226: 2932 Meana JJ,
Gonzlez-Maeso J, Garca-Sevilla JA, Guimn J. m-Opioid receptor and
a2-adrenoreceptor agonist stimulation of [35S]GTPgS binding to
G-proteins in postmortem brains of opioid addicts. Mol Psychiatry
2000; 5: 30815 Schmidt P, Schmolke C, Musshoff F, Menzen M,
Prohaska C, Madea B. Area-specic increased density of m-opioid
receptor immunoreactive neurons in the cerebral cortex of
drug-related fatalities. Forensic Sci Int 2003; 133: 20411
Hashimoto E, Frlich L, Ozawa H, Saito T, Shichinohe S, Takahata N,
Riederer P. Alteration of guanosine triphosphate binding proteins
in postmortem brains of heroin addicts. Alcohol Clin Exp Res 1996;
20: 301A4A Law PY, Wong YH, Loh HH. Molecular mechanisms and
regulation of opioid receptor signaling. Annu Rev Pharmacol Toxicol
2000; 40: 389430 Shichinohe S, Ozawa H, Hashimoto E, Tatschner T,
Riederer P, Saito T. Changes in the cAMP-related signal
transduction mechanism in postmortem human brains of heroin
addicts. J Neural Transm 2001; 108: 33547 Escrib PV, Sastre M,
Garca-Sevilla JA. Increased density of guanine nucleotide-binding
proteins in the
111
112
113
114
115
116
117
118
119 120 121 122 123
124
125
postmortem brains of heroin addicts. Arch Gen Psychiatry 1994;
51: 494501 Shichinohe S, Ozawa H, Saito T, Hashimoto E, Lang C,
Riederer P, Takahata N. Differential alteration of adenyl cyclase
subtypes I, II, and V/VI in postmortem human brains of heroin
addicts. Alcohol Clin Exp Res 1998; 22: 84S7S Lane-Ladd SB, Pineda
J, Boundy VA, Pfeuffer T, Krupinski J, Aghajanian GK, Nestler EJ.
CREB (cAMP response element-binding protein) in the locus
coeruleus: biochemical, physiological, and behavioral evidence for
a role in opiate dependence. J Neurosci 1997; 17: 7890 901 Ozaita
A, Escrib PV, Ventayol P, Murga C, Mayor F Jr, Garca-Sevilla JA.
Regulation of g protein-coupled receptor kinase 2 in brains of
opiate-treated rats and human opiate addicts. J Neurochem 1998; 70:
124957 Busquets X, Escrib PV, Sastre M, Garca-Sevilla JA. Loss of
protein kinase C-ab in brain of heroin addicts and
morphine-dependent rats. J Neurochem 1995; 64: 24752 Garca-Sevilla
JA, Ventayol P, Busquets X, La Harpe R, Walzer C, Guimn J. Marked
decrease of immunolabelled 68 kDa neurolament (NF-L) proteins in
brains of opiate addicts. Neuroreport 1997; 8: 156170 Kish SJ,
Kalasinsky KS, Derkach P, Schmunk GA, Guttman M, Ang L, Adams V,
Furukawa Y, Haycock JW. Striatal dopaminergic and serotonergic
markers in human heroin users. Neuropsychopharmacology 2001; 24:
5617 Gerostamoulos J, Burke MP, Drummer OH. Involvement of codeine
in drug-related deaths. Am J Forensic Med Pathol 1996; 17: 32735
Karch SB, Stephens BG. Toxicology and pathology of deaths related
to methadone: retrospective review. West J Med 2000; 172: 1114
Kintz P. A new series of 13 buprenorphine-related deaths. Clin
Biochem 2002; 35: 51316 Milroy CM, Forrest ARW. Methadone deaths: a
toxicological analysis. J Clin Pathol 2000; 53: 27781 Prakash A,
Das G. Cocaine and the nervous system. Int J Clin Pharmacol Ther
Toxicol 1993; 31: 57581 White SM, Lambe CJT. The pathophysiology of
cocaine abuse. J Clin Forensic Med 2003; 10: 2739 Biegon A, Dillon
K, Volkow ND, Hitzemann RJ, Fowler JS, Wolf AP. Quantitative
autoradiography of cocaine binding sites in human brain postmortem.
Synapse 1992; 10: 12630 Kalasinsky KS, Bosy TZ, Schmunk GA, Ang L,
Adams V, Gore SB, Smialek J, Furukawa Y, Guttman M, Kish SJ.
Regional distribution of cocaine in postmortem brain of chronic
human cocaine users. J Forensic Sci 2000; 45: 10418 McEvoy AW,
Kitchen ND, Thomas DGT. Intracerebral haemorrhage and drug abuse in
young adults. Br J Neurosurg 2000; 14: 44954
2011 The Author Neuropathology and Applied Neurobiology 2011
British Neuropathological Society, 37, 118134
The neuropathology of drug abuse
131
126 Petitti DB, Sidney S, Quesenberry C, Bernstein A. Stroke and
cocaine or amphetamine use. Epidemiology 1998; 9: 596600 127 Kaku
DA, Lowenstein DH. Emergence of recreational drug abuse as a major
risk factor for stroke in young adults. Ann Intern Med 1990; 113:
8217 128 Levine SR, Brust JCM, Futrell N, Brass LM, Blake D, Fayad
P, Schultz LR, Millikan CH, Ho K-L, Welch KMA. A comparative study
of the cerebrovascular complications of cocaine: alkaloidal versus
hydrochloride - a review. Neurology 1991; 41: 11737. 129 Davis GD,
Swalwell CI. The incidence of acute cocaine or methamphetamine
intoxication in deaths due to ruptured cerebral (berry) aneurysms.
J Forensic Sci 1996; 41: 6268 130 Fessler RD, Esshaki CM,
Stankewitz RC, Johnson RR, Diaz FG. The neurovascular complications
of cocaine. Surg Neurol 1997; 47: 33945 131 Konzen JP, Levine SR,
Garcia JH. Vasospasm and thrombus formation as possible mechanism
of stroke related to alkaloidal cocaine. Stroke 1995; 26: 1114 18
132 Mangiardi JR, Daras M, Geller ME, Weitzner I, Tuchman AJ.
Cocaine-related intracranial hemorrhage. Report of nine cases and
review. Acta Neurol Scand 1988; 77: 17780 133 Qureshi AI, Akbar MS,
Czander E, Safdar K, Janssen RS, Frankel MR. Crack cocaine use and
stroke in young patients. Neurology 1997; 48: 3415 134 Rajab R,
Stearns E, Baithun S. Autopsy pathology of cocaine users from the
Eastern district of London: a retrospective cohort study. J Clin
Pathol 2008; 61: 84850 135 Treadwell SD, Robinson TG. Cocaine use
and stroke. Postgrad Med J 2007; 83: 38994 136 Herning RI, King DE,
Better WE, Cadet JL. Neurovascular decits in cocaine abusers.
Neuropsychopharmacology 1999; 21: 11018 137 Kaufman MJ, Levin JM,
Ross MH, Lange N, Rose SL, Kukes TJ, Mendelson JH, Lukas SE, Cohen
BM, Renshaw PF. Cocaine-induced cerebral vasoconstriction detected
in humans with magnetic resonance angiography. JAMA 1998; 279:
37680 138 Schreiber MD, Madden JA, Covert RF, Torgerson LJ. Effects
of cocaine, benzoylecgonine, and cocaine metabolites on cannulated
pressurized fetal sheep cerebral arteries. J Appl Physiol 1994; 77:
8349 139 Jennings LK, White MM, Sauer CM, Mauer AM, Robertson JT.
Cocaine-induced platelets defects. Stroke 1993; 24: 13529 140
Kugelmass AD, Oda A, Monahan K, Cabral C, Ware JA. Activation of
human platelets by cocaine. Circulation 1993; 88: 87683 141 Nolte
KB, Brass LM, Fletterick CF. Intracranial hemorrhage associated
with cocaine abuse: a prospective autopsy study. Neurology 1996;
46: 12916.
142 Peterson PL, Roszler M, Jacob I, Wilner HI. Neurovascular
complications of cocaine abuse. J Neuropsychiatry Clin Neurosci
1991; 3: 1439 143 Vannemreddy P, Caldito G, Willis B, Nanda A.
Inuence of cocaine on ruptured intracranial aneurysms: a case
control study of poor prognostic indicators. J Neurosurg 2008; 108:
4706 144 Martin-Schild S, Albright KC, Hallevi H, Barreto AD,
Philip M, Misra V, Grotta JC, Savitz SI. Intracerebral hemorrhage
in cocaine users. Stroke 2010; 41: 6804 145 Oyesiku NM, Colohan
ART, Barrow DL, Reisner A (1993) Cocaine-induced aneurysmal
rupture: an emergent negative factor in the natural history of
intracranial aneurysms? Neurosurgery 1993; 32: 51826 146 Merkel PA,
Koroshetz WJ, Irizarry MC, Cudkowicz ME. Cocaine-associated
cerebral vasculitis. Semin Arthritis Rheum 1995; 25: 17283 147
Dez-Tejedor E, Frank A, Gutirrez M, Barreiro P. Encephalopathy and
biopsy-proven cerebrovascular inammatory changes in a cocaine
abuser. Eur J Neurol 1998; 5: 1037 148 Gan X, Zhang L, Berger O,
Stins MF, Way D, Taub DD, Chang SL, Kim KS, House SD, Weinand M,
Witte M, Graves MC, Fiala M. Cocaine enhances brain endothelial
adhesion molecules and leukocyte migration. Clin Immunol 1999; 91:
6876 149 Zhang L, Looney D, Taub D, Chang SL, Way D, Witte MH,
Graves MC, Fiala M. Cocaine opens the blood-brain barrier to HIV-1
invasion. J Neurovirol 1998; 4: 61926 150 Hurd YL, Herkenham M.
Molecular alterations in the neostriatum of human cocaine addicts.
Synapse 1993; 13: 35769 151 Little KY, Krolewski DM, Zhang L,
Cassin BJ. Loss of striatal vesicular monoamine transporter protein
(VMAT2) in human cocaine users. Am J Psychiatry 2003; 160: 4755 152
Little KY, McLaughlin DP, Zhang L, McFinton PR, Dalack GW, Cook EH
Jr, Cassin BJ, Watson SJ. Brain dopamine transporter messenger RNA
and binding sites in cocaine users: a postmortem study. Arch Gen
Psychiatry 1998; 55: 7939 153 Little KY, Patel UN, Clark TB, Butts
JD. Alterations of brain dopamine and serotonin levels in cocaine
users: a preliminary report. Am J Psychiatry 1996; 153: 121618 154
Little KY, Kirkman JA, Carroll FI, Clark TB, Duncan GE. Cocaine use
increases [3H]WIN 35428 binding sites in human striatum. Brain Res
1993; 628: 1725 155 Wilson JM, Levey AI, Bergeron C, Kalasinsky K,
Ang L, Peretti F, Adams VI, Smialek J, Anderson WR, Shannak K, Deck
J, Niznik HB, Kish SJ. Striatal dopamine, dopamine transporter, and
vesicular monoamine transporter in chronic cocaine users. Ann
Neurol 1996; 40: 428 39 156 Meador-Woodruff JH, Little KY, Damask
SP, Mansour A, Watson SJ. Effects of cocaine on dopamine receptor
gene
2011 The Author Neuropathology and Applied Neurobiology 2011
British Neuropathological Society, 37, 118134
132
A. Bttner
157
158
159
160
161
162
163
164
165
166
167 168
169
170
expression: a study in the postmortem human brain. Biol
Psychiatry 1993; 34: 34855 Mash DC, Pablo J, Ouyang Q, Hearn WL,
Itzenwasser S. Dopamine transport function is elevated in cocaine
users. J Neurochem 2002; 81: 292300 Segal DM, Moraes CT, Mash DC.
Up-regulation of D3 dopamine receptor mRNA in the nucleus accumbens
of human cocaine fatalities. Mol Brain Res 1997; 45: 3359 Staley
JK, Hearn WL, Ruttenber AJ, Wetli CV, Mash DC. High afnity cocaine
recognition sites on dopamine transporter are elevated in fatal
cocaine overdose victims. J Pharmacol Exp Ther 1994; 271: 167885
Bannon MJ, Pruetz B, Manning-Bog AB, Whitty CJ, Michelhaugh SK,
Sacchetti P, Granneman JG, Mash DC, Schmidt CJ. Decreased
expression of the transcription factor NURR1 in dopamine neurons of
cocaine abusers. Proc Natl Acad Sci USA 2002; 99: 63825 Mash DC,
Ouyang Q, Pablo J, Basile M, Itzenwasser S, Lieberman A, Perrin RJ.
Cocaine users have an overexpression of a-synuclein in dopamine
neurons. J Neurosci 2003; 23: 256472 Staley JK, Rothman RB, Rice
KC, Partilla J, Mash DC. k2 opioid receptors in limbic areas of the
human brain are upregulated by cocaine in fatal overdose victims. J
Neurosci 1997; 17: 822533 Tang W-X, Fasulo WH, Mash DC, Hemby SE.
Molecular proling of midbrain dopamine regions in cocaine overdose
victims. J Neurochem 2003; 85: 91124 Mash DC, Staley JK,
Itzenwasser S, Basile M, Ruttenber AJ. Serotonin transporters
upregulate with chronic cocaine use. J Chem Neuroanat 2000; 20:
27180 Ross BM, Moszczynska A, Peretti F, Adams V, Schmunk GA,
Kalasinsky KS, Ang L, Mamalis N, Turenne SD, Kish SJ. Decreased
activity of brain phospholipid metabolic enzymes in human users of
cocaine and methamphetamine. Drug Alcohol Depend 2002; 67: 739
Kalasinsky KS, Bosy TZ, Schmunk GA, Reiber G, Anthony RM, Furukawa
Y, Guttman M, Kish SJ. Regional distribution of methamphetamine in
autopsied brain of chronic methamphetamine users. Forensic Sci Int
2001; 116: 1639 Heye N, Hankey GJ. Amphetamine-associated stroke.
Cerebrovasc Dis 1996; 6: 14955 Karch SB, Stephens BG, Ho C-H.
Methamphetaminerelated deaths in San Francisco: demographic,
pathologic, and toxicologic proles. J Forensic Sci 1999; 44: 35968
Logan BK, Fligner CL, Haddix T. Cause and manner of death in
fatalities involving methamphetamine. J Forensic Sci 1998; 43: 2834
Moriya F, Hashimoto Y. A case of fatal hemorrhage in the cerebral
ventricles following intravenous use of methamphetamine. Forensic
Sci Int 2002; 129: 104 9
171 Yen DJ, Wang SJ, Ju TH, Chen CC, Liao KK, Fuh JL, Hu HH.
Stroke associated with methamphetamine inhalation. Eur J Neurol
1994; 34: 1622 172 Zhu BL, Oritani S, Shimotouge K, Ishida K, Quan
L, Fujita MQ, Ogawa M, Maeda H. Methamphetaminerelated fatalities
in forensic autopsy during 5 years in southern half of Osaka city
and surrounding areas. Forensic Sci Int 2000; 113: 4437 173 Lee YW,
Hennig B, Yao J, Toborek M. Methamphetamine induces AP-1 and
NF-kappaB binding and transactivation in human brain endothelial
cells. J Neurosci Res 2001; 66: 58391 174 Brown JM, Hanson GR,
Fleckenstein AE. Methamphetamine rapidly decreases vesicular
dopamine uptake. J Neurochem 2000; 74: 22213 175 Davidson C, Gow
AJ, Lee TH, Ellinwood EH. Methamphetamine neurotoxicity: necrotic
and apoptotic mechanisms and relevance to human abuse and
treatment. Brain Res Brain Res Rev 2001; 36: 122 176 Frost DO,
Cadet JL. Effects of methamphetamineinduced neurotoxicity on the
development of neural circuits: a hypothesis. Brain Res Brain Res
Rev 2000; 34: 10318 177 Harvey DC, Lacan G, Tanious SP, Melega WP.
Recovery from methamphetamine induced long-term nigrostriatal
dopaminergic decits without substantia nigra cell loss. Brain Res
2000; 871: 25970 178 Seiden LS, Sabol KE. Methamphetamine and
methylenedioxymethamphetamine neurotoxicity: possible mechanisms of
cell destruction. NIDA Res Monogr 1996; 163: 25176 179 Sekine Y,
Ouchi Y, Takei N, Yoshikawa E, Nakamura K, Futatsubashi M, Okada H,
Minabe Y, Suzuki K, Iwata Y, Tsuchiya KJ, Tsukada H, Iyo M, Mori N.
Brain serotonin transporter density and aggression in abstinent
methamphetamine abusers. Arch Gen Psychiatry 2006; 63: 90100 180
Tong J, Ross BM, Schmunk GA, Peretti FJ, Kalasinsky KS, Furukawa Y,
Ang L-C, Aiken SS, Wickham DJ, Kish SJ. Decreased striatal dopamine
D1 receptor-stimulated adenylyl cyclase activity in human
methamphetamine users. Am J Psychiatry 2003; 160: 896903 181 Volkow
ND, Chang L, Wang G-J, Fowler JS, Leonido-Yee M, Franceschi D,
Sedler MJ, Gatley SJ, Hitzemann R, Ding Y-S. Association of
dopamine transporter reduction with psychomotor impairment in
methamphetamine abusers. Am J Psychiatry 2001; 158: 37782 182
Guilarte TR. Is methamphetamine abuse a risk factor in
parkinsonism? Neurotoxicology 2001; 22: 72531 183 Thrash B,
Thiruchelvan K, Ahuja M, Suppiramaniam V, Dhanasekaran M.
Methamphetamine-induced neurotoxicity: the road to Parkinsons
disease. Pharmacol Rep 2009; 61: 96677 184 Wilson JM, Kalasinsky
KS, Levey AI, Bergeron C, Reiber G, Anthony RM, Schmunk GA, Shannak
K, Haycock JW, Kish SJ. Striatal dopamine nerve terminal
markers
2011 The Author Neuropathology and Applied Neurobiology 2011
British Neuropathological Society, 37, 118134
The neuropathology of drug abuse
133
185
186
187
188
189
190 191
192
193
194
195
196
197
198
199
in human, chronic methamphetamine users. Nat Med 1996; 2: 699703
Cadet JL, Krasnova IN. Molecular bases of methamphetamine-induced
neurodegeneration. Int Rev Neurobiol 2009; 88: 10119 Christophersen
AS. Amphetamine designer drugs an overview and epidemiology.
Toxicol Lett 2000; 112: 12731 Parrott AC. Is ecstasy MDMA? A review
of the proportion of ecstasy tablets containing MDMA, their dosage
levels, and the changing perceptions of purity. Psychopharmacology
(Berl) 2004; 173: 23441 De la Torre R, Farre M, Roset PN, Pizarro
N, Abanades S, Segura M, Segura J, Cami J. Human pharmacology of
MDMA: pharmacokinetics, metabolism and disposition. Ther Drug Monit
2004; 26: 137447 Huether G, Zhou D, Rther E. Causes and
consequences of the loss of serotonergic presynapses elicited by
the consumption of 3,4-methylenedioxy methamphetamine (MDMA,
ecstasy) and its congeners. J Neural Transm 1997; 104: 77194 Kalant
H. The pharmacology and toxicology of ecstasy (MDMA) and related
drugs. CMAJ 2001; 165: 91728 McKenna DJ, Peroutka SJ.
Neurochemistry and neurotoxicity of
3,4-methylenedioxymethamphetamine (MDMA, ecstasy). J Neurochem
1990; 54: 1422 De Letter EA, Espeel M, Craeymeersch M, Lambert WE,
Clauwaert K, Dams R, Mortier KA, Piette M. Immunohistochemical
demonstration of the amphetamine derivatives
3,4-methylenedioxymethamphetamine (MDMA) and
3,4-methylenedioxyamphetamine (MDA) in human post-mortem brain
tissues and the pituitary gland. Int J Legal Med 2003; 117: 29
Fineschi V, Centini F, Mazzeo E, Turillazzi E. Adam (MDMA) and Eve
(MDEA) misuse: an immunohistochemical study on three fatal cases.
Forensic Sci Int 1999; 104: 6574 Gill JR, Hayes JA, deSouza IS,
Marker E, Stajic M. Ecstasy (MDMA) deaths in New York City: a case
series and review of the literature. J Forensic Sci 2002; 47: 121 6
Henry JA, Jeffreys KJ, Dawling S. Toxicity and deaths from
3,4-methylenedioxymethamphetamine (ecstasy). Lancet 1992; 340: 3847
Milroy CM, Clark JC, Forrest ARW. Pathology of deaths associated
with ecstasy and eve misuse. J Clin Pathol 1996; 49: 14953 Bertram
M, Egelhoff T, Schwarz S, Schwab S. Toxic leukoencephalopathy
following ecstasy ingestion. J Neurol 1999; 246: 61718 Bitsch A,
Thiel A, Rieckmann P, Prange H. Acute inammatory CNS disease after
MDMA (ecstasy). Eur Neurol 1996; 36: 3289 Gledhill JA, Moore DF,
Bell D, Henry JA. Subarachnoid haemorrhage associated with MDMA
abuse. J Neurol Neurosurg Psychiatry 1993; 56: 10367
200 Hanyu S, Ikeguchi K, Imai H, Imai N, Yoshida M. Cerebral
infarction associated with 3,4methylenedioxymethamphetamine
(ecstasy) abuse. Eur Neurol 1995; 35: 173 201 Harries DP, De Silva
R. Ecstasy and intracerebral haemorrhage. Scott Med J 1992; 37:
1502 202 Hughes JC, McCabe M, Evans RJ. Intracranial haemorrhage
associated with ingestion of ecstasy. Arch Emerg Med 1993; 10: 3724
203 Manchanda S, Connolly MJ. Cerebral infarction in association
with ecstasy abuse. Postgrad Med J 1993; 69: 8745 204 Spatt J,
Glawar B, Mamoli B. A pure amnestic syndrome after MDMA (ecstasy)
ingestion. J Neurol Neurosurg Psychiatry 1997; 62: 41819 205 Squier
MV, Jalloh S, Hilton-Jones D, Series H. Death after ecstasy
ingestion: neuropathological ndings. J Neurol Neurosurg Psychiatry
1995; 58: 756 206 Commins DL, Vosmer G, Virus RM, Woolverton WL,
Schuster CR, Seiden LS. Biochemical and histological evidence that
methylenedioxymethamphetamine (MDMA) is toxic to neurons in the rat
brain. J Pharmacol Exp Ther 1987; 241: 33845 207 Ricaurte GA,
McCann UD, Szabo Z, Scheffel U. Toxicodynamics and long-term
toxicity of the recreational drug,
3,4-methylenedioxymethamphetamine (MDMA, ecstasy). Toxicol Lett
2000; 112: 1436 208 Curran HV. Is MDMA (ecstasy) neurotoxic in
humans? An overview of evidence and of methodological problems in
research. Neuropsychobiology 2000; 42: 34 41 209 Lyles J, Cadet JL.
Methylenedioxymethamphetamine (MDMA, ecstasy) neurotoxicity:
cellular and molecular mechanisms. Brain Res Brain Res Rev 2003;
42: 15568 210 Sprague JE, Everman SL, Nichols DE. An integrated
hypothesis for the serotonergic axonal loss induced by
3,4-methylenedioxymethamphetamine. Neurotoxicology 1998; 19: 42742
211 Simantov R, Tauber M. The abused drug MDMA (ecstasy) induces
programmed cell death of human serotonergic cells. FASEB J 1997;
11: 1416 212 Zhou JF, Chen P, Zhou YH, Zhang L, Chen HH.
3,4Methylenedioxymethamphetamine (MDMA) abuse may cause oxidative
stress and potential free radical damage. Free Radic Res 2003; 37:
4917 213 Gouzoulis-Mayfrank E, Daumann J. Neurotoxicity of
methylenedioxyamphetamines (MDMA; ecstasy) in humans: how strong is
the evidence for persistent brain damage? Addiction 2006; 101:
34861 214 Kish SJ. How strong is the evidence that brain serotonin
neurons are damaged in human users of ecstasy? Pharmacol Biochem
Behav 2002; 71: 84555 215 McGuire P. Long term psychiatric and
cognitive effects of MDMA use. Toxicol Lett 2000; 112113: 1536 216
Parrott AC, Marsden CA. MDMA (3,4methylenedioxymethamphetamine) or
ecstasy: the
2011 The Author Neuropathology and Applied Neurobiology 2011
British Neuropathological Society, 37, 118134
134
A. Bttner
217
218
219
220
221
222
223
224
225
226
227
228
contemporary human and animal research perspective. J
Psychopharmacol 2006; 20: 1436 Parrott AC. Human psychopharmacology
of ecstasy (MDMA): a review of 15 years of empirical research. Hum
Psychopharmacol Clin Exp 2001; 16: 55777 Reneman L, Booij J, Majoie
CBL, van den Brink W, den Heeten GJ. Investigating the potential
neurotoxicity of ecstasy (MDMA): an imaging approach. Hum
Psychopharmacol Clin Exp 2001; 16: 57988 Verbaten MN. Specic memory
decits in ecstasy users? The results of a meta-analysis. Hum
Psychopharmacol Clin Exp 2003; 18: 28190 Makrigeorgi-Butera M,
Hagel C, Laas R, Pschel K, Stavrou D. Comparative brain pathology
of HIVseronegative and HIV-infected drug addicts. Clin Neuropathol
1996; 15: 3249 Boronat MA, Garca-Fuster MJ, Garca-Sevilla JA.
Chronic morphine induces up-regulation of the proapoptotic Fas
receptor and down-regulation of the antiapoptotic Bcl-2 oncoprotein
in rat brain. Br J Pharmacol 2001; 134: 126370 Hu S, Sheng WS,
Lokensgard JR, Peterson PK. Morphine induces apoptosis of human
microglia and neurons. Neuropharmacology 2002; 42: 82936 Jiang Y,
Yang W, Zhou Y, Ma L. Up-regulation of murine double minute clone 2
(MDM2) gene expression in rat brain after morphine, heroin, and
cocaine administrations. Neurosci Lett 2003; 352: 21620 Mao J, Sung
M, Ji R-R, Lim G. Neuronal apoptosis associated with morphine
tolerance: evidence for an opioidinduced neurotoxic mechanism. J
Neurosci 2002; 22: 765061 Stumm G, Schlegel J, Schfer T, Wrz C,
Mennel HD, Krieg J-C, Vedder H. Amphetamines induce apoptosis and
regulation of bcl-x splice variants in neocortical neurons. FASEB J
1999; 13: 106572 Boronat MA, Olmos G, Garca-Sevilla JA. Attenuation
of tolerance to opioid-induced antinociception and protection
against morphine-induced decrease of neurolament proteins by
idazoxan and other I2-imidazoline ligands. Br J Pharmacol 1998;
125: 17585 Ferrer-Alcn M, Garca-Sevilla JA, Jaquet PE, La Harpe R,
Riederer BM, Walzer C, Guimn J. Regulation of nonphosphorylated and
phosphorylated forms of neurolament proteins in the prefrontal
cortex of human opioid addicts. J Neurosci Res 2000; 61: 33849
Ramage SN, Anthony IC, Carnie FW, Busuttil A, Robertson R, Bell JE.
Hyperphosphorylated tau and amyloid precursor protein deposition is
increased in the brains of
229
230
231
232 233
234
235
236
237
238
239
240
young drug abusers. Neuropathol Appl Neurobiol 2005; 31: 43948
Bttner A, Rohrmoser K, Mall G, Penning R, Weis S. Widespread axonal
damage in the brain of drug abusers as evidenced by accumulation of
b-amyloid precursor protein (b-APP): an immunohistochemical
investigation. Addiction 2006; 101: 133946 Anthony IC, Ramage SN,
Carnie FW, Simmonds P, Bell JE. Does drug abuse alter microglial
phenotype and cell turnover in the context of advancing HIV
infection? Neuropathol Appl Neurobiol 2005; 31: 32538. Tomlinson
GS, Simmonds P, Busuttil A, Chiswick A, Bell JE. Upregulation of
microglia in drug users with and without pre-symptomatic HIV
infection. Neuropathol Appl Neurobiol 1999; 25: 36979
Miguel-Hidalgo JJ. The role of glial cells in drug abuse. Curr Drug
Abuse Rev 2009; 2: 7682 Sorensen RG, Lawrence DMP. Glial cells and
drugs of abuse in the nervous system. Drug Alcohol Depend 2009;
102: 1669 Anderson CE, Tomlinson GS, Pauly B, Brannan FW, Chiswick
A, Brack-Werner R, Simmonds P, Bell JE. Relationship of
Nef-positive and GFAP-reactive astrocytes to drug use in early and
late HIV infection. Neuropathol Appl Neurobiol 2003; 29: 37888
Stadlin A, Lau JWS, Szeto YK. A selective regional response of
cultured astrocytes to methamphetamine. Ann N Y Acad Sci 1998; 844:
10821 Castagnoli N Jr, Castagnoli KP. Metabolic bioactivation
reactions potentially related to drug toxicities. NIDA Res Monogr
1997; 173: 85105 Sastre M, Ventayol P, Garca-Sevilla JA. Decreased
density of I2-imidazoline receptors in the postmortem brains of
heroin addicts. Neuroreport 1996; 7: 50912 Connor MD, Lammie GA,
Bell JE, Warlow CP, Simmonds P, Brettle RP. Cerebral infarction in
adult AIDS patients: observations from the Edinburgh HIV autopsy
cohort. Stroke 2000; 31: 211726 Bttner A, Kroehling C, Mall G,
Penning R, Weis S. Alterations of the vascular basal lamina in the
cerebral cortex in drug abuse: a combined morphometric and
immunohistochemical investigation. Drug Alcohol Depend 2005; 69:
6379 Geibprasert S, Gallucci M, Krings T. Addictive illegal drugs:
structural neuroimaging. AJNR Am J Neuroradiol 2010; 31: 8038
Received 26 July 2010 Accepted after revision 30 September 2010
Published online Article Accepted on 6 October 2010
2011 The Author Neuropathology and Applied Neurobiology 2011
British Neuropathological Society, 37, 118134