Embed Size (px)
Citation preview

Proc. Natl. Acad. Sci. USAVol. 92, pp. 8552-8559, September 1995
Review
Genetic dissection of Alzheimer disease, a heterogeneous disorder(amyloid precursor protein/chromosome 14/apolipoprotein E/Volga Germans)
Gerard D. SchellenbergGeriatric Research Education and Clinical Center (182B), Seattle Veterans Affairs Medical Center, 1660 South Colombian Way, Seattle, WA 98108-1597
ABSTRACT The genetics of Alzhei-mer disease (AD) are complex and notcompletely understood. Mutations in theamyloid precursor protein gene (APP) cancause early-onset autosomal dominantAD. In vitro studies indicate that cellsexpressing mutant APPs overproducepathogenic forms of the Al8 peptide, themajor component of AD amyloid. How-ever, mutations in the APP gene are re-sponsible for 5% or less of all early-onsetfamilial AD. A locus on chromosome 14 isresponsible for AD in other early-onsetAD families and represents the most se-vere form of the disease in terms of age ofonset and rate of decline. Attempts toidentify the AD3 gene by positional clon-ing methods are underway. At least oneadditional early-onset AD locus remainsto be located. In late-onset AD, the apo-lipoprotein E gene allele e4 is a risk factorfor AD. This allele appears to act as adose-dependent age-of-onset modifier.The e2 allele of this gene may be protec-tive. Other late-onset susceptibility fac-tors remain to be identified.
Alzheimer disease (AD) is a devastatingneurodegenerative disorder first recog-nized in 1907 by Alois Alzheimer (1).Though initially described in a 51-year-oldwoman, AD is now recognized as a com-mon disease in the elderly and is thepredominant cause of dementia in peopleover 65 years of age. Clinical symptomstypically begin with subtle short-termmemory problems. As the diseaseprogresses, difficulty with memory, lan-guage, and orientation worsen to the pointof interfering with the ability of the per-son to function independently. Thoughthe pattern and rate of cognitive lossvaries, a common feature of the diseaseis continuous progression until virtuallyall cognitive function is lost. Duration ofAD from first symptoms of memory lossuntil death is, on average, 10 years butcan span from 5 years to more than 20years. Death occurs from secondarycauses such as aspiration pneumonia.The pathology in AD is confined to the
central nervous system. The predominantfeatures are amyloid deposits and neuro-fibrillary tangles (NFTs). Amyloid is as-sociated with the vascular system of thecentral nervous system and is found asfocal deposits in the parenchyma. The
major component in this amyloid is ahighly hydrophobic peptide called the AP3peptide, which ranges in length from 39 to43 amino acids. This peptide was firstpartially sequenced in 1984 (2) in materialpurified from vascular amyloid deposits.Subsequent work showed that plaqueamyloid contained the same peptide, butwith an extended C terminus (3). The AP3peptide aggregates into antiparallel fila-ments in a (3-pleated sheet structure thatresults in the birefringent nature of amy-.loid in the presence of Congo red andpolarized light. Surrounding many plaquesare dystrophic neurites, which are nerveendings containing abnormal filamentousand membranous structures. Activated as-trocytes and microglial cells also surroundplaques. NFTs consist of abnormal pairedhelical filaments bundled together in neu-ronal cell bodies. "Ghost" NFTs are alsoobserved that presumably mark the loca-tion of dead neurons. Other features in-clude granulovacuolar changes, Hiranobodies, neuronal loss, gliosis, and the vari-able presence of Lewy bodies.
In the AD brain, the destructive processis evident on a gross level. Late in thedisease, ventricular enlargement andshrinkage of the brain occurs, but withsparing of the motor strip. Microscopi-cally, extensive gliosis and neuronal lossare observed. Thus, the pathology seen atautopsy is the end-point of a lengthy dis-ease process, far removed from the initi-ating events ofAD. Also, the types of cellsremaining at death are different fromthose of a normal brain, with neuronsmissing that were possibly involved in ini-tiating events. Other cell types such as theactivated microglial cells and astrocyteshave gene expression patterns not ob-served in the normal brain (4). Thus,attempts using biochemical methods toidentify key proteins and genes involved indisease initiation are hampered by the factthat it is not possible to actually observethese critical in vivo events. Rather, bio-chemical dissection of the AD brain atautopsy is akin to molecular archaeology,attempting to reconstruct the pathogenicpathway studying the end-stage diseasebrain. Genetic mapping and positionalcloning approaches to identifying AD genesare attractive because these methods donot rely on a comprehensive understand-ing of pathogenesis but, rather, require
8552
accurate diagnosis of the disease in famil-ial forms of AD. When genes harboringAD mutations are identified, the proteinproducts of these genes must be critical toinitiating events of pathogenesis.
The Amyloid Precursor Protein Gene(APP) and Familial AD (FAD)
TheAPP Gene. The first genetic defectsleading to AD were identified in theAPPgene. Sequences encoding APP were firstcloned (5) by screening cDNA librarieswith oligonucleotide probes deduced fromthe AP3 peptide sequence. The initial full-length cDNA clone identified encoded a695-amino acid protein (APP695) that con-tained, near its C-terminal end, the Af3peptide sequence (Fig. 1). Subsequentwork showed that the APP gene has 19exons (6) and that the A,B peptide isencoded by parts of exons 16 and 17 (6)(exon and codon numbering based on theAPP770 splice variant). A number ofAPPtranscripts have been described in which(exons 7, 8, and 15 are alternativelyspliced. Exon 7 encodes 57 amino acidswith homology to the Kunitz-type pro-tease inhibitor (KPI) domain (7-9), andexon 8 encodes 19 amino acids with ho-mology to the MRC OX-2 antigen (9). Inneurons, the predominant transcript isAPP695 (10), which contains exon 15 butnot exons 7 and 8. The major transcripts inperipheral tissues encode KPI-containingforms ofAPP (APP7s5 and APP770; refs. 7-9and 11). Other splice variants have beenobserved that are missing exon 15 in variouscombinations with exons 7 and 8 and arereferred to as L-APPs (11, 12). While all ofthe above-mentioned splice variants containAP3 sequences, two additional rare tran-scripts, APP365 and APP563, have been iden-tified that lack A,B-encoding sequences (13,14). Other genes have been identified thatare homologous toAPP (15-17). These ho-mologues, calledAPLP andAPLP2, do notcontain the A,B peptide and thus cannot beprocessed to produce A,B.
Abbreviations: I3PP, amyloid precursor protein;AD, Alzheimer disease; APP, amyloid precur-sor protein gene; apoE, apolipoprotein E;FAD, familial AD; HCHWA-D, hereditary ce-rebral hemorrhage with amyloidosis, Dutchtype; lod, logarithm of odds; NFT, neurofibril-lary tangle; STRP, short -tandem repeat poly-morphism; VG, Volga German.
Dow
nloa
ded
by g
uest
on
Apr
il 24
, 202
1

Proc. Natl. Acad. Sci. USA 92 (1995) 8553
{}- COOH
15 16 17exons
signal peptide negatively charged AO3 peptide
III cysteine-rich transmembrane domain
B
-Asp-Leu-
t-Lys-Met-
670 671
ecrtase st,3-secretase ct-secretase
-Gly- -Gln-
-Ala-Glu-692 693
-Gly--Phe--lie-
-Val-71 7
A 3 peptide
,Y-secretase
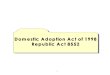
FIG. 1. APP gene structure. (A) The APP695 splice variant is shown along with the locationof alternatively spliced exons 7, 8, and 15. (B) The A,B region of theAPP gene is shown as the thickbox with pathogenic mutations for AD, hereditary cerebral hemorrhage with amyloidosis, Dutchtype (HCHWA-D), and cerebral vascular/dementia disease.
APP Mutations. When the APP genewas first cloned, it was mapped to thecentromeric region of chromosome 21 (5,18, 19). Simultaneously, suggestive posi-tive results were reported for linkage ofAD in four early-onset autosomal domi-nant families to centromeric chromosome21 markers in the vicinity of theAPP gene(19). Chromosome 21 had also been pre-viously implicated in AD because allDown syndrome subjects (trisomy 21) au-
topsied at 40 years or older have AD-typeamyloid plaques and NFTs (20). Thesecombined observations madeAPP a com-pelling candidate gene for early-onsetFAD. However, recombinants betweenAPP and the FAD gene were observed ina number of large FAD kindreds (21, 22),including those used in the original chro-mosome 21 linkage study (19). The pres-ence of obligate recombinants in early-onset FAD kindreds and negative linkageresults obtained from large collections ofboth early and late-onset families usinggenetic markers surroundingAPP (23-25)correctly showed that mutations in APPwere not responsible for AD in most kin-dreds. The positive linkage results wereinterpreted as evidence for a second ADlocus on chromosome 21, located betweenthe APP gene and the centromere.The first pathogenicAPP mutation was
found in a kindred with autosomal dom-inant HCHWA-D. In this disease, strokesoccur after age 25 with death coming bythe sixth decade of life. The disease is
accompanied by cerebral amyloid angiop-athy consisting of the AD AP3 peptide (26).Few AD-type amyloid plaques and NFTsare found on autopsy. Genetic analysis ofHCHWA-D families with polymorphicsites within theAPP gene yielded stronglypositive linkage results with a maximumlogarithm of odds (lod) score (Zmax) of7.59 at a recombination fraction (0) of 0.0(27). A mutation cosegregating withHCHWA-D was identified at APP codon693 in exon 17 (Fig. 1) (28) that results ina Glu -> Gln substitution. This site is at
amino acid 22 of the AP peptide. Thissubstitution has not been observed in a
large number of controls (e.g., ref. 29).Identification of the HCHWA-D muta-tion was the first demonstration that anAPP mutation could result in amyloiddeposition and neurologic disease.
Despite the evidence that APP muta-tions could not account for most AD,several early-onset autosomal dominantkindreds had been analyzed for which theAPP gene could not be excluded as theADlocus (30). DNA sequence analysis of exon17 of theAPP gene in two of these familiesrevealed a mutation at codon 717, result-ing in a Val -> Ile substitution 3 residuesbeyond amino acid 43 of the AP peptide(ref. 31 and Fig. 1). This mutation hassubsequently been identified in a numberofFAD families of different ethnic origins(32-36) but not in a large number ofcontrols, most other early-onset kindreds,and both FAD and "sporadic" late-onset
AD patients (29, 31, 37, 38). (The termsporadic is used here to indicate AD sub-jects with no family history of AD anddoes not necessarily imply a nongeneticetiology.) Subsequently, two other pointmutations at codon 717 were identified,each in a single family (39, 40). One resultsin Phe-717 (39), and the other results inGly-717 (40). A double mutation has beenidentified in a Swedish pedigree at codons670 and 671 resulting in Asn-Leu in placeof the normal Lys-Met (41). These muta-tions are in exon 16 of the APP gene andencode the 2 amino acids immediatelypreceding the beginning of the A,B se-quence. Another pathogenic APP muta-tion has been identified in a Dutch familywith both cerebral hemorrhage diseaseand presenile dementia (42). This muta-tion, also in the A,3 region, is at codon 692and results in a Gly -> Ala replacement.The disease in this family is a variant ofboth HCHWA-D disease and AD. Ex-haustive screening of other early-onsetAD, late-onset FAD, and sporadic ADpatients and a large number of controlshas been performed for each of thesemutations (29, 37, 38, 43), and all are onlyrarely observed in dementia pedigrees andhave never been seen in controls. Thus,these are clearly pathogenic causative mu-tations.The clinical, neuropathologic, and ge-
netic characteristics of AD observed insubjects with APP mutations have severalfeatures in common. (i) Onset of AD isearly. In Ile-717 subjects, the age of onsetranges from 41 to 64 years, with familyage-of-onset means ranging from 48 to 55years (32, 34, 44, 45). For the Gly-717 kin-dred, the onset mean is 59 years (range,40-67 years) (40, 46). In the Phe-717family, the onset mean is 43 years (range,39-51 years) (47). For the Asn-670/Leu-671 mutation, the family onset mean is 55years (range, 45-61 years) (48). (ii) Inher-itance is dominant with complete pen-etrance by the early 60s; noAPP mutationcarrier past the age of 67 years has beenreported. (iii) Other than the age of onset,the clinical and neuropathologic featuresof AD in these families are not differentfrom AD in non-APP mutation subjects.APP Mutations and AD Pathogenesis.
The location of the pathogenic APP mu-tations is intriguing because all are locatedwithin or flanking the Af3 peptide regionof the amyloid precursor protein P3PP andhence may affect proteolytic processing ofthe protein (Fig. 1). Two normal proteo-lytic pathways for f3PP processing havebeen identified. A constitutive secretorypathway involves cleavage at AP aminoacid 16 (49,50), an event that results in therelease of a large soluble ,BPP derivativeand retention of a 8.7-kDa membrane-bound peptide. This endoproteolytic pro-cess destroys the Af peptide and, thus,cannot contribute to A,B and amyloid gen-eration. The protease that performs this
A
695 NH2*2:7I7::::: }
CHO CHO
_-.I
-U-exon 7 exon 8
Review: Schellenberg
Dow
nloa
ded
by g
uest
on
Apr
il 24
, 202
1

Proc. Natl. Acad. Sci. USA 92 (1995)
cleavage, referred to as a-secretase, hasnot been identified. Initially, the a-secre-tase pathway was thought to representnormal processing and the production ofintact AP3 was thought to be a diseaseprocess. Subsequent work in a variety ofsystems has now shown that normal cellscan produce intact AP3 (51-53). Moreover,the detection of A,B in normal cerebralspinal fluid (51, 52) demonstrates that A,Bis produced in the absence of disease. Theproteolytic activities responsible for A,Bproduction are called ,B-secretase andy-secretase (Fig. 1).The location of FAD mutations imme-
diately upstream of the N-terminal aminoacid and downstream of the C terminus ofAP3 suggests that these mutations couldinfluence 3- and y-secretase-mediated,BPP processing. The effects of both theAsn-670/Leu-671 and the position 717mutations on ,BPP processing have beenexamined. In vitro transfection experi-ments have shown that cells transfectedwith APP constructs with the Asn-670/Leu-671 mutation secrete 5- to 8-foldmore AP3 compared to cells transfectedwith the wild-type APP cDNA (54, 55).Also, fibroblast cultures from subjects car-rying this mutation secreted 3-fold moreAP3 than control fibroblasts. This increasein secretion was found in cultures fromaffected and from presymptomatic carri-ers (56). Similar transfection experimentswith the Ile-717 and Phe-717 mutations donot show an increased level of AP3 secre-tion relative to the normal APP sequence.However, in the cells transfected withmutant forms, the ratio of "long" AP3 [e.g.,A,3-(1-42)] to A,3-(1-40) is increased (57,58). The longer peptides form amyloidfibrils more rapidly than A,3-(1-40) andthus are postulated to be more pathogenic(59-61). The Gly-692 mutation, which lieswithin the A,B sequence, also appears toalter O3PP processing; A,B production wasincreased by a factor of 2 (62). Identifica-tion of the proteases responsible for thea-, ,3-, and y-secretase cleavages is essen-tial to testing the hypothesis that theAPPmutations influence O3PP processing.
The Chromosome 14 FAD Locus (AD3)
Identification of a second AD locus wasachieved by a purely genetic approach, agenome scanning strategy using geneticmarkers scattered on all chromosomes(63). The families selected for analysis hadfamily onset means of 52 years or younger(Table 1) and clear autosomal dominantinheritance of AD. In these families, thechromosome 19 region of theAPOE gene(68) and the chromosome 21 APP gene(29) had been excluded as the cause ofAD. This second locus, called AD3, wasinitially detected using the short tandemrepeat polymorphism (STRP) markerD14S43 (63). Evidence for linkage camefrom 9 families with a Zm,a combined lod
Table 1. Early-onset FAD kindreds
Family
Chromosome 14 kindredsFinnish kindredLLH/603Torl.1FAD1FAD2FAD3/SNWFAD4Japanese kindredAD/AAD/B
Volga German (VG) kindredsHHBHDKSRw
Age of onset, years
36 ± 3 (n = 6; 32-39)42 ± 4.6 (n = 16; 30-48)48 ± 6.5 (n = 18; 37-68)
4352 ± 6.23 (n = 25)48.7 ± 5.3 (n = 12)52 ± 2.5 (n = 7; 48-56)39.9 ± 7.18
47.833 ± 434 ± 2
59.5 ± 3.960.8 ± 7.159.6 ± 10.364.8 ± 5.450.2 ± 7.359.2 ± 10.5
(n = 6; 56-68)(n = 22; 54-75)(n = 17; 46-82)(n = 13; 55-71)(n = 17; 40-67)(n = 5; 48-79)
Ref(s).
6463
63, 6565
19, 6519, 6563, 6519, 6566
22, 6722, 67
636363636363
All families listed under chromosome 14 have yielded Zma: values .3.0 with chromosome 14markers in the AD3 region. Age of onset data are the mean ± SD. The number of subjects (n)and range of the age of onset in years are in parentheses.
score of 9.01 (0 = 0.01). One family(family L) gave independent evidence forlinkage with a Zma of 4.89 (0 = 0).Subsequently, the existence of a chromo-some 14 AD locus was confirmed in otherearly-onset non-APP families (64-67, 69,70). To date, a total of 11 families havebeen reported in which independent evi-dence for linkage to chromosome 14markers was observed (Table 1). There ispresently no evidence thatAD3 is involvedin late-onset AD (65, 71, 72).When the AD3 locus was initially iden-
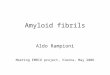
tified, the flanking markers were D14S52and D14S53 with the disease gene intervalbeing 23 centimorgans (Fig. 2). The AD3region has now been refined to betweenD14S61 and D14S289 (66), which spans-8 centimorgans. Initial candidate genesin the region included FOS and HSP70(63). Mutational analysis of the FOS gene(73, 74) failed to detect mutations. Clon-ing and mapping of the HSPA2 gene elim-inated it as a candidate (75). Subsequentto the initial localization ofAD3, the genesfor transforming growth factor /3 (76) anddihydrolipoyl succinyltransferase (77)have been mapped to this region and arecurrently being evaluated for AD3 muta-tions.AD3 and a Second Chromosome 21
Locus. Identification of the chromosome14 locus permitted reevaluation of thehypothesis that there is an FAD gene onchromosome 21, distinct from the APPlocus (19, 21, 22, 78). Initial evidence forlinkage in this region came from fourfamilies referred to as FAD1, FAD2,FAD3, and FAD4, with most of the evi-dence coming from FAD4, a large UnitedStates-French-Italian pedigree (19). Thecombined evidence from the four familieswas Zmax = 2.32 (0 = 0) by using thecentromeric marker D21S1/S11, with
multipoint analysis reaching 4.26 (0 =0.08). In subsequent analysis with anothercentromeric marker, D21S52, a Zmax of2.94 was reported for the FAD4 kindred(79). When these same four families wereanalyzed with D14S43, the combined max-imum lod score was 16.8 (0 = 0) (65). TheFAD4 kindred alone gave a Zm. value of5.21 (0 = 0.05) with D14555. Two Belgianfamilies that had given suggestive lodscores for D21S13/S16 (Zmax = 1.37; 0 =0.10) (78) yielded a Zm. of 13.25 (0 = 0)with D14S43 (70). Thus, all the largefamilies that gave suggestive lod scoreswith chromosome 21 markers yield un-equivocally positive results for chromo-some 14 markers. One interpretation ofthese results was that a gene in the cen-tromeric region of chromosome 21 acts asa modifier of the chromosome 14 locus(65). However, inheritance in these largefamilies is clearly autosomal dominant andthere is no evidence of a phenotype-modifying trait that cosegregates withchromosome 21 markers. Thus, it is un-likely that a second chromosome 21 FADlocus exists.
Clinical and Neuropathological Char-acteristics of AD3 Kindreds. Studies ofthe clinical and neuropathologic featuresofAD3 families (80-88) show that AD inthese families is extremely severe. Onsetcan occur as early as 30 years of age anddisease duration is shorter than observedin late-onset AD (Table 1). For example,in the extensively studied L kindred, onsetcan occur as early as 30 years (family mean= 41.6 + 3.8 years; range = 30-48 years),and the family mean duration of the dis-ease is 5.8 ± 2.5 years (range, 2-10 years)(88). The clinical features characteristic ofAD in these families include prominentseizures, myoclonus, and paratonia, whichhave been observed in many of the sub-
8554 Review: Schellenberg
Dow
nloa
ded
by g
uest
on
Apr
il 24
, 202
1

Proc. Natl. Acad. Sci. USA 92 (1995) 8555
iI
=AD3
!'I X 4 :--C.r.,
FIG. 2. AD3 region of chromosome 14.
jects from different families (81, 83, 87,88). These features are more variable,occurring later in the course of the diseasein other forms ofAD (89, 90). The excep-tion in the AD3 kindreds may be theSNW/FAD3 family (88), in which extra-pyramidal signs, seizures, and myoclonuswere not observed (82). This family, aswell as FAD1 (87), may be examples ofallelic heterogeneity compared to otherAD3 kindreds in that both have a later ageof onset compared to otherAD3 families,and the duration of disease is somewhatlonger with some individuals living up to18 years after onset of symptoms. Neuro-pathologic studies of the AD3 familieshave shown extensive senile plaques,NFTs, and granulovacuolar changes in thehippocampus. Amyloid deposits in thecerebellum were a more variable featureand were not observed in all patientsautopsied (83, 88-90). In summary, theclinical and neuropathologic phenotype ofAD3 families overlaps those observed inother forms of AD. Inheritance is auto-somal dominant, with penetrance com-plete by the age 50 in many families and bythe late 50s in others (Table 1). The AD3locus accounts for about 90% of early-onset autosomal dominant AD.
The VG Kindreds
The APP and AD3 loci do not explain allearly-onset FAD. Evidence for an addi-tional early-onset locus comes from stud-ies of the VG kindreds. These familiescome from a group of Germans who, inthe 1760s, emigrated to the Volga riverregion of Russia (80, 91). The VGs re-mained culturally distinct from the sur-rounding Russian population. At the turnof the 20th century, a second emigrationto the United States occurred. Bird andcolleagues (63, 80, 91) identified seven
VG kindreds with early-onset autosomaldominant AD. Onset of AD in these fam-ilies ranges from 40 to 81 years with familymean age of onsets ranging from 51 to 65years (Table 1). The VG families havebeen extensively studied, including 21 au-
topsies. The clinical and neuropathologiccharacteristics are consistent with AD.
Linkage analysis of the VG familieswith chromosome 21 markers has yieldednegative results (23, 24, 29) and no muta-tions have been identified in theAPP gene(29). Similarly, linkage analysis with chro-mosome 14 markers nearAD3 (63,71) andwith the chromosome 19 APOCII STRPlocus gave negative results (68, 92). Thus,the locus responsible for AD in the VGkindreds remains to be mapped. Otherearly-onset families have been reported inwhich the APP gene and the chromosome14 locus has been excluded (72, 93).
Apolipoprotein E (apoE) andLate-Onset AD
Genetic dissection of late-onset AD isproblematic for the following reasons.First, the disease is common in the elderlywith prevalence estimates reaching as highas 18.7% (94) in the 75-84 year age group.Thus, clustering of cases in a given familydoes not necessarily indicate inheritance ofa common genetic factor. Multiple cases ina kindred could be the result of chance orcould be the result of mixed etiology, in-cluding both genetic and nongenetic formsof AD. Also, different genetic etiologiescould be at work in the same family. Asecond difficulty is age-censoring; othercauses of death may remove individualsfrom the study population before maximumrisk forAD occurs. This not only confoundsanalysis but also makes ascertainment oflarge pedigrees difficult. A third problem isaccurate diagnosis. In the elderly, other
causes of dementia such as multiinfarct dis-ease, overmedication, and depression be-come common and confound the diagnosisof AD.
Despite the difficulties outlined above,theAPOE gene at 19q13.2 has been shownto be a late-onset AD risk factor. TheAPOE gene encodes apoE and is part ofan apolipoprotein gene cluster that spans-40 kb and contains in addition toAPOE,APOCII, APOCI, and an APOCI pseudo-gene. This region was initially implicatedin AD by genetic studies. Positive affectedpedigree member evidence for late-onsetAD was reported by using a cluster ofmarkers (BCL3, D19S13, and ATPJA3)(95) located within 2.5 centimorgans ofthe APOEICI/CII gene cluster. Positivelod scores were also reported for the samemarkers (95). Positive genetic associationresults had also been reported for an alleleof a restriction fragment length polymor-phism locus at APOCII (68, 96).
Definitive identification of the chromo-some 19 AD locus was achieved by screen-ing for proteins that could bind to immo-bilized AP. Strittmatter et al. (97) foundthat an AO3 binding factor in cerebralspinal fluid was apoE. In the same study,the relevance of APOE to late-onset ADwas examined by genotyping patients fromlate-onset FAD kindreds for the APOEE2/£3/£4 polymorphic system. This poly-morphism consists of single-base changesat codons 112 and 158, which encodeCys-112 and Cys-158 for the s2 allele,Cys-112 and Arg-158 for the £3 allele, andArg-112 and Arg-158 for the E4 allele,with respective allele frequencies of 0.08,0.78, and 0.14 in Caucasian controls. Astrong allelic association between AD andthe s4 allele of APOE was reported byusing late-onset FAD families; the fre-quency of e4 in AD patients being 0.52compared to 0.14-0.16 in controls (97).The APOE e4 association with AD was
rapidly confirmed in numerous studies oflate-onset AD (e.g., refs. 92 and 98-107)including familial samples (92, 101, 104),autopsy series (103, 105), clinic-basedcases (98, 102, 104, 105), and population-based studies (99, 106, 107). The highests4 frequencies reported have been in late-onset FAD kindreds (0.51-0.52; refs. 92and 97). The -4 frequencies for sporadiccases range from 0.24 in a French clinicpopulation (98) to 0.40 in an autopsyseries derived from a clinic population(102). Since these initial confirmatory re-ports have appeared, numerous other re-ports of elevated £4 alleles have beenpublished. The association has also beenobserved in a number of different ethnicgroups including Japanese (100, 108-110),African Americans (111, 112), and His-panics (112). The fact that the allelicassociation is observed in different ethnicgroups indicates that the observed rela-tionship between the £4 allele and AD isnot an artifact of population stratification.
Review: Schellenberg
L;l 1A -'-' ; -,li I.."
..-1
F
_ - .;
I-,.
Dow
nloa
ded
by g
uest
on
Apr
il 24
, 202
1

Proc. Natl. Acad. Sci. USA 92 (1995)
While most of the populations studiedhave been late-onset, one report of anearly-onset population-based group (on-set < 65 years; sample mean = 57 years)has also shown an allelic association ofADwith s4 (113). However, in another studyof Japanese early-onset sporadicAD cases(mean age of onset = 52.8 years), noallelic association was observed (s4 fre-quency = 0.08 in AD patients vs. 0.095 incontrols) (110).
E4 Allele Dose Effects. The s4 alleleappears to act as a dose-dependent age-of-onset modifier (114). The highest risk isassociated with the s4/s4 genotype, withsignificant but intermediate risk associ-ated with the s3/s4 genotype. Corder etal. (114) reported that in a late-onset FADgroup, each copy of the e4 allele reducesthe age of onset by 7-9 years, with onsetmean ages of 84.3 years, 75.5 years, and68.4 years reported for no E4, one £4allele, and two £4 alleles, respectively. Adose-dependent age-of-onset effect hasalso been observed in other FAD groups(115, 116), and in late-onset sporadic sub-jects (117), including those from a popu-lation-based study (106).The Protective Effects of the APOE E2
Allele. While the e4 frequency appears tobe elevated in AD cases, in some studies,the E2 allele frequency in AD patients islower than controls, leading to the sugges-tion that s2 may be protective against AD(118). This reduced s2 frequency has beenobserved in numerous ADAPOE studies,although the difference has not alwaysbeen statistically significant (92, 97, 98,102, 106, 110). Most of the evidence for aprotective effect of E2 relative to the ref-erence genotype E3/E3 has come from adecreased risk associated with the E2/E3genotype. The effect of the s2/E2 geno-type is difficult to evaluate since it is sorare. The E2/s4 genotype does not appearto be different from the reference E3/E3genotype in terms of risk for AD.
Interactions of APOE with Other ADLoci. The effects of APOE genotypes onAD expression have been explored in fam-ilies in which APP mutations cause dis-ease. For the Asn-670/Leu-671 mutation,subjects with anAPOE genotype of E2/£3(n = 3) had onset ages of 57-60 years,whereas subjects with £3/E3 (n = 3) hadintermediate onset ages of 51-54 years. Asingle case with an E4/E4 genotype hadthe earliest onset at 44 years (119). In adifferent family with the Ile-717 mutationand a mean age of onset at 47.6 ± 3.0years, the affected subjects (n = 3) areE3/E4, while one mutation carrier, who iss2/E3, remains unaffected at an age 2standard deviations past the onset meanfor the family (120). These data are con-sistent with APOE genotypes modifyingthe age of onset inAPP mutation families,although more subjects need to be ana-lyzed to validate this hypothesis. However,in a much larger study of HCHWA-D and
the Gln-693 mutation, in which 31 af-fected subjects were genotyped forAPOEand extensively clinically and neuropatho-logically characterized, no interaction be-tween APOE genotypes and disease ex-pression was observed (121, 122). Like-wise, APOE genotypes do not influenceexpression of the chromosome 14 AD3locus (123, 124).Linkage Disequilibrium and APOE.
The genetic evidence for a strong allelicassociation between APOE and AD indi-cates that either the s4 form of apoE is thegene product involved inAD pathogenesisor that the actual disease gene is a closelylinked locus in linkage disequilibrium withAPOE. The finding that E4 increases riskfor AD and that s2 is protective in manyCaucasian populations supports but doesnot prove the hypothesis thatAPOE is thepathogenic locus. The reported exceptionto this risk pattern is in an African-American AD population in which both64-containing genotypes and the E2/e3genotype elevated risk of AD relative tothe s3/e3 reference genotype (112).These data could be interpreted as indi-cating that the true disease locus has adifferent disequilibrium pattern withAPOE in Caucasians vs. African Ameri-cans, although other explanations are pos-sible. However, the elevated risk associ-ated with E2/E3 was not observed in an-other study of African Americans (111).Additional studies with larger sample sizesare needed to clarify this discrepancy.A limited number of disequilibrium
studies of AD have been performed byusing markers other thanAPOE. Evidencefor disequilibrium between AD and theSTRP markers D19S178 and APOCII(125) has been reported. However, in an-other study, no evidence for disequilib-rium between the APOCII STRP and ADwas observed (92). Early studies with a2-allele restriction fragment length poly-morphism at the APOCII locus suggestedthat this marker could be in disequilibriumwith AD by using a group of families thatincluded VG kindreds (68). However, oth-ers have not observed this allelic associa-tion between theAPOCII restriction frag-ment length polymorphism and AD (126,127), and thus, the original report mayonly apply to a specific ethnic group.Genetic analysis may not be able to de-finitively demonstrate that APOE is thedisease locus. Biochemical or transgenicanimal studies are needed to unambigu-ously establish the role of APOE in ADpathogenesis.The Role of ApoE in AD Pathogenesis.
Extensive work is now underway to deter-mine the role ofapoE inAD pathogenesis.Work has focused on identifying apoEinteractions that are isoform-dependent.One hypothesis is that apoE interacts withAP and this interaction influences amy-loid formation, with apoE acting as amolecular chaperon for amyloidogenic
peptides (128). In vitro experiments dem-onstrate that apoE binds to AP3 in anisoform-specific fashion (129), withapoE-s4 binding more rapidly to A,3 com-pared to apoE-e3. However, in anotherstudy, Apo-E3 bound better than ApoE-s4(130). Ma et al. (131), who used amyloidfibril formation evaluated by electron mi-croscopy as a measure of ApoE-Af inter-action, noted that apoE-s4 promoted fibrilformation better than apoE-s3. Evans etal. (132) reported that apoE inhibited aninitial nucleation step in fibril formationbut did not affect subsequent growth offibrils. The disulfide form of apoE-e3 wasa more potent nucleation inhibitor thanapoE-e4. Thus, while it is clear that apoEcan bind to A,B in vitro, whether anapoE-A,B interaction occurs in vivo andwhether these interactions are relevant toAD are not presently known.Another hypothesis is that apoE influ-
ences formation of NFTs by binding to tauprotein, the major component of thesestructures (133). apoE isoform-dependentbinding to tau has been reported withapoE-e3 binding more tightly than apoE-£4. Formation of the apoE-tau complexpossibly prevents tau from being phos-phorylated and from forming NFTs.Again, the relevance of apoE-tau inter-actions to AD pathogenesis has not beendemonstrated in vivo.The role of apoE in AD pathogenesis
could involve apoE acting as a neuronalinjury response protein (for a recent re-view, see ref. 134). ApoE production iselevated several hundredfold in a sciaticnerve injury model (135-137). The pre-sumed role of apoE in repair is as a lipidtransport protein that mobilizes choles-terol after injury. During regeneration,apoE particles are taken up via the lowdensity protein receptor (138) as a sourceof cholesterol for membrane synthesis andremyelination. In the central nervous sys-tem, apoE levels are also elevated to alesser extent in an entorhinal cortex lesionmodel (139). Also, apoE appears to pro-mote neuronal extension by an isoform-dependent mechanism. In experimentswith cultures of dorsal root ganglion neu-rons in the presence of /3 very low densitylipoprotein, apoE-e3 promoted neuriteoutgrowth whereas apoE-e4 inhibitedboth outgrowth and branching (140).Thus, the risk for AD associated with thes4 allele could be the result of apoE's roleas a lipid transport protein for synapto-genesis after injury.
Conclusions
The work summarized above shows thatAD is genetically heterogeneous. For ear-ly-onset autosomal dominant AD, in ad-dition to the APP gene and the chromo-some 14 locus AD3, at least one otherlocus remains to be mapped. For late-onset AD, the work onAPOE shows that
8556 Review: Schellenberg
Dow
nloa
ded
by g
uest
on
Apr
il 24
, 202
1

Proc. Natl. Acad. Sci. USA 92 (1995) 8557
the £4 allele is a risk factor for developingAD. However, 50-60% of all AD patientsdo not have an e4 allele. Other loci con-tributing to late-onset AD remain to bedetected and mapped. As in other com-mon complex diseases, these additionalloci may involve gene-gene interactions,perhaps involvingAPOE. Identification ofall susceptibility loci for AD is a majorgoal in resolving the pathogenesis of AD.However, gene identification is only anintermediate step in solving AD or anygenetic disorder. Substantial additionaleffort will be needed to understand howeach susceptibility factor is involved inADpathogenesis.
Note Added in Proof. After this manuscript wasprepared, the AD3 gene was cloned (141). ThecDNA transcript from this gene, designatedS182, is predicted to encode a 467-amino acidprotein. Analysis of the sequence suggests thatit may be a membrane protein with seventransmembrane domains. Five mutations in thecoding region were identified, including muta-tions in families FAD1, FAD2, FAD3, andFAD4. A mouse homologue of the gene wasalso reported. Each mutation occurred at anamino acid conserved between mouse and hu-man. The function of the S182 protein is un-known. Significant homology was reported fora Caenorhabditis elegans protein, SPE-4, that isinvolved in spermatogenesis (142).
In another recent development, the locusresponsible for AD in the VG kindreds wasmapped by linkage analysis (143). Markersspanning the genome were tested for linkageand positive results were obtained for markerson chromosome 1q31-42. For one marker,D1S479, in five of seven VG families tested, acommon allele cosegregating with the diseasewas identified. Subsequent work identified ahomologue of the S182 chromosome 14 gene(144) that is 67% identical to S182. The homo-logue was mapped to chromosome 1 and to ayeast artificial chromosome that also containedDlS479. DNA sequence analysis identified acandidate pathogenic mutation at codon 141that resulted in the substitution of an isoleucinefor the wild-type asparagine. The mutationoccurs at an amino acid conserved in the S182gene and the S182 mouse homologue. Thecombined results suggest that there may be afamily of genes encoding for membrane pro-teins involved in AD.
I also thank Thomas D. Bird and San Sisodiafor helpful suggestions. This work was sup-ported by Grants RO1-AG11762 and Alzhei-mer's Disease Research Center GrantAG08017 from the National Institutes of Agingand a grant from the American Health Assis-tance Foundation.
1. Alzheimer, A. (1907) Alg. Z. Psychiatr.64, 146-148.
2. Glenner, G. G. & Wong, C. W. (1984)Biochem. Biophys. Res. Commun. 120,885-890.
3. Masters, C. L., Simms, G., Weinman,N. A., Multhaup, G., McDonald, B. L. &Beyreuther, K. (1985) Proc. Nati. Acad.Sci. USA 82, 4245-4249.
4. McGeer, P. L. & Rogers, J. (1992) Neu-rology 42, 447-449.
5. Kang, J., Lemaire, H. -G., Unterbeck, A.,Salbaum, J. M., Masters, C. L., Grze-schik, K. H., Multhaup, G., Beyreuther,K. & Muller-Hill, B. (1987) Nature (Lon-don) 325, 733-736.
6. Lemaire, H. G., Salbaum, J. M., Mul-thaup, G., Kang, J., Bayney, R. M., Un-terbeck, A., Beyreuther, K. & Muller-Hill, B. (1989) Nucleic Acids Res. 17,517-522.
7. Ponte, P., Gonzalez-DeWhitt, P., Schill-ing, J., Miller, J., Hsu, D., Greenberg, B.,Davis, K., Wallace W., Lieberburg, I.,Fuller, F. & Cordell, B. (1988) Nature(London) 331, 525-527.
8. Tanzi, R. E., McClatchey, A. I., Lamperti,E. D., Villa-Komaroff, L., Gusella, J. F. &Neve, R. L. (1988) Nature (London) 331,528-530.
9. Kitaguchi, N., Takahashi, Y., To-kushima, Y., Shiojiri, S. & Ito, H. (1988)Nature (London) 331, 530-532.
10. Weidemann, A., Konig, G., Bunke, D.,Fischer, P., Salbaum, J. M., Masters,C. L. & Beyreuther, K. (1989) Cell 57,115-126.
11. Sandbrink, R., Masters, C. L. &Beyreuther, K. (1994) J. Biol. Chem. 269,1510-1517.
12. Konig, G., Monning, U., Czech, C., Prior,R., Banati, R., Schreiter-Gasser, U., Bauer,J., Masters, C. L. & Beyreuther, K (1992)J. Biol. Chem. 267, 10804-10809.
13. De Savage, F. & Octave, J. N. (1989)Science 245, 651-654.
14. Jacobson, J. S., Muenkel, H. A., Blume,A. J. & Vitek, M. P. (1991) Neurobiol.Aging 12, 575-583.
15. Wasco, W., Bupp, K., Magendantz, M.,Gusella, J. F., Tanzi, R. E. & Solomon,F. (1992) Proc. Natl. Acad. Sci. USA 89,10758-10762.
16. Shunt, H. H., Thinakaran, G., Von Koch,C., Lo, A. C. Y., Tanzi, R. E. & Sisodia,S. S. (1994) J. Biol. Chem. 269, 2637-2644.
17. Wasco, W., Gurubhagavatula, S., Para-dis, M. D., Romano, D. M., Sisodia, S. S.,Hyman, B. T., Neve, R. L. & Tanzi, R. E.(1993) Nat. Genet. 5, 95-100.
18. Tanzi, R. E., Gusella, J. F., Watkins,P. C., Bruns, G. A. P., St George-Hyslop,P., Van Keuren, M. L., Patterson, D.,Pagan, S., Kurnit, D. M. & Neve, R. L.(1987) Science 235, 880-884.
19. St George-Hyslop, P., Tanzi, R. E., Po-linsky, R. J., Haines, J. L., Nee, L., et al.(1987) Science 235, 885-890.
20. Oliver, C. & Holland, A. J. (1986) Psy-chol. Med. 16, 307-322.
21. Tanzi, R. E., St George-Hyslop, P.,Haines, J. L., Polinsky, R. J., Nee, L.,Foncin, J. F., Neve, R. L., McClathchey,A. I., Conneally, P. M. & Gusella, J. F.(1987) Nature (London) 329, 156-157.
22. Van Broeckhoven, C., Genthe, A. M.,Vandenberghe, A., Horsthemke, B.,Backhoven, H., et al. (1987) Nature (Lon-don) 329, 153-155.
23. Schellenberg, G. D., Bird, T. D., Wijs-man, E. M., Moore, D. K., Boehnke, M.,Bryant, E. M., Lampe, T. H., Nochlin,D., Sumi, S. M., Deeb, S. S., Beyreuther,K. & Martin, G. M. (1988) Science 241,1507-1510.
24. Schellenberg, G. D., Pericak-Vance,M. A., Wijsman, E. M., Moore, D. K.,
Gaskell, P. C., Yamaoka, L. A., Bebout,J. L., Anderson, L., Welsh, K. A., Clark,C. M., Martin, G. M., Roses, A. D. &Bird, T. D. (1991)Am. J. Hum. Genet. 48,563-583.
25. Pericak-Vance, M. A., Yamaoka, L. H.,Hayes, C. S., Speer, M. C., Haines, J. L.,et al. (1988) Exp. Neurol. 102, 271-279.
26. Van Duinen, S. G., Castano, E. M.,Prelli, F., Bots, G. T. A. B., Luyendijk,W. & Frangione, B. (1987) Proc. Natl.Acad. Sci. USA 84, 5991-5994.
27. Van Broeckhoven, C., Haan, J., Bakker,E., Hardy, J. A., Van Hul, W., Wehnert,A., Vegter-Van Der Vlis, M. & Roos,R. A. C. (1990) Science 248, 1120-1122.
28. Levy, E., Carman, M. D., Fernandez-Madrid, I. J., Power, M. D., Lieberburg,I., van Duinen, S. G., Bots, G. T. A. M.,Luyendijk, W. & Frangione, B. (1990)Science 248, 1124-1126.
29. Kamino, K., Orr, H. T., Payami, H., Wijs-man, E. M., Alonso, M. E., et al. (1992)Am. J. Hum. Genet. 51, 998-1014.
30. Goate, A. M., Owen, M. J., James, L. A.,Mullan, M. J., Rossor, M. N., Haynes,A. R., Farrall, M., Lai, L. Y. C., Roques,P., Williamson, R. & Hardy, J. (1989)Lancet i, 352-355.
31. Goate, A., Chartier-Harlin, M.-C., Mul-lan, M., Brown, J., Crawford, F., et al.(1991) Nature (London) 349, 704-706.
32. Fidani, L., Rooke, K., Chartier-Harlin,M. C., Hughes, D., Tanzi, R. E., Mullan,M., Roques, P., Rossor, M., Hardy, J. &Goate, A. (1992) Hum. Mol. Genet. 1,165-168.
33. Sorbi, S., Nacmias, B., Forleo, P., Pia-centini, S., Amaducci, L. & Provinciali,L. (1993) Nat. Genet. 4, 10.
34. Karlinsky, H., Vaula, G., Haines, J. L.,Ridgley, J., Bergeron, C., Mortilla, M.,Tupler, R. G., Percy, M. E., Robitaille,Y., Noldy, N. E., Yip, T. C. K., Tanzi,R. E., Gusella, J. F., Becker, R., Berg,J. M., Crapper-McLachlan, D. R. & StGeorge-Hyslop, P. H. (1992) Neurology42, 1445-1453.
35. Yoshioka, K., Miki, T., Katsuya, T., Ogi-hara, T. & Sakaki, T. (1991) Biochem.Biophys. Res. Commun. 178, 1141-1146.
36. Naruse, S., Igarashi, S., Aoki, K.,Kaneko, K., Iihara, K., Miyatake, T.,Kobayashi, H., Inuzuka, T., Shimizu, T.,Kojima, T. & Tsuji, S. (1991) Lancet 337,978-979.
37. Schellenberg, G. D., Anderson, L.-J.,O'Dahl, S., Wijsman, E. M., Sadovnick,A. D., Ball, M. J., Larson, E. B., Kukull,W. A., Martin, G. M., Roses, A. D. &Bird, T. D. (1992)Am. J. Hum. Genet. 49,511-517.
38. Tanzi, R. E., Vaula, G., Romano, D. M.,Mortilla, M., Huang, T. L., et al. (1992)Am. J. Hum. Genet. 51, 273-282.
39. Murrell, J., Farlow, M., Ghetti, B. &Benson, M. D. (1991) Science 254,97-99.
40. Chartier-Harlin, M.-C., Crawford, F.,Houlden, H., Warren, A., Hughes, D.,Fidani, L., Goate, A., Rossor, M.,Roques, P., Hardy, J. & Mullan, M.(1991) Nature (London) 353, 844-846.
41. Mullan, M., Crawford, F., Axelman, K.,Houlden, H., Lilius, L., Winblad, B. &Lannfelt, L. (1992) Nat. Genet. 1, 345-347.
Review: Schellenberg
Dow
nloa
ded
by g
uest
on
Apr
il 24
, 202
1

Proc. Natl. Acad. Sci. USA 92 (1995)
42. Hendriks, L., Van Duijn, C. M., Cras, P.,Cruts, M., Van Hul, W., Van Harskamp,F., Warren, A., McInnis, M. G., An-tonarakis, S. E., Martin, J.-J., Hofman,A. & Van Broeckhoven, C. (1992) Nat.Genet. 1, 218-221.
43. Houlden, H., Crawford, F., Rossor, M. &Mullan, M. (1993) Neurosci. Lett. 154,161-162.
44. Mullen, M., Houlden, H., Crawford, F.,Kennedy, A., Rogues, P. & Rossor, M.(1993) Am. J. Med. Genet. 48, 129-130.
45. Mullan, M., Tsuji, S., Miki, T., Katsuya,T., Naruse, S., et al. (1993) Neurobiol.Aging 14, 407-419.
46. Kennedy, A. M., Newman, S., Mccad-don, A., Ball, J., Roques, P., Mullan, M.,Hardy, J., Chartierharlin, M. C., Frack-owiak, R. S. J., Warrington, E. K. & Ros-sor, M. N. (1993) Brain 116, 309-324. .
47. Farlow, M., Murrell, J., Ghetti, B., Un-verzagt, F., Zeldenrust, S. & Benson, M.(1994) Neurology 44, 105-111.
48. Axelman, K., Basun, H., Winblad, B. &Lannfelt, L. (1994) Arch. Neurol. 51,1193-1197.
49. Sisodia, S. S., Koo, E. H., Beyreuther, K.,Unterbeck, A. & Price, D. L. (1990) Sci-ence 248, 492-495.
50. Esch, F. S., Keim, P. S., Beattie, E. C.,Blacher, R. W., Culwell, A. R., Olters-dorf, T., McClure, D. & Ward, P. J.(1990) Science 248, 1122-1124.
51. Shoji, M., Golde, T. E., Ghiso, J.,Cheung, T. T., Estus, S., Shaffer, L. M.,Cai, X.-D., McKay, D. M., Tintner, R.,Frangione, B. & Younkin, S. G. (1992)Science 258, 126-129.
52. Seubert, P., Vigo-Pelfrey, C., Esch, F.,Lee, M., Dovey, H., Davis, D., Sinha, S.,Schlossmacher, M ., Whaley, J., Swindle-hurst, C., McCormack, R., Wolfert, R.,Selkoe, D., Lieberburg, I. & Schenk, D.(1992) Nature (London) 359, 325-327.
53. Haass, C., Schlossmacher, M. G., Hung,A. Y., Vigo-Pelfrey, C., Mellon, A., Os-taszewski, B. L., Liederburg, I., Koo,E. H., Schenk, D., Teplow, D. B. &Selkoe, D. J. (1992) Nature (London)359, 322-325.
54. Cai, X.-D., Golde, T. E. & Younkin,S. G. (1993) Science 259, 514-516.
55. Citron, M., Oltersdorf, T., Haass, C.,McConlogue, L., Hung, A. Y., Seubert,P., Vigo-Pelfrey, C., Lieberburg, I. &Selkoe, D. J. (1992) Nature (London)360, 672-674.
56. Citron, M., Vigo-Pelfrey, C., Teplow,D. B., Miller, C., Schenk, D., Johnston,J., Winblad, B., Venizelos, N., Lannfelt,L. & Selkoe, D. J. (1994) Proc. Natl.Acad. Sci. USA 91, 11993-11997.
57. Suzuki, N., Cheung, T. T., Cai, X-D.,Odaka, A., Otvos, L., Eckman, C., Golde,T. E. & Younkin, S. G. (1994) Science264, 1336-1340.
58. Tamaoka, A., Odaka, A., Ishibashi, Y.,Usami, M., Sahara, N., Suzuki, N.,Nukina, N., Mizusawa, H., Shoji, S., Ka-nazawa, I. & Mori, H. (1994) J. Biol.Chem. 269, 32721-32724.
59. Burdick, D., Soreghan, B., Kwon, M.,Kosmoski, J., Knauer, M., Henschen, A.,Yates, J., Cotman, C. & Glabe, C. (1992)J. Biol. Chem. 267, 546-554.
60. Hilbich, C., Kisters-Woike, B., Reed, J.,Masters, C. L. & Beyreuther, K. (1991)J. Mol. Biol. 218, 149-163.
61. Jarrett, J. T. & Lansbury, P. T. (1993)Cell 73, 1055-1058.
62. Haass, C., Hung, A. Y., Selkoe, D. J. &Teplow, D. B. (1994) J. Biol. Chem. 269,17741-17748.
63. Schellenberg, G. D., Bird, T. D., Wijs-man, E. M., Orr, H. T., Anderson, L,Nemens, E., White, J. A., Bonnycastle,L., Weber, J. L., Alonso, M. E., Potter,H., Heston, L. L. & Martin, G. M. (1992)Science 258, 668-671.
64. Haltia, M., Viitanen, M., Sulkava, R.,Ala-Hurula, V., Poyhonen, M., et al.(1994) Ann. Neurol. 36, 362-367.
65. St George-Hyslop, P., Haines, J., Ro-gaev, E., Mortilla, M., Vaula, G., et al.(1992) Nat. Genet. 2, 330-334.
66. Mitsunaga, Y., Takahashi, K., Tabira, T.,Tasaki, H. & Watanabe, S. (1994) Lancet344, 1154-1155.
67. Van Broeckhoven, C., Backhovens, H.,Cruts, M., De Winter, G., Bruyland, M.,Cras, P. & Martin, J.-J. (1992) Nat.Genet. 2, 335-339.
68. Schellenberg, G. D., Boehnke, M., Wijs-man, E. M., Moore, D. K., Martin, G. M.& Bird, T. D. (1992) Ann. Neurol. 31,223-227.
69. Nechiporuk, A., Fain, P., Kort, E., Nee,L. E., Frommelt, E., Polinsky, R. J., Ko-renberg, J. R. & Pulst, S. M. (1993) Am.J. Med. Genet. 48, 63-66.
70. Mullan, M., Houlden, H., Windelspecht,M., Fidani, L., Lombardi, C., Diaz, P.,Rossor, M., Crook, R., Hardy, J., Duff,K. & Crawford, F. (1992) Nat. Genet. 2,340-342.
71. Schellenberg, G. D., Payami, H., Wijs-man, E. M., Orr, H. T., Goddard,K. A. B., Anderson, L., Nemens, E.,White, J. A., Alonso, M. E., Ball, M. J.,Kaye, J., Morris, J. C., Chui, H., Sa-dovnick, A. D., Heston, L. L., Martin,G. M. & Bird, T. D. (1993) Am. J. Hum.Genet. 53, 619-628.
72. Van Duijn, C. M, Hendriks, L., Farrar,L. A., Backhovens, H., Cruts, M., Weh-nert, A., Hofman, A. & Van Broeck-hoven, C. (1994) Am. J. Hum. Genet. 55,714-727.
73. Bonnycastle, L. L. C., Yu, C. E., Wijs-man, E. M., Orr, H. T., Patterson, D.,Clancy, K. P., Goddard, K. A. B.,Alonso, M. E., Nemens, E., White, J. A.,Heston, L. L., Martin, G. M., Bird, T. D.& Schellenberg, G. D. (1993) Neurosci.Lett. 160, 33-36.
74. Rogaev, E. I., Lukiw, W. J., Vaula, G.,Haines, J. L., Rogaeva, E. A., et al.(1993) Neurology 43, 2275-2279.
75. Bonnycastle, L. L. C., Yu, C. E., Hunt,C. R., Trask, B. J., Clancy, K. P., Weber,J. L, Patterson, D. & Schellenberg, G. D.(1994) Genomics 23, 85-93.
76. Tanzi, R. E., Romano, D. M., Crowley,A. C., Paradis, M. D., Gaston, S. M.,Buckler, W. & Wasco, W. (1994) Am. J.Hum. Genet. 55, Suppl., A272 (abstr.).
77. Ali, G., Wasco, W., Cai, X. G., Szabo, P.,Sheu, K. F. R., Cooper, A. J. L., Gaston,S. M., Gusella, J. F., Tanzi, R. E. &Blass, J. P. (1994) Somatic Cell. Genet.20, 99-105.
78. St George-Hyslop, P. H., Haines, J. L.,Farrer, L. A., Polinsky, R., Van Broeck-hoven, C., et al. (1990) Nature (London)347, 194-197.
79. Tanzi, R. E., St George-Hyslop, P. &Gusella, J. F. (1991) J. Biol. Chem. 266,20579-20582.
80. Bird, T. D., Sumi, S. M., Nemens, E. J.,Nochlin, D., Schellenberg, G. D.,Lampe, T. H., Sadovnick, A., Chui, H.,Miner, G. W. & Tinklenberg, J. (1989)Ann. Neurol. 25, 12-25.
81. Feldman, R. G., Chandler, K. A., Levy,L. L. & Glaser, G. H. (1960) Neurology13, 811-824.
82. Goudsmit, J. (1981) J. Neurol. Sci. 49,79-89.
83. Martin, J. J., Gheuens, J., Bruyland, M.,Cras, P., Vandenberghe, A., Masters,C. L., Beyreuther, K., Dom, R., Ceuter-ick, C., Lubke, U., van Heuverswijn, H.,De Winter, G. & Van Broeckhoven, C.(1991) Neurology 41, 62-68.
84. Nee, L. E., Polinsky, R. J., Eldridge, R.,Weingartner, H., Smallberg, S. & Ebert,M. (1983) Arch. Neurol. 40, 203-208.
85. van Bogaeert, L., Maere, M. & de Smedt,E. (1940) Mschr. Psychiatry Neurol. 102,249-301.
86. Wheelan, L. (1959)Ann. Hum. Genet. 23,300-309.
87. Frommelt, P., Schnabel, R., Kuhne, W.,et al. (1991)AlzheimerDis. Assoc. Disord.5, 36-43.
88. Lampe, T. H., Bird, T. D., Nochlin, D.,Nemens, E., Risse, S. C., Sumi, S. M.,Koerker, R., Leaird, B., Wier, M. &Raskind, M. A. (1994) Ann. Neurol. 36,368-378.
89. Struble, R. G., Polinsky, R. J., Hedreen,J. C., et al. (1991) J. Neuropathol. Exp.Neurol. 50, 82-92.
90. Risse, S. R., Lampe, T. H., Bird, T. D., etal. (1990)AlzheimerDis. Assoc. Disord. 4,217-225.
91. Bird, T. D., Lampe, T. H., Nemens, E. J.,Miner, G. W., Sumi, S. M. & Schellen-berg, G. D. (1988) Ann. NeuroL 23, 25-31.
92. Yu, C., Payami, H., Olson, J. M.,Boehnke, M., Wijsman, E. M., et al.(1994) Am. J. Hum. Genet. 54, 631-642.
93. Lannfelt, L, Lilius, L., Appelgren, H.,Axelman, K., Forsell, C., Liu, L., Johans-son, K. & Gaff, C. (1993) Nat. Genet. 4,218-219.
94. Evans, D. A., Funkenstein, H., Albert,M. S., Scherr, P. A., Cook, N. R., Chown,M. J., Herbert, L. E., Hennekens, C. H.& Taylor, J. 0. (1989) J. Am. Med. Assoc.262, 2551-2556.
95. Pericak-Vance, M. A., Bebout, J. L.,Gaskell, P. C., Yamaoka, L. H., Hung,W.-Y.,Alberts, M. J., Walker,A. P., Bart-lett, R. J., Haynes, C. S., Welsh, K. A.,Earl, N. L., Heyman, A., Clark, C. M. &Roses, A. D. (1991) Am. J. Hum. Genet.48, 1034-1050.
96. Schellenberg, G. D., Deeb, S. S., Boehnke,M., Bryant, E. M., Martin, G. M., Lampe,T. H. & Bird, T. D. (1987)J. Neurogenet. 4,97-108.
97. Strittmatter, W. J., Saunders, A. M.,Schmechel, D., Pericak-Vance, M., Eng-hild, J., Salvesen, G. S. & Roses, A. D.(1993) Proc. Nati. Acad. Sci. USA 90,1977-1981.
8558 Review: Schellenberg
Dow
nloa
ded
by g
uest
on
Apr
il 24
, 202
1

Proc. Nati. Acad. Sci. USA 92 (1995) 8559
98. Brousseau, T., Legrain, S., Berr, C.,Gourlet, V., Vidal, 0. & Amouyel, P.(1994) Neurology 44, 342-344.
99. Mayeux, R., Stem, Y., Ottman, R.,Tatemichi, T. K., Tang, M., Maestre, G.,Nagai, C., Tycko, B. & Ginsberg, H.(1993) Ann. Neurol. 34, 752-754.
100. Noguchi, S., Murakami, K. & Yamada,N. (1993) Lancet 342, 737.
101. Payami, H., Kaye, J., Heston, L. L., Bird,T. D. & Schellenberg, G. D. (1993) Lan-cet 342, 738.
102. Poirier, J., Davignon, J., Bouthillier, D.,Kogan, S., Bertrand, P. & Gauthier, S.(1993) Lancet 342, 697-699.
103. Rebeck, G. W., Reiter, J. S., Strickland,D. K. & Hyman, B. T. (1993) Neuron 11,575-580.
104. Saunders, A. M., Schmader, K., Breitner,J. C. S., Benson, M. D., Brown, W. T.,Goldfarb, L., Goldgaber, D., Manwaring,M. G., Szymanski, M. H., McCown, N.,Dole, K. C., Schmechel, D. E., Strittmat-ter, W. J., Pericak-Vance, M. A. &Roses, A. D. (1993) Lancet 342, 710-711.
105. Saunders, A. M., Strittmatter, W. J.,Schmechel, D., St George-Hyslop, P. H.,Pericak-Vance, M. A., Joo, S. H., Rosi,B. L., Gusella, J. F., Crapper, Mac-Lachlan, D. R., Alberts, M. J., Hulette,C., Crain, B., Goldgaber, D. & Roses,A. D. (1993) Neurology 43, 1467-1472.
106. Tsai, M.-S., Tangalos, E. G., Petersen,R. C., Smith, G. E., Schaid, D. J., Kok-men, E., Ivnik, R. J. & Thibodeau, S. N.(1994) Am. J. Hum. Genet. 54, 643-649.
107. Kuusisto, J., Koivisto, K., Kervinen, K.,Mykkanen, L., Helkala, E.-L., Van-hanen, M., Hanninen, T., Py6rala, K.,Kesaniemi, Y. A., Riekkinen, P. &Laakso, M. (1994) Br. Med. J. 309, 636-638.
108. Ueki, A., Kawano, M., Namba, Y.,Kawakami, M. & Ikeda, K (1993) Neu-rosci. Lett. 163, 166-168.
109. Dai, X. Y., Nanko, S., Hattori, M.,Fukuda, R., Nagata, K., Isse, K., Ueki, A.& Kazamatsuri, H. (1994) Neurosci. Lett.175, 74-76.
110. Yoshizawa, T., Yamakawa-Kobayashi,K., Komatsuzaki, Y., Arinami, T., Oguni,E., Mizusawa, H., Shoji, S. & Hamagu-chi, H. (1994) Ann. Neurol. 36, 656-659.
111. Hendrie, H. C., Hall, K. S., Hui, S., Un-verzagt, F. W., Yu, C. E., Lahiri, D. K.,Sahota, A., Farlow, M., Musick, B.,Class, C. A., Brashear, A., Burdine,V. E., Osuntokun, B. O., Ogunniyi,A. O., Gureje, O., Baiyewu, 0. & Schel-lenberg, G. D. (1995) Ann. Neurol. 37,118-120.
112. Maestre, G., Ottmann, R., Stern, Y.,Gurland, B., Chun, M., Tang, M.-X.,
Shelanski, M., Tycko, B. & Mayeux, R.(1995) Ann. Neurol. 37, 254-259.
113. Van Duijn, C. M., de Kniff, P., Cruts, M.,Wehnert, A., Havekes, L. M., Hofman,A. & Van Broeckhoven, C. (1994) Nat.Genet. 7, 74-78.
114. Corder, E. H., Saunders, A. M., Stritt-matter, W. J., Schmechel, D. E., Gaskell,P. C., Small, G. W., Roses, A. D., Haines,J. L. & Pericak-Vance, M. A. (1993) Sci-ence 261, 921-923.
115. Payami, H., Montee, K. R., Kaye, J. A.,Bird, T. D., Yu, C. E. & Schellenberg,G. D. (1994) J. Am. Med. Assoc. 271,1316-1317.
116. Houlden, H., Crook, R., Hardy, J.,Roques, P., Collinge, J. & Rosser, M.(1994) Neurosci. Lett. 174, 222-224.
117. Lucotte, G., Turpin, J.-C. & Landais, P.(1994) Ann. Neurol. 36, 681-682.
118. Corder, E. H., Saunders, A. M., Risch,N. J., Strittmatter, W. J., Schmechel, D. E.,Gaskell, P. C., Rimmler, J. B., Locke,P. A., Conneally, P. M., Schmader, K E.,Small, G. W., Roses, A. D., Haines, J. L. &Pericak-Vance, M. A. (1994) Nat. Genet. 7,180-184.
119. Alzheimer's Disease CollaborativeGroup (1993) Lancet 342, 737-738.
120. St George-Hyslop, P., Crapper Mc-Lachlan, D., Tuda, T., Rogaev, E., Kar-linsky, H., Lippa, C. F. & Pollen, D.(1994) Science 263, 537.
121. Haan, J., Van Broeckhoven, C., vanDuijn, C. M., Voorhoeve, E., van Har-skamp, F., van Swieten, J. C., Maat-Schie-man, M. L. C., Roos, R. A. C. & Bakker,E. (1994) Ann. Neurol. 36, 434-437.
122. Haan, J., Roos, R. A. C. & Bakker, E.(1995) Ann. Neurol. 37, 282.
123. Locke, P. A., Conneally, P. M., Tanzi,R. E., Gusella, J. F. & Haines, J. L.(1995) Genet. Epidemiol. 12, 83-92.
124. Van Broeckhoven, C., Backhovens, H.,Cruts, M., Martin, J. J., Crook, R., Houl-den, H. & Hardy, J. (1994) Neurosci. Lett.169, 179-180.
125. Chartier-Harlin, M.-C., Parfitt, M., Le-grain, S., Perez-Tur, J., Brousseau, T.,Evans, A., Berr, C., Vidal, O., Roques, P.,Gourlet, V., Fruchart, J.-C., Delacourte,A., Rossor, M. & Amouyel, P. (1994)Hum. Mol. Genet. 3, 569-574.
126. Tsuda, T., Lopez, R., Rogaeva, E. A.,Freedman, M., Rogaev, E., Drachman,D., Pollen, D., Haines, J., Liang, Y.,Crapper McLachlan, D. R., Duara, R. &St George-Hyslop, P. (1994) Ann. Neu-rol. 36, 97-100.
127. Liddell, M., Williams, J., Bayer, A., Kai-ser, F. & Owen, M. (1994) J. Med. Genet.31, 197-200.
128. Wisniewski, T. & Frangione, B. (1992)Neurosci. Lett. 135, 235-238.
129. Strittmatter, W. J., Weisgraber, K. H.,Huang, D. Y., Dong, L.-M., Salvesen,G. S., Pericak-Vance, M., Schemechel,D., Saunders, A. M., Goldgaber, D. &Roses, A. D. (1993) Proc. Natl. Acad. Sci.USA 90, 8098-8102.
130. Ladu, M. J., Falduto, M. T., Manelli,A. M., Reardon, C. A., Getz, G. S. &Frail, D. E. (1994) J. Bio. Chem. 269,23403-23406.
131. Ma, J., Yee, A., Brewer, H. B., Das, S. &Potter, H. (1994) Nature (London) 372,92-94.
132. Evans, K. C., Berger, E. P., Cho, C.-G.,Weisgraber, K. H. & Lansbury, P. T.(1995) Proc. Natl. Acad. Sci. USA 92,763-767.
133. Strittmatter, W. J., Saunders, A. M.,Goedert, M., Weisgraber, K. H., Dong,L. M., Jakes, R., Huang, D. Y., Peri-cakvance, M., Schmechel, D. & Roses,A. D. (1994) Proc. Nat. Acad. Sci. USA91, 11183-11186.
134. Poirier, J. (1994) Trends Neurosci. 17,525-530.
135. Mahley, R. W. (1988) Science 240, 622-630.
136. Boyles, J. K., Zoellner, C. D., Anderson,L. J., Kosik, L. M., Pitas, R. E., Weisgra-ber, K. H., Hui, D. Y., Mahley, R. W.,Gebicke-Haerter, P. J., Ignatius, M. J. &Shooter, E. M. (1989) J. Clin. Invest. 83,1015-1031.
137. Boyles, J. K., Notterpek, L. M. & Ander-son, L. J. (1990) J. Biol. Chem. 265,17805-17815.
138. Ignatius, M. J., Shooter, E. M., Pitas,R. E. & Mahley, R. W. (1987) Science236, 959-962.
139. Poirier, J., Hess, M., May, P. C. & Finch,C. E. (1991) Mol. Brain Res. 11, 97-106.
140. Nathan, B. P., Bellosta, S., Sanan, D. A.,Weisgraber, K. H., Mahley, R. W. & Pi-tas, R. E. (1994) Science 264, 850-852.
141. Sherrington, R., Rogaev, E. I., Liang, Y.,Rogaeva, E. A., Levesque, G., et al.(1995) Nature (London) 375, 754-760.
142. L'Hernault, S. W. & Arduengo, P. M.(1992) J. Cell Biol. 119, 57-68.
143. Levy-Lahad, E., Wijsman, E. M., Nem-ens, E., Anderson, L., Goddard, K. A. B.,Weber, J. L., Bird, T. D. & Schellenberg,G. D. (1995) Science, in press.
144. Levy-Lahad, E., Wasco, W., Poorkaj, P.,Romano, D. M., Oshima, J., Pettingell,W. H., Yu, C. E., Jondo, P. D., Schmidt,S. D., Wang, K., Crowley, A. C., Fu,Y, H., Guenette, S. Y., Galas, D., Ne-mens, E., Wijsman, E. M., Bird, T. D.,Schellenberg, G. D. & Tanzi, R. E.(1995) Science, in press.
Review: Schellenberg
Dow
nloa
ded
by g
uest
on
Apr
il 24
, 202
1