Embed Size (px)
Citation preview

47 | P a g e International Standard Serial Number (ISSN): 2319-8141
Full Text Available On www.ijupbs.com
International Journal of Universal Pharmacy and Bio Sciences 4(6): November-December 2015
INTERNATIONAL JOURNAL OF UNIVERSAL
PHARMACY AND BIO SCIENCES IMPACT FACTOR 2.093***
ICV 5.13***
Pharmaceutical Sciences REVIEW ARTICLE …………!!!
REVIEW ON-COLON TARGATED DRUG DELIVERY SYSTEM
Shinde V.S. 1*
, Shinkar D.M. 2, Saudagar R.B.
3
Department Of Pharmaceutics, R. G. Sapkal College of pharmacy, Anjaneri, Nashik.
KEYWORDS:
Need, Factors affecting
CDDS, Approaches of
CDDS, Evaluation.
For Correspondence:
Shinde V.S. *
Address:
Department Of
Pharmaceutics, R. G.
Sapkal College of
pharmacy, Anjaneri,
Nashik.
ABSTRACT
The colon drug delivery has a number of important implications in the
field of pharmacotherapy. It has been exploited for local as well as
systemic delivery of active drugs. Various diseases including
Inflammatory Bowel Diseases (IBD) can be effectively treated by the local
delivery of drugs to the large intestine. The treatment of large intestine
disorders, such as Crohn's disease, irritable bowel syndrome, colitis, colon
cancer and local infectious disease. The specific release in the colon also
affects a time delay between administration and onset of action, which can
useful for diseases with various degrees of severity, such as asthma and
arthritis.

48 | P a g e International Standard Serial Number (ISSN): 2319-8141
Full Text Available On www.ijupbs.com
INTRODUCTION:
Targeted drug delivery to the colon is highly desirable for local treatment of a variety of
bowel disease such as ulcerative colitis, crohn's disease, amebiosis, colonic cancer and for
local treatment of local colonic pathologies, and the systemic delivery of protein and peptide
drugs1,2
. Dosage forms that deliver drug in the colon rather than upper GIT has number of
advantages. Oral delivery of drugs in the colon is valuable in the treatment of diseases of
colon where by high local concentration can be achieved while minimizing side effects. The
colon is attracting interest as a site where poorly absorbed drug molecule may have an
improved bioavailability because the colon has long retention time and appears highly
responsible to agents that enhance the absorption of poorly absorbed drugs. The simplest
method for targeting of drugs to the colon is to obtain slower release rates or longer release
periods by the application of thicker layers of conventional enteric coating or extremely slow
releasing matrices. There are various method or techniques through which colon drug
targeting can be achieved, for example, formation of prodrug, coating with pH sensitive
polymers, coating with biodegradable polymers, designing formulation using polysaccharide,
timed released systems, pressure-controlled drug delivery systems, osmotic pressure
controlled systems. Coating of the drugs with pH sensitive polymers provides simple
approach for colon specific drug delivery. Drug delivery to the colon is beneficial not only
for the oral delivery of proteins and peptide drugs (degraded by the digestive enzymes of
stomach and small intestine) but also for the delivery of low molecular weight compounds
used to treat diseases associated with the colon or large intestine.
Need of colon targeted drug delivery:3
Targeted drug delivery to the colon would ensure direct treatment at the disease site,
lower dosing and fewer side effect.
Site-specific or targeted drug delivery system would allow oral administration of
peptide and protein drugs, colon specific formulation could also be used to prolong
the drug delivery.
The colon is a site where both local or systemic drug delivery could be achieved,
topical treatment of inflammatory bowel diseases, e.g. ulcerative colitis or Crohn's
disease .Such inflammatory conditions are usually treated with glucocorticoids and
sulfasalazine (targeted).
A number of others serious diseases of the colon, e.g. colorectal cancer, might also be
capable of being treated more effectively if drugs were targeted to the colon.

49 | P a g e International Standard Serial Number (ISSN): 2319-8141
Full Text Available On www.ijupbs.com
Formulations for colonic delivery are also suitable for delivery of drugs which are
polar and/or susceptible to chemical and enzymatic degradation in the upper GI tract,
highly affected by hepatic metabolism, in particular, therapeutic proteins and
peptides.
Advantages over conventional Drug Delivery:18
Ulcerative colitis and cirrhosis disease are currently treated with glucocorticoids,
and other anti-inflammatory agents.
Utilization of drug is more.
Side effects can be reduced.38
Lesser amount of doses required comparatively.39
Limitations:29
Multiple manufacturing steps.
Incomplete release of drug.
Lowering of bioavailability due to binding of drugs to intestinal contents.
Several factors like properties of drug, delivery system, interaction with GIT contents play a
major role in the successful delivery of drug. The luminal fluid in the colon plays a major
role in the absorption of the drugs. The luminal fluid in the colon is less compared to the
small intestine. The drug should be in soluble state for the successful absorption. To prevent
the decreased availability of low soluble drugs the drug should be delivered in presolubilized
form. The key factors to be considerd while targeting the drug to the specific organ like colon
are pH of GIT, drug solubility ,contents of GIT, microbial flora, transit time of the intestine,
etc.
Table-1 Colonic diseases, its site and active drug components4
Targated site Diseases Drug
Local Colorectal cancer, Cystic fibrosis,
Chronic pancreatitis, Pancreatactomy.
5-fluorouracil, Digestive
enzyme.
Systemic Oral delivery of vaccines, To prevent
gastric irritation, To prevent first pass
metabolism of orally administered drugs,
Oral delivery of peptides.
Typhoid, Steroids,
NSAIDS, Insulin.
Topical Inflammatory bowel diseases(Crohn's
diseases, Ulcerative colitis), Irritable
bowel diseases, Amoebiasis.
Hydrocortisone, Prednisolone,
Sulfasalazine, Mesalazine,
Mercaptopurine, Tinidazol,
Mebendazole.

50 | P a g e International Standard Serial Number (ISSN): 2319-8141
Full Text Available On www.ijupbs.com
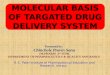
Anatomy of Colon:37
Fig-1 Anatomy of Colon
The GIT measures about 5 meters long. The different parts of GIT are divided into upper and
lower gastrointestinal tract. The upper GIT includes oesophagus, stomach, and duodenum.
The lower GIT includes small intestine and large intestine. The small intestine measures an
average of about 6.9 meters to 7.1 meters. It include duodenum, jejunum and ileum. The main
function of small intestine is the absorption of nutrients and mineral from food. The retension
time of small intestine is 3-5 hr. The large intestine extending from the ileocaecal junction to
the anus is divided into three main parts i.e. colon, the rectum and anal canal. The entire
colon is about 5 feet (150 cm) long, and is divided in to five major segments. Peritoneal folds
called as mesentery which is supported by ascending and descending colon. The right colon
consist of the caecum, ascending colon, hepatic flexure and the right half of the transverse
colon. The left colon contain the left half of the transverse colon, descending colon, splenic
flexure and sigmoid. The rectum is the last anatomic. The colon is having high water
absorption capacity, the colonic contents are considerably viscous and their mixing is not
efficient, thus availability of most drugs to the absorptive membrane is low. The human colon
has over 400 distinct species of bacteria as resident flora, a possible population of up to 1010
bacteria per gram of colonic contents. The major function of colon is the creation of suitable

51 | P a g e International Standard Serial Number (ISSN): 2319-8141
Full Text Available On www.ijupbs.com
environment for the growth of colonic microorganisms, storage reservoir of faecal contents,
expulsion of the contents of the colon at an appropriate time and absorption of potassium and
water from the lumen. The absorptive which more than 90% of the fluid is absorbed. Among
the reactions carried out by these gut flora capacity is very high, each about 2000ml of fluid
enters the colon through the ileocaecal valve are azoreduction and enzymatic cleavage i.e.
glycosides. These metabolic processes may be responsible for the metabolism of many drugs
and may also be applied to colon targeted delivery of peptide based macromolecules such as
insulin by oral administration.
Table-2 Measures of different parts of GIT29
Organ Length
Small intestine:
Duodenum
Jejunum
Ileum
3m
25cm
1m
2m
Large intestine:
Caecum Colon
Ascending colon
Transverse colon
Descending colon
Sigmoid portion
1.5m
6cm
20-25cm
10-15cm
40-45cm
35-40cm
Rectum 20cm
Anal canal 3cm
Factors affecting colon targeted delivery:
1.Physiological factors
2.Pharmaceutical factors
1. Physiological factors
a. Gastric emptying time29
Gastric emptying is test that measures the time it takes for food to empty from the stomach
and enter the small intestine. Drug delivery to the colon upon oral administration depends
mainly on gastric emptying and bowel transit time. Upon reaching the colon the transit time
of dosage form depends on the size of the particles. Smaller particles have more transit time

52 | P a g e International Standard Serial Number (ISSN): 2319-8141
Full Text Available On www.ijupbs.com
compared to larger particles. Diarrhoea patients have shorter transit time where as
constipation patients have longer gastric transit time.
Table-3 Transit time of different parts of colon5
Part of GIT Transit time
Fasted state
Fed state
Small intestine transit
Colon transit
10min – 2hr
>2hr
3-4hr
20-35hr
b. pH of colon:29
The pH of GIT varies between different individuals. The food intake, diseased state, etc.
influences the pH of the GIT. This change in the pH in different parts of GIT is the basis for
the development of colon targeted drug delivery systems. Coating with different polymers is
done to target the drug to the site.
Table-4 pH in different parts of colon
Part of GIT pH
Stomach Fasted state 1.5-2
Fed state 2-6
Small intestine 6.6- 7.5
Colon:
Ascending colon
Transverse colon
Descending colon
6.4
6.6
7.0
c. Colonic microflora and Enzymes29
The GIT contains a variety of microorganism that produces many enzymes need for
metabolism. Growth of this microflora is controlled by the GIT contents and peristaltic
movements. The enzymes released by different microorganism like E.coli ,Clostridia,
Lactobacilli, Eubacteria, Streptococci are responsible for the various metabolic reactions that
takes place in the GIT.

53 | P a g e International Standard Serial Number (ISSN): 2319-8141
Full Text Available On www.ijupbs.com
Table-5 Different microflora, enzymes released and action
Microorganism Enzyme Metabolic reaction
E.coli, Bacteroids Nitroreductase Reduces aromatic and
heterocyclic nitro compound
Clostridia, Lactobacilli Hydrogenase Reduces carbonyl groups &
aliphatic double bonds
Clostridia, Eubacteria Glucosedase Cleavage of b-glycosidase of
alcohols and phenols
Eubacteria,Clostridia,
Streptococci
sulfasetase Cleavage of o-sulphates and
sulfamates
2. Pharmaceutical Factor
a. Drug Candidate6
Drugs which shows poor absorption from stomach as intestne including peptide are most
suitable for CDDS. The drug used in treatment of IBD, ulcerative colitis, diarrhoes and colon
cancers are ideal candidates for local colon delivery.
Table-6 Criteria for selection of drugs for CDDS7
Criteria Pharmacological
class
Non peptide drug Peptide drug
Drugs used for local
action in colon
against GIT diseases
Anti-inflammatory
drugs
Metoprolol,
Nifedipine
Amylin,
Oligonucleotide
Drugs used for colon
cancer
Ant-ineoplastic drugs Pseudoephedrine Epoetin, Glucagon
Drugs poorly
absorbed
Anti-hypertensive
and Anti-anginal drugs
Ibuprofen,
Theophylline
Cyclosporine,
Desmopressin
Drugs that undergo
extensive first pass
metabolism
Nitroglycerin and
Corticosteroids
Bleomycin, Nicotine Sermorelin,
Saloatonin

54 | P a g e International Standard Serial Number (ISSN): 2319-8141
Full Text Available On www.ijupbs.com
b.Drug Carrier8
The selection of carrier for particular drug candidate depends on the physicochemical nature
of the drugs as well as the disease for which the system is to be used. The factor such as
chemical nature, stability and partition coefficient of drug and the type of absorption
enhancers chosen influence the carrier selection. Moreover, the choice of drug carrier
depends on the functional groups of drug molecule, etc.
Approaches for colon targeted drug delivery:33
In general, seven primary approaches have been proposed for targeted colon delivery,
namely,
1.Transit time dependent colonic DDS
2.pH dependent colonic DDS
3.pH and time dependent colonic DDS
4.Bacterial enzyme dependent colonic DDS
Prodrug based systems
a. Azo prodrug
b. Polymerric /Saccharide prodrug
c. Amino acid prodrug
5.pH and bacterial enzyme dependent colonic DDS
6.Colonic pressure controlled DDS
7.Osmotic pressure controlled colonic DDS.
1. Transit time dependent colonic DDS:34
The basic principle involved in the system is that the release of drug from dosage form should
be after a predetermined lag time to deliver the drug at the right site of action at right time
and in the right amount. It is also known as pulsatile release, delayed or sigmoidal release
system. This approach is based on the principle of delaying the release of the drug until it
enters into the colon.
The disadvantages of this systems are:
a. Gasrtic emptying time varies markedly between subject or in a manner dependent on type
and amount of food intake.
b. Gastrointestinal movement, especially peristalsis or contraction in the stomach would
result in change in Gastrointestinal transit of the drug.
c. Accelerated transit through different regions of the colon has been observed in patients
with the IBD, the carcinoid syndrome and diarrhoea and the ulcerative colitis. Combination

55 | P a g e International Standard Serial Number (ISSN): 2319-8141
Full Text Available On www.ijupbs.com
of hydrophilic (HPMC) and hydrophobic polymers has been used as coating for tablets that
release the drug from a core after a lag time.20,28
2. pH dependent colonic DDS:9
In the stomach, pH ranges between 1 and 2 during fasting but increases after eating. The pH
is about 6.5 in the proximal small intestine and about 7.5 in the distal small intestine.From the
ileum to the colon, pH declines significantly. It is about 6.4 in the cecum. However, pH
values as low as 5.7 have been measured in the ascending colon in healthy volunteers. The
pH in the transverse colon is 6.6 and 7.0 in the descending colon. Use of pH dependent
polymers is based on these differences in pH levels. The polymers described as pH dependent
in colon specific drug delivery are insoluble at low pH levels but become increasingly soluble
as pH rises.Although a pH dependent polymer can protect a formulation in the stomach and
proximal small intestine, it may start to dissolve in the lower small intestine and the site-
specificity of formulations can be poor.
Table-7 Different polymer and their pH value18
Polymer Threshold pH
Eudragit L100 6.0
Eudragit S100 7.0
Eudragit L-30D 5.6
Eudragit FS-30D 6.8
HPMC pthalate 50 5.2
HPMC pthalate 55 5.4
Cellulose acetate
Trimellate
4.8
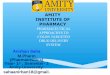
Fig 2: Drug release pattern of a multilayer coated system at different pH conditions in
GIT

56 | P a g e International Standard Serial Number (ISSN): 2319-8141
Full Text Available On www.ijupbs.com
3. pH and time dependent colonic DDS:33
The transit time through the small intestine is independent of the formulation. But, the time
taken by the formulation to leave the stomach varies greatly. Hence, the time of arrival of a
formulation in the colon cannot be accurately predicted. However, the effects of variation in
gastric residence time can be minimized by using systems that prevents drug release until 3-4
hr after leaving the stomach. A multiple coated oral dosage form consisting of core coated
with three polymeric layers has developed. A novel oral time based drug release system for
colon specific delivery. The system designed to exploit the relatively constant small intestinal
transit time of dosage forms consist of drug containing cores coated with three polymeric
layers. The outer layer dissolved at pH >5, then the intermediate swellable layer, made of an
enteric material. The system provides the expected delayed release pattern, as also indicated
by the preliminary in vivo studies on rats. Several other drug delivery systems have
developed that rely upon the relatively constant transit time of small intestine. A novel
delivery system was developed for delivering drugs to the colon by selecting
polymethacrylates with appropriate pH dissolution characteristic for the distal end of the
small intestine.
4. Bacterial enzyme dependent colonic DDS:14,15,16,17
The microflora of the colon is in the range of 1011
-1012
Cfu/ml consisting mainly of anaerobic
bacteria, e.g. Bacteroides Bifid bacterium, Eubacteria, Clostridia, Enterococci, and
Ruminococcus etc. These microflora fulfills its energy needs by fermenting various types of
substrates that been left undigested in the small intestine, like di and trisaccharides,
polysaccharides etc. For this fermentation, the micro flora produces a vast number of
enzymes like glucoronidase, xylosidase, arabinosidase, galactosidase, nitroreductase,
azareductase, deaminase, and urea dehydroxylase. Because of the presence of the
biodegradable enzymes only in the colon, the use of biodegradable polymers for colon-
specific drug delivery seems to be a more site-specific approach as compared to other
approaches. These polymer shield the drug from the enviornment of stomach and small
intestine, and are able to deliver the drug to the colon. On reaching the colon, they undergo
assimilation by micro-organism, or degradation by enzyme or break down of the polymer
back bone leading to a subsequent reduction in their molecular weight and thereby loss of
mechanical strength. They are then anable to hold the drug entity any longer. The majority of
bacteria are present in the colon they are distributed throughout the GI tract. Endogenous and
exogenous substrates, such as carbohydrate and proteins, escape digestion in the upper GI

57 | P a g e International Standard Serial Number (ISSN): 2319-8141
Full Text Available On www.ijupbs.com
tract but are metabolized by the enzyme sercreted by colonic bacteria. Sulfasalazine, a
prodrug consist of the active ingredient of mesalazine, was the first bacteria sensitive delivery
system designed to deliver the drug to the colon. Use of polysaccharides offers an alternative
substrate for the bacterial enzymes present in the colon. Most of the polymers are used in
pharmaceutical composition and are considerd generally regarded as safe (GRAS) recipients.
The enzymes present in the colon are:30
A.Reducing enzymes: Nitroreductase, Azoreductase, N-oxide reductase, Sulfoxide reductase,
Hydrogenase etc.
B.Hydrolytic enzymes: Esterase, Amidase, Glycosidase, Glucuronidase, Sulfatase etc.
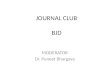
Prodrug based system:37
Fig-3 Prodrug System
Classical prodrugs design often represents a non-specific chemical approach to mask
unwanted drug properties such as low bioavailability, less site specific, and chemical
instability. On the other hand, targeted prodrug design represents a new strategy for directed
and efficient drug delivery. Particularly, prodrugs targeting to the specific enzymes or a
specific membrane transporter, or both, have potential drug delivery system especially for
cancer chemotherapy. Prodrug is the main approach of microbial triggered drug delivery
system in which the drug release from the formulation is triggered by the microflora present
in the gut. Prodrug is inactive form of an active parent drug that undergoes enzymatic
transformation to releasethe active drug. The prodrug are prepared by the linking the active
drug with hydrophobic moietis like amino acid, glucoronic acids, glucose, galactose,
cellulose, etc. These prodrug molecules get hydrolysed in the presence of the enzymes

58 | P a g e International Standard Serial Number (ISSN): 2319-8141
Full Text Available On www.ijupbs.com
released by the micro flora or specific membrane transporter, or both, have potential drug
delivery system especially for the cancer chemotherapy.
a. Azo prodrug:
In this type of conjugation drug is conjugated with an azo bond to the carrier. These azo
compounds are extensively metabolized by the intestinal bacteria, both by intracellular
enzymatic component and extracellular reduction. This azo bond is stable in the upper GIT
and is cleaved in the colon by the azo reductases produced by the micro flora. Ex.
Sulfasalazine is introduced for the treatment of rheumatoid arthritis and anti-inflammatory
disease. Chemically it is salicylazosulphapyridine (SASP), where sulphapyridine is linked to
a salicylate radical by an azo bond. When taken orally, only a small proportion of the
ingested dose is absorbed from the small intestine and the bulk of the sulfasalazine reaches
the colon intact. After reaching the colon there is split at the azo bond by the colonic bacteria
with the liberation of sulphapyridine and 5-ASA. Some new approaches for the treatment of
IBD have emerged due to the side effects of sulfasalazine. This is done by aminohippurate (4
amino benzoyl glycine), 4-amino benzoyl β-alanine in balsalazine, p-aminobenzoate in HB-
313 or a non-absorbable sulphanilamide ethylene polymer in poly-ASA. The most important
prodrug is osalazine (OSZ) which is dimer having two molecule of 5-ASA that are linked via
an azo bond.18,19,20

59 | P a g e International Standard Serial Number (ISSN): 2319-8141
Full Text Available On www.ijupbs.com
b. Polymeric/Saccharide prodrugs:36
The rationale for the development of a polysaccharides based colon delivery system is the
presence of large amount of polysaccharidases in the human colon as it is inhibited by a large
number and variety of bacteria which secrete many enzymes e.g. β- D -glucosidase, β- D -
galactosidase, amylase, pectinase, xylanase, β- D -xylosidase, dextranase etc.10,13
The
bacterial enzymes of colon degrades the carrier polymer and release the content for localized
and systemic absorption through colon.11,12
The list of microbially degradable materials is
given in bellow:
Table-8 Microbially degradable mataerial
Class Example
Disaccharide Lactose, Maltose
Oligosaccharide Cellobiose, Cyclodextrin, Lactulose
Polysaccharide36
Alginates, Amylose, Arabinogalactan, Cellulose,
Chitosan, Dextran, Galactomannan, Inulin, Karaya gum,
Pectin, Starch, Xylan, Xanthan and Tragacanth gum.
C. Amino acid prodrugs:
When free steroids were administered orally, they were almost absorbed in the small intestine
and less than 1% of the oral dose reached the colon. The conjugation of drug molecule to the
polar amino acids and prepared prodrugs for colon drug delivery. Proteins and their basic
units, i.e. amino acids, have polar groups like -NH2 and -COOH. These polar groups are
hydrophilic and reduce the membrane permiability of amino acids and proteins. Various non
essential amino acids such as glycine, tyrosine, methionine, and glutamic acid were
conjugated to salicylic acid. The conjugate showed minimal absorption and degradation in
the upper GI tract and showed more enzymatic specificity for hydrolysis by colonic enzymes.
Glucuronide and sulphate conjugation is the major mechanism for the inactivation and
preparataion for clearance of many drugs. Bacteria of the lower GI tract, however, secrete β-
glucuronidase and can deglucuronidate a variety of drugs in the intestine.
5. pH and bacterial enzyme dependent colonic DDS:
It is also called as CODE(combination of pH dependent and microbial triggered)
This method is developed to minimize the problems associated the pH and time dependent
drug delivery systems. In this systems the pH sensitive polymers are used along with the
polysaccharides that are degraded only by specific bacteria present in the intestine. This

60 | P a g e International Standard Serial Number (ISSN): 2319-8141
Full Text Available On www.ijupbs.com
system consists of a core tablet coated with three layers of polymer coatings.21
The outer
coating is composed of the polymer Eudragit L. This coating gets dissolved once the tablet
passes through the pyloric and duodenum and exposes the next coating. The next coating is
composed of Eudragit E. This layer allows the release of lactulose present in the inner core.
This release lactulose gets metabolized into short chain fatty acids that lower the surrounding
pH where the Eudragit E layer dissolves. The dissolving of Eudragit E results in the exposure
of the drug. The other polysaccharides that are used along with the drug in the core tablet are
mannitol, maltose, etc. The bacteria present in the colon are responsible for the degradation
of polysaccharides that are released from the core tablet. The
degradation of polysaccharides results in organic acids formation that lowers the pH of the
contents surrounding the tablet.
Fig-4 pH and bacterial enzyme dependent colonic DDS
6. Colonic pressure controlled DDS:
As a result of peristalsis, higher pressures are encountered in the colon than in the small
intestine. Developed pressure controlled colon-delivery capsules prepared using
ethylcellulose, which is insoluble in water.22
In such systems, drug release occurs following
the disintegration of a water-insoluble polymer capsule because of pressure in the lumen of
the colon. The thickness of the ethylcellulose membrane is the most important factor for the
disintegration of the formulation.23,24
The system also appeared to depend on capsule size and
density. Because of reabsorption of water from the colon, the viscosity of luminal content is
higher in the colon than in the small intestine. IT has therefore been concluded that drug
dissolution in the colon could present a problem in relation to colon-specific oral drug

61 | P a g e International Standard Serial Number (ISSN): 2319-8141
Full Text Available On www.ijupbs.com
delivery system. In pressure controlled ethylcellulose single unit capsules the drug is in a
liquid25
. Lag time of three to five hours in relation to drug absorption were noted when
preesure-controled were administered to humans.
7.Osmotic pressure controlled colonic DDS:
This system consists of osmotic units. The osmotic units are used either singly or as many as
pull units that are encapsulated in a hard gelatine capsule. The push pull units are bilayered
with outer enteric impermeable membrane and inner semi permeable membrane. The internal
or central part of the push pull consists of the drug layer and push payer. The semipermeable
membrane which is present next to the drug layer consists of an orifice through which the
drug are expelled during the course of time. The capsule body enclosing the push pull units
gets dissolved immediately after administration. During the passage of the push pull units
through the GIT the enteric impermeable membrane prevents the water absorption into the
unit. The coating gets dissolved once it reaches the small intestine due to higher pH(>7).
Water enters the unit through the semi permeable membrane causing the push layer to swell.
The swelling of the push compartment forces the drug into the surrounding environment
through the orifice. These osmotic controlled drug delivery system deliver the drug at a
constant rate for upto 24hr.
Fig-5 Osmotically controlled CDDS

62 | P a g e International Standard Serial Number (ISSN): 2319-8141
Full Text Available On www.ijupbs.com
Evaluation:
a. In vitro evaluation:
No standardized evaluation technique is available for evaluation of CDDS because an ideal in
vitro model should posseses the in vivo conditions of GIT such as pH, volume, stirring,
bacteria, enzymes, enzyme activity and other components of food. Generally these conditions
are influenced by the diet and physical stress and these factors make it difficult to design a
standard in vitro model. In vitro model used for CDDS are:
In vitro dissolution test:
Dissolution of controlled-release formulations used for colon-specific drug delivery are
usually complex, and the dissolution methods described in the USP can not wholly mimic in
vivo conditions such as those relating to pH, bacterial environment and mixing forces.26
Dissolution tests relating to CDDS may be carried out using the conventional basket method.
Parallel dissolution studies in different buffers may be undertaken to characterize the
behaviour of formulations at different pH levels. Dissolution tests of a colon-specific
formulation in various media simulating pH conditions and times likely to be encountered at
various locations in the GIT.27
The media chosen were, e.g. pH 1.2 to simulate gastric fluid,
pH 6.8 to simulate the jejunal region of the small intestine, and pH 7.2 to simulate the ileal
segment. Enteric-coated capsules for CDDS have been investigated in a gradient dissolution
study in three buffers. In vitro test for intactness of coatings and carriers in simulated
conditions of stomach and intestine. Drug released study in 0.1 N HCL for 2 hrs. (mean
gastric emptying time) Drug released study in phosphate buffer for 3 hrs (mean small
intestine transit time).
Preparation of 4% w/v rat caecal content:
Albino rats weighing 150-200 gm were kept on a normal diet and administered 1 ml of 1%
w/v solution of the selected polysaccharide in water. This treatment was continued for 7 days
in induce the specific enzymes responsible for degradation of polysaccharide in vivo. 30 min
before the drug release studies began the anesthetized rats were sacrificed, the rat abdomen
was opened ligatures were made before and after caecum and the caecum was removed under
anaerobic conditions. The caecum bag was opened and its contents were weighed and
homogenized then suspended in phosphate buffer saline (pH 7.4) to give the 4%
concentration of ceacal content. The suspension was centrifuged at 2000 rpm for 10 min at
4˚C to disrupt the bacterial cells followed by sonication. The resultant mixture was

63 | P a g e International Standard Serial Number (ISSN): 2319-8141
Full Text Available On www.ijupbs.com
centrifuged at 2000 rpm for 20 min. Because the caecum environment is naturally anaerobic,
all the operations were performed in a CO2 atmosphere.
In vitro release study in rat caecal medium:
The drug release studies were performed in slightly modified dissolution apparatus which
consist of a 250 ml beaker containing 200 ml of rat ceacal content medium was suspended
using iron string into the original jars containing water at 37±0.1ºC. The tablets were placed
in the 200ml dissolution medium containing 4% w/v rat caecal contents. The studies were
performed for 12-24 hrs. Samples were diluted appropriately with phosphate buffer saline
(pH 7.4) and centrifuged at 2000rpm for 10 min. The supernatant was filtered through
whatman filter paper, and the filterate was analysed for drug content using UV
spectrophotometer at 210nm. All experiment was performed in triplicate.
In vitro enzymatic test:18
1. Incubate carrier drug system in fermenter containing suitable medium for bacteria
(Streptococcus faccium or B. Ovatus) amount of drug released at different time intervals
determined.
2. Drug released study is done in buffer medium containing enzymes (enzyme pectinase,
dextranase), or rat or guinea pig or rabbit cecal.
b.In vivo evaluation
The in vivo evaluation of the CDDS is done in dogs, guinea pigs, rats and pigs as they
resemble the anatomic and physiological conditions, microflora of human GIT. The
distribution of various enzymes in GIT of rat and rabbit is comparable to that in human.
Marketed preparation to treat ulcerative colitis and crohn's disease
Drugs Trade Name Dose
Sulfasalazine Azulfidine 2-4 gm/day
Osalazine Dipentum 1 gm/day
Mesalazine Pentaza
Asacol
1.5-4 gm/day
Budenoside Entocost 9 mg/day
CONCLUSION :
Since two decades, considerable amount of research work has been carried out in the area of
colon targeting. CDDS offers potential therapeutic benefits to patients in term of both local
and systemic treatment. Although the surface area in colon is low compared to small
intestine, this is compensated by the markedly slower rate of transit. Various approaches

64 | P a g e International Standard Serial Number (ISSN): 2319-8141
Full Text Available On www.ijupbs.com
described above are quite promising and further improvments are required to achieve the high
bioavilabiltiy and safe delivery of drugs to the colon.
REFERENCES:
1. Philip AK, Philip B, Colon targeted drug delivery system: a review on primary and novel
approaches. Oman Medical Journal. 2012; 25(2): 79-87.
2. Oluwatoyin AO, John TF. In vitro evaluation of khaya and albizia gums as compression
coating for drug targeting to the colon. J Pharma Pharmacol. 2005; 57: 63-168.
3.Akala EO, Elekwachi O, Chase V, Johnson H, Marjorie L, Scott K. Organic redox initiated
polymerization process for the fabrication of hydrogel for colon specific drug delivery, Drug
Dev Ind Pharm. 2003; (29): 375.
4. Bansode AS, Athare AB, Kasture VS, Kendre PN. Colon targeted drug delivery system:
An Overview. Int. Imperical Journal of Pharmaceutics and Cosmetology. 2012; 2(2): 1-7.
5. Reddy RB, Malleswari K, G. Prasad and G. Pavani. Colon tageted drug delivery system: A
Review. Int. Journal of Pharmaceutical Science and Research. 2013; 4(1): 42-54.
6. Bussemer T, Otto, Bodmeier IR. Pulsatile Drug Delivery Systems. Crit. Rev. There. Drug
Carrier System. 2003, (18): 433-458.
7. Mahale NB, Hase DP, Bhujbal SS, Gaikwad SN, Chaudhari SR. Colon specific drug
delivery system: A Review. Int. Journal of Pharmaceutical research and development. 2013;
4(11): 56-64.
8. Chan RP, Pope DJ, Gilbett AP, Sneta PJ, Baron JH and Bennardjones JF. Studies of Two
Novel Sulphasalazine Analogs I.P. Salazide and Balsalazide. Digestive Diseases Sciences.
1983; (28): 609-716.
9. Sinha VR, Kumria R. Polysaccharide matrices for microbially triggered drug delivery to
the colon, Drug Dev Ind Pharm. 2004; (30): 143.
10. Sinha VR, Kumria R. Microbially triggered drug delivery to the colon. Eur. J. Pharm. Sci.
2003; 18(1): 3-18.
11. Kumar R, Patil MB, Patil SR, Paschapur MS. Polysaccharides based colon specific drug
delivery: A review. Int. J. PharmTech Res. 2009; 1(2): 334-46.
12. Singh BN. Modified-release solid formulations for colonic delivery. Recent Pat. Drug
Deliv. Formul. 2007; 1(1): 53-63.
13. Pawar KS, Pawar SP, Patel VA. Microbial polysaccharidases in colon specific drug
delivery. Int. J. Pharm. Sci. Rev. Res. 2011; 6(2): 188-96.

65 | P a g e International Standard Serial Number (ISSN): 2319-8141
Full Text Available On www.ijupbs.com
14. Brahmanakar BM, Jaiswal SB. Biopharmaceutics and pharmacokinetics to controlled
release medication of oral site specific/colon DDS,1995; 457.
15. Reddy MS, Sinha RV, Reddy DS. Colon targeted systems. Drugs Today, 1995; 35(7):
537.
16. WU, Mcginity C, JW. Non-traditional plasticization of polymeric films. Int. J.Pharm.
1999; 177, 15–27.
17.Flory, P.J. (ED.). Principles of Polymer Chemistry. Cornell University, Ithaca, New York,
1953.
18. patel Asha-Colon Targeted drug delivery system: A review. Journal of Pharmaceutical
and Bio scientific research 2011; 1(1) :37-49.
19. Aurora J, Naresh T and Pathak V. Colonic drug delivery challenges and opportunities
.Pharmaceutical Research and Development.
20. Vijay- Novel approaches for colon specific drug delivery. Phama info.net.
21. Mundhe VS, Dodiya SS. Review Article: Novel Approach for Colon Targeted Drug
Delivery. Indo American Journal of Pharmaceutical Research. 2011; 3:158-173.
22. Takaya T, Niwa K, Muraoka M, Ogita I, Nagai N, Yano R, Kimura G, Yoshikawa Y,
Yoshikawa H, Takada K. Importance of dissolution process on systemic availability of drugs
delivered by colon delivery system. J Control Rel. 1998; 50 (1-3): 111-122.
23. Muraoka M, Hu Z, Shimokawa T, Sekino S, Kurogoshi R, Kuboi Y, Yoshikawa Y,
Takada K. Evaluation of intestinal pressure-controlled colon delivery capsule containing
caffeine as a model drug in human volunteers. J Control Rel. 1998; 52(1-2): 119-129.
24. Jeong Y, Ohno T, Hu Z, Yoshikawa Y, Shibata N, Nagata S, Takada K. Evaluation of an
intestinal pressure-controlled colon delivery capsules prepared by a dipping method. J
Control Rel. 71(2): 175-182.
25. Hay DJ, Sharma H, Irving MH. Spread of steroid containing foam after intrarectal
administration. Brit Med J. 1979; (1) 1751-1753.
26. Yang L, James S, Joseph A. Colon specific drug delivery new approaches and in vitro/ in
vivo evaluation. Int J Pharm 2002; 235:1 -15.
27. Ahmed IS. Effect of simulated gastrointestinal condition on drug release from
pectin/ethyl cellulose as film coating for drug delivery to the colon. Drug Dev Ind Pharm.
2005; 31(4-5): 465-470.
28. Gazzainga A, Busetti C, Morol, Crimella T. Int Symp Control Release Bioact Materials
1995; 22:242.

66 | P a g e International Standard Serial Number (ISSN): 2319-8141
Full Text Available On www.ijupbs.com
29. Danda S, Chandan KB. COLON TARGETED DRUG DELIVERY – A REVIEW ON
PRIMARY AND NOVEL APPROACHES. 2013; 4(3): 1174-1183.
30. Prathap M, Gulshan MD , Rama Rao. COLON: TARGETED DRUG DELIVERY
SYSTEM – A REVIEW. International Journal of Research in Pharmaceutical and Nano
Sciences. 2014; 3(5): 429 – 437.
31. Philip AK, Philip B. Colon Targeted Drug Delivery Systems: A Review on Primary and
Novel Approaches. OMAN MEDICAL JOURNAL. 2010; 25: 70-78.
32. kumar JR, Selvadurai M, Sokkalingam AD and Umadevi SK. A Novel Drug Delivery
Systems Of Colon Targeted : A Review J. Pharm. Sci. & Res. 2013; 5(2): 42 – 47.
33. Gupta VK, Gnanarajan G, Kothiyal P. A Review Article on Colonic Targeted Drug
Delivery System. THE PHARMA INNOVATION. 2012; 1(7).
34. Cherukuri S, Reddy CS, Neelaboina VP, Reddipalli S, Komaragiri K. COLON SPECIFIC
DRUG DELIVERY SYSTEMS: A REVIEW ON APPROACHES WITH CURRENT
TRENDS. PHARMACEUTICAL INTERNATIONAL RESEARCH JOURNAL OF
PHARMACY. 2012; 3 (7).
35. Sharma A, Jain KA. COLON TARGETED DRUG DELIVERY USING DIFFERENT
APPROACHES .International Journal of Pharmaceutical Studies and Research .2010; 1(1):
60-66.
36. Kumar V, Verma S, Mishra DN, and Singh SK. NOVEL APPROACHES IN COLON
TARGETED DRUG DELIVERY SYSTEM. Bulletin of Pharmaceutical Research. 2012;
2(1): 26-33.
37. Rangari NT, Puranik PK. Review on Recent and Novel Approaches to Colon Targeted
Drug Delivery Systems. International Journal of Pharmacy and Pharmaceutical Research.
2015; 3(1).
38. Hita V, Singh R and Jain SK. Colonic Targeting of Metronidazole using Azo Aromatic
Polymers, Development and Characterization Drug delivery. 1997; 4: 19-22.
39. McLeod AD, Friend DR and Toma NT. Glucocorticoid-Dextran Conjugates As Potential Prodrugs
for Colon Specific Delivery-Hydrolysis in Rat Gastrointestinal Tract Contents. J Pharm Sci. 1994;
83(9): 1284-1288.