Embed Size (px)
Citation preview
Agenda Item 15.2
1
Review of Nurse Staffing - Six Month Update
Public Board
25th September 2014
Key points
1. Feedback from the last 6 month acuity and dependency reviews
Information
2. The trend and use of temporary staffing
Information
3. Nursing Staff Retention and Turnover
Information
Presented for: Information
Presented by: Professor Suzanne Hinchliffe CBE, Chief Nurse / Interim Chief Operating Officer
Author Jill Asbury, Head of Nursing, Nursing and Midwifery Education & Workforce
Previous Committees
None
Trust Goals
The best for patient safety, quality and experience
The best place to work
A centre for excellence for research, education and innovation
Seamless integrated care across organisational boundaries
Financial sustainability
Agenda Item 15.2
2
1.0 Summary This paper forms the six monthly review of nurse staffing in line with the commitment requested by the National Quality Board (NQB) (2013) document, Nurse Staff Guide ‘How to ensure the right people, with the right skills are in the right place at the right time!’ the recommendations from which were subsequently aggregated and released as Hard Truths, 2014. This paper will focus on the nurse / midwifery staffing reviews that have occurred in the last 6 months with the associated board paper, Hard Truths : Ward Workforce Health Check focussing on the workforce metrics (numbers of staff / ward current skill mix, sickness absence, maternity leave) recruitment, areas of concern and resulting actions. The impact of nursing, midwifery and care staffing capacity and capability on the quality of care experienced by patients, and on patient outcomes and experience has been well documented, with multiple studies linking low staffing levels to poorer patient outcomes, and to increased mortality rates. Nursing staff are the primary deliverers of 24/7 health-care within the multidisciplinary team in the majority of clinical settings and clinical specialities. In recognition of this and following the previous nurse staffing review the Leeds Teaching Hospitals (LTH) Board agreed an investment in principle of £14,006,985 over a 30 month period commencing 1st April 2014. Progress against this is tracked through the Ward Workforce Health Check paper that the Board receives at each meeting. The increased focus on safe and effective nurse staffing has led the National Institute for Health and Care Excellence (NICE) to develop safe staffing guidance, this was released in July 2014. NICE have a programme to develop a range of guidelines to cover all services, the release in July was Guideline 1 which covers adult inpatient wards in acute hospitals only. Leeds Teaching Hospitals (LTH) has a programme to review the staffing in a range of services, these being :
• Adult In-patient Wards – excluding critical care settings • Children’s Wards - excluding critical care settings • Maternity Services • Emergency Departments
(Critical Care settings for all patients regardless of age, are served by national guidance from their specialist societies and staffing is based and tracked according to these). The following paper brings together a brief description of the methodology used and the outputs from these reviews and includes :
• staff recruitment and progress against the investment into nurse staffing 2014/15 by Clinical Service Unit (CSU) see appendix 1 and 2
• the trend in staff joining and leaving LTH at bands 1 - 5
Agenda Item 15.2
3
• registered and un-registered nurse turnover at bands 2 and 5 • the usage and trend in temporary nurse staffing
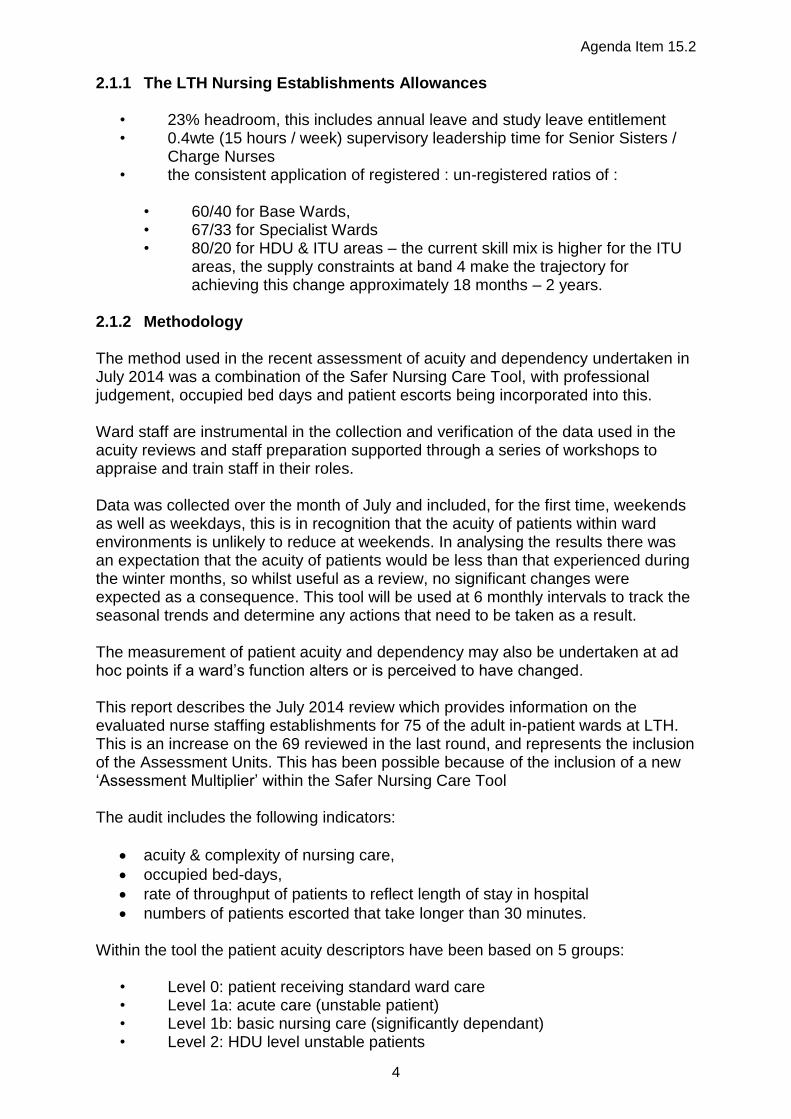
The information from the bi-monthly Ward Workforce Health Check is triangulated with the Ward Healthcheck, whose RAG rating is based on a percentage compliance with 14 key standards that are key to influencing patient outcomes and experience, these are referred to as ‘Red Flag’ events in the NICE and NQB documents. 2.0 Patient Acuity and Dependency Monitoring There are a range of tools and methods available to use in the determination of nurse staffing levels, there are briefly described in the table below. Whilst there is no tool that is recommended above the others, all of the these, when used in combination, provide evidence to ensure that staffing levels and patient outcomes are correlated. NICE do recommend the use of a validated tool Table 1
2.1 Adult Ward Acuity and Nurse Staffing Review
Method Description
Safer Nursing Care Tool (SNCT)
An evidence based tool that enables nurses to assess patient acuity and dependency, incorporating a staffing multiplier to ensure that nursing establishments reflect patient needs in acuity / dependency terms:
Level 0: patient receiving standard ward care
Level 1a: acute care (unstable patient)
Level 1b: basic nursing care (significantly dependant)
Level 2: HDU level unstable patients
Level 3: ITU level ventilated patients Appropriate for use in any acute hospital within the UK (although further work is underway to refine the tool for use in particular clinical environments). Used in conjunction with Nurse Sensitive Indicators (NSI) such as patient falls and pressure ulcer incidence, which can be linked to staffing. Able to support benchmarking activity in organisations when used across Trusts. Facilitates consistent nurse-to-patient ratios in line with agreed standards across similar care settings in England.
The Professional Judgment model (Telford method)
Simple to use and takes into account clinical staff views but is seen to be subjective, has no evidence-base and is not sensitive to workload intensity.
Staff to Bed ratio
Simple to use, allows benchmarking but assumes that base staffing levels are accurate and reflect patient need and is insensitive to changes in workload.
Activity Monitoring (GRASP)
Uses care plans / pathways and related nursing time but is task oriented, can be time consuming (to gather data / undertake workload studies) and may require support from commercial systems.
Nursing hours per patient day (NHPPD)
Widely used in the USA and Australia. Calculates the number of nurses and nursing assistants required in relation to activity levels.
Regression Methods (Teamwork)
Commercial systems are available and have been useful where workload predictions are possible, but is not easily understood by nurses and there is an underlying assumption that all wards are efficient and effective.
Agenda Item 15.2
4
2.1.1 The LTH Nursing Establishments Allowances
• 23% headroom, this includes annual leave and study leave entitlement • 0.4wte (15 hours / week) supervisory leadership time for Senior Sisters /
Charge Nurses • the consistent application of registered : un-registered ratios of :
• 60/40 for Base Wards, • 67/33 for Specialist Wards • 80/20 for HDU & ITU areas – the current skill mix is higher for the ITU
areas, the supply constraints at band 4 make the trajectory for achieving this change approximately 18 months – 2 years.
2.1.2 Methodology The method used in the recent assessment of acuity and dependency undertaken in July 2014 was a combination of the Safer Nursing Care Tool, with professional judgement, occupied bed days and patient escorts being incorporated into this. Ward staff are instrumental in the collection and verification of the data used in the acuity reviews and staff preparation supported through a series of workshops to appraise and train staff in their roles. Data was collected over the month of July and included, for the first time, weekends as well as weekdays, this is in recognition that the acuity of patients within ward environments is unlikely to reduce at weekends. In analysing the results there was an expectation that the acuity of patients would be less than that experienced during the winter months, so whilst useful as a review, no significant changes were expected as a consequence. This tool will be used at 6 monthly intervals to track the seasonal trends and determine any actions that need to be taken as a result. The measurement of patient acuity and dependency may also be undertaken at ad hoc points if a ward’s function alters or is perceived to have changed. This report describes the July 2014 review which provides information on the evaluated nurse staffing establishments for 75 of the adult in-patient wards at LTH. This is an increase on the 69 reviewed in the last round, and represents the inclusion of the Assessment Units. This has been possible because of the inclusion of a new ‘Assessment Multiplier’ within the Safer Nursing Care Tool The audit includes the following indicators:
acuity & complexity of nursing care,
occupied bed-days,
rate of throughput of patients to reflect length of stay in hospital
numbers of patients escorted that take longer than 30 minutes. Within the tool the patient acuity descriptors have been based on 5 groups:
• Level 0: patient receiving standard ward care • Level 1a: acute care (unstable patient) • Level 1b: basic nursing care (significantly dependant) • Level 2: HDU level unstable patients

Agenda Item 15.2
5
• Level 3: ITU level ventilated patients (the multiplier for this patient group does not include all the staffing requirements needed to staff an ICU bed as described in the ICU Society Standards, therefore this was not applied in these areas).
2.1.3 Output of the July 2014 Adult Ward Acuity and Nurse Staffing Review This review was broadly in line with that undertaken in September 2013, wards will always vary slightly when applying these measures, but the requirement by Clinical Service Unit remains the same as that undertaken in September 2013 see below : Table 2
Clinical Service Unit 13/14 Nurse
Establishment Review Output
July 2014 Acuity Review
Acute Medicine 462.45 460.19
Digestive Diseases 276.87 254.12
Cardio - Respiratory 263.73 262.68
Women’s 29.5 26.72
Leeds Cancer Center 244.95 223.27
Neurosciences 264.90 229.62
Head & Neck 49.41 38.86
Hepatorenal 157.1 158.45
Trauma Related Services 189.83 240.59
Chapel Allerton 95.02 71.38
Urgent Care 47.82 25.28
Theatres: Wards Only 15.62 15.89
The addition of the Assessment Units has been useful but will require further work in the next review to better capture the rapid change in patient acuity and dependency that occurs in these environments, much of this work may well be better aligned to using an Emergency Department tool which accounts for this, rather than the Safer Nursing Care Tool which does not. The leads for these areas will help to determine the approach taken in 6 months’ time to improve the accuracy of data capture. 2.1.4 Data Differences Between the 2 Reviews It should be noted that although for some of the CSU’s the difference in nursing requirements between the two reviews looks large (15 – 20 staff), this is spread across a number of wards and only constitutes a small number of nurses per ward. A level of natural variation would be expected between reviews and for some of the areas this is compounded by a number of factors described below :
The ward moves in Trauma and Related Services at the last review caused some discrepancies in the data, and the significant increase is mainly due to the inclusion of the multi-speciality assessment area, L34.

Agenda Item 15.2
6
For a number of the CSU’s e.g. Neurosciences, Digestive Diseases and Urgent Care the change in acuity can have a significant effect on the months data, particularly if that patient is highly dependent on nursing care.
A number of the CSU’s have been operating with a slightly reduced bed base, to ensure the safe balance of nurse staffing and patient dependency, this has the effect of showing the CSU’s as requiring a reduced number of nursing staff at the July review.
The effect of undertaking the data collection to include the weekends needs to be analysed to determine if this has had an effect on the overall results.
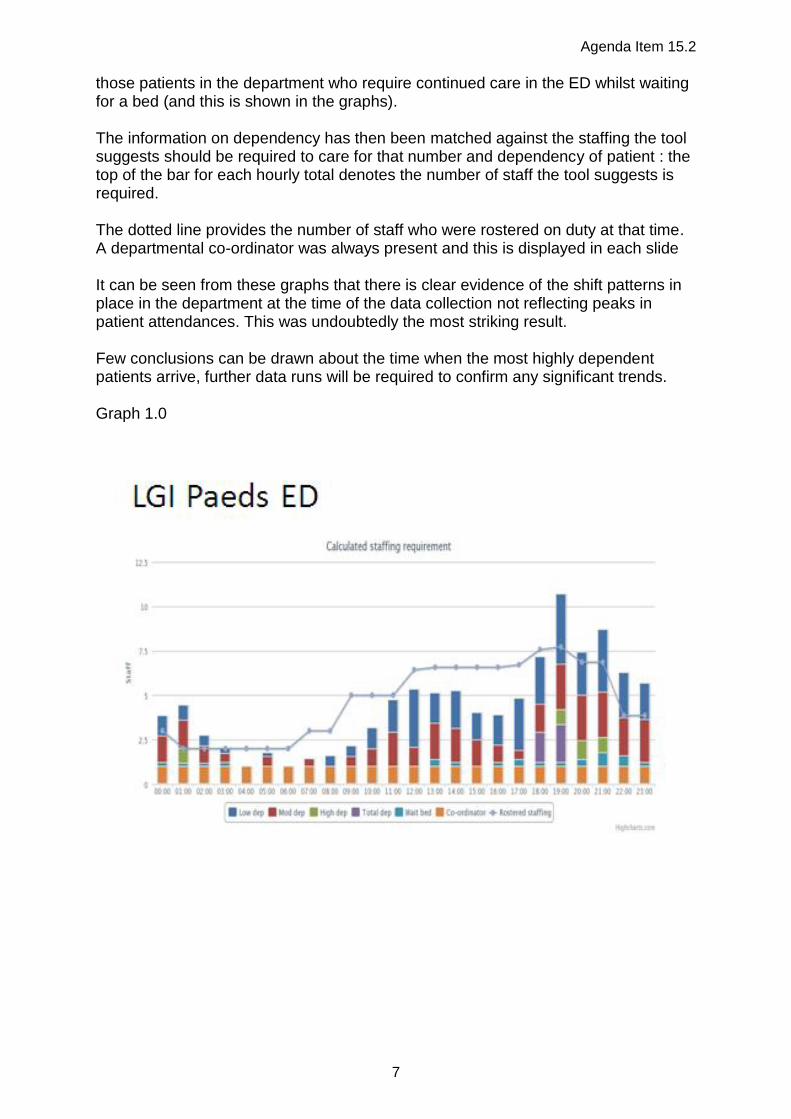
This data was received in the middle of August and there is a recognition that further analysis and professional review is required within a number of the CSU’s. This will be undertaken over the next month in conjunction with the Heads of Nursing. 3.0 Emergency Department Acuity and Nurse Staffing Review The traditional acuity and dependency tools have not been fit to apply in the arena of rapid changes in patient acuity and where the patient stays are of very short duration, hence in previous reviews in LTH these departments have been excluded and professional judgement aligned to patient flow data and red flag events have been used to determine the nurse staffing required. With the need to better understand staffing requirements in these areas the RCN Urgent Care Special Interest Group have devised a tool, the RCN Baseline Emergency Staffing Tool (2013) to enable this. It is validated and represents the best currently available and is one that NICE will incorporate into its’ review of tools suitable for use in this area which is scheduled for early in 2015. The data collection period for this tool is over 7 days, it is labour intensive and requires the staff collecting it to be supernumerary for the entire seven day period. The data was collected at the 2 LGI Emergency Departments (ED), (Children’s and Adults) in one week, followed by the SJH ED being collected the following week. Quality Assurance was provided by the senior nursing team in Urgent Care. The use of the tool was new to LTH and support and advice was kindly offered by the team at Calderdale NHS Trust, who had been instrumental in devising and piloting the tool. 3.1 Output of the ED Acuity and Nurse Staffing Review: The weeks in which the data was collected represented 2 of the highest weeks for patient attendances and caused significant strain on the Emergency Care Standard, the analysis of the data took this into account and corrected for it using historical data for the ‘peak’ days. The outcome of the exercise confirmed the underlying thoughts about the dependency needs of patients at each site resulting from the centralisation of clinical specialities, and the changing patterns of patient presentation Graphs 1.0 – 1.2 (please note : the graphs do not share a common scale) below, show the dependency of patients in each of the 3 departments on an hourly basis, and are displayed as low, medium and highly dependent. It also takes account of
Agenda Item 15.2
7
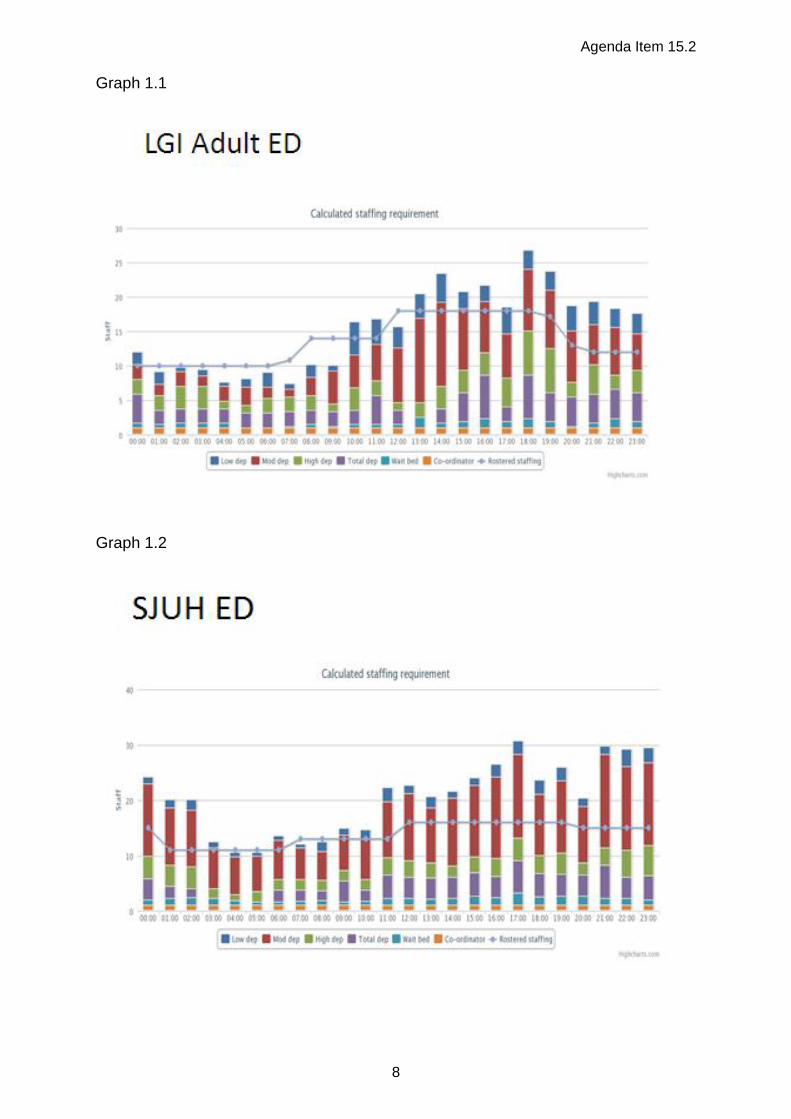
those patients in the department who require continued care in the ED whilst waiting for a bed (and this is shown in the graphs). The information on dependency has then been matched against the staffing the tool suggests should be required to care for that number and dependency of patient : the top of the bar for each hourly total denotes the number of staff the tool suggests is required. The dotted line provides the number of staff who were rostered on duty at that time. A departmental co-ordinator was always present and this is displayed in each slide It can be seen from these graphs that there is clear evidence of the shift patterns in place in the department at the time of the data collection not reflecting peaks in patient attendances. This was undoubtedly the most striking result. Few conclusions can be drawn about the time when the most highly dependent patients arrive, further data runs will be required to confirm any significant trends. Graph 1.0
Agenda Item 15.2
8
Graph 1.1
Graph 1.2
Agenda Item 15.2
9
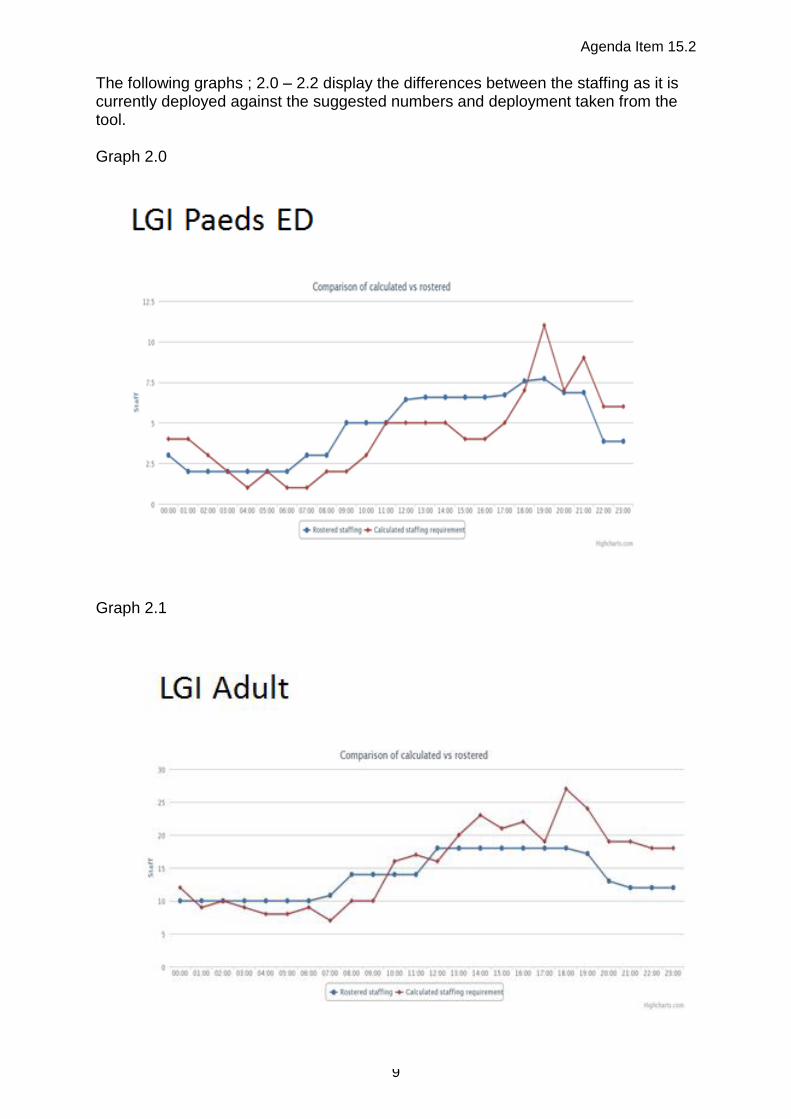
The following graphs ; 2.0 – 2.2 display the differences between the staffing as it is currently deployed against the suggested numbers and deployment taken from the tool. Graph 2.0
Graph 2.1
Agenda Item 15.2
10
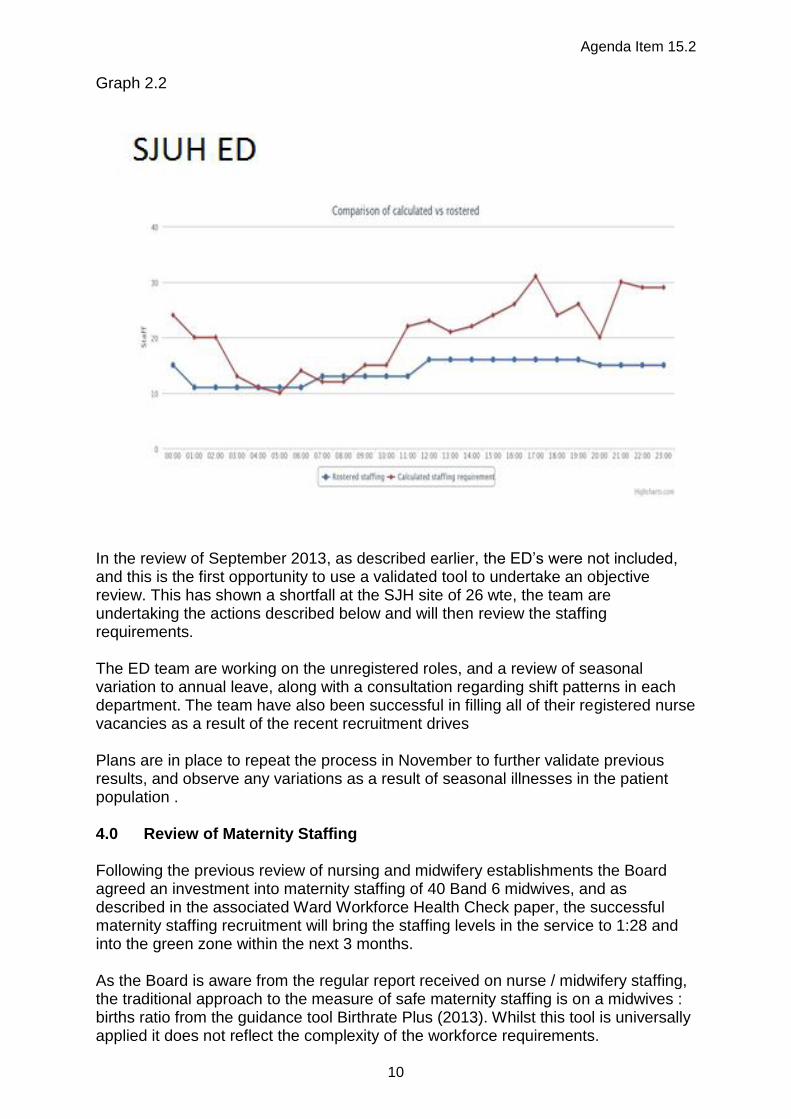
Graph 2.2
In the review of September 2013, as described earlier, the ED’s were not included, and this is the first opportunity to use a validated tool to undertake an objective review. This has shown a shortfall at the SJH site of 26 wte, the team are undertaking the actions described below and will then review the staffing requirements. The ED team are working on the unregistered roles, and a review of seasonal variation to annual leave, along with a consultation regarding shift patterns in each department. The team have also been successful in filling all of their registered nurse vacancies as a result of the recent recruitment drives Plans are in place to repeat the process in November to further validate previous results, and observe any variations as a result of seasonal illnesses in the patient population . 4.0 Review of Maternity Staffing Following the previous review of nursing and midwifery establishments the Board agreed an investment into maternity staffing of 40 Band 6 midwives, and as described in the associated Ward Workforce Health Check paper, the successful maternity staffing recruitment will bring the staffing levels in the service to 1:28 and into the green zone within the next 3 months. As the Board is aware from the regular report received on nurse / midwifery staffing, the traditional approach to the measure of safe maternity staffing is on a midwives : births ratio from the guidance tool Birthrate Plus (2013). Whilst this tool is universally applied it does not reflect the complexity of the workforce requirements.
Agenda Item 15.2
11
4.1 Methodology After considering the variety of tools in use throughout the UK, the Centre for Workforce Intelligence (CfWI), at the request of Health Education England (HEE) were commissioned to work alongside maternity services to devise a workforce planning tool that was accessible, relevant and sufficiently adaptable to be used throughout maternity services in England whatever their size and scope. Earlier this year LTH was afforded the opportunity of taking part in the pilot, which occurred in 14 centres in England of varying sizes. The aim being, to determine if the tool was fit for purpose for general use across all maternity services in England. The tool devised was very different to the ‘traditional’ acuity and dependency tools and worked through pathways of maternity care rather than measuring interactions with patients. The CfWI worked with the current tariff based pathways, 7 in total of which there are 5 antenatal, 1 intrapartum and 1 post natal. The tool required the multi-professional team to identify the minutes of care that each step of the pathway required by the member of staff that would, in the current working arrangements, be expected to deliver that element of care in the pathway. This was achieved through a workshop event. The CfWI provided advice and support to try and ensure consistency of approach across the sites. This information was then totalled across all pathways to provide an indication of the number of staff required to deliver care across the service assuming current levels of activity. The pilot demonstrated that the tool did need refining and there were elements of care that teams delivered that were not included. There has been a de-brief with the CfWI and the tool will be amended to incorporate these. 4.2 Outcome of the Maternity Staffing Review: For LTH the outcomes reflected a number of areas already being addressed by the service, namely: data sourcing, staff roles and competency frameworks. At the time the pilot information was being gathered, the maternity services were in process of updating their IT systems, reviewing the job descriptions of their unregistered workforce, and beginning to discuss how their workforce landscape might look following a robust competency framework review particularly surrounding the role of unregistered staff. Whilst the use of the tool, on this run, will not lead to any changes in the maternity establishment, it has reinforced the current work that is being undertaken both with the recruitment of midwives and the review of the unregistered role The service will re-run the process when the new version becomes available. 5.0 Children’s Ward Acuity and Nurse Staffing Review The staffing for Children’s Wards is guided by the: Royal College of Nursing Skill Mix in Children’s Wards 2012 guidance to the Paediatric Wards and LTH has complied with this.
Agenda Item 15.2
12
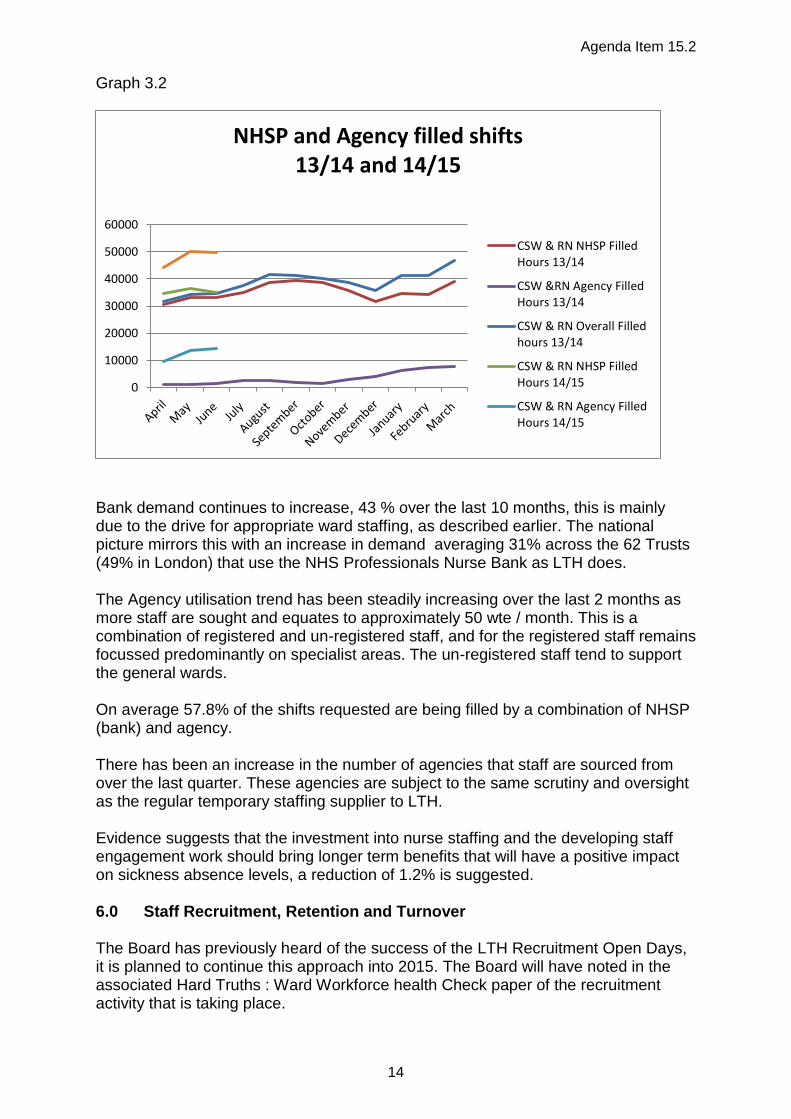
In order to determine if this was the correct application for LTH the team used a version of the Safer Nursing Care Tool that had been adapted to incorporate multipliers sensitive to Children’s requirements. This was the first time that a tool had been used in this environment, and the teams were educated and trained in its’ use, with the quality assurance being provided by the Matrons as in the adult arena. However, the results obtained produced results that suggested nursing establishments could be halved, on review and discussion with the Children’s Senior Nursing Team, the tool had been reasonably accurate in its sensitivity on the acuity of the child and the nursing needs therein, but failed to capture the dependant nature of children at the various ages and stages of illness. Discussions with neighbouring large children’s units have found that where this tool has been used it has yielded similar results, and they feel, for similar reasons. The schedule NICE are working towards suggests that they will be are reviewing tools in this age group in the summer of 2015. Therefore LTH will not re-run this exercise with the Safer Nursing Care Tool until a re-validated version is available. There is an alternative tool, PANDA, used in this age group, it is aligned to the RCN guidance and has been developed by Great Ormond Street. This has been recently revised and is currently being implemented in the Manchester Children’s Service. LTH are liaising with the team to obtain a steer on the efficacy and will review this as a future option for use in LTH. 6.0 Use of Temporary Staffing The average use of temporary staffing has increased from the 5% of 2013/14 to 8.8% or 305 wte on average per month. This is due to the need to maintain safe and effective staffing whilst waiting for the 427 wte new recruits to commence in post in Q3. NHS Professionals are the preferred supplier of temporary staff to LTH, however with the rise in demand for shifts they have been unable to meet all the requirements, as a result LTH has seen a corresponding rise in the use of agency staff. This is expected to reduce as the ward establishments improve over the next 3 months. Temporary staffing demand and supply is detailed in graphs 3.0 – 3.2 below, (please note there are scale differences on each graph)

Agenda Item 15.2
13
Graph 3.0
Graph 3.1
0
5000
10000
15000
20000
25000
NHSP filled shifts 13/14 and 14/15
CSW NHSP Filled Hours13/14
CSW NHSP Filled Hours14/15
RN NHSP Filled Hours 13/14
RN NHSP Filled Hours 14/15
0
1000
2000
3000
4000
5000
6000
7000
8000
9000
Agency filled shifts 13/14 and 14/15
CSW Agency Filled Hours13/14
CSW Agency Filled Hours14/15
RN Agency Filled Hours13/14
RN Agency Filled Hours14/15
Agenda Item 15.2
14
Graph 3.2
Bank demand continues to increase, 43 % over the last 10 months, this is mainly due to the drive for appropriate ward staffing, as described earlier. The national picture mirrors this with an increase in demand averaging 31% across the 62 Trusts (49% in London) that use the NHS Professionals Nurse Bank as LTH does. The Agency utilisation trend has been steadily increasing over the last 2 months as more staff are sought and equates to approximately 50 wte / month. This is a combination of registered and un-registered staff, and for the registered staff remains focussed predominantly on specialist areas. The un-registered staff tend to support the general wards. On average 57.8% of the shifts requested are being filled by a combination of NHSP (bank) and agency. There has been an increase in the number of agencies that staff are sourced from over the last quarter. These agencies are subject to the same scrutiny and oversight as the regular temporary staffing supplier to LTH. Evidence suggests that the investment into nurse staffing and the developing staff engagement work should bring longer term benefits that will have a positive impact on sickness absence levels, a reduction of 1.2% is suggested. 6.0 Staff Recruitment, Retention and Turnover The Board has previously heard of the success of the LTH Recruitment Open Days, it is planned to continue this approach into 2015. The Board will have noted in the associated Hard Truths : Ward Workforce health Check paper of the recruitment activity that is taking place.
0
10000
20000
30000
40000
50000
60000
NHSP and Agency filled shifts 13/14 and 14/15
CSW & RN NHSP FilledHours 13/14
CSW &RN Agency FilledHours 13/14
CSW & RN Overall Filledhours 13/14
CSW & RN NHSP FilledHours 14/15
CSW & RN Agency FilledHours 14/15
Agenda Item 15.2
15
Appendices 3 and 4 provide the detail on both joiners and leavers to LTH at bands 1 – 5 in nursing and midwifery and on turnover at band 2 and 5. LTH has successfully reduced the rate of turnover in the unregistered staff, but has yet to make the same impact within the registered cohort. It can be seen that the numbers of band 5 staff leaving LTH have significantly increased over the year. Heads of Nursing and Matrons are capturing the themes from Exit Interviews and are making changes where they are able. An improvement is expected in retention as the new recruits come into post this will be closely monitored. 7.0 Publication under Freedom of Information Act This paper has been made available under the Freedom of Information Act 2000 8.0 Financial Implications and Risk Investment in nurse staffing has previously been agreed. Vacancies do present an ongoing risk to patient care but the staffing resource is managed on a daily basis by senior nurses to ensure safety, in accordance with the escalation procedure that is displayed on every ward. This has been logged on the Trust Risk Register and an update on the recruitment position and plans has been given by the Chief Nurse to the Audit Committee on 9th July 2014. Rosters are planned 8 weeks in advance, therefore where a planned roster does not demonstrate safe and effective staffing, the CSU Head of Nursing, working in conjunction with their triumvirate teams have an opportunity to review and plan accordingly. 8.0 Equality Analysis All the equality monitoring associated with the recruiting process is not altered by the contents of this paper. Any adjustments that need to be made to accommodate the needs of those being recruited will continue in line with current LTHT policies. 9.0 Summary There is a programme to review the nurse staffing throughout LTH and this will grow as appropriate and validated tools are made available. The ongoing review and escalation of current nursing and midwifery workforce concerns will be through the Ward Workforce Health Check that the Board receive at each meeting. 10.0 Recommendation The Board are asked to receive the report for information and to note the work that is taking place to review ward nursing and midwifery establishments against patient acuity and dependency and the corresponding actions that are taking place at CSU level and organisational level to support and improve nurse staffing.

Agenda Item 15.2
16
Jill Asbury Head of Nursing Education & Workforce 4th September 2014





























