-
8/13/2019 Review of diagnosis and management of dyshidrotic
eczema (a/k/a pompholyx)
1/11
-
8/13/2019 Review of diagnosis and management of dyshidrotic
eczema (a/k/a pompholyx)
2/11
306 o
The aim of this article is to review the clinical features,
dif-ferential diagnosis, and management of pompholyx. A l i
tera-ture search was conducted using the MEDLINE database andthe
terms 'pompholyx' and 'dyshidrotic eczema' f rom January2000 to
April 2010.
1 Ciinicai FeaturesPompholyx or dyshidrotic eczema is a common
disease
affecting palmoplantar skin.f Since palmoplantar skin is r ichin
eccrine sweat glands, it had been suggested that there wasa
relationship between the vesicles and these glands.'- ' Today,the
disease is considered to be a special type of eczema, with
apronounced spongiosis and accumulation of edema fluid inregions
with a thick epidermis and an even thicker overlyinghorny layer.
The spongiotic vesicle is intraepidermal. The acro-syringium of the
sweat glands is not altered by the disease,'^'which makes the term
'dyshidrosis ' a misnomer.
Acco rding to Fo x,'- ' pomp holy x is characterized by
vesiclesand bullae on nonerythematous palmoplantar skin. Based
onnonadherence of many authors to the original clinical
de-scription of this skin condition, Storrs' *' has recently
proposedthe use of the term acu te and recurren t vesicular
handderm atit is . I am not sure whether the terminology will
changein practice or not.
Happ le'^' suggested the term par ap tic eczem a for thiscondit
ion, when pompholyx is el ici ted by the hematogenousaction of an
antigen that has already initiated a T-cell-mediatedeczema response
on the skin.
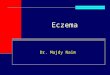
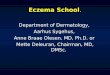
There are two clinical types of presentation: bullous(figure 1)
and vesicular (figure 2 ). Vesicular pom pho lyx isknown as
dyshidrotic eczema in German-speaking countr ies,whereas the
bullous tyjje is named cheiropodop omph olyx. '^ '
Pom pho lyx is associated with itching and bu rning sensa-t
ions. Secondary infection with staphylococci is not in-frequent.
The disease is more common during the warmseasons.'^'
2 PathogenesisPompholyx is seen all over the world, but seems to
be less
common among Asians.'**' In rare cases, there is a
geneticbackground. In a study from China, a gene locus on
chromo-some 18q22.1-18q22.3 between markers D18S465 andD18S1362
could be identified in a large family with an auto-somal dominant
type of pompholyx.'**' However, most cases ofpompholyx are
sporadic.
Patien ts with pom pho lyx show highly significant differein
autonomie vagal modulation under deep respirationspiration and
expiration) , but cardiac autonomie modula
Fig. 1 . Bullous cheiropom pholyx: a) early presentation; b)
later prestion; and c) secondary hemorrhagic bullae in bullous
cheiropom phocontrast to primary hemorrhagic bullae in autoimmune
bulious disease
-
8/13/2019 Review of diagnosis and management of dyshidrotic
eczema (a/k/a pompholyx)
3/11
307
2. Vesicular pompholyx.
Pomp holyx can be associated with atopic dermatit is ,
contact
30%.''^*' In the case of nickel
In another study involving 120 patients with pomp holyx, of
patients had allergic contact dermatitis, and 10% had
mycosis. ' ' ' Other authors have questioned the role of
nickelsensitization. In a study of 398 patients, the relative risk
forvesiculation in nickel-positive individuals was 0.45
comparedwith 3.58 for tinea pedis.'-*'' In a study to identify
factorsassociated with the disease in 100 pompholyx patients in
Togo,West Africa, the odd s ratios were 15.6 for tinea, 12.6 for
ato py ,and 4.5 for hyperhidrosis. richophyton ruhnim was the
mostcommon etiology of the tinea pedis.'-*' '
The blisters and vesicles on the palms do not containinfectious
material. Their formation is thought to be mediatedby an allergic
reaction to the p atho gen , called the id reaction.'-^'
Pompholyx has been observed as a manifestation of infect-ion
with HIV . In this case, antiretro viral therap y w as
beneficialfor the skin disease as well.''^'*'
There is a variety of other aggravating factors, such
asirritants, prolonged use of protective gloves, smoking,
stress,and even endoscopie thoracic sympathectomy for
palmarhyperhidrosis. '-^' Am ong 120 pom pho lyx patients from
Franc e,one-third had hyperhidrosis. ' ' ' Smoking also has a
negative in-fluence on the efficacy of phototherapy, such as
bath-psoralcnplus UVA irradiation (bath-PUVA). ' ' -^ ' However,
diseaseswith disturbed sweating such as Parkinson disease are
notassociated w ith an increased risk of pomp holy x.'- ' In
rarecases, pompholyx can be photoinduced.'-*- '
The cou rse is often chro nic or chronic-cyclic, even in p
atientsin whom the aggravating factors can be avoided. There
mightbe longer periods of remission in these patients, but whenpom
pholyx relapses there is no quick response to treatment.
Contact allergens and drugs associated with pompholyx
immunoglobulins
ilk
=highly active antiretroviral therapy;
AllergenResorcinolDiphencyproneBalsam of Peru,
fragrancesunknownUnknownNickelCobaltChromium from food
RagweedPiroxicamp-phenylenediamineRubber vulcanizerSorbic
acid
IV=intravenous.
FrequencyRareRare
-
8/13/2019 Review of diagnosis and management of dyshidrotic
eczema (a/k/a pompholyx)
4/11
308 o
Table II.Differential diagnoses of
pomphoiyxDiseaseAcropustuiosis of infancyAduit T-celi
leukemia/iympfiomaBuilous impetigoBullous T-cell
iymphomaDyshidrosiform pemphigoidLinear IgA disease with
hemorrhagic) pompholyxEpidermolysis buliosaErythema
muitltormeHand-toot-and-mouth diseaseHerpes intectionHTLV-1
infection aduit cutaneou sT celi iymphoma)Fixed drug
eruptionFriction blistersPemphigus vulgarisPolymorphic dermatitis
in pregnancyPsoriasis pustulosaSAPHO syndromeScabiesSubcorneal
pustular dermatosisVasculitis allergica cutaneous sma ll vessel
vasculitis)
Reference333435363738394041424344454647484933506
HTLV 1= human T-lymph otrophic virus human T-cell leukem ia
virus)-1;SAPHO=synovitis, acne, pustulosis, hyperostosis, and os
teitis.
3. Differential DiagnosisThere are several important
differential diagnoses that have
to be excluded by careful history, clinical evaluation,
histo-pathology, patch testing, microbiologie, and mycologie
in-vestigations (tab le II; figure 3).
Hemorrhagic blisters are suspicious for autoimmune
bullousdisease and Iymphoma'- ' - '- ' but may occur in pompholyx
aswell (figure lc).
4. ManagementManagement is not simple and relapses occur
frequently.
Aggravating factors, such as smoking, should be avoided.Medical
treatment ranges from topical to systemic thera-pies. The targets
for treatment are 3-fold: (i) suppression ofblister formation and
inflammation; (ii) relief from itch; and(iii) prevention or
treatment of infection.f^
As a standardized assessment method for the severity
ofpompholyx, the Dyshidrotic Eczema Area and Severity Index(DASI)
has been developed. It is based on the number of
vesicles per square centimeter, erythema, desquamation, and the
extension of the affected area.'^-*' Th e DA SI ca n alsused to
monitor treatment effects.
Management needs to be adapted to etiopathogenesipatients with
tinea pedis, antifungal therapy is necesPatients with contac t
allergies should avoid identified aller
Fig. 3 . Differential diagnoses of pomp holyx; a) pustular
psoriasis; blous pemp higoid; and c) vasculitis allergica cutaneous
small vesseculitis).
-
8/13/2019 Review of diagnosis and management of dyshidrotic
eczema (a/k/a pompholyx)
5/11
309
4.1 Topical Therapy
4 CortlcosteroldsTopical corticosteroids are the cornerstone of
treatment.ever, pub lished evidence is limited. Veien
etal.'-'''*'reported
120 patien ts with chro nic han d eczema, including 13 with
than palmar or dorsal and palmar.t took to contro l the
dermatitis. ' ' '* ' Imp rovem ent h as been
ol loid dress ing for a l imi ted t i t ^ ^ ' * '4 2
alcineurinInhibitorsTopical tacrolimus was as effective as
mometasone furoate
ointment in a randomized, observer-blind trial in 16
Pimecrolimus 1 cream has been used in combination with
treated w ith topical pimecro limus 1% cream und er
l significance in this stud y (p = 0.068).'''*'
4 3 exaroteneGelBexarotene is a retinoid X receptor agonist that
has been
a. The compou nd is contraindicated in premen opausa l I-II
randomized,
1% gel alone and in combina-on with a hydrocortisone 1% ointment
or a mom etasone
e 0.1% ointm ent, 55 patients with severe chronic ha nddaily.
The response ra te of patients achieving at least 50%SI) was 79%
for bexarotene gel alone, 85% for the com-
n with hydrocortison e. An improvem ent of the HEA SI score
tene alone, in 38% of patients treated with bexaroten e an dmom
etasone furoate, and in 14% of patients with the combi-nation of
bexarotene and hydrocortisone. In a subgroup of'other types of
eczema/dyshidrotic eczema,' the clearance ratewith bexarotene gel
monotherapy was 50%. Adverse effectsrelated to bexarotene gel
included burning, stinging, irritation,and flare of dermatitis. '*
' This study reveals that the combi-nation of bexarotene gel with a
topical mid-potency cortico-steroid such as mometasone furoate is
beneficial, whereasweaker corticosteroids do not add any benefit in
such a com-bination. It has not been evaluated systematically
whether morepotent corticosteroids in combination with bexarotene
gelwould further improve the outcome in pompholyx.
4.2 Systemic Therapy ;4 2 CorticosteroidsThe basic systemic
therapy in bullous pom pholy x consists of
systemic corticosteroids. Depending on the severity and thearea
affected, initial dosages between 40 and lOOmg/day areemplo yed.' '
' ' The dosage is gradu ally tapered after blister for-mation
ceases. Other authors recommend the use of intra-muscular tr
iamcinolone acetonide 40-80 mg . ' ' ' However, thistreatment has
never been investigated by randomized, pro-spective trials.
Systemic corticosteroids are rarely advisable forlong-term use
because of undesirable adverse effects.
4 2 2ImmunosuppressantsIn the case of recalcitrant pompholyx,
other immuno-
suppressive drugs have occasionally been used, such as aza-thiop
rine 100 -150 mg /day,'^ ' ' low-dose metho trexa te (initially15-2
5m g once a week), ' - ' and m ycoph enolate mofeti
Cyclosporine (ciclosporin) was used in four patients
withvesicular pompholyx. A star t ing dosage of at least2.5 mg/kg
/day w as necessary to induce a respo nse. R elapse iscommon after
withdrawal of the treatment. '^ ' These data arenot sufficient to
recommend any of the systemic therapiesahead of any of the others
based on their efficacy and safetyprofile.
4 2 3RetmoidsAlitretinoin (9-cis-retinoic acid) is a retinoid
for systemic
use. I t has been described as a panagonist since the
compoundactivates retinoid X receptors as well as all retinoic acid
re-ceptors. Headach e and m ucocu taneous adverse effects are
seenas with other oral retinoids. Because of teratogenicity, all
oral
-
8/13/2019 Review of diagnosis and management of dyshidrotic
eczema (a/k/a pompholyx)
6/11
310
retinoids are strictly contraindicated in premenopausal w
omenwho are not using sufficient contraception.'^^l
In a European, randomized, double-blind, placebo-controlled,
multicenter trial, 319 patients with chronic handdermatitis
refractory to standard therapy were evaluated.'^^'In a four-armed
study design, patients received either placeboor alitretinoin at
dosages of lOmg,20mg,or40 mgonce dailyfor 12 weeks. Responders were
followed up for another3 months. Alitretinoin led to a significant,
dose-dependentimprovement of the disease status in up to53%of
patien ts, withan up to 70% reduction in disease symptom s and
signs. In thistrial, a group of70patients w ith pompholyx was
included; theresponse rate in this subgrou p was not statistically
differentbetween placebo and alitretinoin.t^^'A recent paper repo
rted the results of a randomized, do uble-blind,
placebo-controlled, multicenter trial in ten Europeancountries and
in Canada.'''^' A total of 1032 patients withrefractory chronic
hand derma titis (eczema) were included. Thetreatment was organized
in three arms, i.e. alitretinoin 10 mgor30 mgor placebo once a day
for 24 weeks. Clear or almost clearhands were achieved in 48% of
alitretinoin-treated patientsversus17%of placebo recipients. There
were mo re responses inthe 30 mg group compared with the lOmg
group. The studyincluded a grou p of377patients with pompholyx. In
this group,the response rate was 16%in the placebo recipients,23%in
thepatients receiving alitretinoin lOmg/day, and33%in the gro
upreceiving alitretinoin 30mg/day.t^^l
In conclusion, although oral alitretinoin is effective in
re-calcitrant hand eczema in general, it is of limited efficacy
inpompholyx. A combination therapy with topical cortico-steroids
could achieve higher response rates; however, this hasyet not been
evaluated in a controlled clinical trial.
4 2 4 iologiesA 40-year-old woman with a 6-yearhistory of
recalcitrant
atopic cheiropompholyx was treated with subcutaneous inject-ions
of the tumor necrosis factor-a inhibitor etanercept25mgtwice
weekly.'^ ' At a 6-week follow-up, the pompholyx hadcleared.
Remission was sustained for 4 months, after whichtime the patient
experienced a flare-up. The dosage of etaner-cept was doubled, but
was ineffective and was, therefore,eventually discontinued.I^**'
Further investigations are neededwith the use of biologies for p
ompho lyx.
4 2 5 AntihistaminesAntihistamines have been used to control
accompanyingpruritus, although there is no proof of their efficacy
in pom-
pholyx. Sodium cromoglicate (disodium cromoglycatefound to be
more effective in the treatment and preventinickel-sensitive
pompholyx than a low-nickel diet by dishing the intestinal
nickeluptake.t ** Th euseof sodium cglicate raises several
questions. First, since only a prtion of pompholyx patients are
nickel sensitized, woulddrug be ineffective in the other patients?
Second, howshould sodium cromoglicate be used for secondary prevein
nickel-sensitized patients? Probably as a life-long treatbut there
are no scientific data to support long-term pre ve
4.3 Botulinum Toxin
Botulinum toxin A (BTXA) shows potent anhidrotitivity, and
sweatingisan aggravating factor in pompholypilot study with
left-right c omp arison, intrac utaneo us
injofBTXA(100UofBotox[AUergan, Inc., Irvine, CA, Uone palm on day
1) was used in addition to topical costeroids. Among the six
patients who completed the 8-trial, the DASI was significantly
lower, and itching and vlation disappeared earlier in the hand
treated with BTXA
Ano ther study involving ten patients compared the effBTXA alone
(mean dose of 162 U of Botox per palm ohand) with the untreated
side as contro l. Seven ofte n paexperienced a good to very good
effect on vesicular pompand a decrease in itching.'^'' Other
reports also mentioneability of BTXA to improve itch, vesiculation,
andthema.t -- - ' Pain on injection is a comm on adverse
effeclimits the use of BTXA in general.
4.4 Phototherapy and PhotochemotherapySelective UVB phototh
erapy (300-320 nm) combined
balneotherapy was found to be more effective in
palmopdermatoses, including pompholyx, than broad-spectrum
(280-320nm .t 41 Narrow-band UVB (311nm) and U(340-400 nm)
irradiation have been proven to be superbroad-band UVB for certain
indications.'^^'
Systemic photochemotherapy with PUVA (320-^00 neffective in
vesicular pompholyx, although it has theadvantage of generalized
photosensitivity and adverse eon the gastrointestinal tract by the
photosensitizer methox(8-methoxypsoralen; 8-MOP). To reduce the
risk of unwadverse effects, there have been modifications to the
clasystemic PUVA therapy, such as bath-PUVA and cPUVA. For
bath-PUVA,8-MOPis used in a water bathto irradiation. Cream-PUVA
employs a cream containinphotosensitizer applied 20 minutes prior
to UV exposure
-
8/13/2019 Review of diagnosis and management of dyshidrotic
eczema (a/k/a pompholyx)
7/11
311
Bath-PUVA is an effective treatment modality for palmo-
Cream-PUV A is as effective as bath-PUVA in the treatmentTopical
PUVA with8 MOPhas been compared with UVA
UVA-1 irradiation was found to be effective in vesicular
27patients with vesicular
III Evidence-based medicine in pompholyx
num toxin A
inhibitors
Evidence level^3^4a' '
224a332222
Levels of evidence-base d medicine in clinical studies. Level
:evidence isavailable for meta-analysis from several randomized
controlled studies;level 2: evidence is available from at least one
random ized controlledtrial;level 3: evidence is available from
good mthodologie studies withoutrandomization; level 4a: evidence
is available from clinical case reports;level 4b: this represents a
consensus of respected experts or expertcommittees.Mostly with
topical corticosteroids.
=psoralen plus UVA.
Table IV General advice for hand an d foot care for patients
with pom pholyxWash hands and feet as infrequently as possibleAvoid
soaps, and direct contact with household cleansers, fresh
fruits,and fresh meatDry hands an d feet carefullyUse protective
gloves for hair care, including shampooingUse protective plastic
gloves only with white cotton gloves beneathUse cotton socks and
change them regularlyStop smoking
4.5 RadiotherapyGrenz rays and conventional superficial x-rays
have beenused either alone or in comb ination w ith topical
corticosteroids
for refractory hand dermatitis (eczema). In a double-blindstudy,
conventional x-rays (300 rad) were superior to
Grenzrays.'^''Complete remission of pompholyx is also possible
withlow-dose external beam m egavoltage radiation.' ^'
4.6 Tap V^ater lonotophoreslsTap water iontophoresis is an
effective measure to control
excessive sweating ofpalmsand soles. In a study of2 patientswith
pomph olyx, it was more effective than corticosteroid-freetopical
treatment alone.'**-^'
In a study with 20 pompholyx patients, tap water ionto-phoresis
resulted in faster relief of symptoms, particularly itch,than
topical corticosteroids alone. There was a statisticallysignificant
difference in the relapse-free interval, i.e. 6 versus2 '***
5 ConclusionIt is surprising that although pompholyx is a common
dis-
ease,relatively few randomized controlled trials of its treatm
enhave been performed and published. For an overview
onevidence-based medicine for pompholyx see table III. Thecurrent
best treatment for pompholyx is a combination oftopical and
systemic therapy. In practice, the most commoncombination used is
topical and short-term systemic cortico-steroids. However, no
randomized study has been published inthe international medical
literature for such a treatment. Goodproof ofevidenceis available
for topical d rugs such as corticosteroids, calcineurin inhibitors,
and bexarotene.
Among phototherapies, PUVA and high-dose UVA-1 seemto be equal
in efficacy, with probably a more balanced risk-
-
8/13/2019 Review of diagnosis and management of dyshidrotic
eczema (a/k/a pompholyx)
8/11
312
benefit ratio for UVA-1.However, the long-term risks are notwell
known, and the equipment is more expensive, for
high-doseUVA-1.Systemic PUVA does not offer any benefit com-pared
with topical PUVA andUVA-1.
Ifthereis aggravation ofthedisease by focal hyperhidrosis,tap
water iontophoresis and BTXA have been proven to notonly improve
abnormal sweating but also to have beneficialeffects on pompholyx.
A better understanding of the mechan-isms of action of botulinum
toxin may be helpful in developinga new class of anti-inflammatory
drugs.
In systemic therapy, corticosteroids remain the cornerstoneof
treatment, although alitretinoin has recently shown efficacy.In
recalcitrant cases, a combination of corticosteroids
withimmunosuppressants or a complete switch to immunosup-pressants
may be useful but none of the systemic pharma-cotherapies
(including biologies) has been evaluated incontrolled trials.
Pharmacologie treatment (and other treatments as well)should be
accompanied by general advice for patients withpompholyx (table
IV).
The current situation in pompholyx dem onstrates the urgentneed
for controlled trials, in particular for systemic
treatmentoptions.
cknowledgmentsNo sources of funding were used to assist in the
preparation of this
review. The author has no conflicts of interest that are
directly relevant tothe content of this review.
eferences1. G uillet M H. Wierzbicka E . Guillet S, et al. A
3-year causative study of pom-pholyx in 120 patients. Arch Dermatol
2007; 143 (12): 1504-82. Fox T. Dyshidrosis: cheiro-pom pholyx
[letter]. Lancet 1876; I: 6513. Kutzner H, Wurzel RM, Wolff HH. Are
acrosyringia involved in the patho-
genesis of dyshidrosis ? Am J D ermatopa thol 1986; 8 (2);
109-164. Storrs FJ. Acute and recurrent vesicular hand dermatitis
not pompholyx ordyshidrosis. Arch Dermatol 2007; 143 (12):
1578-805. Happle R. Paraptic eczema: why a new name? [in German].
Hautarzt 1994;45(1): 1-36. WoUina U. Abdel Naser MB.
Pharmacotherapy of pomphoiyx. Expert OpinPharm acother 2004; 5 (7):
1517-227. Tamer E, Ilhan MN , Polat M . et al. Prevalence of skin
diseases among pdiatriepatients in Turkey . J Dermatol 2008; 35
(7); 413-88. Lee CS. Lim H W. Cutan eous diseases in Asians.
Dermatol Clin 2003;21 (4):668-779. Chen JJ. Liang YH, Zhou FS. et
al. The gene for a rare autosomal dominantform of pompholyx m aps
to chromosome 18q22.1-18q22.3.J Invest Dermatol2006; 126 (2):
300-4
10. Boettger MK, Br KJ, Dohrmann A, et al. Increased vagal
modulation inatopic derm atitis. J Derma tol Sei 2009; 53 (1):
55-9
11. Barbaud A. Reichert-Penetrat S, Trechot P . et al.
Sensitization to resora prescription verrucide preparation; unusual
systemic clinical featuprevalence [in F rench]. Ann Dermatol
Venereol 2001; 128 (5): 615-8
12. Buckley DA, Keane FM, Munn SE. et al. Recalcitrant viral
warts trediphencypron e imm unotherapy. Br J Dermatol 1999; 141
(2); 292-613.Jain VK, Aggarwal K, Passi S, et al. Role of contact
allergens in pom
J Dermatol 2004; 31 (3); 188-9314. Meneghini CL, Angelini G.
Contact and microbial allergy in pomContact Dermatitis 1979; 5(1):
46-5015. Colebunders R .Zolfo M.L yne nL. Severe dyshidrosis in two
patients w
infection shortly after starting highly active antiretroviral
therapy. DOnline J 2005; 11 (2); 31
16. Uyttendaele H, Obadiah J, Grossmann M. Dyshidrotic-like
spongiotiatitis after intravenous immunoglobulin therapy. J Drugs
Dermato2 (3): 337-41
17. Hindsen M . Bruze M, Christensen OB. Individual variation in
nickel pareactivity. Am J Conta ct D ermat 1999; 10 (2); 62-718.
Adachi A, Horikawa T. Pompholyx of the infant possibly induced by
s
metal allergy to chromium in mother's milk [in .lapanese].
Aerugi 2007703-819. Semhoun-Ducloux S. Ducloux D, Mignel JP.
Mycophenolate mofetil-
dyshidrotic eczema [letter]. Ann Intern Med 2000; 132 (5);
41720. Mller H . Spirn A, Svensson A, et al. Con tact allergy to
theA slcrwra
Ambrosia arlemisiifolia L (ragweed) in sesquiterpene
lactone-spatients in southern Sweden. Contact Dermatitis 2002; 47
(3): 157-6021 . Braunstein BL. Dy shidrotic eczema associated with
piroxicam sensitivity. Cu tis 1985; 35 (5): 485-622. Lazzarini R.
Duarte I. Marzag ao C. Con tact derm atitis of the feet: a 53
cases. Dermatitis 2004; 15 (3): 125-3023. Grange-Prunier A, Bezier
M, Perceau G, et al. Tobacco contact de
caused by sensitivity to sorbic acid [in French]. Ann Dermatol
Venereo135(2); 135-824. Gawkrodger DJ. Cook SW, Fell GS. et al.
Nickel dermatitis: the reacoral nickel challenge. Br J Dermatol
1986; 115(1): 33-825 . Bryld LE, Agner T, Menn T. Relation between
vesicular erupt
the hands and tinea pedis, atopic dermatitis and nickel allergy.
ActVenereol 2003;83 (3): 186-8
26. Pitch P, Boukari M, Tchangai-Walla K. Factors associated
withplantar or plantar pompholyx: a case-control study [in French).
Annatol Venereol 2006; 133 (2): 139-43
27. Nowicki R. Allergic phenomena in the course of
dermatomycoses [in Pol Merkur Lekraski 2003; 14 (84): 532-428 .
MacConnachie AA, Smith CC. Pompholyx as a manifestation of HIVion,
response to antiretroviral therapy. Acta Derm Venereol 2007;
378-929. Niinai H. Kawamoto M, Yuge O. Severe pompholyx following
endthoracic sympathectomy for palmar hyperhidrosis. Interact
CarThorac Surg 2004; 3 (4): 593-530. Douwes KE , Karrer S. Abels C.
et al. Does smoking influence the effbath-PUVA therapy in chronic
palnioplantar hand eczema? PhotodPhotoimmunol Photomcd 2000; 16(1):
25-931. Hirayama M. Sweating dysfunctions in Parkinson's disease. J
Neuro253 Su ppl. 7: V1142-732. Ma nI,lb bo tson SH . Fergusan
J.Photoinduced pompholyx: a report ofJ Am Acad Dermatol 2004; 50
1):55-6033. Braun-Falco M, Schnopp C, Abeck D. Palmoplantar
vesicular leschildhood [in German]. Hautarzt 2003;54 (2): 156-934.
Stoyama M, Yamamoto S. Kanzaki T. Adult T-cell
leukaemia/lympresenting with digital gangrene. Dermatology 1997;
195 (2): 150-2
-
8/13/2019 Review of diagnosis and management of dyshidrotic
eczema (a/k/a pompholyx)
9/11
313
Cole C, Gazewood J. Diagnosis and treatment of impetigo. Am Fam
Physi-cians 2007; 75 (6): 859-64
Hliot I. Beylot-Barry M, VergierB .etal.Cutaneo us T-cell
Iymphoma buliosa;2 cases [in French). Ann Dermatoi Venereol
2003;130 (6-7); 639-42Sugimura C. Katsuura J. Motiue T. et al.
Dyshidrosiform pemphigoid; reportof a case. J Dermatoi 2003;30 (7);
525-9
Duhra P, Charles-Holmes R. Linear IgA disease with haem
orrhagicpompholyx and dapsone-induced neutropenia. Br J Dermatoi
1991; 125 (2);172-4
Uitto J. Epidermolysis hullosa; prospec ts for cell-mediated
thera pies. J InvestDermatoi 2008; 128 (9); 2140-2
Parillo SJ. Stevens-Johnsons syndrome and toxic epidermal
necrolysis. CurrAllery Asthma Rep 2007; 7 (4); 243-7
Sutton-Hayes S. Weisse ME, Wilson NW, et al. A recurrent
presentation ofhand, foot and mouth disease. Clin Pediatr (Phila)
2006; 45 (4); 376-7 Fletcher PG, Sterling JG. Recurrent herpes
simplex virus type2infection of the
hand complicated by persistent lymphoedema. Australas J Dermatoi
2005;46(2); 110-3 Wh ittakerS J.Ng YL . Rustin M .eta l.
HTLV-1-associated cutaneous disease; a
clinicopathological and molecular study of patients from the
U.K. Br JDerm atoi 1993; 128 (5); 483-92
Gup ta R. D rugs causing fixed drug eruptions; confirmed by
provocation tests[letter].Indian J Dermatoi Venereol Leprol 2003;69
(2); 120-1
. Woilina U. Disorders caused by physical and chemical damage.
In; Braun-Falco O, Plewig G, Wolff H H, et al., editors.
Dermatology and venerology.6th ed. Heidelberg, New York; Springer,
2007; 571-85
Borradori L, Harms M. Podopompholyx due to pemphigus vulgaris
andTrichophyton rubrum infection; report of an unusual case.
Mycoses 1994;37(3-4); 137-9
Normand F. Amiingaud P, Estve E. Dyshidrosis and acral purpura
duringpolymorphic de rmatitis in pregnancy; 2 cases. Ann Dermatoi
Venereol 2001;128 (4);531-3
. Barta U. Wollina U. Psoriasis der Haut. In; Wollina U, Hein G.
Knopf B,editors. Psoriasis und Gelenkerkrankung en; Pa thogenese.
Klinik. Diagnostikund Therapie der psoriatischen Osteoarthropathie.
Jena; Gustav FischerVerlag, 1996; 38-48 Berbis P. Palmoplan tar
pustulosis [in French]. Rev Prat 1991;4 (22); 2165-8 Cheng S,
Edmonds E, Ben-Gashir M, et al. Subcorneal pustular dermatosis
50 years on. Clin Exp Dermatoi 2008; 33 (3); 220-33 Duhra P.
Ryatt KS. Haemorrhagic pompholyx in bullous pemphigoid. Clin
Exp De rmato i 1988; 13 (5); 342-3 Barth JH. Venning VA.
Wojnarowska F. Palmoplantar involvement in auto-
immune blistering disorders; pemphigoid, linear IgA disease and
herpesgestationis. Clin Exp Dermatoi 1988; 13 (2); 85-6 Vocks E,
Plotz SG, RingJ The D yshidrotic Eczema Area and Severity Index;
a
score developed for the assessment of dyshidrotic eczema.
Dermatology 1999;198 (3); 265-9
Veien NK, 01holm Larsen P, Thestrup-Pedersen K, et al.
Long-term, inter-mittent treatment of chronic hand eczema with
mometasone fuorate. Br JDermatoi 1999; 140 (5); 882-6. Harper J.
Topical corticosteroids for skin disorders in infants and
children.
Drug s 1988; 36 Suppl. 5; 34-7 Volden G. Successful treatment of
chronic skin diseases with clobetasol pro-pionate and a
hydrocolloid occlusive dressing. Acta Derm Venereol 1992;
72(1);69-71 Schnopp C, Remling R. M hrenschlger M, et al.
Topical tacrolimus
(FK 506) and mometasone furoate in treatment of dyshidrotic
palmareczema; a randomized, observer-blinded trial. J Am Acad
Dermatoi 2(K)2;46(1);73-7
58. Schurmeyer-Horst F, Luger T, Bhm M. Long-term efficacy of
occlusivetherapy with topical pimecrolimus in severe dyshidrosiform
hand and footeczema [letter]. Dermatology 2007; 214 (1); 99-100
59. Belsito DV, Fowler Jr JF. Marks Jr JG . et al. Multicenter
Investigator Grou ppimecrolimus cream 1%; a potential new treatment
for chronic hand derm-atitis.Cu tis 2004; 73 (1); 31-8
60. Hanifin JM . Stevens V, Sheth P. et al. Novel treatment of
chronic severe handdermatitis with bexarotene gel. Br J Dermatoi
2004; 105 (3); 545-53
61. Scerri L. Azathioprine in dermatological practise; an
overview with speciaemphasis on its use in non-bullous inflammatory
dermatoses. Adv Exp MedBiol 1999; 455; 343-8
62. Egan CA. Rallis TM, M eadows K P. et al. Low-dose oral
methotrexate treatment for recalcitrant palmoplantar pompholyx. J
Am Acad Dermatoi 1999;40(4);612-4
63. Pickenacker A, Luger TA, Schwarz T. Dyshidrotic eczema
treated withmycophenolate mofetil. Arch Dermatoi 1998; 134 (3);
378-9
64. Reitamo S, Granlund H. Cyclosporin A in the treatment of
chronic dermatitiof the hands. Br J Dermatoi 1994; 130 (1);
75-8
65 . Cheer SM, Foster R H. Alitretinoin. Am J Clin Derm atoi
2000; (5): 307-1466. Ruzicka T, Larsen F G. Galewicz D, et al. Oral
alitretinoin (9-cis-retinoic acidtherapy for chronic hand
dermatitis in patients refractory to standard therapy; results of a
randomized, double-blind, placebo-controlled, multicentertrial.
Arch Dermatoi 2004; 140 (12); 1453-967. Ruzicka T, Lynde CW, Jemec
GBE, et al. Efficacy and safety of oraalitretinoin (9-cis retinoic
acid) in patients with severe chronic handeczema refractory to
topical corticosteroids; results ofa randomized doubleblind,
placebo -controlled , multicen tre trial. Br J Derma toi 2008; 158
(4)808-1768 . Ogden S, Clayton TH, Goodfield MJD. Recalcitrant hand
pompholyx; variable response to e tanercept. Clin Exp D ermatoi
2005; 31 (1); 145-669. Pigatto PD , Gibelli E, Fumagalli M, et al.
Disodium cromoglycate versus die
in the treatment and prevention of nickel-positive pompholyx.
ContactDerm atitis 1990; 22 (1); 27-3170. Wollina U, Karamfilov T.
Adjuvant botulinum toxin A in dyshidrotic handeczema; a controlled
prospective pilot study with left-right comparison. J EurAcad D
ermatoi Venereol 2002; 16 (I); 40-271. Swartling C. Naver H,
Lindberg M, et al. Treatment of dyshidrotic handdermatitis with
intradermal botulinum toxin. J Am Acad Dermatoi 200247 (5);
667-7172. Bansal C, Omlin KJ, Hayes CM, et al. Novel cutaneous uses
for botulinum
toxin type A. J C osmet D ermatoi 2006; 5 (3); 268-7273.
Kontochritopoulos G, GregoHou S, Agiasofitou G, et al. Regression
of relapsing dyshidrotic eczema after treatment of concom itant hyp
erhidrosis withbotulinum toxin-A [letter]. Dermatoi Surg 2007; 33
(10); 1289-9074. H unziker T. Haudenschild-Falb E, Schmidli J, et
al. Aq ua- SU P in chronipalmop lantar d ermatoses [in German]. H
autarzt 1987; 38 (3); 165-775. Krutmann J. Phototherapy for atopic
dermatitis. Clin Exp Dermatoi 2()(K)
25 (7); 552-876. Grundmann-KoUmann M, Behrens S, Peter RU, et
al. Treatment of severrecalcitrant dermatoses of the palms and
soles with PUVA-bath versuPUVA-cream therapy. Photodermatol
Photoimmunol Photomed 199915(2); 87-977. Grattan CE, Carmichael AJ,
Shuttleworth GJ, et al. Comparison of topica
PUVA with UVA for chronic vesicular hand eczema. Acta Derm
Venereo1991;71 (2); 118-22
78. Schmidt T, Abeck D, Boeck K, et al. UVA irradiation is
effective in treatmeof chronic vesicular hand eczema. Acta Derm
Venereol 1998; 78 (4); 318-9
79. Polderman MC, Govaert JC, le Cessie S, et al. A double-blind
placebocontrolled trial of UVA-1 in the treatment of dyshidrotic
eczema. Clin ExpDermatoi 2003;28 (6); 584-7
-
8/13/2019 Review of diagnosis and management of dyshidrotic
eczema (a/k/a pompholyx)
10/11
314
80 . Petering H, BreuerC.Herbst R. et al. Comparision of
localized high-doseUVAl versus topical cream
psoralen-UVAfortreatment of chronic vesiculardyshidrotic eczema.J
Am Acad D erma tol 2004; 50 1): 68-7281. Jansen GT. Grenz rays:
adequa te or antiquated?JDermatol Surg Oncol 1978:4 8): 627-982.
Stambaugh MD , DeNittisAS,Wallner PE, etal.Complete remission of
refractorydyshidrotic eczema with the useofradiation therapy .
Cutis 2000; 65 4): 211-483 . Odia S, Vocks E, Rakoski J. et al.
Successful treatment of dyshidrotic
hand eczema usingtapwater iontophoresis w ith pulsed curren t.
Acta DermVenereol 1996; 76 6): 472-4
84. Wollina U, Uhlemann C, Elstermann D, et al.Therapy of
hyperwith tap water iontophoresis: positive effect on healing time
aof recurrence in hand-foot eczema [in Germ an]. Hautarzt 1998:1 9
13
Correspondence: Prof Dr Uwe Wollina Department of Dermaand
Allergology, Academic Teaching Hospital Dresden
FriedricFriedrichstrasse 41 ,01067 Dresden, Germany.E-mail:
[email protected]
1 ; i
-
8/13/2019 Review of diagnosis and management of dyshidrotic
eczema (a/k/a pompholyx)
11/11
Copyright of American Journal of Clinical Dermatology is the
property of ADIS International Limited and its
content may not be copied or emailed to multiple sites or posted
to a listserv without the copyright holder's
express written permission. However, users may print, download,
or email articles for individual use.