Embed Size (px)
Citation preview
Review of Anticonvulsant Medications: Traditional and Alternative UsesAndrea Michel, PharmD, CACP
Objectives
Review epidemiology of epilepsy
Classify types of seizures
Discuss non-pharmacologic and pharmacologic treatment options for epilepsy
Outline common adverse reactions and prevalent drug-drug interactions associated with anticonvulsant medications
Highlight important considerations for special patient populations with epilepsy
State appropriate plan for anticonvulsant medication therapy discontinuation
Epilepsy
Definition
Central nervous system disorder in which brain activity becomes abnormal, causing seizures or periods of unusual behavior, sensations, and sometimes loss of awareness
Epilepsy diagnosis requires: History of >2 seizures at least 24 hours apart
OR
1 seizure with significant risk of recurrence (e.g. recent stroke, brain structure abnormality, abnormal electroencephalography (EEG))
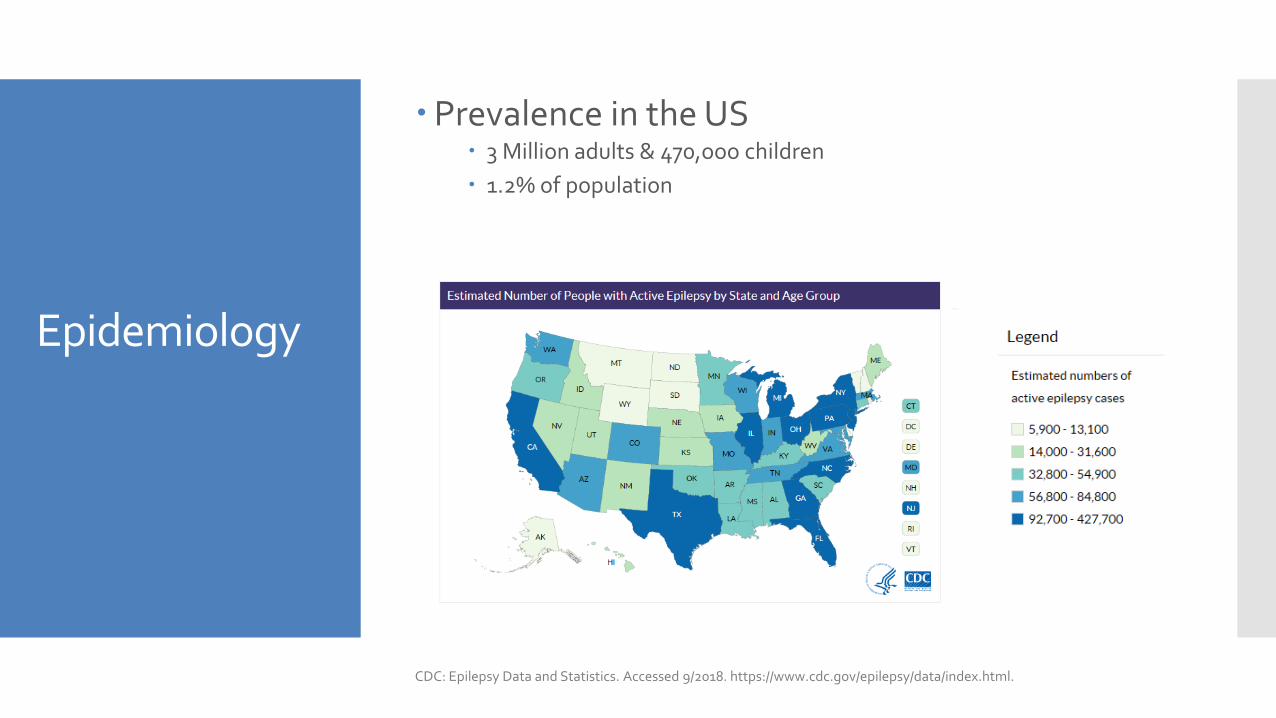
Epidemiology
Prevalence in the US 3 Million adults & 470,ooo children
1.2% of population
CDC: Epilepsy Data and Statistics. Accessed 9/2018. https://www.cdc.gov/epilepsy/data/index.html.
Causes
Mechanical – birth injuries, head trauma, tumors, stroke
Metabolic – electrolyte disturbances, hypoglycemia
Genetic Influence – familial neonatal seizures, juvenile myoclonic epilepsy (JME)
Other – fever, infectious disease
Causes
Drugs
Recreational drugs
Carbapenems
Meperidine
Local anesthetics
Metoclopramide
Theophylline
Tricyclic antidepressants
Anticonvulsant therapy: carbamazepine, phenytoin, phenobarbital
Diagnosis
Medical History
Physical and Neurological Exam
Lab tests
Electroencephalogram (EEG)
Magnetic resonance imaging (MRI)
Classification of Seizures
Focal seizure
Focal Seizure
One hemisphere of the brain
Unilateral, asymmetric movements
Associated with an aura
Other terms: simple partial seizure, complex partial seizure, secondarily generalized seizure
Generalized seizure
Generalized seizure
Begins simultaneously in both brain hemispheres
Types of generalized seizures:1. Absence
2. Myoclonic
3. Tonic-clonic
4. Clonic
5. Tonic
6. Atonic
Unknown onset seizure
Unknown seizure
Reserved for seizures that are unwitnessed
Occur while patient is asleep
Observers cannot provide an adequate description
Status epilepticus
Status Epilepticus
Seizure that lasts >20 minutes OR >2 seizures with incomplete recovery of consciousness between episodes
Medical emergency
Up to 20% mortality rate

Treatment of Epilepsy
Treatment
Non-PharmacologicSurgical Procedures
Vagus Nerve Stimulation
Dietary Restrictions
PharmacologicAnticonvulsant medication therapy
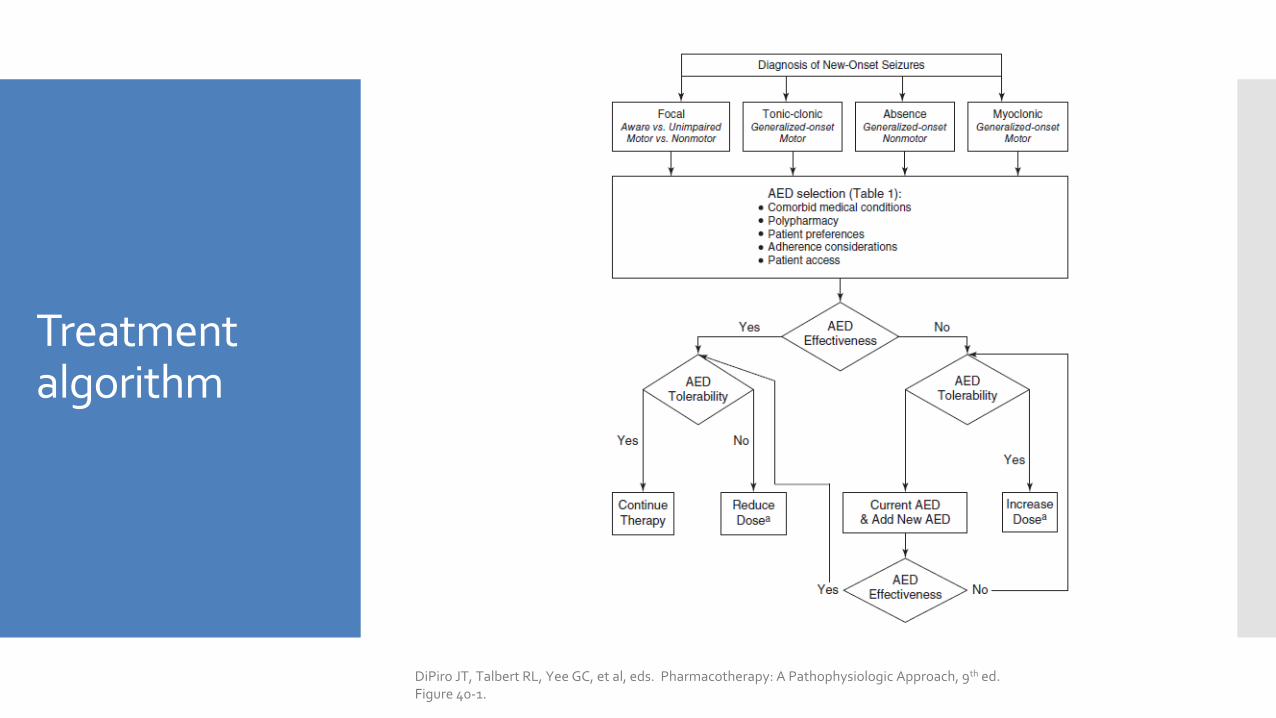
Treatment algorithm
DiPiro JT, Talbert RL, Yee GC, et al, eds. Pharmacotherapy: A Pathophysiologic Approach, 9th ed. Figure 40-1.
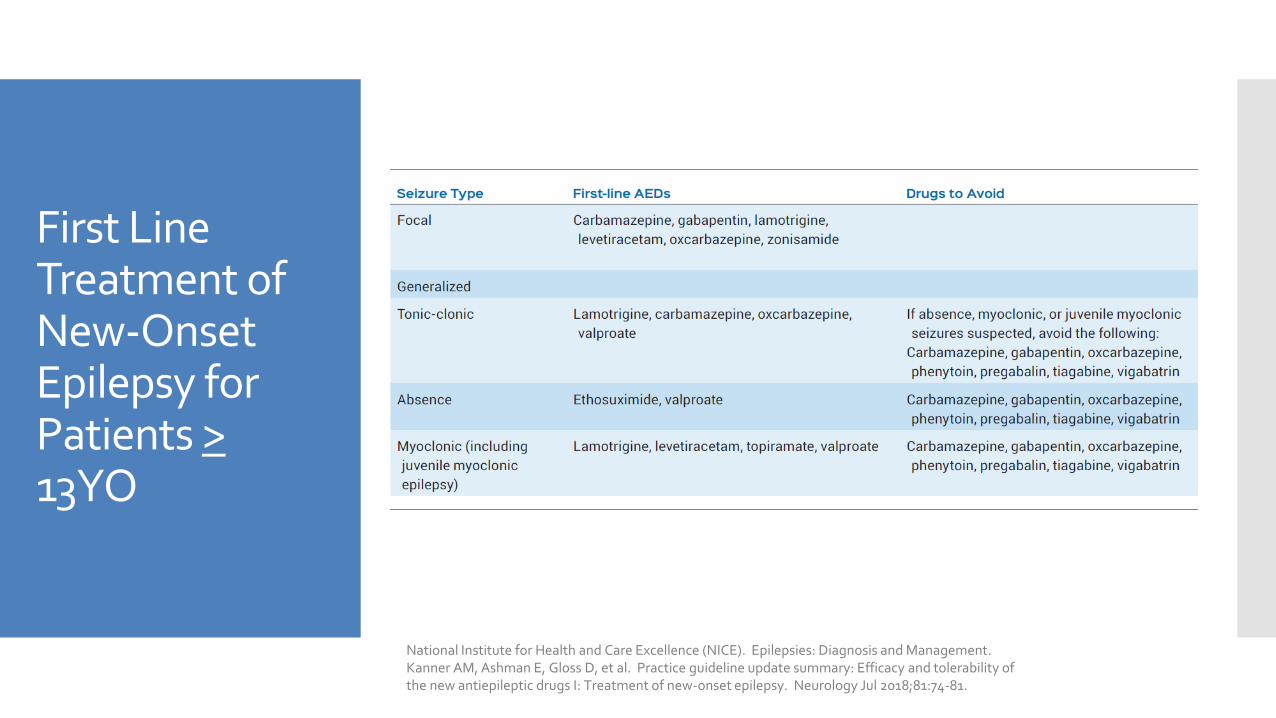
First Line Treatment of New-Onset Epilepsy for Patients >13YO
National Institute for Health and Care Excellence (NICE). Epilepsies: Diagnosis and Management.Kanner AM, Ashman E, Gloss D, et al. Practice guideline update summary: Efficacy and tolerability of the new antiepileptic drugs I: Treatment of new-onset epilepsy. Neurology Jul 2018;81:74-81.
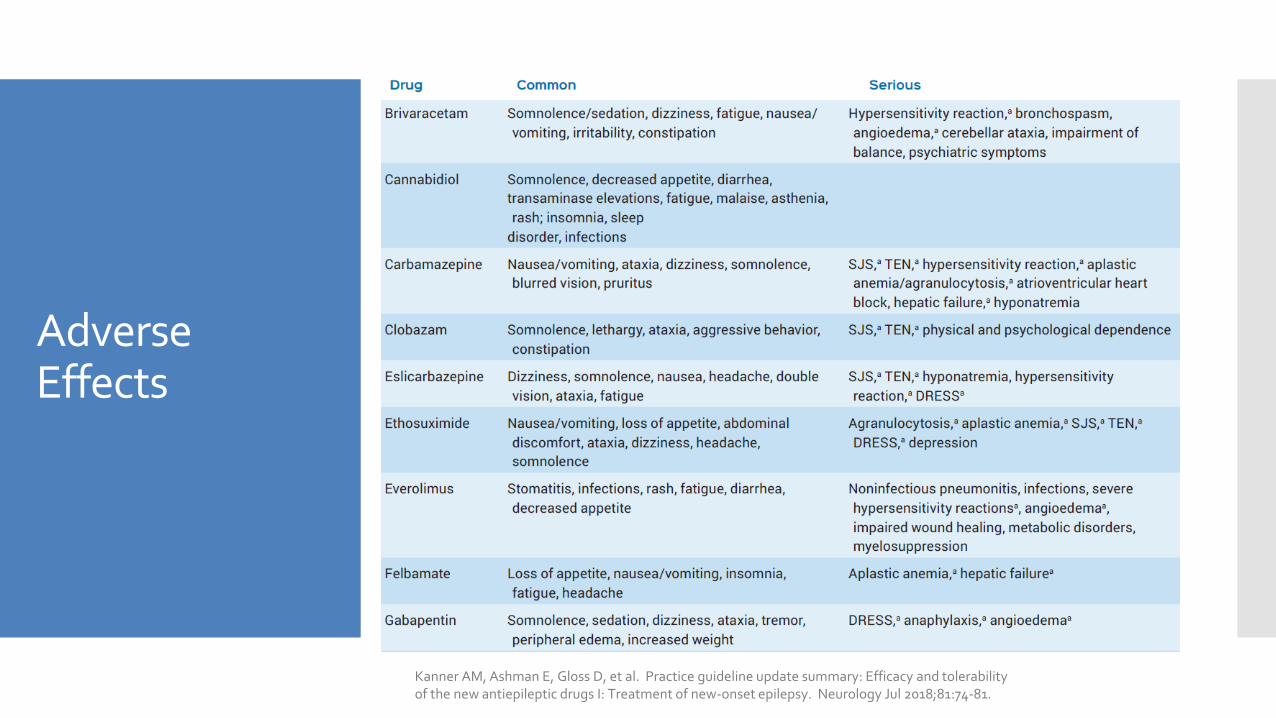
Adverse Effects
Kanner AM, Ashman E, Gloss D, et al. Practice guideline update summary: Efficacy and tolerability of the new antiepileptic drugs I: Treatment of new-onset epilepsy. Neurology Jul 2018;81:74-81.
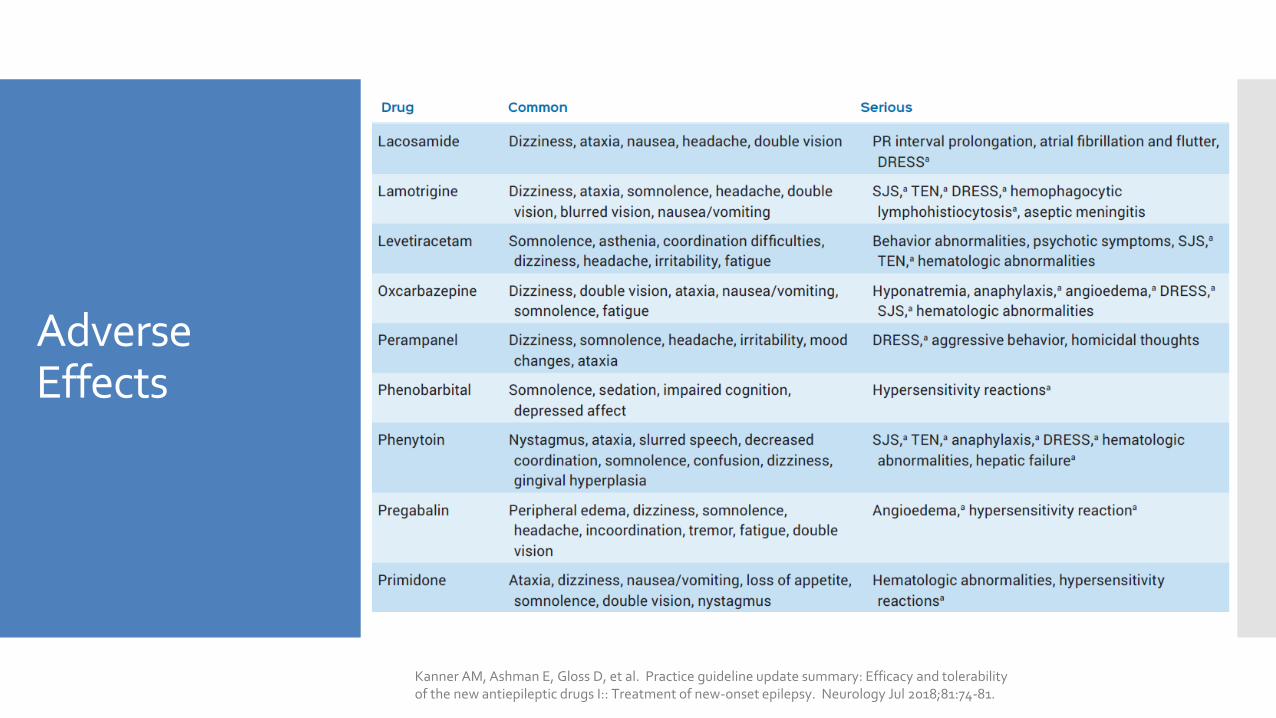
Adverse Effects
Kanner AM, Ashman E, Gloss D, et al. Practice guideline update summary: Efficacy and tolerability of the new antiepileptic drugs I:: Treatment of new-onset epilepsy. Neurology Jul 2018;81:74-81.
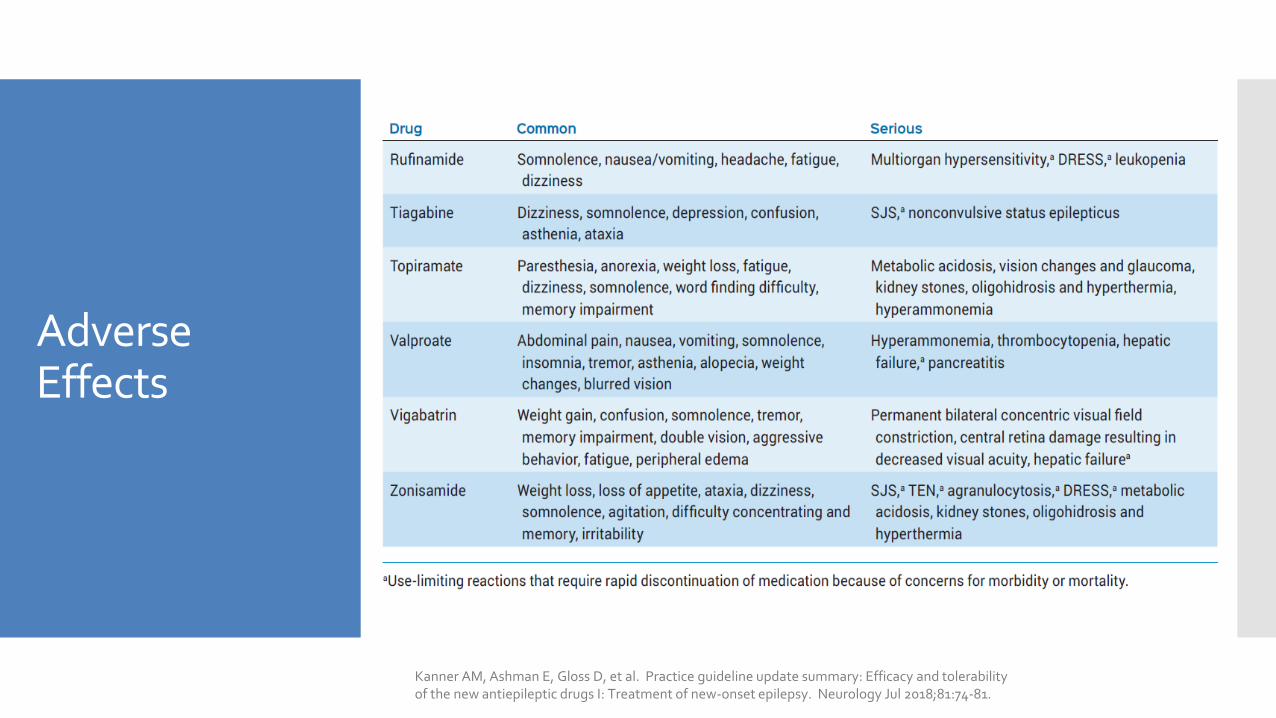
Adverse Effects
Kanner AM, Ashman E, Gloss D, et al. Practice guideline update summary: Efficacy and tolerability of the new antiepileptic drugs I: Treatment of new-onset epilepsy. Neurology Jul 2018;81:74-81.
Drug Selection
Serious adverse effects – rapid discontinuation required Drug reaction with eosinophilia and system
symptoms (DRESS)
Stevens-Johnson syndrome (SJS)
Toxic epidermal necrolysis (TEN)
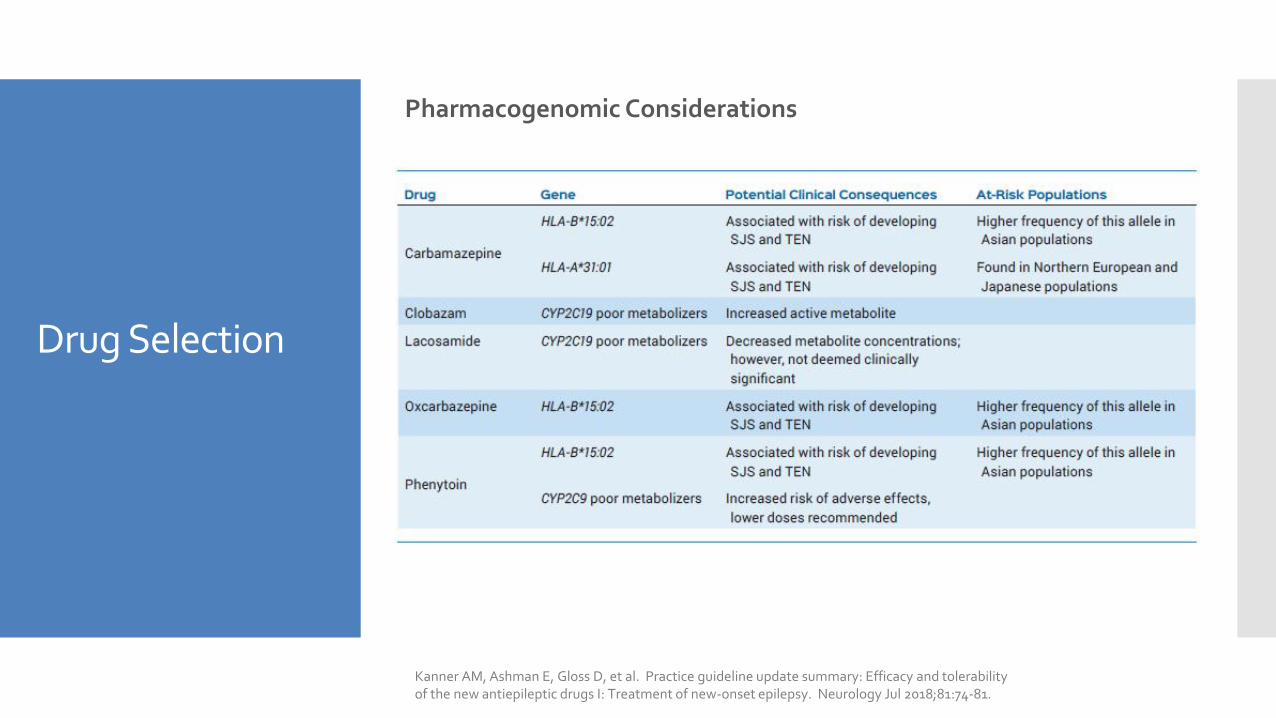
Drug Selection
Pharmacogenomic Considerations
Kanner AM, Ashman E, Gloss D, et al. Practice guideline update summary: Efficacy and tolerability of the new antiepileptic drugs I: Treatment of new-onset epilepsy. Neurology Jul 2018;81:74-81.
Drug Selection
Drug Interactions!
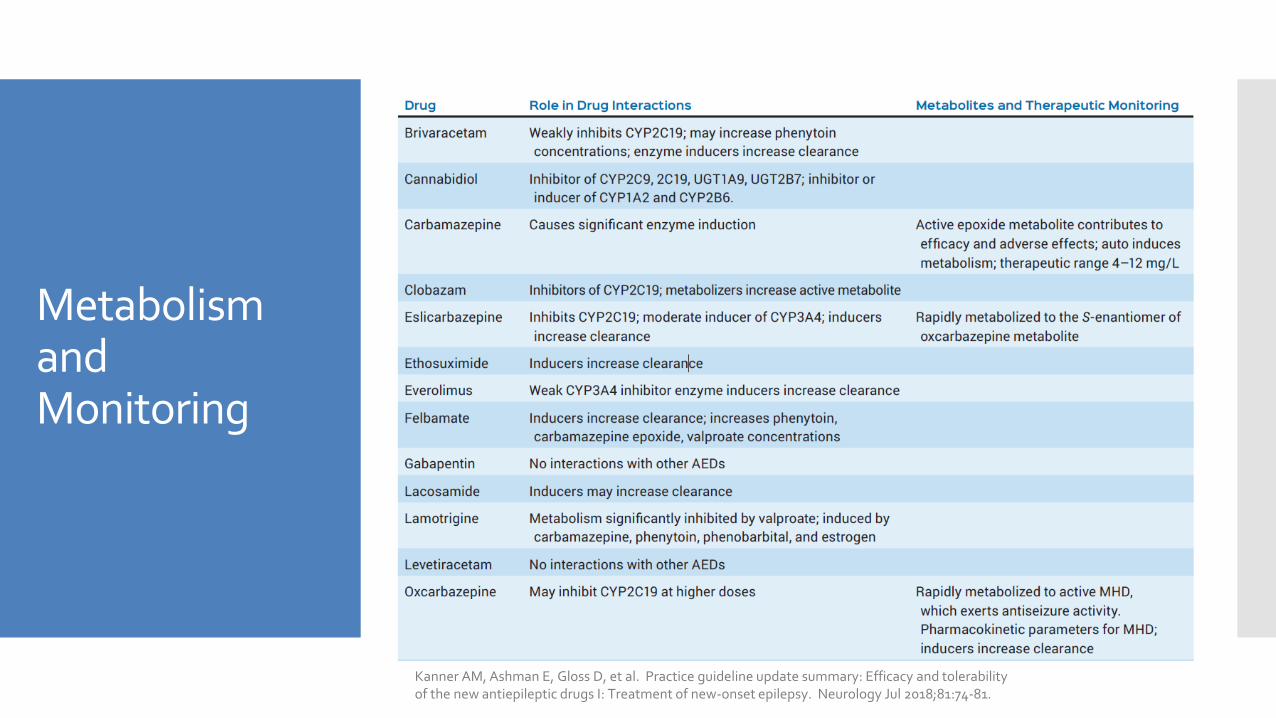
Metabolism and Monitoring
Kanner AM, Ashman E, Gloss D, et al. Practice guideline update summary: Efficacy and tolerability of the new antiepileptic drugs I: Treatment of new-onset epilepsy. Neurology Jul 2018;81:74-81.
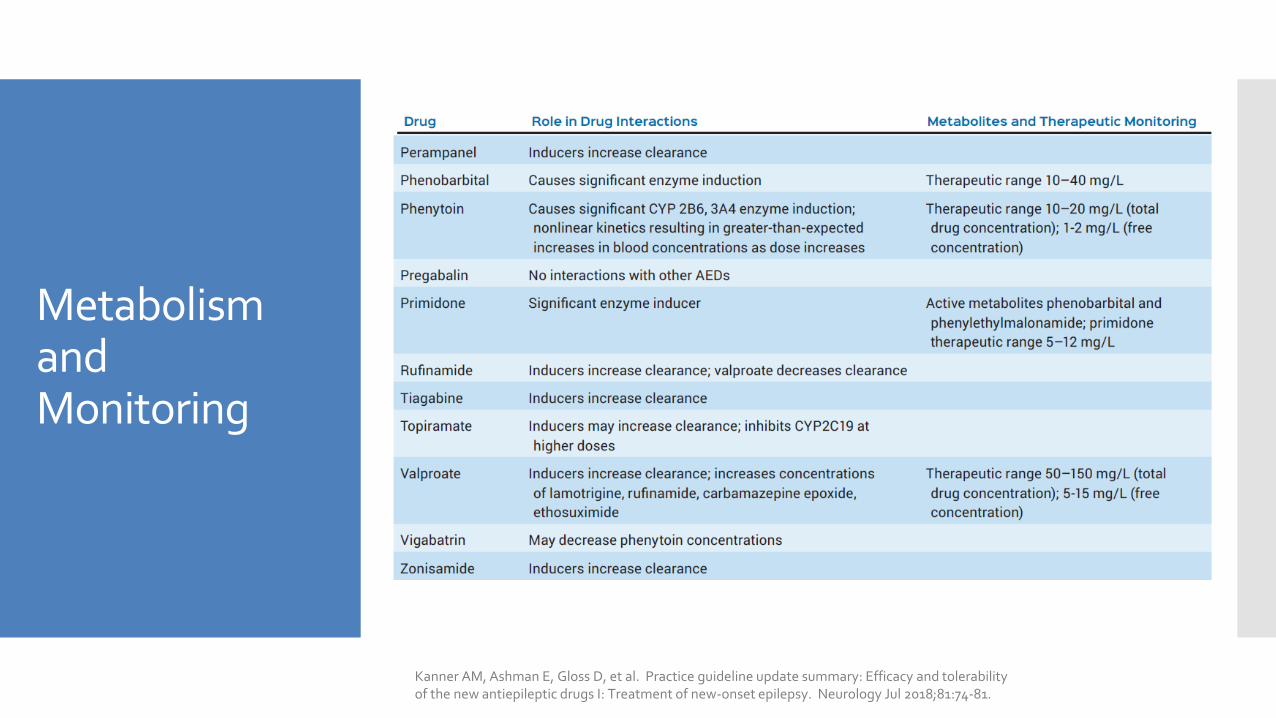
Metabolism and Monitoring
Kanner AM, Ashman E, Gloss D, et al. Practice guideline update summary: Efficacy and tolerability of the new antiepileptic drugs I: Treatment of new-onset epilepsy. Neurology Jul 2018;81:74-81.
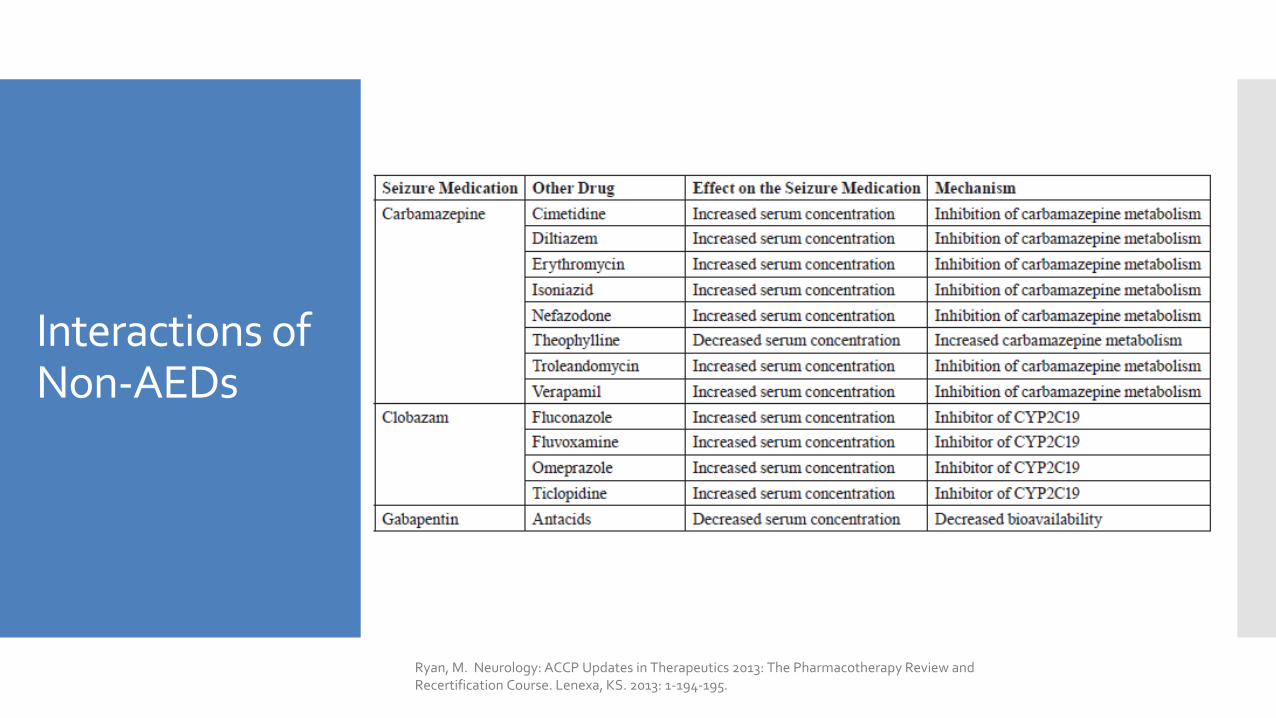
Interactions of Non-AEDs
Ryan, M. Neurology: ACCP Updates in Therapeutics 2013: The Pharmacotherapy Review and Recertification Course. Lenexa, KS. 2013: 1-194-195.
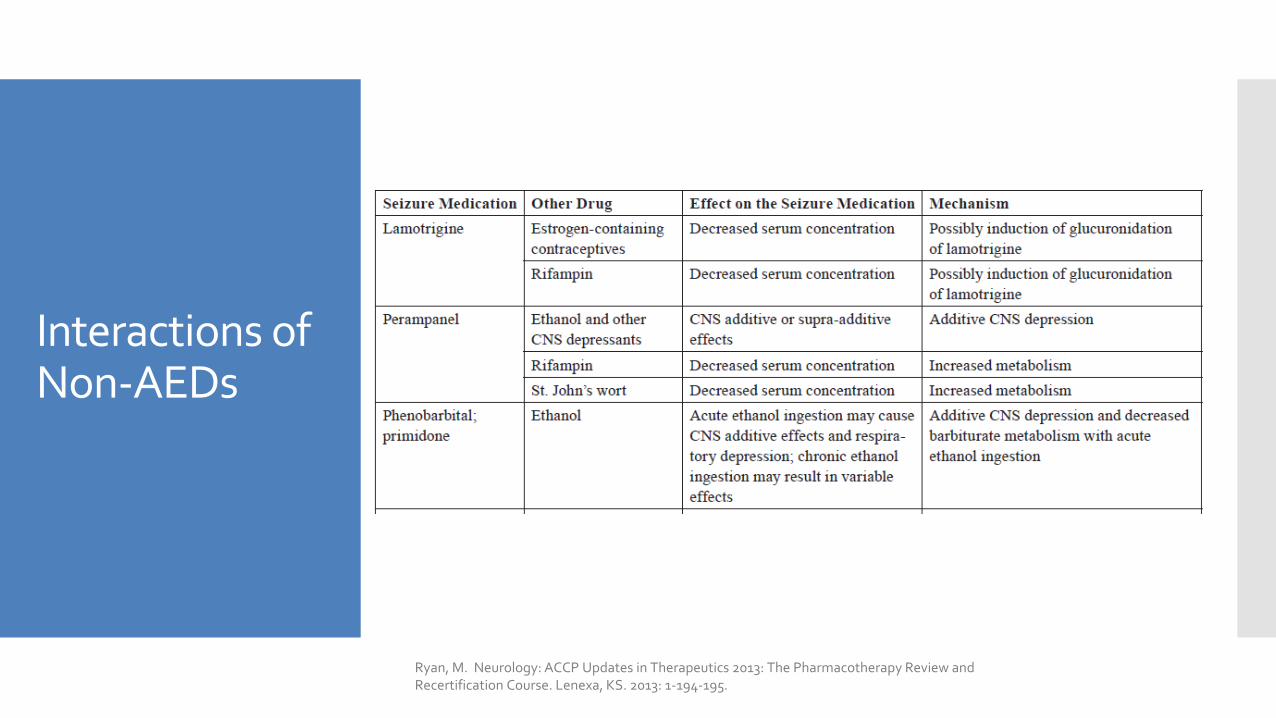
Interactions of Non-AEDs
Ryan, M. Neurology: ACCP Updates in Therapeutics 2013: The Pharmacotherapy Review and Recertification Course. Lenexa, KS. 2013: 1-194-195.
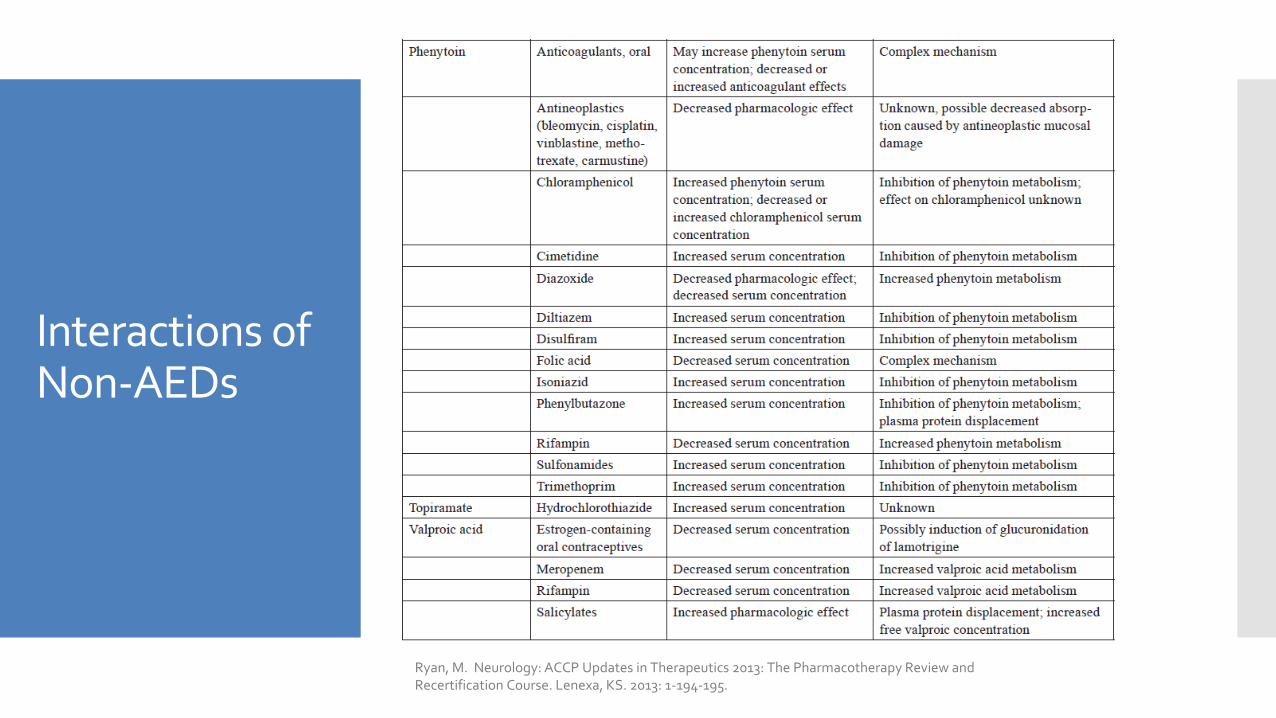
Interactions of Non-AEDs
Ryan, M. Neurology: ACCP Updates in Therapeutics 2013: The Pharmacotherapy Review and Recertification Course. Lenexa, KS. 2013: 1-194-195.
Drug Selection
Alternative indications Mood stabilization related to bipolar disorder:
valproate, carbamazepine, and lamotrigine
Neuropathic pain & postherpetic neuralgia: gabapentin and pregabalin
Migraine prophylaxis: valproate and topiramate
Essential tremor: primidone
Trigeminal neuralgia: carbamazepine
Anxiety: phenobarbital
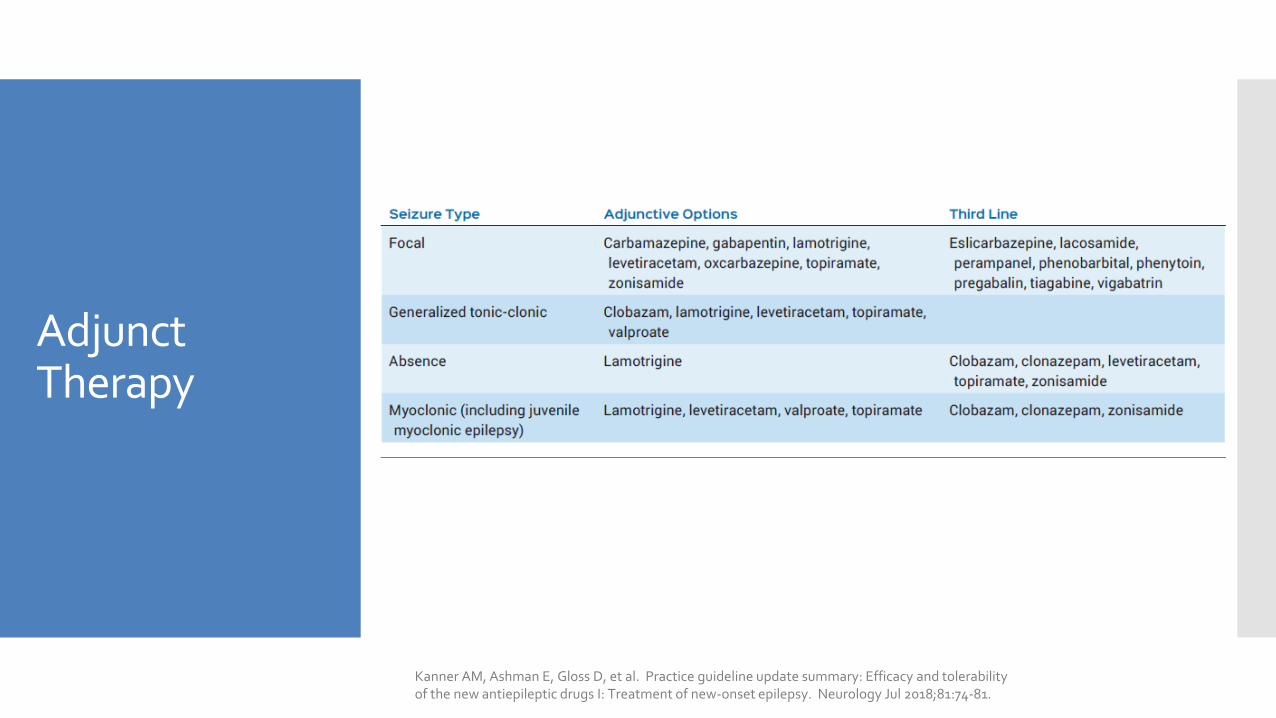
Adjunct Therapy
Kanner AM, Ashman E, Gloss D, et al. Practice guideline update summary: Efficacy and tolerability of the new antiepileptic drugs I: Treatment of new-onset epilepsy. Neurology Jul 2018;81:74-81.
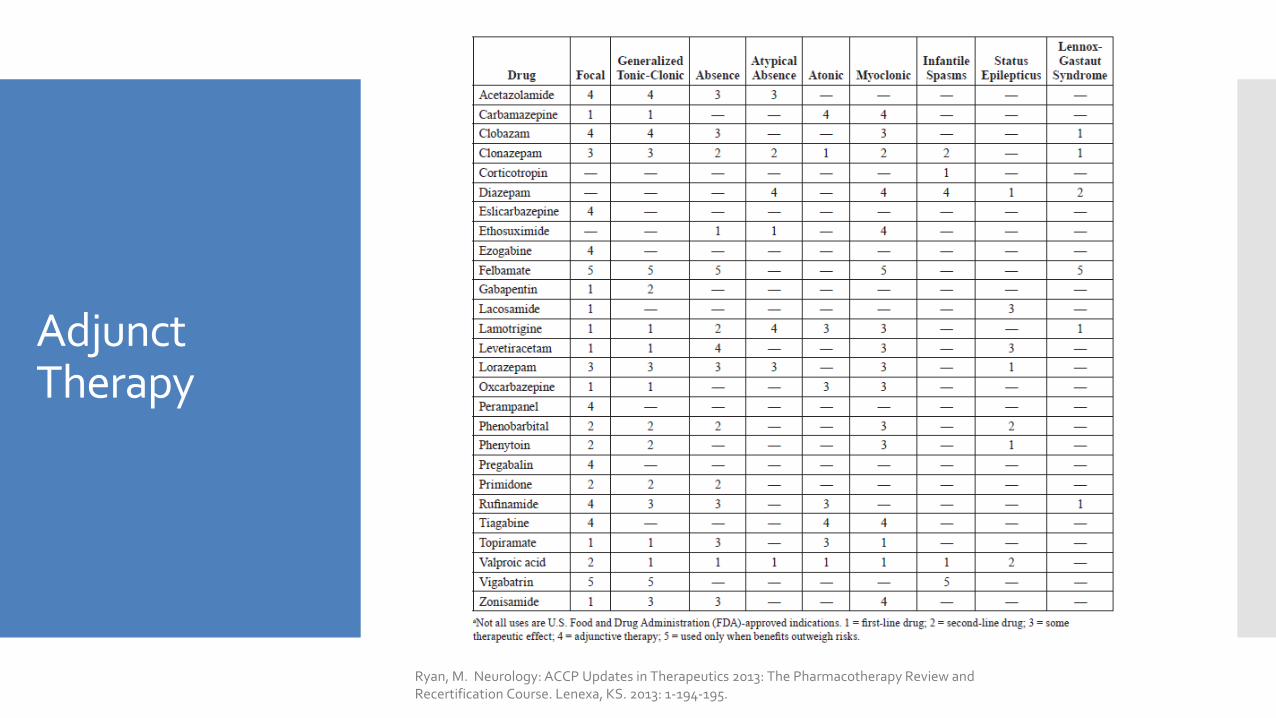
Adjunct Therapy
Ryan, M. Neurology: ACCP Updates in Therapeutics 2013: The Pharmacotherapy Review and Recertification Course. Lenexa, KS. 2013: 1-194-195.

Special Populations
Elderly
Pharmacokinetic changes in aging population may affect therapy1. Carbamazepine: Decreased clearance
2. Phenytoin: Decreased protein binding if renal failure or hypoalbuminemic
3. Valproic acid: Decreased protein binding
4. Diazepam: Increased half-life
5. Lamotrigine: Decreased clearance
6. Seizure medications with renal elimination must be adjusted based on CrCl
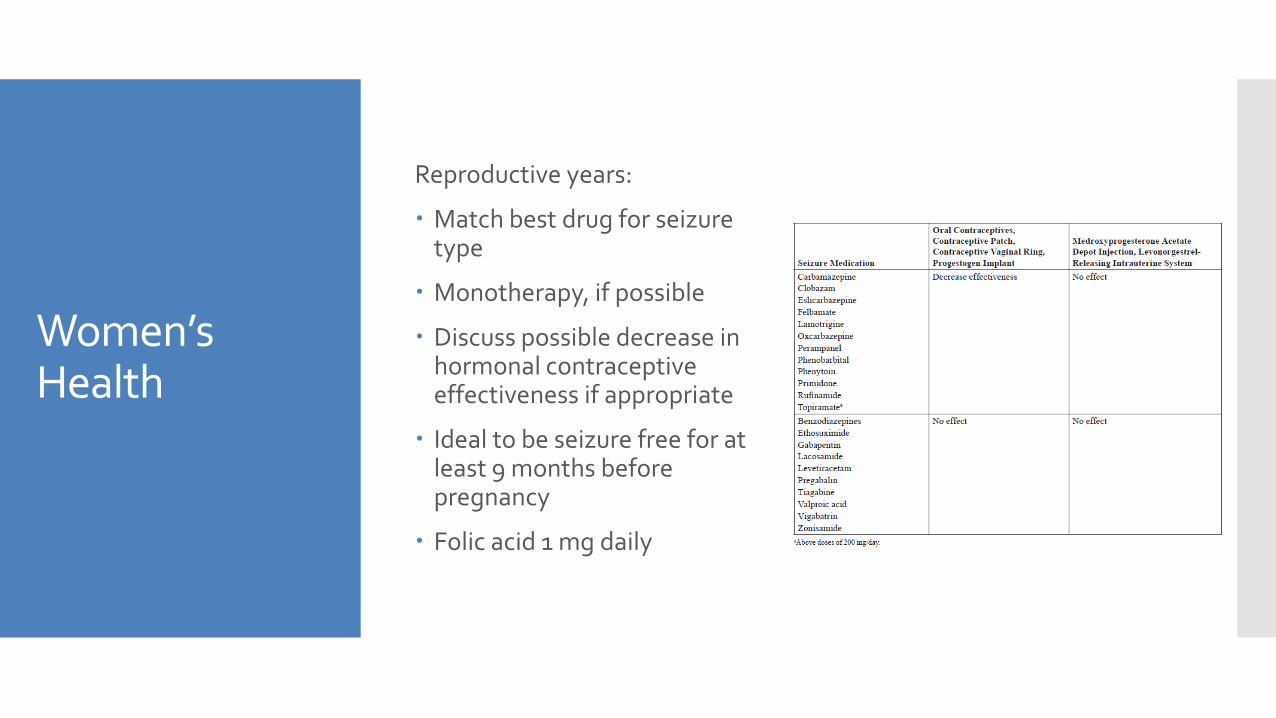
Women’s Health
Reproductive years:
Match best drug for seizure type
Monotherapy, if possible
Discuss possible decrease in hormonal contraceptive effectiveness if appropriate
Ideal to be seizure free for at least 9 months before pregnancy
Folic acid 1 mg daily
Women’s Health
During pregnancy: Avoid valproic acid monotherapy or polytherapy
during 1st trimester
Avoid use of seizure medication polytherapy throughout complete pregnancy
Avoid use of phenytoin, carbamazepine, and phenobarbital, if possible
Lamotrigine has a lower relative risk of congenital malformations

Treatment discontinuation
Treatment discontinuation
Consider withdrawal of anticonvulsants: Remain seizure-free for 2 or more years
Control obtained with 1 drug
Normal neurologic examination
EEG normalized with seizure medication treatment
No history of seizure relapse after drug withdrawal
Withdraw 1 drug at a time
Taper over several months Common regimen: reduce the dose by 1/3 for 1 month,
reduce by another 1/3 for 1 month, and then stop
Other Considerations
SexualDysfunction
Reported in 30-60% of men and women with epilepsy
Mechanism: Induction of CYP
isoenzymes to increase testosterone metabolism
Increased hepatic synthesis of sex hormone-binding globulin
Induction of aromatase; conversion to testosterone and estradiol
Dysfunction associated with: carbamazepine, phenobarbital, phenytoin, pregabalin, topiramate, zonisamide
Improved functioning with: lamotrigine and oxcarbazepine
Bone Health
Osteopenia and osteoporosis reported in 38-60% in tertiary epilepsy clinics
Increased risk based on treatment duration
Evidence that all seizure medications likely contribute
Treatment: Vitamin D (4000 IU/day for adults and 2000 IU/day for
children)

Suicidality
Twice the risk of suicidal behavior or ideation for patients receiving seizure medications
No difference between type of antiepileptic drug or age group
In 2008, FDA required warning and medication guide for all seizure medications
Questions?






























