Embed Size (px)
Citation preview

536 Clinical and Experimental Rheumatology 2020
1Department of Medical and Biological Science, Rheumatology Clinic, University of Udine, Italy; 2Department of Rheumatology and Clinical Immunology, Freiburg University Medical Center, Medical Faculty, Albert Ludwigs University, Freiburg, Germany; 3Rheumazentrum Ruhrgebiet, Herne and Ruhr-University Bochum, Germany; 4Rheumatology Department, Saint-Joseph University, Hotel-Dieu de France Hospital, Beirut, Lebanon; 5Academic Rheumatology Centre, Dipartimento Scienze Cliniche e Biologiche, University of Turin, Italy.Alen Zabotti, MDStephanie Finzel, MDXenofon Baraliakos, MD, PhDKrystel Aouad, MDNelly Ziade, MD, PhD, FRCPAnnamaria Iagnocco, MD, PhDPlease address correspondence to:Annamaria Iagnocco, Academic Rheumatology Centre, Dipartimento Scienze Cliniche e Biologiche, Università degli Studi di Torino, Regione Gonzole 10,10043 Orbassano, Torino, Italy.E-mail: [email protected] on April 11, 2019; accepted in revised form on July 8, 2019.Clin Exp Rheumatol 2020; 38: 536-542© Copyright CLINICAL AND EXPERIMENTAL RHEUMATOLOGY 2020.
Key words: ultrasonography, computed tomography, magnetic resonance imaging, rheumatoid arthritis, prevention
Competing interests: none declared.
ABSTRACTThere is growing evidence that the de-velopment of rheumatoid arthritis (RA) is a multistep process. The European League Against Rheumatism (EULAR) LGHQWLÀHG� GLIIHUHQW� SKDVHV� EHIRUH� WKH�onset of RA, from the presence of ge-netic and environmental risk factors for RA, towards clinically suspected arthralgia and undifferentiated arthri-WLV��&XUUHQWO\��D�QHZ�GHÀQLWLRQ�RI�´ZLQ-dow of opportunity” is emerging; this states that the window could even lie in preclinical phase of RA, preceding di-DJQRVLV� RU� IXOÀOOPHQW� RI� FODVVLÀFDWLRQ�criteria for RA. In this scenario, the de-WHFWLRQ� RI� VXEFOLQLFDO� LQÁDPPDWLRQ� E\�imaging tools could be useful together with autoantibodies and joint symptoms to better stratify people at high risk for developing RA and to plan prevention trials in high-risk cohorts. This review will give an overview on the use of com-puted tomography, magnetic resonance imaging and ultrasonography in the preclinical phases of RA.
Introduction Rheumatoid arthritis (RA) is a debilitat-LQJ��FKURQLF�LQÁDPPDWRU\�DXWRLPPXQH�disease. Bone erosions, especially at the bare areas of joints, are common for RA (1); synovitis and tenosynovitis, as well as bone marrow oedema can be detected frequently even at very early stages of the disease (2–6). Autoanti-bodies characteristic for RA such as rheumatoid factors (RF) and/or anti-citrullinated protein antibodies (ACPA) may precede the clinical manifestation of RA for years, and they have a pre-dictive value for the manifestation of clinical arthritis (7, 8). There is growing evidence that the development of RA is a multistep process. The European League Against Rheumatism (EULAR) LGHQWLÀHG�GLIIHUHQW�SKDVHV��������� SUHVHQFH� RI� JHQHWLF� DQG� HQYLURQ-PHQWDO�ULVN�IDFWRUV�IRU�5$�����V\VWHPLF�
DXWRLPPXQLW\� DVVRFLDWHG� ZLWK� 5$�� ���symptoms without clinical arthritis, UHFHQWO\� GHÀQHG� DV� FOLQLFDOO\� VXVSHFW�DUWKUDOJLD� �&6$�� ����� ��� XQFODVVLÀHG�DUWKULWLV�DQG����5$����������7KH�LGHQWL-ÀFDWLRQ�RI�WKHVH�SKDVHV�LV�DQ�HVVHQWLDO�step to plan prevention trial in people at high risk for RA development. In this scenario, the detection of sub-FOLQLFDO�LQÁDPPDWLRQ�E\�LPDJLQJ�WRROV�could be useful together with autoan-tibodies and joints symptoms to bet-ter stratify people at high risk for RA development. This review will give an overview on the use of imaging in the patient’s journey towards the develop-ment of RA (Fig. 1).
Computed tomographyComputed tomography (CT) is a slice imaging technique enabling excel-lent three-dimensional visualisation of bone structure due to its high contrast between soft tissue and bone. More-over, it is not prone to superimposition artifacts like conventional radiography (CR). Being more sensitive than CR and magnetic resonance imaging (MRI) regarding detection of alterations of bone structure makes CT suitable as gold standard for measuring bone ero-sions (11) (Fig. 2). On the other hand, CT does use radiation, which might be one of the reasons why conventional CT (cCT) is usually not widely being used for assessment of preclinical ar-thritis, strict radiation laws limiting a somewhat all too carefree use of ra-diation in a group of patients, in which other imaging techniques such as MRI or ultrasonography (US) might be more advantageous to use. CCT might how-HYHU�EH�KHOSIXO�LQ�HDUO\�DUWKULWLV��3HOXVR et al. used cCT as a reference method for comparison with three-dimensional ultrasound (3DUS) in a cohort of early arthritis patients without radiographic evidence of bone erosions. CCT could detect 32 erosions in eleven patients
Review
Imaging in the preclinical phases of rheumatoid arthritisA. Zabotti1, S. Finzel2, X. Baraliakos3, K. Aouad4, N. Ziade4, A. Iagnocco5

537Clinical and Experimental Rheumatology 2020
Imaging in pre-RA / A. Zabotti et al.
and found expectedly more frequently erosions in the wrists and in the 3rd and 4th metacarpophalangeal (MCP) joints, since these were more accessible for cCT than for 3DUS (12). Combining CT to positron emission tomography (PET) offers clear advantages over use of CT alone with regards to therapy PRQLWRULQJ�� GLVHDVH� TXDQWLÀFDWLRQ� DQG�detection of subclinical disease activity. However, costs and exposure to radia-tion is increased compared to cCT. First GHVFULEHG�LQ������������WKH�3(7�WUDFHU�[18F]-Flouro-deoxy-glucose (FDG) is still the most frequently used PET tracer in daily clinical practice. [18F]-FDG is being taken up inter alia by cells with a KLJK�PHWDEROLF�UDWH��VXFK�DV�LQÁDPPD-WRU\�FHOOV�LQ�WKH�V\QRYLXP�������,Q������Roivainen et al. (15) examined a co-hort of 17 active early arthritis patients that were starting combination therapy with methotrexate, sulfasalazine, hy-droxychloroquine, and low-dose glu-cocorticosteroids with [18F]-FDG/CT at baseline, as well as after week two and four after therapy onset. As out-
come parameters standardised uptake values (SUV), fractionised uptake rates (FUR), and glucose uptake rates (GU) were used for PET, compared to clinical (DAS28), and laboratory parameters (erythrocyte sedimentation rate, ESR, and C-reactive protein, CRP). Already two weeks after therapy onset SUV was VLJQLÀFDQWO\�UHGXFHG�LQ�����RI�SDWLHQWV��DQG� LQ� ���� RI� SDWLHQWV� IURP� EDVHOLQH�to week 4. Moreover, the percentage 18F-FDG uptake values from baseline to week two correlated with DAS28 at week twelve; changes in ESR and CRP were positively associated with changes assessed by PET. The authors therefore suggested that [18F]-FDG/CT might support prediction of therapy response very early after therapy initiation. PET/CT might even also be relevant for the detection of subclinical arthritis. Re-cently, Gram et al. presented the case of a 67-year-old RF and ACPA-positive male patient with arthralgia for two years, but without clinical arthritis or any signs of pathology in US (16). The group applied a derivate of PET/CT us-
LQJ� D� WUDFHU� VSHFLÀF� IRU� ERQH�PHWDER-lism, [18)@�VRGLXP�ÁXRULGH��>18F]-NaF). The patient showed FDG-uptake in a couple of joints, but increased NaF-uptake in multiple joints. Six months after the initial PET scan the patient manifested highly active RA. These ÀQGLQJV� VXJJHVW� WKDW� >18F]-NaF might be a valuable tool for the detection of subclinical arthritis in patients without clinical joint swelling. High-resolution peripheral quantitative CT (HR-pQCT) is a comparatively novel variety of CT using a nominal isotropic voxel size of 82µm; the applied radiation dose for MCPs adjusted for whole body dose is very low (maximum around 15µSv for a male adult hand). Due to a very high soft tissue to bone contrast bone is depicted meticulously, while soft tis-sue depiction is less pronounced. The technique is still undergoing validation as an imaging outcome parameter for FOLQLFDO�VWXGLHV�������EXW�TXDQWLÀFDWLRQ�algorithms are underway that allow for a more or less user-independent volu-PHWULF� TXDQWLÀFDWLRQ� RI� ERQH� HURVLRQ�
Fig. 1. 7KH�GHWHFWLRQ�RI�LQÁDPPDWLRQ�DQG�GDPDJH�E\�LPDJLQJ�WRROV�LQ�WKH�SUHFOLQLFDO�SKDVHV�RI�5$�†Kleyer et al. Ann Rheum Dis����������������������††Ten Brick RM et al. RMD Open ���������H��������)LJXUH���DGDSWHG�ZLWK�SHUPLVVLRQ�IURP�YDQ�6WHHQ-bergen HW et al��$UWKULWLV�5KHXP��������������������

538 Clinical and Experimental Rheumatology 2020
Imaging in pre-RA / A. Zabotti et al.
volume in early RA. Peters et al. re-cently could show good reproducibil-ity of their algorithm for bone erosion volume assessment; reproducibility of parameters of bone microstructure and bone density was excellent with ICCs ������ ������ 7KHVH� UHVXOWV� DUH� SURPLV-ing, since bone in early arthritis pa-tients should be closely monitored for development of structural damage. The bare area of MCP joints might be a predilection site for bone erosions in LQÁDPPDWRU\� DUWKULWLV�� HVSHFLDOO\� WKH�Cortical Micro-Channels (CoMiCs) 6\VWHP�PD\� SOD\� D� FUXFLDO� UROH�� HDUO\�5$�SDWLHQWV�VKRZHG�VLJQLÀFDQWO\�PRUH�CoMiCs compared to elderly healthy volunteers > 65 years of age (p ������������� +5�S4&7� LV� HYHQ� DEOH� WR� VKRZ�earliest bone changes in ACPA-positive patients without any musculoskeletal FRPSODLQWV��.OH\HU�et al. examined the 2nd and 3rd MCP joints of 15 ACPA positive (ACPA+) individuals and 15 KHDOWK\� FRQWUROV� ZLWK� +5�S4&7� ������Bone erosions were not detected, but bone mineral density as well as corti-FDO�WKLFNQHVV�ZHUH�VLJQLÀFDQWO\�UHGXFHG�in the ACPA+ group (p ��������0HDV-ures of trabecularity did not show any difference between the groups. Corti-cal porosity was more prevalent in the ACPA+ group than in the ACPA nega-tive group (p ��������� 7KHVH� ÀQGLQJV�imply that structural bone alterations might start earlier than clinical manifes-tation of arthritis in ACPA-positive indi-viduals (Fig. 2). As placebo-controlled phases in clinical studies are getting shorter, and since there seems to be a window of opportunity for treatment or even prevention of early RA, it is im-portant to employ highly sensitive im-aging techniques such as HR-pQCT that are able to visualise very subtle chances in bone micro architecture, even before more obvious changes such as bone ero-sions have occurred.
Magnetic resonance imaging MRI is a sensitive imaging modality that allows detailed assessment of in-ÁDPPDWLRQ�DV�ZHOO�DV�VWUXFWXUDO�GDPDJH�in RA, with an excellent content valid-LW\�ZKHUH�ÀQGLQJV�DUH�KLJKO\�FRUUHODWHG�to intra-articular macroscopic altera-tions in the joint of RA patients (21).
Compared to physical examination and CR, MRI is a more sensitive tool for LGHQWLÀFDWLRQ� RI� GLVHDVH�UHODWHG� WLVVXH�damage because of its direct visualisa-tion of synovitis, cartilage destruction, bone erosion, bone marrow oedema (BME), tenosynovitis, and surrounding soft-tissue structures (22) (Fig. 3 a-c). Moreover, MRI can detect subclinical LQÁDPPDWLRQ�LQ�����RI�FOLQLFDOO\�QRQ�VZROOHQ� ZULVW� MRLQWV� DQG� ���� RI� QRQ�swollen MCP joints (23).Recently, the important role of MRI has emerged in the differential diagnosis of XQFODVVLÀHG� HDUO\� DUWKULWLV� DQG� LV� QRZ�recommended in litigious cases when RA diagnosis is still uncertain (21). The rationale behind this is that the pres-HQFH�RI�LQÁDPPDWLRQ�RQ�05,�FDQ�SUH-dict the progression from undifferenti-ated arthritis (UA) to clinical RA (21, 24). In this context, validated scoring systems have been developed for MRI
WR�TXDQWLI\�LQÁDPPDWLRQ�DQG�VWUXFWXUDO�damage in clinical trials (25-27). The OMERACT RA MRI score (RAMRIS) is the most frequently used for hands and wrists with a semi-quantitative as-sessment of synovitis, bone erosion and BME. However, when using MRI for diagnosis purposes, it needs to be inter-preted with caution and in correlation with the clinical context and physical examination. In fact, healthy (espe-cially older) individuals can present with bone erosions and MRI-detected LQÁDPPDWLRQ� UHVHPEOLQJ� WR� 5$� ����������DOWKRXJK�VRPH�HURVLRQ�VLWHV�PLJKW�EH�PRUH�VSHFLÀF�IRU�5$��VXFK�DV�JUDGH���� HURVLRQV�� PHWDWDUVR�SKDODQJHDO���and metatarso-phalangeal-1 erosions) (31). In preclinical phases of RA, sev-eral studies have been conducted using objective tools such as MRI in order to identify which patients with arthralgia will develop RA. A small cohort study
Fig. 2. Three cases visualised by HR-pQCT imaging.&DVH�������\HDU�ROG�IHPDOH�SDWLHQW�ZLWK�UKHXPDWRLG�DUWKULWLV��0HWDFDUSRSKDODQJHDO� MRLQW� LV�GHSLFWHG�in axial (1A), sagittal (1B), and coronal (1C) plane; a clearly marginated erosion is seen in the dorsal quadrant. Note, that erosion in the third plane is not visualised as a cortical break, but as absence of trabecular structure. Bone structure appears coarse (periarticular osteopenia).&DVH�������\HDU�ROG�IHPDOH�SDWLHQW�ZLWK�XQGLIIHUHQWLDWHG�DUWKULWLV�IRU�D�IHZ�ZHHNV��0HWDFDUSRSKDODQ-geal joint is depicted in axial (2A), sagittal (2B), and coronal (2C) plane. Bone structure appears normal.&DVH�������\HDU�ROG��$&3$��IHPDOH�SDWLHQW�ZLWK�DUWKUDOJLD�IRU�VHYHUDO�ZHHNV��0HWDFDUSRSKDODQJHDO�joint is depicted in axial (3A), sagittal (3B), and coronal (3C) plane. Bone structure appears coarse.

���Clinical and Experimental Rheumatology 2020
Imaging in pre-RA / A. Zabotti et al.
by Krabben et al. showed that the MRI-FRPELQHG� LQÁDPPDWLRQ� VFRUHV� �%0(�and synovitis) on MRI were higher in the wrists of ACPA positive patients with arthralgia, as compared to controls (32). Another small pilot study by Gent et al. also found that baseline MRI syn-RYLWLV�ZDV�SUHVHQW�LQ�����RI�DUWKUDOJLD�patients with positive anti-citrullinated protein antibodies (ACPA), but only ����RI�WKHVH�SDWLHQWV�GHYHORSHG�5$�DI-ter 3 years of follow-up (33). This study raised again the question of MRI speci-ÀFLW\�DQG�WKUHVKROGV��D�V\QRYLWLV�VFRUH�of 1 (RAMRIS system) may not always be associated with subsequent develop-ment of arthritis and could be found in healthy controls, likely related to de-generative changes. When a higher ar-ELWUDU\�SUHGHÀQHG�FXW�RII�VFRUH��5$0-5,6�����ZDV�XVHG� WR�GHÀQH� D� SRVLWLYH�MRI in patients with clinically suspect DUWKUDOJLD������KDG�VXEFOLQLFDO�05,�LQ-ÁDPPDWLRQ� DQG� ����RI� WKHVH� SDWLHQWV�progressed to clinical arthritis after 4 months (34). However, baseline sub-FOLQLFDO� 05,� LQÁDPPDWLRQ� FRXOG� QRW�determine which patients progressed to clinical arthritis. Also, initial symp-toms and serology (ACPA, rheumatoid factor, acute phase reactants) were un-able to differentiate patients with CSA, ZLWK� DQG� ZLWKRXW� 05,� LQÁDPPDWLRQ�(34). The largest published MRI study to date by Van Steenbergen et al., us-
LQJ�DQRWKHU�GHÀQLWLRQ�RI�SRVLWLYH�05,�and a longer follow-up period, showed WKDW�����RI�����SDWLHQWV��ZLWK�&6$�DQG�a positive MRI, progressed to arthritis GXULQJ���\HDU�DQG�����RI�WKHVH�SDWLHQWV�were ACPA positive (35). Interestingly, LQÁDPPDWLRQ� RQ� 05,� ZDV� DVVRFLDWHG�with progression to arthritis indepen-dently of ACPA, CRP and clinical fac-tors (35, 36). In the longitudinal study made by Ten Brinck et al. that included 31 patients who converted from CSA to RA, increased tenosynovitis and syno-vitis scores on MRI were noted at CSA onset (earliest features) followed by in-creased synovitis and osteitis during the progression to clinically established RA ������7KHVH�ÀQGLQJV�RQ�VHULDO�05,V�DG-dressed also the chronological order of MRLQW�LQÁDPPDWLRQ�WKDW�VHHP�WR�PDLQO\�start outside the bone and subsequently in the bone (osteitis). However, when the same authors studied the progres-VLRQ�IURP�&6$�WR�LQÁDPPDWRU\�DUWKUL-tis (IA) at the individual joint level, the PDMRULW\� RI� FOLQLFDO� V\QRYLWLV� ������were intriguingly not preceded by base-OLQH� VXEFOLQLFDO� LQÁDPPDWLRQ� DW� WKH�same joint site (38). This observation supports the hypothesis of a systemic LQÁDPPDWRU\� GHUHJXODWLRQ� UDWKHU� WKDQ�a localised exacerbating process. From a practical point of view, clear cut-offs DQG� VSHFLÀF� SDUDPHWHUV� DUH� RI� FUXFLDO�importance to avoid over-diagnosis and
GLIIHUHQWLDWH� VXEFOLQLFDO� LQÁDPPDWLRQ�IURP�QRQ�VSHFLÀF�ÀQGLQJV�RQ�05,�� ,Q�this context, a recent study by Boer et al., was made to determine which MRI VFRUHV� RU� ÀQGLQJV� DUH� FRQVLGHUHG� QRU-PDO��DQG�ZKLFK�UHÁHFW�SDWKRORJ\�������While testing different cut-offs for SRVLWLYH�05,�� WKH� ´��� FRUUHFWHG� GHÀ-nition”, indicating the presence of in-ÁDPPDWLRQ�DW�D�MRLQW�LQ�����RI�KHDOWK\�persons of the same age-category at the same location, resulted in reducing false positives MRI without affecting WKH� VHQVLWLYLW\�� ,Q� IDFW�� 05,� VSHFLÀF-LW\� WR� GHWHFW� LQÁDPPDWLRQ� LQFUHDVHG�IURP�����WR�����LQ�&6$�SDWLHQWV�DQG�IURP�����WR�����LQ�8$�SDWLHQWV��6WLOO��larger studies on healthy individuals are awaited to better specify the cut-RIIV� DQG� UHDFK� D� GDWD�GULYHU� GHÀQLWLRQ�of a positive MRI. Overall, MRI has been of increasing interest in the past two decades with growing evidence on its validity in the detection of subclini-FDO� LQÁDPPDWLRQ� LQ� SDWLHQWV� DW� ULVN� RI�developing RA. While more studies are needed to clarify its practical use in the preclinical stages of RA, MRI is consid-ered as a key research tool for the up-coming years and can be used in clinical practice when there is diagnostic doubt.
Ultrasonography Despite the difference of the US ma-chines used and the possible different level of experience of sonographers, published data support the value of us-ing US in the management of patients ZLWK� LQÁDPPDWRU\� DUWKULWLV� �,$� (21). EULAR recommendations for the man-agement of early arthritis suggest the use of US in case of doubtful synovitis at clinical examination, highlighting previous controlled studies suggesting a greater sensitivity of US than clinical examination in detecting synovitis, par-ticularly in the knee and in small joints ����������7KLV�GLDJQRVWLF� UROH�RI�86�LQ�clinical practice was recently showed in a multicentre study, which aimed to map the way US is used in RA (42). This real-life setting study revealed that formulating a diagnosis was the second most common indication (after monitor-ing disease activity) for performing an US scan (42,43). Furthermore, it is in-WHUHVWLQJ� WR�QRWH� WKDW�VRQRJUDSKLF�ÀQG-
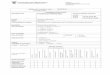
Fig. 3. Magnetic resonance imaging (MRI) of a 37-year-old female patient diagnosed with early RA. )LJ���D��*DGROLQLXP�HQKDQFHG�05,�VKRZLQJ� LQÁDPPDWRU\�V\QRYLWLF�ÀQGLQJV� LQ� WKH�SUR[LPDO� LQWHU-phalangeal and metacarpophalangeal joints (*) and in the carpal area (arrowhead), together with teno-synovitis (abductor pollicis longs muscle, tick arrow) and bone marrow oedema (distal ulnar head, thin DUURZ���)LJ���E��&RUUHVSRQGLQJ�7��ZHLJKWHG�05,�DQG�)LJ���F��FRUUHVSRQGLQJ�FRQYHQWLRQDO�UDGLRJUDSK�RI�WKH�VDPH�SDWLHQW�ZLWKRXW�SDWKRORJLF�ÀQGLQJV�LQ�WKLV�HDUO\�SKDVH�RI�WKH�GLVHDVH��

��� Clinical and Experimental Rheumatology 2020
Imaging in pre-RA / A. Zabotti et al.
ings seemed to have better correlations with histologic scoring than serologic biomarkers of disease activity in the RA rabbit model, particularly at early stages (44). Under these premises, it clearly appears the use of US to detect signs of HDUO\� LQÁDPPDWLRQ�DQG�RU�GDPDJH��i.e. erosions) in patients with or without clinical synovitis at high risk for devel-opment of RA (Fig. 4). Recently, Nam et al� VKRZHG�IRU� WKH�ÀUVW� WLPH� WKH�SUH-dictive value of US for the development of IA (i.e.�5$�LQ�RYHU�����RI�FDVHV��LQ�ACPA positive patients without clinical synovitis (45). This was seen both at a patient level and at an individual joint level (45). In this study, patients with baseline power Doppler (PD) and ero-sion in at least one joint were at higher risk of progression. As expected, the role of PD signal as predictor was afterwards FRQÀUPHG�DORQJ�ZLWK�PRUQLQJ�VWLIIQHVV�and age at baseline as independently as-sociated with the development of IA in patients with arthralgia without current or past synovitis (46). The same authors highlighted the positive and negative predictive value of US as predictor of IA �UHVSHFWLYHO\������DQG�������VXJJHVWHG�
that US had an added value to identify which patients (i.e. patients without US synovitis) would not develop into IA (46). However, considering the low frequency of PD detection in the pre-clinical phases of RA, as highlighted by van Beers-Tas et al. in seropositive arthralgia patients (i.e.� ��� RI� SDWLHQWV�with at least one joint with PD), its role as predictor of RA needs to be further investigated (47). Recently, Horton et al. demonstrated the added value of US RYHU� FOLQLFDO� H[DPLQDWLRQ� IRU� LGHQWLÀ-cation of patients with undifferentiated arthritis (UA) at high risk for RA (48). 7KH�SUHVHQFH�RI�DW�OHDVW�ÀYH�MRLQWV�ZLWK�*6�� JUDGH� �� DSSHDUHG� WR� GLVFULPLQDWH�patients with low or high risk of pro-gression to RA, instead the presence of DW�OHDVW�WZR�MRLQWV�ZLWK�*6���JUDGH���ZDV�clinically relevant in determining the fu-ture use of methotrexate (48). Further-more, over the sonographic detection of V\QRYLWLV��86�GHÀQHG�WHQRV\QRYLWLV�SUR-vided additional predictive data along-side ACPA positivity in a cohort of pa-WLHQWV�ZLWK�HDUO\�8$�������,Q�D�SUDJPDWLF�view of US using in patients with mus-FXORVNHOHWDO�LQÁDPPDWRU\�V\PSWRPV�RU�
with UA, US could be more useful in WKH�DVVHVVPHQW�RI�WKH�FOLQLFDOO\�GLIÀFXOW�$&3$�QHJDWLYH�DUWKULWLV�������,Q�DUWKUDO-gia or UA patients, Freestone et al. sug-gested that the main role for US in the diagnosis of IA may be in the ACPA/RF negative patient group where there LV�VWLOO�VLJQLÀFDQW�GLDJQRVWLF�XQFHUWDLQW\��PD positivity, GS synovitis = 3 and the presence of erosions were the selected VRQRJUDSKLF�YDULDEOHV�WKDW�VLJQLÀFDQWO\�changed the post test probability for the development of RA (51). The combi-QDWLRQ� RI� 86� DQG� VHURORJLFDO� ÀQGLQJV�seem to be the good way to characterise people at risk for developing RA. The best diagnostic performance in a retro-spective cohort of arthralgia patients was provided by the presence of artic-XODU� V\QRYLWLV�ZLWK�3'�JUDGH����RU�E\�the presence of articular synovitis with 3'�JUDGH����FRPELQHG�ZLWK�5)�DQG�RU�ACPA positivity (52). With these crite-ria they obtained a sensitivity of about ����DQG�D�VSHFLÀFLW\�RI�����IRU�D�GL-agnosis of RA (52). In conclusion, ac-cording to these preliminary evidences 86�FRQÀUPV�LWV�UROH�DV�SUHGLFWRU�RI�5$�development. Currently, the sonograph-LF�GHWHFWLRQ�RI�LQÁDPPD�WLRQ�FRXOG�EH�DQ�additional value in clinical practice par-ticularly in seronegative patients with LQÁDPPDWRU\� V\PSWRPV�� &RQYHUVHO\��WKH� DEVHQFH�RI�86� LQÁDPPDWLRQ� FRXOG�be useful to identify pa tients with low ULVN�WR�GHYHORS�,$��7KH�LGHQWLÀFDWLRQ�RI�the best predictive US variables for RA development and the scanning protocol needed are the necessary future steps to include US in the management of pre-RA for everyday practice but also to include such a technique in prevention clinical trials.
Conclusion7KH�GHÀQLWLRQ�RI�´ZLQGRZ�RI�RSSRUWX-nity” in RA is changing over the years, actually there is convincing data that HDUOLHU�WUHDWPHQW����²���PRQWKV�RI�GLV-ease duration) resulted in absolute low-er radiographic joint destruction, slow-er progression rate and higher clinical remission rates (53). However, in the ODVW� \HDUV� D� ´QHZ� GHÀQLWLRQµ� RI� ´ZLQ-dow of opportunity” is emerging, this states that the window could even lie in preclinical phase of RA, preceding di-
Fig. 4. 1a-b��XOWUDVRQRJUDSK\�RI�,,,�0&3�MRLQW�RI�D����\HDU�ROG�PDOH�GLDJQRVHG�ZLWK�HDUO\�XQGLIIHUHQ-tiated arthritis. 1a��6\QRYLDO�K\SHUWURSK\�ZLWK�MRLQW�HIIXVLRQ���E��6\QRYLDO�K\SHUWURSK\�ZLWK�3'�VLJQDO��2a-c�� XOWUDVRQRJUDSK\� DQG� FRQYHQWLRQDO� UDGLRJUDSK\� RI� D� ���\HDU�ROG�PDOH� SDWLHQW� GLDJQRVHG�ZLWK�early RA (RF and ACPA positive). 2a��(URVLRQ�FRQÀUPHG�LQ�WZR�D[HV�RI�WKH��nd MCP joint right (US lateral scan); 2b���'�86�UHFRQVWUXFWLRQ�RI�WKH�HURVLRQ�GLVSOD\HG�LQ��D��2c��FRQYHQWLRQDO�UDGLRJUDSK\�RI�the right hand with small erosion at 2nd MCP.

541Clinical and Experimental Rheumatology 2020
Imaging in pre-RA / A. Zabotti et al.
DJQRVLV� RU� IXOÀOOPHQW� RI� FODVVLÀFDWLRQ�criteria for RA (53). This possibility is not yet supported by evidence from randomised clinical trials, but differ-ent treatment management, including therapies with novel mechanisms of ac-tion could allow to prevent RA devel-opment (54). In this scenario, in which WKH�WUDGLWLRQDO�LQÁDPPDWRU\�V\PSWRPV�signs (e.g. morning stiffness, positive squeeze test) might not be present, the early visualisation of subclinical signs RI�LQÁDPPDWLRQ��VXFK�DV�E\�+5�S4&7��MRI and US, can be crucial to assist WKH�FOLQLFLDQ�LQ�D�EHWWHU�LGHQWLÀFDWLRQ�RI�people at high risk to develop RA.
AcknowledgementsThe authors thank Sarah Manske (As-sociate Professor, McCaig Institute for Bone and Joint Health, Department of Radiology, Cumming School of Medi-cine, University of Calgary) and Cheryl Barnabe (Associate Professor, Depart-ments of Medicine and Community Health Sciences, University of Calgary) for the images in Figure 2.
References 1. MCGONAGLE D, TAN AL, MØLLER DØHN U,
OSTERGAARD M, BENJAMIN M��0LFURDQD-WRPLF�VWXGLHV�WR�GHÀQH�SUHGLFWLYH�IDFWRUV�IRU�the topography of periarticular erosion for-PDWLRQ� LQ� LQÁDPPDWRU\� DUWKULWLV�� Arthritis Rheum���������������²����
2. KLEYER A, KRIETER M, OLIVEIRA I et al.��+LJK� SUHYDOHQFH� RI� WHQRV\QRYLDO� LQÁDPPD-tion before onset of rheumatoid arthritis and its link to progression to RA-A combined MRI/CT study. Semin Arthritis Rheum�������������������
3. SALAFFI F, CIAPETTI A, GASPARINI S, CAROTTI M, FILIPPUCCI E, GRASSI W�� $�clinical prediction rule combining routine assessment and power Doppler ultrasonogra-phy for predicting progression to rheumatoid arthritis from early-onset undifferentiated ar-thritis. Clin Exp Rheumatol ������������������
4. DUER-JENSEN A, HØRSLEV-PETERSEN K, HETLAND ML et al.��%RQH�HGHPD�RQ�PDJQHW-ic resonance imaging is an independent pre-dictor of rheumatoid arthritis development in patients with early undifferentiated arthritis. Arthritis Rheum���������������������
5. ZABOTTI A, ERRICHETTI E, ZULIANI F et al.��(DUO\�SVRULDWLF� DUWKULWLV�YHUVXV�HDUO\� VH-URQHJDWLYH� UKHXPDWRLG�DUWKULWLV�� UROH�RI�GHU-moscopy combined with ultrasonography for differential diagnosis. J Rheumatol ����������648-54.
6. ZABOTTI A, SALVIN S, QUARTUCCIO L, DE VITA S��'LIIHUHQWLDWLRQ� EHWZHHQ� HDUO\� UKHX-matoid and early psoriatic arthritis by the ultrasonographic study of the synovio-enthe-seal complex of the small joints of the hands.
Clin Exp Rheumatol ������������������ 7. BOS WH, WOLBINK GJ, BOERS M et al.��$UWK�
ritis development in patients with arthralgia is strongly associated with anti-citrullinated SURWHLQ�DQWLERG\�VWDWXV��D�SURVSHFWLYH�FRKRUW�study. Ann Rheum Dis �����������������
8. VAN STEENBERGEN HW, ALETAHA D, BEAART-VAN DE VOORDE LJJ et al.��(8/$5�GHÀQLWLRQ� RI� DUWKUDOJLD� VXVSLFLRXV� IRU� SUR-gression to rheumatoid arthritis. Ann Rheum Dis �����������������
����� GERLAG DM, RAZA K, VAN BAARSEN LGM et al.��(8/$5� UHFRPPHQGDWLRQV� IRU� WHUPL-nology and research in individuals at risk of UKHXPDWRLG� DUWKULWLV�� UHSRUW� IURP� WKH� 6WXG\�Group for Risk Factors for Rheumatoid Ar-thritis. Ann Rheum Dis�������������������
�����VAN STEENBERGEN HW, HUIZINGA TWJ, VAN DER HELM-VAN MIL AHM��7KH�SUHFOLQL-FDO�SKDVH�RI�UKHXPDWRLG�DUWKULWLV��ZKDW�LV�DF-knowledged and what needs to be assessed? Arthritis Rheum��������������������
11. DØHN UM, EJBJERG B, BOONEN A et al.�����No overall progression and occasional repair RI� HURVLRQV� GHVSLWH� SHUVLVWHQW� LQÁDPPDWLRQ�in adalimumab-treated rheumatoid arthritis SDWLHQWV��UHVXOWV�IURP�D�ORQJLWXGLQDO�FRPSDUD-tive MRI, ultrasonography, CT and radiogra-phy study. Ann Rheum Dis������������������
12. PELUSO G, BOSELLO SL, GREMESE E et al.��Detection of bone erosions in early rheu-PDWRLG� DUWKULWLV�� �'� XOWUDVRQRJUDSK\� YHUVXV�computed tomography. Clin Rheumatol ������������������
13. PHELPS ME, HUANG SC, HOFFMAN EJ, SE-LIN C, SOKOLOFF L, KUHL DE��7RPRJUDSKLF�measurement of local cerebral glucose meta-EROLF� UDWH� LQ� KXPDQV� ZLWK� �)������ÁXRUR���GHR[\�'�JOXFRVH�� YDOLGDWLRQ� RI� PHWKRG��Ann Neurol������������������
14. MATSUI T, NAKATA N, NAGAI S et al.��,QÁDP-matory cytokines and hypoxia contribute to 18F-FDG uptake by cells involved in pannus formation in rheumatoid arthritis. J Nucl Med �����������������
15. ROIVAINEN A, HAUTANIEMI S, MÖTTÖNEN T et al.��&RUUHODWLRQ�RI���)�)'*�3(7�&7�DV-sessments with disease activity and markers RI� LQÁDPPDWLRQ� LQ�SDWLHQWV�ZLWK�HDUO\� UKHX-matoid arthritis following the initiation of combination therapy with triple oral antirheu-matic drugs. Eur J Nucl Med Mol Imaging ������������������
16. GRAM SB, HESS S, AHLQUIST P, HØILUND-CARLSEN PF, ELLINGSEN T�� >18F]Sodium ÁXRULGH� SRVLWURQ� HPLVVLRQ� WRPRJUDSK\�FRPSXWHG� WRPRJUDSK\�� D� SUHGLFWRU� RI� HDUO\�rheumatoid arthritis? A case report. Scand J Rheumatol������������������
17. BARNABE C, TOEPFER D, MAROTTE H et al.��'HÀQLWLRQ� IRU� UKHXPDWRLG� DUWKULWLV� HURVLRQV�imaged with high resolution peripheral quan-titative computed tomography and interread-er reliability for detection and measurement. J Rheumatol��������������������
18. PETERS M, DE JONG J, SCHARMGA A et al.��An automated algorithm for the detection of cortical interruptions and its underlying loss of trabecular bone; a reproducibility study. BMC Med Imaging���������������
�����WERNER D, SIMON D, ENGLBRECHT M et al.��(DUO\�FKDQJHV�RI�WKH�FRUWLFDO�PLFUR�FKDQ-
nel system in the bare area of the joints of patients with rheumatoid arthritis. Arthritis Rheumatol��+RERNHQ��������������������
�����KLEYER A, FINZEL S, RECH J et al.�� %RQH�loss before the clinical onset of rheumatoid arthritis in subjects with anticitrullinated pro-tein antibodies. Ann Rheum Dis� ������ �������²����
21. COLEBATCH AN, EDWARDS CJ, ØSTER-GAARD M et al.��(8/$5�UHFRPPHQGDWLRQV�for the use of imaging of the joints in the clinical management of rheumatoid arthritis. Ann Rheum Dis ������������������
22. BAKER JF, CONAGHAN PG, GANDJBAKHCH F��8SGDWH�RQ�PDJQHWLF�UHVRQDQFH�LPDJLQJ�DQG�ultrasound in rheumatoid arthritis. Clin Exp Rheumatol ����������6XSSO��������6�������
23. KRABBEN A, STOMP W, HUIZINGA TWJ et al.��&RQFRUGDQFH�EHWZHHQ�LQÁDPPDWLRQ�DW�SK\VL-cal examination and on MRI in patients with early arthritis. Ann Rheum Dis ��������������12.
24. MACHADO PMMC, KOEVOETS R, BOMBAR-DIER C, VAN DER HEIJDE DM�� 7KH� YDOXH� RI�magnetic resonance imaging and ultrasound LQ�XQGLIIHUHQWLDWHG�DUWKULWLV�� D� V\VWHPDWLF� UH-view. J Rheumatol Suppl�����������������
25. ØSTERGAARD M, PETERFY C, CONAGHAN P et al.�� 20(5$&7� 5KHXPDWRLG� $UWKULWLV�Magnetic Resonance Imaging Studies. Core VHW�RI�05,�DFTXLVLWLRQV��MRLQW�SDWKRORJ\�GHÀ-nitions, and the OMERACT RA-MRI scoring system. J Rheumatol ������������������
26. GLINATSI D, BIRD P, GANDJBAKHCH F et al.��Development and validation of the OMER-ACT rheumatoid arthritis magnetic resonance tenosynovitis scoring system in a multireader exercise. J Rheumatol��������������������
27. HAAVARDSHOLM EA, AGA A-B, OLSEN IC et al.�� 8OWUDVRXQG� LQ� PDQDJHPHQW� RI� UKHX-PDWRLG� DUWKULWLV��$5&7,&� UDQGRPLVHG� FRQ-trolled strategy trial. BMJ �����������L������
28. EJBJERG B, NARVESTAD E, ROSTRUP E et al.�� 0DJQHWLF� UHVRQDQFH� LPDJLQJ� RI� ZULVW�DQG� ÀQJHU� MRLQWV� LQ� KHDOWK\� VXEMHFWV� RFFD-sionally shows changes resembling erosions and synovitis as seen in rheumatoid arthritis. Arthritis Rheum���������������������
�����MANGNUS L, VAN STEENBERGEN HW, REI-JNIERSE M, VAN DER HELM-VAN MIL AHM��Magnetic resonance imaging-detected fea-WXUHV�RI�LQÁDPPDWLRQ�DQG�HURVLRQV�LQ�V\PS-tom-free persons from the general popula-tion. Arthritis Rheumatol� �+RERNHQ�� ��������������������
�����BOETERS DM, RAZA K, VAN DER HELM-VAN MIL AHM�� :KLFK� SDWLHQWV� SUHVHQWLQJ� ZLWK�arthralgia eventually develop rheumatoid arthritis? The current state of the art. RMD Open ���������H��������
31. BOETERS DM, NIEUWENHUIS WP, VAN STEENBERGEN HW, REIJNIERSE M, LAN-DEWÉ RBM, VAN DER HELM-VAN MIL AHM��$UH�05,�GHWHFWHG�HURVLRQV�VSHFLÀF�IRU�5$"�A large explorative cross-sectional study. Ann Rheum Dis �����������������
32. KRABBEN A, STOMP W, VAN DER HEIJDE DMFM et al.��05,�RI�KDQG�DQG�IRRW�MRLQWV�RI�patients with anticitrullinated peptide anti-body positive arthralgia without clinical ar-thritis. Ann Rheum Dis�������������������
33. GENT YYJ, TER WEE MM, AHMADI N et al.��

542 Clinical and Experimental Rheumatology 2020
Imaging in pre-RA / A. Zabotti et al.
Three-year clinical outcome following base-line magnetic resonance imaging in anti-cit-rullinated protein antibody-positive arthral-JLD� SDWLHQWV�� DQ� H[SORUDWRU\� VWXG\��Arthritis Rheumatol��+RERNHQ���������������������
34. VAN STEENBERGEN HW, VAN NIES JAB, HUI-ZINGA TWJ, BLOEM JL, REIJNIERSE M, VAN DER HELM-VAN MIL AHM�� &KDUDFWHULVLQJ�arthralgia in the preclinical phase of rheu-matoid arthritis using MRI. Ann Rheum Dis �������������������
35. VAN STEENBERGEN HW, MANGNUS L, REIJ-NIERSE M, HUIZINGA TWJ, VAN DER HELM-VAN MIL AHM�� &OLQLFDO� IDFWRUV�� DQWLFLWUXOOL-nated peptide antibodies and MRI-detected VXEFOLQLFDO� LQÁDPPDWLRQ� LQ� UHODWLRQ� WR� SUR-gression from clinically suspect arthralgia to arthritis. Ann Rheum Dis �������������������
36. VAN STEENBERGEN HW, VAN NIES JAB, HU-IZINGA TWJ, REIJNIERSE M, VAN DER HELM-VAN MIL AHM�� 6XEFOLQLFDO� LQÁDPPDWLRQ�RQ�MRI of hand and foot of anticitrullinated peptide antibody-negative arthralgia patients at risk for rheumatoid arthritis. Arthritis Res Ther ����������5����
37. TEN BRINCK RM, VAN STEENBERGEN HW, VAN DER HELM-VAN MIL AHM�� 6HTXHQFH� RI�MRLQW�WLVVXH�LQÁDPPDWLRQ�GXULQJ�UKHXPDWRLG�arthritis development. Arthritis Res Ther ���������������
38. TEN BRINCK RM, VAN STEENBERGEN HW, VAN DER HELM-VAN MIL AHM��'HYHORSPHQW�RI�FOLQLFDOO\�DSSDUHQW�V\QRYLWLV��D�ORQJLWXGL-nal study at the joint level during progression WR� LQÁDPPDWRU\�DUWKULWLV��RMD Open� ���������H��������
�����BOER AC, BURGERS LE, MANGNUS L et al.��8VLQJ� D� UHIHUHQFH�ZKHQ� GHÀQLQJ� DQ� DEQRU-mal MRI reduces false-positive MRI results-a longitudinal study in two cohorts at risk for rheumatoid arthritis. Rheumatology (Oxford)
�����������������������COMBE B, LANDEWE R, DAIEN CI et al.��
����� XSGDWH� RI� WKH� (8/$5� UHFRPPHQGD-tions for the management of early arthritis. Ann Rheum Dis�������������������
41. ZABOTTI A, BANDINELLI F, BATTICCIOTTO A et al.�� 0XVFXORVNHOHWDO� XOWUDVRQRJUDSK\�IRU� SVRULDWLF� DUWKULWLV� DQG� SVRULDVLV� SDWLHQWV��a systematic literature review. Rheumatology �2[IRUG���������������������
42. AYDIN SZ, PAY S, INANC N et al.��:KLFK�MRLQWV�and why do rheumatologists scan in rheuma-toid arthritis by ultrasonography? A real life experience. Clin Exp Rheumatol ������ ������������
43. ZABOTTI A, MANDL P, ZAMPOGNA G, DE-JACO C, IAGNOCCO A�� 2QH� \HDU� LQ� UHYLHZ�������XOWUDVRQRJUDSK\�LQ�UKHXPDWRLG�DUWKUL-tis and psoriatic arthritis. Clin Exp Rheuma-tol�������������������
44. CHEN S, ZHENG Q, LIU H et al.�� 6RQRJUD-phy is superior to serum-based biomarkers for measuring disease status in experimental rheumatoid arthritis. J Ultrasound Med �������������������
45. NAM JL, HENSOR EMA, HUNT L, CONAGHAN PG, WAKEFIELD RJ, EMERY P�� 8OWUDVRXQG�ÀQGLQJV�SUHGLFW�SURJUHVVLRQ�WR�LQÁDPPDWRU\�arthritis in anti-CCP antibody-positive pa-tients without clinical synovitis. Ann Rheum Dis�������������������
46. VAN DER VEN M, VAN DER VEER-MEERKERK M, TEN CATE DF et al.��$EVHQFH�RI�XOWUDVRXQG�LQÁDPPDWLRQ�LQ�SDWLHQWV�SUHVHQWLQJ�ZLWK�DU-thralgia rules out the development of arthri-tis. Arthritis Res Ther����������������
47. VAN BEERS-TAS MH, BLANKEN AB, NIELEN MMJ et al.�� 7KH� YDOXH� RI� MRLQW� XOWUDVRQR�graphy in predicting arthritis in seropositive SDWLHQWV�ZLWK�DUWKUDOJLD��D�SURVSHFWLYH�FRKRUW�study. Arthritis Res Ther ���������������
48. HORTON SC, TAN AL, WAKEFIELD RJ, FREES-TON JE, BUCH MH, EMERY P��8OWUDVRXQG�GH-tectable grey scale synovitis predicts future IXOÀOPHQW� RI� WKH� ����� $&5�(8/$5� 5$�FODVVLÀFDWLRQ� FULWHULD� LQ� SDWLHQWV� ZLWK� QHZ�onset undifferentiated arthritis. RMD Open ���������H��������
�����SAHBUDIN I, PICKUP L, NIGHTINGALE P et al.��7KH�UROH�RI�XOWUDVRXQG�GHÀQHG�WHQRV\QR-vitis and synovitis in the prediction of rheu-matoid arthritis development. Rheumatology �2[IRUG�������$SU���>(SXE�DKHDG�RI�SULQW@�
�����D’AGOSTINO MA, TERSLEV L, WAKEFIELD R et al.��1RYHO�DOJRULWKPV�IRU�WKH�SUDJPDWLF�use of ultrasound in the management of pa-WLHQWV�ZLWK�UKHXPDWRLG�DUWKULWLV��IURP�GLDJQR-sis to remission. Ann Rheum Dis ������ ������������
51. FREESTON JE, WAKEFIELD RJ, CONAGHAN PG, HENSOR EMA, STEWART SP, EMERY P��A diagnostic algorithm for persistence of YHU\�HDUO\� LQÁDPPDWRU\�DUWKULWLV�� WKH�XWLOLW\�of power Doppler ultrasound when added to conventional assessment tools. Ann Rheum Dis������������������
52. KAWASHIRI S-Y, FUJIK K, NISHINO A et al.��Combination of ultrasound power Doppler-YHULÀHG� V\QRYLWLV� DQG� VHURSRVLWLYLW\� DFFX-UDWHO\� LGHQWLÀHV� SDWLHQWV� ZLWK� HDUO\�VWDJH�rheumatoid arthritis. Int J Rheum Dis������������������
53. BURGERS LE, RAZA K, VAN DER HELM-VAN MIL AH��:LQGRZ�RI�RSSRUWXQLW\�LQ�UKHXPD-WRLG�DUWKULWLV�²�GHÀQLWLRQV�DQG�VXSSRUWLQJ�HYL-GHQFH�� IURP� ROG� WR� QHZ� SHUVSHFWLYHV��RMD Open����������H��������
54. AUNGIER SR, CARTWRIGHT AJ, SCHWEN-ZER A et al.��7DUJHWLQJ�HDUO\�FKDQJHV�LQ� WKH�V\QRYLDO�PLFURHQYLURQPHQW�� D� QHZ� FODVV� RI�immunomodulatory therapy? Ann Rheum Dis �����������������