Upload
others
View
0
Download
0
Embed Size (px)
Citation preview
Review ArticleStem Cells Applications in Regenerative Medicine andDisease Therapeutics
Ranjeet Singh Mahla
Department of Biological Sciences, Indian Institute of Science Education and Research (IISER),Bhopal, Madhya Pradesh 462066, India
Correspondence should be addressed to Ranjeet Singh Mahla; [email protected]
Received 13 March 2016; Accepted 5 June 2016
Academic Editor: Paul J. Higgins
Copyright © 2016 Ranjeet Singh Mahla.This is an open access article distributed under theCreative CommonsAttribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Regenerative medicine, the most recent and emerging branch of medical science, deals with functional restoration of tissues ororgans for the patient suffering from severe injuries or chronic disease. The spectacular progress in the field of stem cell researchhas laid the foundation for cell based therapies of disease which cannot be cured by conventional medicines. The indefiniteself-renewal and potential to differentiate into other types of cells represent stem cells as frontiers of regenerative medicine.The transdifferentiating potential of stem cells varies with source and according to that regenerative applications also change.Advancements in gene editing and tissue engineering technology have endorsed the ex vivo remodelling of stem cells grown into 3Dorganoids and tissue structures for personalized applications.This review outlines the most recent advancement in transplantationand tissue engineering technologies of ESCs, TSPSCs, MSCs, UCSCs, BMSCs, and iPSCs in regenerative medicine. Additionally,this review also discusses stem cells regenerative application in wildlife conservation.
1. Introduction
Regenerativemedicine, themost recent and emerging branchof medical science, deals with functional restoration ofspecific tissue and/or organ of the patients suffering withsevere injuries or chronic disease conditions, in the statewhere bodies own regenerative responses do not suffice [1].In the present scenario donated tissues and organs cannotmeet the transplantation demands of aged and diseasedpopulations that have driven the thrust for search for thealternatives. Stem cells are endorsed with indefinite celldivision potential, can transdifferentiate into other types ofcells, and have emerged as frontline regenerative medicinesource in recent time, for reparation of tissues and organsanomalies occurring due to congenital defects, disease, andage associated effects [1]. Stem cells pave foundation for all tis-sue and organ system of the body andmediates diverse role indisease progression, development, and tissue repair processesin host. On the basis of transdifferentiation potential, stemcells are of four types, that is, (1) unipotent, (2) multipotent,(3) pluripotent, and (4) totipotent [2]. Zygote, the onlytotipotent stem cell in human body, can give rise to whole
organism through the process of transdifferentiation, whilecells from inner cells mass (ICM) of embryo are pluripotentin their nature and can differentiate into cells representingthree germ layers but do not differentiate into cells ofextraembryonic tissue [2]. Stemness and transdifferentiationpotential of the embryonic, extraembryonic, fetal, or adultstem cells depend on functional status of pluripotency fac-tors like OCT4, cMYC, KLF44, NANOG, SOX2, and soforth [3–5]. Ectopic expression or functional restoration ofendogenous pluripotency factors epigenetically transformsterminally differentiated cells into ESCs-like cells [3], knownas induced pluripotent stem cells (iPSCs) [3, 4]. On the basisof regenerative applications, stem cells can be categorized asembryonic stem cells (ESCs), tissue specific progenitor stemcells (TSPSCs), mesenchymal stem cells (MSCs), umbilicalcord stem cells (UCSCs), bone marrow stem cells (BMSCs),and iPSCs (Figure 1; Table 1).The transplantation of stem cellscan be autologous, allogenic, and syngeneic for induction oftissue regeneration and immunolysis of pathogen or malig-nant cells. For avoiding the consequences of host-versus-graft rejections, tissue typing of human leucocyte antigens(HLA) for tissue and organ transplant as well as use of
Hindawi Publishing CorporationInternational Journal of Cell BiologyVolume 2016, Article ID 6940283, 24 pageshttp://dx.doi.org/10.1155/2016/6940283
2 International Journal of Cell Biology
Healthy donor
Patient
(1) ESCs, (2) TSPSCs, (3) MSCs , (4) UCSCs,(5) BMSCs , (6) IPSCs
Promises of stem cells in regenerative medicines
(1)
(2)
(3)
(4)
(5)
(6)
(i) T1DM and T2DM treatment(ii) SLE (autoimmune disease) treatment
(iii) Application for HI treatment(iv) Krabbe’s disease treatment(v) Hematopoiesis in neuroblastoma
(i) Improvement of spinal cord injury(ii) Regeneration of retinal sheet
(iii) Generation of retinal ganglion cells(iv) Healing of heart defects(v) Hepatic cell formation
(vii) Cartilage lesion treatment(viii) Regeneration of pacemaker
(ix) In vitro gametogenesis
(i) Regeneration of kidney tissue(ii) Vision restoration in AMD(iii) Treatment of placental defects (iv) Treatment of brain cortex defects(v) ASD and autism treatment
(vi) Treatment of liver and lung disease(vii) Generation of serotonin neurons(viii) Regeneration of pacemaker
(i) Treatment of diabetes and retinopathy (ii) Neurodental therapeutic applications
(iii) Restoration of cognitive functions(iv) Brain and cancer treatment (v) Ear acoustic function restoration
(vi) Regeneration of intestinal mucosa (vii) Treatment of vision defects
(viii) Muscle regeneration(ix) Regeneration of fallopian tube
(i) Regeneration of bladder tissue(ii) Muscle regeneration
(iii) Regeneration of teeth tissue(iv) Healing of orthopedic injuries (v) Recovery from muscle injuries
(vi) Hear scar repair after attack
(i) Treatment of anemia and blood cancer(ii) Retroviral therapy
(iii) Correction of neuronal defects(iv) Generation of functional platelets(v) Alveolar bone regeneration
(vi) Regeneration of diaphragm tissue
(vi) Formation of insulin secreting 𝛽-cells
Figure 1: Promises of stem cells in regenerative medicine: the six classes of stem cells, that is, embryonic stem cells (ESCs), tissue specificprogenitor stem cells (TSPSCs), mesenchymal stem cells (MSCs), umbilical cord stem cells (UCSCs), bone marrow stem cells (BMSCs), andinduced pluripotent stem cells (iPSCs), have many promises in regenerative medicine and disease therapeutics.
immune suppressant is recommended [6]. Stem cells expressmajor histocompatibility complex (MHC) receptor in lowand secret chemokine that recruitment of endothelial andimmune cells is enabling tissue tolerance at graft site [6].The current stem cell regenerative medicine approaches arefounded onto tissue engineering technologies that combinethe principles of cell transplantation, material science, andmicroengineering for development of organoid; those canbe used for physiological restoration of damaged tissue andorgans. The tissue engineering technology generates nascenttissue on biodegradable 3D-scaffolds [7, 8].The ideal scaffoldssupport cell adhesion and ingrowths, mimic mechanics oftarget tissue, support angiogenesis and neovascularisationfor appropriate tissue perfusion, and, being nonimmuno-genic to host, do not require systemic immune suppres-sant [9]. Stem cells number in tissue transplant impactsupon regenerative outcome [10]; in that case prior ex vivoexpansion of transplantable stem cells is required [11]. Forsuccessful regenerative outcomes, transplanted stem cellsmust survive, proliferate, and differentiate in site specific
manner and integrate into host circulatory system [12]. Thisreview provides framework of most recent (Table 1; Figures1–8) advancement in transplantation and tissue engineeringtechnologies of ESCs, TSPSCs, MSCs, UCSCs, BMSCs, andiPSCs in regenerativemedicine. Additionally, this review alsodiscusses stem cells as the tool of regenerative applications inwildlife conservation.
2. ESCs in Regenerative Medicine
For the first time in 1998, Thomson isolated human ESCs(hESCs) [13]. ESCs are pluripotent in their nature and cangive rise to more than 200 types of cells and promises forthe treatment of any kinds of disease [13]. The pluripo-tency fate of ESCs is governed by functional dynamics oftranscription factors OCT4, SOX2, NANOG, and so forth,which are termed as pluripotency factors. The two allelesof the OCT4 are held apart in pluripotency state in ESCs;phase through homologues pairing during embryogenesis
International Journal of Cell Biology 3Ta
ble1:Ap
plicationof
stem
cells
inregenerativ
emedicine:ste
mcells
(ESC
s,TS
PSCs
,MSC
s,UCS
Cs,B
MSC
s,andiPSC
s)have
diverseapplications
intissueregeneratio
nanddisease
therapeutic
s.
SCs
Dise
ase
Factorsc
ausin
gdisease
Mod
eofstem
cells
application
Physiologicaland
mechanisticaspectso
fste
mcells
therapeutics
Improvem
entsin
diseases
ignatures&
future
use
References
ESCs
Spinalcord
injurie
sInfection,
cancer,and
accidents
ESCs
transplantationto
injury
site
ESCs
andsecreted
vasculogenicand
neurogenicfactor
supp
orttissue
homing
Regeneratio
nof
spinaltissuea
ndim
proved
balancea
ndsensation
[15]
ARM
Dand
glaucoma
Macular
cones
degeneratio
n
ESCs
-derived
conesa
ndRG
Cstransplantationto
eye
COCO
(activatingTG
F-𝛽,B
MP,and
Wnt)&
BRN3(kno
ck-in
byCR
ISPE
R-Ca
s9)m
akeE
SCsb
ecom
econesa
ndRG
Csform
cells
sheet&
neuron
alconn
ectio
n
Recovery
from
ARM
Dandmacular
defects&
resto
ratio
nof
visio
n[16,17]
Cardiovascular
disease
Diabetes,drugs,
genetic
factor,
andlifes
tyle
ESCs
-derived
CMs&
biom
aterialcoaxedES
Cs
Cardiomyocytese
xpressGCa
MP3
,secretingvasculogenicfactors,andTb
ox3
differentiatesE
SCsintoSA
NPC
s
Supp
resses
heartarrhythmias.CM
sele
ctroph
ysiologically
integratetoheart
aspacemaker
[18,19,28]
Liverinjuries
Toxins,drugs,
genetic
factors,
andinfection
Transplantationof
ESCs
-derived
hepatocytes
ESCs
-hepatocytec
onversionismarked
with
expressio
nof
Cytp450,PX
R,CY
PA4&
29,H
NF4
-𝛼,and
UGTA
1;cells
intransplant
repo
pulateinjured
liver
tissue
Regeneratio
nof
liver
tissuec
anbe
used
asmod
elforscreening
ofdrugs
[20,23,24]
Diabetes
Lifesty
le,heart
defects,and
genetic
s
Transplantationof
ESCs
-derived
PPCs
Progenito
rs(C
D24+
,CD49+
&CD
133+)
differentiateinto𝛽-cells,
secreteinsulin,
andexpressP
DX1,G
CK,and
GLU
T2
Improvem
entinglucoselevelandob
esity
canbe
used
fortreatmento
fT1D
Mand
T2DM
[25,26]
Oste
oarthritis
Whencartilage
tissuew
ears
away
Transplantationof
chon
drocytes
organo
ids
Chon
drocytes
(SOX9+
&collagen-II+
)form
cells
aggregate&
remainactiv
efor
12wks
attransplantationsite
Regeneratio
nof
cartilage
tissuec
anbe
used
fortreatmento
finjuriesfaced
byathletes
[27]
TSPS
Cs
Diabetes
Lifesty
leand
genetic
factors
Transplantationof
SCs
deriv
edPP
Csorgano
idPP
Csneed
niches
uppo
rted
activ
eFGF&
Notch
signalling
tobecome𝛽
-cell
PPCs
occupancyas𝛽-cellcan
treatT1DM
&T2
DM
[25,29,30]
Neurodental
prob
lems
Accidents,age,
andgenetic
factors
Transplantationof
DSP
SCsa
sneurons
Neurons
expressn
estin
,GFA
P,𝛽III-tubu
lin,and
L-type
Ca2+
channels
Possibleapplicationin
treatmento
fneurod
entalabn
ormalities
[31,32]
Acou
sticp
roblem
sAge,noise,
drugs,and
infection
IESC
s/IESC
s-deriv
edhaircells
transplantation𝛾-secretase
shutsN
otch
by𝛽-catenin
&Atoh
1inlrg
5+IESC
stobe
haircells
Cochlearregenerationleadsto
resto
ratio
nof
acou
sticfunctio
ns[34,35]
Intestinal
degeneratio
n
Geneticfactors
andfood
borne
infections
IPCs
deriv
edcrypt-v
illi
organo
idtransplantation
M𝜙,m
yofib
roblasts,
andbacteriasig
nals
IPCs
tobe
crypt-v
illiorganoidtissue
Regeneratio
nof
gobletmucosac
antre
atintestinaldefects
[36–
38]
Cornealdiseases
Burns,genetic
s,and
inflammation
LPSC
stransplantatio
nto
cornealtissue
LPSC
sintransplant
markedby
ABC
B5differentiateinto
maturec
ornea
Regeneratio
nof
cornealtissue
might
treat
multip
leeyed
isease
[39,40
]
Muscular
deform
ities
Infection,
drugs,
and
autoim
mun
ity
Transplantationof
PEG
fibrin
ogen
coaxed
MABs
PDGFfro
mMABs
attractvasculogenic
andneurogeniccells
totransplant
site
Muscle
fibril
regeneratio
n;skeletal
muscle
defectstreatment
[41,42]
Eyed
isease&
retin
opathy
Toxins,burns,
andgenetic
factors
AdSC
sintravitre
altransplantation
AdSC
sfrom
healthydo
norp
rodu
cehigh
ervasoprotectiv
efactors
Resto
ratio
nof
vascularisa
tion,
diabetic
retin
opathy
treatment
[44,45]
Cardiac
dysfu
nctio
ns
Age,genetic
factors,and
toxins
Syste
micinfusio
nof
CA-AdS
Csmyocardium
CA-AdS
Csto
epith
elium
differentiatio
nares
uperiortoAd
SCs
Regeneratio
nof
ischemicmyocardium
[47,48]
4 International Journal of Cell Biology
Table1:Con
tinued.
SCs
Dise
ase
Factorsc
ausin
gdisease
Mod
eofstem
cells
application
Physiologicaland
mechanisticaspectso
fste
mcells
therapeutics
Improvem
entsin
diseases
ignatures&
future
use
References
MSC
s
Bladder
deform
ities
Cystitis,cancer,
andinfection
Transplantationof
BD-M
SCstobladder
BDMSC
s(CD
105+,C
D73+
,CD34−
,and
CD45−
)with
SIShealbladderin10wks
Bladderregenerationfro
mdifferent
originsM
SCs
[50,51]
Dentalproblem
sInfection,
cancer
age,and
accidents
Transplantso
fEMSC
s+DSC
sbiopo
lymer
tissue
EMSC
-DSC
sand
vasculogenicfactorsin
biop
olym
ergive
risetomatureteeth
units
Regeneratio
nof
oraltissuea
ndapplicationin
perio
dontics
[31,52]
Bone
degeneratio
nInjurie
sand
tumor
autoim
mun
ity
CoaxedMSC
stransplant
&MSC
sinfusion
Actin
mod
ellin
gby
cytochalasin-D
transfo
rmsM
SCsintoosteob
lasts
Regeneratio
nof
bones,redu
ctionin
injury
pain
[53–55]
Muscle
degeneratio
nGeneticfactors
andworkstr
ess
CoaxedMSC
stransplant
andMSC
sinfusion
Alginateg
elprotectsMSC
sfrom
immun
eattack
andcontrolsGFs
release
Regeneratio
nof
heartscara
ndmuscle
tissueincontrolledway
[56,57]
Alopecia
Age,dise
ase,
andmedicine
use
Transplantationof
GAG
-coatedDPC
s
GAG
coatingmim
icsE
CMmicroenvironm
ent,prom
otingDPC
sregeneratio
n
Regeneratio
nof
hairfollicle
fortreatment
ofalop
ecia
[58]
UCS
Cs
Con
genitalh
eart
defects
Develo
pmental
errors
Transplantationof
fibrin
coaxed
AFS
CsAd
ditio
nof
VEF
Gto
PEGcoaxed
AFS
Csprom
otes
organo
genesis
Regeneratio
nof
tissuer
epairfor
treatmento
fheartdefects
[59,60]
Diabetes
Lifesty
leand
genetic
factors
WJ-SC
s,transplantation,
andintravenou
sinjection
WJ-factors&
M𝜙differentiateWJ-SC
sinto𝛽-cells,
decreasin
gIL6&IL1𝛽
Improvem
entinfunctio
nof𝛽-cellsleads
totre
atmento
fdiabetes
[7,9,61–63]
SLE
Autoim
mun
ityIntravenou
sinfusionof
WJ-SC
sWJ-SC
sdecreaseS
LEDAI&
BILA
G;
reinfusio
nprotectsfro
mdiseaser
elapse
Improvem
entinrenalfun
ctions
&sto
ppingdegeneratio
nof
tissues
[64]
LSD&
neurod
egenerative
diseases
Genetics,tumor,
age,andlife
style
Allo
genicU
CSCs
cells
andbiom
aterialcoaxed
UCS
Csorgano
ids
Organoids
consisted
ofneurob
lasts
(GFA
P+,N
estin+
,and
Ki67+
)&SC
s(O
CT4+,SOC2+
);UCS
Csrecoverfrom
MSE
deficiencyandim
provec
ognitio
n
Treatm
ento
fKrabb
e’sdisease,hu
rler
synd
rome,MLD
,TSD
,ALD
,AD,A
LS,
SCI,SC
I,TB
I,Parkinson's,str
oke,andso
forth
[65–67]
Cartilage
and
tend
oninjurie
sAc
cident
Transplantationof
UCB
-SCs
,UCB
-SCs
-HA
gel
HAgelfactorsprom
oter
egenerationof
hyalinec
artilage&
tend
onsinwks
time
Recovery
from
tend
onsa
ndcartilage
injurie
s[68,69]
Hod
gkin’s
lymph
oma
Geneticand
environm
ental
Transplantationof
UCS
CsSecond
dose
infectionof
allogenic
UCS
Csim
proves
patie
ntslife
by30%
Treatm
ento
fHod
gkin’slymph
omaa
ndotherc
ancers
[10]
Periton
ealfi
brosis
Long
term
renal
dialysisand
fibrosis
WJ-SC
s,transplantation
byIP
injection
WJ-SC
sprevent
programmed
cells
death
andperiton
ealw
allthickness
Effectiv
eintre
atmento
fencapsulatin
gperiton
ealfi
brosis
[70]
International Journal of Cell Biology 5
Table1:Con
tinued.
SCs
Dise
ase
Factorsc
ausin
gdisease
Mod
eofstem
cells
application
Physiologicaland
mechanisticaspectso
fste
mcells
therapeutics
Improvem
entsin
diseases
ignatures&
future
use
References
BMSC
s
Anaem
iaand
bloo
dcancer
Injury,genetics
autoim
mun
ityTw
o-ste
pinfusio
nof
lymph
oidandmyeloid
Haploidentic
alBM
SCsc
anreconstruct
immun
ity,w
hich
ismajor
processfor
minority
Treatm
ento
faplastic
anaemia&
haem
atologicalmalignancies
[71]
AID
SHIV
1infectio
nTransplantationof
HIV
1resistant
CD4+
cells
Anti-H
IV1C
D4+
cells
expressH
IV1
anti-RN
A,w
hich
restric
tHIV
infection
Treatm
ento
fAID
Sas
analternativeo
fantiretroviral
[72,73]
Bloo
dclo
tting
disorders
Lack
ofplatele
tsTransplantationof
megakaryocyte
organo
ids
GFs
insilkspon
ge,m
icrotubu
le3D
scaffolds
mim
icbo
nemarrow
Therapeutic
sofb
urns
andbloo
dclo
tting
diseases
[74,75]
Neurodegenerativ
ediseases
Accidents,age,
trauma,and
stroke
Focaltransplanto
fBM
SCsw
ithLA
LA+
BMSC
sind
ucen
eovascularisa
tion
thatdirectsm
icrogliaforc
olon
ization
Treatm
ento
fneuronald
amaged
isorders
andcogn
itive
resto
ratio
n[76]
Orodental
deform
ities
Trauma,disease,
andbirthdefects
Bone
marrowderiv
edste
m&progenito
r(TRC
)
CD14+
&CD
90+
TRCacceleratealveolar
jawbo
neregeneratio
nRe
generatio
nof
defectsinoralbo
ne,skin,
andgum
[77]
Diaph
ragm
abno
rmalities
Accidents&
birthdefects
Implantatio
nof
decellu
lariz
eddiaphragm
BMSC
sniche
perfused
hemidiaph
ragm
hassim
ilarm
yography
&spiro
metry
Replacem
enttherapy
bydo
nord
erived
niched
diaphragm
[8]
iPSC
s
Eyed
efects
Age,genetics,
andbirthdefects
iPSC
sderived
NPC
stransplantation
NPC
sform
5-6layersof
photoreceptor
nucle
i,resto
ringvisualacuity
Treatm
ento
fARM
Dandother
age-related
eyed
efects
[78–80]
Neurodegenerativ
edisorders
Accidents,age,
trauma,and
stroke
iGABA
-INsa
ndcortical
spheroid
transplantation
(iGABA
-INs)secreteG
ABA
;FOX1G
causeA
SD,sph
eroidmim
icstobrain
ASD
,Alzh
eimer's,seizer,and
obstinate
epilepsiestreatment
[81–84]
Liver&
lung
diseases
A1A
Ddeficiency
Transplantationof
A1A
Dmutationcorrected
iPSC
s
A1A
Disencodedby
SERP
INA1inliver,
andmutationleadstodrugssensitivity
Treatm
ento
fCOPD
causinglung
sand
liver
degeneratio
n[85]
Diabetes
Lifesty
leand
genetic
factors
iPSC
sderived𝛽-cells
transplantation
Skin
to𝛽-cellsreprogrammingph
ase
throug
hcD
E&cPFrequ
iresG
PsTreatm
ento
fT1D
MandT2
DM
and
insulin
prod
uctio
n[86]
Lung
degeneratio
nTu
berculosis,
cancer,and
fibrosis
Biom
aterialcoaxed
iPSC
stransplantatio
nMiniature
iPSC
slun
gresembles
airw
ays
andalveoli,mod
eldrug
testing
Regeneratio
nof
lung
tissue
[87]
SIDsa
ndAID
SAge,genetic
factors,and
infection
Transplantationof
Oct4
andNanog
corrected
iPSC
s
CRISPE
R-Ca
s9generateiPSC
sinsin
gle
step;iPSC
s-M𝜙resistsHIV
1Im
mun
otherapy
ofSIDs,HIV
1,andother
immun
edise
ases
[80,88,89]
6 International Journal of Cell Biology
Egg Blastocyst Embryo Embryonic stem cells
Diabetic treatment
Regeneration ofcardiac tissue
Drug screeningRegeneration of liver
Differentiation
COCO
Cone cells
ARMDtreatment
CardiomyocytesHepatocytes PPCsChondrocytes
Fibrin embedding
Regenerationof cartilage
RGC
Glaucoma treatmentDrug screening
ESCs in regenerative medicine
Pacemakercells
Restorationof heartrhythm
..
IVG
Infertilitytreatment
Ther
apeu
tic ap
plic
atio
ns
Ther
apeu
tic ap
plic
atio
ns
K2 + LA
𝛽-cells
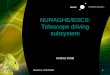
Figure 2: ESCs in regenerative medicine: ESCs, sourced from ICM of gastrula, have tremendous promises in regenerative medicine. Thesecells can differentiate into more than 200 types of cells representing three germ layers. With defined culture conditions, ESCs can betransformed into hepatocytes, retinal ganglion cells, chondrocytes, pancreatic progenitor cells, cone cells, cardiomyocytes, pacemaker cells,eggs, and sperms which can be used in regeneration of tissue and treatment of disease in tissue specific manner.
and transdifferentiation processes [14] has been consideredas critical regulatory switch for lineage commitment of ESCs.The diverse lineage commitment potential represents ESCsas ideal model for regenerative therapeutics of disease andtissue anomalies. This section of review on ESCs discussestransplantation and transdifferentiation of ESCs into retinalganglion, hepatocytes, cardiomyocytes, pancreatic progeni-tors, chondrocytes, cones, egg sperm, and pacemaker cells(Figure 2; Table 1). Infection, cancer treatment, and accidentscan cause spinal cord injuries (SCIs). The transplantation ofhESCs to paraplegic or quadriplegic SCI patients improvesbody control, balance, sensation, and limbal movements [15],where transplanted stem cells do homing to injury sites. Bybirth, humans have fixed numbers of cone cells; degenerationof retinal pigment epithelium (RPE) of macula in centralretina causes age-relatedmacular degeneration (ARMD).Thegenomic incorporation of COCO gene (expressed duringembryogenesis) in the developing embryo leads lineagecommitment of ESCs into cone cells, through suppression of
TGF𝛽, BMP, and Wnt signalling pathways. Transplantationof these cone cells to eye recovers individual from ARMDphenomenon, where transplanted cone cells migrate andform sheet-like structure in host retina [16]. However, estab-lishment of missing neuronal connection of retinal ganglioncells (RGCs), cones, andPRE is themost challenging aspect ofARMD therapeutics. Recently, Donald Z Jacks group at JohnHopkins University School of Medicine has generated RGCsfrom CRISPER-Cas9-m-Cherry reporter ESCs [17]. DuringESCs transdifferentiation process, CRIPER-Cas9 directs theknock-in of m-Cherry reporter into 3UTR of BRN3B gene,which is specifically expressed in RGCs and can be usedfor purification of generated RGCs from other cells [17].Furthermore, incorporation of forskolin in transdifferenti-ation regime boosts generation of RGCs. Coaxing of theseRGCs into biomaterial scaffolds directs axonal differenti-ation of RGCs. Further modification in RGCs generationregime and composition of biomaterial scaffoldsmight enablerestoration of vision for ARMD and glaucoma patients [17].
International Journal of Cell Biology 7
TSPSCs in regenerative medicine
TSPSCs in regenerative medicine
Ther
apeu
ticap
plic
atio
ns
Mesoangioblasts3D culture andtransplantation to mice tibialis
Tibialis anterior muscles
Treatment of myopathies
Fallopian tube organoid
RSPO1 mediumWnt3A medium3D Matrigel
Epithelial stem cells
Regeneration offallopian tube
Inner ear stem cellsLY411575
Auditory hair cells
Restoration ofacoustic function
SSCs
skin/prostate/ intestine
Epithelium
Skin
Prostate
Intestine
Stem cells factors basedtransdifferentiation
Limbal stem cells
Transplantationin mice eye
Corneal occupancy
Restoration of vision
Pancreatic organoid
Pancreaticprogenitors
3Dculture
Insulin therapy
Intestinal progenitor
Intestinal tissue
Regeneration ofintestinal tissue
3D culture
Ther
apeu
ticap
plic
atio
ns
DPSCsNeuronalculture
Neurogenesis
Serotonin neurons
AdSCs
Regeneration ofcardiac tissue
Treatment of ischemicheart disease
Infusion toMI heart
SKPs
VSMCs
WH and vasculatureregenerative therapy
containing 𝛽-cells
+Myofibroblasts+M𝜙/bacteria
+Mesenchyma of
Figure 3: TSPSCs in regenerative medicine: tissue specific stem and progenitor cells have potential to differentiate into other cells of thetissue. Characteristically inner ear stem cells can be transformed into auditory hair cells, skin progenitors into vascular smooth musclecells, mesoangioblasts into tibialis anterior muscles, and dental pulp stem cells into serotonin cells. The 3D-culture of TSPSCs in complexbiomaterial gives rise to tissue organoids, such as pancreatic organoid from pancreatic progenitor, intestinal tissue organoids from intestinalprogenitor cells, and fallopian tube organoids from fallopian tube epithelial cells. Transplantation of TSPSCs regenerates targets tissue such asregeneration of tibialis muscles frommesoangioblasts, cardiac tissue from AdSCs, and corneal tissue from limbal stem cells. Cell growth andtransformation factors secreted by TSPSCs can change cells fate to become other types of cell, such that SSCs coculture with skin, prostate,and intestine mesenchyme transforms these cells fromMSCs into epithelial cells fate.
Globally, especially in India, cardiovascular problems area more common cause of human death, where biomedicaltherapeutics require immediate restoration of heart functionsfor the very survival of the patient. Regeneration of cardiactissue can be achieved by transplantation of cardiomyocytes,ESCs-derived cardiovascular progenitors, and bone marrowderivedmononuclear cells (BMDMNCs); however healing bycardiomyocytes and progenitor cells is superior to BMDM-NCs but mature cardiomyocytes have higher tissue healingpotential, suppress heart arrhythmias, couple electromag-netically into hearts functions, and provide mechanical andelectrical repair without any associated tumorigenic effects
[18, 19]. Like CMdifferentiation, ESCs derived liver stem cellscan be transformed into Cytp450-hepatocytes, mediatingchemical modification and catabolism of toxic xenobioticdrugs [20]. Even today, availability and variability of func-tional hepatocytes are a major a challenge for testing drugtoxicity [20]. Stimulation of ESCs and ex vivo VitK12 andlithocholic acid (a by-product of intestinal flora regulatingdrugmetabolism during infancy) activates pregnaneX recep-tor (PXR), CYP3A4, and CYP2C9, which leads to differ-entiation of ESCs into hepatocytes; those are functionallysimilar to primary hepatocytes, for their ability to producealbumin and apolipoprotein B100 [20]. These hepatocytes
8 International Journal of Cell Biology
MSCs/stromal cells in regenerative medicine
Muscle degenerativedisease treatment
MSCs
DPCS-LBL-GAG
DPCs-EPCsco transplantation
Hair reconstitution
Treatment ofacute liver failure
cirrhosis andregeneration
of bladder tissue
Regenerationof cartilage
Regeneration ofbone tissue
Ligamentregeneration
Heart scar repairafter attack
Transplantationto liver
Healing oforthopedic injuries
Transplantation and trans-differentiation to orthopedic tissues
Muscle regeneration
coculture
leishmanial therapy CD73+,CD90+,CD105+CD34−,CD45−,CD11b−CD14−,CD19−,CD79a−
coating + FGF2
Educated M𝜙 for
AD-MSCs +M𝜙
Figure 4: MSCs in regenerative medicine: mesenchymal stem cells are CD73+, CD90+, CD105+, CD34−, CD45−, CD11b−, CD14−, CD19−, andCD79a− cells, also known as stromal cells.These bodily MSCs represented here do not account for MSCs of bone marrow and umbilical cord.Upon transplantation and transdifferentiation these bodilyMSCs regenerate into cartilage, bones, andmuscles tissue. Heart scar formed afterheart attack and liver cirrhosis can be treated from MSCs. ECM coating provides the niche environment for MSCs to regenerate into hairfollicle, stimulating hair growth.
are excellent source for the endpoint screening of drugs foraccurate prediction of clinical outcomes [20]. Generation ofhepatic cells from ESCs can be achieved in multiple ways,as serum-free differentiation [21], chemical approaches [20,22], and genetic transformation [23, 24].These ESCs-derivedhepatocytes are long lasting source for treatment of liverinjuries and high throughput screening of drugs [20, 23, 24].Transplantation of the inert biomaterial encapsulated hESCs-derived pancreatic progenitors (CD24+, CD49+, andCD133+)differentiates into 𝛽-cells, minimizing high fat diet inducedglycemic and obesity effects inmice [25] (Table 1). Addition ofantidiabetic drugs into transdifferentiation regime can boostESCs conservation into 𝛽-cells [25], which theoretically cancure T2DM permanently [25]. ESCs can be differentiateddirectly into insulin secreting 𝛽-cells (marked with GLUT2,INS1, GCK, and PDX1) which can be achieved throughPDX1 mediated epigenetic reprogramming [26]. Globally,osteoarthritis affects millions of people and occurs whencartilage at joints wears away, causing stiffness of the joints.The available therapeutics for arthritis relieve symptoms butdo not initiate reverse generation of cartilage. For young
individuals and athletes replacement of joints is not feasiblelike old populations; in that case transplantation of stem cellsrepresents an alternative for healing cartilage injuries [27].Chondrocytes, the cartilage forming cells derived fromhESC,embedded in fibrin gel effectively heal defective cartilagewithin 12 weeks, when transplanted to focal cartilage defectsof knee joints in mice without any negative effect [27].Transplanted chondrocytes form cell aggregates, positive forSOX9 and collagen II, and defined chondrocytes are active formore than 12wks at transplantation site, advocating clinicalsuitability of chondrocytes for treatment of cartilage lesions[27]. The integrity of ESCs to integrate and differentiateinto electrophysiologically active cells provides a means fornatural regulation of heart rhythm as biological pacemaker.Coaxing of ESCs into inert biomaterial as well as propagationin defined culture conditions leads to transdifferentiationof ESCs to become sinoatrial node (SAN) pacemaker cells(PCs) [28]. Genomic incorporation TBox3 into ESCs exvivo leads to generation of PCs-like cells; those expressactivated leukocyte cells adhesion molecules (ALCAM) andexhibit similarity to PCs for gene expression and immune
International Journal of Cell Biology 9
Cord cellsbanking
Umbilical arteries
Wharton’s Jelly
Amnion Umbilical cord bloodUmbilical vein
UCSCs in regenerative medicine
Ex vivo expansion of UCSCs
Intravenous delivery
Pancreatictransplantation
Treatment ofdiabetes
Treatment ofsystematic lupus
erythematosusMSCHSCs ProgenitorsUCSCs
Infusion of UCSCs
Treatment ofKrabbe’s disease
Ex vivo neurogenicorganoid culture
Application inneurodegenerative
disease
Treatment ofneuroblastoma
Treatment ofspinal myelitis
injection to pig knee
Regeneration oftendons
Injection of UCB-MSCs to rotor cuff
tendon tear-site
Regeneration of hyalinecartilage of knee
Treatment ofsevere congenital
neutropenia
Treatment ofHodgkin’slymphoma
Intraperitonealtransplantation
Treatment of peritonealfibrosis occurred long
term dialysis
2x tra
nsplan
tation
UCB-MSCs + HA
Figure 5: UCSCs in regenerative medicine: umbilical cord, the readily available source of stem cells, has emerged as futuristic source forpersonalized stem cell therapy. Transplantation of UCSCs to Krabbe’s disease patients regenerates myelin tissue and recovers neuroblastomapatients through restoring tissue homeostasis. The UCSCs organoids are readily available tissue source for treatment of neurodegenerativedisease. Peritoneal fibrosis caused by long term dialysis, tendon tissue degeneration, and defective hyaline cartilage can be regenerated byUCSCs. Intravenous injection of UCSCs enables treatment of diabetes, spinal myelitis, systemic lupus erythematosus, Hodgkin’s lymphoma,and congenital neuropathies. Cord blood stem cells banking avails long lasting source of stem cells for personalized therapy and regenerativemedicine.
functions [28]. Transplantation of PCs can restore pacemakerfunctions of the ailing heart [28]. In summary, ESCs canbe transdifferentiated into any kinds of cells representingthree germ layers of the body, being most promising sourceof regenerative medicine for tissue regeneration and diseasetherapy (Table 1). Ethical concerns limit the applications ofESCs, where set guidelines need to be followed; in that caseTSPSCs, MSCs, UCSCs, BMSCs, and iPSCs can be exploredas alternatives.
3. TSPSCs in Regenerative Medicine
TSPSCs maintain tissue homeostasis through continuouscell division, but, unlike ESCs, TSPSCs retain stem cellsplasticity and differentiation in tissue specific manner, givingrise to few types of cells (Table 1). The number of TSPSCs
population to total cells population is too low; in thatcase their harvesting as well as in vitro manipulation isreally a tricky task [29], to explore them for therapeuticscale. Human body has foundation from various types ofTSPSCs; discussing the therapeutic application for all typesis not feasible. This section of review discusses therapeuticapplication of pancreatic progenitor cells (PPCs), dental pulpstem cells (DPSCs), inner ear stem cells (IESCs), intestinalprogenitor cells (IPCs), limbal progenitor stem cells (LPSCs),epithelial progenitor stem cells (EPSCs), mesoangioblasts(MABs), spermatogonial stem cells (SSCs), the skin derivedprecursors (SKPs), and adipose derived stem cells (AdSCs)(Figure 3; Table 1). During embryogenesis PPCs give riseto insulin-producing 𝛽-cells. The differentiation of PPCsto become 𝛽-cells is negatively regulated by insulin [30].PPCs require active FGF and Notch signalling; growingmore rapidly in community than in single cell populations
10 International Journal of Cell Biology
BMSCs in regenerative medicine
BM-MSCCell perfusion anddecellularization
Diaphragm scaffold
BM-SSCBM-HSCBM-MSCBM-PSC
Application of BMSCs
Appl
icat
ions
Redmarrow
Separation oflymphoid andmyeloid cells
Allogenic transfusion
(i) Stromal stem cells (ii) Hematopoietic stem cells
(iii) Mesenchymal stem cells(iv) Progenitor stem cells
HIV1 resistant
BMSCs BMSCs
Brain tissue
injuries treatment
Megakaryocytes
Monocytes
wound healing
(CD14 and 90+) BMSCs
Craniofacial tissue
Periodonticbone formation
BMSCs
Intravenoustransplantationin diabetic mice Restoration of erectile
function in mice
BMSCs Transplantationto liver of liver
cirrhosis patients Regeneration of liverstissue and restoration
of liver functions
(CD4+) HSC and PSC
CD4+ cells
+3D culture +Epithelium+Spongy silk
+Transplantation +3D culture
+LA+HIV1 antisense
∙ Blood clotting and∙ Traumatic rain∙ HIV1 inhibition∙ Cancer treatment∙ CDD treatment
Figure 6: BMSCs in regenerative medicine: bone marrow, the soft sponge bone tissue that consisted of stromal, hematopoietic, andmesenchymal and progenitor stem cells, is responsible for blood formation. Even halo-HLA matched BMSCs can cure from disease andregenerate tissue. BMSCs can regenerate craniofacial tissue, brain tissue, diaphragm tissue, and liver tissue and restore erectile function andtransdifferentiation monocytes. These multipotent stem cells can cure host from cancer and infection of HIV and HCV.
advocates the functional importance of niche effect in self-renewal and transdifferentiation processes. In 3D-scaffoldculture system, mice embryo derived PPCs grow into holloworganoid spheres; those finally differentiate into insulin-producing 𝛽-cell clusters [29]. The DSPSCs, responsible formaintenance of teeth health status, can be sourced fromapicalpapilla, deciduous teeth, dental follicle, and periodontalligaments, have emerged as regenerative medicine candidate,and might be explored for treatment of various kinds ofdisease including restoration neurogenic functions in teeth[31, 32]. Expansion ofDSPSCs in chemically defined neuronalculture medium transforms them into a mixed populationof cholinergic, GABAergic, and glutaminergic neurons; thoseare known to respond towards acetylcholine, GABA, andglutamine stimulations in vivo. These transformed neuronalcells express nestin, glial fibrillary acidic protein (GFAP),𝛽III-tubulin, and voltage gated L-type Ca2+ channels [32].However, absence of Na+ and K+ channels does not sup-port spontaneous action potential generation, necessary forresponse generation against environmental stimulus. All
together, these primordial neuronal stem cells have pos-sible therapeutic potential for treatment of neurodentalproblems [32]. Sometimes, brain tumor chemotherapy cancause neurodegeneration mediated cognitive impairment, acondition known as chemobrain [33]. The intrahippocampaltransplantation of human derived neuronal stem cells tocyclophosphamide behavioural decremented mice restorescognitive functions in a month time. Here the transplantedstem cells differentiate into neuronal and astroglial lineage,reduce neuroinflammation, and restore microglial functions[33]. Furthermore, transplantation of stem cells, followed bychemotherapy, directs pyramidal and granule-cell neuronsof the gyrus and CA1 subfields of hippocampus which leadsto reduction in spine and dendritic cell density in thebrain. These findings suggest that transplantation of stemcells to cranium restores cognitive functions of the chemo-brain [33]. The hair cells of the auditory system producedduring development are not postmitotic; loss of hair cellscannot be replaced by inner ear stem cells, due to activestate of the Notch signalling [34]. Stimulation of inner ear
International Journal of Cell Biology 11
iPSCs in regenerative medicine
iPSCs
Brain organoidLung organoid Cortical spheroids
Trophoblastic cells
Kidney organoid
Photoreceptor cells
Healthy/patient
iPSC factorsSkin cells
Heart valve cells
Skin cells
Immune cells Melanocytes
Serotonin neuronChimera Pacemaker cells
Treatmentof lungdefects
Regenerationof kidney
tissue
Healing ofbrain
defects
Chimerictransplantation
Brain cortexregeneration
Pacemakerimpairment
recovery
Psychodisordertherapeutics
Generationof placental
tissue
Regenerationof heart valve
Restorationof vision
Treatment of bloodand immune
disorders
Treatment ofskin defects
Appl
icat
ions
Appl
icat
ions
Regenerationof pancreas
+
𝛽-cells
Figure 7: iPSCs in regenerative medicine: using the edge of iPSCs technology, skin fibroblasts and other adult tissues derived, terminallydifferentiated cells can be transformed into ESCs-like cells. It is possible that adult cells can be transformed into cells of distinct lineagesbypassing the phase of pluripotency. The tissue specific defined culture can transform skin cells to become trophoblast, heart valve cells,photoreceptor cells, immune cells, melanocytes, and so forth. ECM complexation with iPSCs enables generation of tissue organoids for lung,kidney, brain, and other organs of the body. Similar to ESCs, iPSCs also can be transformed into cells representing three germ layers such aspacemaker cells and serotonin cells.
progenitors with Υ-secretase inhibitor (LY411575) abrogatesNotch signalling through activation of transcription factoratonal homologue 1 (Atoh1) and directs transdifferentiationof progenitors into cochlear hair cells [34]. Transplantationof in vitro generated hair cells restores acoustic functionsin mice, which can be the potential regenerative medicinecandidates for the treatment of deafness [34]. Generation ofthe hair cells also can be achieved through overexpression of𝛽-catenin and Atoh1 in Lrg5+ cells in vivo [35]. Similar to earprogenitors, intestine of the digestive tract also has its owntissue specific progenitor stem cells, mediating regenerationof the intestinal tissue [34, 36]. Dysregulation of the commonstem cells signalling pathways, Notch/BMP/TGF-𝛽/Wnt, inthe intestinal tissue leads to disease. Information on thesesignalling pathways [37] is critically important in designingtherapeutics. Coaxing of the intestinal tissue specific progeni-tors with immune cells (macrophages), connective tissue cells(myofibroblasts), and probiotic bacteria into 3D-scaffolds ofinert biomaterial, crafting biological environment, is suitablefor differentiation of progenitors to occupy the crypt-villistructures into these scaffolds [36]. Omental implementationof these crypt-villi structures to dogs enhances intestinalmucosa through regeneration of goblet cells containing
intestinal tissue [36]. These intestinal scaffolds are closeapproach for generation of implantable intestinal tissue,divested by infection, trauma, cancer, necrotizing enterocol-itis (NEC), and so forth [36]. In vitro culture conditionscause differentiation of intestinal stem cells to become othertypes of cells, whereas incorporation of valproic acid andCHIR-99021 in culture conditions avoids differentiation ofintestinal stem cells, enabling generation of indefinite poolof stem cells to be used for regenerative applications [38].The limbal stem cells of the basal limbal epithelium, markedwith ABCB5, are essential for regeneration and maintenanceof corneal tissue [39]. Functional status of ABCB5 is criticalfor survival and functional integrity of limbal stem cells,protecting them from apoptotic cell death [39]. Limbal stemcells deficiency leads to replacement of corneal epitheliumwith visually dead conjunctival tissue, which can be con-tributed by burns, inflammation, and genetic factors [40].Transplanted human cornea stem cells to mice regrown intofully functional human cornea, possibly supported by bloodeye barrier phenomena, can be used for treatment of eyediseases, where regeneration of corneal tissue is criticallyrequired for vision restoration [39]. Muscle degenerativedisease like duchenne muscular dystrophy (DMD) can cause
12 International Journal of Cell Biology
Stem cells in wildlife conservation
Dead or livewild animals
Skin biopsies
Other internalorgan biopsies
iPSCs
Immaturegonadsbiopsies
In vitromaturation
In vivo maturation
Tissue specificstem cells
Cryopreservationtransdifferentiation
Cryopreservationin vitro fertilization
Cryopreservationtransdifferentiation
Resurrection of wildlife
Figure 8: Stem cells in wildlife conservation: tissue biopsies obtained from dead and live wild animals can be either cryopreserved ortransdifferentiated to other types of cells, through culture in defined culture medium or in vivo maturation. Stem cells and adult tissuederived iPSCs have great potential of regenerative medicine and disease therapeutics. Gonadal tissue procured from dead wild animals canbe matured, ex vivo and in vivo for generation of sperm and egg, which can be used for assistive reproductive technology oriented captivebreeding of wild animals or even for resurrection of wildlife.
extensive thrashing ofmuscle tissue, where tissue engineeringtechnology can be deployed for functional restoration oftissue through regeneration [41]. Encapsulation of mouseor human derived MABs (engineered to express placentalderived growth factor (PDGF)) into polyethylene glycol(PEG) fibrinogen hydrogel and their transplantation beneaththe skin at ablated tibialis anterior form artificial muscles,which are functionally similar to those of normal tibialisanterior muscles [41]. The PDGF attracts various cell typesof vasculogenic and neurogenic potential to the site oftransplantation, supporting transdifferentiation of mesoan-gioblasts to become muscle fibrils [41]. The therapeuticapplication of MABs in skeletal muscle regeneration andother therapeutic outcomes has been reviewed by others [42].One of the most important tissue specific stem cells, themale germline stem cells or spermatogonial stem cells (SSCs),produces spermatogenic lineage through mesenchymal andepithets cells [43] which itself creates niche effect on othercells. In vivo transplantation of SSCs with prostate, skin,and uterine mesenchyme leads to differentiation of these
cells to become epithelia of the tissue of origin [43]. Thesenewly formed tissues exhibit all physical and physiologicalcharacteristics of prostate and skin and the physical charac-teristics of prostate, skin, and uterus, express tissue specificmarkers, and suggest that factors secreted from SSCs leadto lineage conservation which defines the importance ofniche effect in regenerative medicine [43]. According to anestimate, more than 100 million people are suffering from thecondition of diabetic retinopathy, a progressive dropout ofvascularisation in retina that leads to loss of vision [44]. Theintravitreal injection of adipose derived stem cells (AdSCs)to the eye restores microvascular capillary bed in mice.The AdSCs from healthy donor produce higher amounts ofvasoprotective factors compared to glycemic mice, enablingsuperior vascularisation [44]. However use of AdSCs fordisease therapeutics needs further standardization for cellcounts in dose of transplant and monitoring of therapeuticoutcomes at population scale [44]. Apart from AdSCs, otherkinds of stem cells also have therapeutic potential in regen-erative medicine for treatment of eye defects, which has been
International Journal of Cell Biology 13
reviewed by others [45]. Fallopian tubes, connecting ovariesto uterus, are the sites where fertilization of the egg takesplace. Infection in fallopian tubes can lead to inflammation,tissue scarring, and closure of the fallopian tube which oftenleads to infertility and ectopic pregnancies. Fallopian is alsothe site where onset of ovarian cancer takes place.The studieson origin and etiology of ovarian cancer are restricted dueto lack of technical advancement for culture of epithelialcells. The in vitro 3D organoid culture of clinically obtainedfallopian tube epithelial cells retains their tissue specificity,keeps cells alive, which differentiate into typical ciliated andsecretory cells of fallopian tube, and advocates that ectopicexamination of fallopian tube in organoid culture settingsmight be the ideal approach for screening of cancer [46].Thesustained growth and differentiation of fallopian TSPSCs intofallopian tube organoid depend both on the active state ofthe Wnt and on paracrine Notch signalling [46]. Similar tofallopian tube stem cells, subcutaneous visceral tissue specificcardiac adipose (CA) derived stem cells (AdSCs) have thepotential of differentiation into cardiovascular tissue [47].Systemic infusion of CA-AdSCs into ischemic myocardiumof mice regenerates heart tissue and improves cardiac func-tion through differentiation to endothelial cells, vascularsmooth cells, and cardiomyocytes and vascular smooth cells.The differentiation and heart regeneration potential of CA-AdSCs are higher than AdSCs [48], representing CA-AdSCsas potent regenerative medicine candidates for myocardialischemic therapy [47]. The skin derived precursors (SKPs),the progenitors of dermal papilla/hair/hair sheath, give riseto multiple tissues of mesodermal and/or ectodermal originsuch as neurons, Schwann cells, adipocytes, chondrocytes,and vascular smooth muscle cells (VSMCs). VSMCs mediatewound healing and angiogenesis process can be derivedfrom human foreskin progenitor SKPs, suggesting that SKPsderived VSMCs are potential regenerative medicine candi-dates for wound healing and vasculature injuries treatments[49]. In summary, TSPSCs are potentiated with tissue regen-eration, where advancement in organoid culture (Figure 3;Table 1) technologies defines the importance of niche effectin tissue regeneration and therapeutic outcomes of ex vivoexpanded stem cells.
4. MSCs/Stromal Cells inRegenerative Medicine
MSCs, the multilineage stem cells, differentiate only totissue of mesodermal origin, which includes tendons, bone,cartilage, ligaments, muscles, and neurons [50]. MSCs arethe cells which express combination of markers: CD73+,CD90+, CD105+, CD11b−, CD14−, CD19−, CD34−, CD45−,CD79a−, and HLA-DR, reviewed elsewhere [50]. The appli-cation of MSCs in regenerative medicine can be generalizedfrom ongoing clinical trials, phasing through different stateof completions, reviewed elsewhere [90]. This section ofreview outlines the most recent representative applications ofMSCs (Figure 4; Table 1). The anatomical and physiologicalcharacteristics of both donor and receiver have equal impacton therapeutic outcomes. The bone marrow derived MSCs
(BMDMSCs) from baboon are morphologically and pheno-typically similar to those of bladder stem cells and can be usedin regeneration of bladder tissue. The BMDMSCs (CD105+,CD73+, CD34−, and CD45−), expressing GFP reporter,coaxed with small intestinal submucosa (SIS) scaffolds, aug-ment healing of degenerated bladder tissue within 10wks ofthe transplantation [51].The combinatorial CD characterizedMACs are functionally active at transplantation site, whichsuggests that CD characterization of donorMSCs yields supe-rior regenerative outcomes [51]. MSCs also have potentialto regenerate liver tissue and treat liver cirrhosis, reviewedelsewhere [91]. The regenerative medicinal application ofMSCs utilizes cells in two formats as direct transplantationor first transdifferentiation and then transplantation; exvivo transdifferentiation of MSCs deploys retroviral deliverysystem that can cause oncogenic effect on cells. Nonviral,NanoScript technology, comprising utility of transcriptionfactors (TFs) functionalized gold nanoparticles, can targetspecific regulatory site in the genome effectively and directdifferentiation of MSCs into another cell fate, dependingon regime of TFs. For example, myogenic regulatory factorcontaining NanoScript-MRF differentiates the adipose tissuederived MSCs into muscle cells [92]. The multipotency char-acteristics representMSCs as promising candidate for obtain-ing stable tissue constructs through coaxed 3D organoidculture; however heterogeneous distribution of MSCs slowsdown cell proliferation, rendering therapeutic applicationsof MSCs. Adopting two-step culture system for MSCs canyield homogeneous distribution of MSCs in biomaterialscaffolds. For example, fetal-MSCs coaxed in biomaterialwhen cultured first in rotating bioreactor followed with staticculture lead to homogeneous distribution of MSCs in ECMcomponents [7]. Occurrence of dental carries, periodontaldisease, and tooth injury can impact individual’s health,where bioengineering of teeth can be the alternative option.Coaxing of epithelial-MSCs with dental stem cells into syn-thetic polymer gives rise tomature teeth unit, which consistedof mature teeth and oral tissue, offering multiple regenerativetherapeutics, reviewed elsewhere [52]. Like the tooth decay,both human and animals are prone to orthopedic injuries,affecting bones, joint, tendon,muscles, cartilage, and so forth.Althoughnatural healing potential of bone is sufficient to healthe common injuries, severe trauma and tumor-recessioncan abrogate germinal potential of bone-forming stem cells.In vitro chondrogenic, osteogenic, and adipogenic potentialof MSCs advocates therapeutic applications of MSCs inorthopedic injuries [53]. Seeding of MSCs, coaxed intobiomaterial scaffolds, at defective bone tissue, regeneratesdefective bone tissues, within fourwks of transplantation; bythe end of 32wks newly formed tissues integrate into old bone[54]. Osteoblasts, the bone-forming cells, have lesser actincytoskeleton compared to adipocytes and MSCs. Treatmentof MSCs with cytochalasin-D causes rapid transportationof G-actin, leading to osteogenic transformation of MSCs.Furthermore, injection of cytochalasin-D to mice tibia alsopromotes bone formation within a wk time frame [55].The bone formation processes in mice, dog, and humanare fundamentally similar, so outcomes of research on miceand dogs can be directional for regenerative application to
14 International Journal of Cell Biology
human. Injection of MSCs to femur head of Legg-Calve-Perthes suffering dog heals the bone very fast and reduces theinjury associated pain [55]. Degeneration of skeletal muscleandmuscle cramps are very common to sledge dogs, animals,and individuals involved in adventurous athletics activities.Direct injection of adipose tissue derived MSCs to tear-siteof semitendinosus muscle in dogs heals injuries much fasterthan traditional therapies [56]. Damage effect treatmentfor heart muscle regeneration is much more complex thanregeneration of skeletal muscles, which needs high gradefine-tuned coordination of neurons withmuscles. Coaxing ofMSCs into alginate gel increases cell retention time that leadsto releasing of tissue repairing factors in controlled man-ner. Transplantation of alginate encapsulated cells to miceheart reduces scar size and increases vascularisation, whichleads to restoration of heart functions. Furthermore, trans-planted MSCs face host inhospitable inflammatory immuneresponses and other mechanical forces at transplantationsite, where encapsulation of cells keeps them away from allsorts of mechanical forces and enables sensing of host tissuemicroenvironment, and respond accordingly [57]. Ageing,disease, and medicine consumption can cause hair loss,known as alopecia. Although alopecia has no life threateningeffects, emotional catchments can lead to psychological dis-turbance. The available treatments for alopecia include hairtransplantation and use of drugs, where drugs are expensiveto afford and generation of new hair follicle is challenging.Dermal papillary cells (DPCs), the specialized MSCs local-ized in hair follicle, are responsible for morphogenesis ofhair follicle and hair cycling. The layer-by-layer coating ofDPCs, called GAG coating, consists of coating of geletinas outer layer, middle layer of fibroblast growth factor 2(FGF2) loaded alginate, and innermost layer of geletin. GAGcoating creates tissue microenvironment for DPCs that cansustain immunological andmechanical obstacles, supportinggeneration of hair follicle. Transplantation of GAG-coatedDPCs leads to abundant hair growth and maturation ofhair follicle, where GAG coating serves as ECM, enhanc-ing intrinsic therapeutic potential of DPCs [58]. Duringinfection, the inflammatory cytokines secreted from hostimmune cells attractMSCs to the site of inflammation, whichmodulates inflammatory responses, representing MSCs askey candidate of regenerative medicine for infectious diseasetherapeutics. Coculture of macrophages (M𝜙) and adiposederived MSCs from Leishmania major (LM) susceptible andresistant mice demonstrates that AD-MSCs educate M𝜙against LM infection, differentially inducing M1 and M2phenotype that represents AD-MSC as therapeutic agentfor leishmanial therapy [93]. In summary, the multilineagedifferentiation potential of MSCs, as well as adoption of next-generation organoid culture system, avails MSCs as idealregenerative medicine candidate.
5. UCSCs in Regenerative Medicine
Umbilical cord, generally thrown at the time of child birth,is the best known source for stem cells, procured in nonin-vasive manner, having lesser ethical constraints than ESCs.
Umbilical cord is rich source of hematopoietic stem cells(HSCs) and MSCs, which possess enormous regenerationpotential [94] (Figure 5; Table 1). The HSCs of cord bloodare responsible for constant renewal of all types of blood cellsand protective immune cells. The proliferation of HSCs isregulated by Musashi-2 protein mediated attenuation of Arylhydrocarbon receptor (AHR) signalling in stem cells [95].UCSCs can be cryopreserved at stem cells banks (Figure 5;Table 1), in operation by both private and public sectororganization. Public stem cells banks operate on donationformats and perform rigorous screening for HLA typingand donated UCSCs remain available to anyone in need,whereas private stem cell banks operation is more person-alized, availing cells according to donor consent. Stem cellbanking is not so common, even in developed countries.Survey studies find that educated women are more eagerto donate UCSCs, but willingness for donation decreaseswith subsequent deliveries, due to associated cost and safetyconcerns for preservation [96]. FDA has approved five HSCsfor treatment of blood and other immunological complica-tions [97]. The amniotic fluid, drawn during pregnancy forstandard diagnostic purposes, is generally discarded withoutconsidering its vasculogenic potential. UCSCs are the bestalternatives for those patients who lack donors with fullymatched HLA typing for peripheral blood and PBMCs andbone marrow [98]. One major issue with UCSCs is numberof cells in transplant, fewer cells in transplant require moretime for engraftment to mature, and there are also risks ofinfection and mortality; in that case ex vivo propagation ofUCSCs can meet the demand of desired outcomes. Thereare diverse protocols, available for ex vivo expansion ofUCSCs, reviewed elsewhere [99]. Amniotic fluid stem cells(AFSCs), coaxed to fibrin (required for blood clotting, ECMinteractions, wound healing, and angiogenesis) hydrogel andPEG supplemented with vascular endothelial growth factor(VEGF), give rise to vascularised tissue, when grafted tomice,suggesting that organoid cultures of UCSCs have promisefor generation of biocompatible tissue patches, for treatinginfants born with congenital heart defects [59]. Retroviralintegration of OCT4, KLF4, cMYC, and SOX2 transformsAFSCs into pluripotency stem cells known as AFiPSCswhich can be directed to differentiate into extraembryonictrophoblast by BMP2 and BMP4 stimulation, which can beused for regeneration of placental tissues [60]. Wharton’sjelly (WJ), the gelatinous substance inside umbilical cord,is rich in mucopolysaccharides, fibroblast, macrophages,and stem cells. The stem cells from UCB and WJ can betransdifferentiated into 𝛽-cells. Homogeneous nature of WJ-SCs enables better differentiation into 𝛽-cells; transplanta-tion of these cells to streptozotocin induced diabetic miceefficiently brings glucose level to normal [7]. Easy accessand expansion potential and plasticity to differentiate intomultiple cell lineages represent WJ as an ideal candidatefor regenerative medicine but cells viability changes withpassages with maximum viable population at 5th-6th pas-sages. So it is suggested to perform controlled expansionof WJ-MSCS for desired regenerative outcomes [9]. Studysuggests that CD34+ expression leads to the best regenerativeoutcomes, with less chance of host-versus-graft rejection. In
International Journal of Cell Biology 15
vitro expansion of UCSCs, in presence of StemRegenin-1 (SR-1), conditionally expands CD34+ cells [61]. In type I diabeticmellitus (T1DM), T-cell mediated autoimmune destructionof pancreatic 𝛽-cells occurs, which has been considered astough to treat. Transplantation of WJ-SCs to recent onset-T1DM patients restores pancreatic function, suggesting thatWJ-MSCs are effective in regeneration of pancreatic tissueanomalies [62]. WJ-MSCs also have therapeutic importancefor treatment of T2DM. A non-placebo controlled phase I/IIclinical trial demonstrates that intravenous and intrapancre-atic endovascular injection of WJ-MSCs to T2DM patientscontrols fasting glucose and glycated haemoglobin throughimprovement of 𝛽-cells functions, evidenced by enhanced c-peptides and reduced inflammatory cytokines (IL-1𝛽 and IL-6) and T-cells counts [63]. Like diabetes, systematic lupuserythematosus (SLE) also can be treated with WJ-MSCstransplantation. During progression of SLE host immunesystem targets its own tissue leading to degeneration ofrenal, cardiovascular, neuronal, and musculoskeletal tissues.A non-placebo controlled follow-up study on 40 SLE patientsdemonstrates that intravenous infusion ofWJ-MSC improvesrenal functions and decreases systematic lupus erythemato-sus disease activity index (SLEDAI) and British Isles LupusAssessment Group (BILAG), and repeated infusion of WJ-MSCs protects the patient from relapse of the disease [64].Sometimes, host inflammatory immune responses can bedetrimental for HSCs transplantation and blood transfu-sion procedures. Infusion of WJ-MSC to patients, whohad allogenic HSCs transplantation, reduces haemorrhageinflammation (HI) of bladder, suggesting that WJ-MSCs arepotential stem cells adjuvant in HSCs transplantation andblood transfusion based therapies [100]. Apart from WJ,umbilical cord perivascular space and cord vein are alsorich source for obtaining MSCs. The perivascular MSCsof umbilical cord are more primitive than WJ-MSCs andother MSCs from cord suggest that perivascular MSCsmight be used as alternatives for WJ-MSCs for regenerativetherapeutics outcome [101]. Based on origin, MSCs exhibitdifferential in vitro and in vivo properties and advocatefunctional characterization of MSCs, prior to regenerativeapplications. Emerging evidence suggests that UCSCs canheal brain injuries, caused by neurodegenerative diseaseslike Alzheimer’s, Krabbe’s disease, and so forth. Krabbe’sdisease, the infantile lysosomal storage disease, occurs dueto deficiency of myelin synthesizing enzyme (MSE), affectingbrain development and cognitive functions. Progression ofneurodegeneration finally leads to death of babies agedtwo. Investigation shows that healing of peripheral nervoussystem (PNS) and central nervous system (CNS) tissues withKrabbe’s disease can be achieved by allogenic UCSCs. UCSCstransplantation to asymptomatic infants with subsequentmonitoring for 4–6 years reveals that UCSCs recover babiesfrom MSE deficiency, improving myelination and cognitivefunctions, compared to those of symptomatic babies. Thesurvival rate of transplanted UCSCs in asymptomatic andsymptomatic infants was 100% and 43%, respectively, sug-gesting that early diagnosis and timely treatment are criticalfor UCSCs acceptance for desired therapeutic outcomes.UCSCs are more primitive than BMSCs, so perfect HLA
typing is not critically required, representing UCSCs as anexcellent source for treatment of all the diseases involvinglysosomal defects, like Krabbe’s disease, hurler syndrome,adrenoleukodystrophy (ALD), metachromatic leukodystro-phy (MLD), Tay-Sachs disease (TSD), and Sandhoff disease[65]. Brain injuries often lead to cavities formation, whichcan be treated from neuronal parenchyma, generated ex vivofrom UCSCs. Coaxing of UCSCs into human originatedbiodegradable matrix scaffold and in vitro expansion ofcells in defined culture conditions lead to formation ofneuronal organoids, within threewks’ time frame. Theseorganoids structurally resemble brain tissue and consistedof neuroblasts (GFAP+, Nestin+, and Ki67+) and immaturestem cells (OCT4+ and SOX2+). The neuroblasts of theseorganoids further can be differentiated into mature neurons(MAP2+ and TUJ1+) [66]. Administration of high doseof drugs in divesting neuroblastoma therapeutics requiresimmediate restoration of hematopoiesis. Although BMSCshad been promising in restoration of hematopoiesis UCSCsare sparely used in clinical settings. A case study demonstratesthat neuroblastoma patients who received autologous UCSCssurvive without any associated side effects [12]. Duringradiation therapy of neoplasm, spinal cordmyelitis can occur,although occurrence of myelitis is a rare event and usuallysuch neurodegenerative complication of spinal cord occurs6–24 years after exposure to radiations. Transplantation ofallogenic UC-MSCs in laryngeal patients undergoing radi-ation therapy restores myelination [102]. For treatment ofneurodegenerative disease like Alzheimer’s disease (AD),amyotrophic lateral sclerosis (ALS), traumatic brain injuries(TBI), Parkinson’s, SCI, stroke, and so forth, distributionof transplanted UCSCs is critical for therapeutic outcomes.In mice and rat, injection of UCSCs and subsequent MRIscanning show that transplanted UCSCs migrate to CNS andmultiple peripheral organs [67]. For immunomodulation oftumor cells disease recovery, transplantation of allogenicDCsis required. The CD11c+DCs, derived from UCB, are mor-phologically and phenotypically similar to those of peripheralblood derived CTLs-DCs, suggesting that UCB-DCs can beused for personalized medicine of cancer patient, in need forDCs transplantation [103]. Coculture of UCSCs with radia-tion exposed human lung fibroblast stops their transdifferen-tiation, which suggests that factors secreted fromUCSCsmayrestore niche identity of fibroblast, if they are transplantedto lung after radiation therapy [104]. Tearing of shouldercuff tendon can cause severe pain and functional disability,whereas ultrasound guided transplantation of UCB-MSCsin rabbit regenerates subscapularis tendon in fourwks’ timeframe, suggesting that UCB-MSCs are effective enough totreat tendons injuries when injected to focal points of tear-site[68]. Furthermore, transplantation of UCB-MSCs to chon-dral cartilage injuries site in pig knee along with HA hydrogelcomposite regenerates hyaline cartilage [69], suggesting thatUCB-MSCs are effective regenerative medicine candidatefor treating cartilage and ligament injuries. Physiologicallycirculatory systems of brain, placenta, and lungs are similar.Infusion of UCB-MSCs to preeclampsia (PE) induced hyper-tension mice reduces the endotoxic effect, suggesting thatUC-MSCs are potential source for treatment of endotoxin
16 International Journal of Cell Biology
induced hypertension during pregnancy, drug abuse, andother kinds of inflammatory shocks [105]. Transplantationof UCSCs to severe congenital neutropenia (SCN) patientsrestores neutrophils count from donor cells without anyside effect, representing UCSCs as potential alternative forSCN therapy, when HLA matched bone marrow donorsare not accessible [106]. In clinical settings, the success ofmyocardial infarction (MI) treatment depends on ageing,systemic inflammation in host, and processing of cells forinfusion. Infusion of human hyaluronan hydrogel coaxedUCSCs in pigs induces angiogenesis, decreases scar area,improves cardiac function at preclinical level, and suggeststhat the same strategy might be effective for human [107]. Instem cells therapeutics, UCSCs transplantation can be eitherautologous or allogenic. Sometimes, the autologous UCSCstransplants cannot combat over tumor relapse, observed inHodgkin’s lymphoma (HL), which might require seconddose transplantation of allogenic stem cells, but efficacy andtolerance of stem cells transplant need to be addressed,where tumor replace occurs. A case study demonstrates thatsecond dose allogenic transplants of UCSCs effective for HLpatients, who had heavy dose in prior transplant, increase thelong term survival chances by 30% [10]. Patients undergoinglong term peritoneal renal dialysis are prone to peritonealfibrosis and can change peritoneal structure and failure ofultrafiltration processes. The intraperitoneal (IP) injection ofWJ-MSCs prevents methylglyoxal induced programmed celldeath and peritoneal wall thickening and fibrosis, suggestingthat WJ-MSCs are effective in therapeutics of encapsulatingperitoneal fibrosis [70]. In summary, UCB-HSCs, WJ-MSCs,perivascular MSCs, and UCB-MSCs have tissue regenerationpotential.
6. BMSCs in Regenerative Medicine
Bone marrow found in soft spongy bones is responsible forformation of all peripheral blood and comprises hematopoi-etic stem cells (producing blood cells) and stromal cells(producing fat, cartilage, and bones) [108] (Figure 6; Table 1).Visually bone marrow has two types, red marrow (myeloidtissue; producing RBC, platelets, and most of WBC) andyellow marrow (producing fat cells and some WBC) [108].Imbalance in marrow composition can culminate to thediseased condition. Since 1980, bone marrow transplantationis widely accepted for cancer therapeutics [109]. In order toavoid graft rejection, HLA typing of donors is a must, butcompletely matched donors are limited to family members,which hampers allogenic transplantation applications. Sincematching of all HLA antigens is not critically required, in thatcase defining the critical antigens for haploidentical allogenicdonor for patients, who cannot find fully matched donor,might relieve from donor constraints. Two-step administra-tion of lymphoid and myeloid BMSCs from haploidenticaldonor to the patients of aplastic anaemia and haematologicalmalignancies reconstructs host immune system and theoutcomes are almost similar to fully matched transplants,which recommends that profiling of critically importantHLA
is sufficient for successful outcomes of BMSCs transplan-tation. Haploidentical HLA matching protocol is the majorprocess for minorities and others who do not have accessto matched donor [71]. Furthermore, antigen profiling isnot the sole concern for BMSCs based therapeutics. Forexample, restriction of HIV1 (human immune deficiencyvirus) infection is not feasible through BMSCs transplan-tation because HIV1 infection is mediated through CD4+receptors, chemokine CXC motif receptor 4 (CXCR4), andchemokine receptor 5 (CCR5) for infecting and propagatinginto T helper (Th), monocytes, macrophages, and dendriticcells (DCs). Genetic variation in CCR2 and CCR5 receptorsis also a contributory factor; mediating protection againstinfection has been reviewed elsewhere [110]. Engineering ofhematopoietic stem and progenitor cells (HSPCs) derivedCD4+ cells to express HIV1 antagonistic RNA, specificallydesigned for targeting HIV1 genome, can restrict HIV1infection, through immune elimination of latently infectedCD4+ cells. A single dose infusion of genetically modified(GM), HIV1 resistant HSPCs can be the alternative of HIV1retroviral therapy. In the present scenario stem cells source,patient selection, transplantation-conditioning regimen, andpostinfusion follow-up studies are the major factors, whichcan limit application of HIV1 resistant GM-HSPCs (CD4+)cells application in AIDS therapy [72, 73]. Platelets, essentialfor blood clotting, are formed from megakaryocytes insidethe bone marrow [74]. Due to infection, trauma, and cancer,there are chances of bone marrow failure. To an extent,spongy bone marrow microenvironment responsible forlineage commitment can be reconstructed ex vivo [75]. Theex vivo constructed 3D-scaffolds consisted of microtubuleand silk sponge, flooded with chemically defined organculture medium, which mimics bone marrow environment.The coculture of megakaryocytes and embryonic stem cells(ESCs) in this microenvironment leads to generation offunctional platelets from megakaryocytes [75]. The ex vivo3D-scaffolds of bone microenvironment can stride the pathfor generation of platelets in therapeutic quantities for regen-erativemedication of burns [75] and blood clotting associateddefects. Accidents, traumatic injuries, and brain stroke candeplete neuronal stem cells (NSCs), responsible for genera-tion of neurons, astrocytes, and oligodendrocytes. Brain doesnot repopulate NSCs and heal traumatic injuries itself andtransplantation of BMSCs also can heal neurodegenerationalone. Lipoic acid (LA), a known pharmacological antioxi-dant compound used in treatment of diabetic and multiplesclerosis neuropathy when combined with BMSCs, inducesneovascularisation at focal cerebral injuries, within 8wksof transplantation. Vascularisation further attracts microgliaand induces their colonization into scaffold, which leadsto differentiation of BMSCs to become brain tissue, within16wks of transplantation. In this approach, healing of tissuedirectly depends on number of BMSCs in transplantationdose [76]. Dental caries and periodontal disease are commoncraniofacial disease, often requiring jaw bone reconstructionafter removal of the teeth. Traditional therapy focuses onfunctional and structural restoration of oral tissue, bone,and teeth rather than biological restoration, but BMSCsbased therapies promise for regeneration of craniofacial bone
International Journal of Cell Biology 17
defects, enabling replacement of missing teeth in restoredbones with dental implants. Bone marrow derived CD14+and CD90+ stem and progenitor cells, termed as tissuerepair cells (TRC), accelerate alveolar bone regeneration andreconstruction of jaw bone when transplanted in damagedcraniofacial tissue, earlier to oral implants. Hence, TRCtherapy reduces the need of secondary bone grafts, bestsuited for severe defects in oral bone, skin, and gum,resulting from trauma, disease, or birth defects [77]. Overall,HSCs have great value in regenerative medicine, where stemcells transplantation strategies explore importance of nichein tissue regeneration. Prior to transplantation of BMSCs,clearance of original niche from target tissue is necessaryfor generation of organoid and organs without host-versus-graft rejection events. Some genetic defects can lead todisorganization of niche, leading to developmental errors.Complementation with human blastocyst derived primarycells can restore niche function of pancreas in pigs andrats, which defines the concept for generation of clinicalgrade human pancreas in mice and pigs [111]. Similar toother organs, diaphragm also has its own niche. Congenitaldefects in diaphragm can affect diaphragm functions. Inthe present scenario functional restoration of congenitaldiaphragm defects by surgical repair has risk of reoccurrenceof defects or incomplete restoration [8]. Decellularization ofdonor derived diaphragm offers a way for reconstruction ofnew and functionally compatible diaphragm through nichemodulation. Tissue engineering technology based decel-lularization of diaphragm and simultaneous perfusion ofbonemarrowmesenchymal stem cells (BM-MSCs) facilitatesregeneration of functional scaffolds of diaphragm tissues [8].In vivo replacement of hemidiaphragm in rats with reseededscaffolds possesses similar myography and spirometry as ithas in vivo in donor rats. These scaffolds retaining naturalarchitecture are devoid of immune cells, retaining intactextracellular matrix that supports adhesion, proliferation,and differentiation of seeded cells [8]. These findings suggestthat cadaver obtained diaphragm, seeded with BM-MSCs,can be used for curing patients in need for restoration ofdiaphragm functions (Figure 6; Table 1). However, BMSCs areheterogeneous population, which might result in differentialoutcomes in clinical settings; however clonal expansion ofBMSCs yields homogenous cells population for therapeuticapplication [8]. One study also finds that intracavernousdelivery of single clone BMSCs can restore erectile func-tion in diabetic mice [112] and the same strategy mightbe explored for adult human individuals. The infectionof hepatitis C virus (HCV) can cause liver cirrhosis anddegeneration of hepatic tissue. The intraparenchymal trans-plantation of bone marrow mononuclear cells (BMMNCs)into liver tissue decreases aspartate aminotransferase (AST),alanine transaminase (ALT), bilirubin, CD34, and 𝛼-SMA,suggesting that transplantedBMSCs restore hepatic functionsthrough regeneration of hepatic tissues [113]. In order tomeetthe growing demand for stem cells transplantation therapy,donor encouragement is always required [8]. The stem cellsdonation procedure is very simple; with consent donorgets an injection of granulocyte-colony stimulating factor(G-CSF) that increases BMSCs population. Bone marrow
collection is done from hip bone using syringe in 4-5 hrs,requiring local anaesthesia andwithin a wk time frame donorgets recovered donation associated weakness.
7. iPSCs in Regenerative Medicine
The field of iPSCs technology and research is new to allother stem cells research, emerging in 2006 when, for thefirst time, Takahashi and Yamanaka generated ESCs-likecells through genetic incorporation of four factors, Sox2,Oct3/4, Klf4, and c-Myc, into skin fibroblast [3]. Due toextensive nuclear reprogramming, generated iPSCs are indis-tinguishable from ESCs, for their transcriptome profiling,epigenetic markings, and functional competence [3], but useof retrovirus in transdifferentiation approach has questionediPSCs technology. Technological advancement has enabledgeneration of iPSCs from various kinds of adult cells phasingthrough ESCs or direct transdifferentiation. This section ofreview outlinesmost recent advancement in iPSC technologyand regenerative applications (Figure 7; Table 1). Using thenew edge of iPSCs technology, terminally differentiated skincells directly can be transformed into kidney organoids [114],which are functionally and structurally similar to those ofkidney tissue in vivo. Up to certain extent kidneys healthemselves; however natural regeneration potential cannotmeet healing for severe injuries. During kidneys healingprocess, a progenitor stem cell needs to become 20 typesof cells, required for waste excretion, pH regulation, andrestoration of water and electrolytic ions. The procedure forgeneration of kidney organoids ex vivo, containing functionalnephrons, has been identified for human. These ex vivokidney organoids are similar to fetal first-trimester kidneysfor their structure and physiology. Such kidney organoidscan serve as model for nephrotoxicity screening of drugs,disease modelling, and organ transplantation. However gen-eration of fully functional kidneys is a far seen event withtoday’s scientific technologies [114]. Loss of neurons inage-related macular degeneration (ARMD) is the commoncause of blindness. At preclinical level, transplantation ofiPSCs derived neuronal progenitor cells (NPCs) in rat limitsprogression of disease through generation of 5-6 layers ofphotoreceptor nuclei, restoring visual acuity [78].The variousapproaches of iPSCs mediated retinal regeneration includingARMD have been reviewed elsewhere [79]. Placenta, thecordial connection between mother and developing fetus,gets degenerated in certain pathophysiological conditions.Nuclear programming of OCT4 knock-out (KO) and wildtype (WT) mice fibroblast through transient expressionof GATA3, EOMES, TFAP2C, and +/− cMYC generatestransgene independent trophoblast stem-like cells (iTSCs),which are highly similar to blastocyst derived TSCs for DNAmethylation, H3K7ac, nucleosome deposition of H2A.X, andother epigenetic markings. Chimeric differentiation of iTSCsspecifically gives rise to haemorrhagic lineages and placentaltissue, bypassing pluripotency phase, opening an avenuefor generation of fully functional placenta for human [115].Neurodegenerative disease like Alzheimer’s and obstinateepilepsies can degenerate cerebrum, controlling excitatory
18 International Journal of Cell Biology
and inhibitory signals of the brain. The inhibitory tones incerebral cortex and hippocampus are accounted by 𝛾-aminobutyric acid secreting (GABAergic) interneurons (INs). Lossof these neurons often leads to progressive neurodegen-eration. Genomic integration of Ascl1, Dlx5, Foxg1, andLhx6 to mice and human fibroblast transforms these adultcells into GABAergic-INs (iGABA-INs). These cells havemolecular signature of telencephalic INs, release GABA,and show inhibition to host granule neuronal activity [81].Transplantation of these INs in developing embryo curesfrom genetic and acquired seizures, where transplanted cellsdisperse andmature into functional neuronal circuits as localINs [82]. Dorsomorphin and SB-431542 mediated inhibitionof TGF-𝛽 and BMP signalling direct transformation ofhuman iPSCs into cortical spheroids.These cortical spheroidsconsisted of both peripheral and cortical neurons, sur-rounded by astrocytes, displaying transcription profiling andelectrophysiology similarity with developing fetal brain andmature neurons, respectively [83]. The underlying complexbiology and lack of clear etiology and genetic reprogram-ming and difficulty in recapitulation of brain developmenthave barred understanding of pathophysiology of autismspectrum disorder (ASD) and schizophrenia. 3D organoidcultures of ASD patient derived iPSC generate miniaturebrain organoid, resembling fetal brain few months aftergestation. The idiopathic conditions of these organoids aresimilar with brain of ASD patients; both possess higherinhibitory GABAergic neurons with imbalanced neuronalconnection. Furthermore these organoids express forkheadBox G1 (FOXG1) much higher than normal brain tissue,which explains that FOXG1 might be the leading cause ofASD [84]. Degeneration of other organs and tissues alsohas been reported, like degeneration of lungs which mightoccur due to tuberculosis infection, fibrosis, and cancer. Theunderlying etiology for lung degeneration can be explainedthrough organoid culture. Coaxing of iPSC into inert bio-material and defined culture leads to formation of lungorganoids that consisted of epithelial and mesenchymal cells,which can survive in culture for months. These organoidsare miniature lung, resemble tissues of large airways andalveoli, and can be used for lung developmental studiesand screening of antituberculosis and anticancer drugs [87].The conventional multistep reprogramming for iPSCs con-sumes months of time, while CRISPER-Cas9 system basedepisomal reprogramming system that combines two stepstogether enables generation of ESCs-like cells in less thantwowks, reducing the chances of culture associated geneticabrasions and unwanted epigenetic [80]. This approach canyield single step ESCs-like cells in more personalized wayfrom adults with retinal degradation and infants with severeimmunodeficiency, involving correction for geneticmutationof OCT4 and DNMT3B [80]. The iPSCs expressing anti-CCR5-RNA, which can be differentiated into HIV1 resistantmacrophages, have applications in AIDS therapeutics [88].The diversified immunotherapeutic application of iPSCs hasbeen reviewed elsewhere [89]. The 𝛼-1 antitrypsin deficiency(A1AD) encoded by serpin peptidase inhibitor clade Amember 1 (SERPINA1) protein synthesized in liver pro-tects lungs from neutrophils elastase, the enzyme causing
disruption of lungs connective tissue. A1AD deficiency iscommon cause of both lung and liver disease like chronicobstructive pulmonary disease (COPD) and liver cirrhosis.Patient specific iPSCs from lung and liver cells might explainpathophysiology of A1AD deficiency. COPD patient derivediPSCs show sensitivity to toxic d