Embed Size (px)
Citation preview
Review Article
Perioperative Considerationsin Urgent Surgical Care ofSuspected and ConfirmedCOVID-19 OrthopaedicPatients: Operating RoomProtocols and Recommendationsin the Current COVID-19Pandemic
Abstract
By April 7, 2020, severe acute respiratory syndrome coronavirus 2was responsible for 1,383,436 confirmed cases of Coronavirusdisease 2019 (COVID-19), involving 209 countries around the world;378,881 cases have been confirmed in the United States. During thispandemic, the urgent surgical requirements will not stop. As anexample, the most recent Centers of Disease Control and Preventionreports estimate that there are 2.8million trauma patients hospitalizedin the United States. These data illustrate an increase in the likelihoodof encountering urgent surgical patients with either clinicallysuspected or confirmedCOVID-19 in the near future. Preparation for apandemic involves considering the different levels in the hierarchy ofcontrols and the different phases of the pandemic. Apart from the factthat this pandemic certainly involves many important health,economic, and community ramifications, it also requires severalinitiatives tomandate what measures aremost appropriate to preparefor mitigating the occupational risks. This article provides evidence-based recommendations and measures for the appropriate personalprotective equipment for different clinical and surgical activities invarious settings. To reduce the occupational risk in treating suspectedor confirmed COVID-19 urgent orthopaedic patients, recommendedprecautions and preventive actions (triage area, emergencydepartment consultation room, induction room, operating room, andrecovery room) are reviewed.
InOctober 2019, theDepartment ofHealth andHuman Services’—The
Office for Civil Rights took a cor-rective action against an orthopaedicsurgeon who unlawfully canceled anelective surgery for an HIV-positivepatient. This action was justified via
the requirements of Section 504 ofthe Rehabilitation Act of 1973 thatprohibits discrimination on the basisof disability (including HIV/AIDS) inhealth programs or activities thatreceive Health and Human Servicefunding.1 Over the past few decades,
Mohamed E. Awad, MD
Jacob C.L. Rumley, DO
Jose A. Vazquez, MD, FACP,FIDSA
John G. Devine, MD, FAOA
From the Hull College of Business,Augusta University (Dr. Awad), theDepartment of Orthopedic Surgery,Medical College of Georgia, AugustaUniversity (Dr. Awad, Dr. Rumley, andDr. Devine), the Division of InfectiousDiseases, Department of Medicine,Medical College of Georgia, AugustaUniversity (Dr. Vazquez), andAntimicrobial Stewardship Service,Augusta University (Dr. Vazquez),Augusta, GA.
None of the following authors or anyimmediate family member hasreceived anything of value from or hasstock or stock options held in acommercial company or institutionrelated directly or indirectly to thesubject of this article: Dr. Awad,Dr. Rumley, Dr. Vazquez, andDr. Devine.
J Am Acad Orthop Surg 2020;28:451-463
DOI: 10.5435/JAAOS-D-20-00227
Copyright 2020 by the AmericanAcademy of Orthopaedic Surgeons.
June 1, 2020, Vol 28, No 11 451
Copyright © the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited.
many guidelines and recommendationshave been established to reduce theoccupational risk while educating sur-geons to make them better prepared tooperate on HIV-positive patients.2 Thesevere acute respiratory syndrome co-ronavirus 2 (SARS-Cov-2) (Coronavi-rus disease 2019 [COVID-19]), whichseems to be highly contagious and haseasily spread worldwide, is a muchdifferent virus causing a much differentdisease. Orthopaedic surgeons shouldbe fully aware of the current situationregarding the COVID-19 pandemicand prepare to take proper precautionsagainst the occupational risk of expo-sure, especially in asymptomatic andmildly symptomatic surgical patients.ByApril 7, 2020, the SARS-CoV-2wasresponsible for 1,383,436 confirmedcases of COVID-19, involving 209countries around the world; 378,881cases have been confirmed in theUnited States. As an example, Centersof Disease Control and Prevention
(CDC) reports an estimated 2.8 milliontrauma patients hospitalized in theUnited States. In addition, 791,000older patients are treated in emergencydepartments for fall injuries each year.3
Gleaning from the trauma literature,these data suggest an increased likeli-hood of engaging in COVID-19 ortho-paedic patients in our hospitals.Thousands of healthcare providers(HCP) have been infected with COVID-19, despite their adherence to infectioncontrol measures.4 Approximately 14%of Spain’s confirmed cases are inmedicalprofessionals, per the Spanishminister ofhealth.Despite the current definitions fordiagnosing symptomatic COVID-19patients, the transmission from anasymptomatic carrier has been docu-mented between 25% and 50%.5
It is necessary for the orthopaediccommunity to be prepared for thisglobal pandemic emergency. This isan occupational hazard not only toorthopaedic surgeons and other health-
care providers but also to the familiesand neighbors of exposed healthcareproviders. There is still no definitiveconsensus of the pandemics’ behavior,COVID-19 mode of transmission,diagnostic criteria, and managementprotocols. Preparation for a pandemicinvolves considering the increasing lev-els of protection and infection controland how they should be implementedduring different phases of the pan-demic. In the operating room (OR)setting, these measures include the fol-lowing: modification of healthcareinfrastructure and processes, educatingstaff and patients, implementing infec-tion control strategies, and administra-tive and clinical measures. The surgicalmanagement of traumatic injuriesrequires a complex environment withmultiple stakeholders including sur-geons, anesthesiologists, nurses, ORattendants, andmedical staff; it can be areal challenge to align the perspectivesand concerns of all parties The primary
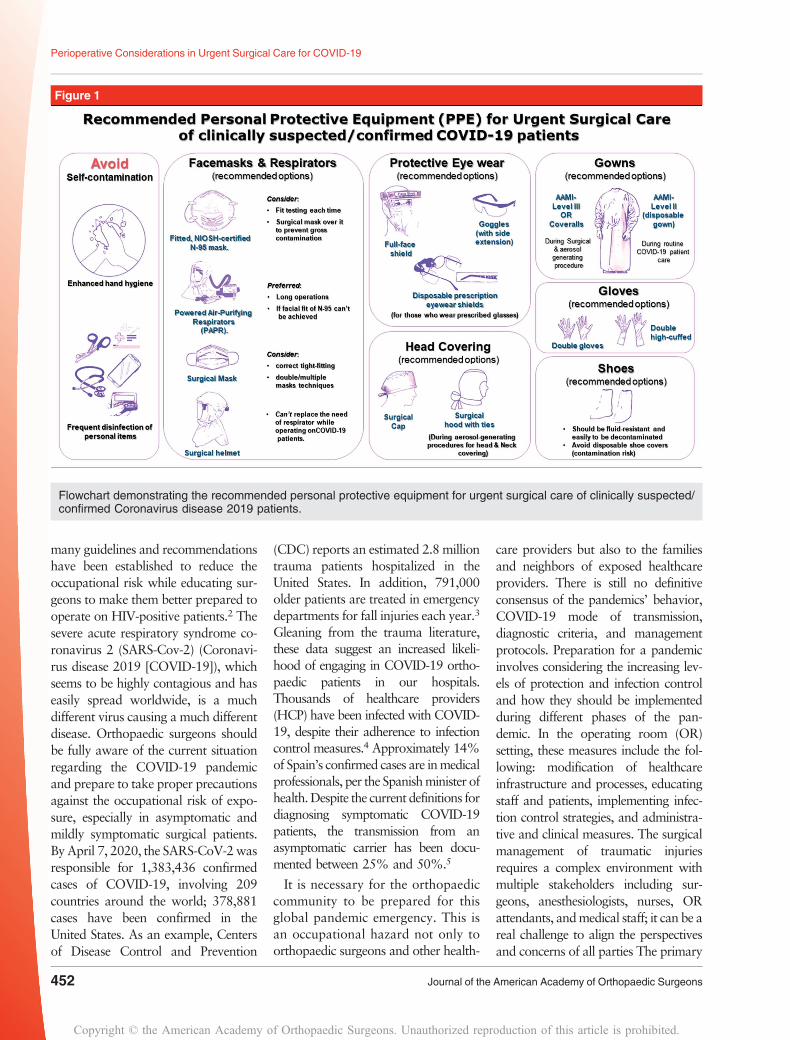
Figure 1
Flowchart demonstrating the recommended personal protective equipment for urgent surgical care of clinically suspected/confirmed Coronavirus disease 2019 patients.
Perioperative Considerations in Urgent Surgical Care for COVID-19
452 Journal of the American Academy of Orthopaedic Surgeons
Copyright © the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited.
aim of this article is to help define theCOVID-19 crisis and discuss effectivemanagement strategies. This articleprovides a brief summary of the currentsituation and understanding of thepandemic, diagnostic criteria, and at-tempts to forecast the extent andprognosis. Finally, recommending pre-cautions and preventive actions toreduce the occupational risk in treatingclinically suspected/confirmed COVID-19 surgical patients.
Recommendation andProactive Measures forManaging theSuspected/Confirmed,Orthopaedic Patients WithCoronavirus Disease 2019
General RecommendationsThe CDC and World Health Organi-zation instituted guidelines for routineinfection prevention measures after
the worldwide spread of the SARS-CoV-2 virus. HCP are recommendedto wear a simple surgical mask andperform regular hand washing whencontacting low-risk individuals toprotect against contamination. HCPsin high-risk areas should adhere toinfection prevention and controlpractices, which includes the appro-priate use of engineering controls(negative pressure rooms), adminis-trative controls, and personal protec-tive equipment (PPE) (Figures 1–3).
Recommended PersonalProtective Equipment andInfection Control Measures
Tominimize the risk of transmissibilityand cross-infection, the CDC has rec-ommended airborne, droplet, and con-tact precautions. This includes themandatory use of PPE which includesgowns, gloves, face masks, and eitherN95, P100, or FFP2 respirators with a
face shield/googles or powered air-purifying respirator (PAPR) to mini-mize the risk of transmissibility andcross-infection.6 Per CDC recom-mendations, a clinically suspected/confirmed COVID-19 patient shouldwear a cloth face covering, over nose,and mouth and a surgical mask shouldbe reserved for HCP and first res-ponders.6 Unfortunately, these PPErecommendations for both providersand patients will fail to prevent trans-mission if frequent surfaces decon-tamination, enhanced hand hygiene,and avoiding self-contamination arenot carefully considered. Providersmust focus onmeticulous hand hygieneand disinfecting personal items, such asstethoscopes, phones, ID tags, laptops,dictation devices, etc. (Figure 1). Aroute to minimize exposure and con-tact between triage to induction room,OR, and then to recovery roomsshould be frequently cleaned and dis-infected. It is recommended for an
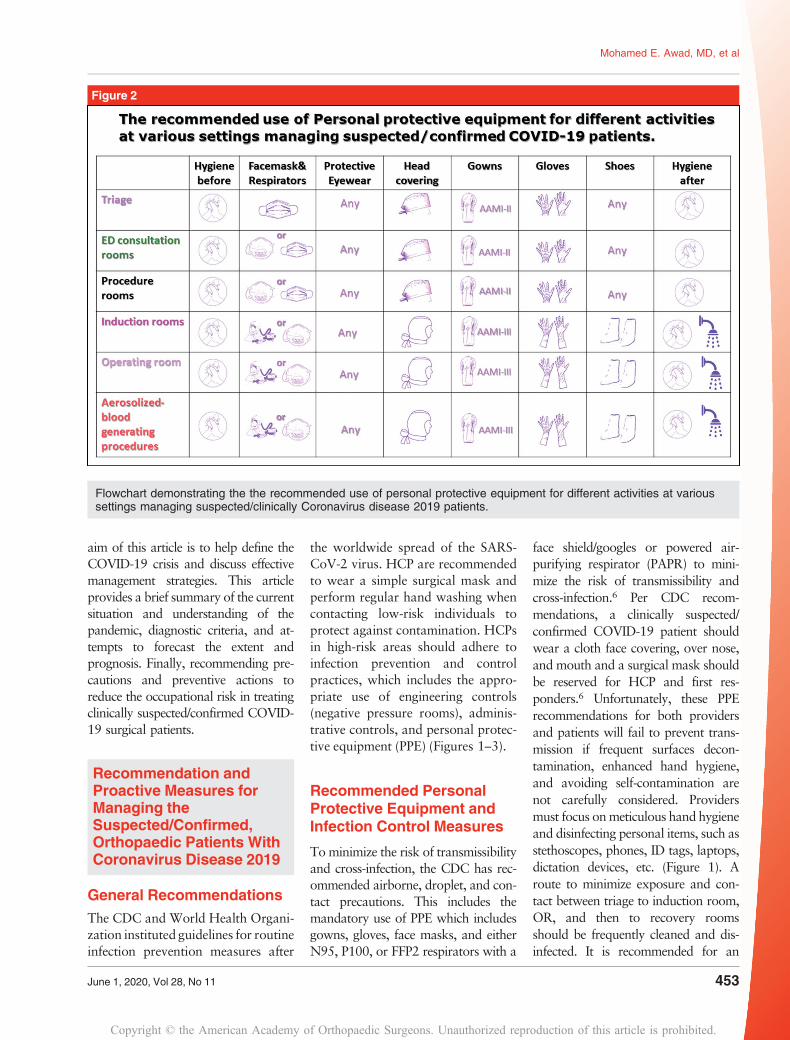
Figure 2
Flowchart demonstrating the the recommended use of personal protective equipment for different activities at varioussettings managing suspected/clinically Coronavirus disease 2019 patients.
Mohamed E. Awad, MD, et al
June 1, 2020, Vol 28, No 11 453
Copyright © the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited.
environmental services worker toincrease the frequency to disinfect themost contaminated and most touchedsurfaces, such as the elevator buttons,door handles, light switches, grab rails,and etc. A recent study examined themost contaminated objects and PPE inthe hospitals of Wuhan, China. Of thesamples collected fromHCP using PPE(hand sanitizer dispensers, gloves, andprotective eyewear/full-face shield),12.9% were positive for SARS-CoV-2RNA. The highest rates of contami-nation were found on hand sanitizerdispensers, gloves, goggles/face-shieldsat a rate of 20.3%, 15.4%, and 1.7%,respectively.7
Facemasks and Respirators;Which to Use?
The CDC had recommended thatHCPs closely interacting with clini-cally suspected/confirmed COVID-19patients should wear N95 respirators,
along with gowns, gloves, and protec-tive eyewear. With the current globaldemand and shortage of PPE, the sup-ply chain of specialized respiratorscannot meet demand but the looser fit-ting surgical face masks might be anacceptable alternative.6 Notably, mostrespirators (eg, N95) require trainingto properly fit them around the max-illofacial region to ensure appropriatefitting. Our recommendations for usingface masks and respirators varies de-pending on the setting and activity(Table 1). The available options forHCPs are the following (Figure 1):(1) Fitted, National Institute for
Occupational Safety and Health(NIOSH)-certified N-95 masks• Each time the N-95 respiratoris taken off, the wearer mustdouble-check that it has notbeen soiled or damaged beforedonning it again.
• If achieving and maintaining avery close facial fit of N-95
cannot be guaranteed duringthe whole time of aerosolizedblood-generating procedure,PAPR is highly recommended.
• Consider placing a simple sur-gical mask on top of the N-95to prevent gross contamination.
(2) PAPR• It is preferred for long oper-ations (if available)
(3) Surgical masks• consider double/multiple masktechniques and correct tight-fitting
• It is not recommended in per-forming aerosolized blood-generating procedures forsuspected/confirmed COVID-19 patients.
• Generally, surgical masks donot provide complete protec-tion from germs and othercontaminants because of itsloose facial fit. Therefore, cau-tion should be exercised.
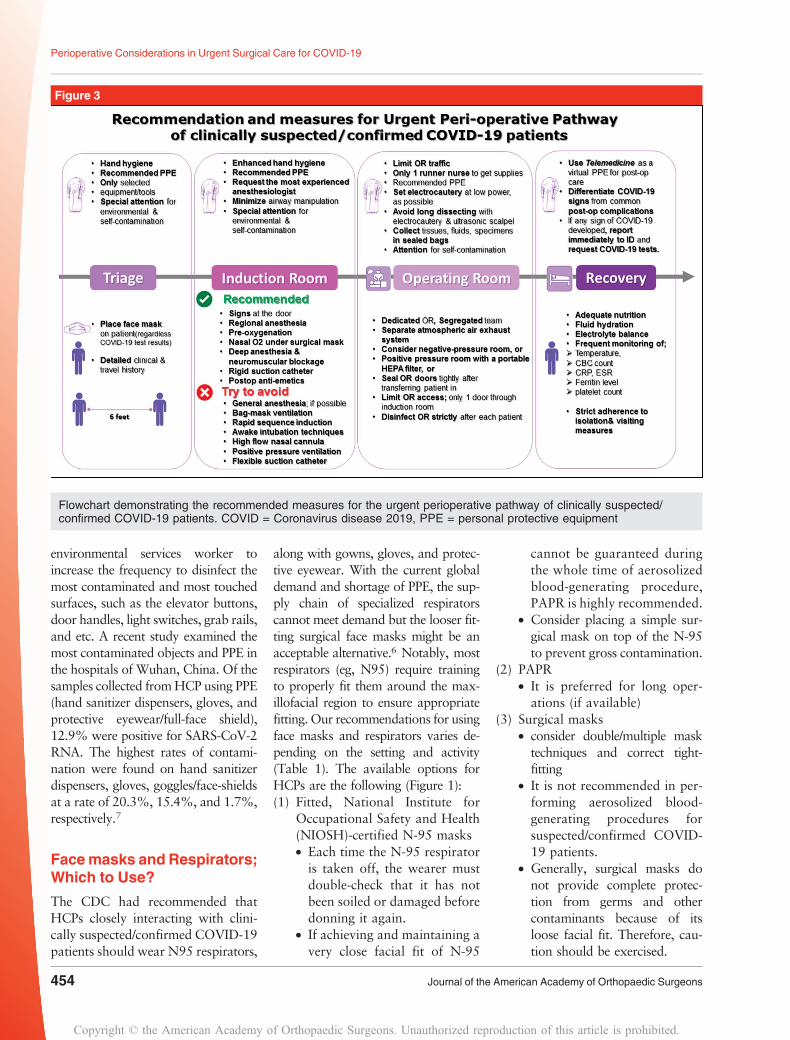
Figure 3
Flowchart demonstrating the recommended measures for the urgent perioperative pathway of clinically suspected/confirmed COVID-19 patients. COVID = Coronavirus disease 2019, PPE = personal protective equipment
Perioperative Considerations in Urgent Surgical Care for COVID-19
454 Journal of the American Academy of Orthopaedic Surgeons
Copyright © the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited.
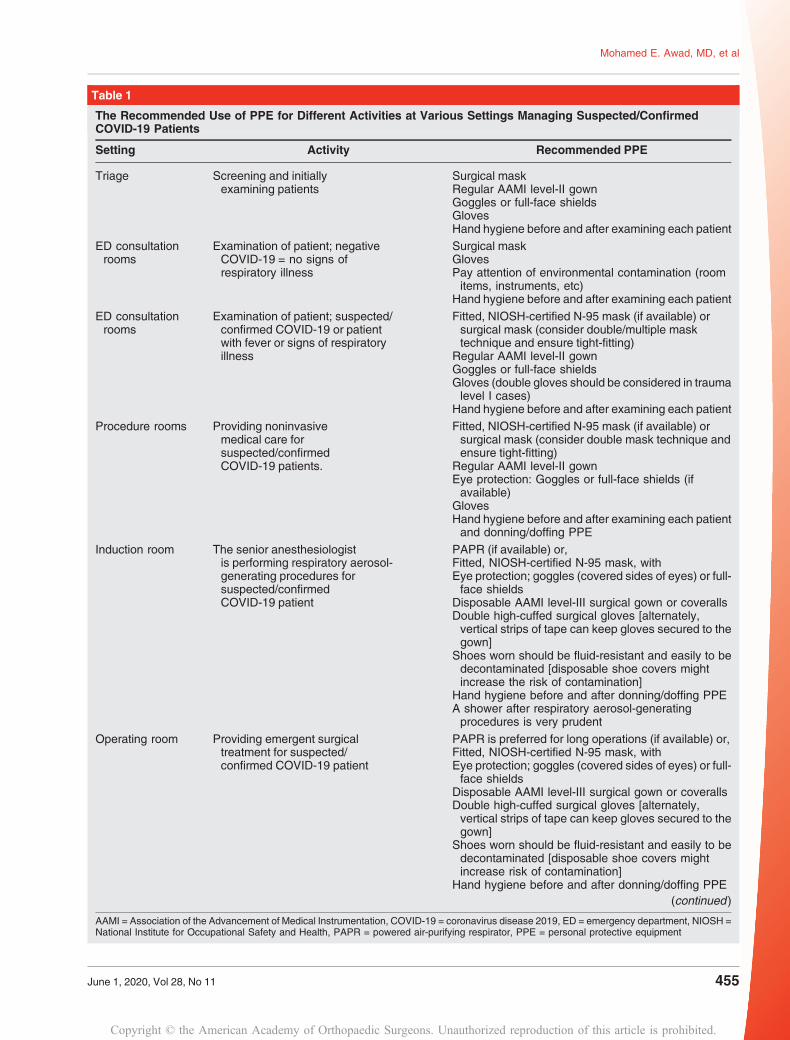
Table 1
The Recommended Use of PPE for Different Activities at Various Settings Managing Suspected/ConfirmedCOVID-19 Patients
Setting Activity Recommended PPE
Triage Screening and initiallyexamining patients
Surgical maskRegular AAMI level-II gownGoggles or full-face shieldsGlovesHand hygiene before and after examining each patient
ED consultationrooms
Examination of patient; negativeCOVID-19 = no signs ofrespiratory illness
Surgical maskGlovesPay attention of environmental contamination (roomitems, instruments, etc)
Hand hygiene before and after examining each patient
ED consultationrooms
Examination of patient; suspected/confirmed COVID-19 or patientwith fever or signs of respiratoryillness
Fitted, NIOSH-certified N-95 mask (if available) orsurgical mask (consider double/multiple masktechnique and ensure tight-fitting)
Regular AAMI level-II gownGoggles or full-face shieldsGloves (double gloves should be considered in traumalevel I cases)
Hand hygiene before and after examining each patient
Procedure rooms Providing noninvasivemedical care forsuspected/confirmedCOVID-19 patients.
Fitted, NIOSH-certified N-95 mask (if available) orsurgical mask (consider double mask technique andensure tight-fitting)
Regular AAMI level-II gownEye protection: Goggles or full-face shields (ifavailable)
GlovesHand hygiene before and after examining each patientand donning/doffing PPE
Induction room The senior anesthesiologistis performing respiratory aerosol-generating procedures forsuspected/confirmedCOVID-19 patient
PAPR (if available) or,Fitted, NIOSH-certified N-95 mask, withEye protection; goggles (covered sides of eyes) or full-face shields
Disposable AAMI level-III surgical gown or coverallsDouble high-cuffed surgical gloves [alternately,vertical strips of tape can keep gloves secured to thegown]
Shoes worn should be fluid-resistant and easily to bedecontaminated [disposable shoe covers mightincrease the risk of contamination]
Hand hygiene before and after donning/doffing PPEA shower after respiratory aerosol-generatingprocedures is very prudent
Operating room Providing emergent surgicaltreatment for suspected/confirmed COVID-19 patient
PAPR is preferred for long operations (if available) or,Fitted, NIOSH-certified N-95 mask, withEye protection; goggles (covered sides of eyes) or full-face shields
Disposable AAMI level-III surgical gown or coverallsDouble high-cuffed surgical gloves [alternately,vertical strips of tape can keep gloves secured to thegown]
Shoes worn should be fluid-resistant and easily to bedecontaminated [disposable shoe covers mightincrease risk of contamination]
Hand hygiene before and after donning/doffing PPE(continued )
AAMI = Association of the Advancement of Medical Instrumentation, COVID-19 = coronavirus disease 2019, ED = emergency department, NIOSH =National Institute for Occupational Safety and Health, PAPR = powered air-purifying respirator, PPE = personal protective equipment
Mohamed E. Awad, MD, et al
June 1, 2020, Vol 28, No 11 455
Copyright © the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited.
Of note, the regular surgical helmetcannot replace the need of respiratorwhile operating on suspected/confirmed COVID-19 patients.
Protective Eye WearDonning eye protection equipment isrecommended because the inoculationof the conjunctival mucousmembraneis a mode of transmission.8,9 Ourrecommendations for using protectiveeyewear are the following:
• Prioritize eye protection equip-ment for certain selected surgi-cal procedures, ie, duringaerosol-generating procedures(splashes, sprays, etc) and wherethere is prolonged face-to-faceor close contact with a sus-pected or confirmed COVID-19patients.
• Full-face shield (if available) orgoggles can be issued to eachprovider.
• Consider using safety goggleswith extensions to cover thesides of eyes.
• Consider using disposable pre-scription eyewear shields (for
those who wear prescribedglasses)
• During supply shortage, use eyeprotection equipment beyondthe manufacturer-designatedexpiration date.
• During supply shortage, followand adhere to the manufacturerinstructions for reuse and dis-infection. If these instructionsare not provided, consider theCDC recommendations.10
Gowns
• Association of the Advancementof Medical Instrumentation(AAMI) ratings are based on thelevel of fluid protection in thecritical zone or chest region of thesurgical gown. The AAMI levelshould be checked on the pack-aging because they may come inseveral different designs, materi-als, and colors.
• Nonsterile, disposable, or reusable-AAMI Level-II gowns (frequentlyseen as disposable isolation gowns)are appropriate for use by pro-
viders during routine COVID-19patient care.
• Surgical gowns AAMI-Level-III(typically those found in oper-ating rooms) or coveralls shouldbe prioritized for surgical andaerosolized blood-generatingprocedures.
Table 1 and Figure 1 provide ourrecommendation in this regard basedon different settings and activities.
Gloves
• Double gloves are recom-mended when handlingCOVID-19 patients as an extraprecaution to minimize con-taminating ORs items, equip-ment, and surfaces. The outerpair should be pulled off beforetouching equipment or surfacesin other areas of OR.11
Surgical Head Cap
• Surgical cap should be used perroutine protocols.
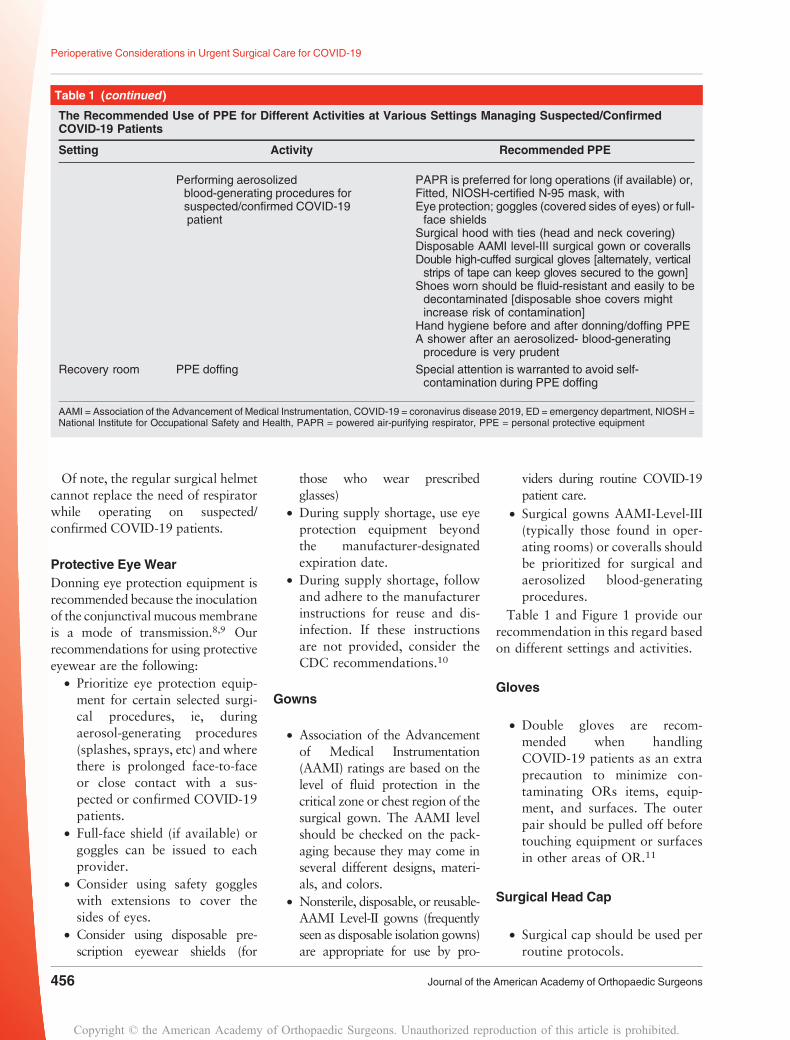
Table 1 (continued )
The Recommended Use of PPE for Different Activities at Various Settings Managing Suspected/ConfirmedCOVID-19 Patients
Setting Activity Recommended PPE
Performing aerosolizedblood-generating procedures forsuspected/confirmed COVID-19patient
PAPR is preferred for long operations (if available) or,Fitted, NIOSH-certified N-95 mask, withEye protection; goggles (covered sides of eyes) or full-face shields
Surgical hood with ties (head and neck covering)Disposable AAMI level-III surgical gown or coverallsDouble high-cuffed surgical gloves [alternately, verticalstrips of tape can keep gloves secured to the gown]
Shoes worn should be fluid-resistant and easily to bedecontaminated [disposable shoe covers mightincrease risk of contamination]
Hand hygiene before and after donning/doffing PPEA shower after an aerosolized- blood-generatingprocedure is very prudent
Recovery room PPE doffing Special attention is warranted to avoid self-contamination during PPE doffing
AAMI = Association of the Advancement of Medical Instrumentation, COVID-19 = coronavirus disease 2019, ED = emergency department, NIOSH =National Institute for Occupational Safety and Health, PAPR = powered air-purifying respirator, PPE = personal protective equipment
Perioperative Considerations in Urgent Surgical Care for COVID-19
456 Journal of the American Academy of Orthopaedic Surgeons
Copyright © the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited.

• Surgical hood with ties can beused for head and neck coveringduring aerosol-generatingprocedures.
Transfusion-transmittedCoronavirus andAerosolized blood-Generating Procedures;What is the Risk?
COVID-19 is presumed to spreaddirectly via infectious respiratory drop-lets and close contact (because SARS-CoV-2 cannot survive without a car-rier).12 However, these transmissionmodes do not explain all cases. Recentdata have shown that COVID-19might survive and be transmittedindirectly from virus contamination ofcommon surfaces and objects aftervirus aerosolization in a confined spacewith by infected individuals.12 Theincubation period for COVID-19 isapproximately 4 days, and studiessuggest that it may range anywherefrom 2 to 14 days.13-15 A recent studyinvestigating SARS-CoV-2 from clini-cal specimens found that RNA virusdetected in blood samples from con-firmed COVID-19 patients (3 of 307;1%).16 Huang et al17 reported that15% of patients with laboratory con-firmed COVID-19 had viral RNA intheir plasma. The implications of thesefindings are still unclear, and thereare no reported cases of transfusion-transmitted coronaviruses throughApril 5, 2020. However, continuedvigilance is essential. Despite studiesdetecting viral RNA in the serumor plasma of confirmed/suspectedCOVID-19 patients, blood transmis-sion and infectivity are still not fullyunderstood. Because there is little evi-dence and vague guidelines for bloodtransfusion in the current setting, it isrecommended to recuse anyone withsymptoms or signs of respiratory illnessfrom blood donation.18 The US FDAhas suggested to retrieve and quaran-tine any blood products collected in the
28 days before, or after, either COVID-19 disease onset or possible exposureto individuals who are COVID-19positive.18 Theoretically, viremia inpatients with asymptomatic or con-firmed COVID-19 patients couldpose a risk of transmissibility to theorthopaedic team during aerosolizedblood-generating procedures.19 Theuse of high-speed drills, bone saws,reamers, electrocautery, and ultrasonicscalpels generate significant amounts ofaerosols, increasing the risk of viralcontamination of the environment.20 Arecent Canadian study described low-fidelity simulation training to evolve themodified PPE used for aerosol-generating procedures of suspected/confirmed COVID-19 patients andassess the sites of contamination21 Thespread of the aerosolized respiratorysecretions and contamination sites werevisualized with a commercial powderproduct and ultraviolet light. Theydemonstrated a significant amount ofcontamination on the provider’s neck,base of the wrist, and their lower pantsand shoes. These sites, however, areprobably not associated with a directmethod of transmission for SARS-CoV-2. However, there are definite sourcesof self-contamination during PPE doff-ing. In addition, the disposable AAMILevel-III fluid-resistant, surgical gownsor coveralls are recommended becausethey detected no contamination ofscrubs beneath the surgical gowncompared with reusable surgical gowns(AAMI, Level-II). The AAMI, level-IIgowns were permeable to aerosolizedsecretions. The recommended PPE forperforming respiratory aerosol oraerosolized blood-generating proce-dures for suspected/confirmed COVID-19 patients (Table 1):
• PAPR is preferred for long op-erations (if available)
• Fitted, NIOSH-certified N-95mask, with the following:
• Eye protection; goggles (coveredsides of eyes) or full-face shields(if available)
• Surgical hood with ties (headand neck covering)
• Disposable AAMI level-III sur-gical gown or coveralls
• Double high-cuffed surgicalgloves (alternately, vertical stripsof tape can keep gloves secured tothe gown and minimize exposingwrist to contamination (N.B.Circumferential taping may makedoffing more challenging)22
• Shoes or booties worn should befluid-resistant and easily to bedecontaminated (disposableshoe covers might increase therisk of contamination)
• Hand hygiene before and afterdonning/doffing PPE
• A shower after an aerosolizedblood-generating procedure isvery prudent.
Strategies for Optimizingthe Supply of PersonalProtective Equipment
During the initial phase of US cases ofCOVID-19, one Washington statehospital reported that staff changedtheir PPE 20 times per shift.23 Manyengineering and administrativemeasures should be consideredespecially if the current pandemicbecomes prolonged. These measuresaim to mitigate the anticipated riskof global shortage of PPEs, such assurgical mask, N-95 mask, gowns,etc. Extended use or limited reuse areapplicable alternatives to prevent theanticipated supply shortage of facemasks, respirators, and protectiveeyewear equipment and to ensurethat healthcare staff have securedaccess to the necessary supplies forpatient care. Limited PPE reuse refersto the practice of using the sameN-95 mask for multiple encounterswith patients removing it betweenencounters and doffing to ensureproper fit and the absence of grosscontamination. In the operative set-ting, this may be done by wearing.
Mohamed E. Awad, MD, et al
June 1, 2020, Vol 28, No 11 457
Copyright © the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited.

Consider placing a simple surgicalmask over the N-95 for preventinggross contamination and change itbetween encounters. Reuse of pro-tective eyewears, such as full-faceshields and goggles, will be allowedif these are individually assigned toeach member and regularly get dis-infected. Reuse practice is permittedfor a single person use (no-sharing).Reuse and reprocessing of the N-95mask guidelines have been released bythe CDC and include the use ofultraviolet light processing, hydrogenperoxide in either liquid or vaporizedstate, and moist heating decontami-nation.24 These guidelines should bereviewed at length before attemptingreprocessing of equipment to preventpotentially catastrophic error.Extended use refers to the practice ofusing the same respirators forrepeated close contact encounterswith multiple patients, without doff-ing it between the encounters. Thispractice might be preferred over reuse,assuming this would reduce the risk ofself-contamination through frequentdonning and doffing of the sameequipment. These practices varybetween institutions especially forusing N-95 masks. Theoretically, theHCP could extend this and toleratewearing N-95 masks for up to 8 to 12hours.25,26 However, most providersusually take breaks during shifts forlunch/toilets. Therefore, extended usebeyond 4 hours might be impracticalin most settings,27 although limitedreuse practice could be adopted withnegative or low-risk patients.28
The Triage Area andPreoperative Measures andRecommendations
Within crisis situations and high-riskenvironments, especially at crowdedtriage and ED, rigor in following thedesigned and recommended meas-ures for all HCP and patients iscrucial.29
(1) Ask patients to wear a clothface covering (a scarf or ban-dana) or face mask on the patient(regardless of the COVID-19 testresults) at arrival, promotingcough etiquette, and providingtissues and for hand hygiene(Figure 3).
(2) Suspected or confirmedCOVID-19 patients should be innegative pressure rooms if pa-tients are coughing or proce-dures that create aerosols arebeing done (if negative pressurerooms are available), or
(3) Clinically suspected/confirmedCOVID-19 patients should sep-arately triaged with at least 6-feet distance from other patientsor nontreating staff.
(4) Surgeons should not approachthe triage area withoutthe minimum standard of PPE.
(5) The recommended PPE in thetriage area is as follows (Table 1and Figure 2):• Surgical mask• Regular AAMI level-II gown• Goggles or full-face shields• Gloves• Eye protection and the respi-rator or face mask should beremoved, and hand hygienedone if they become damagedor soiled before leaving thearea.
(1) Triage personnel should have asupply of PPE, surgical facemasks for the surgical team, andfor the patients with symptomsof respiratory infection.
(2) If the patient is oriented withmoderate Glasgow Coma Scale(GCS) score, ask for the clinicaland epidemiological criteria ofCOVID-19 (The presence ofsymptoms of a respiratory infec-tion, fever, and or contact withpossible COVID-19 patients.)
(3) It is preferred if possible to orderimmediate SARS-CoV-2 reversetranscription polymerase chainreaction assay if patient is being
admitted and especially beforesurgery and possible intubation.
(4) Patient with noninjured faceand/or upper respiratory tractshould wear a surgical face maskand be moved along a designatedroute with a minimal contactwith others as much as possible.
(5) Only selected equipment andassessment tools should bebrought into the triage room tominimize the number of itemsthat need to be disinfected afterthe exposure.
Segregation, Restructure,and Designed Workflow
The main principles of the staff seg-regation, physical restructure, andthe designed workflow should focuson reducing exposure and contami-nation, ensuring adherence to PPE,and subsequent decontamination.Ideally, two types of hospital segre-gation should be done. Location-based segregation of orthopaedicstaff reduces the potential risk ofcross-infection. Orthopaedic sur-geons, for example, should not beperforming screening examinationson the general public because of therisk of exposure. Geographic segre-gation within the OR complex limitsthe OR traffic, decreases the expo-sure, and minimizes the contamina-tion zone.30 With the rapid increasein the number of COVID-19 pa-tients, orthopaedic staff should besegregated into those who are treat-ing suspected/confirmed COVID-19patients and those who are treatingnoninfective patients when possibleis not. This however may not bepossible in smaller hospital systemsand practices. Besides screening andisolation of high-risk, confirmedCOVID-19 patients, strict and fre-quent screening of the segregated ORstaff is mandatory. Members of thesegregated or exposed staff shouldimmediately report any signs of
Perioperative Considerations in Urgent Surgical Care for COVID-19
458 Journal of the American Academy of Orthopaedic Surgeons
Copyright © the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited.
illness and must be taken off dutyimmediately. In addition, all contactevents between patients and staffmust be recorded so that contacttracing and infection control meas-ures can be implemented quickly, incase any member of segregated stafftested positive.
Induction Room(AnesthesiaRecommendations forSuspected/ConfirmedCoronavirus Disease 2019
(1) SARS-CoV-2 test should beconsidered in high-risk in-dividuals, preferably before sur-gery and before intubation ifpossible.28,31-33
(2) Signs must be placed at induc-tion and OR doors to alert otherstaff not to access the dedicatedunit without donning theappropriate PPE (Figures 2 and3).
(3) The most experienced anesthe-siologist should intubate thepatients (The rationale behindthis recommendation is to makecompetent induction attempt inthe shortest possible time, with-out compromising the infectioncontrol measures or the staff’ssafety)
(4) Try to minimize the airwaymanipulation, face mask venti-lation, open airway suction asmuch as possible.
(5) Regional anesthesia is recom-mended over general anesthesia(when using regional anesthesia,patients must always wear sur-gical masks).
(6) Nasal O2 should be adminis-trated under the surgical mask.
(7) Avoid awake intubation techni-ques, high flow nasal canula andpositive pressure ventilation (maylead to virus aerosolization).
(8) Avoid bag-mask ventilation anduse rapid sequence induction (if itcannot be avoided, administratesmall tidal volumes).
(9) Use deep anesthesia and neuro-muscular blockage.
(10) Preoxygenation should be donevia a well-fitting face mask toavoid hypoxia in critically illCOVID-19 patients withrespiratory failure.
(11) Administrate antiemetics toreduce post-op retching andvomiting that would require themask removal.
(12) Use a rigid suction catheterinstead of a soft flexible one(reduce contamination).
(13) The patient should recoverwithin the OR when possible.
Operating Room Measuresand Recommendations
It is a system-saving, necessary act toplan and restructure our surgical carepathwaysandprotocolduringCOVID-19 pandemic to protect our communityand patients and conserve our valuableresources. The restructure shouldmainly focus on developing a reason-ableplan foroperatingonemergentandurgent cases. Dedicating a COVID-19pre-, intra-, and post-operating spacesand training the administrative andsurgical staff on the appropriate use ofPPE and COVID-19 care pathways tothebest of ahospital’s ability minimizesexposure and contamination.(1) If there is suspected COVID-19
diagnosis, the surgical planningshould be re-evaluatedimmediately.
(2) Prepare and set up a separate,isolated OR with separate ven-tilation system (in case of con-firmed COVID-19 case) (Figure3).
(3) Dedicated ORs should have aseparate atmospheric air inlet andoutlet exhaust system. Recentstudies highlighted the necessity to
isolate and operate on suspected/confirmed COVID-19 patientswithin negative pressure OR/isolation room to disseminate theviral load.21,22,28,32 However,heating, ventilation, and air con-ditioning system in most of the USoperating rooms is designed toprovide positive pressure. Consid-ering the current poorly controlledsituation, adding a portable, self-contained high efficiency particu-late air filtration system to thehospital heating, ventilation, andair conditioning systems wouldeconomically create a negativepressure that meets the Occupa-tional Safety and Health Admin-istration and CDC tuberculosisguidelines.34
(4) When possible, entry to the ORmust be only through the anes-thetic induction room.
(5) All OR doors should be wellsealed once the patient is trans-ferred in (except one door).
(6) The OR team involved in thesurgery should be limited.
(7) Limit the OR access and move-ment in and out to medically/surgically essential purposes.
(8) Strict adherence to high standardof infection control andprevention.
(9) Surface-tough equipment andscreens within OR should bewrapped with plastic sheets tofacilitate decontamination (thevirus can survive within tinygrooves, under buttons, screenperipheries, etc.).
Strict adherence to the recom-mended high standard PPE. Our rec-ommendations for operating onsuspected/confirmed COVID-19 pa-tients is as follows (Table 1 and Fig-ure 2).
• PAPRs are preferred for longoperations (if available) or,
• Fitted, NIOSH-certified N-95mask with;
• Eye protection; goggles (coveredsides of eyes) or full-face shields
Mohamed E. Awad, MD, et al
June 1, 2020, Vol 28, No 11 459
Copyright © the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited.

• Disposable AAMI level-III sur-gical gown or coveralls
• High-cuffed surgical gloves(alternately, vertical strips oftape can keep gloves secured tothe gown [double gloves may beconsidered but are not yet con-sidered the standard]).35
• Shoes worn should be fluid-resistant and easily to be de-contaminated (disposable shoecovers might increase the risk ofcontamination)
• Hand hygiene before and afterdonning/doffing PPE
(1) Try to use disposable medicalsupplies/instruments as much aspossible.
(2) The settings of electrocauteryshould be as low as possible andavoid long dissecting timesto minimize the surgical smoke.
(3) Attention is required to avoidsharp injury or damage of PPE.
(4) The body fluids, blood, secre-tions, and pathological speci-mens should be collected indouble sealed bags for inspectionor destruction.
(5) The patient’s case, surgicalplanning, documentation, andearly recovery should be donewithin OR to minimize the con-tamination to one room.
(6) Once the patient has been dis-charged or transferred, HCP,including environmental servicespersonnel, should refrain fromentering the vacated room untilenough time has elapsed forenough air changers to removepotentially infectious particles.
(7) The OR should be strictly dis-infected after use.
(8) Special attention is warranted toavoid self-contamination duringPPE doffing.
(9) All contaminated instrumentsand devices should be disinfectedseparately followed by properlabeling.
Recovery Room(PostoperativeRecommendations)
Postoperative management is a cru-cial phase for clinically suspected/confirmed COVID-19 patients.Trauma, infection, and oncologic sur-geries may be associated with slowrecovery, lengthier hospital stays, andmore complications. After surgery, thepatient’s immune system may becompromised, and there may be lowerrespiratory tract and/or wound in-fections generally associated with fever.In light of this information, surgeonsmust be more vigilant to differentiatecommon postoperative complicationsfrom COVID-19 infections. In thepresence of fever and one of thesymptoms of a respiratory infection(dry cough, etc), laboratory tests forCOVID-19 diagnosis must be ordered.Suspected cases should be reportedimmediately, and under the premise ofensuring the safety of patient, trans-portation to an isolation ward. Sur-geons, nurses, and medical staff sharean equal responsibility for the postop-erative management, particularly inmonitoring the patients’ families andvisitors to ensure the strict adherence tothe pandemic emergency system.Whenpossible, it is important to limit thevisitors as much as possible. In fact,most hospitals have recently dis-continued visitation by anyone. Post-operatively, patients should receiveadequate nutrition, fluid hydration,and electrolyte balance to promoteimmune recovery and rapid rehabili-tation. Frequent monitoring of tem-perature, laboratory complete bloodcounts, C-reactive protein, ferritin levelshould be done in any patient withsuspected COVID-19. There is recentevidence suggesting that a subgroup ofsevere COVID-19 might cause a“cytokine storm syndrome,” which isan under-recognized, hyper-inflammatory syndrome characterizedby a fulminant and fatal hyper-
cytokinemia with multiorgan fail-ure.36,37 An increased level of ferritinoccurs in approximately 50% of pa-tients. All patients with severe COVID-19 should be screened for hyper-inflammation markers such asincreased ferritin, decreased plateletcount, increased LDH or CRP.36
Telemedicine: A VirtualPersonal ProtectiveEquipment forPostoperative Care
One of potential consequences andsystemic changes of dealing with theCOVID-19 pandemic is the adoptionand wide utilization of telemedicinein the surgical care of clinicallysuspected/confirmed COVID-19 pa-tients.Over thepast couple ofmonths,the traditional clinics or postoperativefollow-up visits have been replacedwith telemedicine modalities. Tele-medicine could act as a virtual post-operative PPE to provide impeccablesocial distancing for patients’ safetyand for all HCPs so critically neededin frontline against the pandemic.Orthopaedic surgeons can use tele-medicine postoperatively to follow-up with COVID-19 patients in threemanners38; to schedule follow-up,39-42 for routine monitoring,43-45
andmanagement of recovery issues asneeded.46-48 In addition, the use oftelemedicine-based services for surgi-cal wound care has proven to befeasible and safe in the early postop-erative evaluation.49,50 Both time andcost savings contribute toward highpatient satisfaction.39 A randomizedcontrolled trial demonstrated thatthere was no significant difference inpatient satisfaction between tele-medicine and face-to-face follow-upvisits in an orthopaedic traumacohort.41 Another study after totaljoint arthroplasty showed that tele-medicine significantly reduce thecycle “appointment” time with anaverage Skype follow-up call per
Perioperative Considerations in Urgent Surgical Care for COVID-19
460 Journal of the American Academy of Orthopaedic Surgeons
Copyright © the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited.
patient that was 2.71 minutes shorterthan face-to-face visits.42 Researchshowed that for every 23 miles awayfrom clinic, there is 111% probabilitythat a patient will more likely preferusing telemedicine for their postop-erative follow-up.48 Surgeons formdifferent specialties have expressedtheir satisfaction after using thesetelemedicine modalities to deliverpostoperative care.44,48,50,51 Notably,telemedicine revealed high levels ofprovider-perceived quality of medicalhistory (82%) and therapeutic man-agement (85%), compared with tra-ditional face-to-face visits (72%) and(86%), respectively.52 Preparation,practice, and following telemedicinestart-up checklists would be useful toensure effective implementation oftelemedicine.53,54 The current focusshould be directed in evolving moresecured modalities to protect patient’sconfidentiality and keep their medicalrecords away from any anticipatedbreach.
Training and Intervention ofHealthcare Providers
Thecurrent infectious riskonhealthcarepersonnel would have negative con-sequences, if they are not adequatelyprepared, trained, or equipped to miti-gate the risk. Orthopaedic educatorsshould educate their fellows, residents,students, and ancillary teams in pre-ventingexposure toandthespreadingofCOVID-19. The care teams must learnhow to protect themselves during apandemic. Refresher training regardingthe standard use of PPE is a necessity inthis global pandemic. A recent study atthe University of Illinois Chicago55 as-sessed the PPE doffing practices ofhealthcare workers. The study demon-strated that 90% of observed PPEdoffing was incorrect regarding thedoffing sequence, doffing technique, oruse of appropriate PPE.55 Anothersurvey showed that 14.9% of health-care personnel did not receive previous
training for appropriate PPE doffingpractices.56 Training and educationmight flatten the curve of cross-infection and self-contamination.Training and education of the surgicalstaff should be continually emphasized.It is imperative that all staff be taughtthe proper sequential methods of don-ning and doffing of PPE and mask-fitting techniques to minimize the riskof self-contamination. Frequent auditsof infection control must be conducted.A trained observer should be assignedfor each emergent operation to identifythe weaknesses and implement thenecessary steps.
Simulation-based Training
Simulation-based training might berequired to improve the team commu-nication during medical crisis57 toestablish competencies in PPE donningand doffing practices and workflow ininduction, operating, and recoveryrooms. Simulation can mimic differentclinical scenarios to integrate knowl-edge to practice, evaluate the pro-viders’ performances, and build upself- and team-confidence for real-lifecases. Lockhart et al21 demonstratedthat simulation was a powerful tool totest and adapt PPE as compared tobaseline recommendations alone.Using simulation-based training couldbe an effective method to replicatehighly contiguous COVID-19 casesin a safe, yet challenging, situationwithout jeopardizing the team safety.
Psychological Support ofPatients and Providers
COVID-19 is a major and suddenpublic health crisis, followed by aseries of emergency response meas-ures for community and healthcareservices. The uncertainty of under-standing the pandemic behavior andthe definitive ways for its preventioncause psychological pressures onboth the public andHCPs. The public
panic and fear of getting infected canincrease the burden and use ofhealthcare services. The surgeonsshould be fully aware of the psycho-logical pressure on the patients andtheir families. The knowledge, coun-seling, education, and support maymitigate the psychological pressure infighting the pandemic.
Summary
Apart from the fact that this pan-demic certainly involves manyimportant health, economic, andcommunity ramifications, it also re-quires several initiatives to mandatewhat measures are most appropriateto prepare for mitigating the occu-pational risks. These initiativesinclude understanding the differentaspects in disease and transmissioncontrol in the ongoing pandemic.Strict adherence to CDC and WorldHealth Organization evidence-basedguidelines for PPEand environmentalhygiene enhances the safety and im-proves the mitigation of infection inemergent orthopaedic practice. Nev-ertheless, we think that these recom-mended measures might optimize thehealthcare services provided to con-firmed COVID-19 patients andshould reduce the risk of occupa-tional transmission to other patientsand healthcare professionals.
References
References printed in bold type arethose published or accessed online in2020.
1. The U.S. Department of Health andHuman Services, O.f.C.R.H.O.: HHS officefor civil rights secures corrective action andensures Florida orthopedic practice protectspatients with HIV from discrimination.2019. Available at: https://www.hhs.gov/about/news/2019/10/30/hhs-ocr-secures-corrective-action-and-ensures-fl-orthopedic-practice-protects-patients-with-hiv-from-discrimination.html. AccessedMarch 13, 2020.
Mohamed E. Awad, MD, et al
June 1, 2020, Vol 28, No 11 461
Copyright © the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited.
2. Kuhar DT, Henderson DK, Struble KA,et al: Updated U.S. Public Health Serviceguidelines for the management ofoccupational exposures to HIV andrecommendations for postexposureprophylaxis. Infect Control HospEpidemiol 2013;34:875-892.
3. Centers for Disease Control andPrevention, National Center for InjuryPrevention and Control: 2017. Available at:https://www.cdc.gov/injury/wisqars/overview/key_data.html.
4. Wang D, Hu B, Hu C, et al: Clinicalcharacteristics of 138 hospitalized patientswith 2019 novel coronavirus-infectedpneumonia in Wuhan, China. JAMA 2020;323:1061-1069.
5. Bai Y, Yao L, Wei T, et al: Presumedasymptomatic carrier transmission ofCOVID-19 [published online ahead of printFebruary 21, 2020]. JAMA doi: 10.1001/jama.2020.2565.
6. Centers for Disease Control andPrevention: Interim infection preventionand control recommendations for patientswith suspected or confirmed coronavirusdisease 2019 (COVID-19) in healthcaresettings. 2020. Available at: https://www.cdc.gov/coronavirus/2019-ncov/hcp/infection-control-recommendations.html.
7. Ye G, Lin H, Chen L, et al: Environmentalcontamination of the SARS-CoV-2 inhealthcare premises: An urgent call forprotection for healthcare workers.medRxiv 2020. https://doi.org/10.1101/2020.03.11.20034546.
8. Chang D, Xu H, Rebaza A, Sharma L, DelaCruz CS: Protecting health-care workersfrom subclinical coronavirus infection.Lancet Respir Med 2020;8:e13.
9. Li JPO, Lam DSC, Chen Y, Ting DSW:Novel Coronavirus disease 2019 (COVID-19): The importance of recognising possibleearly ocular manifestation and usingprotective eyewear. Br J Ophthalmol 2020;104:297-298.
10. Centers for Disease Control andPrevention: Strategies to optimize thesupply of PPE and equipment. 2020.Available at: https://www.cdc.gov/coronavirus/2019-ncov/hcp/ppe-strategy/index.html. Accessed April 5, 2020.
11. Peng PWH, Wong DT, Bevan D, GardamM: Infection control and anesthesia:Lessons learned from the Toronto SARSoutbreak. Can J Anaesth 2003;50:989-997.
12. Jing C, Sun W, Huang J, Gamber M, Wu J,He G: Indirect virus transmission in clusterof COVID-19 cases, Wenzhou, China,2020. Emerging Infect Dis J 2020;26.
13. Li Q, Guan X, Wu P, et al: Earlytransmission dynamics inWuhan, China, ofnovel coronavirus-infected pneumonia. NEngl J Med 2020;382:1199-1207.
14. Chan JFW, Yuan S, Kok KH, et al: Afamilial cluster of pneumonia associatedwith the 2019 novel coronavirus indicatingperson-to-person transmission: A study of afamily cluster. Lancet 2020;395:514-523.
15. Chen N, Zhou M, Dong X, et al:Epidemiological and clinical characteristicsof 99 cases of 2019 novel coronaviruspneumonia in Wuhan, China: A descriptivestudy. Lancet 2020;395:507-513.
16. Wang W, Xu Y, Gao R, et al: Detection ofSARS-CoV-2 in different types of clinicalspecimens [published online ahead of printMarch 11, 2020]. JAMA doi: 10.1001/jama.2020.3786
17. Huang C, Wang Y, Li X, et al: Clinicalfeatures of patients infected with 2019novel coronavirus inWuhan, China. Lancet2020;395:497-506.
18. U.S. Food and Drug Administration:Important information for bloodestablishments regarding the novelcoronavirus outbreak. 2020; Available at:https://www.fda.gov/vaccines-blood-biologics/safety-availability-biologics/important-information-blood-establishments-regarding-novel-coronavirus-outbreak. Accessed March 29,2020.
19. Chang L, Yan Y, Wang L: Coronavirusdisease 2019: Coronaviruses and bloodsafety [published online ahead of print,2020 Feb 21]. Transfus Med Rev 2020;S0887-7963(20)30014-6. doi: 10.1016/j.tmrv.2020.02.003.
20. Yeh HC, Muggenburg BA, Lundgren DL,et al: Characterization of AerosolsProduced by Surgical Procedures. LovelaceBiomedical and Environmental ResearchInst., Albuquerque, NM (United States).Inhalation Toxicology Research Inst.,1994, p. Medium: ED; Size: 584 p.
21. Lockhart SL, Naidu JJ, Badh CS, DugganLV: Simulation as a tool for assessing andevolving your current personal protectiveequipment: Lessons learned during thecoronavirus disease (COVID-19)pandemic. Can J Anaesth 2020:1-2.
22. Wax RS, Christian MD: Practicalrecommendations for critical care andanesthesiology teams caring for novelcoronavirus (2019-nCoV) patients. Can JAnaesth 2020:1-9.
23. S.J.s.P.H. System: CDC Conference call.Everett, WA.
24. Centers for Disease Control andPrevention: Decontamination and reuse offiltering facepiece respirators. 2020.Available at: https://www.cdc.gov/coronavirus/2019-ncov/hcp/ppe-strategy/decontamination-reuse-respirators.html.Accessed April 7, 2020.
25. Radonovich LJ, Cheng J, Shenal BV,Hodgson M, Bender BS: Respiratortolerance in health care workers. JAMA2009;301:36-38.
26. Rebmann T, Carrico R, Wang J:Physiologic and other effects andcompliance with long-term respirator useamong medical intensive care unit nurses.Am J Infect Control 2013;41:1218-1223.
27. Fisher EM, Shaffer RE: Considerations forrecommending extended use and limitedreuse of filtering facepiece respirators inhealth care settings. J Occup Environ Hyg2014;11:D115-D128.
28. Wong J, Goh QY, Tan Z, et al: Preparingfor a COVID-19 pandemic: A review ofoperating room outbreak responsemeasures in a large tertiary hospital inSingapore [published online ahead of printMarch 11, 2020]. Can J Anaesth doi: 10.1007/s12630-020-01620-9.
29. Adams JG, Walls RM: Supporting thehealth care workforce during the COVID-19 global epidemic [published online aheadof print March 12, 2020]. JAMA doi: 10.1001/jama.2020.3972.
30. Chee VWT, Khoo MLC, Lee SF, Lai YC,Chin NM: Infection control measures foroperative procedures in severe acuterespiratory syndrome–related patients.Anesthesiology 2004;100:1394-1398.
31. KammingD,GardamM,ChungF:Anaesthesiaand SARS. Br J Anaesth 2003;90:715-718.
32. Liew MF, Siow WT, MacLaren G, See KC:Preparing for COVID-19: Early experiencefrom an intensive care unit in Singapore.Crit Care 2020;24:83.
33. Tompkins BM, Kerchberger JP: Specialarticle: Personal protective equipment forcare of pandemic influenza patients: Atraining workshop for the powered airpurifying respirator. Anesth Analg 2010;111:933-945.
34. Elias B, Bar-Yam Y: Could Air FiltrationReduce COVID-19 Severity and Spread?Cambridge, MA, New England ComplexSystems Institute, 2020.
35. Caputo KM, Byrick R, ChapmanMG,OrserBJ, Orser BA: Intubation of SARS patients:Infection and perspectives of healthcareworkers. Can J Anesth 2006;53:122-129.
36. Puja M, McAuley DF, Brown M, et al:COVID-19: consider cytokine stormsyndromes and immunosuppressio. Lancet2020;395:1033-1034.
37. Seguin A, Galicier L, Boutboul D, Lemiale V,Azoulay E: Pulmonary involvement in patientswith hemophagocytic lymphohistiocytosis.Chest 2016;149:1294-1301.
38. Gunter RL, Chouinard S, Fernandes-TaylorS, et al: Current use of telemedicine for post-discharge surgical care: A systematicreview. J Am Coll Surg 2016;222:915-927.
39. Williams AM, Bhatti UF, Alam HB,Nikolian VC: The role of telemedicine inpostoperative care. Mhealth 2018;4:11.
40. Hwa K, Wren SM: Telehealth follow-up inlieu of postoperative clinic visit for
Perioperative Considerations in Urgent Surgical Care for COVID-19
462 Journal of the American Academy of Orthopaedic Surgeons
Copyright © the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited.
ambulatory surgery: Results of a pilotprogram. JAMA Surg 2013;148:823-827.
41. Sathiyakumar V, Apfeld JC, ObremskeyWT, Thakore RV, Sethi MK: Prospectiverandomized controlled trial usingtelemedicine for follow-ups in anorthopedic trauma population: A pilotstudy. J Orthop Trauma 2015;29:e139-e145.
42. Sharareh B, Schwarzkopf R: Effectivenessof telemedical applications inpostoperative follow-up after total jointarthroplasty. J Arthroplasty 2014;29:918-922.e1.
43. Yoder LH, McFall DC, Cancio LC: Use ofthe videophone to collect quality of life datafrom burn patients. Int J Burns Trauma2012;2:135-144.
44. Finkelstein SM, MacMahon K, LindgrenBR, et al: Development of a remotemonitoring satisfaction survey and its usein a clinical trial with lung transplantrecipients. J Telemed Telecare 2012;18:42-46.
45. Rao R, Shukla BM, Saint-Cyr M, Rao M,Teotia SS: Take two and text me in themorning: Optimizing clinical time with ashort messaging system. Plast ReconstrSurg 2012;130:44-49.
46. Pirris SM, Monaco EA III, Tyler-KabaraEC: Telemedicine through the use of digitalcell phone technology in pediatricneurosurgery: A case series. Neurosurgery2010;66:999-1004.
47. Sidana A, Noori S, Patil N: Utility ofsmartphone camera in patientmanagement in urology. Can J Urol 2014;21:7449-7453.
48. Canon S, Shera A, Patel A, et al: A pilotstudy of telemedicine for post-operativeurological care in children. J TelemedTelecare 2014;20:427-430.
49. Segura-Sampedro JJ, Rivero-Belenchón I,Pino-Díaz V, et al: Feasibility and safetyof surgical wound remote follow-up bysmart phone in appendectomy: A pilotstudy. Ann Med Surg (Lond) 2017;21:58-62.
50. Gunter R, Fernandes-Taylor S, Mahnke A,et al: Evaluating patient usability of animage-based mobile health platform forpostoperative wound monitoring. JMIRMhealth Uhealth 2016;4:e113.
51. Albert MV, McCarthy C, Valentin J,Herrmann M, Kording K, Jayaraman A:Monitoring functional capability of individualswith lower limb amputations using mobilephones. PLoS One 2013;8:e65340.
52. Viers BR, Lightner DJ, Rivera ME, et al:Efficiency, satisfaction, and costs for remotevideo visits following radicalprostatectomy: A randomized controlledtrial. Eur Urol 2015;68:729-735.
53. American Academy of OrthopaedicSurgeons: Telemedicine startup checklist.Available at: https://www.aaos.org/quality/practice-management/telemedicine/. Accessed April 5, 2020.
54. Calton B, Abedini N, Fratkin M:Telemedicine in the time of coronavirus[published online ahead of print March 31,2020]. J Pain Symptom Manage doi: 10.1016/j.jpainsymman.2020.03.019.
55. Phan LT, Maita D, Mortiz DC, et al:Personal protective equipment doffingpractices of healthcare workers. J OccupEnviron Hyg 2019;16:575-581.
56. John A, Tomas ME, Cadnum JL, et al: Arehealth care personnel trained in correct useof personal protective equipment? Am JInfect Control 2016;44:840-842.
57. Vortman R: Using simulation-basededucation to improve team communicationduring a massive transfusion protocol in theOR. AORN J 2020;111:393-400.
Mohamed E. Awad, MD, et al
June 1, 2020, Vol 28, No 11 463
Copyright © the American Academy of Orthopaedic Surgeons. Unauthorized reproduction of this article is prohibited.