Embed Size (px)
Citation preview
Long Head of the BicepsTendinopathy: Diagnosis andManagement
Abstract
Tendinopathy of the long head of the biceps brachii encompassesa spectrum of pathology ranging from inflammatory tendinitis todegenerative tendinosis. Disorders of the long head of the bicepsoften occur in conjunction with other shoulder pathology. Athorough patient history, physical examination, and radiographicevaluation are necessary for diagnosis. Nonsurgical management,including rest, nonsteroidal anti-inflammatory drugs, physicaltherapy, and injections, is attempted first in patients with milddisease. Surgical management is indicated for refractory or severedisease. In addition to simple biceps tenotomy, a variety oftenodesis techniques has been described. Open biceps tenodesishas been used historically. However, promising results haverecently been reported with arthroscopic tenodesis.
Despite considerable researchinto the anatomy of the long
head of the biceps (LHB) brachii ten-don and the pathologic conditionsthat affect it, controversy persists inthe literature regarding the functionof the LHB and the appropriatemanagement of its disorders. Tendi-nopathy of the LHB has inflamma-tory, degenerative, overuse-related,and traumatic causes.
Tendinitis of the LHB is an inflam-matory tenosynovitis that occurs asthe tendon courses along its con-strained path within the bicipitalgroove of the humerus.1,2 Similar toother types of biceps tendinopathy,LHB tendinitis presents with anteriorshoulder pain and is often exacer-bated by overuse. Although isolatedbicipital tendinitis has been de-scribed, LHB tendinitis more com-monly presents in combination withother shoulder pathology, includingimpingement, rotator cuff disorders,
superior labrum anterior-posterior(SLAP) lesions, bursitis, and acro-mioclavicular joint disorders. Thesheath of the LHB is an extension ofthe synovium of the glenohumeraljoint and is closely associated withthe rotator cuff; thus, inflammationof one structure can lead to the de-velopment of disease in the other.3,4
Anatomy
The LHB originates at the supragle-noid tubercle and the superior gle-noid labrum. It inserts distally, alongwith the short head of the biceps,onto the radial tuberosity, with anattachment to the fascia of the me-dial forearm via the bicipital aponeu-rosis. The site of the LHB originfrom the glenoid labrum is variable;in most cases, it arises either mostlyposterior or completely posterior(55.4% and 27.7%, respectively).5
The intra-articular portion of the
Shane J. Nho, MD, MS
Eric J. Strauss, MD
Brett A. Lenart, MD
CDR Matthew T. Provencher,MD, MC, USN
Augustus D. Mazzocca, MD, MS
Nikhil N. Verma, MD
Anthony A. Romeo, MD
From the Department ofOrthopaedic Surgery, Section ofShoulder and Elbow Surgery,Division of Sports Medicine, RushUniversity Medical Center, Chicago,IL (Dr. Nho, Dr. Strauss, Dr. Lenart,Dr. Verma, and Dr. Romeo),Department of Orthopaedic Surgery,Naval Medical Center San Diego,San Diego, CA (Dr. Provencher),and New England MusculoskeletalInstitute, University of ConnecticutHealth Center, Farmington, CT(Dr. Mazzocca).
The views expressed in this articleare those of the authors and do notreflect the official policy or positionof the Department of the Navy,Department of Defense, or USGovernment.
J Am Acad Orthop Surg 2010;18:645-656
Copyright 2010 by the AmericanAcademy of Orthopaedic Surgeons.
Review Article
November 2010, Vol 18, No 11 645
LHB tendon is extrasynovial, and itobliquely spans the glenohumeraljoint anterosuperiorly, adjacent tothe rotator interval.
The bicipital groove is anhourglass-shaped corridor betweenthe greater and lesser tuberosities ofthe humeral head; this groove is nar-rowest and deepest at its mid por-tion.6 Although the contours of thetuberosities help to contain the LHBtendon within the bicipital groove,most of the restraint during tendon
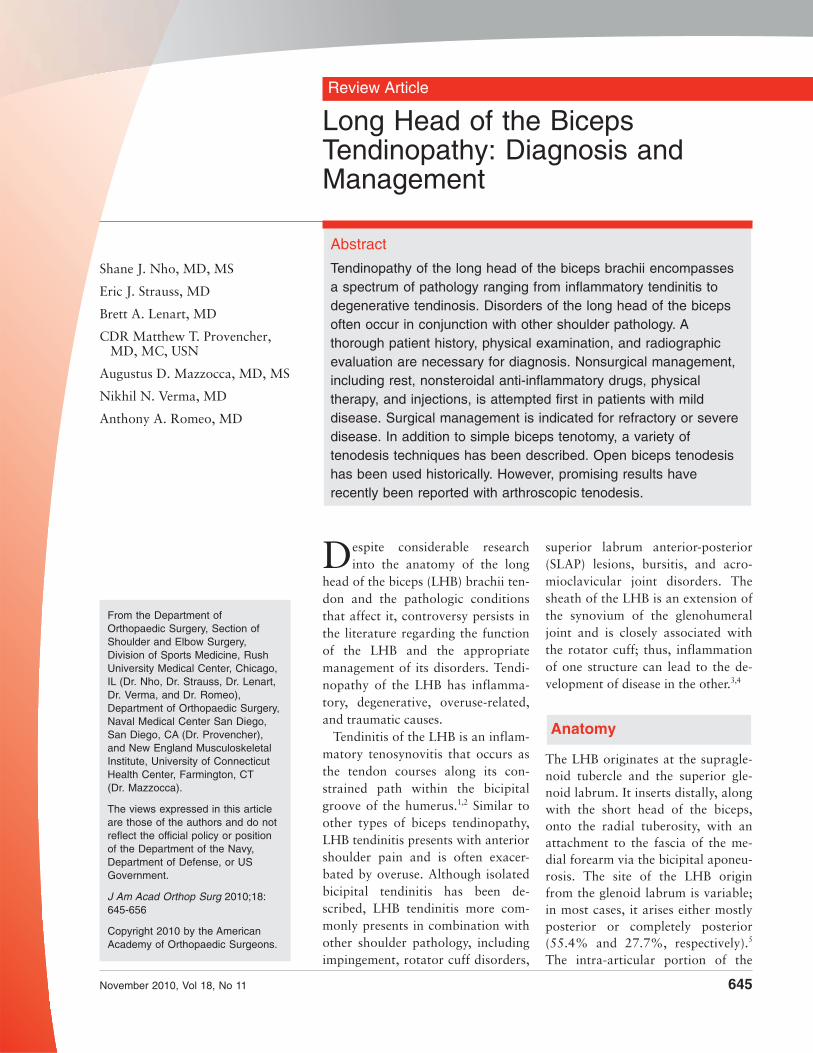
excursion is provided by the sur-rounding soft tissues. Recent clinicaland anatomic studies have attemptedto better define the soft-tissue contri-butions to biceps stability within thegroove.7,8 These studies have notedthe importance of the subscapularistendon, supraspinatus tendon, cora-cohumeral ligament (CHL), andsuperior glenohumeral ligament(SGHL), which together serve as astabilizing tendoligamentous bicepssling or pulley that maintains the bi-ceps within its groove (Figure 1).
In an anatomic study, Gleasonet al7 noted that superficial fibersfrom the subscapularis tendon con-tinued over the biceps and insertedonto the base of the greater tuberos-ity. Along with lateral fibers from thesupraspinatus tendon, these superfi-cial fibers helped to form the roof ofthe biceps sheath. The authors alsonoted that deep fibers from the sub-scapularis tendon continued alongthe bottom of the bicipital groove,thereby helping to form the floor ofthe biceps sheath. Contributions tothe biceps sling were provided by theCHL and SGHL.
The transverse humeral ligamentwas once believed to be of primaryimportance for LHB stability; how-ever, its presence and role have beenquestioned.6,7 Based on their dissec-tions, Gleason et al7 concluded that
no identifiable transverse humeralligament exists. Instead, they foundthe roof of the biceps sheath to beformed by fibers from the subscapu-laris tendon, supraspinatus tendon,and CHL. Distal to the tuberosities,the pectoralis major muscle insertionappears to play a role in stabilizingthe LHB. The falciform ligament, afibrous expansion from the sterno-costal head, has been shown to at-tach to both sides of the bicipitalgroove, enveloping the biceps.6,9
The LHB tendon is a primary paingenerator in the anterior aspect ofthe shoulder, and it has been shownto receive both sensory and sympa-thetic innervation.10 In a cadaverstudy, Alpantaki et al10 demonstratedthe presence of an asymmetricallydistributed neuronal network com-posed of thinly myelinated and un-myelinated fibers along the course ofthe tendon. This innervation wasshown to predominate in the proxi-mal area of the LHB, near its origin.
The blood supply to the LHB is de-rived primarily from branches of theanterior circumflex humeral artery,which course along the bicipitalgroove.1 Labral branches from thesuprascapular artery also may pro-vide blood supply, especially to theproximal portion of the biceps ten-don near its origin.11 However, re-cent studies have shown that there is
Dr. Nho or an immediate family member has received research or institutional support from Arthrex, DJ Orthopaedics, Linvatec, Smith& Nephew, Athletico, and MioMed. Dr. Provencher or an immediate family member serves as a board member, owner, officer, orcommittee member of the American Orthopaedic Society for Sports Medicine, Arthroscopy Association of North America, AmericanAcademy of Orthopaedic Surgeons, and Society of Military Orthopaedic Surgeons. Dr. Mazzocca or an immediate family member is amember of a speakers’ bureau or has made paid presentations on behalf of, serves as a paid consultant to or is an employee of, andhas received research or institutional support from Arthrex. Dr. Verma or an immediate family member is a member of a speakers’bureau or has made paid presentations on behalf of Smith & Nephew and Arthrosurface; serves as a paid consultant to or is anemployee of Smith & Nephew; has received research or institutional support from Smith & Nephew, DJ Orthopaedics, Arthrex, andÖssur; and has stock or stock options held in Omeros. Dr. Romeo or an immediate family member has received royalties fromArthrex; is a member of a speakers’ bureau or has made paid presentations on behalf of Arthrex and DJ Orthopaedics; serves as apaid consultant to or is an employee of Arthrex; has received research or institutional support from Arthrex, Össur, and Smith &Nephew; has received nonincome support (such as equipment or services), commercially derived honoraria, or other non-research–related funding (such as paid travel) from Arthrex and DJ Orthopaedics; and serves as a board member, owner, officer, orcommittee member of the American Orthopaedic Society for Sports Medicine, American Shoulder and Elbow Surgeons, andArthroscopy Association of North America. Neither of the following authors nor any immediate family member has received anythingof value from or owns stock in a commercial company or institution related directly or indirectly to the subject of this article:Dr. Strauss and Dr. Lenart.
Anatomic structures around thelong head of the biceps. Themusculotendinous junction lies justproximal to the inferior border ofthe pectoralis major tendon. Thedashed lines delineate underlyingstructures. CHL = coracohumeralligament
Figure 1
Long Head of the Biceps Tendinopathy: Diagnosis and Management
646 Journal of the American Academy of Orthopaedic Surgeons
a relatively avascular zone in the re-gion of the superior glenoid, whichmay contribute to the overall poorvascularity of the tendon.12 Examina-tion of the LHB within the groovecharacteristically shows vascularityon the superficial portion of the ten-don, whereas the gliding undersur-face has been noted to be avascular.
The biomechanical function of theLHB tendon is debated in the litera-ture, and its role in glenohumeral ki-nematics remains controversial. TheLHB has been described to functionas a head depressor,2,13 an anteriorstabilizer,14-16 and a posterior stabi-lizer.17 It has even been said to have norole and has been described as a vesti-gial structure.18 Cadaver biomechani-cal studies have demonstrated thatthe LHB tendon restricts glenohumeraltranslation in all directions but espe-cially in the anterior and inferior direc-tions; however, the manner in whichthe LHB tendon was loaded in thesestudies may not accurately represent itsloading in vivo.13-16 Recent electro-myographic data presented in studiesusing controlled elbow motion sug-gest little biceps activity specific tothe glenohumeral joint.4,6 However,it is possible that, in vivo, tension onthe LHB during active elbow motionmay contribute to anterior shoulderstability.4,6
Pathophysiology
Disorders of the LHB include a spec-trum of pathologic conditions, frominflammatory tendinitis to degenera-tive tendinosis. This continuum ofdisease likely arises secondary to re-petitive traction, friction, and gleno-humeral rotation, with resultantpressure and shear forces occurringon the tendon at distinct, anatomi-cally narrow sites within the longproximal tendon course.19 Thesheath of the biceps tendon is an ex-tension of the synovial lining of the
glenohumeral joint, and this sheathcan become inflamed in conjunctionwith inflammatory processes that af-fect the rotator cuff tendons. In aprospective arthroscopic evaluationof 89 patients, Neviaser et al3 corre-lated inflammatory changes in theLHB with rotator cuff tendinopathy.This association was found to be-come more pronounced with increas-ing severity of rotator cuff disease.
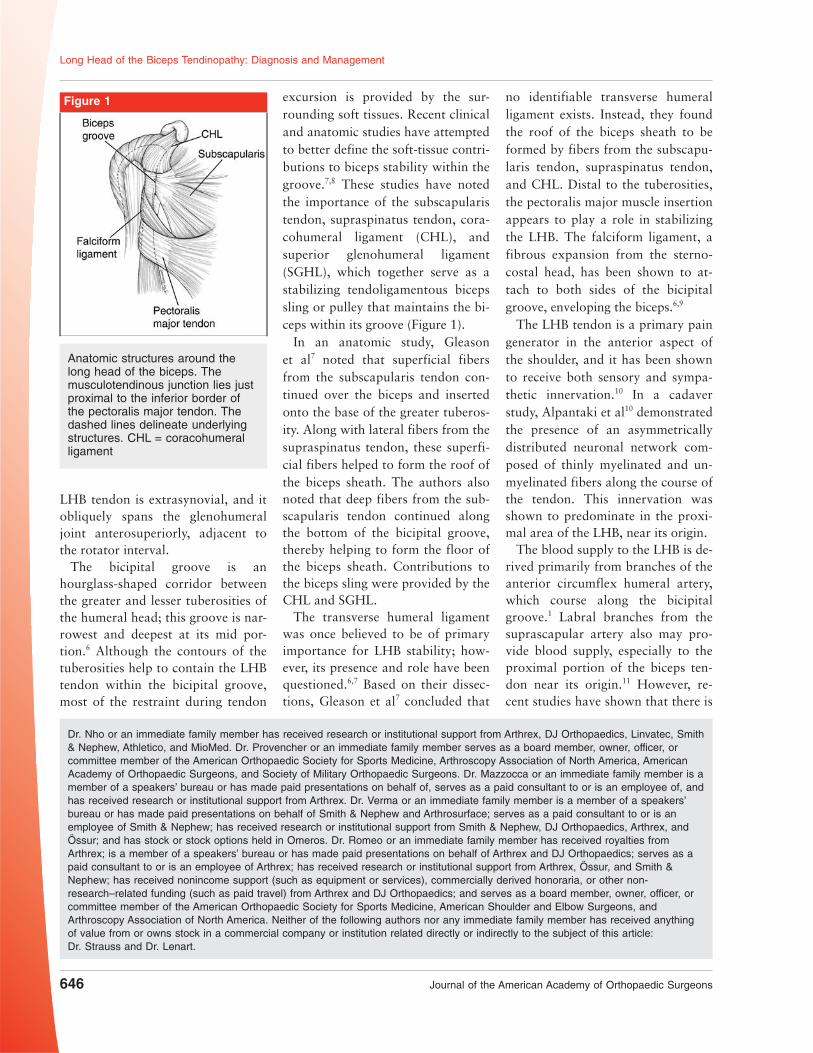
Isolated or primary bicipital tendi-nitis is seen less commonly in con-junction with LHB tendinopathythan with other shoulder pathology.However, it may occur secondary todirect or indirect trauma, underlyinginflammatory disease, and in associ-ation with tendon instability. Suchtendinitis progresses through acourse from LHB tenosynovitis toLHB tendinosis, which is marked byspecific gross and microscopic find-ings3,4,6 (Figure 2).
Clinical Evaluation andDiagnosis
HistoryMost patients report a progressivecourse of anterior shoulder pain anddeclining function as a result ofchronic overuse, typically from re-petitive overhead activities. It is diffi-cult to differentiate the variouscauses of anterior shoulder pain, anda thorough history is important toelucidate activities and positions thatare provocative (Table 1). Often, pa-tients report pain in the anteromedialaspect of the shoulder, in the regionof the bicipital groove. This painmay radiate down anteriorly to thebiceps muscle belly.
Patients with primary isolated bi-ceps tendinitis tend to be youngerand participate in overhead sportssuch as baseball, softball, and volley-
Algorithm demonstrating the pathophysiology of long head of the biceps(LHB) tendinitis.
Figure 2
Shane J. Nho, MD, MS, et al
November 2010, Vol 18, No 11 647
ball.20 Patients with symptoms re-lated to biceps instability may reportan acute event with ensuing clickingor popping in the anterior shoulder,and some patients may hear an audi-ble snap with throwing motions.20,21
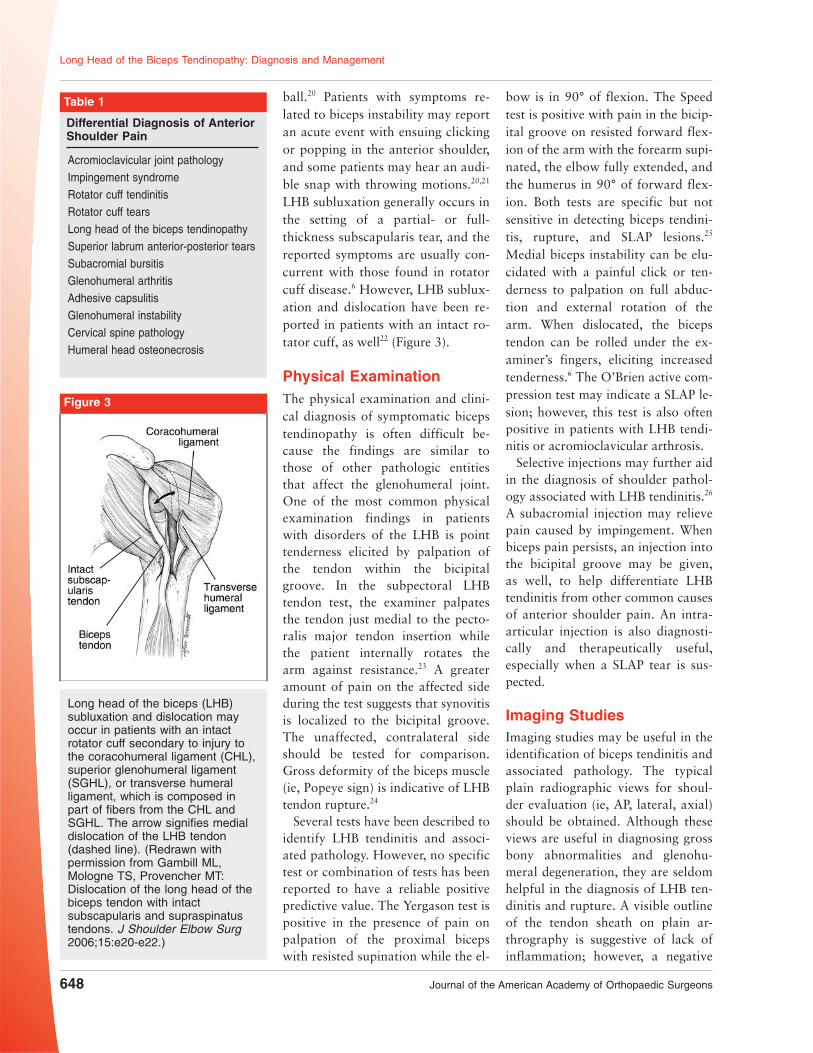
LHB subluxation generally occurs inthe setting of a partial- or full-thickness subscapularis tear, and thereported symptoms are usually con-current with those found in rotatorcuff disease.6 However, LHB sublux-ation and dislocation have been re-ported in patients with an intact ro-tator cuff, as well22 (Figure 3).
Physical ExaminationThe physical examination and clini-cal diagnosis of symptomatic bicepstendinopathy is often difficult be-cause the findings are similar tothose of other pathologic entitiesthat affect the glenohumeral joint.One of the most common physicalexamination findings in patientswith disorders of the LHB is pointtenderness elicited by palpation ofthe tendon within the bicipitalgroove. In the subpectoral LHBtendon test, the examiner palpatesthe tendon just medial to the pecto-ralis major tendon insertion whilethe patient internally rotates thearm against resistance.23 A greateramount of pain on the affected sideduring the test suggests that synovitisis localized to the bicipital groove.The unaffected, contralateral sideshould be tested for comparison.Gross deformity of the biceps muscle(ie, Popeye sign) is indicative of LHBtendon rupture.24
Several tests have been described toidentify LHB tendinitis and associ-ated pathology. However, no specifictest or combination of tests has beenreported to have a reliable positivepredictive value. The Yergason test ispositive in the presence of pain onpalpation of the proximal bicepswith resisted supination while the el-
bow is in 90° of flexion. The Speedtest is positive with pain in the bicip-ital groove on resisted forward flex-ion of the arm with the forearm supi-nated, the elbow fully extended, andthe humerus in 90° of forward flex-ion. Both tests are specific but notsensitive in detecting biceps tendini-tis, rupture, and SLAP lesions.25
Medial biceps instability can be elu-cidated with a painful click or ten-derness to palpation on full abduc-tion and external rotation of thearm. When dislocated, the bicepstendon can be rolled under the ex-aminer’s fingers, eliciting increasedtenderness.6 The O’Brien active com-pression test may indicate a SLAP le-sion; however, this test is also oftenpositive in patients with LHB tendi-nitis or acromioclavicular arthrosis.
Selective injections may further aidin the diagnosis of shoulder pathol-ogy associated with LHB tendinitis.26
A subacromial injection may relievepain caused by impingement. Whenbiceps pain persists, an injection intothe bicipital groove may be given,as well, to help differentiate LHBtendinitis from other common causesof anterior shoulder pain. An intra-articular injection is also diagnosti-cally and therapeutically useful,especially when a SLAP tear is sus-pected.
Imaging StudiesImaging studies may be useful in theidentification of biceps tendinitis andassociated pathology. The typicalplain radiographic views for shoul-der evaluation (ie, AP, lateral, axial)should be obtained. Although theseviews are useful in diagnosing grossbony abnormalities and glenohu-meral degeneration, they are seldomhelpful in the diagnosis of LHB ten-dinitis and rupture. A visible outlineof the tendon sheath on plain ar-thrography is suggestive of lack ofinflammation; however, a negative
Long head of the biceps (LHB)subluxation and dislocation mayoccur in patients with an intactrotator cuff secondary to injury tothe coracohumeral ligament (CHL),superior glenohumeral ligament(SGHL), or transverse humeralligament, which is composed inpart of fibers from the CHL andSGHL. The arrow signifies medialdislocation of the LHB tendon(dashed line). (Redrawn withpermission from Gambill ML,Mologne TS, Provencher MT:Dislocation of the long head of thebiceps tendon with intactsubscapularis and supraspinatustendons. J Shoulder Elbow Surg2006;15:e20-e22.)
Figure 3
Table 1
Differential Diagnosis of AnteriorShoulder Pain
Acromioclavicular joint pathologyImpingement syndromeRotator cuff tendinitisRotator cuff tearsLong head of the biceps tendinopathySuperior labrum anterior-posterior tearsSubacromial bursitisGlenohumeral arthritisAdhesive capsulitisGlenohumeral instabilityCervical spine pathologyHumeral head osteonecrosis
Long Head of the Biceps Tendinopathy: Diagnosis and Management
648 Journal of the American Academy of Orthopaedic Surgeons

arthrogram is seen in >30% of caseswith biceps pathology.27,28
MRI allows visualization of the bi-ceps tendon, bicipital groove, bonyosteophytes, and fluid. MRI is par-ticularly helpful in identifying otherassociated pathology. However, moststudies are neither precise nor accu-rate, and their quality is too variedto allow consistent identification ofbiceps tendinopathy. MRI has dem-onstrated poor concordance with ar-throscopic findings in the detectionof biceps pathology and poor tomoderate sensitivity for inflamma-tion, partial-thickness tear, and rup-ture.29
Magnetic resonance arthrographyis sensitive and moderately specificfor the diagnosis of biceps tendonpathology and aids in detection ofassociated pathology with tendinitisof the LHB, including rotator cufftears and SLAP lesions.30,31 On mag-netic resonance arthrography, theLHB is normally surrounded by con-trast fluid, with a shape similar tothat of a kidney bean; neither findingshould be mistaken as pathologic(Figure 4). Close inspection of ad-vanced imaging studies (ie, MRI,magnetic resonance arthrography) iswarranted in the axial plane and thesagittal oblique plane because LHBsubluxation and dislocation arecorrelated with partial- and full-thickness subscapularis tendontears.22
Ultrasound is cost-effective and ac-curate in the diagnosis of shoulderpathology, although this modality ishighly operator-dependent. Ultra-sound is highly accurate for detec-tion of full-thickness tears of therotator cuff as well as biceps disloca-tion, subluxation, and rupture; how-ever, it is less accurate in detectingpartial-thickness tears of the bicepstendon.32 To date, the role of ultra-sound in the diagnosis of biceps ten-don inflammation has not been in-vestigated.
Nonsurgical Management
LHB tendinopathy is often initiallymanaged nonsurgically, with tech-niques similar to those for the man-agement of tendon disorders. Thisincludes a period of rest and activitymodification coupled with nonsteroi-dal anti-inflammatory drugs. Physi-cal therapy is prescribed to correctthe underlying scapular rhythm andto manage concomitant shoulder dis-orders. Should this initial treatmentprove to be unsuccessful, corticoster-oid injections may be attempted, firstin the subacromial space and gleno-humeral joint, to reduce the extent ofinflammation that occurs secondaryto the commonly associated shoulderpathology seen with biceps tendini-tis. The sheath of the LHB is contin-uous with the synovium of the gleno-humeral joint, and the effects ofthese injections often extend to theLHB, leading to a reduction in in-flammation and an improvement insymptoms.26 When the biceps re-mains symptomatic, the surgeon mayinject the tendon sheath within thebicipital groove. The objective of adirect tendon sheath injection is toinfiltrate the area in and around
the groove without injecting the ten-don itself.26 Although not well-documented, intratendinous cortico-steroid injection may predispose thepatient to tendon rupture.
Nonsurgical management of symp-tomatic biceps tendinopathy is thefirst-line treatment and is often suc-cessful. However, data are lacking inthe literature to support the efficacyof this common approach.
Surgical Management
The decision to perform surgicalmanagement of biceps pathology isdependent on the clinical presenta-tion, results of provocative physicalexamination tests, presence of associ-ated shoulder pathology, and failureof nonsurgical management. Indica-tions for surgical management in-clude partial-thickness tear of theLHB tendon of >25% to 50%, me-dial LHB subluxation, and LHB sub-luxation in the setting of a tear of thesubscapularis tendon or bicepspulley/sling.4,33-36 Relative indicationsfor LHB surgery include type IVSLAP tear, symptomatic type II SLAPtear in an older patient (>50 years),failed SLAP repair, and chronic pain
A, T2-weighted axial magnetic resonance arthrogram demonstrating the longhead of the biceps (LHB) tendon lying in the bicipital groove. B, T2-weightedaxial magnetic resonance image demonstrating a torn subscapularis tendon(SSc) and medial dislocation of the LHB tendon.
Figure 4
Shane J. Nho, MD, MS, et al
November 2010, Vol 18, No 11 649
attributable to LHB tendinitis that isrefractory to nonsurgical manage-ment.1,4,37 Other indications for sur-gical management include intraoper-ative findings of an inflamed“lipstick” biceps tendon and signifi-cant hypertrophy of the tendon (ie,hourglass LHB) during diagnostic ar-throscopy in the setting of persistentsymptoms attributable to biceps pa-thology.23,38
Optimal surgical management ofLHB tendon pathology remains con-troversial.39 The two most commonlyperformed procedures are biceps te-notomy and tenodesis. Biceps tenot-omy can be performed with a rela-tively simple and reproducibletechnique that provides predictablepain relief and requires little post-operative rehabilitation. However,post-tenotomy cosmesis and fatiguediscomfort are potential problems.The Popeye deformity has been re-ported to occur in 3% to 70%of cases following tenotomy.24,39,40
However, this outcome is less likely
to be displeasing to older personsand those with obese arms. Fatiguecramping of the biceps muscle bellyhas also been reported; this occursmore commonly in younger persons,typically aged <40 years.24 In a re-view of 54 patients with biceps ten-dinitis treated with arthroscopic te-notomy, Kelly et al24 reported that38% had fatigue discomfort in thebiceps muscle after resisted elbowflexion activities. Thus, tenotomy isgenerally reserved for persons whoare older, do not work as laborers,are unlikely to be displeased withcosmesis, and are unable or unwill-ing to comply with postoperativecare following tenodesis.
The goal of biceps tenodesis is tomaintain the length-tension relation-ship of the biceps muscle, which mayprevent postoperative muscle atro-phy and which helps to maintain thenormal contour of the biceps muscle.Some authors believe that biceps te-nodesis should be used in younger,active patients with LHB pathology.
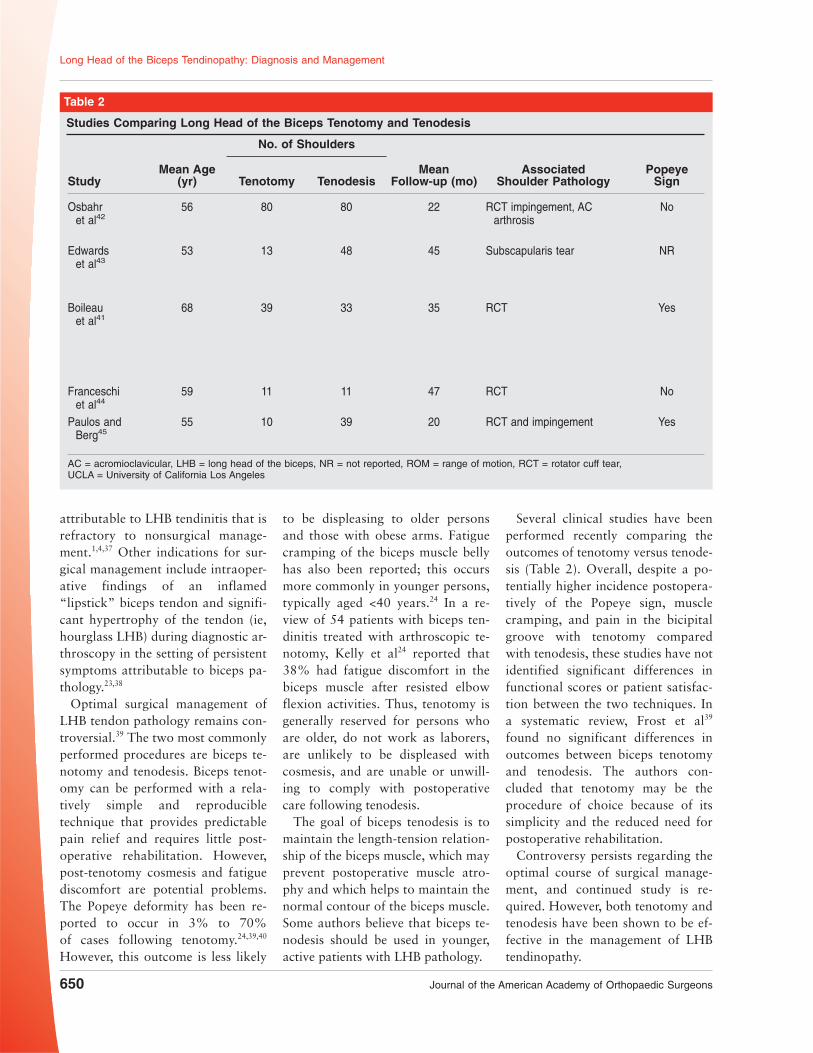
Several clinical studies have beenperformed recently comparing theoutcomes of tenotomy versus tenode-sis (Table 2). Overall, despite a po-tentially higher incidence postopera-tively of the Popeye sign, musclecramping, and pain in the bicipitalgroove with tenotomy comparedwith tenodesis, these studies have notidentified significant differences infunctional scores or patient satisfac-tion between the two techniques. Ina systematic review, Frost et al39
found no significant differences inoutcomes between biceps tenotomyand tenodesis. The authors con-cluded that tenotomy may be theprocedure of choice because of itssimplicity and the reduced need forpostoperative rehabilitation.
Controversy persists regarding theoptimal course of surgical manage-ment, and continued study is re-quired. However, both tenotomy andtenodesis have been shown to be ef-fective in the management of LHBtendinopathy.
Table 2
Studies Comparing Long Head of the Biceps Tenotomy and Tenodesis
No. of Shoulders
StudyMean Age
(yr) Tenotomy TenodesisMean
Follow-up (mo)Associated
Shoulder PathologyPopeye
Sign
Osbahret al42
56 80 80 22 RCT impingement, ACarthrosis
No
Edwardset al43
53 13 48 45 Subscapularis tear NR
Boileauet al41
68 39 33 35 RCT Yes
Franceschiet al44
59 11 11 47 RCT No
Paulos andBerg45
55 10 39 20 RCT and impingement Yes
AC = acromioclavicular, LHB = long head of the biceps, NR = not reported, ROM = range of motion, RCT = rotator cuff tear,UCLA = University of California Los Angeles
Long Head of the Biceps Tendinopathy: Diagnosis and Management
650 Journal of the American Academy of Orthopaedic Surgeons
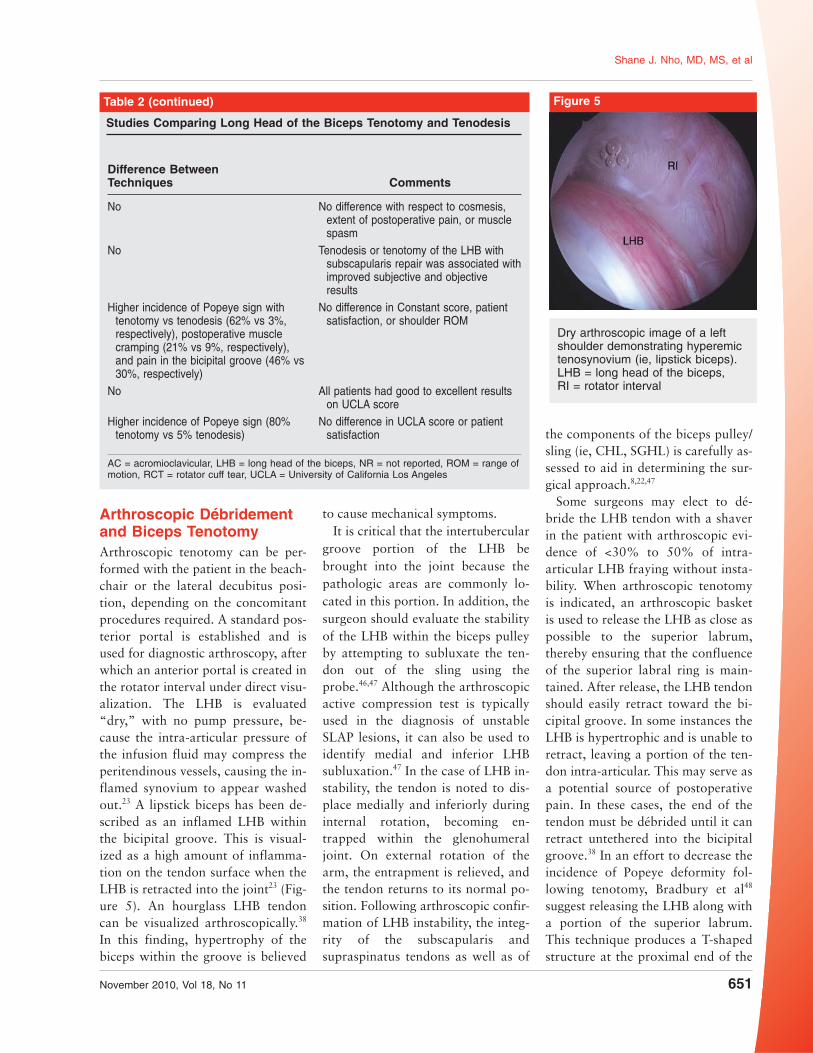
Arthroscopic Débridementand Biceps TenotomyArthroscopic tenotomy can be per-formed with the patient in the beach-chair or the lateral decubitus posi-tion, depending on the concomitantprocedures required. A standard pos-terior portal is established and isused for diagnostic arthroscopy, afterwhich an anterior portal is created inthe rotator interval under direct visu-alization. The LHB is evaluated“dry,” with no pump pressure, be-cause the intra-articular pressure ofthe infusion fluid may compress theperitendinous vessels, causing the in-flamed synovium to appear washedout.23 A lipstick biceps has been de-scribed as an inflamed LHB withinthe bicipital groove. This is visual-ized as a high amount of inflamma-tion on the tendon surface when theLHB is retracted into the joint23 (Fig-ure 5). An hourglass LHB tendoncan be visualized arthroscopically.38
In this finding, hypertrophy of thebiceps within the groove is believed
to cause mechanical symptoms.It is critical that the intertubercular
groove portion of the LHB bebrought into the joint because thepathologic areas are commonly lo-cated in this portion. In addition, thesurgeon should evaluate the stabilityof the LHB within the biceps pulleyby attempting to subluxate the ten-don out of the sling using theprobe.46,47 Although the arthroscopicactive compression test is typicallyused in the diagnosis of unstableSLAP lesions, it can also be used toidentify medial and inferior LHBsubluxation.47 In the case of LHB in-stability, the tendon is noted to dis-place medially and inferiorly duringinternal rotation, becoming en-trapped within the glenohumeraljoint. On external rotation of thearm, the entrapment is relieved, andthe tendon returns to its normal po-sition. Following arthroscopic confir-mation of LHB instability, the integ-rity of the subscapularis andsupraspinatus tendons as well as of
the components of the biceps pulley/sling (ie, CHL, SGHL) is carefully as-sessed to aid in determining the sur-gical approach.8,22,47
Some surgeons may elect to dé-bride the LHB tendon with a shaverin the patient with arthroscopic evi-dence of <30% to 50% of intra-articular LHB fraying without insta-bility. When arthroscopic tenotomyis indicated, an arthroscopic basketis used to release the LHB as close aspossible to the superior labrum,thereby ensuring that the confluenceof the superior labral ring is main-tained. After release, the LHB tendonshould easily retract toward the bi-cipital groove. In some instances theLHB is hypertrophic and is unable toretract, leaving a portion of the ten-don intra-articular. This may serve asa potential source of postoperativepain. In these cases, the end of thetendon must be débrided until it canretract untethered into the bicipitalgroove.38 In an effort to decrease theincidence of Popeye deformity fol-lowing tenotomy, Bradbury et al48
suggest releasing the LHB along witha portion of the superior labrum.This technique produces a T-shapedstructure at the proximal end of the
Dry arthroscopic image of a leftshoulder demonstrating hyperemictenosynovium (ie, lipstick biceps).LHB = long head of the biceps,RI = rotator interval
Figure 5Table 2 (continued)
Studies Comparing Long Head of the Biceps Tenotomy and Tenodesis
Difference BetweenTechniques Comments
No No difference with respect to cosmesis,extent of postoperative pain, or musclespasm
No Tenodesis or tenotomy of the LHB withsubscapularis repair was associated withimproved subjective and objectiveresults
Higher incidence of Popeye sign withtenotomy vs tenodesis (62% vs 3%,respectively), postoperative musclecramping (21% vs 9%, respectively),and pain in the bicipital groove (46% vs30%, respectively)
No difference in Constant score, patientsatisfaction, or shoulder ROM
No All patients had good to excellent resultson UCLA score
Higher incidence of Popeye sign (80%tenotomy vs 5% tenodesis)
No difference in UCLA score or patientsatisfaction
AC = acromioclavicular, LHB = long head of the biceps, NR = not reported, ROM = range ofmotion, RCT = rotator cuff tear, UCLA = University of California Los Angeles
Shane J. Nho, MD, MS, et al
November 2010, Vol 18, No 11 651

LHB, leading to entrapment at theentrance to the bicipital groove.
Gill et al40 explored biceps tenotomyas an option for the management ofprimary LHB pathology. After ar-throscopic tenotomy, patients reportedhigh rates of pain-free recovery, returnto work, and return to sports, with amean American Shoulder and ElbowSurgeons (ASES) score of 81.8. In a sim-ilar study of 40 patients with biceps ten-dinitis with or without associated shoul-der pathology, Kelly et al24 reportedthat patient satisfaction was high fol-lowing arthroscopic tenotomy (aver-age ASES score, 77.6). Although im-provement with respect to pain washigh, 70% of the patients in thisstudy displayed the classic Popeyesign at rest or during active elbowflexion, and 38% reported fatiguediscomfort after resisted elbow flex-ion.
Long Head of theBiceps TenodesisTenodesis is the preferred techniquefor managing pathology of the LHBin younger persons, athletes and la-borers, and those who wish to avoidcosmetic deformity. Tenodesis allowsfor preservation of the length-tensionrelationship of the biceps muscle,which may prevent postoperativemuscle atrophy and fatigue cramp-ing, and which helps to maintain thenormal contour of the biceps muscle.
Recent controversy surrounding bi-ceps tenodesis pertains to the loca-tion and method of fixation. Bicepstenodesis can be performed proxi-mally, with the tendon maintainedwithin the bicipital groove,41,49,50 ordistally, with the tendon removedfrom the groove.9,35,36,50-53 Advocatesof distal fixation report that remov-ing the LHB from the bicipitalgroove and excising the proximalportion of the tendon limits the po-tential for postoperative pain sec-ondary to residual tenosynovitis
within the biceps sheath.54,55 Sanderset al56 reported a 12% revision ratewith proximal tenodesis techniquesin which the LHB remained withinthe bicipital groove, compared witha 2.7% rate when the LHB was fixeddistally, outside the groove.
Proximal fixation can be performedwith an all-arthroscopic techniquewithin the glenohumeral joint or sub-deltoid space to the surrounding intactrotator cuff57 or to the conjoint ten-don,58 or just proximal within the bi-cipital groove.9,24,35,36,50,51,53 In a re-view of 43 patients treated witharthroscopic proximal tenodesis us-ing interference screw fixation, Boi-leau and Neyton52 found the powerof the biceps to be 90% that ofthe unaffected contralateral side.Elkousy et al57 reported preliminaryresults in 11 patients following ar-throscopic biceps tenodesis using apercutaneous intra-articular trans-tendon technique. All 11 patientshad biceps strength equal to that ofthe contralateral side, and all weresatisfied with their postoperativeoutcome.
Distal fixation may involve the use ofbone tunnels,55 keyholes,33 suture to abed of decorticated bicipital groove,interference screws,23,33,36,50,51,53,55,58-60
and suture anchors.24,33,55,59,60 Severalbiomechanical studies have shownthe interference screw technique tohave the highest ultimate load to fail-ure and the least amount of displace-ment on cyclic loading comparedwith suture anchor and other meth-ods of fixation.33,55,60-62
ArthroscopicBiceps TenodesisArthroscopic biceps tenodesis can beperformed in either the lateral decu-bitus or beach-chair position. Priorto tenotomy, the tendon undergoesintra-articular transfixion with a spi-nal needle at its entrance into the bi-cipital groove (Figure 6). Following
tenotomy, the arthroscope, which isplaced in the posterior portal, andthe anteromedial working cannulaare redirected into the subacromialspace. The arthroscope is then in-serted into an anterolateral portal forviewing. A probe is used to identifythe location of the bicipital groove,which typically lies just medial to thelateral aspect of the greater tuberos-ity.58
The bicipital groove is opened us-ing a cautery device, exposing theLHB. The LHB is then grasped whilethe spinal needle is removed, whichallows removal of the tendon fromthe groove (Figure 7). Using a shaveror cautery device, the bicipitalgroove is cleared of tissue in prepara-tion for drilling of the humeralsocket. Approximately 1 cm distal tothe most superior aspect of thegroove, a guidewire is drilled perpen-dicular to the humerus and parallelto the lateral border of the acromion.Using a 7- or 8-mm cannulatedreamer, the guidewire is then over-drilled to a depth of 25 mm (Figure8). An arthroscopic grasper is usedto apply tension to the LHB, and theLHB tendon is inserted into the hu-meral socket using a tendon fork. Aguidewire for the interference screwis inserted through the tendon fork,maintaining appropriate tension onthe LHB. The tendon is then fixedwithin the socket using a 9- × 25-mminterference screw with the patient’selbow in 45° to 90° of flexion (Fig-ure 9). Tension in the tenodesed LHBis assessed using the probe.58
Subpectoral OpenBiceps TenodesisSeveral open techniques have beendescribed for both proximal and dis-tal LHB tenodesis. However, we pre-fer to use a mini-open subpectoralapproach. Following release of theLHB tendon, the head of the bed islowered to 30° from the beach-chair
Long Head of the Biceps Tendinopathy: Diagnosis and Management
652 Journal of the American Academy of Orthopaedic Surgeons
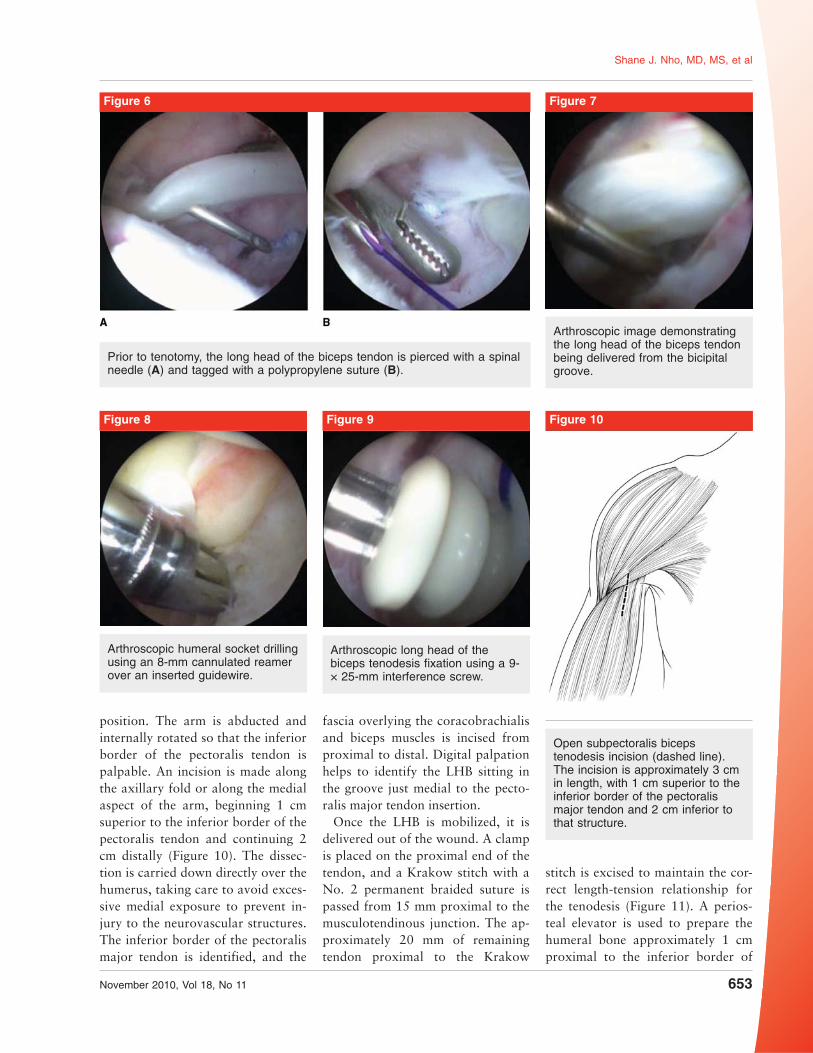
position. The arm is abducted andinternally rotated so that the inferiorborder of the pectoralis tendon ispalpable. An incision is made alongthe axillary fold or along the medialaspect of the arm, beginning 1 cmsuperior to the inferior border of thepectoralis tendon and continuing 2cm distally (Figure 10). The dissec-tion is carried down directly over thehumerus, taking care to avoid exces-sive medial exposure to prevent in-jury to the neurovascular structures.The inferior border of the pectoralismajor tendon is identified, and the
fascia overlying the coracobrachialisand biceps muscles is incised fromproximal to distal. Digital palpationhelps to identify the LHB sitting inthe groove just medial to the pecto-ralis major tendon insertion.
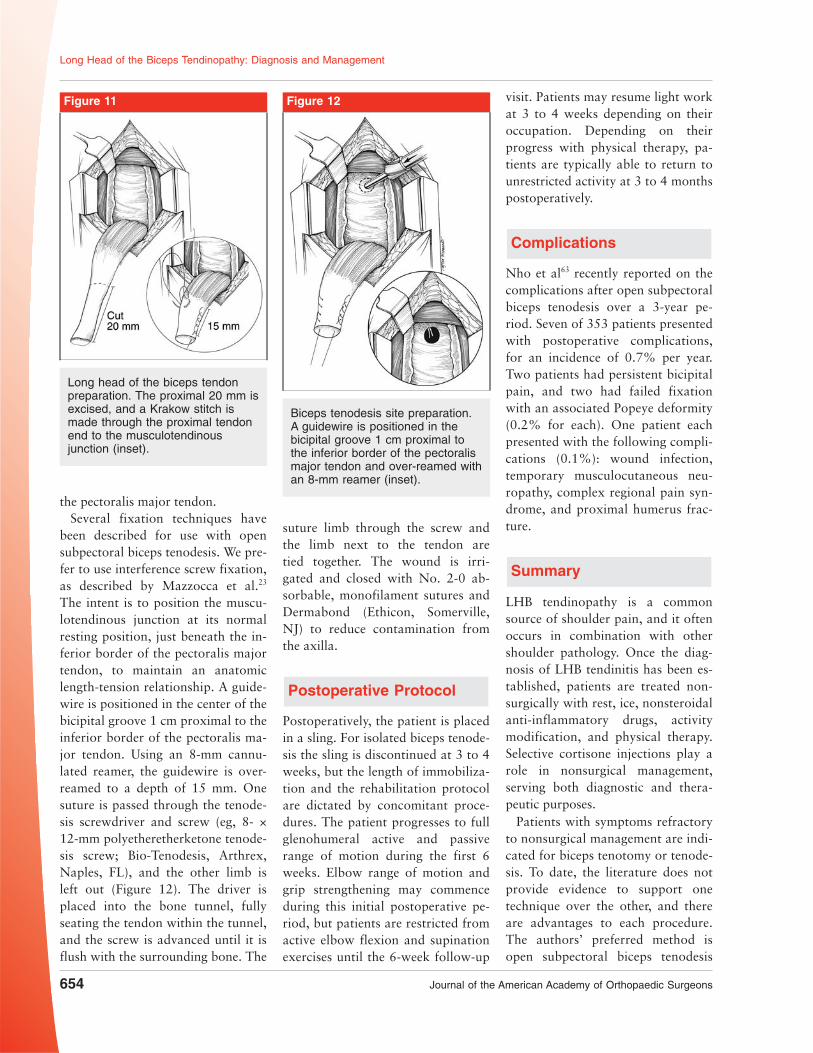
Once the LHB is mobilized, it isdelivered out of the wound. A clampis placed on the proximal end of thetendon, and a Krakow stitch with aNo. 2 permanent braided suture ispassed from 15 mm proximal to themusculotendinous junction. The ap-proximately 20 mm of remainingtendon proximal to the Krakow
stitch is excised to maintain the cor-rect length-tension relationship forthe tenodesis (Figure 11). A perios-teal elevator is used to prepare thehumeral bone approximately 1 cmproximal to the inferior border of
Prior to tenotomy, the long head of the biceps tendon is pierced with a spinalneedle (A) and tagged with a polypropylene suture (B).
Figure 6
Arthroscopic image demonstratingthe long head of the biceps tendonbeing delivered from the bicipitalgroove.
Figure 7
Open subpectoralis bicepstenodesis incision (dashed line).The incision is approximately 3 cmin length, with 1 cm superior to theinferior border of the pectoralismajor tendon and 2 cm inferior tothat structure.
Figure 10
Arthroscopic humeral socket drillingusing an 8-mm cannulated reamerover an inserted guidewire.
Figure 8
Arthroscopic long head of thebiceps tenodesis fixation using a 9-× 25-mm interference screw.
Figure 9
Shane J. Nho, MD, MS, et al
November 2010, Vol 18, No 11 653
the pectoralis major tendon.Several fixation techniques have
been described for use with opensubpectoral biceps tenodesis. We pre-fer to use interference screw fixation,as described by Mazzocca et al.23
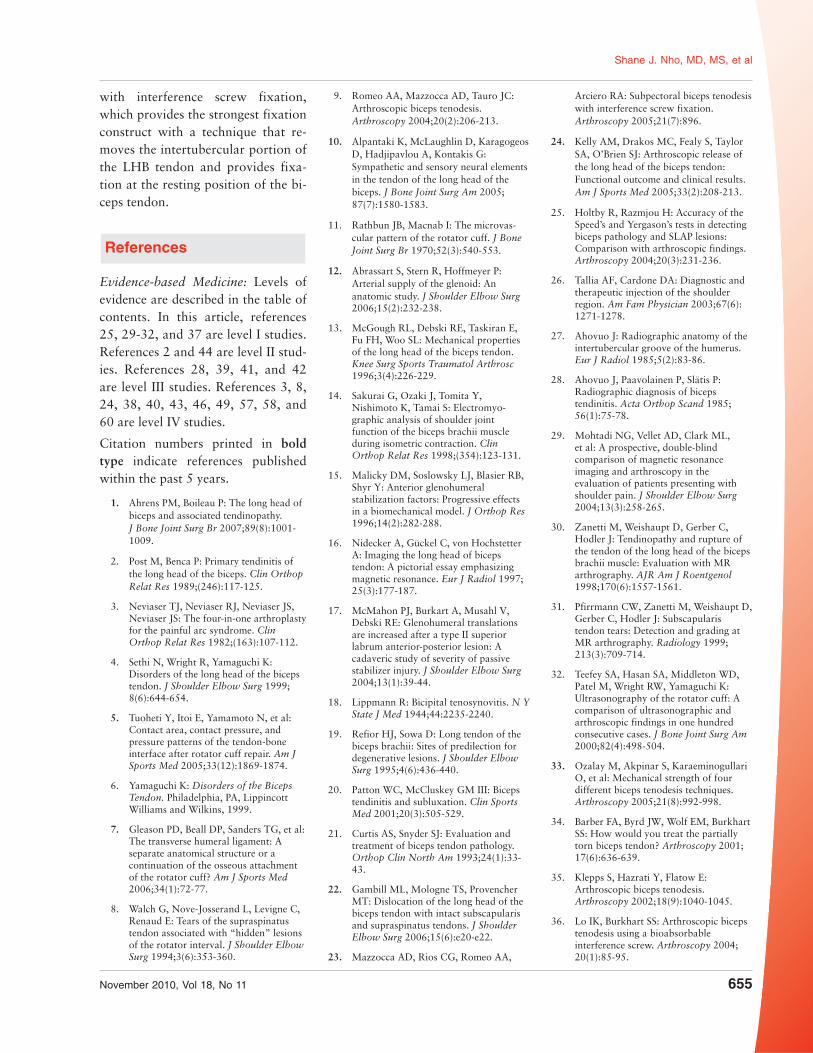
The intent is to position the muscu-lotendinous junction at its normalresting position, just beneath the in-ferior border of the pectoralis majortendon, to maintain an anatomiclength-tension relationship. A guide-wire is positioned in the center of thebicipital groove 1 cm proximal to theinferior border of the pectoralis ma-jor tendon. Using an 8-mm cannu-lated reamer, the guidewire is over-reamed to a depth of 15 mm. Onesuture is passed through the tenode-sis screwdriver and screw (eg, 8- ×12-mm polyetheretherketone tenode-sis screw; Bio-Tenodesis, Arthrex,Naples, FL), and the other limb isleft out (Figure 12). The driver isplaced into the bone tunnel, fullyseating the tendon within the tunnel,and the screw is advanced until it isflush with the surrounding bone. The
suture limb through the screw andthe limb next to the tendon aretied together. The wound is irri-gated and closed with No. 2-0 ab-sorbable, monofilament sutures andDermabond (Ethicon, Somerville,NJ) to reduce contamination fromthe axilla.
Postoperative Protocol
Postoperatively, the patient is placedin a sling. For isolated biceps tenode-sis the sling is discontinued at 3 to 4weeks, but the length of immobiliza-tion and the rehabilitation protocolare dictated by concomitant proce-dures. The patient progresses to fullglenohumeral active and passiverange of motion during the first 6weeks. Elbow range of motion andgrip strengthening may commenceduring this initial postoperative pe-riod, but patients are restricted fromactive elbow flexion and supinationexercises until the 6-week follow-up
visit. Patients may resume light workat 3 to 4 weeks depending on theiroccupation. Depending on theirprogress with physical therapy, pa-tients are typically able to return tounrestricted activity at 3 to 4 monthspostoperatively.
Complications
Nho et al63 recently reported on thecomplications after open subpectoralbiceps tenodesis over a 3-year pe-riod. Seven of 353 patients presentedwith postoperative complications,for an incidence of 0.7% per year.Two patients had persistent bicipitalpain, and two had failed fixationwith an associated Popeye deformity(0.2% for each). One patient eachpresented with the following compli-cations (0.1%): wound infection,temporary musculocutaneous neu-ropathy, complex regional pain syn-drome, and proximal humerus frac-ture.
Summary
LHB tendinopathy is a commonsource of shoulder pain, and it oftenoccurs in combination with othershoulder pathology. Once the diag-nosis of LHB tendinitis has been es-tablished, patients are treated non-surgically with rest, ice, nonsteroidalanti-inflammatory drugs, activitymodification, and physical therapy.Selective cortisone injections play arole in nonsurgical management,serving both diagnostic and thera-peutic purposes.
Patients with symptoms refractoryto nonsurgical management are indi-cated for biceps tenotomy or tenode-sis. To date, the literature does notprovide evidence to support onetechnique over the other, and thereare advantages to each procedure.The authors’ preferred method isopen subpectoral biceps tenodesis
Long head of the biceps tendonpreparation. The proximal 20 mm isexcised, and a Krakow stitch ismade through the proximal tendonend to the musculotendinousjunction (inset).
Figure 11
Biceps tenodesis site preparation.A guidewire is positioned in thebicipital groove 1 cm proximal tothe inferior border of the pectoralismajor tendon and over-reamed withan 8-mm reamer (inset).
Figure 12
Long Head of the Biceps Tendinopathy: Diagnosis and Management
654 Journal of the American Academy of Orthopaedic Surgeons
with interference screw fixation,which provides the strongest fixationconstruct with a technique that re-moves the intertubercular portion ofthe LHB tendon and provides fixa-tion at the resting position of the bi-ceps tendon.
References
Evidence-based Medicine: Levels ofevidence are described in the table ofcontents. In this article, references25, 29-32, and 37 are level I studies.References 2 and 44 are level II stud-ies. References 28, 39, 41, and 42are level III studies. References 3, 8,24, 38, 40, 43, 46, 49, 57, 58, and60 are level IV studies.
Citation numbers printed in boldtype indicate references publishedwithin the past 5 years.
1. Ahrens PM, Boileau P: The long head ofbiceps and associated tendinopathy.J Bone Joint Surg Br 2007;89(8):1001-1009.
2. Post M, Benca P: Primary tendinitis ofthe long head of the biceps. Clin OrthopRelat Res 1989;(246):117-125.
3. Neviaser TJ, Neviaser RJ, Neviaser JS,Neviaser JS: The four-in-one arthroplastyfor the painful arc syndrome. ClinOrthop Relat Res 1982;(163):107-112.
4. Sethi N, Wright R, Yamaguchi K:Disorders of the long head of the bicepstendon. J Shoulder Elbow Surg 1999;8(6):644-654.
5. Tuoheti Y, Itoi E, Yamamoto N, et al:Contact area, contact pressure, andpressure patterns of the tendon-boneinterface after rotator cuff repair. Am JSports Med 2005;33(12):1869-1874.
6. Yamaguchi K: Disorders of the BicepsTendon. Philadelphia, PA, LippincottWilliams and Wilkins, 1999.
7. Gleason PD, Beall DP, Sanders TG, et al:The transverse humeral ligament: Aseparate anatomical structure or acontinuation of the osseous attachmentof the rotator cuff? Am J Sports Med2006;34(1):72-77.
8. Walch G, Nove-Josserand L, Levigne C,Renaud E: Tears of the supraspinatustendon associated with “hidden” lesionsof the rotator interval. J Shoulder ElbowSurg 1994;3(6):353-360.
9. Romeo AA, Mazzocca AD, Tauro JC:Arthroscopic biceps tenodesis.Arthroscopy 2004;20(2):206-213.
10. Alpantaki K, McLaughlin D, KaragogeosD, Hadjipavlou A, Kontakis G:Sympathetic and sensory neural elementsin the tendon of the long head of thebiceps. J Bone Joint Surg Am 2005;87(7):1580-1583.
11. Rathbun JB, Macnab I: The microvas-cular pattern of the rotator cuff. J BoneJoint Surg Br 1970;52(3):540-553.
12. Abrassart S, Stern R, Hoffmeyer P:Arterial supply of the glenoid: Ananatomic study. J Shoulder Elbow Surg2006;15(2):232-238.
13. McGough RL, Debski RE, Taskiran E,Fu FH, Woo SL: Mechanical propertiesof the long head of the biceps tendon.Knee Surg Sports Traumatol Arthrosc1996;3(4):226-229.
14. Sakurai G, Ozaki J, Tomita Y,Nishimoto K, Tamai S: Electromyo-graphic analysis of shoulder jointfunction of the biceps brachii muscleduring isometric contraction. ClinOrthop Relat Res 1998;(354):123-131.
15. Malicky DM, Soslowsky LJ, Blasier RB,Shyr Y: Anterior glenohumeralstabilization factors: Progressive effectsin a biomechanical model. J Orthop Res1996;14(2):282-288.
16. Nidecker A, Gückel C, von HochstetterA: Imaging the long head of bicepstendon: A pictorial essay emphasizingmagnetic resonance. Eur J Radiol 1997;25(3):177-187.
17. McMahon PJ, Burkart A, Musahl V,Debski RE: Glenohumeral translationsare increased after a type II superiorlabrum anterior-posterior lesion: Acadaveric study of severity of passivestabilizer injury. J Shoulder Elbow Surg2004;13(1):39-44.
18. Lippmann R: Bicipital tenosynovitis. N YState J Med 1944;44:2235-2240.
19. Refior HJ, Sowa D: Long tendon of thebiceps brachii: Sites of predilection fordegenerative lesions. J Shoulder ElbowSurg 1995;4(6):436-440.
20. Patton WC, McCluskey GM III: Bicepstendinitis and subluxation. Clin SportsMed 2001;20(3):505-529.
21. Curtis AS, Snyder SJ: Evaluation andtreatment of biceps tendon pathology.Orthop Clin North Am 1993;24(1):33-43.
22. Gambill ML, Mologne TS, ProvencherMT: Dislocation of the long head of thebiceps tendon with intact subscapularisand supraspinatus tendons. J ShoulderElbow Surg 2006;15(6):e20-e22.
23. Mazzocca AD, Rios CG, Romeo AA,
Arciero RA: Subpectoral biceps tenodesiswith interference screw fixation.Arthroscopy 2005;21(7):896.
24. Kelly AM, Drakos MC, Fealy S, TaylorSA, O’Brien SJ: Arthroscopic release ofthe long head of the biceps tendon:Functional outcome and clinical results.Am J Sports Med 2005;33(2):208-213.
25. Holtby R, Razmjou H: Accuracy of theSpeed’s and Yergason’s tests in detectingbiceps pathology and SLAP lesions:Comparison with arthroscopic findings.Arthroscopy 2004;20(3):231-236.
26. Tallia AF, Cardone DA: Diagnostic andtherapeutic injection of the shoulderregion. Am Fam Physician 2003;67(6):1271-1278.
27. Ahovuo J: Radiographic anatomy of theintertubercular groove of the humerus.Eur J Radiol 1985;5(2):83-86.
28. Ahovuo J, Paavolainen P, Slätis P:Radiographic diagnosis of bicepstendinitis. Acta Orthop Scand 1985;56(1):75-78.
29. Mohtadi NG, Vellet AD, Clark ML,et al: A prospective, double-blindcomparison of magnetic resonanceimaging and arthroscopy in theevaluation of patients presenting withshoulder pain. J Shoulder Elbow Surg2004;13(3):258-265.
30. Zanetti M, Weishaupt D, Gerber C,Hodler J: Tendinopathy and rupture ofthe tendon of the long head of the bicepsbrachii muscle: Evaluation with MRarthrography. AJR Am J Roentgenol1998;170(6):1557-1561.
31. Pfirrmann CW, Zanetti M, Weishaupt D,Gerber C, Hodler J: Subscapularistendon tears: Detection and grading atMR arthrography. Radiology 1999;213(3):709-714.
32. Teefey SA, Hasan SA, Middleton WD,Patel M, Wright RW, Yamaguchi K:Ultrasonography of the rotator cuff: Acomparison of ultrasonographic andarthroscopic findings in one hundredconsecutive cases. J Bone Joint Surg Am2000;82(4):498-504.
33. Ozalay M, Akpinar S, KaraeminogullariO, et al: Mechanical strength of fourdifferent biceps tenodesis techniques.Arthroscopy 2005;21(8):992-998.
34. Barber FA, Byrd JW, Wolf EM, BurkhartSS: How would you treat the partiallytorn biceps tendon? Arthroscopy 2001;17(6):636-639.
35. Klepps S, Hazrati Y, Flatow E:Arthroscopic biceps tenodesis.Arthroscopy 2002;18(9):1040-1045.
36. Lo IK, Burkhart SS: Arthroscopic bicepstenodesis using a bioabsorbableinterference screw. Arthroscopy 2004;20(1):85-95.
Shane J. Nho, MD, MS, et al
November 2010, Vol 18, No 11 655
37. Franceschi F, Longo UG, Ruzzini L,Rizzello G, Maffulli N, Denaro V: Noadvantages in repairing a type II superiorlabrum anterior and posterior (SLAP)lesion when associated with rotator cuffrepair in patients over age 50: Arandomized controlled trial. Am J SportsMed 2008;36(2):247-253.
38. Boileau P, Ahrens PM, Hatzidakis AM:Entrapment of the long head of thebiceps tendon: The hourglass biceps. Acause of pain and locking of theshoulder. J Shoulder Elbow Surg 2004;13(3):249-257.
39. Frost A, Zafar MS, Maffulli N:Tenotomy versus tenodesis in themanagement of pathologic lesions of thetendon of the long head of the bicepsbrachii. Am J Sports Med 2009;37(4):828-833.
40. Gill TJ, McIrvin E, Mair SD, HawkinsRJ: Results of biceps tenotomy fortreatment of pathology of the long headof the biceps brachii. J Shoulder ElbowSurg 2001;10(3):247-249.
41. Boileau P, Baqué F, Valerio L, Ahrens P,Chuinard C, Trojani C: Isolatedarthroscopic biceps tenotomy ortenodesis improves symptoms in patientswith massive irreparable rotator cufftears. J Bone Joint Surg Am 2007;89(4):747-757.
42. Osbahr DC, Diamond AB, Speer KP:The cosmetic appearance of the bicepsmuscle after long-head tenotomy versustenodesis. Arthroscopy 2002;18(5):483-487.
43. Edwards TB, Walch G, Sirveaux F, et al:Repair of tears of the subscapularis:Surgical technique. J Bone Joint Surg Am2006;88(suppl 1 pt 1):1-10.
44. Franceschi F, Longo UG, Ruzzini L,Papalia R, Rizzello G, Denaro V: Todetach the long head of the bicepstendon after tenodesis or not: Outcomeanalysis at the 4-year follow-up of twodifferent techniques. Int Orthop 2007;31(4):537-545.
45. Paulos LE, Berg T: A novel approach tobiceps tenodesis. Operative Techniquesin Sports Medicine 2007;15(1):27-34.
46. Bennett WF: Arthroscopic repair ofanterosuperior (supraspinatus/subscapularis) rotator cuff tears: Aprospective cohort with 2- to 4-yearfollow-up. Classification of bicepssubluxation/instability. Arthroscopy2003;19(1):21-33.
47. Verma NN, Drakos M, O’Brien SJ: Thearthroscopic active compression test.Arthroscopy 2005;21(5):634.
48. Bradbury T, Dunn WR, Kuhn JE:Preventing the popeye deformity afterrelease of the long head of the bicepstendon: An alternative technique andbiomechanical evaluation. Arthroscopy2008;24(10):1099-1102.
49. Becker DA, Cofield RH: Tenodesis of thelong head of the biceps brachii forchronic bicipital tendinitis: Long-termresults. J Bone Joint Surg Am 1989;71(3):376-381.
50. Richards DP, Burkhart SS: Arthroscopic-assisted biceps tenodesis for ruptures ofthe long head of biceps brachii: Thecobra procedure. Arthroscopy 2004;20(suppl 2):201-207.
51. Kim SH, Yoo JC: Arthroscopic bicepstenodesis using interference screw: End-tunnel technique. Arthroscopy 2005;21(11):1405.
52. Boileau P, Neyton L: Arthroscopictenodesis for lesions of the long head ofthe biceps. Oper Orthop Traumatol2005;17(6):601-623.
53. Gartsman GM, Hammerman SM:Arthroscopic biceps tenodesis: Operativetechnique. Arthroscopy 2000;16(5):550-552.
54. Friedman DJ, Dunn JC, Higgins LD,Warner JJ: Proximal biceps tendon:Injuries and management. Sports MedArthrosc 2008;16(3):162-169.
55. Mazzocca AD, Bicos J, Santangelo S,Romeo AA, Arciero RA: Thebiomechanical evaluation of fourfixation techniques for proximal bicepstenodesis. Arthroscopy 2005;21(11):1296-1306.
56. Sanders BS, Warner JJ, Pennington S,Lavery KP: Biceps tendon tenodesis:Success with proximal versus distalfixation. 74th Annual MeetingProceedings. Rosemont, IL, AmericanAcademy of Orthopaedic Surgeons,2007, p 572.
57. Elkousy HA, Fluhme DJ, O’Connor DP,Rodosky MW: Arthroscopic bicepstenodesis using the percutaneous, intra-articular trans-tendon technique:Preliminary results. Orthopedics 2005;28(11):1316-1319.
58. Boileau P, Krishnan SG, Coste JS, WalchG: Arthroscopic biceps tenodesis: A newtechnique using bioabsorbableinterference screw fixation. Arthroscopy2002;18(9):1002-1012.
59. Richards DP, Burkhart SS: Abiomechanical analysis of two bicepstenodesis fixation techniques.Arthroscopy 2005;21(7):861-866.
60. Kilicoglu O, Koyuncu O, Demirhan M,et al: Time-dependent changes in failureloads of 3 biceps tenodesis techniques: Invivo study in a sheep model. Am J SportsMed 2005;33(10):1536-1544.
61. Golish SR, Caldwell PE III, Miller MD,et al: Interference screw versus sutureanchor fixation for subpectoral tenodesisof the proximal biceps tendon: Acadaveric study. Arthroscopy 2008;24(10):1103-1108.
62. Kusma M, Dienst M, Eckert J, SteimerO, Kohn D: Tenodesis of the long headof biceps brachii: Cyclic testing of fivemethods of fixation in a porcine model.J Shoulder Elbow Surg 2008;17(6):967-973.
63. Nho SJ, Reiff SN, Verma NN, SlabaughMA, Mazzocca AD, Romeo AA:Complications associated withsubpectoral biceps tenodesis: Low ratesof incidence following surgery.J Shoulder Elbow Surg 2010;19(5):764-768.
Long Head of the Biceps Tendinopathy: Diagnosis and Management
656 Journal of the American Academy of Orthopaedic Surgeons