Embed Size (px)
Citation preview
Hindawi Publishing CorporationJournal of Nutrition and MetabolismVolume 2012, Article ID 542698, 21 pagesdoi:10.1155/2012/542698
Review Article
Diet, Inflammation, and Glycemic Control in Type 2 Diabetes:An Integrative Review of the Literature
Sarah Y. Nowlin, Marilyn J. Hammer, and Gail D’Eramo Melkus
College of Nursing, New York University, 726 Broadway, 10th Floor, New York, NY 10003, USA
Correspondence should be addressed to Sarah Y. Nowlin, [email protected]
Received 9 August 2012; Accepted 19 September 2012
Academic Editor: Maria Luz Fernandez
Copyright © 2012 Sarah Y. Nowlin et al. This is an open access article distributed under the Creative Commons AttributionLicense, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properlycited.
Type 2 diabetes (T2D) is a growing national health problem affecting 35% of adults ≥20 years of age in the United States.Recently, diabetes has been categorized as an inflammatory disease, sharing many of the adverse outcomes as those reported fromcardiovascular disease. Medical nutrition therapy is recommended for the treatment of diabetes; however, these recommendationshave not been updated to target the inflammatory component, which can be affected by diet and lifestyle. To assess the current stateof evidence for which dietary programs contain the most anti-inflammatory and glycemic control properties for patients with T2D,we conducted an integrative review of the literature. A comprehensive search of the PubMed, CINAHL, Scopus, and Web of Sciencedatabases from January 2000 to May 2012 yielded 786 articles. The final 16 studies met the selection criteria including randomizedcontrol trials, quasiexperimental, or cross-sectional studies that compared varying diets and measured inflammatory markers.The Mediterranean and DASH diets along with several low-fat diets were associated with lower inflammatory markers. TheMediterranean diet demonstrated the most clinically significant reduction in glycosylated hemoglobin (HbA1c). Information onbest dietary guidelines for inflammation and glycemic control in individuals with T2D is lacking. Continued research is warranted.
1. Background
Thirty-five percent of Americans who are aged 20 yearsand older have type 2 diabetes (T2D) [1]. The etiologybehind such impressive statistics is complex but can beattributed in part to recent changes in the lifestyle choicesof Americans, including changes in habitual diet. The WhatWe Eat in America (WWEIA) report, based on data obtainedfrom the National Health and Nutrition Examination Survey(NHANES), demonstrated that grains (mainly refined) havecontributed to the bulk of the rise in caloric intake inthe US in the last 60 years [2]. Increased consumption ofadded sugars, processed grains, and saturated fat contributedto excess weight gain, which is an influential risk factorin the development of T2D [3, 4]. In fact, results fromimplementation of the Diabetes Prevention Program (DPP)illuminated that up to 58% of diabetes can be preventedthrough lifestyle changes alone, including changes in diet [5].
One underlying pathophysiological process resultingfrom poor lifestyle habits is inflammation. Inflammation is
present prior to the development of T2D and cardiovasculardisease (CVD), contributing to evidence to support the“common soil” hypothesis, which is a reference to thecommon risk factors for the development of these twodiseases [6]. CVD is one of the major complications andcauses of death in persons with T2D, supporting thishypothesis [7]. The Multi-Ethnic Study of Atherosclerosis(MESA) showed that higher levels of the inflammatorymarkers, C-reactive protein (CRP) and interleukin (IL)-6,were associated with an increased risk of developing T2D [8].Chronic inflammation in T2D initiates with states of obesity,hyperglycemia, insulin resistance, and the overexpressionof proinflammatory proteins like CRP and cytokines (IL-1β, IL-6, and tumor necrosis factor-alpha (TNF-α)) [9].These proinflammatory molecules activate the cells of innateimmunity, which cause damage to tissues in the vasculature,adipose tissue, and pancreas. Acute responses through thisproinflammatory pathway are needed for tissue damagerepair and can improve function in tissues such as thepancreas, for example; however, chronic expression can

2 Journal of Nutrition and Metabolism
lead to pathological changes which result in disease [9].These changes clinically manifest as CVD, nephropathy, andsymptomatic T2D, as the innate immune system attemptsto repair the damaged tissue. Moreover, inflammation isstimulated in times of stress, which can be induced byenvironmental, behavioral, individual, and psychosocial fac-tors [10] and diet-induced hyperglycemia and hypertriglyc-eridemia [4]. Hyperglycemia and hypertriglyceridemia aresignificant stressors that have also been shown to causechronic inflammation and contribute to the pathogenesis ofT2D [4].
2. Problem and Research Aims
Although the published literature is populated with arti-cles and systematic reviews demonstrating the relationshipbetween dietary patterns, individual dietary factors, andincidence of diabetes [11, 12], the primary literature linkinginflammation to diet and T2D is minimal. One of thefew reported areas is with the Mediterranean-style diet,which has been associated with lower inflammatory markersand decreased incidence of T2D [12, 13]. Although severalreviews have investigated the effects of diet for T2D control,few disclosed the association with underlying inflammatoryresponses. Therefore, the aim of this study was to presentan integrative review of the published literature on theassociations between dietary intake and markers of chronicinflammation in patients with T2D. This review and synthe-sis of the relevant literature seeks to answer the followingresearch question: what is the current state of the scienceregarding the association between diet and inflammation inestablished T2D?
3. The Literature Search
This review targeted adults (≥18 years) diagnosed withT2D. All studies that included a dietary intervention, eitherexclusively or as part of an intervention, were included.Eligibility criteria included diet, inflammatory markers,and T2D evaluated in randomized clinical trial (RCT),quasiexperimental, or cross-sectional studies. The followingdatabases were searched: PubMed, CINAHL, Scopus, andWeb of Science. Keywords used in the search were combina-tions of the “diet,” “chronic inflammation,” “type 2 diabetes,”“C-reactive protein,” “interleukins,” and “tumor necrosisfactor” (TNF). A health sciences librarian was consulted onthe selection of these search terms. The search was conductedon articles published between January 2000 (the year ofthe first appearance of diet, inflammation, and T2D in theliterature) and May 2012. Studies were limited to only thosewritten in the English language. Studies that focused onprevention of T2D were excluded, as they did not offerdata to assist in the exploration of how diet relates to theinflammatory process within the pathogenesis of T2D. Otherexclusion criteria were studies that focused on supplementsalone or exercise without an evaluation of, or comparison to,diet.
4. Search Outcomes
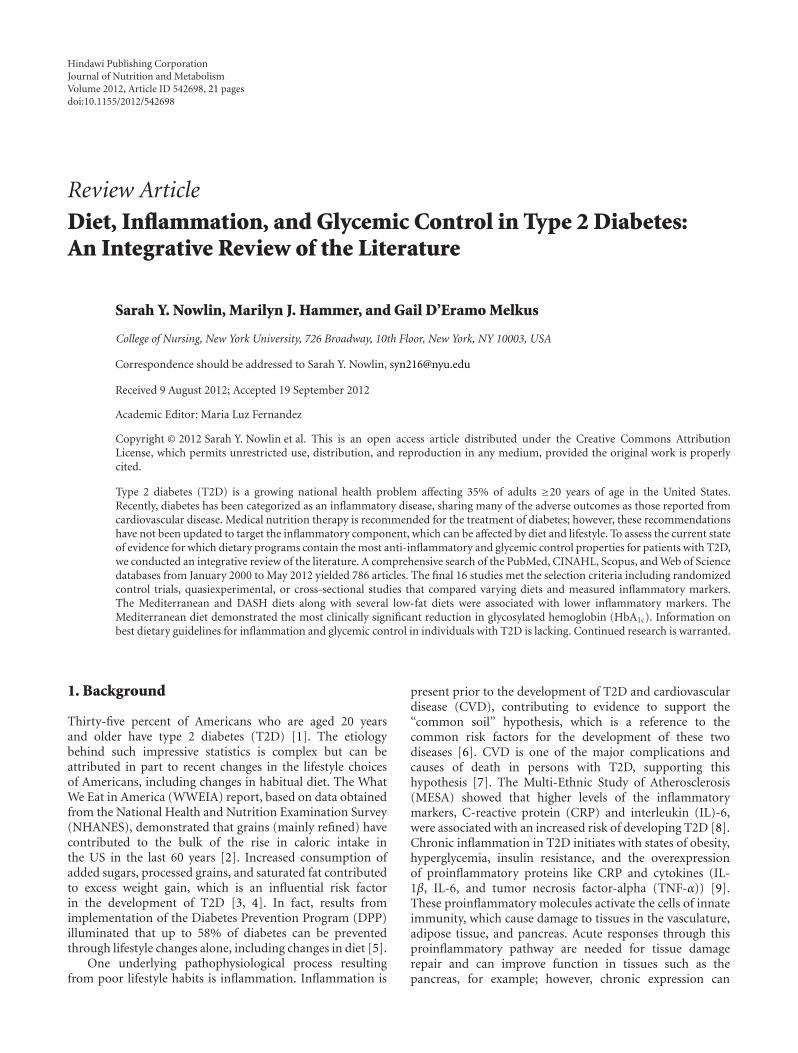
The search produced 371 studies in PubMed, 265 studies inWeb of Science, and 150 studies in CINAHL (see Figure 1).Titles and abstracts were initially screened. Among these,19 studies met the full inclusion criteria. The full textfrom these articles was carefully reviewed. Six more studieswere discarded. Two were eliminated because they includedpredominantly healthy subjects in a cross-sectional study;one was eliminated because it included exercise only, onewas eliminated due to its focus on prevention of T2D,and two were eliminated because they focused on acuteresponses to dietary interventions. Three additional studieswere identified by hand-searching reference lists of theselected articles. A final total of 16 papers were includedfor critical analysis with synthesis of findings. Experimentaland nonexperimental studies were included in the analysis.In this integrative review, two studies were cross-sectional[14, 15], two were experimental [16, 17], and twelve werequasiexperimental, as follows: three were crossover experi-mental designs [18–20], three were pretest-posttest designswith only one group [21–23], and six were pretest-posttestdesigns with two or more comparison groups [24–29]. Morethan half of the studies were international with one fromthe Middle East, one from Canada, three from Australia,and six from Europe. The other five were from the US. Allwere published in English. All subjects in the cross-sectionalstudies had a diagnosis of T2D, while several experimentalstudies utilized healthy and/or obese controls. Acceptablemeasures for inflammation included serum evaluations ofCRP, IL-6, TNF, or a combination of one or more of thesewith other markers of inflammation.
5. Methods
Each study was read twice to ensure identification of salienttopics for analysis. Three tables were created to aid synthesisof the data. Table 1 is an overview of information for broadtopics created to aid in abstracting those aspects that weredefinitive in interpreting the implications of the findings.From this table, it became clear that each study reportedinflammatory markers at different time points (e.g., somestudies did not report baseline values), which was infor-mative for the data reduction process. Quality assessmentratings were established, and each article was scored basedon these criteria (Table 2). Tables 3 and 4 contain the resultsof data abstraction and synthesis, respectively.
5.1. Quality Assessment. Articles retrieved for review wereassessed for quality of study conduct and reporting [30].Quality assessment scores were assigned based on 11 ques-tions designed to capture the essence of the study design,methods, and analyses (Table 2). The quality score for eachquestion was assigned based on how well the article fulfilledthe expectations. A score of 0 represented absence of thecriteria in question, and a score of 1 designated fulfillment ofeach criterion. These categories included aims, methods (3questions), diet (3 questions), inflammatory measures, andanalysis (2 questions). There was also one question related
Journal of Nutrition and Metabolism 3
3 articles found through searching references
16 articles included in final
synthesis
PubMed = 371 articles, CINAHL = 150 articles,and web of science= 265 articles;
titles and abstracts searched
2 articles identified by hand-searching
reference section of selected articles
19 full-text articles pulled and reviewed
6 articles discarded:
(1) included exercise,
(2) 2 did not separatehealthy/T2DM pts,
(3) incidence,
(4) not tx focused.
Figure 1: PRISMA flowchart.
to results and conclusions with a rating of 0–2, with 2 beingof highest quality, which was weighted more heavily due toits importance in interpretation of the study findings. Thehighest achievable score was 12.
5.2. Data Reduction. Studies were grouped by design methodto differentiate results sections for accurate synthesis [30].Studies were first grouped into experimental (n = 14) andcorrelational (n = 2). Studies were then further delineatedby diet categories of association with inflammation and thosewith a focus on diabetes control (glycemic control). Tables 3and 4 detail these findings.
6. Results
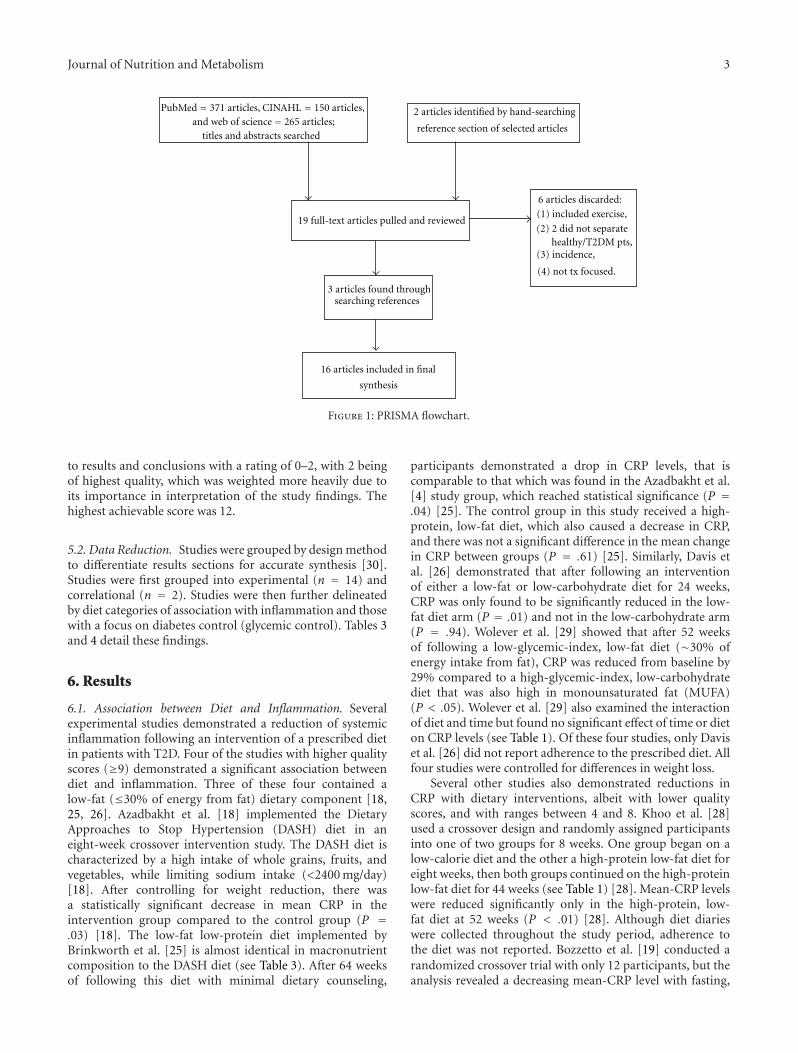
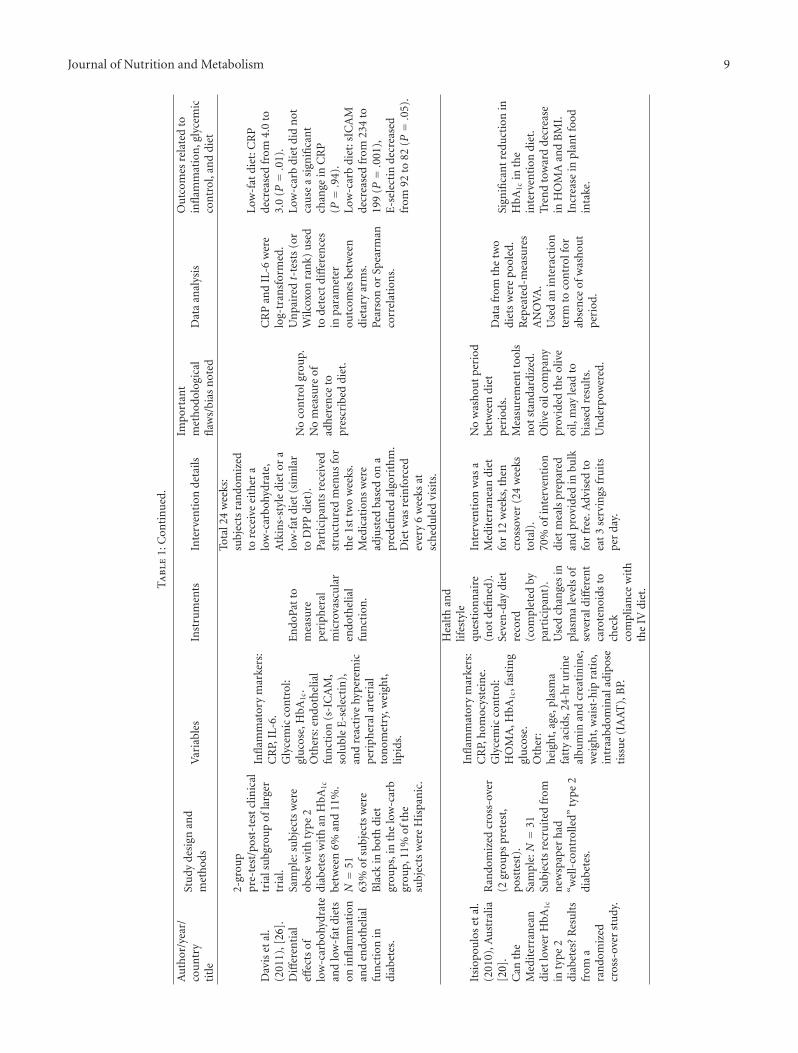
6.1. Association between Diet and Inflammation. Severalexperimental studies demonstrated a reduction of systemicinflammation following an intervention of a prescribed dietin patients with T2D. Four of the studies with higher qualityscores (≥9) demonstrated a significant association betweendiet and inflammation. Three of these four contained alow-fat (≤30% of energy from fat) dietary component [18,25, 26]. Azadbakht et al. [18] implemented the DietaryApproaches to Stop Hypertension (DASH) diet in aneight-week crossover intervention study. The DASH diet ischaracterized by a high intake of whole grains, fruits, andvegetables, while limiting sodium intake (<2400 mg/day)[18]. After controlling for weight reduction, there wasa statistically significant decrease in mean CRP in theintervention group compared to the control group (P =.03) [18]. The low-fat low-protein diet implemented byBrinkworth et al. [25] is almost identical in macronutrientcomposition to the DASH diet (see Table 3). After 64 weeksof following this diet with minimal dietary counseling,
participants demonstrated a drop in CRP levels, that iscomparable to that which was found in the Azadbakht et al.[4] study group, which reached statistical significance (P =.04) [25]. The control group in this study received a high-protein, low-fat diet, which also caused a decrease in CRP,and there was not a significant difference in the mean changein CRP between groups (P = .61) [25]. Similarly, Davis etal. [26] demonstrated that after following an interventionof either a low-fat or low-carbohydrate diet for 24 weeks,CRP was only found to be significantly reduced in the low-fat diet arm (P = .01) and not in the low-carbohydrate arm(P = .94). Wolever et al. [29] showed that after 52 weeksof following a low-glycemic-index, low-fat diet (∼30% ofenergy intake from fat), CRP was reduced from baseline by29% compared to a high-glycemic-index, low-carbohydratediet that was also high in monounsaturated fat (MUFA)(P < .05). Wolever et al. [29] also examined the interactionof diet and time but found no significant effect of time or dieton CRP levels (see Table 1). Of these four studies, only Daviset al. [26] did not report adherence to the prescribed diet. Allfour studies were controlled for differences in weight loss.
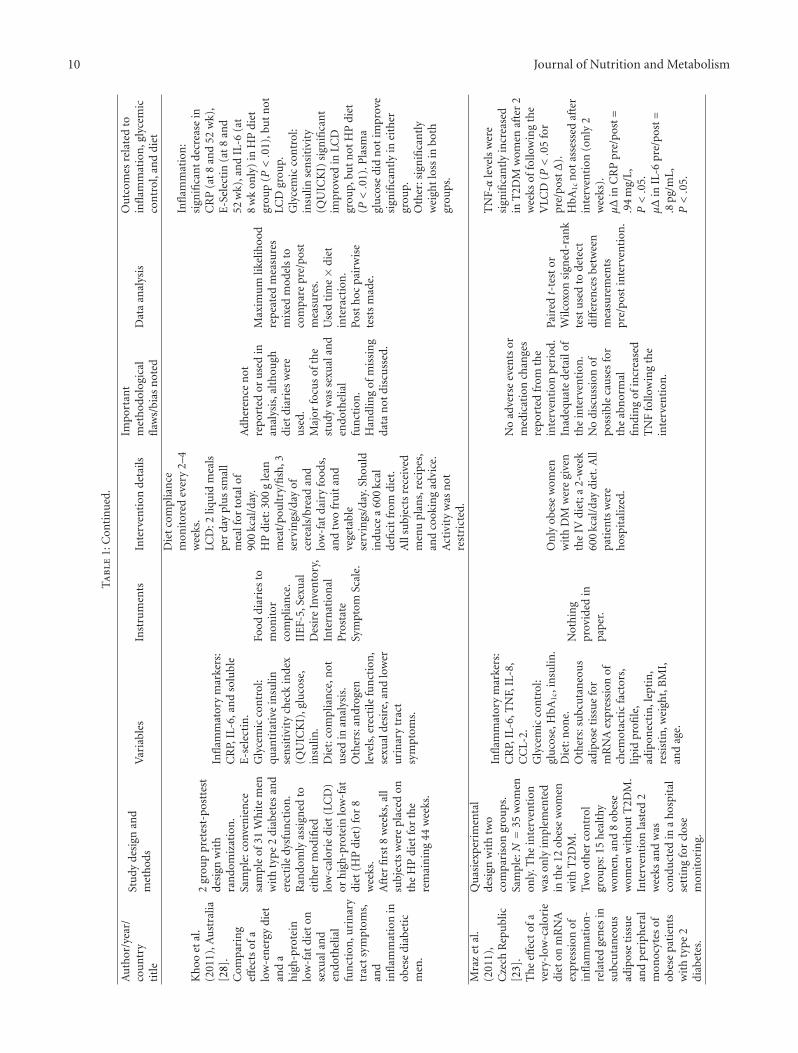
Several other studies also demonstrated reductions inCRP with dietary interventions, albeit with lower qualityscores, and with ranges between 4 and 8. Khoo et al. [28]used a crossover design and randomly assigned participantsinto one of two groups for 8 weeks. One group began on alow-calorie diet and the other a high-protein low-fat diet foreight weeks, then both groups continued on the high-proteinlow-fat diet for 44 weeks (see Table 1) [28]. Mean-CRP levelswere reduced significantly only in the high-protein, low-fat diet at 52 weeks (P < .01) [28]. Although diet diarieswere collected throughout the study period, adherence tothe diet was not reported. Bozzetto et al. [19] conducted arandomized crossover trial with only 12 participants, but theanalysis revealed a decreasing mean-CRP level with fasting,
4 Journal of Nutrition and Metabolism
Ta
ble
1:St
udy
met
hod
s,de
tails
,an
dou
tcom
es.
Au
thor
/yea
r/co
un
try
titl
e
Stu
dyde
sign
and
met
hod
sV
aria
bles
Inst
rum
ents
Inte
rven
tion
deta
ilsIm
port
ant
met
hod
olog
ical
flaw
s/bi
asn
oted
Dat
aan
alys
isO
utc
omes
rela
ted
toin
flam
mat
ion
,gly
cem
icco
ntr
ol,a
nd
diet
Bri
nkw
orth
etal
.(2
004)
,Au
stra
lia[2
5].
Lon
g-te
rmeff
ects
ofad
vice
toco
nsu
me
ah
igh
-pro
tein
,lo
w-f
atdi
etra
ther
than
aco
nven
tion
alw
eigh
t-lo
ssdi
et,
inob
ese
adu
lts
wit
hty
pe
2di
abet
es:o
ne-
year
follo
wu
pof
ara
ndo
miz
edtr
ial.
2-gr
oup
pret
est/
post
test
desi
gnw
ith
ran
dom
izat
ion
,lo
ngi
tudi
nal
follo
w-u
p.Sa
mpl
e:N=
38ob
ese
orov
erw
eigh
tad
ult
sw
ith
type
2di
abet
es.
Infl
amm
ator
ym
arke
rs:
hs-
CR
P,IL
-6,u
rin
ary
15-k
eto-
dihy
ro-P
GF.
Gly
cem
icco
ntr
ol:
glu
cose
,HbA
1c,i
nsu
lin.
Oth
ers:
body
com
posi
tion
,BP,
wei
ght,
lipid
s.
Du
alX
-ray
abso
rpti
omet
ry.
24-h
our
uri
ne
colle
ctio
nto
mea
sure
prot
ein
inta
kefr
omu
rin
ary
ure
a:c
reat
inin
era
tio.
(1)
8w
eeks
of30
%en
ergy
rest
rict
ion
,(2
)4
wee
ksof
ener
gyba
lan
ce(d
uri
ng
firs
t12
wee
ksm
etw
ith
diet
icia
nev
ery
2w
eeks
),(3
)52
-wee
km
ain
ten
ance
peri
odw
ith
min
imal
cou
nse
ling
(wei
gh-i
nev
ery
3m
onth
s).
No
con
trol
for
con
fou
ndi
ng
vari
able
s(i
.e.
diff
eren
ces
inw
eigh
tlo
ss,c
han
ges
inm
edic
atio
ns
over
the
stu
dyp
erio
d).
39%
attr
itio
nra
te,
disc
uss
edad
equ
atel
y.
Rep
eate
dm
easu
res
AN
OV
A.
Adj
ust
men
tsfo
rba
selin
eva
lues
and
body
wei
ght
wit
hA
NC
OV
A.
Reg
ress
ion
anal
ysis
for
rela
tion
ship
sbe
twee
nch
ange
sin
para
met
ers
over
tim
e.
Th
ere
was
ade
crea
sein
CR
Pfo
rbo
thgr
oups
of14
%(P=.0
4),b
ut
no
diff
eren
cebe
twee
ngr
oups
(P=.6
1).
No
diff
eren
ceov
eral
lin
glyc
emic
con
trol
at64
wee
ksfr
omba
selin
e.U
sed
uri
nar
yu
rea
:cre
atin
ine
rati
oto
dete
rmin
ead
her
ence
toth
edi
et,w
hic
hw
asad
equ
ate
(i.e
.hig
her
inh
igh
-pro
tein
diet
grou
p).
Gia
nn
opou
lou
etal
.(20
05),
U.S
.[2
7].
Eff
ects
ofdi
etan
d/or
exer
cise
onth
ead
ipoc
ytok
ine
and
infl
amm
ator
ycy
toki
ne
leve
lsof
post
men
opau
sal
wom
enw
ith
typ
e2
diab
etes
.
3-gr
oup
pret
est-
post
test
desi
gnw
ith
ran
dom
izat
ion
.1
of3
inte
rven
tion
s:(1
)on
lydi
et,(
2)on
lyex
erci
se,o
r(3
)di
etan
dex
erci
se.T
he
inte
rven
tion
last
ed14
wee
ks.
Sam
ple:N=
33po
stm
enop
ausa
l,ob
ese
wom
enw
ith
typ
e2
diab
etes
.
Infl
amm
ator
ym
arke
rs:
lept
in,C
RP,
adip
onec
tin
,TN
F-α
,an
dIL
-6.A
llm
easu
red
bybl
ood
sam
ples
.G
lyce
mic
con
trol
:H
bA1c
,fas
tin
gbl
ood
glu
cose
,in
sulin
.All
mea
sure
dby
bloo
dsa
mpl
es.
Die
t:24
hr
reca
llev
ery
two
wee
ks,b
ut
did
apo
stm
eale
valu
atio
nof
mar
kers
.O
ther
s:bo
dyco
mpo
siti
on(a
bdom
inal
fat
dist
ribu
tion
),m
etab
olic
data
,EK
G.
24h
our
reca
lls.
Exe
rcis
est
ress
test
.B
odPo
du
sed
tode
term
ine
perc
enta
geof
body
fat.
MR
Ifo
rab
dom
inal
fat
dist
ribu
tion
test
ing.
(1)
Die
ton
ly:h
igh
MU
FAFa
t40
%,
CH
O40
%,
Pro
tein
20%
,In
divi
dual
mod
ifica
tion
sm
ade
toen
ergy
inta
keba
sed
onen
ergy
expe
ndi
ture
from
exer
cise
and
met
abol
icra
te.
Init
ialn
utr
itio
nal
cou
nse
ling
con
duct
edat
the
begi
nn
ing
and
atw
eekl
yin
terv
als.
(2)
Exe
rcis
eon
ly:
60m
inw
alki
ng
3-4
tim
esp
erw
eek.
(3)
Com
bo.
Exe
rcis
ein
terv
enti
onw
as“s
upe
rvis
ed”
but
not
spec
ified
how
.Su
bjec
tsco
mpl
eted
24-h
rdi
etar
yre
calls
but
no
expl
anat
ion
give
nas
tow
hat
was
don
ew
ith
thes
e.N
om
enti
onof
wh
ere
subj
ects
cam
efr
om.
On
lyge
ner
aliz
able
topo
stm
enop
ausa
lob
ese
wom
enw
ith
typ
e2
DM
.C
RP
corr
elat
edw
ith
wei
ght,
BM
I,to
tal
body
fat
mas
s,SA
T,an
dIL
-6.
Des
crip
tive
data
:2-
way
AN
OV
Aw
ith
post
hoc
anal
ysis
wh
ere
appr
opri
ate.
Cov
aria
tes:
tota
lbod
yfa
tm
ass,
abdo
min
alfa
tdi
stri
buti
on.
For
allg
rou
ps:
CR
Pde
crea
sed
pre/
post
wit
hP<.0
1.IL
-6ch
ange
pre/
post
was
NS
for
allg
rou
ps.
HbA
1cch
ange
was
NS
for
allg
rou
ps.
TN
F-α
chan
gew
asN
Sfo
ral
lgro
ups
.

Journal of Nutrition and Metabolism 5
Ta
ble
1:C
onti
nu
ed.
Au
thor
/yea
r/co
un
try
titl
e
Stu
dyde
sign
and
met
hod
sV
aria
bles
Inst
rum
ents
Inte
rven
tion
deta
ilsIm
port
ant
met
hod
olog
ical
flaw
s/bi
asn
oted
Dat
aan
alys
isO
utc
omes
rela
ted
toin
flam
mat
ion
,gly
cem
icco
ntr
ol,a
nd
diet
Mar
fella
etal
.(2
006)
,Ita
ly[1
6].
Eff
ect
ofm
oder
ate
red
win
ein
take
onca
rdia
cpr
ogn
osis
afte
rre
cen
tac
ute
myo
card
ial
infa
rcti
onof
subj
ects
wit
hty
pe2
diab
etes
mel
litu
s.
RC
T.Sa
mpl
e:13
1pa
rtic
ipan
tsw
ith
type
2di
abet
esw
ith
rece
nt
(<2
mon
ths)
myo
card
iali
nfa
rcti
on(M
I),<
70yr
,an
dca
ndr
ink
alco
hol
.All
pati
ents
wer
etr
eate
dw
ith
insu
lin.B
asel
ine
dem
ogra
phic
sbe
twee
ngr
oups
wer
esi
mila
r.Su
bjec
tsra
ndo
miz
edto
inte
rven
tion
orco
ntr
olgr
oup
for
52w
eeks
.
Infl
amm
ator
ym
arke
rs:
TN
F-α
,IL-
6,IL
-18,
CR
P.G
lyce
mic
con
trol
:in
sulin
sen
siti
vity
(HO
MA
scor
e),i
nsu
lin,
HbA
1c.
Die
t:re
dw
ine
con
sum
ptio
n.
Oth
ers:
nit
roty
rosi
ne,
BM
I,lip
ids,
myo
card
ial
syn
chro
niz
atio
n,o
ther
mea
sure
sof
fun
ctio
nal
card
iac
outc
omes
.
24-h
rdi
etar
yre
call:
atfi
rst
visi
t.4-
day
food
diar
y:ev
ery
thre
em
onth
s.E
choc
ardi
ogra
m.
Bot
hgr
oups
advi
sed
2000
kcal
/day
diet
sim
ilar
toM
edit
erra
nea
ndi
et.
Win
egr
oup:
4-oz
.gl
ass
ofre
dw
ine
each
day.
Com
pari
son
grou
p:n
ore
dw
ine
con
sum
ptio
n.
On
ly11
5pa
tien
tsco
mpl
eted
the
stu
dy(8
died
).B
oth
grou
psgi
ven
diet
ary
advi
ce,
wh
ich
was
not
ava
riab
lein
the
anal
ysis
.
On
e-w
ayA
NO
VA
for
base
line,
then
Sch
effe’
ste
stto
com
pare
pair
sof
data
.Fo
rn
onn
orm
ally
dist
ribu
ted
data
(IL-
6,T
NFα
,IL-
18,H
OM
A,
trig
lyce
ride
s),
Wilc
oxon
’ste
stw
asu
sed.
Lin
ear
regr
essi
onu
sed
toas
sess
corr
elat
ion
s.
Sign
ifica
nt
hig
her
leve
lsof
TN
Fα,I
L-6,
IL-1
8,C
RP,
and
nit
roty
rosi
ne
(P<.0
1fo
ral
l)in
the
con
trol
grou
pth
anw
ine
grou
p.C
han
gein
HbA
1cw
asN
Sdi
ffer
ent
betw
een
grou
ps.
Wol
ever
etal
.(2
008)
,Can
ada
[29]
.T
he
Can
adia
ntr
ialo
fca
rboh
ydra
tes
indi
abet
es(C
CD
),a
1-y
con
trol
led
tria
lofl
ow-
glyc
emic
-in
dex
diet
ary
carb
ohyd
rate
inty
pe2
diab
etes
:n
oeff
ect
ongl
ycat
edh
emog
lobi
nbu
tre
duct
ion
inC
-rea
ctiv
epr
otei
n.
3-gr
oup
pre-
test
/pos
t-te
stde
sign
wit
hra
ndo
miz
atio
n.
Sam
ple:N=
162.
Subj
ects
wer
ead
ult
sag
e35
–75
y/o
wit
hty
pe
2di
abet
esan
da
BM
Iof
24–4
0.
Infl
amm
ator
ym
arke
rs:
CR
P.G
lyce
mic
con
trol
:in
sulin
sen
siti
vity
(HO
MA
scor
e),f
asti
ng
glu
cose
,fas
tin
gin
sulin
,H
bA1c
.D
iet:
mac
ron
utr
ien
tin
take
.O
ther
s:lip
idpr
ofile
,w
eigh
t,bl
ood
pres
sure
,fr
eefa
tty
acid
s.C
RP
:log
-tra
nsf
orm
ed(t
hos
ew
hos
est
atin
dose
sw
ere
chan
ged
duri
ng
the
stu
dyw
ere
not
incl
ude
din
the
anal
ysis
ofC
RP,
lipid
s,an
dlip
opro
tein
s).
3-da
yfo
oddi
ary
reco
rds
colle
cted
7ti
mes
duri
ng
the
12m
onth
per
iod
.K
eyfo
oddi
arie
sfr
om91
%of
subj
ects
.
12m
onth
sin
len
gth
.A
llsu
bjec
tsad
vise
d“h
eart
hea
lthy
”di
et.
Hig
h-G
Idi
et:a
void
low
-GI
food
s,ea
tlo
w-f
atfo
ods.
Low
-GI
diet
:ex
chan
geh
igh
-GI
food
sfo
rlo
w-G
Ifo
ods,
eat
low
-fat
food
s.Lo
w-C
HO
:dec
reas
eSF
Ain
take
,in
crea
seM
UFA
inta
ke.
Indi
vidu
aldi
etar
yco
un
selin
gpr
ovid
edat
2an
d4
wee
ks,t
hen
ever
y4
wee
ks.
No
con
trol
grou
p.
Gen
eral
linea
rm
ixed
mod
el.S
tats
CR
Pu
sed
log-
tran
sfor
med
data
pres
ente
das
mea
ns
and
CI’s
.T
ime
trea
ted
asa
regr
essi
onva
riab
le.
Mod
elco
vari
ates
:ag
e,B
MI,
sex,
and
cen
ter
that
corr
elat
edsi
gnifi
can
tly
wit
hth
ere
spon
seva
riab
le.
Tim
e×
diet
:in
tera
ctio
ns.
∗ dat
afo
rsu
bjec
tsth
atw
ere
excl
ude
dfr
oman
alys
isw
ere
incl
ude
du
pu
nti
lth
ep
oin
tth
eyw
ere
drop
ped.
Con
side
red
MA
R.
CR
Pin
low
-GI
diet
29%
low
erth
anh
igh
-GI
diet
.C
RP
was
1.95
(1.6
8,2.
27)
for
the
low
-GI
diet
,2.7
5(2
.33,
3.24
)fo
rth
eh
igh
-GI
diet
,an
d2.
35(2
.01,
2.75
)fo
rth
elo
w-C
HO
diet
(P<.0
5fo
rdi
ffer
ence
ingr
oups
).C
RP
incr
ease
dw
ith
hig
h-G
Idi
et.
HbA
1cro
sefr
om6.
1to
6.3%
,bu
tbe
twee
ngr
oup
effec
ton
HbA
1c
was
NS
from
diet
:hig
hG
IH
bA1c=
6.34±
0.05
,lo
wG
IH
bA1c=
6.34±
0.05
,low
GI
HbA
1c=
6.35±
0.05
.Si
gnifi
can
teff
ect
ofti
me
onw
eigh
t,bu
tn
otsi
gnifi
can
tly
diff
eren
tbe
twee
ndi
etgr
oups
.

6 Journal of Nutrition and Metabolism
Ta
ble
1:C
onti
nu
ed.
Au
thor
/yea
r/co
un
try
titl
e
Stu
dyde
sign
and
met
hod
sV
aria
bles
Inst
rum
ents
Inte
rven
tion
deta
ilsIm
port
ant
met
hod
olog
ical
flaw
s/bi
asn
oted
Dat
aan
alys
isO
utc
omes
rela
ted
toin
flam
mat
ion
,gly
cem
icco
ntr
ol,a
nd
diet
Bar
nar
det
al.
(200
9),U
nit
edSt
ates
[24]
.A
low
-fat
vega
ndi
etan
da
conv
enti
onal
diab
etes
diet
inth
etr
eatm
ent
ofty
pe2
diab
etes
:ara
ndo
miz
ed,
con
trol
led,
74-w
eek
clin
ical
tria
l.
2gr
oup
pret
est-
post
test
desi
gn.
Sam
ple:N=
99Su
bjec
tsw
ere
adu
lts
wit
hty
pe2
diab
etes
.(1
)V
egan
diet
.(2
)C
onve
nti
onal
AD
Adi
et(2
003
guid
elin
es).
Infl
amm
ator
ym
arke
rs:
CR
P.G
lyce
mic
con
trol
:H
bA1c
,fas
tin
gpl
asm
agl
uco
se.
Oth
ers:
lipid
profi
le,
wei
ght,
BM
I,w
aist
circ
um
fere
nce
,al
bum
in,b
lood
pres
sure
.D
ieta
ryad
her
ence
:ve
gan
-no
anim
alpr
odu
cts
in24
-hre
calls
,low
fat,
low
chol
este
rol
conv
enti
onal
-fol
low
ing
pres
crib
eden
ergy
rest
rict
ion
s,lo
wSF
A.
Bot
hgr
oups
:att
ende
dat
leas
t10
ofth
e22
wee
kly
diet
ary
info
sess
ion
s.
24h
our
reca
lls×7
.3-
day
diet
ary
reco
rd×4
.Pe
dom
eter
.B
ouch
ard
3-da
yph
ysic
alac
tivi
tyre
cord
.
Init
ial1
-hr
mee
tin
gw
ith
diet
icia
nfo
rea
chgr
oup.
Th
en,2
2w
eekl
ygr
oup
sess
ion
ssp
ecifi
cto
grou
p.O
ptio
nal
sess
ion
sev
ery
two
wee
ksfo
rth
ere
mai
nin
g52
wee
ks.
Med
icat
ion
sw
ere
adju
sted
for
safe
tyby
anen
docr
inol
ogis
t.
Not
alla
nal
yses
wer
epe
rfor
med
only
usi
ng
thos
epa
rtic
ipan
tsw
ith
good
adh
eren
ce.
Goo
dad
her
ence
not
defi
ned
.O
nly
CR
Pm
easu
red,
was
not
apr
imar
yfo
cus
ofth
est
udy
.
Rep
eate
dm
easu
res
AN
OV
Afo
rH
bA1c
(as
ITT
)u
sin
gti
me,
diet
grou
p,an
din
tera
ctio
nbe
twee
nti
me×
diet
wit
hH
bA1c
asD
V.
Bet
wee
nsu
bjec
tt-
test
sfo
ral
lDV
sto
dete
ctsi
gnifi
can
tch
ange
sfr
omba
selin
eto
74w
eeks
(or
un
til
last
mea
sure
men
t)an
dpa
ired
-com
pari
son
t-te
sts.
Aft
erad
just
men
tfo
rm
edic
atio
nch
ange
s,LD
Lan
dn
on-H
DL
chol
este
rolv
alu
esde
crea
sed,
and
mor
eso
inth
eve
gan
grou
p.C
RP
decr
ease
dsi
gnifi
can
tly
inbo
thgr
oups
,bu
tn
odi
ffer
ence
betw
een
grou
ps.
Dos
tlov
aet
al.
(200
9),C
zech
Rep
ubl
ic[2
1].
Incr
ease
dse
rum
con
cen
trat
ion
sof
mac
roph
age
inh
ibit
ory
cyto
kin
e-1
inpa
tien
tsw
ith
obes
ity
and
type
2di
abet
esm
ellit
us:
the
infl
uen
ceof
very
-low
-cal
orie
diet
.
Qu
asie
xper
imen
talo
ne
grou
pw
ith
two
com
pari
son
grou
ps(m
onit
ored
inth
eh
ospi
tal)
.Sa
mpl
e:to
talN
=54
Gro
up
no.
1(c
ompa
riso
n):
(n=
17)
obes
e,n
ondi
abet
icw
omen
.G
rou
pn
o.2
(tre
atm
ent
grou
p):(n=
14)
obes
ew
omen
w/t
ype
2D
M.
Gro
up
no.
3(c
ompa
riso
n):
(n=
23)
hea
lthy
lean
wom
en.
Infl
amm
ator
ym
arke
rs:
CR
P.G
lyce
mic
con
trol
:gl
uco
se,h
omeo
stas
ism
odel
asse
ssm
ent
ofin
sulin
resi
stan
ce(H
OM
A-I
R).
Oth
ers:
MIC
-1le
vels
lipid
s,B
MI,
body
fat
com
posi
tion
.A
not
her
prim
ary
focu
sof
the
stu
dyw
asto
test
leve
lsof
mac
roph
age
inh
ibit
ory
cyto
kin
e-1
(MIC
-1)
and
mR
NA
expr
essi
onof
MIC
-1in
subc
uta
neo
us
and
visc
eral
fat.
No
mea
sure
ofad
her
ence
todi
et.
2-w
eek
very
-low
-cal
orie
diet
.O
nly
obes
ew
omen
wit
han
dw
ith
out
DM
wer
egi
ven
the
IVdi
et;
a2-
wee
k55
0kc
al/d
aydi
et.A
llpa
tien
tsw
ere
hos
pita
lized
.
Hig
hly
con
trol
led
envi
ron
men
tfo
rst
udy
.No
adve
rse
even
tsre
por
ted.
Not
asu
stai
nab
lein
terv
enti
onfo
rlo
ng-
term
use
.T
he
subs
tudy
exam
inin
gM
IC-1
mR
NA
expr
essi
onw
asto
tally
un
rela
ted
toth
e3
grou
psre
ceiv
ing
the
inte
rven
tion
,an
dth
ese
pati
ents
wer
ere
ceiv
ing
surg
ery
and
can
not
beco
mpa
red.
On
e-w
ayA
NO
VA
follo
wed
bypo
sth
octe
sts.
Spea
rman
corr
elat
ion
sp
erfo
rmed
toev
alu
ate
the
rela
tion
ship
ofM
IC-1
expr
essi
onto
oth
erva
riab
les.
For
wom
enw
ith
T2D
M(n=
14),
sign
ifica
nt
chan
ges
inth
efo
llow
ing
para
met
ers
wer
eob
serv
edaf
ter
the
VLC
D:B
MI,
chol
este
rol,
TG
s,gl
uco
se,i
nsu
lin,C
RP,
and
HO
MA
-IR
.
Journal of Nutrition and Metabolism 7
Ta
ble
1:C
onti
nu
ed.
Au
thor
/yea
r/co
un
try
titl
e
Stu
dyde
sign
and
met
hod
sV
aria
bles
Inst
rum
ents
Inte
rven
tion
deta
ilsIm
port
ant
met
hod
olog
ical
flaw
s/bi
asn
oted
Dat
aan
alys
isO
utc
omes
rela
ted
toin
flam
mat
ion
,gly
cem
icco
ntr
ol,a
nd
diet
Koz
łow
ska
etal
.(2
010)
,Pol
and
[22]
.A
dipo
nec
tin
,re
sist
in,a
nd
lept
inre
spon
seto
diet
ary
inte
rven
tion
indi
abet
icn
eph
ropa
thy.
Qu
asie
xper
imen
talo
ne
grou
ppr
etes
t/po
stte
stde
sign
.Sa
mpl
e:N=
17Su
bjec
tsw
ere
obes
ew
ith
T2D
M,a
llto
okan
tihy
pert
ensi
ves,
anti
diab
etic
dru
gs,
phos
phat
ebi
nde
rs,a
nd
diu
reti
cs.S
tudy
dura
tion
was
8w
eeks
.
Infl
amm
ator
ym
arke
rs:
TN
F-α
,CR
PG
lyce
mic
con
trol
:in
sulin
sen
siti
vity
(HO
MA
scor
e),i
nsu
lin,
HbA
1c.
Die
t:n
otm
easu
red.
Oth
ers:
adip
onec
tin
,re
sist
in,l
epti
n,t
otal
prot
ein
,met
abol
icra
teu
sin
gox
ygen
and
CO
2
mea
sure
men
ts.
DE
XA
scan
for
body
com
posi
tion
.
Inte
rven
tion
diet
:20
%en
ergy
defi
cit
0.8–
1g/
kgid
ealb
ody
wei
ght,
30%
calf
rom
fat,
60%
calf
rom
CH
O.
Con
sult
wit
hdi
etic
ian
Q2w
k.
No
men
tion
ofh
owdi
etar
yin
take
was
mea
sure
d,ju
stre
port
edin
ach
art
(Tab
le2)
.N
oco
ntr
olgr
oup.
Smal
lsam
ple
size
,w
eak
desi
gn.
Pear
son
orSp
earm
an’s
test
sfo
rco
rrel
atio
ns.
Rep
eate
dm
easu
res.
Stu
den
t’st-
test
orW
ilcox
onm
atch
edpa
irs.
No
corr
elat
ion
sbe
twee
nfo
odin
take
and
infl
amm
ator
ym
arke
rsm
ade.
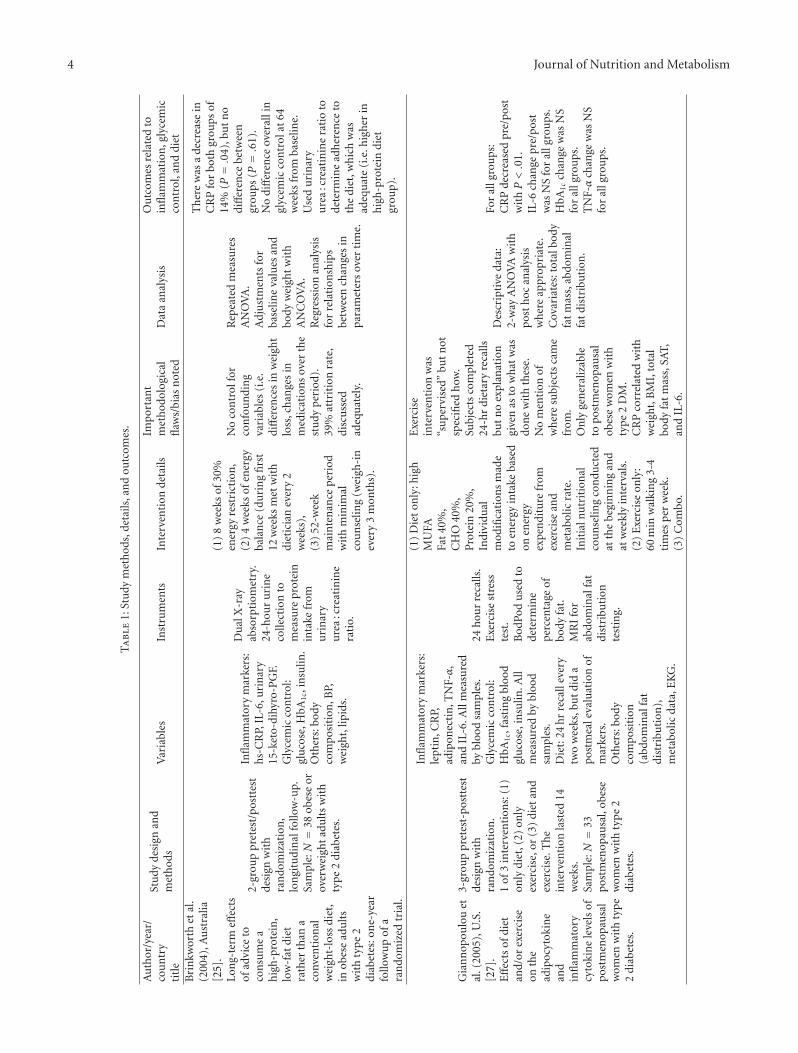
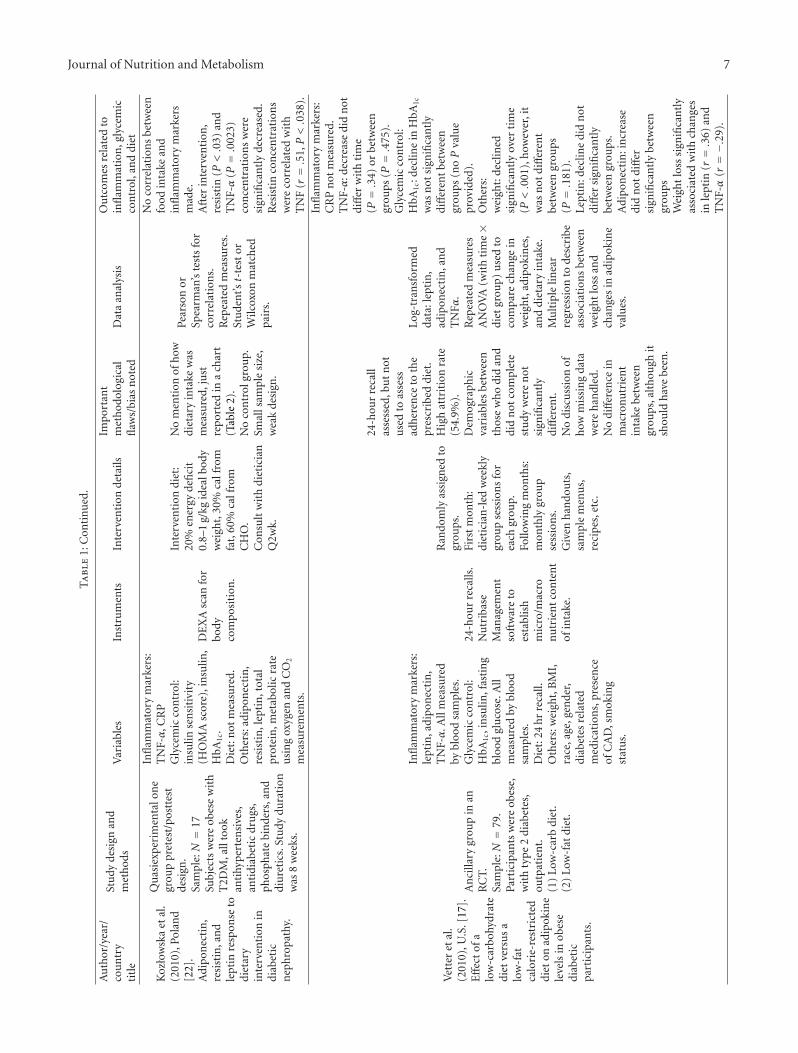
Aft
erin
terv
enti
on,
resi
stin
(P<.0
3)an
dT
NF-α
(P=.0
023)
con
cen
trat
ion
sw
ere
sign
ifica
ntl
yde
crea
sed.
Res
isti
nco
nce
ntr
atio
ns
wer
eco
rrel
ated
wit
hT
NF
(r=.5
1,P<.0
38).
Vet
ter
etal
.(2
010)
,U.S
.[17
].E
ffec
tof
alo
w-c
arbo
hydr
ate
diet
vers
us
alo
w-f
atca
lori
e-re
stri
cted
diet
onad
ipok
ine
leve
lsin
obes
edi
abet
icpa
rtic
ipan
ts.
An
cilla
rygr
oup
inan
RC
T.Sa
mpl
e:N=
79.
Part
icip
ants
wer
eob
ese,
wit
hty
pe2
diab
etes
,ou
tpat
ien
t.(1
)Lo
w-c
arb
diet
.(2
)Lo
w-f
atdi
et.
Infl
amm
ator
ym
arke
rs:
lept
in,a
dipo
nec
tin
,T
NF-α
.All
mea
sure
dby
bloo
dsa
mpl
es.
Gly
cem
icco
ntr
ol:
HbA
1c,i
nsu
lin,f
asti
ng
bloo
dgl
uco
se.A
llm
easu
red
bybl
ood
sam
ples
.D
iet:
24h
rre
call.
Oth
ers:
wei
ght,
BM
I,ra
ce,a
ge,g
ende
r,di
abet
esre
late
dm
edic
atio
ns,
pres
ence
ofC
AD
,sm
okin
gst
atu
s.
24-h
our
reca
lls.
Nu
trib
ase
Man
agem
ent
soft
war
eto
esta
blis
hm
icro
/mac
ron
utr
ien
tco
nte
nt
ofin
take
.
Ran
dom
lyas
sign
edto
grou
ps.
Firs
tm
onth
:di
etic
ian
-led
wee
kly
grou
pse
ssio
ns
for
each
grou
p.Fo
llow
ing
mon
ths:
mon
thly
grou
pse
ssio
ns.
Giv
enh
ando
uts
,sa
mpl
em
enu
s,re
cip
es,e
tc.
24-h
our
reca
llas
sess
ed,b
ut
not
use
dto
asse
ssad
her
ence
toth
epr
escr
ibed
diet
.H
igh
attr
itio
nra
te(5
4.9%
).D
emog
raph
icva
riab
les
betw
een
thos
ew
ho
did
and
did
not
com
plet
est
udy
wer
en
otsi
gnifi
can
tly
diff
eren
t.N
odi
scu
ssio
nof
how
mis
sin
gda
taw
ere
han
dled
.N
odi
ffer
ence
inm
acro
nu
trie
nt
inta
kebe
twee
ngr
oups
,alt
hou
ghit
shou
ldh
ave
been
.
Log-
tran
sfor
med
data
:lep
tin
,ad
ipon
ecti
n,a
nd
TN
Fα.
Rep
eate
dm
easu
res
AN
OV
A(w
ith
tim
e×
diet
grou
p)u
sed
toco
mpa
rech
ange
inw
eigh
t,ad
ipok
ines
,an
ddi
etar
yin
take
.M
ult
iple
linea
rre
gres
sion
tode
scri
beas
soci
atio
ns
betw
een
wei
ght
loss
and
chan
ges
inad
ipok
ine
valu
es.
Infl
amm
ator
ym
arke
rs:
CR
Pn
otm
easu
red.
TN
F-α
:dec
reas
edi
dn
otdi
ffer
wit
hti
me
(P=.3
4)or
betw
een
grou
ps(P=.4
75).
Gly
cem
icco
ntr
ol:
HbA
1c:d
eclin
ein
HbA
1c
was
not
sign
ifica
ntl
ydi
ffer
ent
betw
een
grou
ps(n
oP
valu
epr
ovid
ed).
Oth
ers:
wei
ght:
decl
ined
sign
ifica
ntl
yov
erti
me
(P<.0
01),
how
ever
,it
was
not
diff
eren
tbe
twee
ngr
oups
(P=.1
81).
Lept
in:d
eclin
edi
dn
otdi
ffer
sign
ifica
ntl
ybe
twee
ngr
oups
.A
dipo
nec
tin
:in
crea
sedi
dn
otdi
ffer
sign
ifica
ntl
ybe
twee
ngr
oups
Wei
ght
loss
sign
ifica
ntl
yas
soci
ated
wit
hch
ange
sin
lept
in(r=.3
6)an
dT
NF-α
(r=−.
29).

8 Journal of Nutrition and Metabolism
Ta
ble
1:C
onti
nu
ed.
Au
thor
/yea
r/co
un
try
titl
e
Stu
dyde
sign
and
met
hod
sV
aria
bles
Inst
rum
ents
Inte
rven
tion
deta
ilsIm
port
ant
met
hod
olog
ical
flaw
s/bi
asn
oted
Dat
aan
alys
isO
utc
omes
rela
ted
toin
flam
mat
ion
,gly
cem
icco
ntr
ol,a
nd
diet
Aza
dbak
ht
etal
.(2
011)
,stu
dyco
ndu
cted
inIr
an[1
8].
Th
eD
ieta
ryA
ppro
ach
esto
Stop
Hyp
erte
nsi
onea
tin
gpl
anaff
ects
C-r
eact
ive
prot
ein
,co
agu
lati
onab
nor
mal
itie
s,an
dh
epat
icfu
nct
ion
test
sam
ong
typ
e2
diab
etic
pati
ents
.
Cro
ssov
erin
terv
enti
onde
sign
wit
hra
ndo
miz
atio
n.
Sam
ple:N=
31,
Con
ven
ien
cesa
mpl
eof
adu
lts
wit
hty
pe2
diab
etes
atth
eSh
ahee
dM
otah
ariH
ospi
talo
fFo
olad
shah
r.
Infl
amm
ator
ym
arke
rs:
CR
P.G
lyce
mic
con
trol
:n
otm
easu
red.
Die
t:m
acro
nu
trie
nt
inta
ke.
Oth
ers:
ALT
,AST
,AL
P,bi
liru
bin
.
3ddi
etar
yre
call
toas
sess
adh
eren
ceto
the
pres
crib
eddi
et.
Mon
thly
3-da
yph
ysic
alac
tivi
tydi
ary.
8-w
eek
cros
sove
rst
udy
wit
hra
ndo
miz
atio
nto
con
trol
orD
ASH
diet
.C
ontr
oldi
eth
adfe
wer
PU
FA.
En
ergy
inta
kein
divi
dual
lyta
ilore
d.M
onth
lyvi
sits
.4-
wee
kw
ash
out
per
iod
.
Un
clea
rh
owst
udy
was
con
duct
ed,n
otea
syto
follo
wm
eth
ods.
R/o
carr
yove
reff
ects
.N
om
enti
onof
how
lon
gea
chdi
etw
asm
ain
tain
ed,i
fth
ere
was
aw
ash
out
peri
od,o
rw
hyth
ose
wh
oh
adle
ftth
epr
otoc
olle
ft(r
/ofa
tigu
eeff
ect)
.
Ass
essi
ng
effec
tof
inte
rven
tion
:pai
red
t-te
stw
ith
and
wit
hou
tad
just
men
tfo
rw
eigh
t.G
rou
psco
mpa
red
usi
ng
a%
chan
geca
lcu
lati
on.
Pati
ents
wh
o“d
evia
ted
from
the
stu
dypr
otoc
ol”
wer
en
otin
clu
ded
inth
ean
alys
is(p
.108
4).
Pati
ents
wh
ore
ceiv
edth
eD
ASH
diet
show
eda
redu
ctio
nin
CR
P,pl
asm
afi
brin
ogen
,an
dliv
ertr
ansf
eras
een
zym
es.
Th
ese
redu
ctio
ns
wer
esi
gnifi
can
tan
dre
mai
ned
sign
ifica
nt
afte
rad
just
ing
for
the
effec
tof
wei
ght.
Boz
zett
oet
al.
(201
1),I
taly
[19]
.T
he
asso
ciat
ion
ofh
s-C
RP
wit
hfa
stin
gan
dpo
stpr
andi
alpl
asm
alip
ids
inpa
tien
tsw
ith
type
2di
abet
esis
disr
upt
edby
diet
ary
mon
oun
satu
rate
dfa
tty
acid
s.
Pre
exp
erim
enta
lpos
ttes
ton
lyC
ross
-ove
rw
ith
ran
dom
izat
ion
(no
was
hou
t).
Sam
ple:
12pa
rtic
ipan
tsw
ith
type
2di
abet
esH
bA1c
ingo
odco
ntr
ol.
4w
eeks
onea
chdi
et.N
ow
ash
out
per
iod
men
tion
ed.
Infl
amm
ator
ym
arke
rs:
CR
P.G
lyce
mic
con
trol
:n
otm
easu
red.
Die
t:n
otm
easu
red.
Oth
ers:
trig
lyce
ride
-ric
hlip
opro
tein
s(c
hylo
mic
ron
s,la
rge
VL
DL
,sm
allV
LD
L),
chol
este
rola
nd
trig
lyce
ride
.
Not
hin
gpr
ovid
edin
pape
r.
Die
tsw
ere
isoe
ner
geti
c:bo
thh
adkc
alof
948
per
day.
Ran
dom
ized
,cr
osso
ver
desi
gn.
CH
O/fi
ber/
low
-GI:
C52
%,
MU
FA17
%,
GI
58%
.
Hig
h-M
UFA
diet
:C
45%
,M
UFA
23%
,G
I88
%.
No
deta
ilsgi
ven
con
cern
ing
diet
ary
advi
sem
ent.
Die
tary
adh
eren
cen
otm
easu
red.
Con
fou
ndi
ng
vari
able
sn
otex
plor
ed.
Bod
yw
eigh
tdi
dn
otch
ange
sign
ifica
ntl
yov
erth
est
udy
per
iod,
but
itsh
ould
hav
ech
ange
d,
con
side
rin
gth
elim
ited
calo
ric
pres
crip
tion
.
Pair
edt-
test
sto
iden
tify
diff
eren
ces
inou
tcom
em
easu
res
betw
een
the
two
diet
s(g
rou
psw
ere
mer
ged
for
anal
ysis
).R
epea
ted
mea
sure
sA
NO
VA
toev
alu
ate
diff
eren
ces
inpo
stpr
andi
alte
stin
g(m
ult
iple
test
s).T
hey
clai
mn
oca
rryo
ver
effec
tw
asde
tect
ed.
Die
tan
din
flam
mat
ion
:af
ter
inte
rven
tion
,fa
stin
gC
RP
valu
esw
ere
not
sign
ifica
ntl
ydi
ffer
ent
betw
een
stu
dydi
ets,
alth
ough
CR
Pdi
dde
crea
sesi
gnifi
can
tly
afte
rth
eM
UFA
mea
l(P
<.0
5),n
otth
eC
HO
/fibe
rm
eal.
Journal of Nutrition and Metabolism 9
Ta
ble
1:C
onti
nu
ed.
Au
thor
/yea
r/co
un
try
titl
e
Stu
dyde
sign
and
met
hod
sV
aria
bles
Inst
rum
ents
Inte
rven
tion
deta
ilsIm
port
ant
met
hod
olog
ical
flaw
s/bi
asn
oted
Dat
aan
alys
isO
utc
omes
rela
ted
toin
flam
mat
ion
,gly
cem
icco
ntr
ol,a
nd
diet
Dav
iset
al.
(201
1),[
26].
Diff
eren
tial
effec
tsof
low
-car
bohy
drat
ean
dlo
w-f
atdi
ets
onin
flam
mat
ion
and
endo
thel
ial
fun
ctio
nin
diab
etes
.
2-gr
oup
pre-
test
/pos
t-te
stcl
inic
altr
ials
ubg
rou
pof
larg
ertr
ial.
Sam
ple:
subj
ects
wer
eob
ese
wit
hty
pe
2di
abet
esw
ith
anH
bA1c
betw
een
6%an
d11
%.
N=
5163
%of
subj
ects
wer
eB
lack
inbo
thdi
etgr
oups
,in
the
low
-car
bgr
oup,
11%
ofth
esu
bjec
tsw
ere
His
pan
ic.
Infl
amm
ator
ym
arke
rs:
CR
P,IL
-6.
Gly
cem
icco
ntr
ol:
glu
cose
,HbA
1c.
Oth
ers:
endo
thel
ial
fun
ctio
n(s
-IC
AM
,so
lubl
eE
-sel
ecti
n),
and
reac
tive
hyp
erem
icp
erip
her
alar
teri
alto
nom
etry
,wei
ght,
lipid
s.
En
doPa
tto
mea
sure
per
iph
eral
mic
rova
scu
lar
endo
thel
ial
fun
ctio
n.
Tota
l24
wee
ks:
subj
ects
ran
dom
ized
tore
ceiv
eei
ther
alo
w-c
arbo
hydr
ate,
Atk
ins-
styl
edi
etor
alo
w-f
atdi
et(s
imila
rto
DP
Pdi
et).
Part
icip
ants
rece
ived
stru
ctu
red
men
us
for
the
1st
two
wee
ks.
Med
icat
ion
sw
ere
adju
sted
base
don
apr
edefi
ned
algo
rith
m.
Die
tw
asre
info
rced
ever
y6
wee
ksat
sch
edu
led
visi
ts.
No
con
trol
grou
p.N
om
easu
reof
adh
eren
ceto
pres
crib
eddi
et.
CR
Pan
dIL
-6w
ere
log-
tran
sfor
med
.U
npa
ired
t-te
sts
(or
Wilc
oxon
ran
k)u
sed
tode
tect
diff
eren
ces
inpa
ram
eter
outc
omes
betw
een
diet
ary
arm
s.Pe
arso
nor
Spea
rman
corr
elat
ion
s.
Low
-fat
diet
:CR
Pde
crea
sed
from
4.0
to3.
0(P=.0
1).
Low
-car
bdi
etdi
dn
otca
use
asi
gnifi
can
tch
ange
inC
RP
(P=.9
4).
Low
-car
bdi
et:s
ICA
Mde
crea
sed
from
234
to19
9(P=.0
01),
E-s
elec
tin
decr
ease
dfr
om92
to82
(P=.0
5).
Itsi
opou
los
etal
.(2
010)
,Au
stra
lia[2
0].
Can
the
Med
iter
ran
ean
diet
low
erH
bA1c
inty
pe2
diab
etes
?R
esu
lts
from
ara
ndo
miz
edcr
oss-
over
stu
dy.
Ran
dom
ized
cros
s-ov
er(2
grou
pspr
etes
t,po
stte
st).
Sam
ple:N=
31Su
bjec
tsre
cru
ited
from
new
spap
erh
ad“w
ell-
con
trol
led”
typ
e2
diab
etes
.
Infl
amm
ator
ym
arke
rs:
CR
P,h
omoc
yste
ine.
Gly
cem
icco
ntr
ol:
HO
MA
,HbA
1c,f
asti
ng
glu
cose
.O
ther
:h
eigh
t,ag
e,pl
asm
afa
tty
acid
s,24
-hr
uri
ne
albu
min
and
crea
tin
ine,
wei
ght,
wai
st-h
ipra
tio,
intr
aabd
omin
alad
ipos
eti
ssu
e(I
AA
T),
BP.
Hea
lth
and
lifes
tyle
ques
tion
nai
re(n
otde
fin
ed).
Seve
n-d
aydi
etre
cord
(com
plet
edby
part
icip
ant)
.U
sed
chan
ges
inpl
asm
ale
vels
ofse
vera
ldiff
eren
tca
rote
noi
dsto
chec
kco
mpl
ian
cew
ith
the
IVdi
et.
Inte
rven
tion
was
aM
edit
erra
nea
ndi
etfo
r12
wee
ks,t
hen
cros
sove
r(2
4w
eeks
tota
l).
70%
ofin
terv
enti
ondi
etm
eals
prep
ared
and
prov
ided
inbu
lkfo
rfr
ee.A
dvis
edto
eat
3se
rvin
gsfr
uit
sp
erda
y.
No
was
hou
tp
erio
dbe
twee
ndi
etpe
riod
s.M
easu
rem
ent
tool
sn
otst
anda
rdiz
ed.
Oliv
eoi
lcom
pany
prov
ided
the
oliv
eoi
l,m
ayle
adto
bias
edre
sult
s.U
nde
rpow
ered
.
Dat
afr
omth
etw
odi
ets
wer
epo
oled
.R
epea
ted-
mea
sure
sA
NO
VA
.U
sed
anin
tera
ctio
nte
rmto
con
trol
for
abse
nce
ofw
ash
out
per
iod
.
Sign
ifica
nt
redu
ctio
nin
HbA
1cin
the
inte
rven
tion
diet
.Tr
end
tow
ard
decr
ease
inH
OM
Aan
dB
MI.
Incr
ease
inpl
ant
food
inta
ke.
10 Journal of Nutrition and Metabolism
Ta
ble
1:C
onti
nu
ed.
Au
thor
/yea
r/co
un
try
titl
e
Stu
dyde
sign
and
met
hod
sV
aria
bles
Inst
rum
ents
Inte
rven
tion
deta
ilsIm
port
ant
met
hod
olog
ical
flaw
s/bi
asn
oted
Dat
aan
alys
isO
utc
omes
rela
ted
toin
flam
mat
ion
,gly
cem
icco
ntr
ol,a
nd
diet
Kh
ooet
al.
(201
1),A
ust
ralia
[28]
.C
ompa
rin
geff
ects
ofa
low
-en
ergy
diet
and
ah
igh
-pro
tein
low
-fat
diet
onse
xual
and
endo
thel
ial
fun
ctio
n,u
rin
ary
trac
tsy
mp
tom
s,an
din
flam
mat
ion
inob
ese
diab
etic
men
.
2gr
oup
pret
est-
post
test
desi
gnw
ith
ran
dom
izat
ion
.Sa
mpl
e:co
nven
ien
cesa
mpl
eof
31W
hit
em
enw
ith
type
2di
abet
esan
der
ecti
ledy
sfu
nct
ion
.R
ando
mly
assi
gned
toei
ther
mod
ified
low
-cal
orie
diet
(LC
D)
orh
igh
-pro
tein
low
-fat
diet
(HP
diet
)fo
r8
wee
ks.
Aft
erfi
rst
8w
eeks
,all
subj
ects
wer
epl
aced
onth
eH
Pdi
etfo
rth
ere
mai
nin
g44
wee
ks.
Infl
amm
ator
ym
arke
rs:
CR
P,IL
-6,a
nd
solu
ble
E-s
elec
tin
.G
lyce
mic
con
trol
:qu
anti
tati
vein
sulin
sen
siti
vity
chec
kin
dex
(QU
ICK
I),g
luco
se,
insu
lin.
Die
t:co
mpl
ian
ce,n
otu
sed
inan
alys
is.
Oth
ers:
andr
ogen
leve
ls,e
rect
ilefu
nct
ion
,se
xual
desi
re,a
nd
low
eru
rin
ary
trac
tsy
mpt
oms.
Food
diar
ies
tom
onit
orco
mpl
ian
ce.
IIE
F-5,
Sexu
alD
esir
eIn
ven
tory
,In
tern
atio
nal
Pro
stat
eSy
mpt
omSc
ale.
Die
tco
mpl
ian
cem
onit
ored
ever
y2–
4w
eeks
.LC
D:2
liqu
idm
eals
per
day
plu
ssm
all
mea
lfor
tota
lof
900
kcal
/day
.H
Pdi
et:3
00g
lean
mea
t/po
ult
ry/fi
sh,3
serv
ings
/day
ofce
real
s/br
ead
and
low
-fat
dair
yfo
ods,
and
two
fru
itan
dve
geta
ble
serv
ings
/day
.Sh
ould
indu
cea
600
kcal
defi
cit
from
diet
.A
llsu
bjec
tsre
ceiv
edm
enu
plan
s,re
cipe
s,an
dco
okin
gad
vice
.A
ctiv
ity
was
not
rest
rict
ed.
Adh
eren
cen
otre
port
edor
use
din
anal
ysis
,alt
hou
ghdi
etdi
arie
sw
ere
use
d.M
ajor
focu
sof
the
stu
dyw
asse
xual
and
endo
thel
ial
fun
ctio
n.
Han
dlin
gof
mis
sin
gda
tan
otdi
scu
ssed
.
Max
imu
mlik
elih
ood
rep
eate
dm
easu
res
mix
edm
odel
sto
com
pare
pre/
pos
tm
easu
res.
Use
dti
me×
diet
inte
ract
ion
.Po
sth
ocpa
irw
ise
test
sm
ade.
Infl
amm
atio
n:
sign
ifica
nt
decr
ease
inC
RP
(at
8an
d52
wk)
,E
-Sel
ecti
n(a
t8
and
52w
k),a
nd
IL-6
(at
8w
kon
ly)
inH
Pdi
etgr
oup
(P<.0
1),b
ut
not
LCD
grou
p.G
lyce
mic
con
trol
:in
sulin
sen
siti
vity
(QU
ICK
I)si
gnifi
can
tim
prov
edin
LCD
grou
p,bu
tn
otH
Pdi
et(P
<.0
1).P
lasm
agl
uco
sedi
dn
otim
prov
esi
gnifi
can
tly
inei
ther
grou
p.O
ther
:sig
nifi
can
tly
wei
ght
loss
inbo
thgr
oups
.
Mra
zet
al.
(201
1),
Cze
chR
epu
blic
[23]
.T
he
effec
tof
ave
ry-l
ow-c
alor
iedi
eton
mR
NA
expr
essi
onof
infl
amm
atio
n-
rela
ted
gen
esin
subc
uta
neo
us
adip
ose
tiss
ue
and
per
iph
eral
mon
ocyt
esof
obes
epa
tien
tsw
ith
typ
e2
diab
etes
.
Qu
asie
xper
imen
tal
desi
gnw
ith
two
com
pari
son
grou
ps.
Sam
ple:N=
35w
omen
only
.Th
ein
terv
enti
onw
ason
lyim
plem
ente
din
the
12ob
ese
wom
enw
ith
T2D
M.
Two
oth
erco
ntr
olgr
oups
:15
hea
lthy
wom
en,a
nd
8ob
ese
wom
enw
ith
out
T2D
M.
Inte
rven
tion
last
ed2
wee
ksan
dw
asco
ndu
cted
ina
hos
pita
lse
ttin
gfo
rcl
ose
mon
itor
ing.
Infl
amm
ator
ym
arke
rs:
CR
P,IL
-6,T
NF,
IL-8
,C
CL-
2.G
lyce
mic
con
trol
:gl
uco
se,H
bA1c
,in
sulin
.D
iet:
non
e.O
ther
s:su
bcu
tan
eou
sad
ipos
eti
ssu
efo
rm
RN
Aex
pres
sion
ofch
emot
acti
cfa
ctor
s,lip
idpr
ofile
,ad
ipon
ecti
n,l
epti
n,
resi
stin
,wei
ght,
BM
I,an
dag
e.
Not
hin
gpr
ovid
edin
pape
r.
On
lyob
ese
wom
enw
ith
DM
wer
egi
ven
the
IVdi
et;a
2-w
eek
600
kcal
/day
diet
.All
pati
ents
wer
eh
ospi
taliz
ed.
No
adve
rse
even
tsor
med
icat
ion
chan
ges
repo
rted
from
the
inte
rven
tion
per
iod.
Inad
equ
ate
deta
ilof
the
inte
rven
tion
.N
odi
scu
ssio
nof
poss
ible
cau
ses
for
the
abn
orm
alfi
ndi
ng
ofin
crea
sed
TN
Ffo
llow
ing
the
inte
rven
tion
.
Pair
edt-
test
orW
ilcox
onsi
gned
-ran
kte
stu
sed
tode
tect
diff
eren
ces
betw
een
mea
sure
men
tspr
e/po
stin
terv
enti
on.
TN
F-α
leve
lsw
ere
sign
ifica
ntl
yin
crea
sed
inT
2DM
wom
enaf
ter
2w
eeks
offo
llow
ing
the
VLC
D(P
<.0
5fo
rpr
e/p
ostΔ
).H
bA1c
not
asse
ssed
afte
rin
terv
enti
on(o
nly
2w
eeks
).μΔ
inC
RP
pre/
post=
.94
mg/
L,P<.0
5.μΔ
inIL
-6pr
e/po
st=
.8pg
/mL
,P<.0
5.
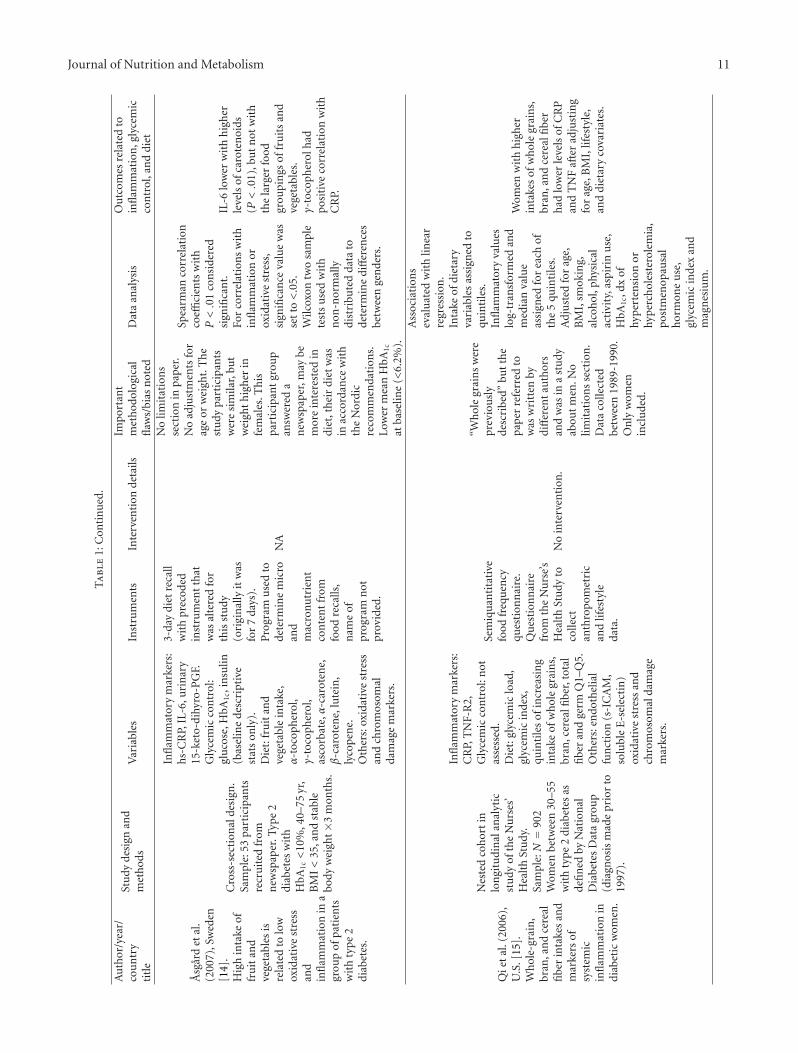
Journal of Nutrition and Metabolism 11
Ta
ble
1:C
onti
nu
ed.
Au
thor
/yea
r/co
un
try
titl
e
Stu
dyde
sign
and
met
hod
sV
aria
bles
Inst
rum
ents
Inte
rven
tion
deta
ilsIm
port
ant
met
hod
olog
ical
flaw
s/bi
asn
oted
Dat
aan
alys
isO
utc
omes
rela
ted
toin
flam
mat
ion
,gly
cem
icco
ntr
ol,a
nd
diet
Asg
ard
etal
.(2
007)
,Sw
eden
[14]
.H
igh
inta
keof
fru
itan
dve
geta
bles
isre
late
dto
low
oxid
ativ
est
ress
and
infl
amm
atio
nin
agr
oup
ofpa
tien
tsw
ith
typ
e2
diab
etes
.
Cro
ss-s
ecti
onal
desi
gn.
Sam
ple:
53pa
rtic
ipan
tsre
cru
ited
from
new
spap
er.T
ype
2di
abet
esw
ith
HbA
1c<
10%
,40–
75yr
,B
MI<
35,a
nd
stab
lebo
dyw
eigh
t×3
mon
ths.
Infl
amm
ator
ym
arke
rs:
hs-
CR
P,IL
-6,u
rin
ary
15-k
eto-
dihy
ro-P
GF.
Gly
cem
icco
ntr
ol:
glu
cose
,HbA
1c,i
nsu
lin(b
asel
ine
desc
ript
ive
stat
son
ly).
Die
t:fr
uit
and
vege
tabl
ein
take
,α
-toc
oph
erol
,γ-
toco
pher
ol,
asco
rbat
e,α
-car
oten
e,β
-car
oten
e,lu
tein
,ly
cope
ne.
Oth
ers:
oxid
ativ
est
ress
and
chro
mos
omal
dam
age
mar
kers
.
3-da
ydi
etre
call
wit
hpr
ecod
edin
stru
men
tth
atw
asal
tere
dfo
rth
isst
udy
(ori
gin
ally
itw
asfo
r7
days
).P
rogr
amu
sed
tode
term
ine
mic
roan
dm
acro
nu
trie
nt
con
ten
tfr
omfo
odre
calls
,n
ame
ofpr
ogra
mn
otpr
ovid
ed.
NA
No
limit
atio
ns
sect
ion
inpa
per.
No
adju
stm
ents
for
age
orw
eigh
t.T
he
stu
dypa
rtic
ipan
tsw
ere
sim
ilar,
but
wei
ght
hig
her
infe
mal
es.T
his
part
icip
ant
grou
pan
swer
eda
new
spap
er,m
aybe
mor
ein
tere
sted
indi
et,t
hei
rdi
etw
asin
acco
rdan
cew
ith
the
Nor
dic
reco
mm
enda
tion
s.Lo
wer
mea
nH
bA1c
atba
selin
e(<
6.2%
).
Spea
rman
corr
elat
ion
coeffi
cien
tsw
ith
P<.0
1co
nsi
dere
dsi
gnifi
can
t.Fo
rco
rrel
atio
ns
wit
hin
flam
mat
ion
orox
idat
ive
stre
ss,
sign
ifica
nce
valu
ew
asse
tto
<.0
5.W
ilcox
ontw
osa
mpl
ete
sts
use
dw
ith
non
-nor
mal
lydi
stri
bute
dda
tato
dete
rmin
edi
ffer
ence
sbe
twee
nge
nde
rs.
IL-6
low
erw
ith
hig
her
leve
lsof
caro
ten
oids
(P<.0
1),b
ut
not
wit
hth
ela
rger
food
grou
pin
gsof
fru
its
and
vege
tabl
es.
γ-to
coph
erol
had
posi
tive
corr
elat
ion
wit
hC
RP.
Qie
tal
.(20
06),
U.S
.[15
].W
hol
e-gr
ain
,br
an,a
nd
cere
alfi
ber
inta
kes
and
mar
kers
ofsy
stem
icin
flam
mat
ion
indi
abet
icw
omen
.
Nes
ted
coh
ort
inlo
ngi
tudi
nal
anal
ytic
stu
dyof
the
Nu
rses
’H
ealt
hSt
udy
.Sa
mpl
e:N=
902
Wom
enbe
twee
n30
–55
wit
hty
pe2
diab
etes
asde
fin
edby
Nat
ion
alD
iabe
tes
Dat
agr
oup
(dia
gnos
ism
ade
prio
rto
1997
).
Infl
amm
ator
ym
arke
rs:
CR
P,T
NF-
R2,
Gly
cem
icco
ntr
ol:n
otas
sess
ed.
Die
t:gl
ycem
iclo
ad,
glyc
emic
inde
x,qu
inti
les
ofin
crea
sin
gin
take
ofw
hol
egr
ain
s,br
an,c
erea
lfibe
r,to
tal
fibe
ran
dge
rmQ
1–Q
5.O
ther
s:en
doth
elia
lfu
nct
ion
(s-I
CA
M,
solu
ble
E-s
elec
tin
)ox
idat
ive
stre
ssan
dch
rom
osom
alda
mag
em
arke
rs.
Sem
iqu
anti
tati
vefo
odfr
equ
ency
ques
tion
nai
re.
Qu
esti
onn
aire
from
the
Nu
rse’
sH
ealt
hSt
udy
toco
llect
anth
ropo
met
ric
and
lifes
tyle
data
.
No
inte
rven
tion
.
“Wh
ole
grai
ns
wer
epr
evio
usl
yde
scri
bed”
but
the
pape
rre
ferr
edto
was
wri
tten
bydi
ffer
ent
auth
ors
and
was
ina
stu
dyab
out
men
.No
limit
atio
ns
sect
ion
.D
ata
colle
cted
betw
een
1989
-199
0.O
nly
wom
enin
clu
ded.
Ass
ocia
tion
sev
alu
ated
wit
hlin
ear
regr
essi
on.
Inta
keof
diet
ary
vari
able
sas
sign
edto
quin
tile
s.In
flam
mat
ory
valu
eslo
g-tr
ansf
orm
edan
dm
edia
nva
lue
assi
gned
for
each
ofth
e5
quin
tile
s.A
dju
sted
for
age,
BM
I,sm
okin
g,al
coh
ol,p
hysi
cal
acti
vity
,asp
irin
use
,H
bA1c
,dx
ofhy
per
ten
sion
orhy
per
chol
este
role
mia
,po
stm
enop
ausa
lh
orm
one
use
,gl
ycem
icin
dex
and
mag
nes
ium
.
Wom
enw
ith
hig
her
inta
kes
ofw
hol
egr
ain
s,br
an,a
nd
cere
alfi
ber
had
low
erle
vels
ofC
RP
and
TN
Faf
ter
adju
stin
gfo
rag
e,B
MI,
lifes
tyle
,an
ddi
etar
yco
vari
ates
.

12 Journal of Nutrition and Metabolism
Ta
ble
2:Q
ual
ity
Ass
essm
ent
tool
and
scor
es.
Art
icle
Aim
sM
eth
ods
Die
tof
inte
rest
Rec
ruit
men
tIn
flam
mat
ion
Con
fou
ndi
ng
vari
able
sM
issi
ng
Con
clu
sion
sQ
ual
ity
rati
ng
(1pt
)(1
ptea
ch)
wel
l-de
fin
ed?
(1pt
each
)(1
pt)
(1pt
)(1
pt)
data
/att
riti
on(1
pt)
(2pt
s)(o
ut
of12
pts)
1st
Au
thor
Cle
arly
desc
ribe
dR
ead
Rep
rA
dT
OD
iet
Dis
cuss
edM
easu
res
appr
opri
ate
Con
trol
led
Pro
per
lyh
andl
edA
ppro
pria
teTo
tal
Asg
ard
10
11
00
11
01
17
Itsi
opou
los
11
01
11
11
00
07
Dav
is1
10
11
01
11
02
9Q
i1
10
11
10
11
02
8D
ostl
ova
10
01
00
01
10
15
Aza
dbak
ht
11
01
11
11
10
210
Boz
zett
o1
00
00
11
10
02
6G
ian
nop
oulo
u1
10
01
10
11
02
8B
arn
ard
01
01
11
11
01
18
Wol
ever
11
01
11
01
11
19
Vet
ter
01
00
10
00
10
14
Kos
łow
ska
10
00
10
01
00
14
Mar
fella
11
00
10
01
00
15
Kh
oo1
10
11
01
10
01
7M
raz
10
00
10
01
00
14
Bri
nkw
orth
11
11
11
11
01
110
Not
e.A
d:ad
her
ence
;Die
t:di
etar
yin
terv
enti
onde
fin
ed;R
ead:
read
abili
ty;R
epr:
repr
odu
cibi
lity;
TO
:app
ropr
iate
use
ofte
mpo
ralo
rder
ing.

Journal of Nutrition and Metabolism 13T
abl
e3:
Exp
erim
enta
lstu
dies
:ch
arac
teri
stic
san
dre
sult
sof
data
abst
ract
ion
.
Au
thor
/yea
r/co
un
try
Des
ign
Stu
dyle
ngt
h(w
eek)
Subj
ects
Die
tary
inte
rven
tion
Ou
tcom
esQ
ual
ity
rati
ng
Die
tde
tails
Con
trol
for
wei
ght
loss
diff
eren
ces?
ΔC
RP
ΔH
bA1c
%O
ther
Bri
nkw
orth
etal
.(2
004)
,Au
stra
lia[2
5]
2gr
oup
pret
est/
post
test
com
pari
son
desi
gnw
ith
ran
dom
izat
ion
64
N=
38F=
61%
M=
39%
μag
e=
61.8
Low
-pro
tein
(15%
)C
HO
55%
Fat
30%
vers
us
Hig
h-p
rote
in(3
0%)
CH
O40
%Fa
t30
%
Yes
Wei
ght
P=.6
1di
ffer
ence
betw
een
diet
s,bu
tov
eral
lde
crea
seP=.0
4Lo
w-p
rote
in:
pre:
4.2
post
(64
wk)
:3.6
Hig
h-p
rote
in:
pre:
5.0
post
(64
wk)
:3.8
P=.3
8∗
Low
-pro
tein
:pr
e:6.
2po
st(6
4w
k):6
.6H
igh
-pro
tein
:pr
e:6.
5po
st(6
4w
k):6
.6
NA
10
Gia
nn
opou
lou
etal
.(20
05),
U.S
.[2
7]
3-gr
oup,
pret
est-
post
test
wit
hra
ndo
miz
atio
n
14N=
33Fe
mal
eon
lyμ
age=
57
Die
ton
lyC
HO
40%
Fat
40%
(MU
FA30
%)
Exe
rcis
eon
lyD
iet
and
exer
cise
No
P<.0
1fo
ral
lth
ree
grou
psN
ora
wda
taav
aila
ble
NSΔ
NSΔ
inT
NF-α
orIL
-6fo
ral
lth
ree
grou
ps8
Mar
fella
etal
.(2
006)
,Ita
ly[1
6]R
CT
52
N=
115
M/F
data
not
give
nμ
age=
35.8
Win
e:4
oz.p
erda
y+
Med
iter
ran
ean
diet
Con
trol
grou
p:n
ow
ine
+M
edit
erra
nea
ndi
et
No
P<.0
1∗
Ch
ange
sin
raw
CR
Pva
lues
not
avai
labl
e
P=
NS∗
Ch
ange
sin
HbA
1c
Win
e:−1
.1±
0.06
Con
trol
:−1.
2±
0.7
TN
F-αP<.0
1∗
Ch
ange
sin
raw
TN
Fva
lues
not
avai
labl
eIL
-6P<.0
1∗
Ch
ange
sin
raw
IL-6
valu
esn
otav
aila
ble
5
Wol
ever
etal
.(2
008)
,Can
ada
[29]
3gr
oups
,pr
etes
t-po
stte
stw
ith
ran
dom
izat
ion
52
N=
162
F=
54%
M=
46%
μag
e=
59.9
Hig
hG
ILo
wG
ILo
wC
HO
CH
O20
%–2
5%Fa
tn
otpr
ovid
ed,
but
hig
hM
UFA
inLo
w-C
HO
diet
Yes
BM
I
Low
GI-
diet
:P<.0
5(d
iffer
ent
inμ
CR
Ppo
stin
terv
enti
onbe
twee
nlo
wan
dh
igh
GI
diet
s)po
stin
terv
enti
onμ
:H
igh
GI:
2.75
Low
GI:
1.95
Low
CH
O:2
.35
NS
diff
eren
cebe
twee
ngr
oups
,H
bA1c
rose
duri
ng
inte
rven
tion
Hig
hG
I:6.
34Lo
wG
I:6.
34Lo
wC
HO
:6.3
5
NA
9
Bar
nar
det
al.
(200
9),U
.S.[
24]
2gr
oups
,pr
etes
t-po
stte
st74
N=
99F=
61%
M=
39%
μag
e=
55.7
Veg
andi
etC
HO
75%
Fat
10%
Con
ven
tion
alA
DA
diet
C60
–70%
Fat<
7%sa
tura
ted
fat
Yes
Wei
ght
chan
ge
P=.6
5∗
Veg
an:(P<.0
1)−1
.9±
0.6.
Con
ven
tion
al:
(P<.0
1)−2
.4±
0.13
P=.0
3∗
(on
lyu
sin
gda
tapr
ior
tom
edia
nad
just
men
ts)
Veg
an:
(P<.0
1)−0
.4±
0.14
Con
ven
tion
al:
(P=
NS)
0.01±
0.8
P=.0
1To
talc
hol
este
rol
decr
ease
dm
ore
inve
gan
grou
p
8

14 Journal of Nutrition and Metabolism
Ta
ble
3:C
onti
nu
ed.
Au
thor
/yea
r/co
un
try
Des
ign
Stu
dyle
ngt
h(w
eek)
Subj
ects
Die
tary
inte
rven
tion
Ou
tcom
esQ
ual
ity
rati
ng
Die
tde
tails
Con
trol
for
wei
ght
loss
diff
eren
ces?
ΔC
RP
ΔH
bA1c
%O
ther
Dos
tlov
aet
al.
(200
9),C
zech
Rep
ubl
ic[2
1]
Qu
asi-
expe
rim
enta
lon
egr
oup
wit
htw
oco
mpa
riso
ngr
oups
(mon
itor
edin
the
hos
pita
l)
2
T2D
Mgr
oup
n=
14F
only
μag
e=
56.1
Ver
y-lo
w-c
alor
iedi
et(5
50kc
al/d
ay)
No
P<.0
5(Δ
inμ
CR
Ppr
e:13
.2±
3.5/
post
:7.
1±
2.4)
Fast
ing
glu
cose
P<.0
5(Δ
inμ
fast
ing
glu
cose
pre/
post
)
HO
MA
:P<.0
55
Koz
łow
ska
etal
.(2
010)
,Pol
and
[22]
Qu
asi-
exp
erim
enta
l(o
ne-
grou
ppr
etes
t-po
stte
st)
8
N=
17F=
41%
M=
59%
μag
e=
66.6
Low
ener
gy/L
owpr
otei
ndi
et(2
0%en
ergy
defi
cit,
0.8–
1.0
g/kg
)C
HO
60%
F30
%
No
P=.7
78(Δ
inμ
CR
Ppr
e/po
stin
terv
enti
on)
pre:
2.6
(0.4
–13.
9)po
st:3
.4(0
.3–1
2.4)
P=.4
85(Δ
inμ
HbA
1c
pre/
pos
tin
terv
enti
on)
pre:
7.7±
1.4
post
:7.3±
1.4
P=.0
02(Δ
inμ
TN
Fpr
e/po
stin
terv
enti
on)
pre:
10.6±
7.5
post
:7.8±
5.1
4
Vet
ter
etal
.(20
10),
U.S
.[17
]R
CT
subg
rou
p26
N=
79F=
11%
M=
89%
μag
e=
59.7
Low
-car
bC
HO<
30g/
day
vers
us
Low
-fat
(DP
Pdi
et)
Fat<
30%
+50
0kc
al/d
ayde
fici
t
No
Not
mea
sure
d
P=
NS∗
Ch
ange
sin
HbA
1c
Low
-car
b:−0
.6(1
.2)
Low
-fat
:−0
.1(1
.2)
TN
F-α
P=
NS∗
Ch
ange
sin
TN
FLo
w-c
arb:
−1.5
(7.1
)Lo
w-f
at:
−1.5
(5.6
)
4
Aza
dbak
ht
etal
.(2
011)
,stu
dyco
ndu
cted
inIr
an.
[18]
Cro
ss-o
ver
wit
hra
ndo
miz
atio
n(w
ith
4w
eek
was
hou
tp
erio
d)
8
N=
31F=
59%
M=
41%
μag
e=
55
DA
SHdi
etC
HO
50–6
0%Fa
t<
30%
∗ Hig
hin
wh
ole
grai
ns,
fru
its,
vege
tabl
es.L
owso
diu
mve
rsu
sco
ntr
oldi
et
Yes
Wei
ght
chan
ge
P=.0
3∗
DA
SH:
pre:
2.9±
0.31
post
:2.0
3±
0.27
Con
trol
:pr
e:3.
11±
0.30
post
:2.9
2±
0.20
No
mea
sure
ofgl
ycem
icco
ntr
ol
Fibr
inog
en:
P=.0
01∗
DA
SH:
μch
ange
:38.
7C
ontr
ol:
μch
ange
:140
10
Boz
zett
oet
al.
(201
1),
Ital
y[1
9]
Pre
exp
erim
enta
lpo
stte
ston
ly.
Cro
ss-o
ver
wit
hra
ndo
miz
atio
n(n
ow
ash
out)
4
N=
12F=
25%
M=
75%
μag
e=
59
Hig
h-c
arb/
hig
h-
fibe
r/lo
wG
IC
HO
52%
MU
FA17
%∗ G
I58
%ve
rsu
sH
igh
-MU
FAdi
etC
HO
45%
MU
FA23
%∗ G
I88
%
No
MU
FAm
eal:
P<.0
5(Δ
inμ
CR
Pw
hen
com
pare
dw
ith
fast
ing
CR
P)
Fast
ing:
2.11±
2.02
3h
:1.9
8±
1.99
6h
:2±
2.06
NSΔ
inμ
CR
Paf
ter
CH
O/fi
ber
mea
l
No
mea
sure
ofgl
ycem
icco
ntr
olN
A6

Journal of Nutrition and Metabolism 15
Ta
ble
3:C
onti
nu
ed.
Au
thor
/yea
r/co
un
try
Des
ign
Stu
dyle
ngt
h(w
eek)
Subj
ects
Die
tary
inte
rven
tion
Ou
tcom
esQ
ual
ity
rati
ng
Die
tde
tails
Con
trol
for
wei
ght
loss
diff
eren
ces?
ΔC
RP
ΔH
bA1c
%O
ther
Dav
iset
al.(
2011
),U
.S.[
26]
2gr
oups
pret
est-
post
test
wit
hra
ndo
miz
atio
nsu
bgro
up
ofla
rger
tria
l
24
N=
51F=
76%
M=
24%
μag
e=
54.5
Low
-fat
(DP
Pdi
et)
Fat<
25%
vers
us
Low
-CH
O(A
tkin
sdi
et)
CH
O<
20%
Yes,
wei
ght
loss
equ
albe
twee
ngr
oups
Low
-fat
:P=.0
1Δ
inμ
CR
Ppr
e:4.
0±
0.77
post
:3.0±
0.77
Low
-CH
O:P=.9
4Δ
inμ
CR
Ppr
e:3.
1±
0.42
post
:3.6±
0.68
P=.7
2n
sμ
HbA
1cre
duce
dby
0.18±
0.16
for
pool
edgr
oups
IL-6
ns
μW
tlo
ss:1
1lb
.P=.7
2fo
rpo
oled
grou
ps
9
Itsi
opou
los
etal
.(2
010)
,Au
stra
lia[2
0]
Cro
ss-o
ver
wit
hra
ndo
miz
atio
n(n
ow
ash
out)
24
N=
27F=
41%
M=
16%
μag
e=
59
Med
iter
ran
ean
Die
t:C
HO
44%
Fat
40%
(>50
%M
UFA
)ve
rsu
sC
ontr
oldi
et:a
dlib
.
No
P=.5
76∗
Med
diet
:2.
38[1
.66,
3.10
]C
ontr
ol:
2.49
[1.6
9,3.
30]
P=.0
12∗
Med
diet
:6.
8[6
.3,7
.3]
Con
trol
:7.
1[6
.5,7
.7]
HO
MA
,P=.0
61∗
Med
diet
:5.
2(3
.9,6
.6)
Con
trol
:6.
1(4
.4,7
.8)
7
Kh
ooet
al.(
2011
),A
ust
ralia
[28]
2gr
oups
pret
est-
post
test
wit
hra
ndo
miz
atio
n52
N=
31M
only
μag
e=
60.2
Low
-cal
orie
diet
900
kcal
/day
vers
us
Hig
h-p
rote
in,
low
-fat
Fat<
30%
+60
0kc
al/d
ayde
fici
t
No
Low
-cal
orie
:NS
pre:
3.82±
1po
st(5
2w
eeks
):3.
79±
0.82
Hig
h-p
rote
in:
P<.0
1pr
e:8.
32±
1.29
post
(52
wee
ks):
2.85±
1.01
Not
prov
ided
,ch
ange
inpl
asm
agl
uco
sew
asn
s.
IL-6
Low
-cal
orie
:P=
NS
pre:
1.59±
0.29
post
(52
wee
ks):
1.7±
0.42
Hig
h-p
rote
in:P
=N
Spr
e:3.
28±
0.37
post
(52
wee
ks):
2.4±
0.52
(P<.0
5gr
oup
and
tim
eeff
ect)
7
Mra
zet
al.(
2011
),C
zech
Rep
ubl
ic[2
3]
Qu
asi-
exp
erim
enta
lde
sign
wit
htw
oco
mpa
riso
ngr
oups
2N=
35F
only
μag
e=
65.6
Ver
y-lo
w-c
alor
iedi
et60
0kc
al/d
ayH
ealt
hyan
dob
ese
subj
ects
did
not
rece
ive
diet
No
μΔ
inC
RP
pre/
post=
0.94
mg/
LP<.0
5R
awda
tan
otpr
ovid
ed
Not
prov
ided
μΔ
inIL
-6pr
e/p
ost=
0.8
pg/
mL
P<.0
5
4
Not
e:C
RP
:C-r
eact
ive
prot
ein
;HbA
1c:g
lyco
syla
ted
hem
oglo
bin
;F:f
emal
es;M
:mal
es;μ
:mea
n;μ
age:
mea
nag
e;Δ
:ch
ange
in;H
OM
A:h
omeo
stat
icm
odel
asse
ssm
ent;
DP
P:D
iabe
tes
Pre
ven
tion
Pro
gram
;DA
SH:
Die
tary
App
roac
hes
toSt
opH
yper
ten
sion
;G
I:G
lyce
mic
Inde
x;M
UFA
:m
onou
nsa
tura
ted
fatt
yac
id;
ns:
not
sign
ifica
nt;
C:
ener
gyfr
omca
rboh
ydra
tes;
F:en
ergy
from
fat;∗ :
Sign
ifica
nce
ofbe
twee
ngr
oup
diff
eren
ces.
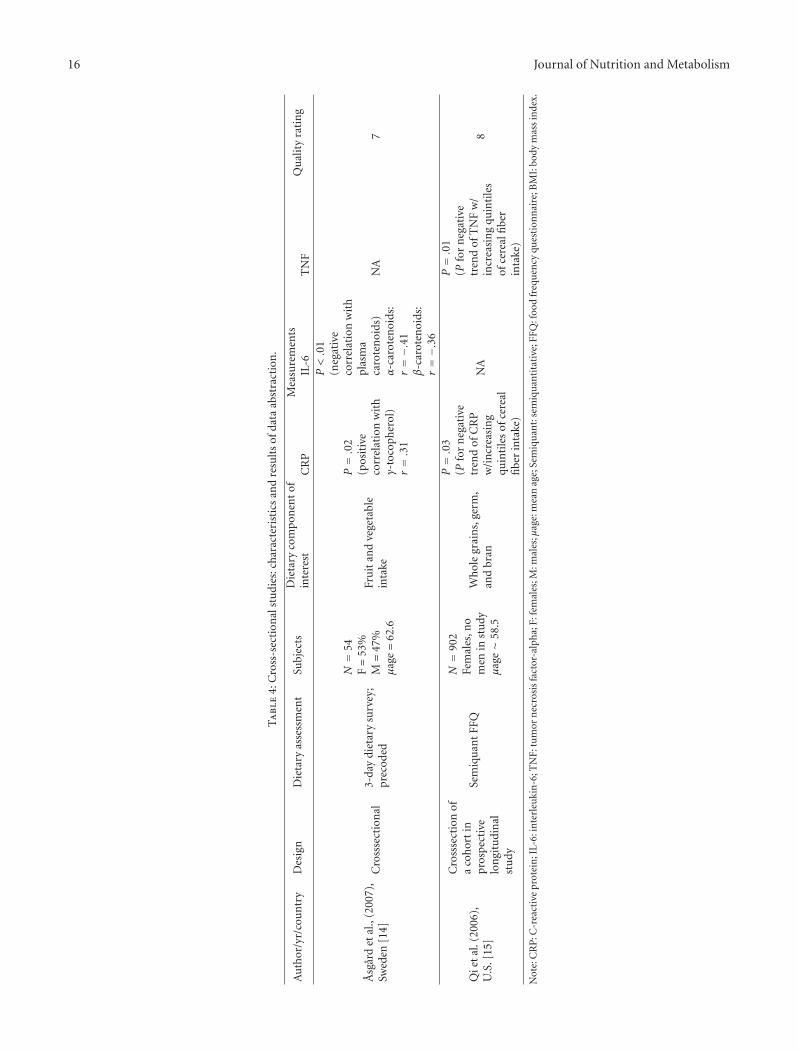
16 Journal of Nutrition and Metabolism
Ta
ble
4:C
ross
-sec
tion
alst
udi
es:c
har
acte
rist
ics
and
resu
lts
ofda
taab
stra
ctio
n.
Au
thor
/yr/
cou
ntr
yD
esig
nD
ieta
ryas
sess
men
tSu
bjec
tsD
ieta
ryco
mpo
nen
tof
inte
rest
Mea
sure
men
tsQ
ual
ity
rati
ng
CR
PIL
-6T
NF
Asg
ard
etal
.,(2
007)
,Sw
eden
[14]
Cro
ssse
ctio
nal
3-da
ydi
etar
ysu
rvey
;pr
ecod
ed
N=
54F=
53%
M=
47%
μag
e=
62.6
Fru
itan
dve
geta
ble
inta
ke
P=.0
2(p
osit
ive
corr
elat
ion
wit
hγ-
toco
pher
ol)
r=.3
1
P<.0
1(n
egat
ive
corr
elat
ion
wit
hpl
asm
aca
rote
noi
ds)
α-c
arot
enoi
ds:
r=−.
41β
-car
oten
oids
:r=−.
36
NA
7
Qie
tal
.(20
06),
U.S
.[15
]
Cro
ssse
ctio
nof
aco
hor
tin
pros
pec
tive
lon
gitu
din
alst
udy
Sem
iqu
ant
FFQ
N=
902
Fem
ales
,no
men
inst
udy
μag
e∼
58.5
Wh
ole
grai
ns,
germ
,an
dbr
an
P=.0
3(P
for
neg
ativ
etr
end
ofC
RP
w/i
ncr
easi
ng
quin
tile
sof
cere
alfi
ber
inta
ke)
NA
P=.0
1(P
for
neg
ativ
etr
end
ofT
NF
w/
incr
easi
ng
quin
tile
sof
cere
alfi
ber
inta
ke)
8
Not
e:C
RP
:C-r
eact
ive
prot
ein
;IL-
6:in
terl
euki
n-6
;TN
F:tu
mor
nec
rosi
sfa
ctor
-alp
ha;
F:fe
mal
es;M
:mal
es;μ
age:
mea
nag
e;Se
miq
uan
t:se
miq
uan
tita
tive
;FFQ
:foo
dfr
equ
ency
ques
tion
nai
re;B
MI:
body
mas
sin
dex.

Journal of Nutrition and Metabolism 17
3-hour postprandial, and 6-hour postprandial following 4weeks of a diet high in MUFAs, compared to the alternatediet which was high in carbohydrates and fiber with a lowglycemic index (P < .05) [19]. A study by Giannopoulouet al. [27] also demonstrated the anti-inflammatory effectsof a diet high in MUFAs (see Table 1). This study was 14weeks long, and comparison groups included an exercise-only group and a group that was prescribed exercise as wellas the high MUFA diet. All three groups demonstrated asignificant reduction in mean-CRP at final data collection(P < .01); however, there was not a significant difference inthis reduction between groups [27]. It is interesting to notehere that the diet and exercise group did not have a greaterdecrease in inflammatory markers than the diet-only group.These results indicate that exercise may not add benefit toimproving inflammatory markers in patients with T2D. Inanother longitudinal study, Barnard et al. [24] randomized99 participants to receive either a low-fat vegan diet or aconventional American Diabetes Association (ADA) diet for74 weeks. Results showed a significant reduction of CRPwithin groups (P < .01 for each group) but a nonsignificantdifference between the two diet groups [24], perhaps dueto the similar macronutrient content of the two dietaryinterventions.
Following on the premise that increased fat mass inT2D contributes to inflammation, three other studies imple-mented diets that were low or very low in energy content[21–23]. Kozłowska et al. [22] implemented a diet with a20% energy deficit and low protein for eight weeks withouta comparison group. This diet did not produce a significantreduction in CRP; however, the 17 participants did exhibitsignificantly lower TNF-α levels (P = .002) following theintervention [22]. Additional two studies implemented twoweeks of a very-low-calorie diet (VLCD) with obese subjectswith T2D in highly controlled hospital environments [21,23]. Dostlova et al. [21] demonstrated a significant dropin mean-CRP after two weeks of following a VLCD diet(P < .05). Mraz et al. [23] found that 2 weeks of a VLCDsignificantly decreased mean-CRP (P < .05), as well asdecreased IL-6 levels (P < .05). Although significant resultswere found, such diets cannot be maintained, and as such thelong-term effects are not known.
Marfella et al. [16] conducted an RCT in Italy withtwo groups that were advised to follow a Mediterranean-style diet. The Mediterranean diet is characterized by threeservings of fruits and six servings of vegetables or wildleafy greens per day [31]. Fish is consumed 5 to 6 timesper week and contributes to the main source of fat, whichis monounsaturated and polyunsaturated. The interventiongroup consumed 4 oz. of red wine per day, while the controlgroup abstained from alcohol. Results revealed significantlygreater reductions in CRP (P < .01), TNF-α (P < .01), andIL-6 (P < .01) in the intervention group compared to thecontrol group after the 52-week study period [16].
In contrast, there were several diets that did notalter inflammatory marker expression significantly. Theseincluded the high-carbohydrate/high-fiber/low-glycemicindex diet [19], the low-carbohydrate diet implemented byDavis et al. [26], the low-carbohydrate and DPP-style diet
implemented by Vetter et al. [17], and the Mediterraneandiet [20].
The two cross-sectional studies included in this analysisexamined associations between two different aspects of dietand differed significantly in terms of quality in reporting.Asgard et al. [14] quantified fruit and vegetable intake, whileQi et al. [15] categorized whole grain, germ, and bran intakeinto quintiles. Qi et al. demonstrated a significant associationbetween CRP and the dietary intake of interest, showingthat with increasing quintiles of cereal fiber intake, CRP wassignificantly lower (P for trend = .03) [15]. This inverserelationship was also present between TNF-α and cerealfiber intake (P for trend = .01). Asgard et al. [14] alsodemonstrated a significant inverse correlation between alpha(α) and beta (β) carotenoids (foods that contain vitamin A)and inflammation (r = −.41 and r = −.36, resp.).
6.2. Diet Influences Glycemic Control. The positive influenceof a dietary intervention on glycemic control [16, 20, 21, 24,27] was examined in five studies. Dostlova et al. [21] mea-sured fasting blood glucose (FBG) as a proxy for glycemiccontrol and demonstrated a significant improvement inFBG following the two-week dietary intervention of a very-low-calorie diet (P < .05). Itsiopoulos et al. [20] alsodemonstrated an improvement in glycemic control followinga 24-week crossover intervention with a Cretan Mediter-ranean diet as evidenced by a significantly reduced meanglycosylated hemoglobin (HbA1c) (P = .012), compared tothe control diet which was the participants’ normal eatingpattern. Both studies also demonstrated improvement in thehomeostatic model assessment (HOMA) score, a measureof insulin resistance (see Table 1), although this change wasnot statistically significant following the Mediterranean diet[20, 21]. A third study by Barnard et al. [24] found thatafter following a vegan diet for 72 weeks, subjects hadsignificantly improved HbA1c levels compared to those whofollowed a conventional diet as recommended by the ADA(P = .03) (see Table 3). A Mediterranean diet was alsoimplemented by Marfella et al. [16], along with either fourounces per day of red wine or no alcohol. HbA1c levelswere not significantly different between the two groups;however, the mean change in HbA1c was greater than inall other studies included in this review (−1.1% for theintervention group and −1.2% for the control group) [16].The clinical significance of such a large change in HbA1c willbe discussed later. Finally, Giannopoulou et al. [27] reportedthat although none of the intervention groups demonstrateda significant improvement in HbA1c, both the diet-only anddiet and exercise groups had a significant reduction in fastingglucose levels (P < .05 for both groups). Interestingly, onlythe two interventions with exercise produced a significantreduction in insulin resistance [27].
7. Discussion
The great variability between studies decreases the abilityto draw definitive conclusions about associations betweendiet, inflammation, and T2D; however, particular themes

18 Journal of Nutrition and Metabolism
emerged that are worth noting both from this review andin light of previous research. First, of the ten different dietsprescribed that were low in fat, both within and acrossstudies, eight of those diets led to significant reductions ininflammatory markers. These included the DASH diet [18],the low-fat DPP-style diet [26], the low-energy low-proteindiet [22], the vegan and ADA diets [24], the high-proteinlow-fat diet [28], and both the high-protein and low-proteindiets [25]. However, this review also supported the hypothe-sis that the high-MUFA diet decreased inflammation.
Previous reports from the Whitehall and PREDIMEDstudies indicated that diets high in MUFA and polyunsat-urated fatty acids (PUFAs) were correlated with decreasedCRP [32, 33] and IL-6 [33], while diets high in saturated fattyacids were positively correlated with CRP [32]. High intakeof PUFA was also inversely correlated with incidence of T2Din the Nurse’s Health Study [3]. Therefore, it was not sur-prising that the High-MUFA diet showed anti-inflammatoryeffects in the diabetic population [16, 19, 20, 29]. Bozzetto etal. [19] lacked baseline values for participants; therefore, it isnot appropriate to infer causality for a change in CRP overthe 4 weeks of the study period, but rather only in the acutepostprandial response. Unfortunately, glycemic control wasnot concurrently assessed.
Dietary patterns, as opposed to specific aspects of diet,have also been shown to correlate with levels of chronicinflammatory markers, but this concept was not adequatelyexamined in the selected studies. For example, the westerndietary pattern, characterized by a high consumption ofsugary drinks, red meat, and poultry and a low consumptionof fruits, vegetables, and fiber, was correlated with higherlevels of CRP in two large cross-sectional studies conductedin the US [34, 35].
The impact of diet on the metabolic milieu of T2Dis evident from the results of this integrative review andothers. However, statistical significance does not necessarilytranslate into clinical significance or meaningfulness. Forexample, of the two studies that were able to demonstratea significantly reduced HbA1c following the prescribed diet,one failed to report baseline values of glycemic control,[20] and the other only demonstrated a mean reductionof 0.4% [24]. While this result is statistically significant, itmight not result in improvement in long-term outcomes ofT2D, as demonstrated by findings from the United KingdomProspective Diabetes Study [36], which showed that a 1%reduction in HbA1c levels can lead to improvements inlong-term outcomes and decreased mortality [36]. Theimplementation of a Mediterranean-style diet and a glass ofred wine per day produced a mean decrease in HbA1c of1.1% (±0.06) [16]. The control group that did not receivethe red wine intervention but did follow a Mediterraneandiet had a similar decrease in HbA1c, as well as CRP, TNF-α, and IL-6 [16]. The reductions in HbA1c were not foundto be significantly different between intervention and controlgroups, though the drop in this important glycemic markeris clinically relevant, as it points to decreased incidence ofdiabetes-related complications and decreased mortality [36].
To further increase their clinical relevance, it is impor-tant for studies implementing dietary changes to examine
sustainability of the prescribed diet. Although both studiesof VLCD reported significant decreases in inflammatorymarkers, such a diet is not sustainable and is likely harmfulfor the individuals as evidenced by the significant increasein TNF-α following the 2-week VLCD implemented by Mrazet al. [23]. The rationale behind this intensive diet is rapidimprovement in metabolic parameters. The lack of long-term followup of the selected patients prevents us fromextrapolating from these findings that patients will havesustained results. In fact, the crossover experimental studyby Khoo et al. [28] illuminates that after 52 weeks of theprescribed diets, the group that initially received a low-calorie diet did not show a significant decrease in CRP,while the group that was prescribed the high-protein, low-fat diet for all 52 weeks did achieve significant reductionsin CRP. This highlights that there may not be merit behindthe rapid weight-loss from calorie-restricted programs in theaforementioned studies.
7.1. Gaps in Knowledge in the State of the Science. Due tothe limited availability of data for analysis on this topic andthe suboptimal quality of reporting within the studies, theresults of this integrative review are inconclusive. Many of thestudies reviewed suffered from significant methodologicalshortcomings. First, most of the studies had small samplesizes, with a range between 12 and 162 (mean sample size of53, and median of 32), limiting the power of the interventionto detect an effect. The two studies with the largest samplesizes implemented the low-glycemic-index diet and Mediter-ranean diet with wine and showed significant reductionin inflammatory marker expression [16, 29]. Only threestudies included in this integrative review conducted a poweranalysis [18, 24, 29], and one conducted a retrospectivepower analysis [25], which is paramount in substantiatingfindings or validating the need for further research if thefindings were insignificant.
Second, several studies did not include transparentdefinitions of the dietary intervention, rendering it difficultto infer specific dietary factors that decrease inflammationfrom the results. In previous studies with healthy volunteers,decreased inflammation was correlated with several individ-ual dietary factors including fiber, antioxidant vitamins suchas vitamin C and carotenoids, and fruit and vegetable intake.For example, in large prospective studies, whole grain intakehas been associated with both decreased inflammatory mark-ers [37] and decreased incidence of T2D [38]. Of the threeexperimental studies in the current review that indicatedwhole grains as an aspect of the diet, only one demonstrateddecreased CRP levels following the intervention [18]. Sim-ilarly, the cross-sectional study examining intake of wholegrains showed an inverse association between increasingintake of cereal fiber and CRP levels [15]. However, onestudy that implemented a high-carbohydrate, high-fiber dietand another that implemented a Cretan-Mediterranean diet,both of which are high in fiber, failed to demonstrate adecrease in CRP following the intervention [19, 20].
A third and final gap in knowledge related to thistopic is adherence and change over time. Though several

Journal of Nutrition and Metabolism 19
studies included in this study were longitudinal, the longeststudy was 74 weeks, which does not necessarily indicatethat benefits obtained will be sustained in the long-term.This issue was highlighted in the study by Brinkworth etal. [25] in which two low-fat diets, one low-protein, andone high-protein were prescribed to 38 participants withregular dietary counseling for the first 12 weeks. At 12weeks, HbA1c had decreased by 9.4% (P < .001) in bothgroups [39]. Results in glycemic control were attenuated,however, at 64 weeks due to the fact that participants hadnot received regular dietary counseling between weeks 12 and64 [25]. Recidivism such as this will likely be experienced inother long-term studies, underscoring the need for consistentcounseling as well as followup in long-term studies thatrequire behavior change [40].
7.2. Limitations. There are several limitations of this integra-tive review. First, the review is limited to the published litera-ture, so it is subject to publication bias. Several authors werecontacted via email with requests for unpublished research,but none were available. Second, the articles reviewed foranalysis only included a population with diagnosed T2D.This limited the available literature on the influence of dieton inflammation and glycemic control markedly. There ismerit in restriction of the search to this population, giventhat their inflammatory markers will be elevated relative tothe general population and would, therefore, benefit fromdietary changes in a more clinically significant way. However,this strength may have limited the conclusions in this paper.Finally, it should be noted that this integrative review doesnot address the mechanism of action underlying reductionof systemic inflammation following a dietary intervention.Discussion of such is beyond the scope of this paper. Thereview by Visioli et al. [41] concluded that antioxidants,essential fatty acids, and plant extracts have been shown toreduce systemic inflammation. Extrapolating results fromthis integrative review to make inferences about specificnutrient effects is not possible; however, it can be inferredthat nutrient content of the Mediterranean, vegan, and ADAdiets may contain more of those qualities mentioned in thereview [41].
7.3. Implication for Future Research. Given the limitationsof the findings and the inconclusive results reached by thisreview, it is clear that more rigorous research is needed. Thepresent level of evidence on this topic is Level III, giventhat most of the studies were quasiexperimental. This paper,therefore, increases the level of evidence by providing anintegrative review of the available research. However, dis-parate methods of reporting findings have rendered synthesisof extant findings difficult and unnecessarily labor-intensive.Studies should adhere to the transparent reporting standardsoutlined by the Consolidated Standards of Reporting Trials[42]. Researchers should also focus their efforts on increasingvalidity and reliability in research conduct. Adherence todietary interventions needs to be reported and included inanalysis of the findings, possibly by including a measure ofadherence as a regression variable. Failure to include this
critical factor could explain the variability in the findings ofthis integrative review, for a dose response is a likely influencein the success or failure of an intervention effect. Adequately-powered, high quality studies examining the associationbetween dietary intake and inflammation in T2D are alsoneeded.
Medical nutrition therapy is one aspect of preventionand care of T2D recommended by the ADA. Although theDPP demonstrated a reduction in the incidence of T2Dfollowing the adaptation of lifestyle changes, there have beenfew studies examining the influence of dietary interventionson inflammation and glycemic control in individuals withestablished T2D in the US. It is important to conductthese studies domestically because of the diversity of thepopulations affected by this disease and the increasingrates of T2D. For example, further analysis of the resultsfrom the DPP revealed an attenuated benefit from theintervention in non-Hispanic Black women, highlightingthe need for an understanding of the complex socioculturalfactors influencing the African American population [43].Studies examining the current dietary practices of individu-als diagnosed with T2D are necessary, with a particular focuson differences in culturally-bound beliefs surrounding diet,food, and health.
None of the studies included in this review used atheoretical framework to guide the research, which couldhave contributed to the disparate findings of the includedstudies. Theoretical frameworks guide research questionsand facilitate the process of asking a complete question.Considering that T2D is both a metabolic and inflammatorydisease, it is imperative to design studies that address both ofthese issues in the methods and the outcome measures. Forexample, if an intervention of a high MUFA diet is imple-mented, it may be helpful not only to address inflammatorymarkers in the outcome measures, but also other influenceson inflammation that could confound results such as physicalactivity, socioeconomic status, environmental stressors, andgenetic factors as suggested by Kang’s Biobehavioral Modelof Stress and Inflammation [10]. It is unclear from theaforementioned studies how exercise, stress, and geneticscontributed to the metabolic and inflammatory outcomesmeasured, and larger, more rigorous studies are needed thatcontrol these variables. Finally, based on the results of theaforementioned studies, RCTs using participants with T2Dare needed for which the nutrition content of the dietaryintervention has been optimized for the treatment of T2D.This includes high intake of fruits and vegetables that arehigh in flavonoids, which Gonzalez-Castejon and Rodriguez-Casado [44] report in their review on phytochemicals tohave anti-inflammatory and antioxidant activities that mayimprove the metabolic status of individuals with T2D.The Mediterranean diet is an extremely palatable diet richin fruits, vegetables, fiber, and olive oil which has beenshown with and without the addition of alcohol to improveinflammation, prevent the onset of T2D, and improveglycemic control in established T2D [16, 41, 44]. More high-quality RCTs implementing this diet are needed to providethe evidence base for modifying clinical practice guidelinesin medical nutrition therapy for patients with T2D.
20 Journal of Nutrition and Metabolism
References
[1] Centers for Disease Control and Prevention, National DiabetesFact Sheet: National Estimates and General Information onDiabetes and Prediabetes in the United States, U.S. Departmentof Health and Human Services, Centers for Disease Controland Prevention, Atlanta, Ga, USA, 2011.
[2] D. Grotto and E. Zied, “The standard American diet and itsrelationship to the health status of Americans,” Nutrition inClinical Practice, vol. 25, no. 6, pp. 603–612, 2010.
[3] J. Salmeron, F. B. Hu, J. E. Manson et al., “Dietary fat intakeand risk of type 2 diabetes in women,” American Journal ofClinical Nutrition, vol. 73, no. 6, pp. 1019–1026, 2001.
[4] A. Astrup and N. Finer, “Redefining type 2 diabetes: “Dia-besity” or “obesity dependent diabetes mellitus”?” ObesityReviews, vol. 1, no. 2, pp. 57–59, 2000.
[5] W. C. Knowler, E. Barrett-Connor, S. E. Fowler et al.,“Reduction in the incidence of type 2 diabetes with lifestyleintervention or metformin,” The New England Journal ofMedicine, vol. 346, no. 6, pp. 393–403, 2002.
[6] M. P. Stern, “Diabetes and cardiovascular disease: the “com-mon soil” hypothesis,” Diabetes, vol. 44, no. 4, pp. 369–374,1995.
[7] R. C. Turner, H. Millns, H. A. W. Neil et al., “Risk factorsfor coronary artery disease in non-insulin dependent dia-betes mellitus: United Kingdom prospective diabetes study(UKPDS: 23),” British Medical Journal, vol. 316, no. 7134, pp.823–828, 1998.
[8] A. G. Bertoni, G. L. Burke, J. A. Owusu et al., “Inflammationand the incidence of type 2 diabetes: the Multi-Ethnic Studyof Atherosclerosis (MESA),” Diabetes Care, vol. 33, no. 4, pp.804–810, 2010.
[9] B. B. Duncan, M. I. Schmidt, J. S. Pankow et al., “Low-grade systemic inflammation and the development of type2 diabetes: the atherosclerosis risk in communities study,”Diabetes, vol. 52, no. 7, pp. 1799–1805, 2003.
[10] D. H. Kang, M. Rice, N. J. Park, A. Turner-Henson, and C.Downs, “Stress and inflammation: a biobehavioral approachfor nursing research,” Western Journal of Nursing Research, vol.32, no. 6, pp. 730–760, 2010.
[11] C. M. Kastorini and D. B. Panagiotakos, “Dietary patternsand prevention of type 2 diabetes: from research to clinicalpractice—a systematic review,” Current Diabetes Reviews, vol.5, no. 4, pp. 221–227, 2009.
[12] M. A. Martınez-Gonzalez, C. De La Fuente-Arrillaga, J. M.Nunez-Cordoba et al., “Adherence to Mediterranean diet andrisk of developing diabetes: prospective cohort study,” BMJ,vol. 336, no. 7657, pp. 1348–1351, 2008.
[13] F. Centritto, L. Iacoviello, R. di Giuseppe et al., “Dietarypatterns, cardiovascular risk factors and C-reactive proteinin a healthy Italian population,” Nutrition, Metabolism andCardiovascular Diseases, vol. 19, no. 10, pp. 697–706, 2009.
[14] R. Asgard, E. Rytter, S. Basu, L. Abramsson-Zetterberg, L.Moller, and B. Vessby, “High intake of fruit and vegetables isrelated to low oxidative stress and inflammation in a group ofpatients with type 2 diabetes,” Scandinavian Journal of Foodand Nutrition, vol. 51, no. 4, pp. 149–158, 2007.
[15] L. Qi, R. M. Van Dam, S. Liu, M. Franz, C. Mantzoros, and F. B.Hu, “Whole-grain, bran, and cereal fiber intakes and markersof systemic inflammation in diabetic women,” Diabetes Care,vol. 29, no. 2, pp. 207–211, 2006.
[16] R. Marfella, F. Cacciapuoti, M. Siniscalchi et al., “Effect ofmoderate red wine intake on cardiac prognosis after recent
acute myocardial infarction of subjects with Type 2 diabetesmellitus,” Diabetic Medicine, vol. 23, no. 9, pp. 974–981, 2006.
[17] M. L. Vetter, A. Wade, L. G. Womble, C. Dalton-Bakes, T.A. Wadden, and N. Iqbal, “Effect of a low-carbohydrate dietversus a low-fat, calorie-restricted diet on adipokine levelsin obese, diabetic participants,” Diabetes, Metabolic Syndromeand Obesity, vol. 3, pp. 357–361, 2010.
[18] L. Azadbakht, P. J. Surkan, A. Esmaillzadeh, and W. C.Willett, “The dietary approaches to stop hypertension eatingplan affects C-reactive protein, coagulation abnormalities, andhepatic function tests among type 2 diabetic patients,” Journalof Nutrition, vol. 141, no. 6, pp. 1083–1088, 2011.
[19] L. Bozzetto, C. De Natale, L. Di Capua et al., “The associationof hs-CRP with fasting and postprandial plasma lipids inpatients with type 2 diabetes is disrupted by dietary monoun-saturated fatty acids,” Acta Diabetologica. In press.
[20] C. Itsiopoulos, L. Brazionis, M. Kaimakamis et al., “Can theMediterranean diet lower HbA1c in type 2 diabetes? Resultsfrom a randomized cross-over study,” Nutrition, Metabolismand Cardiovascular Diseases, vol. 21, no. 9, pp. 740–747, 2010.
[21] I. Dostlova, T. Roubcek, M. Brtlov et al., “Increasedserum concentrations of macrophage inhibitory cytokine-1 in patients with obesity and type 2 diabetes mellitus:the influence of very low calorie diet,” European Journal ofEndocrinology, vol. 161, pp. 397–404, 2009.
[22] L. Kozłowska, A. Rydzewski, B. Fiderkiewicz, A. Wasinska-Krawczyk, A. Grzechnik, and D. Rosołowska-Huszcz,“Adiponectin, resistin and leptin response to dietaryintervention in diabetic nephropathy,” Journal of RenalNutrition, vol. 20, no. 4, pp. 255–262, 2010.
[23] M. Mraz, Z. Lacinova, J. Drapalova et al., “The effect ofvery-low-calorie diet on mRNA expression of inflammation-related genes in subcutaneous adipose tissue and peripheralmonocytes of obese patients with type 2 diabetes mellitus,”Journal of Clinical Endocrinology and Metabolism, vol. 96, no.4, pp. E606–E613, 2011.
[24] N. D. Barnard, J. Cohen, D. J. A. Jenkins et al., “A low-fatvegan diet and a conventional diabetes diet in the treatmentof type 2 diabetes: a randomized, controlled, 74-wk clinicaltrial,” American Journal of Clinical Nutrition, vol. 89, no. 5, pp.1588S–1596S, 2009.
[25] G. D. Brinkworth, M. Noakes, B. Parker, P. Foster, and P.M. Clifton, “Long-term effects of advice to consume a high-protein, low-fat diet, rather than a conventional weight-lossdiet, in obese adults with Type 2 diabetes: one-year follow-upof a randomised trial,” Diabetologia, vol. 47, no. 10, pp. 1677–1686, 2004.
[26] N. J. Davis, J. P. Crandall, S. Gajavelli et al., “Differential effectsof low-carbohydrate and low-fat diets on inflammation andendothelial function in diabetes,” Journal of Diabetes and ItsComplications, vol. 25, pp. 371–376, 2011.
[27] I. Giannopoulou, B. Fernhall, R. Carhart et al., “Effects ofdiet and/or exercise on the adipocytokine and inflammatorycytokine levels of postmenopausal women with type 2 dia-betes,” Metabolism, vol. 54, no. 7, pp. 866–875, 2005.
[28] J. Khoo, C. Piantadosi, R. Duncan et al., “Comparing effectsof a low-energy diet and a high-protein low-fat diet onsexual and endothelial function, urinary tract symptoms,and inflammation in obese diabetic men,” Journal of SexualMedicine, vol. 8, pp. 2868–2875, 2011.
[29] T. M. S. Wolever, A. L. Gibbs, C. Mehling et al., “The CanadianTrial of Carbohydrates in Diabetes (CCD), a 1-y controlledtrial of low-glycemic-index dietary carbohydrate in type 2
Journal of Nutrition and Metabolism 21
diabetes: no effect on glycated hemoglobin but reduction inC-reactive protein,” American Journal of Clinical Nutrition, vol.87, no. 1, pp. 114–125, 2008.
[30] R. Whittemore and K. Knafl, “The integrative review: updatedmethodology,” Journal of Advanced Nursing, vol. 52, no. 5, pp.546–553, 2005.
[31] J. Moschandreas and A. Kafatos, “Food and nutrient intakesof Greek (Cretan) adults. Recent data for food-based dietaryguidelines in Greece,” British Journal of Nutrition, vol. 81,supplement 2, pp. S71–S76, 1999.
[32] R. Clarke, M. Shipley, J. Armitage, R. Collins, and W. Harris,“Plasma phospholipid fatty acids and CHD in older men:whitehall study of London civil servants,” British Journal ofNutrition, vol. 102, no. 2, pp. 279–284, 2009.
[33] J. Salas-Salvado, A. Garcia-Arellano, R. Estruch et al., “Com-ponents of the mediterranean-type food pattern and seruminflammatory markers among patients at high risk for cardio-vascular disease,” European Journal of Clinical Nutrition, vol.62, no. 5, pp. 651–659, 2008.
[34] T. T. Fung, F. B. Hu, M. A. Pereira et al., “Whole-grain intakeand the risk of type 2 diabetes: a prospective study in men,”American Journal of Clinical Nutrition, vol. 76, no. 3, pp. 535–540, 2002.
[35] E. Lopez-Garcia, M. B. Schulze, J. E. Manson et al., “Consump-tion of (n-3) fatty acids is related to plasma biomarkers ofinflammation and endothelial activation in women,” Journalof Nutrition, vol. 134, no. 7, pp. 1806–1811, 2004.
[36] American Diabetes Association, “Implications of the UnitedKingdom prospective siabetes study,” Diabetes Care, vol. 25,pp. S28–S32, 2002.
[37] Y. Ma, J. R. Hebert, W. Li et al., “Association between dietaryfiber and markers of systemic inflammation in the Women’sHealth Initiative Observational Study,” Nutrition, vol. 24, no.10, pp. 941–949, 2008.
[38] S. Liu, M. J. Stampfer, F. B. Hu et al., “Whole-grain con-sumption and risk of coronary heart disease: results from theNurses’ Health Study,” American Journal of Clinical Nutrition,vol. 70, no. 3, pp. 412–419, 1999.
[39] B. Parker, M. Noakes, N. Luscombe, and P. Clifton, “Effect ofa high-protein, high-monounsaturated fat weight loss diet onglycemic control and lipid levels in type 2 diabetes,” DiabetesCare, vol. 25, no. 3, pp. 425–430, 2002.
[40] M. S. Song and H. S. Kim, “Intensive management program toimprove glycosylated hemoglobin levels and adherence to dietin patients with type 2 diabetes,” Applied Nursing Research, vol.22, no. 1, pp. 42–47, 2009.
[41] F. Visioli, A. Poli, D. Richard, and R. Paoletti, “Modula-tion of inflammation by nutritional interventions,” CurrentAtherosclerosis Reports, vol. 10, no. 6, pp. 451–453, 2008.
[42] K. F. Schulz, D. G. Altman, and D. Moher, “CONSORT, 2010Statement: updated guidelines for reporting parallel grouprandomised trials,” Journal of Clinical Epidemiology, vol. 63,pp. 813–814, 2010.
[43] D. S. West, T. Elaine Prewitt, Z. Bursac, and H. C. Felix,“Weight loss of black, white, and Hispanic men and womenin the diabetes prevention program,” Obesity, vol. 16, no. 6,pp. 1413–1420, 2008.
[44] M. Gonzalez-Castejon and A. Rodriguez-Casado, “Dietaryphytochemicals and their potential effects on obesity: areview,” Pharmacological Research, vol. 64, pp. 438–455, 2011.
Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com













![Review Article Fructose: A Key Factor in the Development ...downloads.hindawi.com/journals/jnme/2013/682673.pdf · within hour [ ]. Uncontrolled fructose metabolism leads to postprandial](https://img.pdfslide.us/doc/110x75/5fa1f92ac6ddaf18315ea33c/review-article-fructose-a-key-factor-in-the-development-within-hour-uncontrolled.jpg)















