Embed Size (px)
Citation preview
![Page 1: Review Article - Hindawi · 2019. 7. 31. · 67 M CT 24 hours CT N Uneventful 31 F CT 3 days CT N Uneventful Caustic ingestion [38] 55 F CT 24 hours CT N Uneventful Colchicine [39]](https://reader035.pdfslide.us/reader035/viewer/2022071419/6118464c8cdd773d83092c89/html5/thumbnails/1.jpg)
International Scholarly Research NetworkISRN Emergency MedicineVolume 2012, Article ID 480795, 7 pagesdoi:10.5402/2012/480795
Review Article
Self-Limited Pneumoporta in the Era of Computed Tomography:A Case Report and Review of the Literature
Yu-Tso Liao, Hong-Shee Lai, Rey-Heng Hu, Po-Huang Lee, and Cheng-Maw Ho
Department of Surgery, National Taiwan University Hospital, No. 7 Chung-Shan South Road, 10002 Taipei, Taiwan
Correspondence should be addressed to Cheng-Maw Ho, [email protected]
Received 25 October 2012; Accepted 18 November 2012
Academic Editors: A. K. Attri, R. Cirocchi, and A. Pazin-Filho
Copyright © 2012 Yu-Tso Liao et al. This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Pneumoporta in patients with abdominal pain has been thought to be suggestive of fatal underlying conditions, such as mesentericinfarct, requiring emergency treatment. Widespread use of computed tomography (CT) has increased the frequency of detectionof pneumoporta in patients with diseases other than mesenteric infarct. The natural course of resolution of pneumoporta hasbeen rarely discussed in the literature and mainly focused on patients with iatrogenic diseases. Herein, we report the case of a64-year-old woman who presented at our emergency department with positive peritoneal signs and pneumoporta. A 10 cm longsegment of resolved ischemic bowel was detected on exploratory laparotomy, and bowel resection was not performed. Follow-upCT performed 62 hours later revealed complete resolution of pneumoporta. The patient was discharged uneventfully and wasadministered short-term prophylactic therapy with enoxaparin for thromboembolism. The epidemiology, etiology, and resolutionof pneumoporta are also reviewed.
1. Background
Pneumoporta has been thought to be an ominous radiolog-ical sign. However, the etiology is associated with variousdiseases ranging from severe fatal conditions requiring rapidsurgical intervention to medical diseases with a benigncourse. Treatment of pneumoporta should be based on theetiology of the condition. The natural course of resolutionof pneumoporta has rarely been discussed in the literature.Here, we report a case of a 64-year-old woman with sponta-neously resolved ischemic bowel and pneumoporta, and theepidemiology, etiology, and resolution of pneumoporta arereviewed.
2. Case Presentation
A 64-year-old woman presented at our emergency depart-ment with intermittent abdominal pain for 3 days withoutvomiting or dysentery. The patient was otherwise healthy,but had a history of spinal surgery and was a carrierof the hepatitis B virus. She did not have a history ofhydrogen peroxide ingestion. Upon arrival at the emergencydepartment, her vital signs were stable and consciousness
was clear. Physical examination revealed distended abdomenand diffuse peritoneal sign. Laboratory examination showedno leukocytosis, but a mild left shift. Lactic acid levelswere within the normal range. Abdominal CT scan showedthe presence of air in the portal venous tree in the lefthepatic lobe, patent superior mesenteric artery (SMA), andsuperior mesenteric vein, and bowel wall thickening anddistension of the ileum were noted (Figures 1 and 2). Thepatent SMA, as detected by the abdominal CT scan, wasalso observed. The patient underwent emergency exploratorylaparotomy. Intraoperative examination revealed a 10 cmlong segment of the resolved ischemic ileum with a thickenedwall and no transmural infarction. The liver surface wasnoncontributory. Follow-up abdominal CT performed 62hours after laparotomy revealed complete resolution ofhepatic portal venous gas (Figure 3). A series of workupsfor the thromboembolic event, including cardiac echographyand coagulation studies for autoantibodies, factor VIII,protein C, and protein S, yielded no abnormal data exceptelevated levels of D-D dimer and factor VIII. The patientwas discharged uneventfully and was administered short-term prophylactic therapy with enoxaparin for thromboem-bolism.
![Page 2: Review Article - Hindawi · 2019. 7. 31. · 67 M CT 24 hours CT N Uneventful 31 F CT 3 days CT N Uneventful Caustic ingestion [38] 55 F CT 24 hours CT N Uneventful Colchicine [39]](https://reader035.pdfslide.us/reader035/viewer/2022071419/6118464c8cdd773d83092c89/html5/thumbnails/2.jpg)
2 ISRN Emergency Medicine
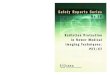
Figure 1: Computed tomography (CT) scan showed the presenceof gas in the portal vein, mainly in the left hepatic lobe.
Figure 2: Thickening of the ileum wall (arrow).
3. Discussion
Pneumoporta has been considered to be an ominous radi-ological sign. However, pneumoporta may be associatedwith conditions ranging from severe fatal diseases requiringurgent surgical intervention to medical diseases that follow abenign course, such as gastroenteritis, which can be managedwith only conservative treatment [1, 2]. A mortality rateas high as 75–90% has been reported, mainly owing tothe occurrence of mesenteric infarction [3–5]. Nowadays,the widespread utilization of CT scan has increased thefrequency of detection of pneumoporta in the clinicalscenario [6, 7]. Indeed, mesenteric infarctions are the mainetiological factors that lead to potentially fatal outcomes andshould always be considered when diagnosing the cause ofpneumoporta [8, 9]. In addition, because of the increasedfrequency of occurrence of benign diseases [2, 6], promptclinical evaluation and surgical decision are paramount incases of pneumoporta.
CT scan enables early detection due to high sensitivityfor pneumoporta and is superior to other radiologicalmodalities, including ultrasound and abdominal plain film,
Figure 3: CT performed 62 hours after laparotomy showed com-plete resolution of hepatic portal vein gas.
in diagnosis of underlying abdominal diseases [7]. Sincethe 1970s, the introduction of the CT scan has graduallyadvanced the ability of physicians to accurately diagnosepneumoporta, and pneumoporta can now be detected atless advantaged stages [7]. More than half of the etiolo-gies of pneumoporta were mesenteric infarct, reported toaccount for 61–75% of cases [3, 8, 10]. Other etiologiesinclude gastrointestinal dysmotility, infectious/inflammatoryprocesses, toxicity-related conditions, and iatrogenic lesions[11, 12]. Notably, the appearance of pneumoporta in relationto iatrogenic causes increase in frequency over recent decades[8].
The correlation of outcomes and the presence ofpneumoporta, as well as the duration of pneumoporta,have not been clearly elucidated [3, 9]. The appearanceof pneumoporta is associated with poor outcomes inpatients experiencing cardiac arrest outside of the hospital[13]. Nevertheless, the notoriously high mortality generallyencountered in patients with pneumoporta has decreasedto 25–29% in recent reports, mainly due to early detectionand incidental findings during the diagnosis of other diseases[9, 14, 15]. Furthermore, the resolution of pneumoporta hasbeen shown to be associated with the improvement of theunderlying diseases.
In order to investigate the clinical characteristics ofpneumoporta resolution in the era of CT scan, we reviewedthe English literature by searching for the keyword “portalvenous gas” or “hepatic portal venous gas” in PubMed. Theage, sex, etiology, diagnostic modality (including conven-tional roentgenography, ultrasound, and CT scan), durationof pneumoporta, and patient outcomes were reviewed.Patients who were diagnosed as pneumoporta on CT scanwere included in the study. The exclusion criteria werelisted as following: the patients died of fulminant mesentericinfarct without CT followup, the unclear recording aboutresolution of pneumoporta, or the detection of pneumoportaby the radiological modalities other than CT scan. A totalof 61 cases were eligible and are listed according to theetiology (Table 1). Several classifications have been proposedin literature, and the system we used here was based on
![Page 3: Review Article - Hindawi · 2019. 7. 31. · 67 M CT 24 hours CT N Uneventful 31 F CT 3 days CT N Uneventful Caustic ingestion [38] 55 F CT 24 hours CT N Uneventful Colchicine [39]](https://reader035.pdfslide.us/reader035/viewer/2022071419/6118464c8cdd773d83092c89/html5/thumbnails/3.jpg)
ISRN Emergency Medicine 3
Ta
ble
1:C
linic
alch
arac
teri
stic
san
dou
tcom
esof
pneu
mop
orta
reso
luti
onin
repo
rted
case
sin
the
liter
atu
re.
Cau
seA
ge(y
ears
)Se
xD
etec
ted
mod
alit
yD
ura
tion
ofpn
eum
opor
taFo
llow
-up
mod
alit
ySu
rger
yO
utc
ome
Non
iatr
ogen
ic
Bow
elis
chem
ia/n
ecro
sis
[19–
22]
73F
CT
3da
ysC
TY
Exp
ired
82F
CT
24h
ours
CT
NU
nev
entf
ul
51F
CT
2m
onth
sC
TY
Un
even
tfu
l
86M
CT
6da
ysC
TY
Un
even
tfu
l
Isch
emic
colit
is[2
3]61
MC
T20
days
CT
NU
nev
entf
ul
Dys
mot
ility
Smal
lbow
elob
stru
ctio
n[2
4,25
]64
FX
R7
days
CT
YU
nev
entf
ul
61M
CT
3h
CT
NU
nev
entf
ul
Supe
rior
mes
ente
ric
arte
rysy
ndr
ome
[26]
10F
CT
48h
CT
NU
nev
entf
ul
Infe
ctio
n/i
nfl
amm
atio
n
Gas
troe
nte
riti
s[1
]58
MC
T4
days
CT
NU
nev
entf
ul
Pye
lon
eph
riti
s[2
7]56
MC
T1
mon
thC
TY
Un
even
tfu
lSe
ptic
thro
mbo
phle
biti
s[2
8]52
MC
T2
mon
ths
CT
NU
nev
entf
ul
Term
inal
ileit
is[2
9]64
FC
T18
hou
rsC
TN
Un
even
tfu
l
Cro
hn’
sdi
seas
e[3
0–32
]40
FC
T7
days
CT
NU
nev
entf
ul
70M
CT
2da
ysC
TN
Un
even
tfu
l26
FC
T9
hou
rsC
TN
Un
even
tfu
lR
etro
per
iton
eala
bsce
ss[3
3,34
]31
MC
T10
days
CT
YU
nev
entf
ul
64M
CT
3da
ysC
TY
—
Med
icat
ion
/tox
icit
y-re
late
dco
ndi
tion
s
Acc
iden
tali
nge
stio
nof
hydr
ogen
per
oxid
e[3
5–37
]67
MC
T24
hou
rsC
TN
Un
even
tfu
l31
FC
T3
days
CT
NU
nev
entf
ul
Cau
stic
inge
stio
n[3
8]55
FC
T24
hou
rsC
TN
Un
even
tfu
lC
olch
icin
e[3
9]57
MC
T4
days
CT
NU
nev
entf
ul
Oth
ers
Gra
ft-v
ersu
s-h
ost
dise
ase
[15,
40]
29M
CT
2w
eeks
CT
NU
nev
entf
ul
52M
CT
3w
eeks
CT
NE
xpir
ed(d
ied
due
tou
nde
rlyi
ng
dise
ase)
Pn
eum
atos
iscy
stoi
des
inte
stin
alis
[41]
94F
CT
11da
ysC
TY
Un
even
tfu
lIa
trog
enic
Rad
iofr
equ
ency
abla
tion
[42]
—∗
—∗
CT
20m
ins
CT
NU
nev
entf
ul
Cry
oth
erap
y[4
3]50
MC
T24
hou
rsC
TN
Exp
ired
(por
talv
ein
thro
mbo
sis
and
seps
is)
En
dosc
opy
orre
late
dpr
oced
ure
[40,
44]
26F
CT
24h
ours
XR
NU
nev
entf
ul
76M
CT
2da
ysC
TN
Un
even
tfu
l
En
dosc
opic
ballo
ondi
lata
tion
[45]
31M
CT
5da
ysC
TN
Un
even
tfu
lE
soph
agea
lvar
icea
lban
dlig
atio
nor
endo
scop
icsc
lero
ther
apy
[46]
77F
CT
3da
ysC
TN
Un
even
tfu
l
![Page 4: Review Article - Hindawi · 2019. 7. 31. · 67 M CT 24 hours CT N Uneventful 31 F CT 3 days CT N Uneventful Caustic ingestion [38] 55 F CT 24 hours CT N Uneventful Colchicine [39]](https://reader035.pdfslide.us/reader035/viewer/2022071419/6118464c8cdd773d83092c89/html5/thumbnails/4.jpg)
4 ISRN Emergency Medicine
Ta
ble
1:C
onti
nu
ed.
Cau
seA
ge(y
ears
)Se
xD
etec
ted
mod
alit
yD
ura
tion
ofpn
eum
opor
taFo
llow
-up
mod
alit
ySu
rger
yO
utc
ome
Lin
ton
prob
ein
sert
ion
[47]
54M
CT
24h
ours
CT
NU
nev
entf
ul
Bar
ium
enem
a[4
8]86
MC
T3
days
CT
NU
nev
entf
ul
Oxy
gen
per
oxid
een
ema
[36]
31M
CT
48h
ours
CT
NU
nev
entf
ul
Lum
bar
pun
ctu
re[4
9]19
FU
ltra
sou
nd
4da
ysC
TN
Un
even
tfu
l
Intr
a-ao
rtic
ballo
onpu
lsat
ion
[50]
49—
CT
2da
ysU
ltra
sou
nd
NU
nev
entf
ul
Pan
crea
tico
duod
enec
tom
y[5
1]63
MC
TC
T:1
8da
ys;u
ltra
sou
nd:
22da
ysC
T,u
ltra
sou
nd
NU
nev
entf
ul
Res
usc
itat
ion
[52]
25M
CT
24h
ours
CT
NU
nev
entf
ul
CT
:com
pute
dto
mog
raph
y;E
US:
endo
scop
icu
ltra
sou
nd.
—:n
otm
enti
oned
inth
elit
erat
ure
.∗ 2
5ca
ses
wer
ere
port
ed.
![Page 5: Review Article - Hindawi · 2019. 7. 31. · 67 M CT 24 hours CT N Uneventful 31 F CT 3 days CT N Uneventful Caustic ingestion [38] 55 F CT 24 hours CT N Uneventful Colchicine [39]](https://reader035.pdfslide.us/reader035/viewer/2022071419/6118464c8cdd773d83092c89/html5/thumbnails/5.jpg)
ISRN Emergency Medicine 5
whether the causes were iatrogenic or not because theclassification conveyed clinical usefulness and prognosticprediction [12, 16].
For demography available in the literature, themale/female ratio was 1.5, with a mean age of 53.4years (range, 10 to 94 years). Iatrogenic etiologies werethe main causes of pneumoporta (61%). The resolutionof pneumoporta was associated with the improvementof underlying diseases, and the reported duration ofpneumoporta ranged from 20 min to 2 months.
The correlation between lethal potentiality and pneumo-porta is unclear. The risk of hepatic flow compromise byair accumulating in the portal systems may be taken intoconsideration. However, pneumoporta itself rarely affectedhepatic flow in both animal and human studies. Theobservation might be explained by the anatomy of the dualblood supply of liver [17, 18]. Accordingly, researchers haveassumed that the pathophysiological mechanism responsiblefor the onset of pneumoporta is the cause of death, notthe air bubbles themselves [17]. The detailed mechanismnecessitated further study.
4. Noniatrogenic Causes
For noniatrogenic causes, improvement of pneumoportain patients with mesenteric infarct was rarely reported,possibly because of the fulminant course of these underlyingconditions. The appearance of pneumoporta in mesentericinfarct is associated with high mortality and morbidity[53]. Other diseases in which pneumoporta has been notedinclude gastrointestinal dysmotility, infection/inflammation,and medication/toxicity-related conditions. The outcomesin these situations were satisfactory following prompt sur-gical intervention. Notably, various medical diseases arepredisposing factors for pneumoporta and do not mandatesurgical intervention. In these cases, pneumoporta is usuallynoticed incidentally, and the course is usually self-limited.Transient ischemic enteritis has been reported to be a causeof pneumoporta and can also be successfully managedconservatively [54].
5. Iatrogenic Causes
The course of pneumoporta after iatrogenic events is gen-erally benign and transient, lasting no more than 1 day inthe majority of cases. Incidental discovery of pneumoportausually urges clinicians to repeat the imaging examinationand followup with the patients closely, as shown in theliterature. The appropriate treatment for iatrogenic casesseems to “wait and see,” except in one patient who died ofportal vein thrombosis and sepsis after cryotherapy [43].
Diffuse peritoneal signs and wall thickening of thesmall bowel revealed by physical examination and CT scan,respectively, in the presence of pneumoporta is a conditionthat requires urgent surgical intervention [6]. The conditionmay be suggestive of an underlying clinical condition, such asmesenteric ischemia/infarction. However, in our case, onlyone segment of the thickened small bowel, which seemed
to be the resolved ischemic bowel, was observed during theintraoperative examination. This patient is alive, and bowelresection was not required.
The natural course of pneumoporta is rarely discussedsystemically in the literature and is only sporadically reportedin patients with iatrogenic diseases [24, 29, 44]. In our case,sequential CT scan performed 62 hours after laparotomyrevealed complete resolution of pneumoporta. This observa-tion implies that pneumoporta may be a paraphenomenonthat disappears when the underlying pathology is improved.
There were some limitations in our review. First, theduration of pneumoporta was ambiguous, lacking a cleardefinition and strict control. Actually the duration recordedin the paper indicated a potential period that the pneumo-porta may exist. Second, the appearance of pneumoportawas regarded as a paraphenomenon in benign diseases;therefore, the follow-up modalities depended on clinicians’judgment in the absence of standard protocol. Third,the real incidence of self-limited pneumoporta might beunderestimated because the “benign” pneumoporta woulddisappear spontaneously. We believed the occurrence ofpneumoporta would outnumber the cases recorded in theliterature. In despite of the above-mentioned limitations, weare convinced that our study offers a general description ofcurrent self-limited pneumoporta reported in the Englishliterature. The overall survey pointed out some undiscoveredissues concerning the pathophysiology and clinical outcomesof pneumoporta.
6. Conclusion
Mesenteric infarct should always be considered when diag-nosing the cause of pneumoporta accompanied by positiveperitoneal signs. The diagnosis of pneumoporta merelybased on radiological findings is an intriguing possibility,and the management of pneumoporta should be based onetiological findings. In our case, spontaneous resolution ofpneumoporta was observed.
Abbreviations
CT: Computed tomographySMA: Superior mesenteric artery.
Conflict of Interests
The authors declare that there is no conflict of interests.
Authors’ Contribution
C.-M. Ho and Y.-T. Liao participated in the patient’s care,including the operative procedures. Y.-T. Liao drafted thepaper. H.-S. Lai, R.-H. Hu, and P.-H. Lee supervised anddirected the review of the literature.
![Page 6: Review Article - Hindawi · 2019. 7. 31. · 67 M CT 24 hours CT N Uneventful 31 F CT 3 days CT N Uneventful Caustic ingestion [38] 55 F CT 24 hours CT N Uneventful Colchicine [39]](https://reader035.pdfslide.us/reader035/viewer/2022071419/6118464c8cdd773d83092c89/html5/thumbnails/6.jpg)
6 ISRN Emergency Medicine
References
[1] A. Mancebo, E. Alvarez-Hornia, M. Rodrıguez-Pelaez, M.Ibanez, L. H. Luyando, and M. Varela, “Indolent evolutionof an episode of acute gastroenteritis complicated with portalpneumatosis,” Revista Espanola de Enfermedades Digestivas,vol. 102, no. 9, pp. 557–559, 2010.
[2] A. L. Nelson, T. M. Millington, D. Sahani et al., “Hepatic portalvenous gas: the ABCs of management,” Archives of Surgery, vol.144, no. 6, pp. 575–581, 2009.
[3] P. R. Liebman, M. T. Patten, and J. Manny, “Hepatic-portalvenous gas in adults: etiology, pathophysiology and clinicalsignificance,” Annals of Surgery, vol. 187, no. 3, pp. 281–287,1978.
[4] W. C. G. Peh and M. Muttarak, “Clinics in diagnostic imaging(53). Hepatic portal venous gas due to mesenteric infarction,”Singapore Medical Journal, vol. 41, no. 9, pp. 471–473, 2000.
[5] R. A. Bloom, P. D. Lebensart, P. Levy, E. Craciun, H. Anner,and J. Manny, “Survival after ultrasonographic demonstrationof portal venous gas due to mesenteric artery occlusion,”Postgraduate Medical Journal, vol. 66, no. 772, pp. 137–139,1990.
[6] E. Wayne, M. Ough, A. Wu et al., “Management algorithm forpneumatosis intestinalis and portal venous gas: treatment andoutcome of 88 consecutive cases,” Journal of GastrointestinalSurgery, vol. 14, no. 3, pp. 437–448, 2010.
[7] S. T. Schindera, J. Triller, P. Vock, and H. Hoppe, “Detectionof hepatic portal venous gas: its clinical impact and outcome,”Emergency Radiology, vol. 12, no. 4, pp. 164–170, 2006.
[8] A. Hussain, H. Mahmood, and S. El-Hasani, “Portal vein gas inemergency surgery,” World Journal of Emergency Surgery, vol.3, no. 1, article 21, 2008.
[9] H. Kinoshita, M. Shinozaki, H. Tanimura et al., “Clinicalfeatures and management of hepatic portal venous gas: fourcase reports and cumulative review of the literature,” Archivesof Surgery, vol. 136, no. 12, pp. 1410–1414, 2001.
[10] N. Peloponissios, N. Halkic, M. Pugnale et al., “Hepatic portalgas in adults: review of the literature and presentation of aconsecutive series of 11 cases,” Archives of Surgery, vol. 138,no. 12, pp. 1367–1370, 2003.
[11] B. Abboud, J. El Hachem, T. Yazbeck, and C. Doumit, “Hepaticportal venous gas: physiopathology, etiology, prognosis andtreatment,” World Journal of Gastroenterology, vol. 15, no. 29,pp. 3585–3590, 2009.
[12] P. A. Shah, S. C. Cunningham, T. A. Morgan, and B. D. Daly,“Hepatic gas: widening spectrum of causes detected at ct andus in the interventional era,” Radiographics, vol. 31, pp. 1403–1413, 2011.
[13] W. C. Lien, W. T. Chang, S. P. Huang et al., “Hepatic portalvenous gas associated with poor outcome in out-of-hospitalcardiac arrest patients,” Resuscitation, vol. 60, no. 3, pp. 303–307, 2004.
[14] R. S. Faberman and W. W. Mayo-Smith, “Outcome of 17patients with portal venous gas detected by CT,” AmericanJournal of Roentgenology, vol. 169, no. 6, pp. 1535–1538, 1997.
[15] W. Wiesner, K. J. Mortele, J. N. Glickman, H. Ji, and P. R.Ros, “Portal-venous gas unrelated to mesenteric ischemia,”European Radiology, vol. 12, no. 6, pp. 1432–1437, 2002.
[16] J. J. Hong, D. Gadaleta, P. Rossi, J. Esquivel, and J. M. Davis,“Portal vein gas, a changing clinical entity: report of 7 patientsand review of the literature,” Archives of Surgery, vol. 132, no.10, pp. 1071–1075, 1997.
[17] B. D. Butler, C. Fife, T. Sutton, M. Pogodsky, and P. Chen,“Hepatic portal venous gas with hyperbaric decompression:
ultrasonographic identification,” Journal of Ultrasound inMedicine, vol. 14, no. 12, pp. 967–970, 1995.
[18] I. Gersh and H. R. Catchpole, “Appearance and distributionof gas bubbles in rabbits decompressed to altitude,” Journal ofCellular and Comparative Physiology, vol. 28, no. 3, pp. 253–269, 1946.
[19] K. Ohtsubo, T. Okai, Y. Yamaguchi et al., “Pneumatosisintestinalis and hepatic portal venous gas caused by mesentericischemia in an aged person,” Journal of Gastroenterology, vol.36, no. 5, pp. 338–340, 2001.
[20] D. Fukumori, T. Sasaki, H. Matsumoto, H. Ohmori, T. Kakazu,and F. Yamamoto, “Necrotizing enteritis with hepatic portalvenous gas and pneumatosis intestinalis: report of a case,”European Journal of Gastroenterology and Hepatology, vol. 15,no. 2, pp. 201–203, 2003.
[21] Y. Morimoto, T. Yamakawa, Y. Tanaka, T. Hiranaka, andM. Kim, “Recurrent hepatic portal venous gas in a patientwith hemodialysis-dependent chronic renal failure,” Journal ofHepato-Biliary-Pancreatic Surgery, vol. 8, no. 3, pp. 274–278,2001.
[22] A. Hashimoto, H. Fuke, A. Shimizu, and K. Shiraki, “Hepaticportal venous gas caused by non-obstructive mesentericischemia,” Journal of Hepatology, vol. 37, no. 6, p. 870, 2002.
[23] S. H. Jung, K. M. Lee, W. C. Chung, C. N. Paik, J. D. Kim,and J. W. Kwak, “Ischemic colitis and portal venous gas,”Gastrointestinal Endoscopy, vol. 71, no. 7, pp. 1302–1303, 2010.
[24] B. Coulier, S. Van den Broeck, and J. P. Coppens, “Transientand rapidly resolving intrahepatic portal gas: CT findings,”Journal Belge de Radiologie, vol. 91, no. 5, pp. 214–216, 2008.
[25] M. Yamamuro and J. L. Ponsky, “Hepatic portal venous gas:report of a case,” Surgery Today, vol. 30, no. 7, pp. 647–650,2000.
[26] J. Rod, S. Sarnacki, T. Petit, and P. Ravasse, “Portal venousgas and thrombosis complicating superior mesenteric arterysyndrome (Wilkie’s syndrome) in a child,” Journal of PediatricSurgery, vol. 45, no. 4, pp. 826–829, 2010.
[27] Y. C. Mao, J. D. Wang, and L. M. Wang, “Hepatic portalvenous gas caused by emphysematous pyelonephritis,” ClinicalGastroenterology and Hepatology, vol. 7, no. 10, article A25,2009.
[28] T. N. Chau, T. K. L. Loke, V. K. S. Leung, S. T. Law, M. H. Y. Lai,and Y. W. Ho, “Hepatic portal venous gas complicating septicthrombophlebitis of the superior mesenteric vein,” Hong KongMedical Journal, vol. 13, no. 1, pp. 69–72, 2007.
[29] M. Niki, I. Shimizu, T. Horie et al., “Hepatic portal venous gasdisappearing within 24 hours,” Internal Medicine, vol. 41, no.11, pp. 950–952, 2002.
[30] M. Kirsch, J. Bozdech, and D. A. Gardner, “Hepatic portalvenous gas: an unusual presentation of Crohn’s disease,”American Journal of Gastroenterology, vol. 85, no. 11, pp. 1521–1523, 1990.
[31] J. Delamarre, J. P. Capron, J. L. Dupas, B. Deschepper, C. Jouet-Gondry, and A. Rudelli, “Spontaneous portal venous gas ina patient with Crohn’s ileocolitis,” Gastrointestinal Radiology,vol. 16, no. 1, pp. 38–40, 1991.
[32] H. Al-Jahdali, C. Pon, W. G. Thompson, and F. R. Matzinger,“Non-fatal portal pyaemia complicating Crohn’s disease of theterminal ileum,” Gut, vol. 35, no. 4, pp. 560–561, 1994.
[33] S. G. Chang, S. C. Lee, D. H. Hong, and S. E. Chai, “Portal andsuperior mesenteric venous gas with retroperitoneal abscess—CT diagnosis (case report),” Journal of Korean medical science,vol. 7, no. 1, pp. 62–65, 1992.
[34] T. Ochiai, K. Igri, Y. Kumagai, M. Iida, and S. Yamazaki,“Gastrointestinal: massive portal venous gas and pneumatosis
![Page 7: Review Article - Hindawi · 2019. 7. 31. · 67 M CT 24 hours CT N Uneventful 31 F CT 3 days CT N Uneventful Caustic ingestion [38] 55 F CT 24 hours CT N Uneventful Colchicine [39]](https://reader035.pdfslide.us/reader035/viewer/2022071419/6118464c8cdd773d83092c89/html5/thumbnails/7.jpg)
ISRN Emergency Medicine 7
intestinalis,” Journal of Gastroenterology and Hepatology, vol.25, no. 6, p. 1178, 2010.
[35] L. K. French, B. Z. Horowitz, and N. J. McKeown, “Hydrogenperoxide ingestion associated with portal venousgas andtreatment with hyperbaric oxygen: a case seriesand review ofthe literature,” Clinical Toxicology, vol. 48, no. 6, pp. 533–538,2010.
[36] F. Volonte, P. Gervaz, P. A. Poletti, and P. Morel, “Portal veingas embolism following oxygen peroxide enema,” ColorectalDisease, vol. 12, no. 10, pp. e335–e336, 2010.
[37] S. Ghai and M. E. O’Malley, “Portal vein gas resultingfrom ingestion of hydrogen peroxide,” American Journal ofRoentgenology, vol. 181, no. 6, pp. 1719–1720, 2003.
[38] M. Lewin, M. Pocard, S. Caplin, A. Blain, J. M. Tubiana, andR. Parc, “Benign hepatic portal venous gas following causticingestion,” European Radiology, vol. 12, no. 3, pp. S59–S61,2002.
[39] M. Saksena, M. G. Harisinghani, J. Wittenberg, and P. R.Mueller, “Hepatic portal venous gas: transient radiographicfinding associated with colchicine toxicity,” British Journal ofRadiology, vol. 76, no. 911, pp. 835–837, 2003.
[40] S. Alqahtani, C. S. Coffin, K. Burak, F. Chen, J. MacGregor,and P. Beck, “Hepatic portal venous gas: a report of two casesand a review of the epidemiology, pathogenesis, diagnosis andapproach to management,” Canadian Journal of Gastroenterol-ogy, vol. 21, no. 5, pp. 309–313, 2007.
[41] C. Konoeda, K. Adachi, and Y. Morita, “Pneumatosis cystoidesintestinalis presenting with portal vein gas and pneumoperi-toneum,” American Surgeon, vol. 77, no. 6, pp. E119–E120,2011.
[42] T. Oei, E. VanSonnenberg, S. Shankar, P. R. Morrison, K.Tuncali, and S. G. Silverman, “Radiofrequency ablation of livertumors: a new cause of benign portal venous gas,” Radiology,vol. 237, no. 2, pp. 709–717, 2005.
[43] M. J. Alfredson, A. J. Brooks, M. L. Talbot, and D. L. Morris,“Hepatic portal vein gas as a complication of cryotherapy,”HPB, vol. 7, no. 2, pp. 159–160, 2005.
[44] S. M. Kuo, W. K. Chang, C. Y. Yu, and C. B. Hsieh, “Silenthepatic portal venous gas following upper gastrointestinalendoscopy,” Endoscopy, vol. 41, supplement 2, pp. E121–E122,2009.
[45] C. G. Lee, H. W. Kang, M. K. Song et al., “A case of hepaticportal venous gas as a complication of endoscopic balloondilatation,” Journal of Korean Medical Science, vol. 26, no. 8,pp. 1108–1110, 2011.
[46] K. Ahmed, M. Atiq, E. Richer, G. Neff, N. Kemmer, andK. Safdar, “Careful observation of hepatic portal venous gasfollowing esophageal variceal band ligation,” Endoscopy, vol.40, supplement 2, p. E103, 2008.
[47] C. G. Schulze, U. Blum, and K. Haag, “Hepatic portalvenous gas imaging modalities and clinical significance,” ActaRadiologica, vol. 36, no. 4, pp. 377–380, 1995.
[48] D. Zhang, D. Weltman, and A. Baykal, “Portal vein gasand colonic pneumatosis after enema, with spontaneousresolution,” American Journal of Roentgenology, vol. 173, no.4, pp. 1140–1141, 1999.
[49] D. Karaosmanoglu, S. O. Oktar, M. Arac, and G. Erbas, “Portaland systemic venous gas in a patient after lumbar puncture,”British Journal of Radiology, vol. 78, no. 932, pp. 767–769,2005.
[50] F. Artunc, S. Heller, M. Heuschmid, R. Riessen, and M. Haap,“Gastrointestinal: hepatic portal venous gas after cardiogenicshock and intraaortic ballon pulsation therapy,” Journal ofGastroenterology and Hepatology, vol. 25, no. 3, p. 644, 2010.
[51] T. Tsubono, K. Sato, and M. Fukuda, “Hepatic portal venousgas associated with cholangitis following pancreaticoduo-denectomy: report of a case,” Surgery Today, vol. 24, no. 4, pp.375–377, 1994.
[52] H. Reuter, C. Bangard, F. Gerhardt, S. Rosenkranz, and E.Erdmann, “Extensive hepatic portal venous gas and gastricemphysema after successful resuscitation,” Resuscitation, vol.82, no. 2, pp. 238–239, 2011.
[53] J. M. Wu, M. S. Tsai, M. T. Lin, Y. W. Tien, and T. H. Lin, “HighAPACHE II score and long length of bowel resection impairthe outcomes in patients with necrotic bowel induced hepaticportal venous gas,” BMC Gastroenterology, vol. 11, article 18,2011.
[54] T. Morisaki, K. Ohba, A. Yoshida, Y. Mizuta, and K. Nakao,“A case of hepatic portal venous gas caused by transient typeischemic enteritis,” Journal of Japanese Society of Gastroenterol-ogy, vol. 107, no. 3, pp. 407–415, 2010.
![Page 8: Review Article - Hindawi · 2019. 7. 31. · 67 M CT 24 hours CT N Uneventful 31 F CT 3 days CT N Uneventful Caustic ingestion [38] 55 F CT 24 hours CT N Uneventful Colchicine [39]](https://reader035.pdfslide.us/reader035/viewer/2022071419/6118464c8cdd773d83092c89/html5/thumbnails/8.jpg)
Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
International Journal of
EndocrinologyHindawi Publishing Corporationhttp://www.hindawi.com
Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
BioMed Research International
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
PPARRe sea rch
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Parkinson’s DiseaseHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com