Embed Size (px)
Citation preview

Int J Clin Exp Med 2017;10(12):15866-15877www.ijcem.com /ISSN:1940-5901/IJCEM0059120
Review ArticleEffect of dezocine administration in the prevention of fentanyl-induced cough during general anesthesia induction: a systematic review and meta-analysis of randomized controlled trials
Wen-Xiu Jiang1*, Jun-Ming Huang2*, Jin-Ming Zhang2, Han-Ning Li3, Xiang Lu4, Jia Zhang1, Zheng-Tao Lv2
1Department of Otolaryngology, Affiliated Eye and ENT Hospital of Fudan University, Shanghai, China; Depart-ments of 2Orthopedics, 3Thyroid-Breast Surgery, 4Otolaryngology-Head and Neck Surgery, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan 430030, Hubei, China. *Equal contribu-tors.
Received June 10, 2017; Accepted November 6, 2017; Epub December 15, 2017; Published December 30, 2017
Abstract: Objectives: The aim of this study is to evaluate the efficacy and safety of dezocine administration in the prevention of fentanyl induced cough (FIC). Methods: Literature search based on Pubmed, EMBASE, ISI Web of Sci-ence, CENTRAL, CNKI was performed to identify potential randomized controlled trials (RCTs) assessing the effect of dezocine in FIC. Two reviewers selected each article independently according to predetermined inclusion criteria. Meta-analysis was conducted via RevMan 5.3. Results: A total of 15 RCTs involving 2074 patients that scheduled for elective surgeries were included, low dose dezocine administration, 0.1 mg/kg dezocine and high dose dezocine were effective in preventing FIC (low dose: RR 0.01 95% CI 0.00, 0.08; 0.1 mg/kg: RR 0.11 95% CI 0.06, 0.17; high dose: RR 0.15 95% CI 0.10, 0.23). The combined incidence of FIC in normal saline groups were around 51%. Subgroup-analysis and sensitivity analysis were performed. Discussion: The results of our study indicated a definite effect of dezocine administration, which is irrespective of the dosage of dezocine injection. Future studies with larger scale and strict design are recommended.
Keywords: Fentanyl induced cough, dezocine, anesthesia, meta-analysis, systematic review
Introduction
Fentanyl is a µ-opioid receptor agonist and has a clinical potency ratio of 50 to 100 times that of morphine, which was firstly synthesized in 1960. Fentanyl and its derivatives, such as suf-entanil, alfentanil and remifentanil [1], are the most frequently used opioids in clinical anes-thesia. These synthetic potent opioids derived from phenylpiperidine are frequently adminis-tered for their analgesic effect especially prior to induction of anesthesia. Fentanyl has the advantage of rapid onset, short duration of action, profound dose-dependent analgesia, and cardiovascular stability as well as less release of histamine mainly during laryngosco-py and endotracheal intubation [2, 3]. Like other opioids, several side effects of fentanyl were also reported, such as nausea, dry mouth, somnolence, hypoventilation, asthenia, consti-
pation, and apnea. Another side effect under the spotlight is the fentanyl-induced cough (FIC).
Many reports have confirmed that fentanyl at induction of anesthesia can cause coughing with varying degrees and its derivatives trigger cough as well [4-6]. Some articles state that the incidence of fentanyl-induced cough varies between 2.7% and 65% [7, 8]. Although fentan-yl-induced cough is transient, benign and self-limiting in most patients, its severity should not be ignored in the patients who are at the risk of an increase or increased intracranial pressure such as cerebral aneurysms, cerebral tumor, ruptured cerebral aneurysms, and the patients with acute glaucoma, penetrating eye injuries, or arterial aneurysm resection, and hypersensi-tive airway disease [9, 10].

Dezocine in fentanyl-induced cough
15867 Int J Clin Exp Med 2017;10(12):15866-15877
With more and more attention focused on FIC, a growing number of intervention were intro-duced in reducing the incidence of FIC. Most reports demonstrated that pretreatment with some inhaled drugs, such as salbutamol, beclo-methasone or cromolyn sodium, or with intra- venous administration, ketamine, propofol or magnesium sulphate, can reduce the incidence of FIC before induction of anesthesia [11-13]. Uvelin and Rakic proposed some instructions on prevention of FIC, including (1) patients in condition of potentially raised intracranial pres-sure, acute glaucoma, serious airway respon-siveness, raised intracranial pressure, pene-trating eye injuries and younger non-smokers should be pre-treated against the occurrence of FIC even on a regular basis, because in most American Society of Anesthesiologists (ASA) I and II patients undergoing surgery, even if FIC occurs, it causes no serious effects; (2) intrave-nous lidocaine 0.5 mg/kg should be given at least 1 min before fentanyl administration and if we wish to prevent a hemodynamic response to laryngoscopy and intubation, the lidocaine dose can be higher (1-1.5 mg/kg i.v.) and ephedrine should be used in patients who are hypovolemic or hypotensive; (3) in the case of asthmatic patients who may benefit from avoid-ing FIC and already use salbutamol, beclometh-asone or sodium chromoglycate aerosol, these agents should be used 15 min before fentanyl; (4) prolongation of fentanyl injection time to about 20 s helps prevent FIC [14].
Dezocine which is a mixed agonist-antagonist opioid, a full agonist of κ-receptor resulting in strong analgesic effect, sedation and mild respiratory depression and partial agonist of μ-receptor causing a weak effect or some effect against agonist, namely partial blocking effect, is a potent opioid drug [15, 16]. Dezocine, which has good analgesic effect and has less side effect than traditional opioid, was widely used in the clinical treatment of pain and auxil-iary anesthesia. Several clinical studies have reported that dezocine had a significant effect in reducing incidence of FIC in general anesthe-sia cases. However, no published evidence based on randomized controlled trials (RCTs) could proved that applying dezocine was an effective approach to prevent the occurrence of FIC. Thus, our current study aims at evaluating the clinical effect and safety of dezocine on FIC in general anesthesia, compared with placebo control.
Methods
The protocol of this systematic review is regis-tered with PROSPERO (registration number: CRD42016037034). This systematic review was conducted in accordance to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guideline [17].
Search strategy
A comprehensive literature search of PubMed, EMBASE, CENTRAL, ISI Web of Science and CNKI was conducted. All the above databases were searched from their inception dates up to the latest issue (June 2017), without language restriction. A combination of Medical Subhe- adings (MeSH) and free terms were used to retrieve all the potential articles. MeSH were manually modified based upon the specifica-tions of each database. The following search strategy was used for the literature search in Pubmed, CENTRAL and ISI Web of Science: (“Cough” [Mesh] or cough or coughs) and (“dezocine” [Supplementary Concept] or Wy 16225 or dezocine). For CNKI, search terms were “Dizuoxin” and “Ke”, which means dezo-cine and cough respectively. In addition, the bibliographies of relevant systematic reviews and clinical guidelines were manually search- ed. The reference section for each study was also searched.
Types of participants
To be included in our systematic review, the enrolled subjects had to be scheduled for elec-tive surgery under general anesthesia and ASA physical status classification of I-II. Exclusive criteria included a history of chronic cough or smoking, known allergies, severe neurological, cardiovascular diseases, narcotic drug depen-dence and recent history of opioid application, pregnancy and delivery surgery.
Interventions
Patients in experimental groups were adminis-tered with dezocine solution prior to the anes-thesia induction. No specific dosage of dezo-cine was imposed. Patients in the control groups received normal saline with an equal volume of dezocine solution in experimental group. Studies that compared dezocine with other pharmaceutical treatments were ex- cluded.

Dezocine in fentanyl-induced cough
15868 Int J Clin Exp Med 2017;10(12):15866-15877
Outcome measurements
The primary outcome measure was the inci-dence of FIC within 2 minutes after the ad- ministration of fentanyl, side-effects associat-ed with dezocine administration were also do- cumented.
Types of publication
The included studies were limited to be RCT aiming at assessing the efficacy and safety of dezocine in the prevention of FIC. Animal exper-iments, review articles, case reports and expert experience reports were excluded.
Data extraction
Two investigators (W. X. Jiang and J.M. Huang) screened each article independently and were blinded to the findings of the other reviewer. According to the predetermined inclusion crite-
generation, allocation concealment, blinding of participants and personnel, blinding of out-come assessment, incomplete outcome data, selective reporting, and other sources of bias [18]. Two reviewers (J.M. Huang and Z.T. Lv) assessed the risk of bias among studies inde-pendently, the results of risk of bias judgement were not revealed until both reviewers finished the evaluation of all included studies. The results were compared afterwards, disagree-ments regarding the risk of bias assessment were settled by discussion until a consensus was reached.
Data synthesis and analysis
Risk ratio (RR) and the associated 95% confi-dence intervals (CIs) were calculated for inci-dence of FIC. Random-effect model was em- ployed for meta-analysis in case of heteroge- neity among our included studies; otherwise,
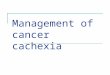
Figure 1. Flowchart of literature selec-tion according to PRISMA guideline.
ria, two reviewers performed a strict screening to identify the qualification of articles independently, and they ex- tracted data from these eli-gible articles using a stan-dardized data collection fo- rm, which included first author, time of the publica-tion, study of design, popula-tion characteristics of partic-ipants in different groups, interventions and control treatment, application of anesthesia, main outcome assessments.
Any disagreement between the two reviewers was re- solved through discussion until a consensus was achi- eved. The third review author (J.M. Zhang) was consulted if a consensus could not be achieved.
Quality assessment
The Cochrane Collaboration’s tool was applied to evaluate the risk of bias among the selected RCTs, the evalua-tion was based on seven items: random sequence

Dezocine in fentanyl-induced cough
15869 Int J Clin Exp Med 2017;10(12):15866-15877
Table 1. Characteristics of included studiesStudy Study-design Population Intervention and Control Application of anesthesia OutcomeCai et al., 2015 China RCT Scheduled for elective surgery;
ASA I-II; D: 40 patients; 48.2±11.6 years; C: 40 patients; 47.6±12.5 years
D: 0.1 mg/kg before the induction of anesthesia; C: 0.9% saline (10 ml) before the induction of anesthesia
Intravenous injection of dezocine/saline, fentanyl 3 ug/kg and etomidate 0.3 mg/kg; fentanyl and etomidate were injected in less than 5 s
Incidence of cougha
Gao et al., 2013 China RCT Scheduled for elective surgery; ASA I-II; D1: 40 patients; 46.3±7.6 years; D2: 40 patients; 44.7±6.3 years; D3: 40 patients; 46.9±5.4 years; C: 40 patients; 43.1±8.7 years
D1: 0.05 mg/kg; D2: 0.1 mg/kg; D3: 0.15 mg/kg 10 min before the induction of anesthesia; C: 0.9% saline (5 ml) 10 min before the induction of anesthesia
Sequentially intravenously injection of fentanyl 3 ug/kg, midazolam 0.04 mg/kg, propofol 2 mg/kg, cisatracurium 0.15 mg/kg
Incidence of cougha
Fang, 2016 China RCT Scheduled for elective surgery; ASA I-II; D: 62 patients; 20-60 years; S: 62 patients; 20-60 years
D: 0.1 mg/kg 10 min before the induction of anesthesia; C: 0.9% saline 10 min before the induction of anesthesia
Fentanyl 5 ug/kg intravenously injection in 3 s; 2 min later, midazolam 0.1 mg/kg, etomidate 0.3 mg/kg, rocuronium bromide 0.8 mg/kg
Incidence of cougha
Huang et al., 2015 China RCT Scheduled for elective surgery; ASA I-II; D: 50 patients; 44±11 years; C: 50 patients; 45±11 years
D: 0.1 mg/kg (10 ml) 5 min before the induction of anesthesia; C: 0.9% saline (10 ml) 5 min before the induction of anesthesia
Sequentially intravenously injection of fentanyl 3 ug/kg (within 5 s) and other anesthetics (not reported in detail)
Incidence of cougha
Liu et al., 2015 China Double-blind, RCT
Scheduled for elective surgery; ASA I-II; D: 185 patients; 52±13 years; C: 185 patients; 53±11 years
D: 0.1 mg/kg 3-5 s before the induction of anesthesia; C: 0.9% saline 3-5 s before the induction of anesthesia
Standardized anesthesia induction (details not reported); 2 min after anesthesia induction, all patients received 0.5 ug/kg sufentanil over 3 s
Incidence of cougha
Meng et al., 2013 China RCT Scheduled for elective surgery; ASA I-II; D: 40 patients; 43.5±13.3 years; C: 40 patients; 43.4±9.6 years
D: 0.1 mg/kg 8 min before the induction of anesthesia; C: 0.9% saline 8 min before the induction of anesthesia
Midazolam 0.1 mg/kg, 2 min later intravenously injection of fentanyl 0.4 ug/kg (in 2 s), propofol 2 mg/kg and rocuronium bromide 1 mg/kg
Incidence of coughb
Pi et al., 2015 China RCT Scheduled for elective surgery; ASA I-II; D: 50 patients; 46.2±8.6 years; C: 50 patients; 44.8±7.7 years
D: 0.1 mg/kg 10 min before the induction of anesthesia; C: 0.9% saline 10 min before the induction of anesthesia
Fentanyl 4 ug/kg intravenously injection in 3 s; propofol 2 mg/kg and rocuronium bromide 0.6 mg/kg
Incidence of coughb
Qiu et al., 2016 China RCT Scheduled for elective surgery; ASA I-II; D: 60 patients; 33±10 years; N: 60 patients; 36±8 years
D: 0.1 mg/kg 2 min before the induction of anesthesia; C: 0.9% saline 2 min before the induction of anesthesia
Fentanyl 3 ug/kg intravenously injection in 3 s; 2 min later, propofol and cetatriptan were injected (not reported in detail)
Incidence of cougha
Sun et al., 2011 China Double-blind, RCT
Scheduled for elective surgery; ASA I-II; D: 60 patients; 46.6±10.3 years; C: 60 patients; 48.2±10.6 years
D: 0.1 mg/kg 10 min before the induction of anesthesia; C: 0.9% saline 10 min before the induction of anesthesia
Midazolam 0.1 mg/kg, fentanyl 5 ug/kg, propofol 1-1.5 mg/kg, and suxamethonium 1.5 mg/kg; the injection time of fentanyl was limited to under 2 s; propofol and suxamethonium were administered 2 min later, after the fentanyl bolus
Incidence of cougha

Dezocine in fentanyl-induced cough
15870 Int J Clin Exp Med 2017;10(12):15866-15877
Wang et al., 2016 China RCT Scheduled for elective surgery; ASA I-II; D: 30 patients; 41±13 years; C: 30 patients; 39±13 years
D: 0.1 mg/kg 1 min before the induction of anesthesia; C: 0.9% saline (2 ml) 1 min before the induction of anesthesia
Fentanyl 4 ug/kg intravenously injection in 3 s; 1 min later, midazolam 0.1 mg/kg, propofol 2 mg/kg, cisatriptan 0.2 mg/kg
Incidence of coughb
Wang and Liu, 2015 China RCT Scheduled for elective surgery; ASA I-II; D: 30 patients; 45±12 years; C: 30 patients; 40±11 years
D: 0.1 mg/kg 1 min before the induction of anesthesia; C: 0.9% saline 1 min before the induction of anesthesia
Fentanyl 4 ug/kg intravenously injection in 3 s; 15 s later, intravenously injection of midazolam 0.1 mg/kg, propofol 2 mg/kg and cisatracurium 0.2 mg/kg
Incidence of coughc
Wang, 2015 China RCT Scheduled for elective surgery; ASA I-II; D1: 25 patients; 72.0±2.8 years; D2: 25 patients; 69.6±3.1 years; D3: 25 patients; 70.7±2.7 years; C: 25 patients; 71.1±3.3 years
D1: 0.04 mg/kg; D2: 0.08 mg/kg; D3: 0.12 mg/kg 5 min before the induction of anesthesia; C: 0.9% saline (5 ml) 5 min before the induction of anesthesia
Fentanyl 0.3 ug/kg intravenously injection in 5 s Incidence of coughb
Xu et al., 2015 China Double-blind, RCT
Scheduled for elective surgery; ASA I-II; D1: 100 patients; 46±13 years; D2: 100 patients; 43±14 years; D3: 100 patients; 44±14 years; C: 100 patients; 45±12 years
D1: 0.025 mg/kg; D2: 0.05 mg/kg; D3: 0.1 mg/kg just before the induction of anesthesia; C: 0.9% saline just before the induction of anesthesia
Fentanyl 3 ug/kg intravenously injection in 5 s Incidence of cougha
Yuan and Chen, 2015 China RCT Scheduled for elective surgery; ASA I-II; D1: 30 patients; 22-55 years; D2: 30 patients; 22-55 years; D3: 30 patients; 22-55 years; C: 30 patients; 22-55 years
D1: 0.05 mg/kg; D2: 0.1 mg/kg; D3: 0.2 mg/kg 10 min before the induction of anesthesia; C: 0.9% saline 10 min before the induction of anesthesia
Intravenously injection of fentanyl 3 ug/kg; 2 min later, midazolam 0.05 mg/kg, etomidate 0.3 mg/kg, cisatracurium 0.2 mg/kg
Incidence of cougha
Zhang and Cao, 2013 China RCT Scheduled for elective surgery; ASA I-II; D: 40 patients; 46±5.9 years; C: 40 patients; 47±4.8 years
D: 0.1 mg/kg 10 min before the induction of anesthesia; C: 0.9% saline (2 ml) 10 min before the induction of anesthesia
Midazolam 0.1 mg/kg; 2 min later, intravenously injection of fentanyl 3 ug/kg in 3 s, propofol 1.5-2 mg/kg and rocuronium bromide 1 mg/kg
Incidence of coughb
RCT: randomized controlled trial; D: dezocine group; C: control group; incidence of cougha: incidence of cough in 2 minutes after fentanyl injection; incidence of coughb: incidence of cough in 1 minute after fentanyl injection; incidence of coughc: incidence of cough in 15 seconds after fentanyl injection.

Dezocine in fentanyl-induced cough
15871 Int J Clin Exp Med 2017;10(12):15866-15877
neity existed. Sensitivity analysis was per-formed to determine the potential source of heterogeneity by removing each of the related studies one at a time and evaluating the result-ing effect. Funnel plots were used to assess the publication bias, forest plot and funnel plot were generated via RevMan 5.3 (Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014).
Results
Literature search results
An initial literature search yielded a total of 172 potential eligible studies including 6 from Pubmed, 37 from EMBASE, 5 from CENTRAL, 17 from ISI Web of Science and 107 from CNKI. 24 duplicates for retrieving were deleted and 148 potential relevant studies were screened for titles and abstracts. Finally, 18 studies were downloaded for a full-text screen, 1 study was duplicate for publication, 1 was not relevant and 1 used unsuitable intervention. The remain-ing 15 articles [19-33] were deemed eligible to be included in this review (Figure 1).
Characteristics of included studies
Twelve studies were included in our systematic review, all of them were conducted in China and published from 2011 to 2015. Each study was performed in a single center, 3 of them [22, 25, 28] were written in English while the remaining 9 studies [19-21, 23, 24, 26, 27, 29, 30] were written in Chinese and published in Chinese academic journals. A total of 1080 subjects scheduled for elective surgeries were assigned into dezocine groups and 690 homogeneous participants were allocated into control groups. All the enrolled subjects were administered
Figure 2. Risk of bias graph: review authors’ judgements about each risk of bias item presented as percentages across all included studies.
Figure 3. Risk of bias summary: review authors’ judgements about each risk of bias item for each in-cluded study.
the fixed-effect model would be used. The chi-squared test and the Higgins I2 test were used to assess the het-erogeneity among studies (P>0.1 and I2 indicate accept-able heterogeneity). The inci-dences of FIC in control groups were combined using the same method. Subgroup-analysis according to meth-odological quality and dose of fentanyl injection was per-formed if obvious heteroge-

Dezocine in fentanyl-induced cough
15872 Int J Clin Exp Med 2017;10(12):15866-15877
with dezocine solution or normal saline with the same volume prior to anesthesia induction. Four studies [20, 26, 28, 29] employed a four-arm parallel design to compare clinical effect of different doses of dezocine administration with placebo control, the other eight studies used a two-arm parallel design. The doses of dezocine administration varied from 0.05 mg/kg to 0.20 mg/kg, occurrence of FIC within two minutes after fentanyl injection was observed in all the studies (Table 1).
Risk of bias assessment
The risk of bias among studies were assess- ed using the Cochrane Collaboration’s Tool. All
the included studies claimed that they have assigned patients randomly into dezocine and control groups, but only half of the studies reported method of random sequence genera-tion. Two studies [22, 28] provided detailed information about allocation concealment and double-blind. Study conducted by Sun and co-workers [25] employed double-blind, but they failed to report procedure of allocation conceal-ment. In addition, two studies [27, 30] as- sessed outcomes by a postoperative obser- ver who was blind to the patients’ assigned groups. Good compliance seemed to be achi- eved by all studies, all the recruited subjects finished their trial (Figure 2 and Figure 3).
Figure 4. Forest plot of low dose dezocine versus control: incidence of FIC.
Figure 5. Forest plot of 0.1 mg/kg dezocine versus control: incidence of FIC, subgroup by study design.

Dezocine in fentanyl-induced cough
15873 Int J Clin Exp Med 2017;10(12):15866-15877
Meta-analyses
Before the meta-analysis was conducted, we divided different comparisons into three groups according to the doses of dezocine administra-tion: low-dose (<0.1 mg/kg), 0.1 mg/kg and high-dose (>0.1 mg/kg). Four studies [20, 26, 28, 29] compared low-dose dezocine with nor-mal saline injection. No obvious heterogeneity was present (P=0.76, I2=0%), so the fixed-effect model was employed for statistical analysis. The pooled data indicated that low-dose dezo-cine administration could significantly reduce the incidence of FIC when compared with pla-cebo control (RR 0.20, 95% CI 0.13, 0.30; P<0.00001) (Figure 4). Fourteen studies [19-25, 27-30] administered dezocine with a dos-age of 0.1 mg/kg. As the heterogeneity across studies was obvious, random-effect model was used (P<0.0002, I2=67%). The combination of
data showed that 0.1 mg/kg of dezocine ad- ministration could significantly reduce the inci-dence of FIC (RR 0.10, 95% CI 0.08, 0.14; P<0.00001) (Figure 5 and Figure 6). Three studies [20, 26, 29] compared high-dose dezo-cine with normal saline control, we used fixed-effect model because no obvious heterogene-ity was present (P=0.56, I2=0%). The result of meta-analysis indicated a significant lower incidence of FIC in dezocine groups than it in control groups (RR 0.20, 95% CI 0.11, 0.36; P<0.00001) (Figure 7).
Subgroup-analysis
Subgroup-analysis in the comparison of 0.1 mg/kg dezocine versus control was conducted according to pre-determined criteria, three studies [22, 25, 28] with double-blinding and the remaining eight studies without double-
Figure 6. Forest plot of 0.1 mg/kg dezocine versus control: incidence of FIC, subgroup by dosage of fentanyl injec-tion.

Dezocine in fentanyl-induced cough
15874 Int J Clin Exp Med 2017;10(12):15866-15877
Figure 7. Forest plot of high dose dezocine versus control: incidence of FIC.
blinding were assigned into two subgroups. The heterogeneity within two subgroups were then acceptable and the results of two groups were consistent (double-blind RCT: RR 0.01, 95% CI 0.00, 0.05; P<0.00001; I2=0%; RCT without double-blinding: RR 0.19, 95% CI 0.12, 0.28; P<0.00001; I2=46%) (Figure 5). Stratified anal-ysis by dose of fentanyl injection indicated that 0.1 mg/kg dezocine was effective in attenuat-ing FIC when patients were injected with differ-ent dose of fentanyl (<3 ug/kg group: RR 0.01, 95% CI 0.00, 0.08; 3 ug/kg group: RR 0.11, 95% CI 0.06, 0.17; >3 ug/kg group: RR 0.15, 95% CI 0.10, 0.23) (Figure 6). Sensitivity-ana- lysis also revealed that the effect of 0.1 mg/ kg dezocine administration was firm when we removed each of the related studies one at a time (detailed data not shown).
Adverse events
Wang et al. [27] reported that six patients in dezocine groups were with dizziness and 4 patients were with somnolence, Yuan and co-workers [29] documented that two patients who were administered with dezocine were with dizziness and one patient was with somno-lence. Four studies [22, 25, 27, 28] reported that there were no adverse events associated with dezocine administration.
Discussion
To the best of our knowledge, there is no pub-lished systematic review that summarizes all the potential RCTs to assess the clinical effect of dezocine in the prevention of FIC. Our current work highlights the definite efficacy of dezocine administration, the curative effect of dezocine injection was consistent when administered with different doses. However, the conclusion is hampered by methodological deficiencies of several studies, and the evidence supporting the safety of dezocine was insufficient.
Fentanyl was widely used in many areas among the world, especially in those developing coun-tries. Although various mechanisms responsi-ble for FIC have been proposed, the exact mechanism remains unclear. Several hypothe-ses have been proposed, including (1) some kind of opioid receptors, perhaps μ-receptor, exist the respiratory tract, which participated in cough and played an important mediating role [34]; (2) fentanyl could inhibit central sympa-thetic outflow, thereafter activating the vagus nerve [35]; (3) histamine and neuropeptides released after intravenous fentanyl administra-tion involve in FIC [34, 36]; (4) a pulmonary che-moreflex mediated by either irritant receptors (rapidly adapting receptors) or vagal C-fiber receptors near the pulmonary vessels might play a role in FIC [37]; and (5) stimulation of the irritant receptors in the upper pulmonary muco-sa secondary to fentanyl-induced tracheal smooth muscle constriction [38].
Animal experiments have demonstrated that the use of a low-efficacy opioid in association with a high efficacy opioid will not only enhance the analgesic effect but also antagonize some of undesirable side effects of the higher effica-cy opioid, such as pruritus and nausea. The double benefit effect may due to the opioid receptors agonized and antagonized [25]. A potential explanation for the clinical effect of dezocine is that dezocine suppresses FIC by κ-receptor antagonism or inhibits norepineph-rine and serotonin reuptake. In addition, the documented adverse events associated with dezocine administration seemed scarce, but the existing evidence to support the safety of dezocine is not sufficient, only six studies re- ported slight side effects in dezocine groups.
The pooled data in our analysis revealed a 51% incidence of FIC in normal saline injec- tion groups. There were several factors report-

Dezocine in fentanyl-induced cough
15875 Int J Clin Exp Med 2017;10(12):15866-15877
ed involving discrepancies on incidence of FIC, including: (1) age, incidence of fentanyl-induced cough is high in infants and children, even in small doses (1 µg/kg) [39]; (2) smoking, a con-troversy conclude on the implication of smok-ing, even considered a protective factor against fentanyl-induced cough [40]; (3) ethnicity, the incidence of FIC in Asian population is more obvious than it in European one [41]; (4) dose of fentanyl injection, incidence of FIC increases proportionally with the doses [42]; (5) speed of injection, a longer injection time can reduce the incidence of FIC [40]; (6) route of administra-tion, peripheral intravenous injection could re- duce incidence of FIC than injection by a cen-tral line [7].
All of our included studies achieved a baseline similarity, and the ethnicity of enrolled subjects were all Han nationality, fentanyl was injected intravenously. However, the dose and speed of fentanyl injection were inconsistent across studies. We firstly stratified all included studies based upon the doses of dezocine injection, each comparison revealed a significant efficacy of dezocine in the prevention of FIC. As the het-erogeneity within 0.1 mg/kg group was pres-ent, we subsequently divided these studies according to whether double-blinding was per-formed in their studies, both subgroups indi-cated that dezocine was more effective than saline. Considering that the lack of blinding might lead to exaggeration of conclusions, the results of subgroup-analysis was in contrary to our expectation, RCTs with double-blinding yielded a significantly better effect of dezocine than RCTs without blinding, no FIC occurred in the studies with double-blinding. With regard to this discrepancy, future studies with rigorous study design and sufficient sample-size are urgently needed. Subgroup-analysis was also conducted according to the dose of fentanyl injection, dezocine administration was effec-tive in attenuating FIC regardless of dose of fentanyl injection. However, the heterogeneity in high dose fentanyl group (>3 ug/kg) was still obvious, suggesting that some other con-founding factors such as speed of fentanyl injection, insufficient sample sizes should be questioned.
There are several limitations of our study. Firstly, the majority of included studies had sev-eral methodological deficiencies, which could limit the value of conclusions regarding the
clinical effect of dezocine administration in general anesthesia; the majority of studies failed to provide detailed information about method for random sequence generation and procedure of allocation concealment. Secondly, the now-existing evidence in terms of the safety of dezocine was insufficient to guarantee that dezocine is a routine medication in general anesthesia, the majority of our included studies did not document adverse events associated with dezocine administration. Thirdly, our in- cluded studies were all conducted in China, only three trials were published in English, the remaining were written in Chinese, making it difficult for foreign researchers to get access and understand the content. This might be a result of different countries’ drugs admittance system, dezocine may not be accessible in every country nor available for clinical applica-tion in all hospitals. Thus, future larger-scale RCTs within western context are recommend-ed. Lastly, as the baseline incidence of FIC was reported to be around 40%, assuming a 50% decrease of incidence of FIC after dezocine administration, 81 patients were required in each group to achieve 80% power at a two-sid-ed 5% significance level based on our calcula-tion (PASS software, version 12.0, available on www.ncss.com). However, only two of our selected studies reached this standard.
In conclusion, the findings of this meta-analysis suggest that dezocine administration could effectively suppress the occurrence of fentanyl-induced cough during general anesthesia, irre-spective of dosage. Conclusion regarding the safety of dezocine administration could not be drawn due to the paucity of evidence provided by our included studies. Additional studies with larger-scale and rigorous study-design are still needed.
Conclusion
The findings of our current work suggested a definite effect of dezocine administration in the prevention of FIC in general anesthesia induc-tion, conclusions regarding the safety of dezo-cine could not be drawn due to the paucity of existing evidence. Additional RCTs with larger scale and rigorous design are still needed.
Acknowledgements
Project supported by National Nature Science Foundation of China (NO: 81670911).

Dezocine in fentanyl-induced cough
15876 Int J Clin Exp Med 2017;10(12):15866-15877
Disclosure of conflict of interest
None.
Abbreviations
FIC, Fentanyl induced cough; RCTs, Randomized controlled trials; ASA, American Society of Anesthesiologists; PRISMA, Preferred Repo- rting Items for Systematic Reviews and Meta-Analyses; MeSH, Medical Subheadings; RR, Risk ratio; CIs, confidence intervals.
Address correspondence to: Zheng-Tao Lv, Depart- ment of Orthopedics, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Te- chnology, 1095#, Jie-Fang Avenue, Qiaokou District, Wuhan 430030, Hubei, China. Tel: +86-13147104- 691; Fax: +86-027-83663670; E-mail: 630105- [email protected]; Jia Zhang, Department of Otolary- ngology, Affiliated Eye and ENT Hospital of Fudan University, Shanghai, China. E-mail: sysuzhangjia@ 163.com
References
[1] Zawilska JB. An expanding world of novel psy-choactive substances: opioids. Front Psychia-try 2017; 8: 110.
[2] Ko SH, Kim DC, Han YJ and Song HS. Small-dose fentanyl: optimal time of injection for blunting the circulatory responses to tracheal intubation. Anesth Analg 1998; 86: 658-661.
[3] Adachi YU, Satomoto M, Higuchi H and Wata-nabe K. Fentanyl attenuates the hemodynamic response to endotracheal intubation more than the response to laryngoscopy. Anesth Analg 2002; 95: 233-237, table of contents.
[4] Shen JC, Xu JG, Zhou ZQ, Liu HJ and Yang JJ. Effect of equivalent doses of fentanyl, sufent-anil, and remifentanil on the incidence and severity of cough in patients undergoing ab-dominal surgery: a prospective, randomized, double-blind study. Curr Ther Res Clin Exp 2008; 69: 480-487.
[5] Ho CN and Hung KC. Effect of swallowing ma-neuver on fentanyl-induced coughing. J Anesth 2017; 31: 920.
[6] Kelly HE, Shaw GM, Brett CN, Greenwood FM and Huckabee ML. The effect of titrated fen-tanyl on suppressed cough reflex in healthy adult volunteers. Anaesthesia 2016; 71: 529-534.
[7] Bohrer H, Fleischer F and Werning P. Tussive effect of a fentanyl bolus administered through a central venous catheter. Anaesthesia 1990; 45: 18-21.
[8] Lin CS, Sun WZ, Chan WH, Lin CJ, Yeh HM and Mok MS. Intravenous lidocaine and ephedrine, but not propofol, suppress fentanyl-induced cough. Can J Anaesth 2004; 51: 654-659.
[9] Yu MS, Kim JY and Kim HY. Intravenous dexa-methasone pretreatment reduces remifentanil induced cough. Korean J Anesthesiol 2011; 60: 403-407.
[10] Tweed WA and Dakin D. Explosive coughing af-ter bolus fentanyl injection. Anesth Analg 2001; 92: 1442-1443.
[11] Liu HL, An LJ, Su Z, Zhang Y and Gui B. Magne-sium sulphate suppresses fentanyl-induced cough during general anesthesia induction: a double-blind, randomized, and placebo-con-trolled study. Int J Clin Exp Med 2015; 8: 11332-11336.
[12] Firouzian A, Emadi SA, Baradari AG, Mousavi R and Kiasari AZ. Can low dose of propofol ef-fectively suppress fentanyl-induced cough dur-ing induction of anaesthesia? A double blind randomized controlled trial. J Anaesthesiol Clin Pharmacol 2015; 31: 522-525.
[13] Saleh AJ, Zhang L, Hadi SM and Ouyang W. A priming dose of intravenous ketamine-dexme-detomidine suppresses fentanyl-induced cou- ghing: a double-blind, randomized, controlled study. Ups J Med Sci 2014; 119: 333-337.
[14] Uvelin A and Rakic G. Guidelines for prevention of fentanyl-induced cough. Acta Anaesthesiol Scand 2009; 53: 1228-1229.
[15] Downing JW, Brock-Utne JG, Barclay A and Schwegmann IL. WY 16225 (dezocine), a new synthetic opiate agonist-antagonist and potent analgesic: comparison with morphine for relief of pain after lower abdominal surgery. Br J An-aesth 1981; 53: 59-64.
[16] Sun Q, Zhou W, Wu B, Ji MH and Peng YG. Dezocine: a novel drug to prevent fentanyl-in-duced cough during general anesthesia induc-tion? J Anesth 2012; 26: 470.
[17] Moher D, Liberati A, Tetzlaff J, Altman DG and Group P. Preferred reporting items for system-atic reviews and meta-analyses: the PRISMA statement. PLoS Med 2009; 6: e1000097.
[18] Higgins JPT, Green S, editors. Cochrane Hand-book for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Co-chrane Collaboration, 2011. Available from www.cochrane-handbook.org.
[19] Cai H, Li L and Han XP. Effect of combined use of fentanyl and dezocine on etomidate-in-duced myoclonus during anesthesia induction. Shanghai Medical Journal 2015; 38: 103-105.
[20] Gao YP, Liang XN, Sun JH and Li XR. Efficacy of different doses of dezocine injection in the pre-vention of fentanyl induced cough. Journal of Clinical Medicine in Practice 2013; 17: 155-156.

Dezocine in fentanyl-induced cough
15877 Int J Clin Exp Med 2017;10(12):15866-15877
[21] Huang MH, Wang H, Xu J and Li P. Comparison of oxycodone and dezocine for prevention of fentanyl-induced cough during anesthesia in-duction. Chinese Journal of Anesthesiology 2015; 35: 787-789.
[22] Liu XS, Xu GH, Shen QY, Zhao Q, Cheng XQ, Zhang J and Gu EW. Dezocine prevents sufent-anil-induced cough during general anesthesia induction: a randomized controlled trial. Phar-macological Reports 2015; 67: 52-55.
[23] Meng ZZ, Zhang L, Wang SD, Li Q and Ma JB. Feasibility of dezocine required to prevent suf-entanil-induced cough during anesthesia in-duction. Progress in Modern Biomedicine 2013; 13: 1911-1913.
[24] Pi MF, Chen C, Hou J, Lin L and Tang WY. Effect of dezocine premediation on inhibition of fen-tanyl induced irritating cough. Jilin Medical Journal 2015; 36: 1971-1972.
[25] Sun ZT, Yang CY, Cui Z, Zhang J and Han XP. Effect of intravenous dezocine on fentanyl-in-duced cough during general anesthesia induc-tion: a double-blinded, prospective, random-ized, controlled trial. Journal of Anesthesia 2011; 25: 860-863.
[26] Wang LP. Comparison of different doses of dezocine injection in the treatment of fentanyl induced cough. Contemporary Medical Sympo-sium 2015; 13: 222-223.
[27] Wang Z and Liu W. Dezocine and dexametha-sone inhibition of choking cough reflex induced by fentanyl. Journal of Clinical Medical Litera-ture 2015; 2: 1198-1199.
[28] Xu Y, Zhu Y, Wang S, Ren Y and Miao C. Dezo-cine attenuates fentanyl-induced cough in a dose-dependent manner-a randomized con-trolled trial. International Journal of Clinical and Experimental Medicine 2015; 8: 6091-6096.
[29] Yuan MF and Chen Y. Effect of dezocine injec-tion in fentanyl induced cough. Jiangsu Medi-cal Journal 2015; 41: 2176-2177.
[30] Zhang JF and Cao HZ. Clinical effect of dezo-cine in the prevention of fentanyl induced cough, observation of 40 case. Medical Jour-nal of Communications 2013; 27: 680-681.
[31] Fang L. Inhibitory effect of dezocine on fentan-yl-induced cough during general anesthesia induction. Journal of Clinical Medical 2016; 3: 5457-5460.
[32] QIU LC, Yao YS, Wu XD, Chen YQ, Dai DS and Guo YH. Comparison of oxycodone hydrochlo-ride versus dizocine for suppression of fentan-ylinduced coughing during induction of general anesthesia. Journal of Trauma and Emergency 2016; 4: 89-91.
[33] Wang Z, Dong YH and Chen ZY. Comparison of the supressive effect of dezocine, lidocine and ephedrine on fentanyl-induced cough. Journal of Pharmaceutical Practice 2016; 34: 463-463.
[34] Yu J, Lu Y, Dong C, Zhu H and Xu R. Premedica-tion with intravenous dexmedetomidine-mid-azolam suppresses fentanyl-induced cough. Ir J Med Sci 2012; 181: 517-520.
[35] Ai Q, Hu Y, Wang Y, Wu S, Qin Z, Wang J, Wang G, Zhang J and An M. Pentazocine pretreat-ment suppresses fentanyl-induced cough. Ph- armacol Rep 2010; 62: 747-750.
[36] Gu C, Zhou M, Wu H, Li F and Tang Q. Effects of different priming doses of fentanyl on fentanyl-induced cough: a double-blind, randomized, controlled study. Pharmacol Rep 2012; 64: 321-325.
[37] Ambesh SP, Singh N, Gupta D, Singh PK and Singh U. A huffing manoeuvre, immediately be-fore induction of anaesthesia, prevents fentan-yl-induced coughing: a prospective, random-ized, and controlled study. Br J Anaesth 2010; 104: 40-43.
[38] Schlimp CJ and Wiedermann FJ. Does fentanyl-induced cough justify pre-treatment with iv li-docaine 2 mg.kg-1. Can J Anaesth 2005; 52: 207.
[39] Han JI, Lee H, Kim CH and Lee GY. The frequen-cy of fentanyl-induced cough in children and its effects on tracheal intubation. J Clin Anesth 2010; 22: 3-6.
[40] Lin JA, Yeh CC, Lee MS, Wu CT, Lin SL and Wong CS. Prolonged injection time and light smoking decrease the incidence of fentanyl-induced cough. Anesth Analg 2005; 101: 670-674, table of contents.
[41] Phua WT, Teh BT, Jong W, Lee TL and Tweed WA. Tussive effect of a fentanyl bolus. Can J Anaesth 1991; 38: 330-334.
[42] Iida K, Handa M, Fukuda K, Saita N, Kasahara M, Koukita Y, Urabe A, Hayashida M, Ichinohe T and Kaneko Y. Incidence and onset time of fentanyl-induced cough depends on the dose of IV fentanyl. Masui 2009; 58: 962-965.