Embed Size (px)
Citation preview

Review ArticleCognitive Interventions in Older Persons: Do They Changethe Functioning of the Brain?
Yindee van Os,1 Marjolein E. de Vugt,2 and Martin van Boxtel2
1Department of Medical Psychology, Elkerliek Hospital, Wesselmanlaan 25, 5507 HA Helmond, Netherlands2School for Mental Health and Neuroscience, Alzheimer Centre Limburg, Department of Psychiatry and Neuropsychology,Maastricht University, P.O. Box 616, 6200 MDMaastricht, Netherlands
Correspondence should be addressed to Yindee van Os; [email protected]
Received 13 February 2015; Revised 5 May 2015; Accepted 18 May 2015
Academic Editor: Emmanuel Moyse
Copyright © 2015 Yindee van Os et al. This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Background. Cognitive interventions for older persons that may diminish the burden of cognitive problems and could delayconversion to dementia are of great importance. The underlying mechanisms of such interventions might be psychologicalcompensation and neuronal plasticity. This review provides an overview of the literature concerning the evidence that cognitiveinterventions cause brain activation changes, even in damaged neural systems. Method. A systematic search of the literature wasconducted in several international databases, Medline, Embase, Cinahl, Cochrane, and Psychinfo. The methodological qualitywas assessed according to the guidelines of the Dutch Institute for Health Care Improvement (CBO). Results. Nineteen relevantarticles were included with variedmethodological quality. All studies were conducted in diverse populations from healthy elderly topatients with dementia and show changes in brain activation after intervention.Conclusions.The results thus far show that cognitiveinterventions cause changes in brain activation patterns.The exact interpretation of these neurobiological changes remains unclear.More study is needed to understand the extent to which cognitive interventions are effective to delay conversion to dementia. Futurestudies should more explicitly try to relate clinically significant improvement to changes in brain activation. Long-term follow-updata are necessary to evaluate the stability of the effects.
1. Introduction
Aging is accompanied by changes in our cognitive function-ing based on structural and functional changes in the brain [1,2]. Many older persons complain about diminished cognitivefunctioning [3]. Cognitive complaints and cognitive deficitsare often a burden for older persons and their family [4–6]. Cognitive deficits could also be a precursor for dementia.In that case it is important to intervene in an early stage toprevent or delay conversion to dementia and to minimizethe impact of these objective or perceived cognitive problems[5, 7].
Pharmacological interventions are of limited efficacy,may have serious side effects, and are only available forpatients with a clinical diagnosis of dementia [8]. Cognitiveinterventions have gained a lot of attention over the last
years.Themain goal of cognitive interventions is to stimulatethe cognitive system or offer compensatory methods toaddress difficulties with cognitive functioning [7, 9]. Clin-icians acknowledge the benefits of cognitive interventionssuch as changing a patient’s sets of beliefs, affective states, orbehavioural patterns and compensating for cognitive losses[10].
A literature review performed by Buschert and colleaguesin 2010 highlights the effectiveness of cognitive interventionsin improving global cognitive functioning, daily activities,quality of life, and diminishing behavioural problems inpatients withMild Cognitive Impairment (MCI) or dementia[8]. A review of randomized controlled trials on this topicin persons with MCI concluded that there is evidence forintervention success in overall cognition, overall self-ratings,episodic memory, and executive function/working memory.
Hindawi Publishing CorporationBioMed Research InternationalVolume 2015, Article ID 438908, 14 pageshttp://dx.doi.org/10.1155/2015/438908

2 BioMed Research International
The quality of the evidence is limited due to several method-ological issues such as a small amount of long-term follow-upmeasures with generally small effect sizes. Moreover there aredifferences in design, sample sizes, and types of intervention[11].
Cognitive stimulation in a social setting such as remi-niscence with reality orientation is associated with benefitsin cognitive functioning as well as quality of life, well-being, communication, and social interaction skills [9].In healthy elderly, cognitive interventions lead to fewernegative emotional reactions towards cognitive functioning[3, 12, 13], improvement in coping with reported cognitivefailures [12, 13], and better objective cognitive functioning[13, 14]. Another important goal of cognitive interventionsis intervening at an early stage of cognitive decline to slowor prevent progression to dementia. Cognitive interventionscould even have the potential to delay the onset ofAlzheimer’sDementia (AD) by 5 years in those patients at risk for AD[8]. The evidence for the efficacy of cognitive interventionsis promising yet inconclusive due to differences in design,outcome measures, interventions, and sample sizes. The lowcosts, absence of adverse effects, and the possibility to delaythe onset of Alzheimer’s dementia make cognitive interven-tions attractive [8]. Some even stated that neurobiologicaloutcomes might be used as a sensitive biomarker for theefficacy of cognitive training [15].
Themechanisms underlying the effectiveness of cognitiveinterventions are not well understood. A better understand-ing of these mechanisms can help us tailor our cognitiveinterventions and possibly improve the effectiveness.
One mechanism might be psychological compensation.Cognitive interventions would then improve coping strate-gies to deal with the still existing cognitive problems [3].In clinical practice, the working mechanism and goalsof cognitive interventions are explained to participants interms of this psychological compensation. But recent neuralmodels suggest that neuronal plasticity may also underliethe effectiveness of cognitive interventions [5, 8, 16–18].Cognitive interventions might increase cognitive reserve thatis reflected in changes in brain activation patterns [4, 8].Cognitive reserve, the capacity of an adult brain to copewith brain pathology in order to minimize symptomatology,is linked to efficiency (less activation of brain networks) inhealthy elderly. On the other hand, in pathological aging,cognitive reserve enhances the recruitment of compensatingbrain networks particularly the frontal areas, hippocampus,and the precentral gyrus [1, 19].
The aim of this paper is to review the evidence that cog-nitive interventions cause brain activity changes. Eventually,early intervention in prodromal stages to delay conversion topathological aging is the ultimate goal.Therefore the effects ofcognitive interventions on brain activity changes are studiedin the brain of healthy older persons and in the brain of olderpersons suffering from pathological aging. To relate changesin brain activation to intervention effect, evidence of changesin performance, function, behaviour, and cognition are alsoreviewed.
2. Methods
2.1. Search Strategy. A systematic literature search of articlespublished from 1993 to March 2012 was conducted in Med-line, Embase, Cinahl, Psychinfo, and the Cochrane Database.Medical Subject Headings (MeSH) terms, thesaurus terms,and an age selection> 60 yearswere used in the search (searchterms used in selection of studies) as follows:
(1) Psychinfo: cognitive impairment OR dementia ORage selection set on > 60 years, Medline and Cinahl:cognition disorder OR dementia OR aged OR elderly,and Embase: cognitive defect OR dementia OR agedOR elderly;
(2) Psychinfo: behavioural therapy OR cognitive therapyMedline, Cinahl, Embase: behavior therapy OR cog-nitive therapy;
(3) Psychinfo: magnetic resonance imaging OR tomog-raphy OR electrophysiology, Medline and Cinahl:magnetic resonance imaging OR electroencephalog-raphyOR tomography, andEmbase: nuclearmagneticresonance imaging OR electroencephalogram ORtomography.
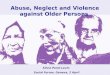
Reference lists of the retrieved studies were searched to iden-tify any relevant articles that had not yet been included. Tobe selected for this review, papers had to meet the followingcriteria: (i) the study had to involve the healthy elderly, thehealthy elderly with cognitive complaints, and the elderlywith Mild Cognitive Impairment or elderly with dementia;(ii) the study had to contain a cognitive intervention; (iii) thestudy had comparisons of brain activitymeasurements beforeand after the intervention; (iv) the study had a full reportavailable; (v) the articles were in English. A flowchart of theinclusion process is shown in Figure 1.
2.2. Selection of Studies. The search resulted in 735 papers.One reviewer (YvO) screened all titles and abstract forsuitability. Six hundred ninety-six studies were rejectedbecause of duplication, lack of full data, lack of brain activitymeasures, or lack of a cognitive intervention. The remaining39 studies were obtained in full text and assessed by tworeviewers (YvO, MdV). There was full agreement on theexclusion of 23 papers because they did not meet all inclusioncriteria. Amanual search of the reference lists of the includedstudies resulted in 3 additional papers. A total of 19 studiesmet all inclusion criteria. Figure 1 shows the flowchart of theselection process of the papers.
2.3. Methodological Quality. The methodological quality ofthe included studies was assessed according to the guidelinesof the Dutch Institute for Health Care Improvement (CBO).The CBO aims to improve healthcare by providing guide-lines for evidence-based interventions both nationally andinternationally (CBO, http://www.cbo.nl/). For randomizedcontrolled trials, the following aspects were evaluated: ran-domization, blinding of randomization, blinding of partici-pants, blinding of outcome assessors, baseline comparability,

BioMed Research International 3
Possible relevant studies from literature search in databases: 735
Rejected: 696, lack of (functional) neurobiological outcome measurements, lack of full data, lack of cognitive intervention, duplicates
Full text studies for further assessment: 39. Reviewers: YvO,MdV
A total of 16 studies met all inclusion criteria. A manual search of the references resulted in3 more articles that met all inclusion criteria. Reviewers: YvO, MdV
Studies included in this review: 19
Rejected: 23, lack of (functional) neurobiological outcome measurements, lack of full data, lack of a cognitive intervention, participants with acquired brain injury
Figure 1: Flowchart of the search strategy.
loss to follow, use of intent-to-treat analysis, comparability ofintervention, and a judgment of the validity and applicabilityof the study. Because it is impossible in cognitive interventiontrials to blind the therapists to the intervention, this item wasnot included as one of the quality criteria. With regard tostudies that did not contain a randomized controlled design,the following aspects were evaluated: definition of studypopulation, selection bias, intervention description, outcomedefinition, blinded outcome assessments, completeness ofthe dataset/follow-up, loss to follow, confounders, and ajudgment of the validity and applicability of the study.
Eventually, the overall quality of the individual studieswas rated in a level of evidence, ranging from A1 to D. A1 isa systematic review of at least two independent, randomizeddouble-blind studies of sufficient quality and size. A2 isa randomized double blind study of sufficient quality andsize. B is a comparative study, which does not meet all thecriteria of an A2 study. C is a noncomparative study and D isthe opinion of experts (http://www.cbo.nl/). Two reviewers(YvO and MdV) independently assessed the methodologicalquality of the studies. The level of agreement was 96%. Aftera consensus meeting, both reviewers reached full agreementon the quality ratings. The quality ratings of the studies aredisplayed in Tables 1 and 2.
3. Results
3.1. The Healthy Elderly
3.1.1. Study Characteristics. Six studies focused on healthyolder adults [18, 20–23, 30]. Two studies investigated theeffect of the method of loci, a mnemonic technique, onbrain activation [18, 30]. The intervention duration variedbetween these two studies from one day [30] to five weeks[18]. The neurobiological outcomes were different; the one-day intervention used Positron Emission Tomography (PET)measures and a memory test as outcomes [30]. The otherstudy used magnetic resonance imaging (MRI), MagneticResonance Spectroscopy (MRS), performance on a memorytest, and level of depression and anxiety as outcomes. Onestudy lacked a control group [30], and the other study hada randomized controlled trial (RCT) design with a smallsample size.
A third study [20] used a RCT design and studiedthe effect of a multicomponent intervention in 17 olderpersons with mild subjective memory complaints. Eight ofthem took part in the intervention that consisted of a diet,relaxation exercises, brain-teasers, memory strategies, andcardiovascular physical training. The PET and MRI data,performance on cognitive tasks, and scores on the subscale

4 BioMed Research International
Table1:Metho
dologicalqualityof
rand
omized
controlledtrials.
RCT
Theh
ealth
yeld
erly
MCI
Dem
entia
Valenzuela
etal.2003
[18]
Small
etal.200
6[20]
Erickson
etal.2007
[21]
Brehmer
etal.2011
[22]
Belleville
etal.2014
[23]
Rosen
etal.2011
[16]
Ham
pstead
etal.2012
[24]
Heiss
etal.1994
[25]
Akanu
ma
etal.2011
[26]
Forster
etal.2011
[27]
vanPaasschen
etal.2013
[28]
Baglio
etal.2014
[29]
Rand
omized
11
11
11
11
11
11
Blindedrand
omization
00
10
11
10
10
01
Blindedparticipants
00
01
11
10
00
00
Blindedou
tcom
eassessors
00
00
01
00
11
01
Baselin
ecom
parability
01
11
11
11
11
11
Lossto
follo
w1
11
11
11
11
01
1Intention-to-tr
eatanalysis
01
00
01
10
11
10
Com
parabilityinterventio
n0
00
11
11
10
10
1Va
lidity
andapplicability
11
11
11
11
11
11
Total
35
56
79
85
76
56
CBOcla
ssificatio
nB
BB
BA2
A2
BB
BB
BB
TheCB
Ocla
ssificatio
nreflectsthe
levelo
fevidence.A1isa
syste
maticreview
ofatleasttwoindepend
entrando
mized
doub
leblindstu
dies
ofsufficientq
ualityandsiz
e.A2isarand
omized
doub
leblindstu
dyof
sufficientq
ualityandsiz
e.Bisac
omparativ
estudy,w
hich
does
notm
eetallthec
riteriaof
anA2stu
dy.C
isan
oncomparativ
estudy
andDistheo
pinion
ofexperts(http://www.cbo.nl/).

BioMed Research International 5
Table 2: Methodological quality of observational studies.
Observational studiesThe healthyelderly MCI Dementia
Nyberg et al.2003 [30]
Clare et al.2009 [31]
Hampstead2011 [32]
Belleville etal. 2011 [33]
Nagaya etal. 2005 [34]
Tanaka et al.2007 [35]
Spironelli etal. 2013 [36]
Definition study population 0 1 1 1 0 1 1Selection bias 0 0 0 1 0 0 0Intervention description and allocation 1 1 1 1 1 1 1Outcome definition 1 1 1 1 1 1 1Blinded outcome assessments 0 0 0 1 0 0 0Completeness dataset/follow-up 0 1 1 1 0 1 1Loss to follow 0 1 1 1 1 1 1Confounders 1 0 0 1 0 0 0Validity and applicability 0 1 0 1 0 0 1Total 3 6 5 9 3 5 6CBO classification C C C B C C CThe CBO classification reflects the level of evidence. A1 is a systematic review of at least two independent randomized double blind studies of sufficient qualityand size. A2 is a randomized double blind study of sufficient quality and size. B is a comparative study, which does not meet all the criteria of an A2 study. C isa noncomparative study and D is the opinion of experts (http://www.cbo.nl/).
self-awareness of memory ability of the Mood and FeelingsQuestionnaire (MFQ) were collected.
A fourth study [22] evaluated the benefits of 25 sessions ofcomputerized workingmemory training on neuropsycholog-ical tests varying in level of similarity to those practiced in thetraining. FMRImeasures were studied to evaluate differencesin brain activity post intervention. The strength of this studyis the use of an active control group that also received aworkingmemory training but with a fixed low level task load.The intervention group received an adaptive training withincreasing task load.
Two studies [21, 23] studied the effect of repeated practicewith performance feedback on brain activity. Both usedsingle and dual tasks to study focused and divided attention.Belleville and collaborators [23] added a condition in whichparticipants were instructed on themodulation of their atten-tion to the tasks. They were interested if the training formatwould influence brain activity patterns after intervention.To investigate this hypothesis, all 48 community dwellingolder adults were randomly assigned to one of the threeintervention conditions, for example, single task, dual task,or top down control of attention. In the other study the 34older participants were randomly assigned to either a waitinglist or the intervention.
The intervention consists of 5 [21] or 6 [23] sessions.Both used fMRI and MRI as neurobiological outcomes. Thereaction time and accuracy of the task performances werecollected and served in both studies as behavioural data.Moreover both studies statistically examined the relationbetween performance gains and brain activity changes afterintervention.
3.1.2. Findings. The six studies differ in the type of inter-vention, sample size, design, neurobiological outcomes, andthe presence of more clinically relevant outcomes to measure
intervention success (Table 2). All six studies found brainactivity differences after intervention.
Participants in the study of Valenzuela et al. learned thesame mnemonic (method of loci). They showed increases inbrain activation in the hippocampus [18] and the left occipitalparietal cortex and left retrosplenial cortex [30]. These areasare known to be associated with the cognitive domains thatwere targeted in the intervention. Post hoc relation betweenperformance improvement and brain activity changes wasidentified in the Nyberg study. Only the older adults whoalso improved on a memory test showed these brain activityincreases [30].
The study of Small and colleagues (2006) demonstrateddecrease in the dorsolateral brain activation after interven-tion and an improvement in verbal fluency. There was nosignificant intervention effect on subjective measures of self-awareness of memory performance and a memory task [20].
There are three studies that explicitly tried to linkintervention related performance gains to brain activationchanges. Participants that profit the most from an adaptiveworking memory training showed the largest activationdecreases in regions known to be involved in memoryand attention processes (e.g., right inferior frontal, rightinferior parietal, left fusiform region, and insula) and thelargest activation increases in the caudate [22]. Anotherstudy provided evidence that training induced dual taskperformance improvement was related to increased activityin the left ventral prefrontal cortex and decreased activity inthe dorsolateral prefrontal cortex. Compared with an adultsample, age related differences in brain activity were reducedafter intervention [21]. The study of Belleville and colleagues[23] found significant correlations between performance andtraining related activity. They provide evidence that type ofintervention influenced the loci and type of brain activity.Repeated practice in single tasking was associated with a

6 BioMed Research International
decreased activity in the inferior and middle frontal gyribilaterally and the left thalamus. The computed correlationsrevealed that a better performance in single tasking wascorrelated with decreased activity in the right inferior andmiddle frontal gyrus. Repeated training in dual taskingresulted in greater activity in the prefrontal cortex during dualtasking. There were no significant correlations between per-formance gains and brain activity changes for this condition.For the strategic control of attention condition, dependenton the type of instruction, increased activity after training inthe right middle frontal gyrus or the right cerebellum wasseen. An improved ability to modulate attention accordingto task instruction was correlated with a greater activity inBrodmann area 10 [23].
However, how the brain activity changes in all studieswere related to clinical relevant improvement is not clear, dueto a lack of such outcomes and a fail to link brain activationchanges to clinically meaningful improvement [18, 20–23,30]. The stability of the intervention effects was unclear andlong-term follow-up measures were lacking [18, 20–23, 30].
3.2. Patients with MCI
3.2.1. Study Characteristics. All five studies [16, 24, 31–33]that focused on MCI patients used fMRI to investigatethe influence of a cognitive intervention on brain activity.However the targets of the cognitive intervention as well asthe design of the studies differed.
The most recent study with an RCT design evaluated theeffects of a mnemonic strategy training on object locationassociations and brain activation in the hippocampus viafMRI. Amatched control group was also exposed to the samelists of object location associations, but without learning themnemonic. Eighteen participants had a diagnosis of amnesticMCI. A group of 16 healthy controls were allocated to thesame treatment conditions. Both diagnostic groups werecomparable in terms of prognostic factors, and interventionsuccess was evaluated by amodified change score for learningobject location associations [32].
One study used an episodic memory training of 6 weeks(mnemonics and psychoeducation) with proven effectivenessfor a MCI population. Fifteen participants with the diagnosisamnestic MCI and 15 matched healthy controls took partin the intervention. The data on visual memory, MRI, andfMRI were collected at baseline and after intervention. Brainactivity was studied during encoding and retrieval of amemory test. A double baseline was used to study the pos-sibility of a repetition effect. Furthermore preexisting brainactivation differences between both groups were investigatedby comparing fMRI data at baseline [33].
Another study [16] randomly assigned 12 MCI patientsto a cognitive intervention or an active control group. Thecomputer-based cognitive intervention aimed to improveprocessing speed and accuracy of auditory processing. Itwas a time consuming intervention. Participants used thecognitive training five days a week for a hundred minutesper day for two months. The active control group madecomputer-based exercises with comparable time intensity.
Pre- and postintervention fMRI data and a memory test wereadministered [16].
A face-name association learning task was used as anintervention in an earlier study of Hampstead and colleagues[32]. They studied the effect of this face-name associationlearning in six amnestic multidomain MCI patients. ThefMRI was administered before and after the 5 training ses-sions. They compared fMRI results of trained with untrainedlists in different sessions to compensate for repetition effectsof fMRI. Furthermore they computed a functional connectiv-ity analysis [32].
In a single case design, the effect of a goal oriented cogni-tive rehabilitationwas studied in a personwith amnesticMCI.Besides fMRI data, performance on a memory tests and ananxiety and depression questionnaire were collected. Finally,the progress in personal rehabilitation goals was evaluated. Aface-name association learning task was administered duringthe fMRI [31].
3.2.2. Findings. Despite the differences in methodologies,types of intervention, and sample sizes in the studies (seeTable 3), all investigations found evidence for neurobiologicalchanges in brain activation after intervention.
In an RCT study with an active control group, an inter-vention related increase in brain activity in the hippocam-pus was seen, whereas the active control group showeda decreased activity in the hippocampus. Participants thatunderwent the auditory processing training also improved ona memory test and the training tasks [16].
The other RCT study that evaluated amnemonic training,found evidence for an intervention related increased activityin the left hippocampal body and the right hippocampusduring retrieval of the trained stimuli. For retrieval of theuntrained stimuli there was an intervention related increasedactivity in the right hippocampal. Performance improvedafter training for the trained stimuli, not for untrained stimuli[24].
In an earlier multiple cases study by the same author,increased connectivity and increased activity in frontal, pari-etal, temporoparietal areas and precuneus were seen after aface-name association learning training. The six participantsalso improved on trained and untrained memory tasks [32].
A study that evaluated the effect of an episodic memorytraining found increased activity in frontal, temporal, andparietal areas. Some areas were already active at baseline;other areas were new, alternative areas. Only increasedactivity in the right inferior parietal lobe correlated withimprovement on a memory test [33].
A single case study found evidence for a pattern ofbrain activity increases and decreases after a goal orientedcognitive training. Decreases were seen in sensory areasduring both encoding and retrieval, such as the highervisual areas, left fusiform gyrus, left medial occipital gyrus.Increased activity was seen in frontal areas, temporoparietaljunction, parahippocampal gyrus, and right globus pallidus.Both subjective memory satisfaction and subjective memoryperformance improved after the intervention [31].

BioMed Research International 7
Table3:Maincharacteris
ticso
fsele
cted
studies.
Stud
y
Design
Duration
Long
-term
follo
w-u
p𝑛
Interventio
nRe
sultneurob
iologicaloutcomes
Resultbehaviou
raloutcomes
Health
yTh
eelderly
Valenzuelaetal.
(2003)
[18]
RCT
5weeks
Nofollo
w-up
n=20
Metho
dof
loci
Increasedcreatin
eand
cholineinhipp
ocam
pus
Improvem
entinreprod
uctio
nmem
orytask
Noeffecto
ndepressio
nor
anxietyscores
Nybergetal.
(2003)
[30]
Prospectivec
ohort
1day
Nofollo
w-up
n=24
Metho
dof
loci
Acqu
isitio
n:no
grou
pdifferences
Use
phase:adultsandim
proved
elderlyincreased
activ
ityin
interventio
nrelated
areas
8of
16olderp
ersons
noim
provem
entinmem
ory
task
(theu
nimproved
elderly
).8of
16olderp
ersons
andall8
adultsim
proved
inmem
orytask
Smalletal.(200
6)[20]
RCT
14days
Nofollo
w-up
n=17
Multic
ompo
nent
health
prom
otion
Interventio
ngrou
p:decreasedactiv
ityprefrontalcortex
Bette
rverbalfl
uencyin
interventio
ngrou
pno
significanteffecton
mem
orytask
and
subjectiv
emem
oryability
Erickson
etal.
(2007)
[21]
RCT
2-3weeks
Nofollo
w-up
n=65
Attentionaltraining
Improvem
entindu
altask
perfo
rmance
iscorrelated
with
increasedactiv
ityin
leftventral
prefrontalcortex
anddecreasedactiv
ityin
the
dorsolateralprefrontalcortex
Both
reactio
ntim
eand
accuracy
improved
most
inthed
ualtaskinterventio
ngrou
pYo
ungandoldadultsshow
edthes
amed
egreeo
fperfo
rmance
improvem
entafterintervention.
Brehmer
etal.
(2011)[22]
RCT
5weeks
Nofollo
w-up
n=24
Adaptiv
eworking
mem
orytraining
.Con
trolgroup
:low
levelfi
xedworking
mem
orytraining
Allparticipantsdecreasedbrainactiv
ityParticipantswho
profi
tthe
mostsho
wedthe
largestd
ecreases
ininterventio
nrelated
brain
areasa
ndlargestincreaseincaud
ate
Both
grou
psIm
proved
inspan
boardbackward,
digitspanbackward,PA
SAT,RA
VLT
Nointerventio
nrelated
perfo
rmance
gainsfor
inscannertask
Interventio
ngrou
pshow
edtraining
related
improvem
entinspan
boardbackwardtask
and
PASA
Tcomparedto
controls
Belleville
etal.
(2014)
[23]
RCT
3weeks
Nofollo
w-up
n=46
Attentionaltraining
Bette
rperform
ance
insin
gletasking
correlated
with
decreasedactiv
ityin
right
inferio
rand
middlefrontalgyrus
Inthes
trategiccontrolofatte
ntioncond
ition
,abette
rabilityto
mod
ulatea
ttentionaccordingto
task
instructioncorrela
tedwith
increasedactiv
ityin
Brod
mannarea
10
Allinterventio
ngrou
psim
proved
inreactio
ntim
eandaccuracy
fora
lphanu
merictask,noeffectfor
visualdetectiontask
Both
dualtask
cond
ition
sbetterp
erform
ance
dualtaskingcomparedto
singletaskinterventio
ngrou
pStrategicc
ontro
lofatte
ntioncond
ition
significant
effecto
ftaskinstr
uctio
n.Th
eywerea
bleto
mod
ifyattentionaccordingto
instr
uctio
n.Mild
Cognitiv
eIm
pairm
ent
Claree
tal.(2009)
[31]
Sing
lecase
study
8weeks
Nofollo
w-up
n=1
Goalorie
nted
cogn
itive
interventio
n
Encoding
:increased
activ
ityin
interventio
nrelated
brainareas,decreasedactiv
ityhigh
ervisualareas,andfro
ntalareas
Recogn
ition
:increased
activ
ityin
interventio
nrelated
brainareas,decreasedactiv
ityhigh
ervisualareas,andfro
ntalareas
Bette
rsub
jectivem
emoryperfo
rmance,m
emory
satisfaction

8 BioMed Research International
Table3:Con
tinued.
Stud
y
Design
Duration
Long
-term
follo
w-u
p𝑛
Interventio
nRe
sultneurob
iologicaloutcomes
Resultbehaviou
raloutcomes
Ham
pstead
etal.
(2011)[32]
Multip
lesin
glec
ases
2weeks
Nofollo
w-up
n=6
Face-nam
eassociationlearning
Encoding
:increased
activ
ityin
defaultn
etwork
Effectiv
econ
nectivity
chan
ges:increased
conn
ectiv
ity
Sign
ificant
improvem
entinperfo
rmance
trainedandun
trainedmem
orytask
Belleville
etal.
(2011)[33]
Case
control
6weeks
Nofollo
w-up
n=15
Episo
dicm
emory
training
Encoding
healthye
lderly:decreased
activ
ityin
brainareasrelated
tointerventio
n.En
coding
MCI
:increased
activ
ityin
brainareas
relatedto
interventio
nRe
trievalh
ealth
yelderlyan
dMCI
:increased
activ
itynewbrainareasa
ndaccumulated
activ
ityin
specialized
areasb
othrelated
tointerventio
n.
Both
grou
psim
proved
onam
emorytest
Rosenetal.(2011)
[16]
RCT
2mon
ths
Nofollo
w-up
n=12
Auditory
processin
gtraining
Increasedactiv
ityhipp
ocam
pusininterventio
ngrou
pdecreasedactiv
ityhipp
ocam
pusincontrol
grou
p
Interventio
ngrou
pim
proved
inmem
orytestand
training
tasks
Ham
pstead
etal.
(2012)
[24]
RCT
2weeks
Nofollo
w-up
n=34
Mnemon
ictraining
Encoding
MCI
:increased
activ
ityleft
hipp
ocam
palbod
yRe
trievalM
CI:increased
activ
ityhipp
ocam
pal
body
andtailbilaterally
Health
ycon
trols:decreasedactiv
ityrig
hthipp
ocam
palbod
y
MCI
grou
pandhealthycontrolsim
proved
inencoding
andretrieving
trainedob
jectlocatio
ns.
Nointerventio
neffectfor
untrainedob
ject
locatio
ns.
Dem
entia
Heissetal.(1994)
[25]
RCT
6mon
ths
Nofollo
w-up
n=80
(1)S
ocialsup
port
(2)C
ognitiv
etraining
(3)C
ognitiv
etraining
+pyritinol
(4)C
ognitiv
etraining
+ph
osph
atidylserin
e
EEG:increased
glob
alpo
wer
gr3+4Decreased
delta
power
gr4
PET:
significantcorrelationMMSE
scorea
ndglucosem
etabolism
tempero-parietalcortex.
Gr.4increasedactiv
ityprim
aryvisualcortex
durin
ginterventio
n,bu
tnot
atthee
ndof
the
interventio
n
Gr4
morer
espo
ndersa
ndsig
nificanth
igher
scores
onorientationthan
gr1+
2in
week8+16.
Atthee
ndof
theintervention(6
mon
ths)there
weren
odifferences.
Nagayae
tal.
(2005)
[34]
With
insubjects
Unk
nown
Nofollo
w-up
n=11
Recreatio
nal
rehabilitation
Respon
ders:decreased
activ
ityfro
ntalregion
sNon
respon
ders:decreased
activ
ityallregions
Respon
ders:improved
3MMSE
points
Tanaka
etal.
(2007)
[35]
Sing
lecase
2mon
ths
Follo
w-upfor6
mon
ths
n=1
Reminisc
ence
increasedactiv
ityfro
ntalareas,po
stcingu
late
gyrus,andprecun
eus
Improvem
entincogn
ition
,vita
lity,volition,
and
daily
lifea
ctivities

BioMed Research International 9
Table3:Con
tinued.
Stud
y
Design
Duration
Long
-term
follo
w-u
p𝑛
Interventio
nRe
sultneurob
iologicaloutcomes
Resultbehaviou
raloutcomes
Forstere
tal.(2011)
[27]
RCT
6mon
ths
Nofollo
w-up
n=36
Multip
urpo
se
MCI
controls:
decreasedactiv
ityin
brainregion
stypically
impaire
din
AD
MCI
interventio
n:no
declines
ADcontrols:
decreasedactiv
ityin
brainregion
stypically
impaire
din
AD
ADinterventio
n:decreasedactiv
ityin
2clu
sters;
lingualgyrus,leftinferio
rtem
poralgyrus
Nochanges
Akanu
mae
tal.
(2011)[26]
RCT
3mon
ths
Nofollo
w-up
n=24
Reminisc
ence
with
reality
orientation
Interventio
ngrou
p:increasedactiv
ityanterio
rcing
ulateb
ilateral,leftinferio
rtem
poralcortex.
Correlationbetweenincreasedactanterior
cing
ulatea
ndim
provem
entsocialand
commun
icationscales
brse
Interventio
ngrou
p:im
proved
insocialand
commun
icationscales
(brse)
Spiro
nelli
etal.
(2013)
[36]
Observatio
nalstudy
5weeks
Nofollo
w-up
n=11
Cognitiv
etraining
Thea
mplitu
deso
fthe
recogn
ition
potential
(negativep
otentia
l)weres
ignificantly
increased
ontheleft
sides
ofpo
sterio
rregions
forh
igh
frequ
ency
words
Amarginally
significantimprovem
ento
nthe
verbalreason
ingscore
Nosig
nificanttreatmenteffecton
thed
ementia
screeningtests
,fou
rout
offivec
ognitiv
etasks,
andtheind
ependent
functio
ning
questio
nnaires.
vanPaasschenet
al.(2013)[28]
RCT
8weeks
Nofollo
w-up
n=19
Tailo
redcogn
itive
rehabilitation
Interventio
ngroup
Encoding
:nosig
nificantchanges.
Recogn
ition
:significantincreased
activ
itybilateralprefro
ntalareasa
ndtheb
ilateralinsula
Controlg
roup
Recogn
ition
:decreased
activ
ityin
bilateral
prefrontalareasa
ndtheb
ilateralinsula
Interventio
ngrou
pim
proved
onsatisfactionand
perfo
rmance
ofindividu
algoals(CO
PM)
Notre
atmenteffecton
theinscannerface-name
associationtask
Baglio
etal.(2014)
[29]
RCT
10weeks
Follo
w-upfor2
2weeks𝑛=60,𝑛=30
Follo
w-up
Multid
imensio
nal
stim
ulationprogram
Postinterventio
n:increasedactiv
itybilateral
superio
rtem
poralgyrus
(right>left),right
lentifo
rmnu
cleus,and
thalam
us
Interventio
ngrou
pshow
edclinicalrele
vant
improvem
entinNPI,language,andmem
ory
scales
ofADAS-cog
Nosig
nificantchangeinfunctio
nalstatuso
rph
ysicalwell-b
eing
Long
-term
follo
w-up
:improvem
entinthe
lang
uage
andmem
oryscales
oftheA
DAS-cogis
preserved
Legend
a:qo
l:qu
ality
oflife.
MMSE
:minim
entalstateexam
ination.
ADAScog:dementia
screeningtest.
BRSE
:scaleforsocialand
commun
icationskills.
GDS:geria
tricdepressio
nscale.

10 BioMed Research International
In conclusion, mostly an increase in brain activationspecifically in areas typically involved in intervention relatedcognitive processes [16, 24, 31, 33] was seen, as well asactivation of the default network [24, 32]. In several studies,the authors claimed that normalisation of the pattern of brainactivation after intervention had occurred as a possible resultof restoration [24, 31–33] whereas the activation of additionalareas was interpreted as a compensatory mechanism [24, 32].
Most of the studies tried to relate the changes in brainactivation to intervention success.Most studies formulate thisintervention success as performance improvement on a cog-nitive task that was the target of the intervention. One singlecase study also studied subjective complaints of cognition,mood, and anxiety. These authors reported improvement insubjectivemeasures ofmemory performance and satisfaction[31].
3.3. Patients with Dementia
3.3.1. Study Characteristics. Eight studies [25–29, 34–36]focused on patients with dementia. Four of the studies useda RCT design [25–27, 29]. Study population, interventiontargets, and outcome measures differed.
The most recent RCT study [29] aimed to improvecognition, behaviour, andmotor functioning with an intense,multidimensional stimulation program. The effectivenessof this program was studied in 60 persons with AD ona questionnaire for behavioural and psychiatric problems(NPI), language, and memory scales of the Alzheimer’s Dis-easeAssessment Scale-Cognitive subscale (ADAS-cog), func-tional status, physical well-being, and fMRI.The interventiongroupwas compared to awaiting list. Twenty healthy controlsserved as a reference for the typical activation pattern whileperforming the in-scanner verbal fluency task. The strengthof this study was a long-term follow-up measurement [29].
In another RCT study [27] the effect of a six-monthcognitive intervention program designed to improve globalcognitive functioning, mood, and quality of life in patientswith MCI and mild AD was investigated. To study disease-related brain activation differences at baseline, PET dataof the MCI and AD group were compared with PET dataof a group of eleven healthy elderly. In the active controlcondition, participants made pencil and paper assignmentsfocused on sustained attention (mostly intact in MCI andAD). A specific PET method was used that is known tobe more sensitive in detecting disease related metabolicdisturbances inmild tomoderate stages of neurodegenerativediseases [27].
The RCT study of Heiss et al. [25] also used a six-monthintervention for 80 participants with AD. The content oftheir intervention was different. The 17 participants receivedsocial support (group 1), 18 participants received cognitivetraining twice a week (group 2), 18 participants received acombination of the cognitive training and the drug pyritinolthat is used for symptomatic treatment of AD (group 3),and finally 18 participants received cognitive training andthe dietary supplement phosphatidylserine. At baseline andat several times during intervention and postintervention
neuropsychological tasks, the quantitative EEG, resting statePET, and stimulation PET were administered [25].
The fourth RCT study [26] investigated 24 residents of ageriatric nursing home with a diagnosis of vascular dementia(VaD). They were randomly assigned to reminiscence withreality approach condition or were treated to the standard ofcare.Theduration of the interventionwas 3months. Reminis-cence with reality approach claimed to invokememories withthe aid of materials and generated a better awareness of the“here and now.” Scores on a cognitive screening test (MMSE),a mood questionnaire (GDS), a behavioural observationalquestionnaire (BRSE), and PET data were all collected. Aregion of interest analysis (anterior cingulate left and right)was conducted with the PET data. [26].
The efficacy of tailored cognitive rehabilitation in 19people with early stage AD or mixed AD/VaD was evaluatedby van Paasschen et al. [28]. The goal of this study wasto relate clinically relevant improvement and differences inbrain activity. A passive control group with no treatment aswell as an active control group with relaxation therapy wasused. In 8 weekly sessions, personalized goals concerningmemory were targeted in the cognitive rehabilitation. Themain outcome measure was the Canadian OccupationalPerformanceMeasure (COPM) that rated the satisfaction andperformance of participants on several goals with respect todaily living. Brain activity was studied with fMRI [28].
Whereas most studies selected fMRI to study brainactivation, Spironelli et al. [36] used Event Related Potentials(ERP) to evaluate possible changes in brain functioning aftercognitive training in 11 people with mild to moderate AD.Their intervention aimed to stimulate different cognitivedomains based on everyday activities and exercises. The 11matched healthy controls underwent one experimental ERPsession to serve as a reference for possible altered responsepatterns. The intervention success was also evaluated withneuropsychological tests and questionnaires of everydayactivities [36].
Two studies used PET data as the neurobiological out-come. One study was a single case design on the effect ofeight weekly reminiscence sessions on activities of daily liv-ing, cognition, volition, vitality, behavioural problems, well-being, caregiver burden, and PET data. A comprehensivegeriatric assessment was also administered six months afterintervention [35]. The other study provided 11 VaD patientswith recreational rehabilitation. They used PET to studyblood flow differences after intervention. The group of 11patients was divided into responders (improved more than3 points on the MMSE) and nonresponders [34].
3.3.2. Findings. The eight studies that investigated cognitiveintervention effects on brain functioning of people sufferingfrom dementia differed in design, type of intervention,duration of the intervention, type of neurobiological andbehavioural outcomes, and the presence of follow-up mea-sures (Table 3). Despite those differences, all studies foundneurobiological changes after intervention.
In the most recent RCT study, an increased activity inthe superior temporal gyrus bilaterally, the thalamus and the

BioMed Research International 11
right lentiform nucleus was seen after a multidimensionalstimulation program. The intervention group also showedclinical relevant improvement in neuropsychiatric symptoms,language, and memory scales of a cognitive screening.There is a significant correlation between the magnitudeof increased activity in the left superior temporal gyrus,precuneus and left thalamus, and the change in cognitivescreening performance. The improvement in these scalesof the cognitive screening is preserved at 22 weeks afteintervention [29].
Another multidimensional intervention found evidencethat participants with AD showed decreased activity in twoclusters (lingual gyrus, left inferior temporal gyrus), whereasthe active control group showed decreased activity in a largernetwork prefrontal, parieto-occipital and parieto-temporal.However, therewere no significant changes in the behaviouraloutcomes [27].
Another RCT study showed that tailored cognitive reha-bilitation induced increased activity in prefrontal areas andinsula bilaterally, whereas both active and waiting list controlgroups showed decreased activity in those areas. The inter-vention group improved on satisfaction and performance ofindividual goals; both control groups showed no improve-ment [28].
A RCT study that evaluated the effect of reminiscencewith reality orientation found that intervention relatedincreased activity in the anterior cingulate correlated signifi-cantly with improvement in social and communication scales[26].
A single case study on the effect of reminiscence reportedincreased activity in frontal areas, precuneus and poste-rior cingulate gyrus after intervention. The participant alsoimproved on measures of cognition, vitality, volition, anddaily life activities [35].
In a RCT study hat evaluated the effect of four dif-ferent interventions, global EEG power increased in bothintervention groups that combined cognitive training witha dietary supplement or a symptomatic drug for dementia.There were no significant changes in brain metabolism afterintervention in predetermined target regions. Additionalregions of interest were analysed; this revealed an increase inmetabolism in the visual association area during functionalactivation for the cognitive training and phosphatidylserinegroup. For this intervention group there was also an increasein resting state metabolism in temporal regions, but only forthe participants in this particular intervention group thathad initial metabolism values below 90% of normal in thetemporal region. There were also some behavioural benefitsfor this intervention group. In weeks 8 and 16, the group thatreceived cognitive training and phosphatidylserine scoredsignificantly better on orientation than the other interventiongroups. This effect was no longer present at the end of theintervention [25].
An increased amplitude of the recognition potential forhigh frequency words on the left sides of posterior regionsafter cognitive training was demonstrated in an ERP study.Most behavioural outcomes fail to show a significant inter-vention effect, despite a marginally significant improvementon verbal reasoning [36].
Responders of a recreational rehabilitation interventionshowed decreased activity in frontal areas after intervention.The nonresponders showed activity decreases in a largenetwork of brain areas after intervention [34].
Thus, most studies found an increase in brain activationafter intervention or less decrease in activation versus thecontrol group.One study reported that the responders in theirintervention showed a significant decrease in cerebral bloodflow in the frontal regions, whereas nonresponders showeda decrease in a larger network of brain areas. Their study,however, is the least quality of all the included studies [34].According to one study [25], the changes in neuropsycho-logical measurements and brain activity were temporary anddisappeared at the end of the six-month intervention. Twostudies however demonstrated a behavioural interventionsuccess of 22 weeks and six months after intervention.Both studies did not follow up with the neurobiologicalchanges [29, 35]. The three most recent studies [28, 29, 36]and the study of Tanaka and colleagues [35] tried to linkclinical improvement to changes in brain activation by usingbehavioural outcomes that were not only cognitive tasks butmore related to daily functioning, individual goals, subjectivecomplaints, or social skills. Baglio and colleagues took thisone step further to statistically relate the brain activationchanges to the behavioural outcomes [29].
3.4. Methodological Quality. The selected 19 studies werequite heterogeneous in terms of design, sample size, popu-lation, intervention methods, and neurobiological outcomemeasurements. Therefore, it was decided to not statisticallypool the data to perform a quantitative meta-analysis. Eightstudies were comprised of patients with a diagnosis ofdementia; five studies involved patients with Mild CognitiveImpairment; and six studies included healthy elderly. Of theselected studies there were 13 randomized controlled trials,3 prospective studies, 1 study using a within-subjects design,and 2 single case studies.
Theoverallmethodological quality of the included studiesvaried. For the RCTs, the overall score of the methodologicalquality varied from 3 to 9 (maximum 9) with a level ofevidence ranging from A2 to B according to the CBO(Table 1). The overall score for the methodological quality ofthe observational studies varied from 3 to 9 (maximum 9).The CBO level of evidence ranged from B to C (Table 2).
Six of the 13 RCT studies lacked an intention to treatanalysis. Randomization was blind in only six of the 13 RCTstudies. In more than half of the studies the outcome assessorwas not blind to the treatment condition. In the observationalstudies, almost none of the studies had blinded outcomeassessors and almost every study had a selection bias.
A hierarchy of quality was composed based on the designand methodology. With regard to the studies that focusedon healthy elderly, the study of Belleville et al. [23] had thehighest methodological quality. For the studies that comprisepatients with MCI, the studies of Belleville and Bherer [15]and Erickson et al. [21] had the highest methodologicalquality. The study with the highest methodological qualitythat involved patients with dementia was that of Baglio et al.

12 BioMed Research International
[29]. Akanuma et al. [26] was limited in the informative valuedue to a lack of detailed methods and results.
4. Discussion
In this paper, the literature was reviewed to investigatewhether cognitive interventions in elderly lead to changesin brain activation suggestive of neural plasticity even indamaged neural systems. The methodological quality ofthe 19 studies was rated according to the guidelines ofthe Dutch Institute for Health Care Improvement (CBO,http://www.cbo.nl/).
The results illustrate that all studies, conducted in diversepopulations from healthy elderly to patients with dementia,show changes in brain activation post intervention. Themethodological quality of the studies varied with the CBOlevel of evidence ranging from A2 to C (Tables 1 and 2).
All four studies in healthy elderly found brain activationdifferences after intervention. Two studies found increases inbrain activation post intervention, primarily in the occipitalparietal cortex and retrosplenial cortex [30] as well as inthe hippocampus [18]. Post hoc only the older participantsthat improved on a memory test showed these brain activityincreases [30]. However, this could not be documented bymore clinical outcomes due to a lack of such outcomes or afail to link brain activation changes to clinically meaningfulimprovement.
On the contrary, another study found a decrease afterintervention in the dorsolateral brain activity [20]. Therelationship between this decreased activity dorsolateral andclinically relevant improvement was not evident. Only animprovement in verbal fluency was found, but no sig-nificant intervention effects were found on the subjectivemeasurements of self-awareness of memory performanceand other cognitive tasks [20]. Three studies successfullylinked intervention-related performance gains to brain acti-vation changes by statistical analyses. One study foundperformance-related brain activity decreases in the corticalregions known to be involved in cognitive functions tar-geted by the intervention and performance related brainactivity increases in subcortical areas [22]. Another studyprovided evidence that training induced dual task perfor-mance improvement was related to increased activity inthe left ventral prefrontal cortex and decreased activity inthe dorsolateral prefrontal cortex. Compared with an adultsample, age related differences in brain activity were reducedafter intervention [21]. The study of Belleville and colleagues[23] concluded that the type of intervention influenced theloci and type of brain activity. A better performance insingle tasking was correlated with decreased activity in theright inferior and middle frontal gyrus. An improved abilityto modulate attention according to task instruction wascorrelated with a greater activity in Brodmann area 10 [23].
Two studies argued that the decreases in brain activitycould be explained by an increased cognitive efficiency, thusdemanding less effort [20, 22]. The increase in subcorticalbrain activity was, according to these authors, evidence thatthe performance was becoming less executively demanding
andmore proceduralized as the training proceeded [22].Thisis in line with the theory of Bartres-Faz and Arenaza-Urquijoon cognitive efficiency [19]. In addition, the study with thehighest methodological quality highlighted the importanceof the type of intervention format. Intervention format haseffect on the loci and type of brain activation changes afterintervention. They refer to the framework of Lorden andtheir own theoretical framework named INTERACTIVE[21]. These models state that repeated practice would leadto decreased activity in the brain areas involved in the task,indicating increased cognitive efficiency. Interventions thataim to learn participants new strategies will lead to increasedactivity in alternative networks involved in learning thosestrategies [21].
Another study interpreted the performance related brainactivity pattern of increased activity in the left ventralprefrontal cortex and decreased activity in the dorsolateralprefrontal cortex, as evidence conflicting with views of com-pensation related reduced brain activity asymmetry. Whilebrain activity differences between adults and older adultswere significantly reduced after training, they interpreted thisas evidence that cognitive training can modulate age relatedpatterns of brain activity [23].
All of the reviewed studies of cognitive interventions inMCI patients found neurobiological changes in brain acti-vation after intervention despite differences in methodology.There was mostly an increase in brain activation, in areastypically involved in intervention related cognitive processes.This was seen as well as activation of the default network.In several studies, even normalisation of the pattern ofbrain activation after intervention was claimed. The studyof Rosen et al. had the highest methodological quality inthis review and showed that even brain structures known tobe injured in patients with MCI such as the hippocampusretained sufficient brain plasticity to benefit from cognitiveinterventions [16]. This activation of the default networkand hippocampus is in line with Bartres’ assumption that,in pathological aging, the cognitive reserve enhances therecruitment of compensating brain networks particularlythe frontal areas, hippocampus, and the precentral gyrus[19]. Cognitive behavioural interventions might increasethis cognitive reserve [4, 8]. Functionally relevant clinicalimprovement has been given little attention in these studies.A statistical approach to the relationship between interven-tion success on behavioural measures and brain activationchanges was only made by one study [26]. Long-term follow-up measures to determine the stability of the interventionsuccess were not included.
Studies in dementia patients also found neurobiologicalchanges after intervention. Most of the studies found anincrease in brain activation or a diminished decrease inactivation after intervention. The study of Forster et al. [27]was the only one that found a decrease in activation postintervention, but the construct of this study has poormethod-ology with little detailed information about the methodsand results. According to one study that used a six-monthintervention, the increased brain activity and improvementon neuropsychological tests were temporary in persons with

BioMed Research International 13
AD and then disappear over time [35]. Other studies demon-strated a preserved improvement in the clinical outcomessuch as cognitive tasks, daily life activities, and vitality at22 weeks and six months after intervention. However, theydid not follow up the neurobiological outcomes [26, 32].Thus, it remained unclear if the changes in brain functioningwere temporary. The study with the highest methodologicalquality correlated improvement in social and communicationscales with increased activity in the anterior cingulate, an areaknown to be involved in social behaviour [26].
One study excluded [27]; all of the authors interpretedtheir findings as evidence for brain plasticity. Some evenstated that cognitive interventions activate compensatingbrain networks in pathological ageing and could possiblyrestore brain activation. However, the stability of this effectremains unclear.
Overall, these results suggest that cognitive interventionslead to neurobiological changes even in potentially damagedneural systems. However, the interpretation of changes inactivation patterns is complicated. For instance, a decrease inbrain activation can indicate increased cognitive efficiency assuggested in the cognitive reserve hypotheses of Bartres-Fazand Arenaza-Urquijo [19] and the learning phases model ofDoyon in Lustig et al. [37]. On the other hand, a decrease inbrain activation might reflect exhaustion of neural resourcesaccompanied by a decline in clinical performance as sug-gested by the CRUNCHmodel [37].
Moreover, the type of intervention would influence theloci and type of activation changes after intervention [21].
The complexity of interpreting these neurobiological dataunderlines the importance of including clinical measure-ments to gain insight into the clinical relevance of neu-robiological changes. Unfortunately, in several studies, thisinformation is lacking or neurobiological data is interpretedas evidence for plasticity/restoration of function in theabsence of a demonstrated intervention success on clinicaloutcomes. In the more recent studies, there is increasedattention for the clinical relevance of neurobiological changeswith promising results. In five studies [21–23, 26, 32] per-formance gains were linked to brain activation. Four studiesused correlations to correlate improvement on a dementiascreening test [22], social and communication scales [26]and changes in performance on different attentional tasks[21, 23] to relevant changes in brain activation. A fourth studyused the maximum gain score on working memory tasks as acovariate in statistical analysis [32].
These studies focus on relating performance improve-ment to brain activity changes. However, the transfer of theseperformance gains to untrained tasks and more importantlyto daily life functioning is a great issue [21].
The heterogeneity in populations, outcome measuresand interventions as well as the small sample sizes andrelatively large amount of case studies further complicate thecomparability of the findings between studies.
We recommend that future studies should include mea-sures of clinically meaningful improvement as well as long-term follow-up data to evaluate the stability of the effects.Theinfluence of task demands, premorbid cognitive reserve, andlearning phases on brain activation should be considered to
increase comparability between studies. The results thus farindicate that the elderly show changes in brain activation aftercognitive interventions. However, the exact interpretationand stability of these changes remain unclear just like towhat extent cognitive interventions are effective to reach theultimate goal: to delay conversion to or prevent progressionof dementia.
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper.
References
[1] Y. Stern, “What is cognitive reserve? Theory and researchapplication of the reserve concept,” Journal of the InternationalNeuropsychological Society, vol. 8, no. 3, pp. 448–460, 2002.
[2] N. Raz, “Aging of the brain and its impact on cognitiveperformance: integration of structural and functional findings,”in The Handbook of Aging and Cognition, F. I. M. Craik and T.A. Salthouse, Eds., Lawrence Erlbaum Associates, Mahwah, NJ,USA, 2000.
[3] E. M. Hoogenhout, R. H. M. de Groot, and J. Jolles, “A newcomprehensive educational group program for older adultswith cognitive complaints: background, content, and processevaluation,” Educational Gerontology, vol. 37, no. 1, pp. 51–73,2011.
[4] E. M. Hoogenhout, R. H. M. de Groot, W. van der Elst,and J. Jolles, “Effects of a comprehensive educational groupintervention in older women with cognitive complaints: arandomized controlled trial,”Aging&Mental Health, vol. 16, no.2, pp. 135–144, 2012.
[5] N. L. Hill, A. M. Kolanowski, and D. J. Gill, “Plasticity in earlyalzheimer disease: an apportunity for intervention,” Topics inGeriatric Rehabilitation, vol. 27, no. 4, pp. 257–267, 2011.
[6] M. E. M. Mol, M. P. J. van Boxtel, D. Willems, F. R. J. Verhey,and J. Jolles, “Subjective forgetfulness is associated with lowerquality of life in middle-aged and young-old individuals: a 9-year follow-up in older participants from the Maastricht AgingStudy,” Aging and Mental Health, vol. 13, no. 5, pp. 699–705,2009.
[7] A. Bahar-Fuchs, L. Clare, and B. Woods, “Cognitive trainingand cognitive rehabilitation for mild to moderate Alzheimer’sdisease and vascular dementia,” The Cochrane Database ofSystematic Reviews, vol. 6, Article ID CD003260, 2013.
[8] V. Buschert, A. L. W. Bokde, and H. Hampel, “Cognitiveintervention in Alzheimer disease,” Nature Reviews Neurology,vol. 6, no. 9, pp. 508–517, 2010.
[9] B. Woods, E. Aguirre, A. E. Spector, and M. Orrell, “Cognitivestimulation to improve cognitive functioning in people withdementia,”The Cochrane Database of Systematic Reviews, no. 2,Article ID CD005562, 2012.
[10] D. E. J. Linden, “How psychotherapy changes the brain—thecontribution of functional neuroimaging,” Molecular Psychia-try, vol. 11, no. 6, pp. 528–538, 2006.
[11] H. Li, J. Li, N. Li, B. Li, P. Wang, and T. Zhou, “Cognitiveintervention for persons with mild cognitive impairment: ameta-analysis,” Ageing Research Reviews, vol. 10, no. 2, pp. 285–296, 2011.

14 BioMed Research International
[12] S. A. H. van Hooren, S. A. M. Valentijn, H. Bosma et al., “Effectof a structured course involving goal management training inolder adults: a randomised controlled trial,” Patient Educationand Counseling, vol. 65, no. 2, pp. 205–213, 2007.
[13] S. A. M. Valentijn, S. A. H. Van Hooren, H. Bosma et al.,“The effect of two types of memory training on subjectiveand objective memory performance in healthy individuals aged55 years and older: a randomized controlled trial,” PatientEducation and Counseling, vol. 57, no. 1, pp. 106–114, 2005.
[14] Y. Kondo, M. Suzuki, S. Mugikura et al., “Changes in brain acti-vation associated with use of a memory strategy: a functionalMRI study,” NeuroImage, vol. 24, no. 4, pp. 1154–1163, 2005.
[15] S. Belleville and L. Bherer, “Biomarkers of cognitive trainingeffects in aging,” Current Translational Geriatrics and Experi-mental Gerontology Reports, vol. 1, no. 2, pp. 104–110, 2012.
[16] A. C. Rosen, L. Sugiura, J. H. Kramer, S. Whitfield-Gabrieli,and J. D. Gabrieli, “Cognitive training changes hippocampalfunction in mild cognitive impairment: a pilot study,” Journalof Alzheimer’s Disease, vol. 26, no. 3, pp. 349–357, 2011.
[17] J. J. Palop, J. Chin, and L. Mucke, “A network dysfunctionperspective on neurodegenerative diseases,” Nature, vol. 443,no. 7113, pp. 768–773, 2006.
[18] M. J. Valenzuela, M. Jones, W. Wen et al., “Memory trainingalters hippocampal neurochemistry in healthy elderly,” Neu-roReport, vol. 14, no. 10, pp. 1333–1337, 2003.
[19] D. Bartres-Faz and E. M. Arenaza-Urquijo, “Structural andfunctional imaging correlates of cognitive and brain reservehypotheses in healthy and pathological aging,” Brain Topogra-phy, vol. 24, no. 3-4, pp. 340–357, 2011.
[20] G.W. Small, D.H. S. Silverman, P. Siddarth et al., “Effects of a 14-day healthy longevity lifestyle program on cognition and brainfunction,” American Journal of Geriatric Psychiatry, vol. 14, no.6, pp. 538–545, 2006.
[21] K. I. Erickson, S. J. Colcombe, R. Wadhwa et al., “Training-induced plasticity in older adults: effects of training on hemi-spheric asymmetry,” Neurobiology of Aging, vol. 28, no. 2, pp.272–283, 2007.
[22] Y. Brehmer, A. Rieckmann, M. Bellander, H. Westerberg, H.Fischer, and L. Backman, “Neural correlates of training-relatedworking-memory gains in old age,” NeuroImage, vol. 58, no. 4,pp. 1110–1120, 2011.
[23] S. Belleville, S. Mellah, C. de Boysson, J. Demonet, B. Bier,and L. Chao, “The pattern and loci of training-induced brainchanges in healthy older adults are predicted by the nature ofthe intervention,” PLoS ONE, vol. 9, no. 8, Article ID e102710,2014.
[24] B. M. Hampstead, A. Y. Stringer, R. F. Stilla, M. Giddens, andK. Sathian, “Mnemonic strategy training partially restores hip-pocampal activity in patients with mild cognitive impairment,”Hippocampus, vol. 22, no. 8, pp. 1652–1658, 2012.
[25] W.-D. Heiss, J. Kessler, R. Mielke, B. Szelies, and K. Herholz,“Long-term effects of phosphatidylserine, pyritinol, and cog-nitive training in Alzheimer’s disease. A neuropsychological,EEG, and PET investigation,”Dementia, vol. 5, no. 2, pp. 88–98,1994.
[26] K. Akanuma, K. Meguro, M. Meguro et al., “Improved socialinteraction and increased anterior cingulate metabolism aftergroup reminiscencewith reality orientation approach for vascu-lar dementia,” Psychiatry Research: Neuroimaging, vol. 192, no. 3,pp. 183–187, 2011.
[27] S. Forster, V. C. Buschert, H.-G. Buchholz et al., “Effects of a6-month cognitive intervention program on brain metabolism
in amnestic mild cognitive impairment and mild Alzheimer’sdisease,” Journal of Alzheimer’s Disease, vol. 25, no. 4, pp. 695–706, 2011.
[28] J. van Paasschen, L. Clare, K. S. L. Yuen et al., “Cognitiverehabilitation changes memory-related brain activity in peoplewith Alzheimer disease,”Neurorehabilitation andNeural Repair,vol. 27, no. 5, pp. 448–459, 2013.
[29] F. Baglio, L. Griffanti, F. L. Saibene et al., “Multistimulationgroup therapy in Alzheimer’s disease promotes changes in brainfunctioning,”Neurorehabilitation and Neural Repair, vol. 29, no.1, pp. 13–24, 2014.
[30] L. Nyberg, J. Sandblom, S. Jones et al., “Neural correlatesof training-related memory improvement in adulthood andaging,” Proceedings of the National Academy of Sciences of theUnited States of America, vol. 100, no. 23, pp. 13728–13733, 2003.
[31] L. Clare, J. van Paasschen, S. J. Evans, C. Parkinson, R. T.Woods,and D. E. J. Linden, “Goal-oriented cognitive rehabilitation foran individual with Mild Cognitive Impairment: behaviouraland neuroimaging outcomes,” Neurocase: The Neural Basis ofCognition, vol. 15, no. 4, pp. 318–331, 2009.
[32] B. M. Hampstead, A. Y. Stringer, R. F. Stilla et al., “Activationand effective connectivity changes following explicit-memorytraining for face-name pairs in patients with mild cognitiveimpairment: a pilot study,” Neurorehabilitation and NeuralRepair, vol. 25, no. 3, pp. 210–222, 2011.
[33] S. Belleville, F. Clement, S.Mellah, B. Gilbert, F. Fontaine, and S.Gauthier, “Training-related brain plasticity in subjects at risk ofdeveloping Alzheimer’s disease,” Brain, vol. 134, no. 6, pp. 1623–1634, 2011.
[34] M. Nagaya, H. Endo, T. Kachi, Y. Abe, and T. Ota, “Recreationalrehabilitation improved cognitive function in vascular demen-tia,” Journal of the American Geriatrics Society, vol. 53, no. 5, pp.911–912, 2005.
[35] K. Tanaka, Y. Yamada, Y. Kobayashi et al., “Improved cognitivefunction, mood and brain blood flow in single photon emissioncomputed tomography following individual reminiscence ther-apy in an elderly patient with Alzheimer’s disease,” Geriatrics &Gerontology International, vol. 7, no. 3, pp. 305–309, 2007.
[36] C. Spironelli, S. Bergamaschi, S. Mondini, D. Villani, and A.Angrilli, “Functional plasticity in Alzheimer’s disease: effectof cognitive training on language-related ERP components,”Neuropsychologia, vol. 51, no. 8, pp. 1638–1648, 2013.
[37] C. Lustig, P. Shah, R. Seidler, and P. A. Lustig-Lorenz, “Aging,training, and the brain: a review and future directions,” Neu-ropsychology Review, vol. 19, no. 4, pp. 504–522, 2009.

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com