Embed Size (px)
Citation preview

1
REVERSING FATTY LIVER DISEASE
WITH HEALTHY LIFESTYLE
2021
Authors: Massimiliano Ruscica, Paola Dongiovanni, Leen Heyens, Geert Robaeys

Affiliations of the authors:
Massimiliano Ruscica1
Paola Dongiovanni2
Leen Heyens3-5
Geert Robaeys3,5,6
1 Università degli studi di Milano, Department of Pharmacological and Biomolecular Sciences, Milan, Italy 2 General Medicine and Metabolic Diseases, Fondazione IRCCS Ca' Granda Ospedale Maggiore Policlinico,
Milan, Italy 3 Hasselt University, Faculty of Health and Life Sciences, Diepenbeek, Belgium
4 Maastricht University, School of Nutrition and Translational Research in Metabolism, NUTRIM, Maastricht, the
Netherlands 5 Ziekenhuis Oost-Limburg, Department of Gastro-enterology and Hepatology, Genk, Belgium
6 University Hospital KU Leuven, Department of Gastroenterology and Hepatology, Leuven, Belgium
Editor:
Stephanie De Vriese7
7 Secretary of Alpro Foundation
This review is fully supported by the Scientific Advisory Committee of the Alpro Foundation:
Harry Aiking (VU University Amsterdam); Anna Arnoldi (University Milano);
Peter Clarys (Vrije Universiteit Brussel); Christine Debeuf (Alpro); Stephanie De Vriese (Alpro);
Helmut Heseker (University Paderborn); Sander Kersten (University Wageningen);
Ian Rowland (University Reading); Cesare Sirtori (University Milano);
and Kurt Widhalm (University Vienna)
Date: June 2021

CONTENT
Introduction .............................................................................................................................................................................. 4
Genetic and environmental factors associated with NAFLD ......................................................................................... 6
Primary therapeutic advice: lifestyle changes emphasizing weight reduction........................................................ 7
Mediterranean diet ............................................................................................................................................................................... 9
Role of plant protein .......................................................................................................................................................................... 10
The role of gut microbiome .............................................................................................................................................................. 11
Other treatment options ..................................................................................................................................................................... 11
NAFLD and childhood ........................................................................................................................................................... 12
Conclusion ............................................................................................................................................................................... 12
References ............................................................................................................................................................................... 13

4
INTRODUCTION
Non-alcoholic fatty liver disease (NAFLD) is considered the most frequent cause of liver disorders with a prevalence above 30% in many adult populations.1,2 The highest prevalence is
reported in the Middle East (32%) and South
America (31%), followed by Asia (27%), USA (24%)
and Europe (23%), with the lowest in Africa (14%).
Because of its close association with metabolic
syndrome (MetS), NAFLD is seen in 47.3–63.7% of
people with type 2 diabetes (T2DM) and up to 80%
of people with obesity. However, some people
with a healthy body mass index (BMI) can still
develop NAFLD, often described as non-obese or
lean NAFLD. These patients usually have central
obesity or other metabolic risk factors.3 Patients
with NAFLD have 2.5 times higher incidence of
cardiovascular disease (CVD).
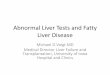
F IG UR E 1 . THE NA TU RA L EV OLUT ION OF NA F LD OR ME TABO LIC A SSOCIA TED FAT T Y L IV ER D IS EAS E (M AF LD) .
The mechanisms underlying NAFLD pathogenesis are multifactorial. Histologically, NAFLD encompasses a continuum including steatosis
with or without mild inflammation (NAFL), NASH with/without fibrosis, cirrhosis, and hepatocellular carcinoma. Equally, environment, gut
microbiota, genetics, and epigenetics influence the disease onset and progression. The first step in NAFLD development is hepatic fat
infiltration, mainly due to IR. This leads to a rise in the adipose tissue lipolysis with the consequent efflux of free fatty acids to the liver. The
compensatory hyperinsulinemia exacerbates fat accumulation. Excess fat is cleared from the liver by an enhanced lipoprotein secretion
and mitochondrial β-oxidation. The latter results in increased reactive oxygen species production leading to the activation of inflammatory
pathways.
Abbreviations: IR, insulin resistance; MAFLD, metabolic associated fatty liver disease; NAFL, non-alcoholic fatty liver; NAFLD, non-alcoholic
fatty liver disease; NASH, non-alcoholic steatohepatitis.
Adapted from: Dongiovanni P et al. 2021 and Heyens LJM et al. 2021. 68,69

5
As proposed by Shaffner and Thaler in 1986, NAFLD4 is an "umbrella" definition encompassing a spectrum of histological liver changes, namely
steatosis (affecting at least 5% of hepatocytes), non-
alcoholic steatohepatitis (NASH) with/without
fibrosis, cirrhosis, and hepatocellular carcinoma
(figure 1).5 About 20% of patients with NAFLD will
develop NASH in three to seven years6, which is
considered the potentially progressive form of the
disease.7 About 9 to 25% of individuals with NASH
develop cirrhosis over a 10 to 20 year period.8 The
imbalance between hepatic synthesis and uptake
of fatty acids and their oxidation and efflux plays a
key role in the pathogenesis of NAFLD, mainly due
to a condition of insulin resistance (IR) associated
with obesity or diabetes.9
The term NAFLD was first described in 198010 as a
condition of ‘exclusion’ since it exists only in the
absence of other liver diseases, e.g., viral hepatitis B
and hepatitis C, alcohol intake or autoimmune
disease. Furthermore, the current threshold on
alcohol intake (2 drinks for women and 3 for men or
20g/day – 30g/day) has been a constant topic of
debate.11-13 The term NAFLD could also represent an
element of confusion since the use of words such
as “non” and “alcoholic” is disliked by patients
leading to a fear of stigma.14
Consequently, the diagnosis of the disease should
thus be based on the presence of metabolic
dysfunction, not the absence of other conditions.15
Therefore, in 2020 a milestone decision was
reached by an international panel of experts, that
recommended a name change to “metabolic associated fatty liver disease (MAFLD)”.
To meet the diagnosis of MAFLD in adults, patients require the presence of hepatic steatosis as assessed
by either imaging or blood markers/scores indicative of fat accumulation or histology.
This feature must be accompanied by one of the following phenotypes:
• overweight or obesity (BMI ≥ 25 Kg/m2 in Caucasians and ≥ 23 Kg/m2 in Asians) • diagnosis of T2DM • lean or normal weight with signs of metabolic dysregulation 15,16
If you view this diagnosis in terms of concrete metabolic risk biomarkers, at least two or more of the
following conditions must be present:
• enlarged waist circumference (≥ 102/88 cm in Caucasian men and women)
• raised blood pressure (BP, ≥ 130/85 mmHg) or specific drug treatment
• raised triglycerides (TG, ≥ 150 mg/dL) or specific drug treatment
• low high-density lipoprotein (HDL) cholesterol (< 40 mg/dL for men and < 50 mg/dL for
women) or specific drug treatment
• prediabetes (as assessed by fasting plasma glucose levels, 2-hour post-load glucose levels or
haemoglobin A1c (HbA1c))
• homeostatic model assessment of insulin resistance (HOMA-IR) score ≥ 2.5
• inflammation with raised levels of high-sensitivity C-reactive protein (hs-CRP, > 2 mg/L)

6
In spite of the mounting interest in the MAFLD
definition, words of caution have also been
expressed by a distinguished group of US experts
on the possible consequences of a premature
change in NAFLD terminology.17 Further research is
required to better understand the risk of disease
progression among “lean” NAFLD individuals
without any metabolic dysregulation. Hence, we
will focus on NAFLD in this expert opinion.
GENETIC AND ENVIRONMENTAL FACTORS ASSOCIATED WITH NAFLD The development of NAFLD is strongly linked to obesity and IR. However not all obese individuals
nor patients with diabetes develop NAFLD and vice
versa. NAFLD can occur in normal-weight
individuals with normal glucose and lipid levels.18
Thus, there are clearly multiple genetic and
environmental factors determining NAFLD
development and progression (figure 2).
The genetic associations with NAFLD severity are
beyond the scope of this expert opinion. Yet,
genetic predisposition must be placed in the
context of dietary habits and physical activity
which play an important role in the development of
NAFLD.
NAFLD's leading cause has been defined as a multi-factorial behavioural phenotype that consists of sedentary behaviour and poor diet.19
Excess food intake and lack of exercise contribute
to the development/progression of NAFLD via
overweight and obesity and the induction of
specific inflammatory pathways.20 High intake of
low-nutrient, high-sodium and high-fat foods, and
overnutrition appear to contribute to chronic low-
grade inflammation.20-22 Moreover, diet can also
negatively affect the immune system and the gut
microbiota.23 The high salt content present in a
typical Western diet can induce interleukin 17 (IL-17)
producing T-helper cells and inflammation. Low
intakes of polyunsaturated fatty acid (PUFA) and
high intakes of saturated fat and cholesterol were
also shown to be associated with NAFLD. Fatty acids
directly affect immune cells by activating toll-like
receptors and cytokine cascades and influencing
intestinal permeability.20,24 Dietary consumption of
phosphatidylcholine and L-carnitine has been
associated with the generation of specific
metabolites and future CVD events.25 Not only
excessive calorie consumption, but also how food
consumption is distributed throughout the day,
affects fat accumulation in the liver.19 High
carbohydrate intake, especially in soft drink
beverages, is associated with alterations in the gut
microbiota, increased intestinal permeability, and
lipid peroxidation thereby promoting fatty liver
disease.19,21

7
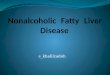
F IG UR E 2 . E FF ECT OF ENV IR ONMENTA L AND GENETIC F ACTORS ON NAFLD DEV ELO PMENT AND PROGR ESS ION, D IREC TL Y AND IND IR ECTL Y V IA COMORB IDI T IES .
Solid lines show how comorbidities (obesity, IR, hyperlipidaemia and inflammation) affect the development and progression of NAFLD,
together with environmental and genetic factors. Dashed lines indicate how environmental and genetic factors affect the development of
comorbidities.
Abbreviations: NAFLD, non-alcoholic fatty liver disease.
Adapted from: Moore JB, 2010.18
PRIMARY THERAPEUTIC ADVICE: LIFESTYLE CHANGES EMPHASIZING WEIGHT REDUCTION
To date, the primary therapeutic advice for NAFLD is a lifestyle intervention focused on diet, physical activity, and behaviour modification to attain a 7-10% weight reduction, that may lead to a
significant improvement in liver histology in NASH
patients (step 1 - figure 3).
Previous studies have indicated that a weight
reduction of more than ten percent can induce the
resolution of NASH and improve fibrosis by at least
one stage.19,26 Even a modest weight reduction of
five percent can improve the intrahepatic TG
content and reduce steatosis (figure 4).19,27
Unfortunately, it is often challenging for an NAFLD
patient to make and maintain these lifestyle
changes without the appropriate motivation and
background knowledge concerning their disease.

8
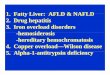
F IG UR E 3 . SCH EMAT IC OV ERV IE W OF THE D IF FE RENT STEPS IN THE TR EA TMENT OF NON-ALCOHOL IC FA TT Y L IV E R D IS EAS E .
First step in the management of NAFLD patients is to achieve a weight reduction of 7-10% BW by means of lifestyle changes. Secondly, in
individuals with BMI > 35 Kg/m2 who do not reach the weight loss goal, medication or bariatric surgery, as a last resort, are advisable.
Abbreviations: BMI, body mass index; CVD, cardiovascular disease; GLP-1RA, glucagon-like peptide-1 receptor agonist; NAFLD, non-alcoholic
fatty liver; OCA, obeticholic acid; SGLT-2, sodium-glucose cotransporter-2. Adapted from: Polyzos et al. 2019 and Mundi et al. 2020.28,29
Remission of steatosis can be achieved by weight
reduction through different diets, such as calorie
restriction or an isocaloric Mediterranean diet
(which induces metabolic and anti-inflammatory
benefits), as indicated by several clinical trials.27,32-34
The evidence that certain foods and nutrients
prevent the progression of liver cancer is currently
derived only from large observational studies and
needs further confirmation.19 General
recommendations encourage a reduced intake of
saturated fatty acids, trans fatty acids, and fructose.
These macronutrients usually characterize the
Western dietary pattern.
Conversely a plant-based diets typically high in
fibre, with lower caloric density, lower saturated fat,
beneficial fatty acid composition (higher in
unsaturated fats) and anti-inflammatory
compounds, has been associated with a reduced
risk of NAFLD.30 Researchers have also investigated
functional food bioactives (omega 3 fatty acids,
polyphenols, vitamin E and D), whose consumption
may protect against NAFLD.31

9
F IG UR E 4 . IM PAC T OF L I F ESTY LE MOD IF ICA TIONS O N HISTO LOG ICAL FE AU TUR ES IN OV ER WE IGH T/OB ESE NAF LD PA TI ENTS .
Lifestyle intervention includes a hypocaloric (low carbohydrate) diet, combined with exercise. A dose-response relationship is evident
between weight loss % and overall histological improvements, with the greatest reduction observed in those with the greatest weight loss.
Weight reductions of >10% are required for inducing NASH resolution (reaching 90% of patients who achieved this weight reduction) or
improving fibrosis by at least one stage (81%). A more moderate weight loss of 5-7% is associated with a clinically meaningful regression of
disease status.
Abbreviations: NASH, non-alcoholic steatohepatitis; WL, weight loss.
Adapted from: Romero-Gomez M et al. 2017.19
MEDITERRANEAN DIET The Mediterranean diet can reduce liver fat even without weight loss and is the most recommended dietary pattern for NAFLD.
The diet is characterized by a reduced intake of
simple carbohydrates and an increased intake of
monounsaturated and omega-3 fatty acids.19 It
consists of high consumption of olive oil, nuts, fruits,
vegetables, fish, and a low intake of red meat and
sweets.19 This type of diet has been shown to
reduce the risk of CVD and diabetes.
Both outcomes are relevant to NAFLD patients.19
Moreover, adherence to the Mediterranean diet in
T2DM patients has been shown to be a protective
factor for the absence of liver fibrosis in these
patients.35 For example, in a single-arm trial among
overweight patients with NAFLD, adherence to the
Mediterranean diet led to a significant reduction in
liver fat.36 Giraldi et al. also indicated that a higher
vegetable and fish consumption was associated
with protective effects against NAFLD in a large
case-control study.37

10
ROLE OF PLANT PROTEIN The Mediterranean diet can reduce liver fat even when iso-caloric and not leading to changes in body weight.38 This strengthens the hypothesis that specific functional foods, characterized by components with a clear activity on specific metabolic pathways, may provide benefit in the management of the disease. Plant proteins deserve a special consideration: plant protein-enriched diets have become a common strategy to improve weight management and increased intake has a potential role in the prevention of T2DM.39 Among dietary approaches, soy proteins offer an optimal choice. Soy foods are rich sources of protein, polyunsaturated fat, fibre, vitamins and isoflavones (naturally occurring plant polyphenols) including genistein, daidzein and glycitein. According to a meta-analysis from 17 observational studies, consumption of soy foods has been associated with a reduced risk of CVD, which is the most common comorbidity in NAFLD.40 Moreover, a systematic review and meta-analysis of randomized controlled trials (RCT) have reported that supplementation of soy isoflavones reduces arterial stiffness.41 Hypertension is one of the most important risk factors of CVD, as well as a major condition characterizing MetS. These trials have shown that soy consumption improves systolic and diastolic BP in adults.42 The BP-lowering effect appears to be ascribable to soy isoflavones and peptides: genistein activates the endothelial nitric oxide (NO) synthase (eNOS) and stimulates NO release, whereas bioactive peptides found in soy protein inhibit the angiotensin-converting enzyme activity and reduce vasoconstrictor responses.43 Soy drinks (240 ml/day), as a part of low-calorie diet (500-deficit calorie diet), reduce serum alanine aminotransferase (ALT) and hs-CRP in patients with NAFLD.44 This approach has also shown to exert a beneficial effect on IR and BP in overweight/obese patients with NAFLD.45 Similar conclusions were drawn in 58 NAFLD patients who received a
low-calorie, low-carbohydrate soy diet, although the protective effect was dependent on baseline weight.46 This latter diet also reduced ALT, malondialdehyde and serum fibrinogen levels (markers of oxidative stress) in NAFLD patients.47 Genistein is a biologically active isoflavone extracted from soybean products and contained in several soy-based foods. Some studies have investigated the impact of genistein on NAFLD-related MetS. Consuming 54 mg of genistein daily for 1 year improved the HOMA-IR and led to reductions in fasting glucose and insulin in postmenopausal women with MetS. Genistein increased HDL-cholesterol and adiponectin and reduced low-density lipoprotein (LDL) cholesterol and TG levels.48 In a double-blind RCT, NAFLD patients received either 250 mg genistein (n= 41) or placebo (n= 41) daily for 8-weeks. Genistein improved IR, reduced inflammation by lowering tumour necrosis factor alpha (TNF-α) and interleukin 6 (IL-6) levels, and improved fat metabolism.49 In a large population-based cross-sectional study on 23,529 participants, the higher dietary fibre intake from whole grain, soy foods, vegetables and nuts was associated with lower prevalence of newly diagnosed NAFLD in men.50 This dietary approach can also be of value in more advanced stages of disease. Comparing a 24-week lifestyle intervention program with a soy protein-based meal replacement therapy in NASH patients, both lifestyle changes or soy intervention showed similar effects on weight loss and hepatic fat content, as well as in reducing markers of liver inflammation.51 Overall, it appears that the protective effect of soy against fatty liver accumulation is mediated by an improvement of IR, a reduction in hepatic TG synthesis and inflammatory milieu. At present, availability of robust patient series with well characterized dietary intakes provides satisfactory information on the differential positive responses to vegetable-enriched dietary approaches in patients diagnosed with NAFLD or MAFLD. However, further larger-scale research is needed to fully clarify the efficacy of soy supplementation and better define the impact of specific diets on NAFLD versus MAFLD.

11
THE ROLE OF GUT MICROBIOME The interaction between gut microbiota and liver is a critical player in the development and progression of NAFLD. An intact intestinal barrier
antagonizes the translocation of bacterial products,
allowing active transport of nutrients across tight
junctions. Several studies have shown the
connection between gut and liver. For example,
diet and gut dysbiosis led to increased intestinal
permeability and was associated with the degree
of hepatic steatosis in NAFLD patients.52
Microbiome derived metabolites predict fibrosis
and cirrhosis in NAFLD.53 Gut flora and intestinal
permeability regulate glucose, lipid and choline
metabolism and affect intestinal permeability.54
Increased circulating levels of lipopolysaccharides
and other bioactive compounds lead to the
intrahepatic activation of proinflammatory cells and
hepatocytes, e.g. via stimulation of toll-like
receptor-2.55
OTHER TREATMENT OPTIONS
There are currently no drugs approved by the Food and Drug Administration (FDA) or European Medicines Agency (EMA) specifically for NAFLD. Nonetheless, there are antidiabetic medications with a direct and/or indirect effect on NAFLD such as glucagon-like peptide-1 receptor agonists (GLP-1RAs) and glitazones.58,59
GLP-1RAs accelerate satiety by slowing gastric
emptying, decreasing glucagon secretion, and
improving liver enzymes.56
Statins have effects on lipid metabolism and are
likely to be useful in the treatment of NAFLD, but
effects on histology or long-term prognosis of
NAFLD patients are not yet known.57 Vitamin E has a
proven effect on liver histology in non-diabetic and
non-cirrhotic NASH patients.58 Another potentially
useful medication in the treatment of NAFLD is
metformin (although no effect was shown on
histology).
Orlistat or GLP-1RAs are medications that support
weight loss, which is naturally difficult to maintain in
the long term for some patients.59 The only option
in high-risk patients who cannot obtain weight
reduction, is bariatric surgery such as gastric bypass
or a sleeve gastrectomy (step 3 - figure 3). These
procedures result in a potentially important effect
on weight by, amongst others, promoting satiety
and providing a reduced calorie intake. This
decrease in weight results in an improvement in the
severity of NAFLD. A recent meta-analysis described
that 59% of individuals with NAFLD who underwent
bariatric surgery saw an improvement in NASH and
30% had a reduction in fibrosis.60 But these
procedures are highly invasive, not without
complications, and long-term medical follow-up is
necessary.61

12
NAFLD AND CHILDHOOD
Not only has NAFLD reached epidemic proportions
in adults but childhood cases are also rising.62
NAFLD is a frequent complication of childhood
obesity.63 The incidence may be as high as 30% in
obese children, which increases with age and
weight.64
Paediatric NAFLD has distinctive histological and
pathogenic features and is an escalating cause of
chronic liver disease, with the potential of
impacting health outcomes in adolescents and
young adults.65 Once developed, NAFLD in
childhood is associated with T2DM, hypertension,
increased CVD risk, and end-stage liver disease.66 A
retrospective review of 742 American children and
adolescents between the ages of 2 and 19 years
who had an autopsy, showed that NAFLD is the
most common liver abnormality.67 Aside from the
extensive knowledge on the incidence and
concomitant associated factors of NAFLD, there has
been little advancement in non-pharmacological
treatments of NAFLD up until now, particularly in
obese children. Dietary approaches to NAFLD in
children/adolescents, have been infrequently
studied, although some findings are promising.
CONCLUSION Healthy lifestyle and weight reduction remains crucial for the prevention and treatment of NAFLD. The weight decline will lead to a decrease in hepatic steatosis, inflammation, and fibrosis. Patients with NAFLD
should be advised to aim at losing 7–10% of their total body weight by eating a modestly hypocaloric diet
(- 500 kcal/day) and engaging in regular exercise (30–60 min on 3–5 days/week).
To achieve this weight loss, a plant-based diet (e.g. Mediterranean diet) is recommended in the treatment of NAFLD. The use of soy products combined with a low-calorie, low-carbohydrate diet may be effective in ameliorating different NAFLD parameters. However, research on soy products and their specific effects on
NAFLD, especially in the long term, is still missing and needs to be addressed in future clinical studies.
To improve patient care, there is a strong need for a multidisciplinary approach from internists, gastro-
enterologists, cardiologists, diabetologists, and nutritionists.
Moreover, renaming NAFLD to MAFLD may bring this disease back to reality and closer, not only to its
pathophysiology, but also to other metabolic disorders like T2DM and CVD.

13
References
1. Younossi ZM, Koenig AB, Abdelatif D, Fazel Y, Henry L, Wymer M: Global epidemiology of nonalcoholic fatty liver disease-Meta-analytic assessment of prevalence, incidence, and outcomes. Hepatology 2016, 64:73-84.
2. Younossi Z, Anstee QM, Marietti M, Hardy T, Henry L, Eslam M, George J, Bugianesi E: Global burden of NAFLD and NASH: trends, predictions, risk factors and prevention. Nat Rev Gastroenterol Hepatol 2018, 15:11-20.
3. Powell EE, Wong VW, Rinella M: Non-alcoholic fatty liver disease. Lancet 2021.
4. Schaffner F, Thaler H: Nonalcoholic fatty liver disease. Prog Liver Dis 1986, 8:283-98.
5. Tanaka N, Kimura T, Fujimori N, Nagaya T, Komatsu M, Tanaka E: Current status, problems, and perspectives of non-alcoholic fatty liver disease research. World J Gastroenterol 2019, 25:163-77.
6. Estes C, Anstee QM, Arias-Loste MT, Bantel H, Bellentani S, Caballeria J, Colombo M, Craxi A, Crespo J, Day CP, Eguchi Y, Geier A, Kondili LA, Kroy DC, Lazarus JV, Loomba R, Manns MP, Marchesini G, Nakajima A, Negro F, Petta S, Ratziu V, Romero-Gomez M, Sanyal A, Schattenberg JM, Tacke F, Tanaka J, Trautwein C, Wei L, Zeuzem S, Razavi H: Modeling NAFLD disease burden in China, France, Germany, Italy, Japan, Spain, United Kingdom, and United States for the period 2016-2030. J Hepatol 2018, 69:896-904.
7. Bian Z, Ma X: Liver fibrogenesis in non-alcoholic steatohepatitis. Front Physiol 2012, 3:248.
8. Kumar R, Priyadarshi RN, Anand U: Non-alcoholic Fatty Liver Disease: Growing Burden, Adverse Outcomes and Associations. J Clin Transl Hepatol 2020, 8:76-86.
9. Meroni M, Longo M, Rustichelli A, Dongiovanni P: Nutrition and Genetics in NAFLD: The Perfect Binomium. Int J Mol Sci 2020, 21.
10. Ludwig J, Viggiano TR, McGill DB, Oh BJ: Nonalcoholic steatohepatitis: Mayo Clinic experiences with a hitherto unnamed disease. Mayo Clin Proc 1980, 55:434-8.
11. Ekstedt M, Franzen LE, Holmqvist M, Bendtsen P, Mathiesen UL, Bodemar G, Kechagias S: Alcohol consumption is associated with progression of hepatic fibrosis in non-alcoholic fatty liver disease. Scand J Gastroenterol 2009, 44:366-74.
12. Aberg F: Liver fibrosis scores in the general population: Better risk indices are needed! Hepatology 2018, 67:1186.
13. Siddiqui MS, Harrison SA, Abdelmalek MF, Anstee QM, Bedossa P, Castera L, Dimick-Santos L, Friedman SL, Greene K, Kleiner DE, Megnien S, Neuschwander-Tetri BA, Ratziu V, Schabel E, Miller V, Sanyal AJ, Liver Forum Case Definitions Working G: Case definitions for inclusion and analysis of endpoints in clinical trials for nonalcoholic steatohepatitis through the lens of regulatory science. Hepatology 2018, 67:2001-12.
14. Shiha G, Korenjak M, Eskridge W, Casanovas T, Velez-Moller P, Hogstrom S, Richardson B, Munoz C, Sigurethardottir S, Coulibaly A, Milan M, Bautista F, Leung NWY, Mooney V, Obekpa S, Bech E, Polavarapu N, Hamed AE, Radiani T, Purwanto E, Bright B, Ali M, Dovia CK, McColaugh L, Koulla Y, Dufour JF, Soliman R, Eslam M: Redefining fatty liver disease: an international patient perspective. Lancet Gastroenterol Hepatol 2021, 6:73-9.
15. Eslam M, Newsome PN, Sarin SK, Anstee QM, Targher G, Romero-Gomez M, Zelber-Sagi S, Wai-Sun Wong V, Dufour JF, Schattenberg JM, Kawaguchi T, Arrese M, Valenti L, Shiha G, Tiribelli C, Yki-Jarvinen H, Fan JG, Gronbaek H, Yilmaz Y, Cortez-Pinto H, Oliveira CP, Bedossa P, Adams LA, Zheng MH, Fouad Y, Chan WK, Mendez-Sanchez N, Ahn SH, Castera L, Bugianesi E, Ratziu V, George J: A new definition for metabolic dysfunction-associated fatty liver disease: An international expert consensus statement. J Hepatol 2020, 73:202-9.
16. Eslam M, Sanyal AJ, George J, International Consensus P: MAFLD: A Consensus-Driven Proposed Nomenclature for Metabolic Associated Fatty Liver Disease. Gastroenterology 2020, 158:1999-2014 e1.
17. Younossi ZM, Rinella ME, Sanyal AJ, Harrison SA, Brunt EM, Goodman Z, Cohen DE, Loomba R: From NAFLD to MAFLD: Implications of a Premature Change in Terminology. Hepatology 2020.
18. Moore JB: Non-alcoholic fatty liver disease: the hepatic consequence of obesity and the metabolic syndrome. Proc Nutr Soc 2010, 69:211-20.
19. Romero-Gomez M, Zelber-Sagi S, Trenell M: Treatment of NAFLD with diet, physical activity and exercise. J Hepatol 2017, 67:829-46.
20. Adams LA, Anstee QM, Tilg H, Targher G: Non-alcoholic fatty liver disease and its relationship with cardiovascular disease and other extrahepatic diseases. Gut 2017, 66:1138-53.
21. Assy N, Nasser G, Kamayse I, Nseir W, Beniashvili Z, Djibre A, Grosovski M: Soft drink consumption linked with fatty liver in the absence of traditional risk factors. Can J Gastroenterol 2008, 22:811-6.
22. Stephenson K, Kennedy L, Hargrove L, Demieville J, Thomson J, Alpini G, Francis H: Updates on Dietary Models of Nonalcoholic Fatty Liver Disease: Current Studies and Insights. Gene Expr 2018, 18:5-17.
23. Singh RK, Chang HW, Yan D, Lee KM, Ucmak D, Wong K, Abrouk M, Farahnik B, Nakamura M, Zhu TH, Bhutani T, Liao W: Influence of diet on the gut microbiome and implications for human health. J Transl Med 2017, 15:73.
24. Khoshbin K, Camilleri M: Effects of dietary components on intestinal permeability in health and disease. Am J Physiol Gastrointest Liver Physiol 2020, 319:G589-G608.
25. Wang Z, Klipfell E, Bennett BJ, Koeth R, Levison BS, Dugar B, Feldstein AE, Britt EB, Fu X, Chung YM, Wu Y, Schauer P, Smith JD, Allayee H, Tang WH, DiDonato JA, Lusis AJ, Hazen SL: Gut flora metabolism of phosphatidylcholine promotes cardiovascular disease. Nature 2011, 472:57-63.
26. Hallsworth K, Adams LA: Lifestyle modification in NAFLD/NASH: Facts and figures. JHEP Rep 2019, 1:468-79.
27. Sandby K, Geiker NRW, Dalamaga M, Gronbaek H, Magkos F: Efficacy of Dietary Manipulations for Depleting Intrahepatic Triglyceride Content: Implications for the Management of Non-alcoholic Fatty Liver Disease. Curr Obes Rep 2021.
28. Polyzos SA, Kountouras J, Mantzoros CS: Obesity and nonalcoholic fatty liver disease: From pathophysiology to therapeutics. Metabolism 2019, 92:82-97.
29. Mundi MS, Velapati S, Patel J, Kellogg TA, Abu Dayyeh BK, Hurt RT: Evolution of NAFLD and Its Management. Nutr Clin Pract 2020, 35:72-84.
30. Zelber-Sagi S, Salomone F, Mlynarsky L: The Mediterranean dietary pattern as the diet of choice for non-alcoholic fatty liver disease: Evidence and plausible mechanisms. Liver Int 2017, 37:936-49.

14
31. Dongiovanni P, Lanti C, Riso P, Valenti L: Nutritional therapy for nonalcoholic fatty liver disease. J Nutr Biochem 2016, 29:1-11.
32. Abenavoli L, Greco M, Milic N, Accattato F, Foti D, Gulletta E, Luzza F: Effect of Mediterranean Diet and Antioxidant Formulation in Non-Alcoholic Fatty Liver Disease: A Randomized Study. Nutrients 2017, 9.
33. Abenavoli L, Boccuto L, Federico A, Dallio M, Loguercio C, Di Renzo L, De Lorenzo A: Diet and Non-Alcoholic Fatty Liver Disease: The Mediterranean Way. Int J Environ Res Public Health 2019, 16.
34. Suarez M, Boque N, Del Bas JM, Mayneris-Perxachs J, Arola L, Caimari A: Mediterranean Diet and Multi-Ingredient-Based Interventions for the Management of Non-Alcoholic Fatty Liver Disease. Nutrients 2017, 9.
35. Aller R, Siguenza R, Pina M, Laserna C, Antolin B, Burgueno B, Dura M, Izaola O, Primo D, de Luis DA: Insulin resistance is related with liver fibrosis in type 2 diabetic patients with non-alcoholic fatty liver disease proven biopsy and Mediterranean diet pattern as a protective factor. Endocrine 2020, 68:557-63.
36. Trovato FM, Catalano D, Martines GF, Pace P, Trovato GM: Mediterranean diet and non-alcoholic fatty liver disease: the need of extended and comprehensive interventions. Clin Nutr 2015, 34:86-8.
37. Giraldi L, Miele L, Aleksovska K, Manca F, Leoncini E, Biolato M, Arzani D, Pirro MA, Marrone G, Cefalo C, Racco S, Liguori A, Rapaccini G, Miggiano GA, Gasbarrini A, Boccia S, Grieco A: Mediterranean diet and the prevention of non-alcoholic fatty liver disease: results from a case-control study. Eur Rev Med Pharmacol Sci 2020, 24:7391-8.
38. Berna G, Romero-Gomez M: The role of nutrition in non-alcoholic fatty liver disease: Pathophysiology and management. Liver Int 2020, 40 Suppl 1:102-8.
39. Zhao M, Chen S, Ji X, Shen X, You J, Liang X, Yin H, Zhao L: Current innovations in nutraceuticals and functional foods for intervention of non-alcoholic fatty liver disease. Pharmacol Res 2021, 166:105517.
40. Yan Z, Zhang X, Li C, Jiao S, Dong W: Association between consumption of soy and risk of cardiovascular disease: A meta-analysis of observational studies. Eur J Prev Cardiol 2017, 24:735-47.
41. Man B, Cui C, Zhang X, Sugiyama D, Barinas-Mitchell E, Sekikawa A: The effect of soy isoflavones on arterial stiffness: a systematic review and meta-analysis of randomized controlled trials. Eur J Nutr 2021, 60:603-14.
42. He J, Wofford MR, Reynolds K, Chen J, Chen CS, Myers L, Minor DL, Elmer PJ, Jones DW, Whelton PK: Effect of dietary protein supplementation on blood pressure: a randomized, controlled trial. Circulation 2011, 124:589-95.
43. Dellafiora L, Pugliese R, Bollati C, Gelain F, Galaverna G, Arnoldi A, Lammi C: "Bottom-Up" Strategy for the Identification of Novel Soybean Peptides with Angiotensin-Converting Enzyme Inhibitory Activity. J Agric Food Chem 2020, 68:2082-90.
44. Eslami O, Shidfar F, Maleki Z, Jazayeri S, Hosseini AF, Agah S, Ardiyani F: Effect of Soy Milk on Metabolic Status of Patients with Nonalcoholic Fatty Liver Disease: A Randomized Clinical Trial. J Am Coll Nutr 2019, 38:51-8.
45. Maleki Z, Jazayeri S, Eslami O, Shidfar F, Hosseini AF, Agah S, Norouzi H: Effect of soy milk consumption on glycemic status, blood pressure, fibrinogen and malondialdehyde in patients with non-alcoholic fatty liver disease: a randomized controlled trial. Complement Ther Med 2019, 44:44-50.
46. Kani AH, Alavian SM, Esmaillzadeh A, Adibi P, Haghighatdoost F, Azadbakht L: Effects of a Low-Calorie, Low-Carbohydrate Soy Containing Diet on Systemic Inflammation Among Patients with Nonalcoholic Fatty Liver Disease: A Parallel Randomized Clinical Trial. Horm Metab Res 2017, 49:687-92.
47. Kani AH, Alavian SM, Esmaillzadeh A, Adibi P, Azadbakht L: Effects of a novel therapeutic diet on liver enzymes and coagulating factors in patients with non-alcoholic fatty liver disease: A parallel randomized trial. Nutrition 2014, 30:814-21.
48. Squadrito F, Marini H, Bitto A, Altavilla D, Polito F, Adamo EB, D'Anna R, Arcoraci V, Burnett BP, Minutoli L, Di Benedetto A, Di Vieste G, Cucinotta D, de Gregorio C, Russo S, Corrado F, Saitta A, Irace C, Corrao S, Licata G: Genistein in the metabolic syndrome: results of a randomized clinical trial. J Clin Endocrinol Metab 2013, 98:3366-74.
49. Amanat S, Eftekhari MH, Fararouei M, Bagheri Lankarani K, Massoumi SJ: Genistein supplementation improves insulin resistance and inflammatory state in non-alcoholic fatty liver patients: A randomized, controlled trial. Clin Nutr 2018, 37:1210-5.
50. Xia Y, Zhang S, Zhang Q, Liu L, Meng G, Wu H, Bao X, Gu Y, Sun S, Wang X, Zhou M, Jia Q, Song K, Wu Q, Niu K, Zhao Y: Insoluble dietary fibre intake is associated with lower prevalence of newly-diagnosed non-alcoholic fatty liver disease in Chinese men: a large population-based cross-sectional study. Nutr Metab (Lond) 2020, 17:4.
51. Deibert P, Lazaro A, Schaffner D, Berg A, Koenig D, Kreisel W, Baumstark MW, Steinmann D, Buechert M, Lange T: Comprehensive lifestyle intervention vs soy protein-based meal regimen in non-alcoholic steatohepatitis. World J Gastroenterol 2019, 25:1116-31.
52. De Munck TJI, Xu P, Verwijs HJA, Masclee AAM, Jonkers D, Verbeek J, Koek GH: Intestinal permeability in human nonalcoholic fatty liver disease: A systematic review and meta-analysis. Liver Int 2020, 40:2906-16.
53. Caussy C, Loomba R: Gut microbiome, microbial metabolites and the development of NAFLD. Nat Rev Gastroenterol Hepatol 2018, 15:719-20.
54. Ilan Y: Leaky gut and the liver: a role for bacterial translocation in nonalcoholic steatohepatitis. World J Gastroenterol 2012, 18:2609-18.
55. Miura K, Yang L, van Rooijen N, Brenner DA, Ohnishi H, Seki E: Toll-like receptor 2 and palmitic acid cooperatively contribute to the development of nonalcoholic steatohepatitis through inflammasome activation in mice. Hepatology 2013, 57:577-89.
56. Snyder HS, Sakaan SA, March KL, Siddique O, Cholankeril R, Cummings CD, Gadiparthi C, Satapathy SK, Ahmed A, Cholankeril G: Non-alcoholic Fatty Liver Disease: A Review of Anti-diabetic Pharmacologic Therapies. J Clin Transl Hepatol 2018, 6:168-74.
57. Kothari S, Dhami-Shah H, Shah SR: Antidiabetic Drugs and Statins in Nonalcoholic Fatty Liver Disease. J Clin Exp Hepatol 2019, 9:723-30.
58. Francque S, Vonghia L: Pharmacological Treatment for Non-alcoholic Fatty Liver Disease. Adv Ther 2019, 36:1052-74.
59. Garber AJ, Abrahamson MJ, Barzilay JI, Blonde L, Bloomgarden ZT, Bush MA, Dagogo-Jack S, DeFronzo RA, Einhorn D, Fonseca VA, Garber JR, Garvey WT, Grunberger G, Handelsman Y, Henry RR, Hirsch IB, Jellinger PS, McGill JB, Mechanick JI, Rosenblit PD, Umpierrez GE, American Association of Clinical E, American College of E: Consensus Statement by the American Association of Clinical Endocrinologists and American College of Endocrinology on the Comprehensive Type 2 Diabetes Management Algorithm--2016 Executive Summary. Endocr Pract 2016, 22:84-113.
60. Fakhry TK, Mhaskar R, Schwitalla T, Muradova E, Gonzalvo JP, Murr MM: Bariatric surgery improves nonalcoholic fatty liver disease: a contemporary systematic review and meta-analysis. Surg Obes Relat Dis 2019, 15:502-11.
61. Huang TD, Behary J, Zekry A: Non-alcoholic fatty liver disease: a review of epidemiology, risk factors, diagnosis and management. Intern Med J 2020, 50:1038-47.

15
62. Anderson EL, Howe LD, Jones HE, Higgins JP, Lawlor DA, Fraser A: The Prevalence of Non-Alcoholic Fatty Liver Disease in Children and Adolescents: A Systematic Review and Meta-Analysis. PLoS One 2015, 10:e0140908.
63. Feldstein AE, Charatcharoenwitthaya P, Treeprasertsuk S, Benson JT, Enders FB, Angulo P: The natural history of non-alcoholic fatty liver disease in children: a follow-up study for up to 20 years. Gut 2009, 58:1538-44.
64. Clemente MG, Mandato C, Poeta M, Vajro P: Pediatric non-alcoholic fatty liver disease: Recent solutions, unresolved issues, and future research directions. World J Gastroenterol 2016, 22:8078-93.
65. Lonardo A, Leoni S, Alswat KA, Fouad Y: History of Nonalcoholic Fatty Liver Disease. Int J Mol Sci 2020, 21.
66. Castillo-Leon E, Cioffi CE, Vos MB: Perspectives on youth-onset nonalcoholic fatty liver disease. Endocrinol Diabetes Metab 2020, 3:e00184.
67. Schwimmer JB, Deutsch R, Kahen T, Lavine JE, Stanley C, Behling C: Prevalence of fatty liver in children and adolescents. Pediatrics 2006, 118:1388-93.
68. Dongiovanni P, Paolini E, Corsini A, Sirtori RS, Ruscica M: Nonalcoholic fatty liver disease or metabolic dysfunction-associated fatty liver disease diagnoses and cardiovascular diseases: From epidemiology to drug approaches . Eur J Clin Invest 2021.
69. Heyens LJM, Busschots D, Koek GH, Robaeys G, Francque S: Liver Fibrosis in Non-alcoholic Fatty Liver Disease: From Liver Biopsy to Non-invasive Biomarkers in Diagnosis and Treatment. eCollection 2021

16
MORE INFORMATION ON
WWW.ALPROFOUNDATION.ORG
LinkedIn@AlproFoundation