Embed Size (px)
Citation preview

Reverse Shoulder Arthroplasty forthe Treatment of ProximalHumeral Fractures
Michael S. George, MD
Michael Khazzam, MD
Paul Chin, MD, PhD
Guillaume Dumont, MD
Robert Russell, MD
Investigation performed at KSFOrthopaedic Center, Houston, Texas,and University of Texas SouthwesternMedical Center, Dallas, Texas
COPYRIGHT © 2014 BY THEJOURNAL OF BONE AND JOINTSURGERY, INCORPORATED
» Reverse shoulder arthroplasty for the treatment of complex fracturesof the proximal part of the humerus appears to have good results atshort and intermediate-term follow-up.
» Malunion or nonunion of the tuberosities does not affect thefunctional result after reverse total shoulder arthroplasty as much as itdoes after hemiarthroplasty, but it does lead to decreased postoper-ative external rotation.
» Long-term outcomes of reverse shoulder arthroplasty for thetreatment of fractures have still not been well established.
Proximal humeral fractures ac-count for approximately 5% offractures that are seen in theemergency department and can
present difficult challenges to the treatingphysician1. These fractures are most com-monly classified according to the systemproposed by Neer2. Complex proximalhumeral fractures that require operativetreatment can be treated with osteosyn-thesis, hemiarthroplasty, total shoulderarthroplasty, or, more recently, reverseshoulder arthroplasty3. While locked plat-ing may result in improved fixation inosteopenic bone compared with traditionalunlocked plating, the outcomes may stillbe limited by the risk of complications,including stiffness, osteonecrosis, implantfailure, and loss of reduction4,5. Hemiar-throplasty traditionally has been performedfor the treatment of three or four-partfractures, particularly in patients withosteopenic bone, and can yield good results
for low-demand patients6,7. The outcomesof hemiarthroplasty for the treatment ofproximal humeral fracture are satisfactoryfor long-term pain relief but are lesspredictable in terms of shoulder motion8.Reverse shoulder arthroplasty can be usedfor the treatment of cuff tear arthropathyand recently has gained popularity for thetreatment of severe proximal humeralfractures. The present review of the currentliterature on the use of reverse shoulderarthroplasty for the treatment of complexproximal humeral fractures focuses onindications, preoperative planning, surgicaltechniques, and complications.
BackgroundDemographic CharacteristicsInjuries involving the proximal part of thehumerus prompted approximately184,000 visits to the emergency depart-ment in 2008 in the United States. Theoverwhelming majority of these injuries
Disclosure: None of the authors received payments or services, either directly or indirectly (i.e., via
his or her institution), from a third party in support of any aspect of this work. None of the
authors, or their institution(s), have had any financial relationship, in the thirty-six months prior
to submission of this work, with any entity in the biomedical arena that could be perceived to
influence or have the potential to influence what is written in this work. Also, no author has
had any other relationships, or has engaged in any other activities, that could be perceived to
influence or have the potential to influence what is written in this work. The complete
Disclosures of Potential Conflicts of Interest submitted by authors are always provided with the
online version of the article.
|
JBJS REVIEWS 2014;2(10) :e1 · http:/ /dx.doi .org/10.2106/JBJS.RVW.M.00140 1

occurred inpatients older than fifty yearsof age, with the number peaking in theeighty to eighty-five-year age range. Theincidence increased exponentially be-tween the ages of forty and eighty-fouryears for women and between the ages ofsixty and eighty-nine years for men9.The most common mechanism of frac-ture in elderly patients is a fall fromstanding.
DiagnosisA complete history and physical exami-nation, including an assessment ofgeneral health status, is necessary whenevaluating a patientwhohas a suspectedproximal humeral fracture. Rangeof motion and strength are usuallylimited because of pain. A detailedneurovascular examination of theaffected extremity should be performedbecause injuries to the axillary andsuprascapular nerves and the axillaryartery can occur in association withproximal humeral fractures10,11. In theacute setting, axillary and suprascapularnerve function can be evaluated bytesting isometric muscle contractionas well as sensibility in the distributionof the axillary nerve.
Radiographs include a minimumof two orthogonal radiographs of theglenohumeral joint12. A true antero-posterior (Grashey) radiograph andan axillary lateral radiograph can beused to assess the congruity of theglenohumeral joint13. When painprecludes abduction of the arm for anaxillary lateral radiograph, a truescapulolateral (scapular-Y) and/or aVelpeau axillary radiograph should bemade14,15. Computed tomography(CT) with three-dimensional recon-struction can provide excellentvisualization of fracture fragmentsand also can be used to evaluate forassociated fractures of the glenoid andscapular body. Magnetic resonanceimaging (MRI) can be used to deter-mine the status of the rotator cuff andto aid in surgical decision-making,particularly when choosing betweenhemiarthroplasty and reverse shoulderarthroplasty.
Fracture ClassificationThe most commonly employed classi-fication system for proximal humeralfractures is the Neer classificationsystem2. This system describes frac-tures in terms of displacement offour segments of the proximal partof the humerus as identified originallyby Codman: the greater tuberosity,lesser tuberosity, head, and shaft16.Displaced fractures include two-part,three-part, and four-part fractures;the definition of a part requires anindividual fragment to be displacedby.1 cm or rotated 45° from itsnormal anatomic position. Minimallydisplaced fractures, therefore, canhave fracture lines through multiplefragments but are classified as one-part fractures. Furthermore, thesystem classifies articular surface head-splitting fractures as well as fracture-dislocations according to parts andanterior or posterior displacementof the head. The AO Muller classifi-cation system divides proximalhumeral fractures into three groups(A, B, C) with three separatesubgroups (A1, A2, A3, etc.), withconsideration being given to thenumber of fracture lines, the locationof fractures, impaction, dislocation,and displacement17.
The limitations of the Neerand AO Muller proximal humeralclassification systems rest in their lowintraobserver reproducibility andinterobserver reliability15; neverthe-less, they represent the best attemptsat organizing a natural continuumof injury into separate categorieswith prognostic and treatmentimplications.
Surgical IndicationsThe majority of proximal humeralfractures in elderly patients can besuccessfully treated nonoperativelywith an initial period of immobilizationin a sling followed by a gradual returnto activities. However, nonoperativetreatment of three and four-part frac-tures often results in a poor functionalresult because of nonunion, malunion,
posttraumatic glenohumeral arthritis,or stiffness18,19. Surgical options in-clude closed reduction and percutane-ous pinning, open reduction andinternal fixation with locked orunlocked plating, lockedintramedullary nailing, or shoulderarthroplasty, depending on the fracturepattern and on patient and surgeonpreference.
Adequate reduction and fixationof three and four-part fractures istechnically very difficult to obtain andmaintain with closed reduction andpercutaneous pinning.Open reductionand internal fixation is possible but isassociated with a high rate of compli-cations, including screw penetration,loss of fixation, and osteonecrosis ofthe humeral head, leading to pooroutcomes and a failure rate of 15%to 20%20,21.
Neer described the use of hemiar-throplasty to treat three and four-partfractures of the proximal part of thehumerus6. Although Neer reportedgood results, subsequent studies failedto produce predictably good functionaloutcomes8,22,23. Complications ofhemiarthroplasty for the treatmentof proximal humeral fracture haveincluded poor range of motion, glenoiderosion, component loosening ormigration, and persistent pain. Themost common complication associatedwith a poor outcome after hemiar-throplasty for the treatment of aproximal humeral fracture is malunionor nonunion of the greater tuberosity,which occurs in 39% to 50% ofcases3,23-25.
Because of a lack of consistentlygood outcomes for patients managedwith the above-mentioned techniques,surgeons began to explore the efficacy ofreverse shoulder arthroplasty for thesecomplicated and difficult fractures.Fractures associated with severe tuber-osity comminution may be associatedwith a higher rate of failure when treatedwith traditional open reduction andinternal fixation or hemiarthroplasty,and, therefore, reverse shoulder arthro-plasty may be a better option for these
| R e v e r s e S h o u l d e r A r t h r o p l a s t y f o r t h e Tr e a tm e n t o f P r o x im a l Hum e r a l F r a c t u r e s
2 OCTOBER 2014 · VOLUME 2, ISSUE 10 · e1

fractures. Reverse shoulder arthroplastymay be indicated for acute, comminutedthree or four-part proximal humeralfractures in elderly patients or acutefractures in patients with preexistingrotator cuff deficiency. In addition,reverse shoulder arthroplasty is indi-cated for the treatment of fracturesequelae in patients who have under-gone osteosynthesis that has resultedin rotator cuff or tuberosity deficiencyor those who have had a failed hemi-arthroplasty that has resulted intuberosity deficiency. Reverse shoul-der arthroplasty should be avoidedin younger, active patients as theresults have been shown to deteriorateas early as six years postoperatively26.The surgeon should be very familiarwith the operative technique ofreverse shoulder arthroplasty, andconsideration should be given tomastering the technique on a cadaverspecimen.
Operative TechniqueA standard deltopectoral approachwith the patient in the beach-chairposition allows for exposure of theproximal humeral fracture as well asfor identification and mobilizationof the greater and lesser tuberosities.Although a superolateral approachfrequently is used in the setting ofreverse shoulder arthroplasty for thetreatment of rotator cuff tear arthrop-athy, this approach can also be usedin the fracture setting, but access tothe lesser tuberosity fragment may bedifficult.
The rotator interval is delineated,and the greater and lesser tuberosities aremobilized. The greater and lesser tu-berosities should be mobilized enoughso that they can be retracted out of theway for access to the glenoid. Heavytraction sutures are placed through thegreater and lesser tuberosities and therotator cuff, with any comminuted tu-berosity fragments being left attached tothe rotator cuff. Any remaining soft-tissue attachment of the lesser tuberosityis left undisturbed. A subpectoral soft-tissue biceps tenodesis is performedwith
heavy nonabsorbable suture, and theintra-articular biceps tendon stump isresected.
The fractured humeral head isextracted and measured. No furtherhumeral resection is typically needed.The humeral canal is sequentiallyreamed by hand to prevent iatrogenicfracture propagation. A trial humeralcomponent is placed to confirm properhumeral canal sizing and to approximatehumeral height, although proper hu-meral height cannot be confirmed untilafter the glenosphere is placed. The hu-meral trial component is then removed,and attention is turned to glenoidpreparation.
The greater tuberosity is retractedposteriorly, and the lesser tuberosityis retracted anteriorly, with care beingtaken not to detach any remainingsoft-tissue attachment. The labrumand the biceps tendon stump arecircumferentially excised. The glenoidcentral drill hole is placed slightlyinferior and posterior to the centerof the glenoid. The glenoid is thenreamed to remove articular cartilage,which is usually present in the settingof acute fractures. The glenoid base-plate is placedwith a 10° to 15° tilt frominferior to superior to avoid scapularnotching27-29. The proper glenosphereis selected, keeping in mind that alarger glenosphere provides optimalrange of motion and stability. Whenthe glenosphere is placed and stabilityis confirmed, attention is then turnedto the humeral side.
It is critical to place the humeralcomponent at the proper height toensure that proper soft-tissue tension-ing is achieved in order to preventcomponent instability and to maxi-mize range of motion. Humeral heightcan be established with use of one ofseveral methods, including use ofpreoperative radiographs of thecontralateral humerus to measureanatomic humeral height30 and therelationship of the superior aspectof the humeral head and the upperborder of the pectoralis major tendon(approximately 5.6 cm)31,32, with the
goal being anatomic reconstructionso that the normal position of thegreater tuberosity relative to thehumeral shaft can be restored.
Trial humeral stem and polyeth-ylene components are placed. Provi-sional suture fixation of the tuberositiesprovides an approximation of appropri-ate height and proper tension. A trialreduction is performed to further assessproper humeral height and tension.After removal of the trial componentand thorough canal irrigation, heavynonabsorbable sutures are placed inthe humerus through drill holes fortuberosity repair. A cemented humeralcomponent should be used as the frac-tured proximal part of the humeruscannot provide enough osseous stabilityto stabilize a press-fit humeral stem.The humeral stem is cemented in placein minimal posterior version with useof the markings on the trial componentas a guide to the appropriate height.Humeral version can be confirmed withuse of a guide pin in the humeral stemhandle or by marking the handle withamarkingpen. Placing the stembetweenneutral and 20° of retroversion has beenshown to provide optimal stabilityand to minimize scapular notching33,34.The trial humeral cup is again inserted.The proper tension can be assessed onthe basis of the tension of the deltoid andconjoined tendon. The tuberosities arerepaired horizontally to each other andto the prosthesis itself or around themedial neck of the prosthesis and thenare repaired vertically with transosseoussutures.
Preservation of the tuberositiesallows as much rotator cuff function aspossible and provides bone stock tosupport the implant. Bone graft fromthe humeral head is packed betweenthe tuberosities as well as between thetuberosities and the implant. Therotator interval is usually nonrepairablebecause of the inferior tension on thehumeral component. Intraoperativefluoroscopy with C-arm imaging isused to confirm tuberosity and implantplacement as well as concentricglenohumeral reduction as well as the
R e v e r s e S h o u l d e r A r t h r o p l a s t y f o r t h e Tr e a tm e n t o f P r o x im a l Hum e r a l F r a c t u r e s |
OCTOBER 2014 · VOLUME 2, ISSUE 10 · e1 3

avoidance of intraoperative glenoid orhumeral fracture (Fig. 1).
Each step in glenoid and humeralpreparation is performed with an eyetoward avoiding the most commoncomplications of reverse shoulderarthroplasty, including dislocation,intraoperative fracture, hematoma,infection, and scapular notching10,35-37.Risk factors that contribute to instabilityafter reverse shoulder arthroplasty in-clude poor soft-tissue tension, improperhumeral version, and deltoid dysfunc-tion38. Repair of the subscapularistendon and lesser tuberosity is importantgiven the increased rate of dislocationafter reverse shoulder arthroplasty inpatients with a nonrepairable subscapu-laris tendon39. Meticulous hemostasisis achieved, and the wound is closed overa drain. The risk of scapular notching canbe reduced by inferior placement andinferior angulation of the glenosphere.
Physical therapy involving gentlepassive range of motion is started im-mediately after surgery. Active abduc-tion and internal and external rotationare avoided for the first six weeks
postoperatively. The patient is instruc-ted to absolutely avoid using the affectedarm to push up from a seated position,particularly for the first six weeks post-operatively. Active range of motionand strengthening are advanced aftertuberosity healing is confirmedradiographically.
Results of Reverse ShoulderArthroplasty for ProximalHumeral FractureReverse shoulder arthroplasty for thetreatment of complex fractures of theproximal part of the humerus appears tohave acceptable short and intermediate-term results for as long as six years(Table I and Table II). Patients aretypically able to achieve the ultimatefunctional result by twelve monthspostoperatively35. Furthermore, mal-union or nonunion of the tuberositiesdoes not affect the functional result asmuch as it does in patients who haveundergone hemiarthroplasty, but it doeslead to decreased postoperative externalrotation10,35. Although some studieshave demonstrated superior outcomes
after reverse shoulder arthroplasty ascompared with hemiarthroplasty, mostreports have presented Level-IVevidence40-42, and we are not aware ofany prospective randomized trials com-paring reverse shoulder arthroplastywith hemiarthroplasty.
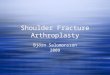
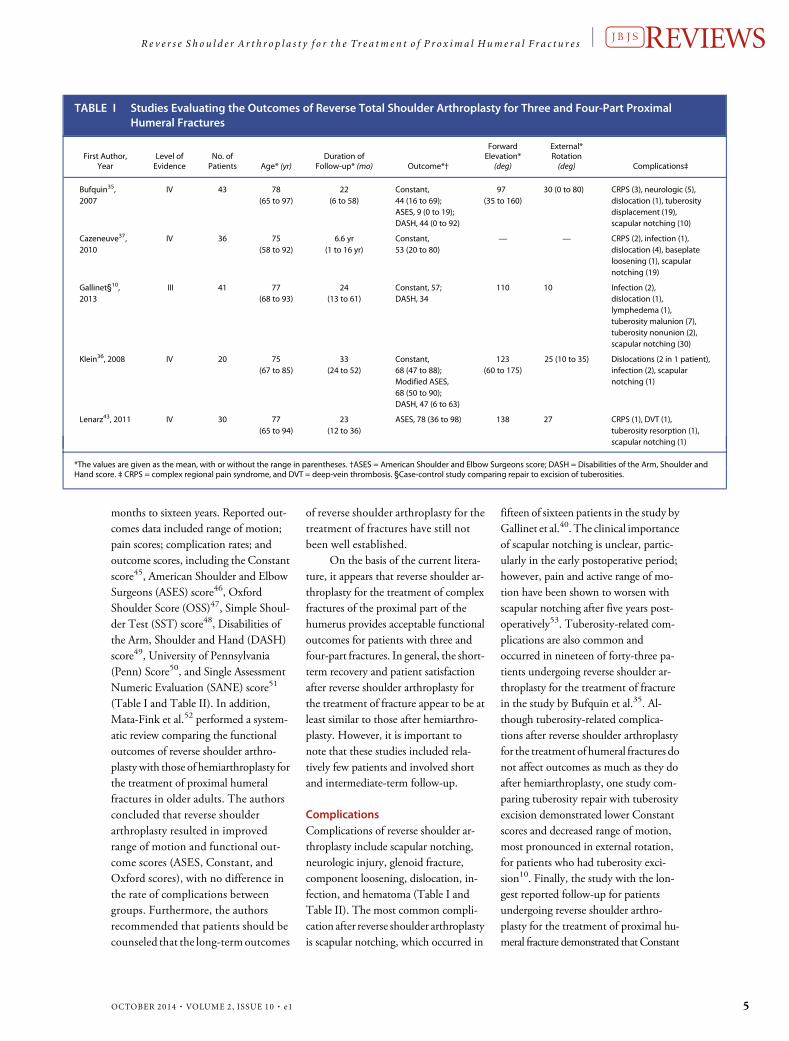
A review of the literature revealedfive case series10,35-37,43, includingone Level-III case-control study10, ofpatients undergoing reverse shoulderarthroplasty for the treatment of threeand four-part fractures of the proximalpart of the humerus (Table I). Thereview also revealed three retrospectivereviews40-42, one Level-III retrospectivecase-control study44, and one Level-IIprospective cohort11 in which theoutcomes of hemiarthroplasty werecompared with those of reverse shoulderarthroplasty for the treatment ofcomplex fractures of the proximal partof the humerus (Table II). Twostudies37,40 on reverse shoulder arthro-plasty involved patients as young as fifty-eight years old; otherwise, all patientswere sixty-five years or older. Theduration of follow-up ranged from four
Fig. 1Radiograph made after reverse shoul-der arthroplasty for the treatment of aproximal humeral fracture.
| R e v e r s e S h o u l d e r A r t h r o p l a s t y f o r t h e Tr e a tm e n t o f P r o x im a l Hum e r a l F r a c t u r e s
4 OCTOBER 2014 · VOLUME 2, ISSUE 10 · e1
months to sixteen years. Reported out-comes data included range of motion;pain scores; complication rates; andoutcome scores, including the Constantscore45, American Shoulder and ElbowSurgeons (ASES) score46, OxfordShoulder Score (OSS)47, Simple Shoul-der Test (SST) score48, Disabilities ofthe Arm, Shoulder and Hand (DASH)score49, University of Pennsylvania(Penn) Score50, and Single AssessmentNumeric Evaluation (SANE) score51
(Table I and Table II). In addition,Mata-Fink et al.52 performed a system-atic review comparing the functionaloutcomes of reverse shoulder arthro-plasty with those of hemiarthroplasty forthe treatment of proximal humeralfractures in older adults. The authorsconcluded that reverse shoulderarthroplasty resulted in improvedrange of motion and functional out-come scores (ASES, Constant, andOxford scores), with no difference inthe rate of complications betweengroups. Furthermore, the authorsrecommended that patients should becounseled that the long-termoutcomes
of reverse shoulder arthroplasty for thetreatment of fractures have still notbeen well established.
On the basis of the current litera-ture, it appears that reverse shoulder ar-throplasty for the treatment of complexfractures of the proximal part of thehumerus provides acceptable functionaloutcomes for patients with three andfour-part fractures. In general, the short-term recovery and patient satisfactionafter reverse shoulder arthroplasty forthe treatment of fracture appear to be atleast similar to those after hemiarthro-plasty. However, it is important tonote that these studies included rela-tively few patients and involved shortand intermediate-term follow-up.
ComplicationsComplications of reverse shoulder ar-throplasty include scapular notching,neurologic injury, glenoid fracture,component loosening, dislocation, in-fection, and hematoma (Table I andTable II). The most common compli-cation after reverse shoulder arthroplastyis scapular notching, which occurred in
fifteen of sixteen patients in the study byGallinet et al.40. The clinical importanceof scapular notching is unclear, partic-ularly in the early postoperative period;however, pain and active range of mo-tion have been shown to worsen withscapular notching after five years post-operatively53. Tuberosity-related com-plications are also common andoccurred in nineteen of forty-three pa-tients undergoing reverse shoulder ar-throplasty for the treatment of fracturein the study by Bufquin et al.35. Al-though tuberosity-related complica-tions after reverse shoulder arthroplastyfor the treatment of humeral fractures donot affect outcomes as much as they doafter hemiarthroplasty, one study com-paring tuberosity repair with tuberosityexcision demonstrated lower Constantscores and decreased range of motion,most pronounced in external rotation,for patients who had tuberosity exci-sion10. Finally, the study with the lon-gest reported follow-up for patientsundergoing reverse shoulder arthro-plasty for the treatment of proximal hu-meral fracture demonstrated that Constant
TABLE I Studies Evaluating the Outcomes of Reverse Total Shoulder Arthroplasty for Three and Four-Part ProximalHumeral Fractures
First Author,Year
Level ofEvidence
No. ofPatients Age* (yr)
Duration ofFollow-up* (mo) Outcome*†
ForwardElevation*
(deg)
External*Rotation(deg) Complications‡
Bufquin35,2007
IV 43 78(65 to 97)
22(6 to 58)
Constant,44 (16 to 69);ASES, 9 (0 to 19);DASH, 44 (0 to 92)
97(35 to 160)
30 (0 to 80) CRPS (3), neurologic (5),dislocation (1), tuberositydisplacement (19),scapular notching (10)
Cazeneuve37,2010
IV 36 75(58 to 92)
6.6 yr(1 to 16 yr)
Constant,53 (20 to 80)
— — CRPS (2), infection (1),dislocation (4), baseplateloosening (1), scapularnotching (19)
Gallinet§10,2013
III 41 77(68 to 93)
24(13 to 61)
Constant, 57;DASH, 34
110 10 Infection (2),dislocation (1),lymphedema (1),tuberosity malunion (7),tuberosity nonunion (2),scapular notching (30)
Klein36, 2008 IV 20 75(67 to 85)
33(24 to 52)
Constant,68 (47 to 88);Modified ASES,68 (50 to 90);DASH, 47 (6 to 63)
123(60 to 175)
25 (10 to 35) Dislocations (2 in 1 patient),infection (2), scapularnotching (1)
Lenarz43, 2011 IV 30 77(65 to 94)
23(12 to 36)
ASES, 78 (36 to 98) 138 27 CRPS (1), DVT (1),tuberosity resorption (1),scapular notching (1)
*The values are given as the mean, with or without the range in parentheses. †ASES = American Shoulder and Elbow Surgeons score; DASH = Disabilities of the Arm, Shoulder andHand score. ‡ CRPS = complex regional pain syndrome, and DVT = deep-vein thrombosis. §Case-control study comparing repair to excision of tuberosities.
R e v e r s e S h o u l d e r A r t h r o p l a s t y f o r t h e Tr e a tm e n t o f P r o x im a l Hum e r a l F r a c t u r e s |
OCTOBER 2014 · VOLUME 2, ISSUE 10 · e1 5
scores decreased over time and scapularnotching increased over time, althoughthere was no comparison group37.
ConclusionThe results of reverse shoulder arthroplastyfor the treatment of proximal humeralfractures are encouraging. Prospective ran-domized studies are needed to compare theoutcomes of reverse shoulder arthroplastywith those of hemiarthroplasty in this sce-nario. Longer follow-up documentingcomponent longevity and late complica-tions is also necessary.
Source of FundingNo funds were received in support ofthis study.
Michael S. George, MD1,Michael Khazzam, MD2,Paul Chin, MD, PhD2,Guillaume Dumont, MD2,Robert Russell, MD2
1KSF Orthopaedic Center,17270 Red Oak Drive, Suite 200,Houston, TX 77090
2University of TexasSouthwestern Medical Center,
5323 Harry Hines Boulevard,Dallas, TX 75390
E-mail address for M.S. George:[email protected]
References1. Horak J, Nilsson BE. Epidemiology of fractureof the upper end of the humerus. Clin OrthopRelat Res. 1975 Oct;(112):250-3.
2. Neer CS 2nd. Displaced proximal humeralfractures. I. Classification and evaluation.J Bone Joint Surg Am. 1970 Sep;52(6):1077-89.
3. Boileau P, Trojani C, Walch G, Krishnan SG,RomeoA, SinnertonR. Shoulder arthroplasty forthe treatment of the sequelaeof fractures of the
TABLE II Studies Comparing Reverse Total Shoulder Arthroplasty (RSA) with Hemiarthroplasty (Hemi) for Three andFour-Part Proximal Humeral Fractures
First Author,Year
Level ofEvidence
No. ofPatients Age* (yr)
Duration ofFollow-up*
(mo) Outcome*†
ForwardElevation*
(deg)
External*Rotation(deg) Complications‡
Gallinet40, 2009 IV
RSA 16 74(58 to 84)
12(4 to 18)
Constant,53 (34 to 76)§;DASH, 37 (12 to 65)
98(20 to 150)§
9(0 to 80)§
Infection (2), CRPS (1),scapular notching (15)
Hemi 17 74(49 to 95)
16(6 to 55)
Constant,39 (19 to 61);DASH, 41 (18 to 60)
54(30 to 100)
14(0 to 30)
Neurologic (1), CRPS (2),infection (1), tuberositymalunion (3)
Garrigues42, 2012 IV
RSA 10 80(67 to 97)§
3.6 yr(1.3 to 3.8 yr)
Penn, 82 (73 to 99)§;ASES, 81 (75 to 88)§;SANE, 85 (70 to 95)§
121(90 to 145)§
34(10 to 45)
Scapular notching (1)
Hemi 9 69(57 to 87)
3.6 yr(1.3 to 3.8 yr)
Penn, 53 (29 to 86);ASES, 47 (30 to 81);SANE, 39 (0 to 90)
91 (30 to 140) 31(5 to 60)
Tuberosity nonunion (2),neurologic (2)
Cuff11, 2013 II
RSA 27 74.8(70 to 86)
29(24 to 36)
ASES, 77 (67 to 82)§;SST, 7.4 (6 to 9)§
139(102 to 172)§
24(8 to 42)
Transient ulnarparesthesia (1),periprosthetic fractureafter a fall (1)
Hemi 26 74.1(70 to 88)
39(36 to 48)
ASES, 62 (28 to 84);SST, 5.8 (1 to 9)
100(30 to 170)
25(0 to 48)
Tuberositynonunion (3),hematoma (1),pneumothoraxfrom intrascalenenerve block (1)
Boyle44, 2013 III
RSA 55 79.6(57 to 90)
5 yr Oxford, 41.5§ Revision rate, 1.7%
Hemi 313 71.9(27 to 96)
5 yr Oxford, 32.3 Revision rate, 1.1%
Young41, 2010 IV
RSA 10 77 22(16 to 37)
ASES, 65 (40 to 88);Oxford, 28.7 (15 to 56)
115(45 to 140)
49(5 to 105)
Scapular notching(2; 20%), tuberositynonunion (1)
Hemi 10 76 44(24 to 56)
ASES, 67 (26 to 100);Oxford, 22 (12 to 34)
108(50 to 180)
48(10 to 90)
Tuberosity malunion(2; 20%), infection (1),persistent painrequiring revision (1)
*The values are given as the mean, with or without the range in parentheses. †DASH = Disabilities of the Arm, Shoulder and Hand score; Penn = University of Pennsylvania shoulderscore; ASES = American Shoulder and Elbow Surgeons score; SANE = Single Assessment Numeric Evaluation; SST = Simple Shoulder Test. ‡CRPS = complex regional pain syndrome.§Significantly different from hemiarthroplasty group (p, 0.05).
| R e v e r s e S h o u l d e r A r t h r o p l a s t y f o r t h e Tr e a tm e n t o f P r o x im a l Hum e r a l F r a c t u r e s
6 OCTOBER 2014 · VOLUME 2, ISSUE 10 · e1
proximal humerus. J Shoulder ElbowSurg. 2001Jul-Aug;10(4):299-308.
4. Solberg BD, Moon CN, Franco DP, PaiementGD. Locked plating of 3- and 4-part proximalhumerus fractures in older patients: the effectof initial fracture pattern on outcome. J OrthopTrauma. 2009 Feb;23(2):113-9.
5. Jost B, Spross C, Grehn H, Gerber C. Lockingplate fixation of fractures of the proximalhumerus: analysis of complications, revisionstrategies and outcome. J Shoulder ElbowSurg.2013 Apr;22(4):542-9. Epub 2012 Sep 06.
6. Neer CS 2nd. Articular replacement for thehumeral head. J Bone Joint Surg Am. 1955 Apr;37(2):215-28.
7. Cai M, Tao K, Yang C, Li S. Internal fixationversus shoulder hemiarthroplasty for displaced4-part proximal humeral fractures in elderlypatients. Orthopedics. 2012 Sep;35(9):e1340-6.
8.Antuña SA, Sperling JW, Cofield RH. Shoulderhemiarthroplasty for acute fractures of theproximal humerus: aminimum five-year follow-up. J Shoulder Elbow Surg. 2008 Mar-Apr;17(2):202-9. Epub 2008 Jan 11.
9. Kim SH, Szabo RM, Marder RA. Epidemiologyof humerus fractures in the United States:nationwide emergency department sample,2008. Arthritis Care Res (Hoboken). 2012Mar;64(3):407-14.
10.GallinetD,AdamA,GasseN, Rochet S,ObertL. Improvement in shoulder rotation in complexshoulder fractures treated by reverse shoulderarthroplasty. J Shoulder Elbow Surg. 2013 Jan;22(1):38-44. Epub 2012 Jun 15.
11. Cuff DJ, Pupello DR. Comparison ofhemiarthroplasty and reverse shoulderarthroplasty for the treatment of proximalhumeral fractures in elderly patients. J BoneJoint Surg Am. 2013 Nov 20;95(22):2050-5.
12. Jensen KL, Rockwood CA. Radiographicevaluation of shoulder problems. In: RockwoodCA,Matsen FA,WirthMA, Lippitt SB, editors. Theshoulder. Philadelphia, PA: Elsevier ScienceHealth Science Division; 2009. p. 177-212.
13. Grashey R. Atlas typischer rontgenfilder.Munchen:Lehman;1923.
14.BloomMH,ObataWG.Diagnosisofposteriordislocation of the shoulder with use of Velpeauaxillary and angle-up roentgenographic views.J Bone Joint Surg Am. 1967 Jul;49(5):943-9.
15.NeerCS 2nd. Four-segment classificationofproximal humeral fractures: purpose andreliable use. J Shoulder Elbow Surg. 2002 Jul-Aug;11(4):389-400.
16. Codman EA. The shoulder: rupture of thesupraspinatus tendon and other lesions in orabout the subacromial bursa. Boston, MA:Thomas Todd; 1934. p 313-333.
17. Muller ME, Nazarian S, Koch P, Schatzker J.The comprehensive classificationof fractures oflong bones. Berlin, Germany: Springer-Verlag;1990.
18. Foruria AM, de Gracia MM, Larson DR,Munuera L, Sanchez-Sotelo J. The pattern of thefracture and displacement of the fragmentspredict the outcome in proximal humeralfractures. J Bone Joint Surg Br. 2011 Mar;93(3):378-86.
19. Olerud P, Ahrengart L, Ponzer S, Saving J,Tidermark J. Internal fixation versus nonopera-tive treatment of displaced 3-part proximalhumeral fractures in elderly patients: a ran-domizedcontrolled trial. J ShoulderElbowSurg.2011 Jul;20(5):747-55. Epub 2011 Mar 24.
20. Owsley KC, Gorczyca JT. Fracturedisplacement and screw cutout after openreduction and locked plate fixation of proximalhumeral fractures [corrected]. J Bone Joint SurgAm. 2008 Feb;90(2):233-40.
21. Lee CW, Shin SJ. Prognostic factors forunstable proximal humeral fractures treatedwith locking-plate fixation. J Shoulder ElbowSurg. 2009 Jan-Feb;18(1):83-8.
22. Neer CS 2nd. Displaced proximal humeralfractures. II. Treatment of three-part and four-part displacement. J Bone Joint Surg Am. 1970Sep;52(6):1090-103.
23. Boileau P, Krishnan SG, Tinsi L, Walch G,Coste JS, Mole D. Tuberosity malposition andmigration: reasons for poor outcomes afterhemiarthroplasty for displaced fractures of theproximal humerus. J Shoulder ElbowSurg. 2002Sep-Oct;11(5):401-12.
24. Tanner MW, Cofield RH. Prostheticarthroplasty for fractures and fracture-dislocations of the proximal humerus. ClinOrthop Relat Res. 1983 Oct;(179):116-28.
25. Bigiliani L, Flatow E, McCluskey G, Fischer R.Failed prosthetic replacement for displacedproximalhumeral fractures.OrthopTrans. 1991;15:747-8.
26.Guery J, Favard L, Sirveaux F, Oudet D, MoleD,Walch G. Reverse total shoulder arthroplasty.Survivorship analysis of eighty replacementsfollowed for five to ten years. J Bone Joint SurgAm. 2006 Aug;88(8):1742-7.
27. Boileau P, Watkinson DJ, Hatzidakis AM,Balg F. Grammont reverse prosthesis: design,rationale, and biomechanics. J Shoulder ElbowSurg. 2005 Jan-Feb;14(1)(Suppl S):147S-61S.
28.Werner CM, Steinmann PA, Gilbart M,Gerber C. Treatment of painful pseudoparesisdue to irreparable rotator cuff dysfunction withthe Delta III reverse-ball-and-socket totalshoulder prosthesis. J Bone Joint Surg Am. 2005Jul;87(7):1476-86.
29.Wall B, Nove-Josserand L, O’Connor DP,Edwards TB, Walch G. Reverse total shoulderarthroplasty: a review of results according toetiology. J Bone Joint Surg Am. 2007 Jul;89(7):1476-85.
30. Boileau P, Walch G, Krishnan S. Tuberosityosteosynthesis and hemiarthoplasty for four-part fractures of the proximal humerus. TechShoulder Elbow Surg. 2000;1:96-109.
31. Murachovsky J, Ikemoto RY, NascimentoLG, Fujiki EN, Milani C, Warner JJ. Pectoralismajor tendon reference (PMT): a new methodfor accurate restoration of humeral length withhemiarthroplasty for fracture. J Shoulder ElbowSurg. 2006 Nov-Dec;15(6):675-8. Epub 2006Oct 19.
32. Ponce BA, Thompson KJ, Rosenzweig SD,Tate JP, SarverDB, Thorpe JB 2nd, Sheppard ED,Lopez RR. Re-evaluation of pectoralis majorheight as an anatomic reference for humeralheight in fracture hemiarthroplasty. J ShoulderElbow Surg. 2013 Nov;22(11):1567-72. Epub2013 Apr 22.
33. Favre P, Sussmann PS, Gerber C. The effect ofcomponent positioning on intrinsic stability of thereverse shoulder arthroplasty. J Shoulder ElbowSurg. 2010 Jun;19(4):550-6. Epub 2010 Mar 23.
34. Berhouet J, Garaud P, Favard L. Evaluationof the role of glenosphere design and humeralcomponent retroversion in avoiding scapularnotching during reverse shoulder arthroplasty.J Shoulder Elbow Surg. 2014 Feb;23(2):151-8.Epub 2013 Jul 12.
35. Bufquin T, Hersan A, Hubert L, Massin P.Reverse shoulder arthroplasty for thetreatment of three- and four-part fractures ofthe proximal humerus in the elderly: aprospective review of 43 cases with a short-term follow-up. J Bone Joint Surg Br. 2007Apr;89(4):516-20.
36. Klein M, Juschka M, Hinkenjann B, SchergerB, Ostermann PA. Treatment of comminutedfractures of the proximal humerus in elderlypatients with the Delta III reverse shoulderprosthesis. J Orthop Trauma. 2008 Nov-Dec;22(10):698-704.
37. Cazeneuve JF, Cristofari DJ. The reverseshoulder prosthesis in the treatment offracturesof theproximalhumerus in theelderly.J Bone Joint Surg Br. 2010 Apr;92(4):535-9.
38. Cheung E, Willis M, Walker M, Clark R,Frankle MA. Complications in reverse totalshoulder arthroplasty. J Am Acad Orthop Surg.2011 Jul;19(7):439-49.
39. Edwards TB, Williams MD, Labriola JE,Elkousy HA, Gartsman GM, O’Connor DP.Subscapularis insufficiency and the risk ofshoulder dislocation after reverse shoulderarthroplasty. J Shoulder Elbow Surg. 2009 Nov-Dec;18(6):892-6. Epub 2009 Mar 17.
40. Gallinet D, Clappaz P, Garbuio P, Tropet Y,Obert L. Three or four parts complex proximalhumerus fractures: hemiarthroplasty versusreverse prosthesis: a comparative study of 40cases. Orthop Traumatol Surg Res. 2009 Feb;95(1):48-55. Epub 2009 Feb 06.
41. Young SW, Segal BS, Turner PC, Poon PC.Comparison of functional outcomes of reverseshoulder arthroplasty versus hemiarthroplastyin the primary treatment of acute proximalhumerus fracture. ANZ J Surg. 2010 Nov;80(11):789-93.
42. Garrigues GE, Johnston PS, Pepe MD,Tucker BS, Ramsey ML, Austin LS.Hemiarthroplasty versus reverse total shoulderarthroplasty for acute proximal humerusfractures in elderly patients. Orthopedics. 2012May;35(5):e703-8.
43. Lenarz C, Shishani Y, McCrum C, NowinskiRJ, Edwards TB, Gobezie R. Is reverse shoulderarthroplasty appropriate for the treatment offractures in the older patient? Early observa-tions. Clin Orthop Relat Res. 2011 Dec;469(12):3324-31.
44. Boyle MJ, Youn SM, Frampton CM, Ball CM.Functional outcomes of reverse shoulderarthroplasty compared with hemiarthroplastyfor acute proximal humeral fractures. JShoulder ElbowSurg. 2013 Jan;22(1):32-7. Epub2012 May 29.
45. Constant CR, Murley AH. A clinicalmethod of functional assessment of theshoulder. Clin Orthop Relat Res. 1987 Jan;(214):160-4.
46. Michener LA, McClure PW, Sennett BJ.American Shoulder and Elbow SurgeonsStandardized Shoulder Assessment Form,patient self-report section: reliability, validity,and responsiveness. J Shoulder Elbow Surg.2002 Nov-Dec;11(6):587-94.
47. Dawson J, Fitzpatrick R, Carr A.Questionnaire on the perceptions of patientsabout shoulder surgery. J Bone Joint Surg Br.1996 Jul;78(4):593-600.
48. Lippitt SB, Harryman DT, Matsen FA. Apractical tool for evaluating function: the simpleshoulder test. In: Matsen FA, Fu FH, Hawkins RJ,editors. The shoulder: a balance of mobility and
R e v e r s e S h o u l d e r A r t h r o p l a s t y f o r t h e Tr e a tm e n t o f P r o x im a l Hum e r a l F r a c t u r e s |
OCTOBER 2014 · VOLUME 2, ISSUE 10 · e1 7

stability. Rosemont, IL: American Academy ofOrthopaedic Surgeons;1993. p 501-518.
49. Hudak PL, Amadio PC, Bombardier C; TheUpper Extremity Collaborative Group (UECG).Development of an upper extremity outcomemeasure: the DASH (disabilities of the arm, shoulderand hand) [corrected] [Erratum in: Am J IndMed1996 Sep;30]. Am J IndMed. 1996 Jun;29(6):602-8.
50. Leggin BG, Michener LA, Shaffer MA,Brenneman SK, Iannotti JP, Williams GR Jr. The
Penn shoulder score: reliability and validity. JOrthop Sports Phys Ther. 2006 Mar;36(3):138-51.
51.Williams GN, Gangel TJ, Arciero RA,Uhorchak JM, Taylor DC. Comparison of theSingle AssessmentNumeric Evaluationmethodand two shoulder rating scales. Outcomesmeasures after shoulder surgery. Am J SportsMed. 1999 Mar-Apr;27(2):214-21.
52.Mata-Fink A, Meinke M, Jones C, Kim B, BellJE. Reverse shoulder arthroplasty for treatment
of proximal humeral fractures in older adults: asystematic review. J Shoulder Elbow Surg. 2013Dec;22(12):1737-48.
53. Sadoghi P, Leithner A, Vavken P, Holzer A,Hochreiter J, Weber G, Pietschmann MF, MullerPE. Infraglenoidal scapular notching in reversetotal shoulder replacement: a prospectiveseries of 60 cases and systematic review of theliterature. BMC Musculoskelet Disord. 2011;12:101. Epub 2011 May 19.
| R e v e r s e S h o u l d e r A r t h r o p l a s t y f o r t h e Tr e a tm e n t o f P r o x im a l Hum e r a l F r a c t u r e s
8 OCTOBER 2014 · VOLUME 2, ISSUE 10 · e1