Embed Size (px)
Citation preview
Reversal of DOACs and Lab Measurement
With thanks to Dr Adam Cuker
Disclosures
MarkCrowther
Currentstateofaffairs
• Fiveoralanticoagulantsincommonuse– Warfarin– aboutwhichwewillnottalkmuch
• INRtestingisprettygood
– Rivaroxaban– oralXainhibitor– Apixaban– oralXainhibitor– Edoxaban – oralXainhibitor– Dabigatran– oralIIainhibitor
• Heparinandlowmolecularweightheparin
Firstlywhatshouldwecallthem?
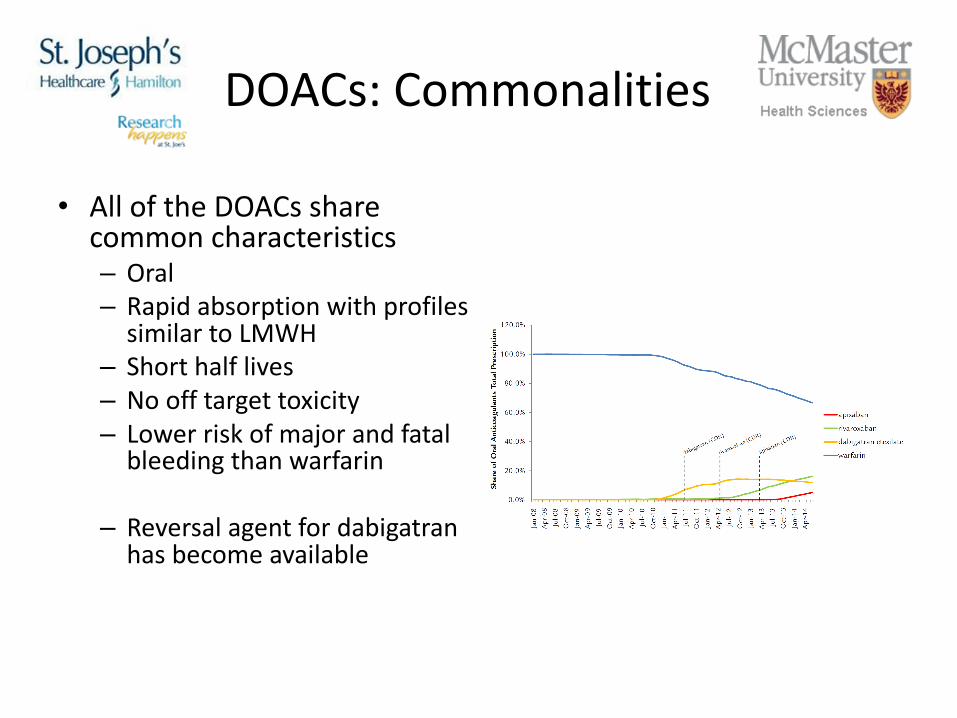
DOACs:Commonalities
• AlloftheDOACssharecommoncharacteristics– Oral– RapidabsorptionwithprofilessimilartoLMWH
– Shorthalflives– Noofftargettoxicity– Lowerriskofmajorandfatalbleedingthanwarfarin
– Reversalagentfordabigatranhasbecomeavailable
Case (1)
• A 71-year old man presents to the emergency department at 8 PM on Saturday night with abdominal pain and hypotension. Imaging reveals a ruptured AAA.
• PMH: Non-valvular atrial fibrillation, Hypertension, Dyslipidemia, Stroke 1 year ago
• Meds: HCTZ 25 mg QD, Atorvastatin 20 mg QD, Apixaban 5 mg BID
• Last dose of apixaban was 12 hours ago
• The surgeon calls the lab and wants proof there is no anticoagulant effect present
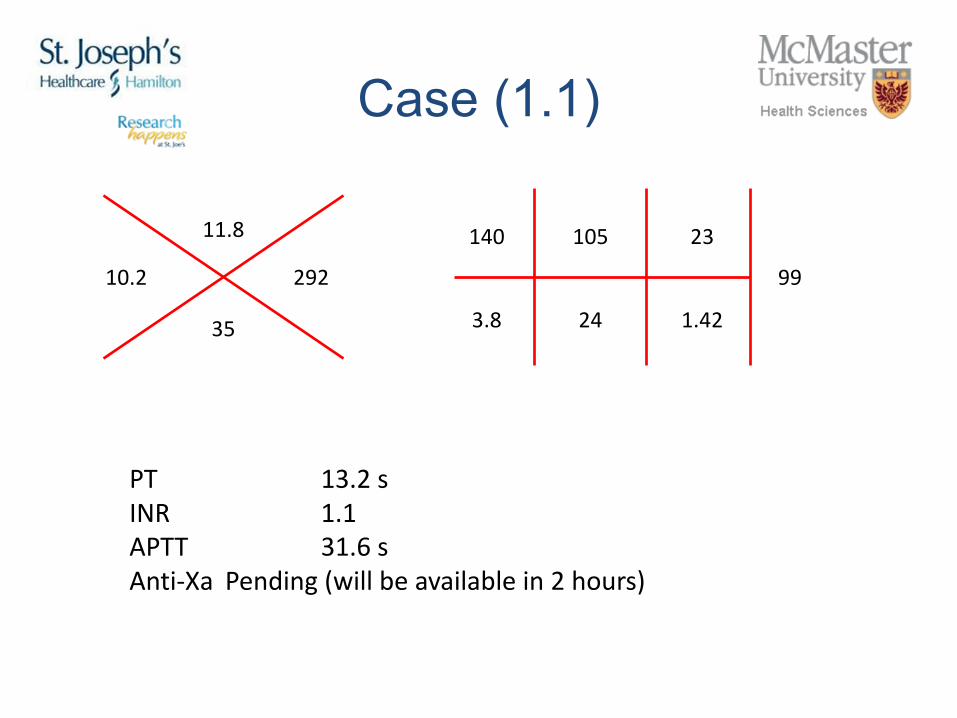
Case (1.1)
10.2 292
11.8
35
140
3.8
23
1.42
99
105
24
PT 13.2sINR 1.1APTT 31.6sAnti-Xa Pending(willbeavailablein2hours)
Case (3)
Vascular surgery recommends emergent open repair. Two hours is too long to wait.
What do you recommend?a) PT and APTT are normal. Patient is cleared to go to the OR without anticoagulant
reversal.b) Treat patient empirically with PCC before releasing him to the OR.c) PT and APTT are normal. Patient may have drug present however OR cannot wait.
PCC likely ineffective – advise surgeons that there may be excess bleedingd) A rapid Xa heparin level is available - and the result is less than the lower limit of
detection
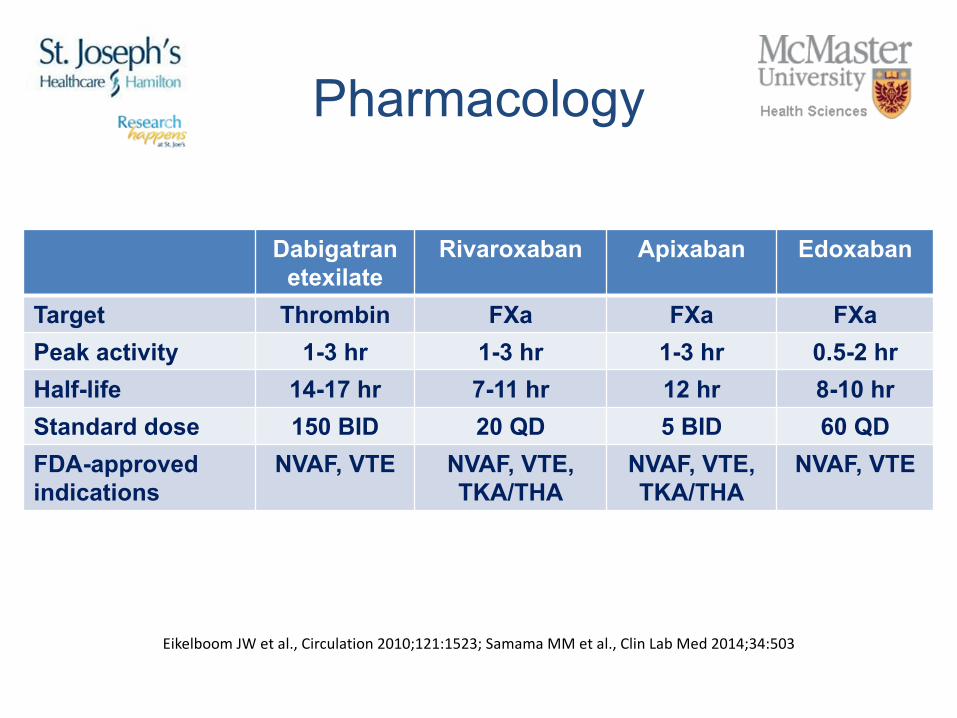
Pharmacology
Dabigatran etexilate
Rivaroxaban Apixaban Edoxaban
Target Thrombin FXa FXa FXaPeak activity 1-3 hr 1-3 hr 1-3 hr 0.5-2 hrHalf-life 14-17 hr 7-11 hr 12 hr 8-10 hrStandard dose 150 BID 20 QD 5 BID 60 QDFDA-approved indications
NVAF, VTE NVAF, VTE, TKA/THA
NVAF, VTE, TKA/THA
NVAF, VTE
Eikelboom JWetal.,Circulation2010;121:1523;Samama MMetal.,Clin LabMed2014;34:503
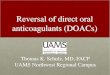
Laboratory MonitoringMeasurement
Exclude clinically relevant drug levels
Determine whether above on-therapy levels are present
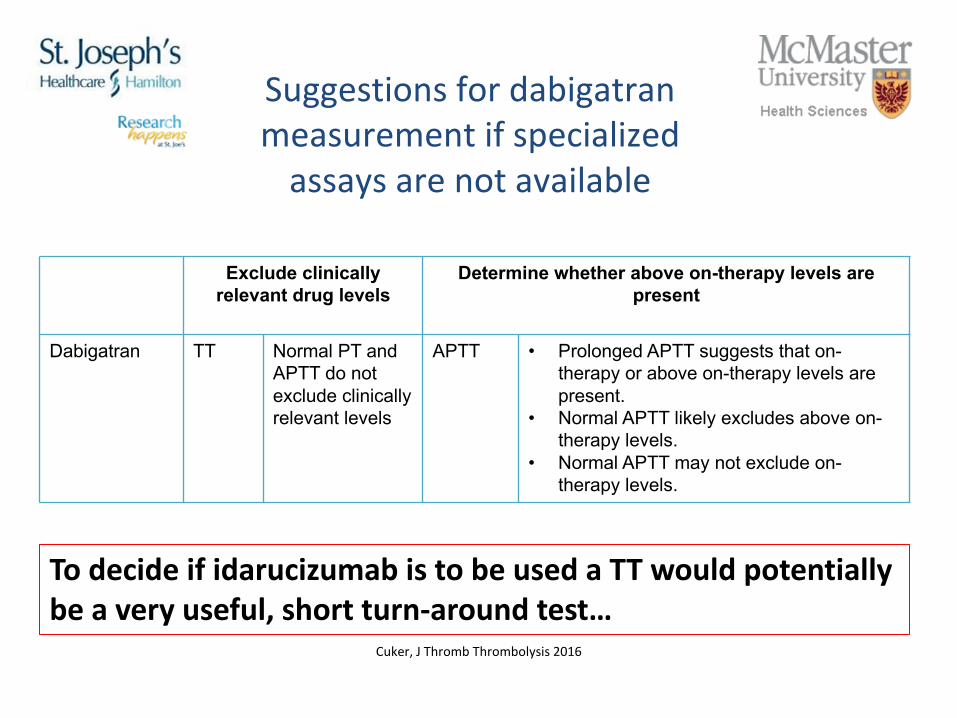
Dabigatran TT Normal PT and APTT do notexclude clinically relevant levels
APTT • Prolonged APTT suggests that on-therapy or above on-therapy levels are present.
• Normal APTT likely excludes above on-therapy levels.
• Normal APTT may not exclude on-therapy levels.
Suggestionsfordabigatranmeasurementifspecializedassaysarenotavailable
Cuker,JThromb Thrombolysis2016
TodecideifidarucizumabistobeusedaTTwouldpotentiallybeaveryuseful,shortturn-aroundtest…
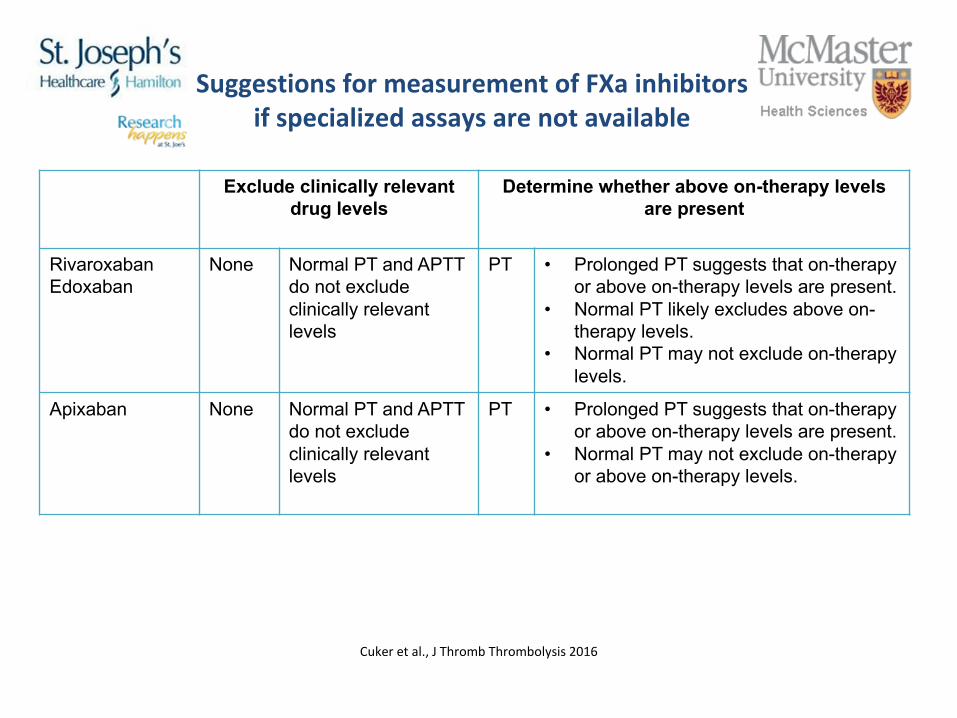
Exclude clinically relevant drug levels
Determine whether above on-therapy levels are present
RivaroxabanEdoxaban
None Normal PT and APTT do not exclude clinically relevant levels
PT • Prolonged PT suggests that on-therapyor above on-therapy levels are present.
• Normal PT likely excludes above on-therapy levels.
• Normal PT may not exclude on-therapy levels.
Apixaban None Normal PT and APTT do not exclude clinically relevant levels
PT • Prolonged PT suggests that on-therapyor above on-therapy levels are present.
• Normal PT may not exclude on-therapy or above on-therapy levels.
SuggestionsformeasurementofFXa inhibitorsifspecializedassaysarenotavailable
Cukeretal.,JThromb Thrombolysis2016
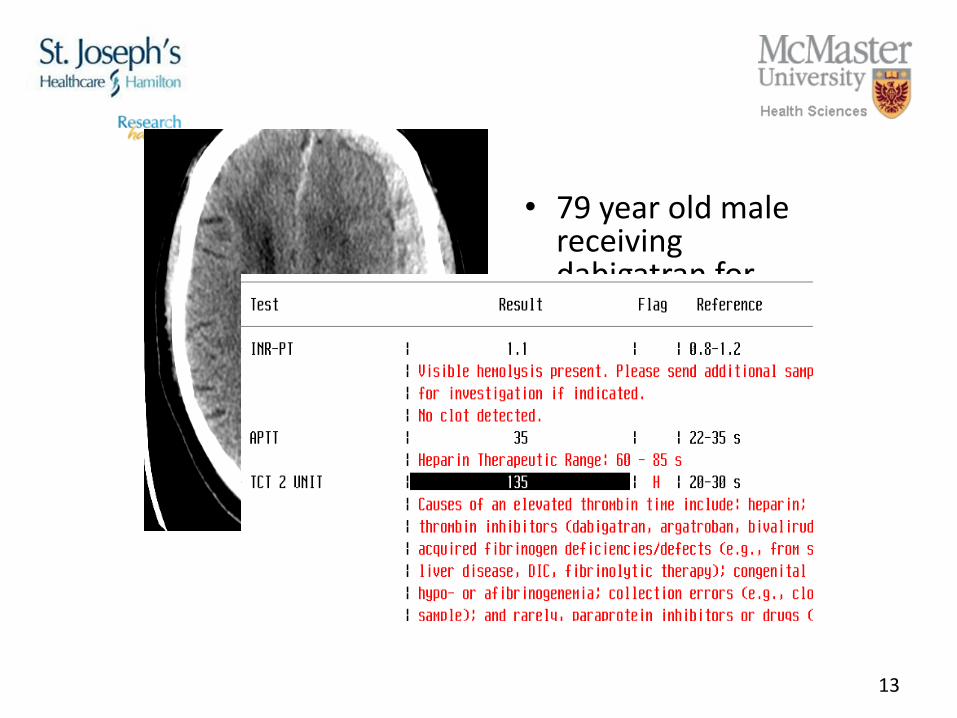
• 79yearoldmalereceivingdabigatranforstrokepreventioninthesettingofatrialfibrillation
• Presentswithnewhemiparesisandaphasia
13
Back to the case
What do you recommend?a) PT and APTT are normal. Patient is cleared to go to the OR
without anticoagulant reversal.b) Treat patient empirically with PCC before releasing him to the
OR.c) PT and APTT are normal. Patient may have drug present
however OR cannot wait. PCC likely ineffective – advise surgeons that there may be excess bleeding
d) A rapid Xa heparin level is available - and the result is less than the lower limit of detection
ReversingtheDOACs
17
Reversalagents
• Atpresent,XaDOACsdonothavereversalagents– IdarucizumabnowavailableintheUnitedStatesfordabigatran
• Availablereversalstrategiesrelyonnon-specificstrategiesthathaveunknowneffectiveness
• PCC/aPCC widelyusedbutwithNOevidenceofefficacy
• Whyisthisrelevanttothelaboratoryprofessional?– Youarelikelytobeaskedtogetinvolvedindecisionsaboutaccessduetocost
Per 977/Ciraparantag/Aripazine
• Smallmolecularweightmoietythatbindstoawidevarietyofanticoagulantsneutralizingtheiranticoagulantactivity
• Doesnotappeartoreversewarfarinorargatroban• Per977reportedlyinterfereswithassayssystemsforcoagulation
assays– Efficacyreportedusingchangesin“wholebloodclottingtime”
19
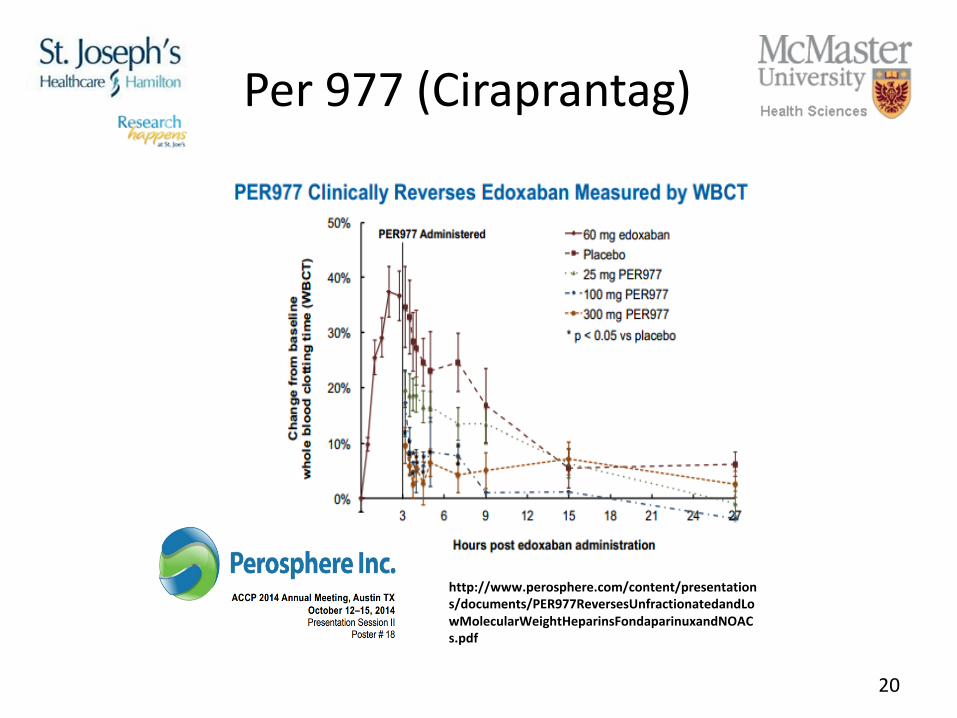
Per977(Ciraprantag)
20
http://www.perosphere.com/content/presentations/documents/PER977ReversesUnfractionatedandLowMolecularWeightHeparinsFondaparinuxandNOACs.pdf
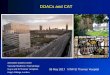
Andexanet(aFXa decoy)
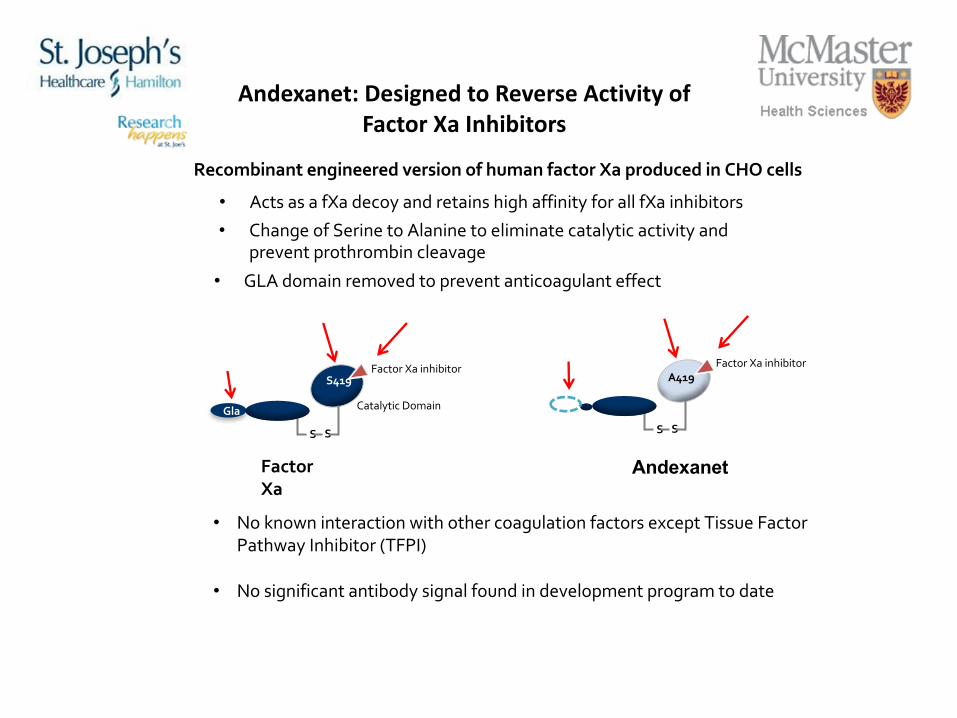
Andexanet:DesignedtoReverseActivityofFactorXa Inhibitors
Factor Xa
Andexanet
Catalytic DomainGla
Recombinant engineered version of human factor Xa produced in CHO cells
S S
S419
S S
A419Factor Xa inhibitor Factor Xa inhibitor
• No known interaction with other coagulation factors except Tissue Factor Pathway Inhibitor (TFPI)
• No significant antibody signal found in development program to date
• Acts as a fXa decoy and retains high affinity for all fXa inhibitors• Change of Serine to Alanine to eliminate catalytic activity and
prevent prothrombin cleavage
• GLA domain removed to prevent anticoagulant effect
Gla
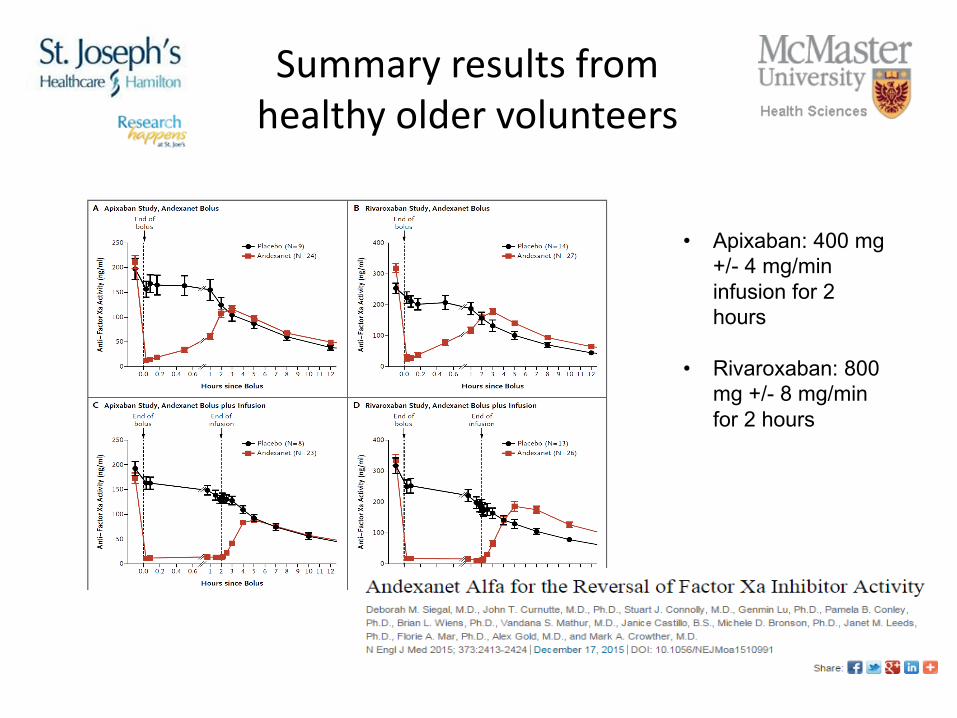
Summaryresultsfromhealthyoldervolunteers
• Apixaban: 400 mg +/- 4 mg/min infusion for 2 hours
• Rivaroxaban: 800 mg +/- 8 mg/min for 2 hours
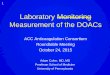
Idarucizumab: a specific reversal agent for dabigatran
24
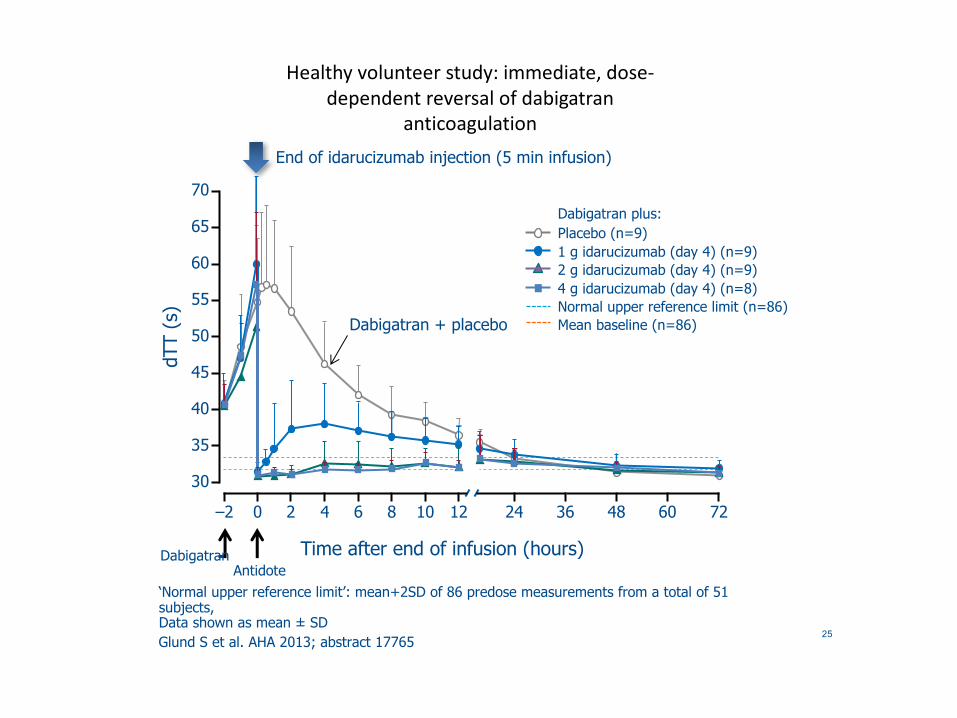
Healthyvolunteerstudy:immediate,dose-dependentreversalofdabigatran
anticoagulation
25
‘Normal upper reference limit’: mean+2SD of 86 predose measurements from a total of 51 subjects, Data shown as mean ± SDGlund S et al. AHA 2013; abstract 17765
Dabigatran plus:Placebo (n=9)1 g idarucizumab (day 4) (n=9)2 g idarucizumab (day 4) (n=9)4 g idarucizumab (day 4) (n=8)Normal upper reference limit (n=86)Mean baseline (n=86)
End of idarucizumab injection (5 min infusion)
Dabigatran + placebo
–2
Time after end of infusion (hours)
dTT
(s)
DabigatranAntidote
70
65
60
55
50
45
40
35
30
0 2 4 6 8 10 12 24 36 48 7260
Reversal
• Majororlifethreateningbleedingshouldleadtotheinitiationofaanticoagulantreversalstrategythatisgeneric
• Thekeycomponentofthisstrategyisinvestigatingandtreatingthecauseofthebleed
• Theavailabilityofhighlyeffective“antidotes”forwarfarinhasnotmitigatedthehighriskofdeathwithwarfarinassociatedbleeding– ImpactofPCCsawaitedwithinterest
• Yourlabislikelytogetcalledandaskedifapatienthasdrugonboardbeforeaveryexpensiveagentisadministered– Inthedabigatranstudyalargefractionofpatientshadnodrugonboard
26