Embed Size (px)
Citation preview

Reversal in mortality trends: evidence from the Agincourt field site, South Africa, 1992- 1995
. . i
Stephen M. Tollman”, Kathleen Kahn”, Michel Garenneb and John S.S. Ceara
i Objective: To examine changes in mortality in rural South Africa over the period 1992-1 995 by age, sex and cause of death.
Design: As with much of sub-Saharan Africa, South Africa lacks effective vital registration and information on mortality is lacking. The Agincourt demographic and health surveillance system was established to inform health policy and practice with regard to rural subdistrict populations.
Methods: Prospective community-based study involving annual update of a household census with enquiry into all birth, death and migration events. All reported deaths (n = 1001) are the subject of a verbal autopsy.
Results: An increasing trend in overall mortality relative to general population growth in the study area is apparent. There is evidence for a reversal in the previously declining trend in mortality among women 20-44 years. A comparison of 1992-1 993 with 1994-1 995 shows that most of the increase in mortality is concentrated in the younger adult (20-49 year) age group. AIDS and related diseases, particularly tuberculosis, appear primarily responsible. Injuries and violence (especially homicide) and circulatory disease are important, under-recognized causes of death, although their levels have remained constant over the period.
Conclusions: Mortality from AIDS and related diseases appears responsible for the probable reversal in mortality emerging in South Africa‘s rural northeast. Findings carry implications for the emerging system of decentralized health care.
O 1999 Lippincott Williams & Wilkins
AIDS 1999 13:1091-1097
Keywords: demographic surveillance, mortality, trends, reversal, AIDS, health reform
Introduction
Lack of vital registration in sub-Saharan Africa has seri- ously compromised the application of mortality data to health planning and practice. Trends in health sector reform away from centralized towards decentralized, usually district-based, health systems accentuate this gap [l]. While global ‘burden of disease’ studies are proving highly influential in shaping intervention and research
priorities at regional and international level [2], they do not remove the critical need for empirically derived data on national and district mortality patterns.
The Agincourt field site was established in 1992 and covers a subdistrict in the Bushbuckridge area of South Africa’s rural northeast, adjacent to its border with Mozambique. Part of the Bushbuckridge district health initiative, the site was established to support the
From the aHealth Systems Development Unit, Department of Community Health, University of the Witwatersrand, Johannesburg, South Africa and the bFrench Centre for Population and Development (CEPED), Paris, France, Sponsorship: This study was supported by the European Union and Kagiso Trust, the Henry J. Kaiser Family Foundation and the Trust for Health Systems Planning and Development. Stephen Tollman was supported by the British Council and a Wellcome Trust Travelling Research Fellowship (049336/Z/96/Z), and Kathleen Kahn by the British Council, during the analysis and write-up of this work. Requests for {eprints to Dr S.M. Tollman, Department of Community Health, Faculty of Health Sciences, University of the Witwatersrand, 7 York Road, Parktown 21 93, Johannesburg, South Africa. Documentaire L ? R S T G ~ ~
cote : ß # - - --__ ~ --- -
I 1 o91
I


a - 4 A
1092 AIDS 1999, Vol 13 No 9 -.
national effort in decentralized health system develop- ment. Demographic and health surveillance in Agincourt provides population-based information to support district health planning and practice, as well as a programme of advanced community-based research ~31.
’ Here we examine changes in mortality over the period 1992-1995 by age, sex and cause of death. Despite the short time period, clear changes can be discerned. They will impact on local health services and have wider implications for South Africa’s new system of decentralized (district-based) health care. The data should also contribute to addressing the substantial gaps in our understanding of mortality in sub-Saharan Africa [4] and South Africa in particular [5].
Methods
Study area South Africa’s apartheid policy resulted in the forced resettlement and concentration of Africans into geo- graphically dispersed and economically inhospitable ‘homelands’. Part of the former Gazankulu area, Agincourt is home to some 63 O00 people, of whom 44% are below the age of 15 and 26% are of Mozambican origin [3]. Given a population density of 148 persons per square kilometre and the low rainfall, there is little opportunity for subsistence agriculture and the area is better suited to cattle or game farming. Opportunities for employment outside the public sec- tor are scarce and labour migration is high, affecting more than half of all men aged 25-59 years. The popu- lation lives in 20 village settlements, most with a pri- mary school that is attended (despite late enrollment) by a majority of children. Only 6% of school-goers complete secondary school. One health centre linked to four satelLite clinics serves the area, with the district hospital some 40 km away.
Fertility and mortality indicators established by surveil- lance [total fertility rate (TFR) = 3.5; life expectancy 65 years] seem to be close to the national average, although more precise comparisons are not possible because of a lack of reliable data at the national level (when available, results fi-om the national census of 1996-1997 and the demographic and health survey 1998 should improve comparative work considerably). More information on the demographic characteristics of the Agincourt population can be found elsewhere [3].
.
Data collection In 1992, all 20 villages of the field site were mapped and a household census conducted [2]. This baseline has been updated approximately annually, including documentation of all special events (births, deaths and
in- and out-migrations). Data is computer-entered using a custom-made data entry program onto an Access database. Analysis to date has used the Microsoft Excel spreadsheet program, statistical packages includ- ing STATA and SYSTAT, and Epiinfo 6.02.
All recorded deaths are the subject of a verbal autopsy during which a questionnaire is administered by a trained, lay fieldworker to the closest caregiver of the deceased. The verbal autopsies are assessed by three medical officers who, blind to each other, use a series of consensus criteria to amve at a diagnosis. Where a diagnosis cannot be reached, the cause of death is described as ‘undetermined’. The verbal autopsy instrument used in Agincourt is an adaptation of that developed in Niakhar, Senegal [6].
The field team comprises local youth, recruited firom villages of the field site, who have completed secondaiy school. Community acceptance of their work, and the repeated process of household visits that this entails, is high and is reinforced by efforts to maintain a stable relationship between the field team and the study community. Regular opportunities for village-level feedback and dialogue, based on survey results, have characterized the project and constitute part of the ‘contract’ between study team and local communities.
Community acceptance of the project, quality checks on a 2% random sample of households, manual checking of data-capture forms, computerized validation routines and repeat visits to households where necessary contribute to the reliability of the census and special events data. A proportion of verbal autopsy diagnoses have been vali- dated against hospital reference diagnoses by calculating the sensitivity, specificity and positive predictive value of each cause of death for which a hospital diagnosis could be found (K. Kahn, S.M. Tollman, M. Garenne, J.S.S. Gear, manuscript submitted).
Three census rounds have resulted in a longitudinal data set covering births, deaths and migrations for the period 1992-1995. Verbal autopsies have been con- ducted on 932 of the total 1001 deaths recorded during this time. No suitable respondent could be found for the outstanding 7% of deaths, largely because of out- migration of family members and sometimes whole households.
Analysis of female mortality During the baseline census in 1992, the survival status of the mothers of all those in the resident population was established as completely as possible. This allowed retrospective study of survival among adult women using indirect demographic methods (matemal orphan- hood technique); this technique estimates adult survivorship from the proportions of respondents not orphaned. The method is based on an equation that relates the female probability of surviving fi-om age x
+
-4

Reversal in mortality trends Tollman et a/. 1093
(e.g. 20 years) to x + rz years to the proportion of respondents (in contiguous age groupings) whose mother was still alive at the time of interview. From the resulting survivorship probabilities, life-table esti- mates can be made [7]. The approach adopted was that described by Timaeus [SI, which improves on the methods of Brass and Hill-Trussell [7] and yields more accurate estimates.
Estimates of maternal survival were converted to esti- mates of the mortality quotient (probability of dying) for women between the ages of 20 and 44 years using United Nations model life tables. From the prospective data (not shown), the general model life table was chosen as closest to the Agincourt situation. In the matemal orphanhood method, the probability of dying estimated fiom the youngest age group of respondents (i.e., the most recent estimate) is virtually insensitive to the choice of model life table. This choice can only affect the slope of t'he trend in the retrospective estimate. The indirect (retrospective) estimates could then be compared with the direct (prospective) life- table estimates of the same quotient (25q20 = the probability of dying between 20 and 44 years of age) derived from the routine demographic and health surveillance system. These estimates are comparable provided that the quality of the data is adequate.
Ethical considerations Community consent and informed consent at individ- ual and household level have been obtained and are integral to the research process. The University of the Witwatersrand's Committee for Research on Human Subjects (Medical) has reviewed and approved the research protocol (No. M 960720).
Results
Detailed analysis of the mortality profile, based on 1001 deaths between 1992 and 1995, provides insight into the cause-of-death pattem. Of note, is the continuing high level of deaths from infectious and nutritional causes among children (diarrhoea and kwashiorkor) ~
coupled with strikingly few deaths from the vaccine- preventable diseases and acute respiratory infections. Notable amongst adults is the high level of circulatory disease among the older middle-aged and young elderly (heart failure and cerebrovascular accidents) and an unexpectedly high level of violent death among young men [9].
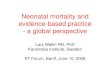
Trends in mortality Figure 1 shows the number of deaths occurring in Agincourt each month during the period June 1992 to July 1995. The observed trend in mortality differs sig- nificantly from the trend that would be expected if
40 -- 35 -_ Obsewed trend
10 Population increase - - 5 o . . . . . . . . . . . . . . . . . . . . I . I . . . I I . I . I 1 I I .
A O D F A J A O D F A J A O D F A J 5.92
Fig. 1. Number of deaths by month in Agincourt, June 1992 to July 1995.
deaths were increasing only because of population growth ( P < 0.038). This finding is independent of population migration and indicates a relative increase in mortality over the three years 1992 to 1995.
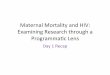
Evidence of a steady, declining trend in adult female mortality for the 4 to 13 years prior to the survey (1979-1988) was found in the analysis of retrospective data (Fig. 2). In contrast, in the period of the prospec- tive study (1992-1995), adult female mortality between 20 and 44 years was sigdicantly higher (25q20 = 61.6 per 1000; P = 0.014) than the most recent indirect esti- mate (43.3 per 1000 in 1984-1985), indicating a recent rise in the mortality of younger female adults. When the earlier trend is taken into account, the prospective estimates are 4.2 times higher than the 1979-1988 trend prolonged to 1992-1995. Even though the value of the slope based on indirect estimates can be questioned, the results suggest a serious reversal in the previously downward trend in mortality among women of reproductive age.
Age and sex patterns of mortality 1992-1 995 Based on data from the prospective study, life tables were prepared for the periods between the censuses: between census 1 and 2 covering 19 months in 1992-1993 and between census 2 and 3 covering 21 months in 1994-1995.
Results show that most of the increase in mortality is concentrated in the 20-49 year age group (Table 1). There was a slight decline in mortality among children under 15 years (not shown). However, in somewhat less than 2 years, the mortality increase at age 20-49 was 23% for both sexes combined, and slightly higher
25Q208 0.0900 0.0800 0,0700 0.0600 0.osw 0.0.100 0,0300 0.0200 nnnin i
Observed @raspocrive) x.
o.CQo0 .I I 1978 1980 1982 1984 1986 1988 1990 1992 1994 1996
Fig. 2. Estimates of female mortality at age 20-24 years at Agincourt. *The probability of dying between 20 and 44 years of age.
. .. :, ;L-:. ' : >. , :. . . / . / . .

1094 AIDS 1999. Vol 13 No 9
Table 1. Changes in adult mortality, by age and sex, Agincourt 1992-1 995.
1992-1 993a 1994-1 995b
Age (years) Quotient' (1) Deaths Quotient' (2) Deaths Relative risk (2/1) P value
Both sexes 20-49 50-74 75-84
Males 20-49 50-74 75-84
Females 20-49 50-74 75-84
0.09751 0.40255 0.51 572
0.1 2342 0.50225 0.51 201
0.07039 0.30415 0.51 834
92 148
59
55 87 26
37 61 33
0.1 1966 0.42224 0.53319
0.15385 0.5021 O 0.60976
0.08384 0.34496 0.47689
127 177
69
79 97 38
48 80 31
1.23 1 .O5 1 .O3
1.25 1 .o0 1.19
1.19 1.13 0.92
0.135 NS NS
0.070 NS NS
0.424 NS NS
aCensus 1 to census 2. bCensus 2 to census 3. 'Quotient: probability of dying within age group.
for males (+25%) than for females (+19%). There was no evidence of mortality increase in the other age groups.
The increase in death rates between the two prospec- tive periods selected (1992-1993 and 1994-1995) was not statistically significant. However, consideriog the significant increasing trend in deaths over the whole period, together with the evidence for a reversal of the previous declining mortality among women aged 20-44 years, the results support a finding of continuous i-ncrease in mortality during the prospective period. This conclusion is reinforced when changes in the cause-of-death pattem are examined.
Cause of death To examine the cause-of-death profile during the period of prospective study (1992-1995), all diagnosed deaths were classified into four main categories: infec- tious and parasitic, non-communicable, accidents and injuries, and undetermined causes. Contrasting 1992-1993 with 1994-1995, there was no major change in the cause-of-death pattem, with the excep- tion of the infectious and parasitic category. Breaking down this category by disease type called attention to AIDS, tuberculosis and chronic diarrhoea, three causes of death that are closely related to HIV infection. In addition, the number of deaths from undetermined causes showed a slight but sustained increase, suggest- ing that some AIDS-related deaths might have presented atypical clinical pattems that were not recog- nized by the verbal autopsies.
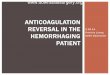
Figure 3 shows the pattern of deaths from AIDS, pul- monary tuberculosis and chronic diarrhoea combined. In the period July1992 to July 1993 there was a declin- ing trend with all but one of the deaths resulting from tuberculosis. The trend reverses thereafter, with deaths resulting fiom AIDS and chronic diarrhoea manifesting in the study area from July 1993 onwards.
Deaths from these causes affect primarily younger adults, and children to a lesser extent (Table 2). AIDS
deaths are concentrated in the middle to younger ages. While in the first period there was only a single AIDS death, an adult woman, there were 20 in the second period, 11 males and nine females. Thirteen were adults 15-49 years, and seven were children under the age of 2 years. Of the children, the youngest died at 4 months, the oldest at 19 months, with an average of 12 months. Adult AIDS deaths ranged from 22 to 47 years, the average being 35 years. The four cases of chronic.diarrhoea were all in the second period and mainly among young children. The increase in tuber- culosis between the two periods (+lo deaths) afZected males and females similarly and was concentrated among younger men and older women.
Death by injury and deaths from non-communicable causes The verbal autopsy analysis reveals violent death (suicide and homicide, especially in young men), accidents (motor vehicle and household accidents) and circulatory disease [cerebrovascular accidents and heart failure among the older middle-aged (50+) and elderly] to be of major public health importance. However, the level of mortality from violent deaths and circulatory disease showed little change over the period 1992-1995. Close examination of homicide deaths does indicate an increase in the number of female deaths 15 years and over, from two to seven. This computes to a relative risk of 3.25, accentuating the issue of physical violence as a threat to women's health and raising the possibility of an increasing trend. The
14 I
0 4 : : : : ; : ; : : : JUL92 JAN93 JUL93 JAN94 JULY4 JAN95
Fig. 3. Deaths caused by AIDS, pulmonary tuberculosis and chronic diarrhoea in Agincourt July 1992 to July 1995. -.

A Y
Reversal in mortality trends Tollman et a/. 1095
Table 2. Number of deathsa from AIDS, tuberculosis and chronic diarrhoea, by age, sex and time period.
Males Females 1992- 1994- 1992- 1994-
Age group (years) 1993b 1995' 1993b 1995'
AIDS 0-1 4 15-49 50+
0-1 4 15-49 50+
0-1 4 15-49 50+
Tuberculosis
Chronic diarrhoea
O 1 O 10 0 . 0
O 1 1 6
14 13
O 2 O O O O
O 6 1 3 O O
1 O 2 2 1 7
O 2 O O O 1
Total 15 33 5 21
aNumbers in the table are small and so should be interpreted with caution. Nevertheless, the changes are largely in .one direction and suggestive of an emerging trend. bCensus 1 to census 2. 'Census 2 to census 3.
circumstances of death range &om domestic violence (n = 3) to accusations of witchcraft (n = 3).
Undetermined causes Combining deaths for both sexes from undetermined causes, the relative risk for the ages 15-49 and 50+ is 1.25 and 1.21, respectively, when the 1994-1995 period is compared with 1992-1993. These figures, in light of the rising .mortality from AIDS and related diseases, may include further AIDS-related deaths that are difficult to diagnose.
Discussion
The results presented cover a relatively short period, 1992 to 1995. Nevertheless, they relate to a time of great social and political change and open a window onto a situation and context for which information on mortality is largely unavailable [4,10-121. The most striking finding is the steep 42% rise in adult female mortality between the mid-1980s and the early 1990s. Evidence for this increase is compelling since it cannot be attributed to the demographic model chosen, is unlikely to be a consequence of defects in the retrospective data (which are consistent over the many age groups considered) and is consistent with other available epidemiological data (see below).
As documented in Zambia and the Ivory Coast [13,14] and comprehensively discussed in Timaeus' recent work based on national surveys and censuses [15], reversals of what was once assumed to be a generally declining trend in mortahty are now recognized in sub- Saharan Africa. Although AIDS and its sequelae are, in many cases, the prime factors responsible, it is important to examine the evidence for other potential
contributors. In Zambia in 1993, persisting levels of poor nutrition, declining access to Westem health ser- vices (affecting rural areas particularly) and short birth intervals have been cited as partial explanatioris for worsening child mortality [13]. In contrast, and despite the impact of the HIV epidemic, infant and child mortality in Uganda as a whole appears to have fallen during the early 1990s', very likely as a result of effective child health interventions [15]. The Agincourt evidence to-date highlights rapidly growing AIDS- related mortality, particularly among younger to mid- dle-age adults but also among infants and young children in parts of rural northeastem South Africa.
The significant impact of AIDS-associated mortality on mortality rates in rural Zimbabwe, Tanzania and Uganda has been well documented in a few district or provincial settings [16-191. In rural Tanzania, in a pop- ulation of relatively low HIV prevalence (4%), HIV was shown to increase overall adult mortality by more than 50% over the 2-year period 1991-1992 and 1993-1994 [17]. Similar results were obtained in Masaka district, Uganda over the 1-year period between 1989-1990 and 1990-1991 [19]; while mor- tality hdings between 1990 and 1991 &om the higher Sero-prevalence Rakai district complement these results and show a gradation of population attributable risk from a level of 83% in high-prevalence trading centres (HIV prevalence of 35%), to 59% in intermediate trad- ing villages, to 48% in lower prevalence (11.8%) rural villages [18] (the last being consistent with findings from nearby Masaka as well as &om Mwanza in north- west Tanzania).
This picture derives from empirical work, often prospective community studies, seeking to establish the extent of AIDS-related mortality, and rates of infection, at different stages of the HIV epidemic. In South Africa, despite the extent and impact of HIV/AIDS, as evidenced by antenatal clinic studies and data on hospital patient mix [20], little empirical work on the evolving mortality impact of the epidemic is available. As a middle-income country somewhat further along the demographic transition than other countries of southern and east Africa, it is useful to be able consider the mortality impact of AIDS in a broader context of overall adult and child mortality.
AIDS and related diseases (in particular tuberculosis) and homicide, affecting both men and women, can be identified as critical emerging health problems in the Agincourt subdistrict. However, attention to these emerging concems must be balanced against the major burden of illness posed by long-standing pioblems (diarrhoea and kwashiorkor in children) and the weakly recognized contribution of circulatory disease in adults.
Data reliability and validity can be assessed by compari- son with other sources of data. The demographic finding
. . . . 3@%?--:' . ,. i . .. .. . '!
. .

1096 AIDS 1999, Vol 13 No 9
of increasing mortality is consistent with the epidemio- logical data available. Progression of the AIDS epi- demic in South Africa has been well documented, primarily in urban settings [21,22] but also with consid- eration for the mode of spread into rural populations. Recent estimates of HIV seroprevalence amongst ante- natal clinic attenders in the public sector show a steady increase nationwide, with a figure of 17.7% for this part of South Aitiica in 1996 [23].
Projections of overall mortality based on the Metropolitan/Doyle model for this part of northeastern South Africa (Mpumalanga and Northern Province) show rapidly rising mortality among both sexes that does not plateau by the year 2010 (projections made by T. Miihr, Metropolitan Life Insurance, South Africa). In the age group 15-59 years, overall female mortality, while clearly lower than male mortality up until the year 2000, begins to exceed that of males from the year 2005. When the ‘best estimates’ for adults aged 15-59 years in Mpumalanga are contrasted with Agincourt findings for the same age group, there is a marked difference, the Agincourt results being approximately half those estimated for men and women in Mpumalanga in 1995 (and closer to estimates for the late 1980s). The higher male mortality rates are, how- ever, also found in Agincourt. The difference does not nedessarily mean that the projections are flawed (although our understanding of fertility levels makes it possible that the model’s assumptions regarding prevail- ing fertilty rates are overestimates); rather, the Agincourt findings may more closely approximate the Northern Province situation (regarded as 4-5 years behind the Mpumalanga epidemic). The contrast does, however, highlight that the HIV/AIDS epidemic in Agincourt is at an earlier stage, with a window of opportunity still open for concerted action.
Verbal autopsy interviews were assessed in the same way throughout the study, with assessing medical officers unaware that the earlier and later periods were to be compared. Validation of 127 adequately documented verbal autopsies, involving comparison with hospital reference diagnoses, showed relatively high sensitivity (82%) and specificity (93%) for infec- tious and parasitic diseases overall. For pulmonary tuberculosis alone, the sensitivity was 92% and speci- ficity 99%, while for diarrhoea these were 83% and 99%, respectively. Numbers of hospital deaths from AIRS were too low to permit such calculations (K. Kahn, S.M. Tollman, M. Garenne, J.S.S. Gear, manuscript submitted).
It is essential to locate the evolving pattern of mortality within the context of change in South African health care. The country is moving rapidly towards a decen- tralized health system involving the devolution of resources and authority to the district level [24,25]. If
.
the Agincourt findings are sustained, the brunt of responsibility for coping with the added - and chang- ing - disease burden will fall onto local and district health services and their associated communities. In anticipation, there are important initiatives that can be taken. These include drawing on lessons and experi- ence from elsewhere in Africa and beyond; taking deliberate steps to ensure health personnel have the appropriate skills; strengthening health centre and out- reach services and supporting home-based and other forms of non-institutional care [26]; and introducing demonstration programmes designed to inform the rural public health sector and other public sector groups on a range of feasible and appropriate responses.
South Africa lacks a vital registration system able to cover its rurd population as well as expanding urban centres adequately. However, a number of recent ini- tiatives offer the opportunity to substantially strengthen access to population-based information and, in some cases, to allow national averages to be broken down to provincial and/or district-specific levels. Improving the system of national health statistics will require a coordi- nated effort to link three related activities effectively: (i) the ongoing efforts to further develop the vital registra- tion system [27], which is a vital component of data collection, must be strengthened; (ii) the three existing fieldsites based on demographic and health surveillance should be linked and coupled with strategic development of additional field and/or facility-based surveillance sites [28,29] (In addition to Agincourt there are 11 Hlabisa fieldsites in northern Kwazulu- Natal, part of the University of Natal, University of Rurban-Westville and Medical Research Council’s Wellcome Africa Centre; and the Dikgale site just out- side Pietersburg in the Northern Province, University of the North.); and (iii) the just-introduced annual national household survey. The cost implications, when weighed against the substantial investments already committed, may well not be excessive. In the longer run, however, developing a nationwide comprehensive vital registration system is imperative to support the country’s emerging local government and decentraliz- ing health system.
Acknowledgements
This work could not have been conducted without the active support of community leadership, the willing participation of community members, and the interest of health providers to respond to findings. We acknowledge the role of Obed Mokoena, Susan Khosa and the field team; Marc Pienaar, Kobus Herbst and Julia Moorman; and the Northern Province Health Department. Thanks to Ian Timaeus for his contribu- tion to estimating the trend in female mortality, and to *
-*
..: ><: .. . .. . . . , .
I ,: , . ..,:..,:>y, . . . . . . .

Reversal in mortality trends Tollman et a/.
two anonymous reviewers for their helpful comments. We are indebted to Thomas Mühr of AIDS Research at Metropolitan Life Insurance, South Afkica for mak- ing available projections of overall mortality for Mpumalanga and Northem Province.
References 1.
2.
3.
4.
5.
6.
7.
8.
9.
1 o.
I I .
12.
13.
Cassels A. Health sector reform: key issues in less developed countries. 1 Int Devel 1995;7329-347. WHO. Investing in health research and development. Report of the Ad Hoc Committee on Health Research relating to future intervention options. Geneva: World Health Organization; 1996. Tollman S, Herbst K, Garenne M. The Agincourt Demographic and Health Study: Phase 7. Health Systems Development Unit, Department of Community Health, University of the Witwatersrand, Johannesburg; August 1995. Timaeus I. Adult mortality. In Demographic change in Sub- Saharan Africa. Edited by Foote KA, Hill KH, Martin LG. Washington, DC: National Academy Press; 1993:218-255. Bradshaw D, Laubscher R, Schneider M. Estimated cause of death profiles for nine new provinces based on 7990 data. CERSA, MRC South Africa, Cape Town; February 1995. Garenne M, Fontaine O. Assessing probable causes of death using a standardized questionnaire: a study in rural Senegal. In Measurement and Analysis of Mortality: New Approaches. Edited by Vallin J, D'Souza S, Palloni A. Oxford: Clarendon Press; 1990:123-142. Department of International Economic and Social Affairs. Population Studies, No. 81 : Manual X. lndirect Techniques for Demographic Estimation. New York: United Nations; 1983. Timaeus IM. Estimation of adult mortality from paternal orphanhood: a reassessment and a new approach. Pop Bull
Kahn K, Tollman SM, Garenne M, Gear JSS. "Who dies from what": determining cause of death in South Africa's rural northeast. Tropical Medicine and International Health (in press). Herman AAB, Wyndham CH. Changes in infant mortality rates among whites, coloureds and urban blacks in the RSA over the period 1970-1983. SAfr Medl 1985;68:215-218. Bradshaw D, Dorrington RE, Sitas F. The level of mo,rtality in South Africa in 1985 -what does it tell us about health? S Afr Medl 1992;82:237-240. Chimere-Dan O. Demographic patterns. In South African Health Review 7995:Durban: Health Systems Trust and the Henry J. Kaiser Family Foundation; 1995: 3-15. Gaisie K, Cross AR, Nsemukila G. Zambia Demographic and Health Survey 7992. Columbia, MD: Macro International for
UN 1992;33:47-63.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
27.
2a
29
University of Zambia and Central Statistical Office, Zambia; 1993. Garenne ML, Madison M, Tarantola D, et al. Mortality impact of AIDS in Abidjan, 1986-1992. AlDS 1996;10:1279-1286., Timaeus IM. Impact of the HIV epidemic on mortality in sub- Saharan Africa: evidence from national surveys and censuses.
Gregson 5, Anderson RM, Ndlovu I, Zhuwau T, Chandiwana SK. Recent upturn in mortality in rural Zimbabwe: evidence for an early demographic impact of HIV-1 infection? AIDS
Todd J, Balira R, Grosskurth H, et al. HIV-associated adult mor- tality in a rural Tanzanian population. AIDS 1997;11:801-807. Sewankambo NK, Wawer MJ, Gray RH, et al. Demographic impact of HIV infection in rural Rakai District, Uganda: results of a population-based cohort study. AIDS
Mulder DW, Nunn Al, Wagner HU, Kamali A, Kengeya-Kayondo JF. HIV-1 incidence and HIV-1 associated mortality in a rural Ugandan population cohort. ADS 1994;8:87-92. Kinghorn A, Steinberg M. HIVIAIDS in South Africa: The impacts and the priorities. Pretoria: HlV Management Services/Department of Health, South Africa; 1998. Schoub BD. Estimations of the total size of the HIV and hepatitis B epidemics in South Africa. S Afr Med
Jochelson K, Mothibeli M, Leger JP. Human immunodeficiency virus and migrant labour in South Africa. lnt Health Services
Department of Health, South Africa. Seventh national HIVsurvey of women attending antenatal clinics of the public health services, October/November 1996. Pretoria; Department of Health; 1997. Department of Health, National District Health Systems Committee. A policy for the development of a district health sys- tem for South Africa. Pretoria: Health Policy Coordinating Unit and Department of Health; 1995. Tollman 5, Rispe1 L. Organisation, planning and management. In South African Health Review 7995. Durban: Health Systems Trust and the Henry J. Kaiser Family Foundation; 1995: 75-88. Schopper D, Walley J. Care for AIDS patients in developing countries: a review. AlDS Care 1992;4:89-102. Wood K, Jewkes R. Opportunities and threats in proposed changes to birth and death registration. S Afr Med
Sitas F, Zwarenstein M, Yach D, Bradshaw D. A national sen- tinel surveillance network for the measurement of ill-health in South Africa: a prerequisite for epidemiological research and health planning. SAfr Medl 1994;84:91-94. Morse SS, Rosenberg BH, Woodall J, for ProMED Steering Committee Drafting Subgroup. ProMED Global monitoring of emerging diseases: design for a demonstration program. Health Policy 1996;38:135-153.
AIDS 1998;12(S~ppl. 1):SI 5-527.
1997;11:1269-1280.
1994;8:1707-1713.
1992;81:63-66.
1991 ;21:157-173.
1998;88:28-29.
~~ '9
1097

'I O W Introduction of H N drug-resistance testing in clinical practice R. Rodriguez-Rosodo, C. Briones and V. Soriano
CONCISE COMMUNKATON 'B O1 S CD4 T cells remain the major source of HIV-1 during end stage disease M.E. van der Ende, M. Schulten, B. Roschdorff, G. Großschupff, P. Raa, A.D.M.E. Osterhous and K. Tenner-Rau
3 Q2r The C domain of HN-1 qp41 binds the putative cellular receptor protein P62 Y-H. Chen, Y. Xioo, W. Wu, J. Yang, S. Sui and M.P. Dierich
5 Q95 Protection against parenteral HN-1 infection b homozygous deletion in the C-C chemoLne receptor 5 gene B. Kupfer, R. Koiser, H.H. Broch", W. Effenberger, J.K. Rocktroh, B. Motz ond K.E. Schneweir
1029 HIV-specific cytotoxi~ T lymphocyte precursors exkt in a CD28-CD8+ T cell subset and increase with loss of CD4 T cells D.E. Lewis, L. Yang. W. Luo, X.p. Wang, and1.R. Rodgers
IQ83 Rates of HN-1 transmission within marriage in rural Uganda in relation to the H N sem-stabs of the partners L.M. Carpenler, A. Komoli, A. Ruberontwori, S.S. Molombo and J.A.G. Whitworth
II O811 Reversal in mortality hnds: evidence from the Agincourt field site, South Africa, 1992- 1995 S.M. Tollmon, K. Kahn, M. Garenne and J.S.S. G w r
3 a99 The value of w-ent-reported adherence tu antiretraviral thera y in predicting virologic and immunol$gic response R.H. Houbrich, SJ. Little, J.S. Currier, D.N. Forthol, C.A. Kemper, G.N. Beoll, D. Johnson, M.P. Dubé, J.Y. Hwang, J.A. McCutchon ond the California Colloborative Treolment Group
9 309 The im act of the 1993 AIDS case definition on $e completeness and timeliness of AIDS surveillance S.K. Schwarcr, L.C. Hsu, M.K. Poriri ond M.H. Kak
S It 3 5 Cost effectiveness of highly active antiretmviral therapy in HIV-infected patients P.P. Sendi, H.C. Bucher, T. Ham, B.A. Croig, M. Schwietert, D. Pfluger, A. Gofni and M. Boftegoy for the Swiss HIV Cohort Siudy
5035 Joint effects of HN-1 RNA levels and CD4 lymphocyte cells on the r isk of specific opportunistic infections P.L. Willioms, J.S. Currier ond S. Swindells
li 04s Quantification of inteqrated and total HN-1 DNA after long-tem highly active antirehoviral therapy in HIV-1-infected patients A. Ibónez, T. Puig, J. Elios, B. Clotet, L. Ruiz and &A. Martinez
3 CBSl Time caurse of cerebrospinal fluid responses tci antiretraviral therapy. evidence for variable comparhnentalization of infedion S. Stopranr, N. Marlowe, D. Glidden, T. Novakovic-Agopion, R.M. Grant, M. Heyer, F. Aweeko, S. Deekr and R.W. Price
P ab3 Treahnent of visceral leishmaniasis in HIV-infected patients a randomized m'al com arin meglumine antimoniak with amptotezcin B F. Loguno. R López-VQlez, F. Pulido, A. Solos, J. Torrecisneros, E. Torres, F.J. Medrono, J. Som, G. Picó, J. Gómez-Rodriga, J. Porquou and J. Alvor, for the Spanish HIVieishmonio Study Group
P I29 The quali communicahon a k u f end-of-life care: a study of patients with advanced AID5 and their primary care clinicians J.R. Curtis, D.L. Patrick, E. Caldwell, H. Greenlee ond A.C. Collier
of patient-d-doctor
1 133 Motherto-child transmission of HIV-I: the 'all mucosal' hypothesis as a predominant mechanism of transmission P. Von de Perre
CORRESPONDENCE
Meetings Guidance for authors Fast Track 'submission form
Listed inside
dq4 LlPPlNCOlT WILLIAMS OWILKINS 7
CONCISE COMMUNICATION 1811 BK virus as the cause of
ISS^ 0-267- q3W meningoencephalitis, retinitis and nephritis in a patient w'hh AIDS G. Bron, A.L. Hommorin, M. Grandien, B.G. Hedquist, I. Nennermo, B. Sundelin and S. Seregard
8 OFF T cell changes after combined nucleoside analogue therapy in H N primary infection G. Corceloin, C. Blanc, J. Leibowitch, P. Mariol, D. Mother. V. Schneider, A.G. Saimot, F. Damond. F. Simon, P. Debré, B. Autron and P.M. Girard