Embed Size (px)
Citation preview

1
Diabetes mellitus (DM) is a rapidly expanding global pan-demic, affecting over 350 million people worldwide.1,2
DM is also one of the most important risk factors for coronary artery disease (CAD), and 40% of patients with acute coro-nary syndrome (ACS) have DM.3–5 Among patients presenting
with an ACS, patients with DM are at least 80% more likely than patients without DM to have multivessel CAD on angiography.6,7
Current American College of Cardiology Foundation/American Heart Association guidelines recommend coronary
Background—Current guidelines recommend surgical revascularization (coronary artery bypass graft [CABG]) over percutaneous coronary intervention (PCI) in patients with diabetes mellitus and multivessel coronary artery disease. Few data are available describing revascularization patterns among these patients in the setting of non–ST-segment–elevation myocardial infarction.
Methods and Results—Using Acute Coronary Treatment and Intervention Outcomes Network Registry–Get with the Guidelines (ACTION Registry–GWTG), we compared the in-hospital use of different revascularization strategies (PCI versus CABG versus no revascularization) in diabetes mellitus patients with non–ST-segment–elevation myocardial infarction who had angiography, demonstrating multivessel coronary artery disease between July 2008 and December 2014. Factors associated with use of CABG versus PCI were identified using logistic multivariable regression analyses. A total of 29 769 patients from 539 hospitals were included in the study, of which 10 852 (36.4%) were treated with CABG, 13 760 (46.2%) were treated with PCI, and 5157 (17.3%) were treated without revascularization. The overall use of revascularization increased over the study period with an increase in the proportion undergoing PCI (45% to 48.9%; P
trend=0.0002) and no change in the proportion
undergoing CABG (36.1% to 34.7%; ptrend
=0.88). There was significant variability between participating hospitals in the use of PCI and CABG (range: 22%–100%; 0%–78%, respectively; P value <0.0001 for both). Patient-level, but not hospital-level, characteristics were statistically associated with the use of PCI versus CABG, including anatomic severity of the disease, early treatment of adenosine diphosphate receptor antagonists at presentation, older age, female sex, and history of heart failure.
Conclusions—Among patients with diabetes mellitus and multivessel coronary artery disease presenting with non–ST-segment–elevation myocardial infarction, only one third undergo CABG during the index admission. Furthermore, the use of PCI, but not CABG, increased modestly over the past 6 years. (Circ Cardiovasc Qual Outcomes. 2016;9:00-00. DOI: 10.1161/CIRCOUTCOMES.115.002084.)
Key Words: coronary artery bypass graft surgery ◼ diabetes mellitus ◼ myocardial infarction ◼ non–ST-segment elevation acute coronary syndrome ◼ percutaneous coronary intervention
© 2016 American Heart Association, Inc.
Circ Cardiovasc Qual Outcomes is available at http://circoutcomes.ahajournals.org DOI: 10.1161/CIRCOUTCOMES.115.002084
Received June 13, 2015; accepted March 21, 2016.From the Department of Internal Medicine, Division of Cardiology, UT Southwestern Medical Center, Dallas, TX (A.P., D.K.M., J.A.d.L., S.R.D.,
J.D.B., E.S.B., S.B., S.P.M., D.J.K.); Veterans Affairs North Texas Health Care System, Dallas, TX (E.S.B., S.B.); Division of Cardiology, Mayo Clinic, Rochester, MN (G.W.B.); Department of Medicine, Division of Cardiology, Duke Clinical Research Institute, Durham, NC (D.N.S., M.R.); Department of Medicine, Division of Cardiology, Emory University School of Medicine, Atlanta, GA (A.G.); Department of Medicine, Saint Luke’s Mid America Heart Institute and University of Missouri-Kansas City, Kansas City, MO (M.K.); and Department of Internal Medicine, University of California Davis, Sacramento, CA (E.A.A.).
The Data Supplement is available at http://circoutcomes.ahajournals.org/lookup/suppl/doi:10.1161/CIRCOUTCOMES.115.002084/-/DC1.Correspondence to Dharam J. Kumbhani, MD, SM, UT Southwestern Medical Center, 5323 Harry Hines Blvd, Dallas, TX 75390. E-mail dharam@
post.harvard.edu
Revascularization Trends in Patients With Diabetes Mellitus and Multivessel Coronary Artery Disease Presenting With
Non–ST Elevation Myocardial InfarctionInsights From the National Cardiovascular Data Registry Acute Coronary
Treatment and Intervention Outcomes Network Registry–Get with the Guidelines (NCDR ACTION Registry–GWTG)
Ambarish Pandey, MD; Darren K. McGuire, MD, MHSc; James A. de Lemos, MD; Sandeep R. Das, MD, MPH; Jarett D. Berry, MD, MS; Emmanouil S. Brilakis, MD, PhD;
Subhash Banerjee, MD; Steven P. Marso, MD; Gregory W. Barsness, MD; DaJuanicia N. Simon, MS; Matthew Roe, MD; Abhinav Goyal, MD, MHS;
Mikhail Kosiborod, MD; Ezra A. Amsterdam, MD; Dharam J. Kumbhani, MD, SM
Original Article
by guest on July 12, 2018http://circoutcom
es.ahajournals.org/D
ownloaded from
by guest on July 12, 2018
http://circoutcomes.ahajournals.org/
Dow
nloaded from
by guest on July 12, 2018http://circoutcom
es.ahajournals.org/D
ownloaded from
by guest on July 12, 2018
http://circoutcomes.ahajournals.org/
Dow
nloaded from
by guest on July 12, 2018http://circoutcom
es.ahajournals.org/D
ownloaded from
by guest on July 12, 2018
http://circoutcomes.ahajournals.org/
Dow
nloaded from

2 Circ Cardiovasc Qual Outcomes May 2016
artery bypass graft (CABG) over percutaneous coronary inter-vention (PCI) as the preferred revascularization strategy in patients with multivessel CAD and DM (Class IIA).8 These recommendations are based largely on randomized control trials enrolling patients with stable CAD.9–13 However, in a subgroup analysis of the Future Revascularization Evaluation in Patients with Diabetes Mellitus: Optimal Management of Multivessel Disease (FREEDOM) trial, in which approxi-mately one third of the cohort (n=583) was enrolled after an ACS event, the superiority of CABG in the ACS subset was comparable to the overall trial population.11
Despite the guideline recommendations favoring CABG, previous studies have identified an implementation gap between the available evidence base and routine medical prac-tice in patients with DM, with at least 1 in 4 eligible patients with multivessel CAD receiving PCI instead of CABG.14 In addition, revascularization decisions in patients present-ing with non–ST-segment–elevation myocardial infarction (NSTEMI) may be different than patients with stable CAD. A previous study from the Can Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes With Early Implementation of the ACC/AHA Guidelines (CRUSADE) Quality Improvement Initiative reported greater use of PCI as compared with CABG among NSTEMI patients with multivessel disease in the early 2000s.15 However, contemporary trends in revascularization among the high-risk subset of participants with multivessel CAD and type 2 DM are not known. Accordingly, we used the National Cardiovascular Data Registry (NCDR) Acute Coronary
Treatment and Intervention Outcomes Network Registry–Get with the Guidelines (ACTION Registry–GWTG) database to study temporal trends and hospital-level variation in perfor-mance of CABG and PCI among DM patients with NSTEMI and angiography, demonstrating multivessel CAD. We also sought to determine the major clinical factors associated with use of PCI compared with CABG.
MethodsData SourceThe present study was performed using data obtained from the NCDR ACTION Registry-GWTG, a large national quality improve-ment registry that focuses exclusively on patients presenting with an acute myocardial infarction. Details of the ACTION Registry-GWTG have been previously described.16 The registry uses trained hospital personnel from >1000 participating centers across the United States to collect data from medical records using a standardized data set with written definitions (https://www.ncdr.com/webncdr/action/home/datacollection). Abstracted data include patient demographics, clinical information, medical therapies, use and timing of cardiac pro-cedures, and in-hospital outcomes. The registry has requirements in place to ensure uniform data entry and transmission and is subject to data quality checks (www.ncdr.com). Because all data are abstracted retrospectively and anonymously without unique patient identifiers, institutional review boards by policy waive the need for informed consent.
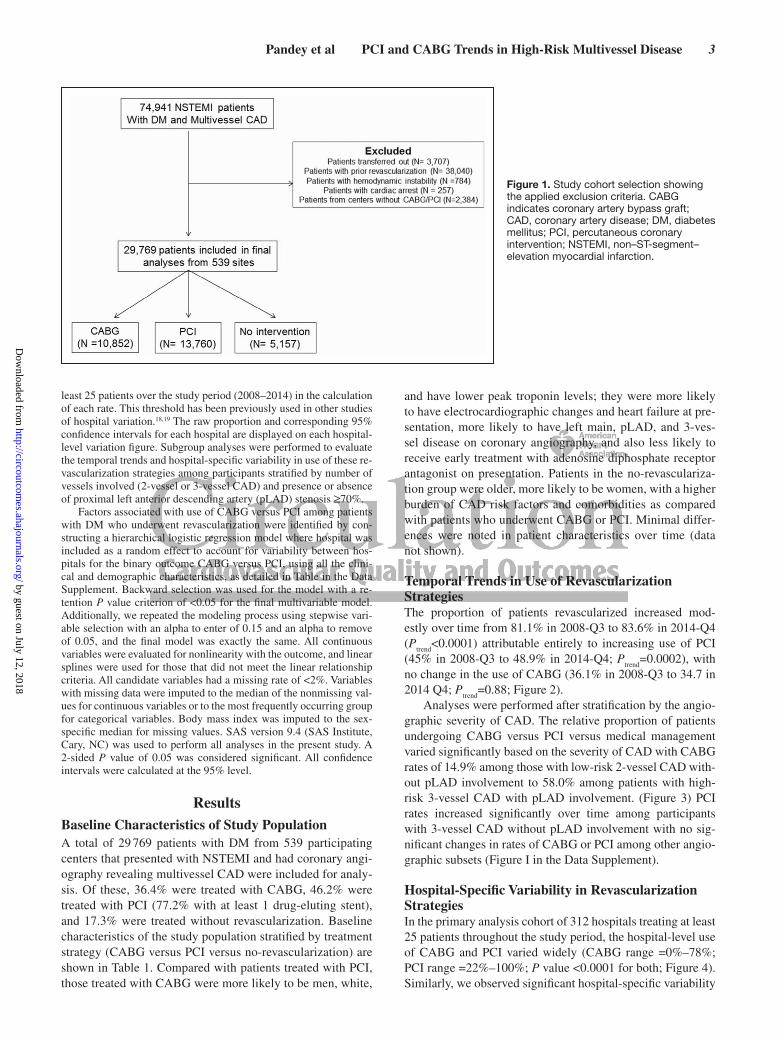
Study PopulationFor the present study, we included DM patients who presented with NSTEMI between July 2008 and December 2014 and had angiog-raphy demonstrating multivessel CAD (n=74 941). Major exclusion criteria included transfer out of the presenting hospital for further management (n=3707), prior history of revascularization (n=38 040), hemodynamic instability or cardiac arrest at presentation (n=1041), and presentation to centers lacking CABG and PCI capabilities (n=2384; Figure 1). The final study population included 29 769 pa-tients from 539 hospitals. Prevalent DM was defined as a documented medical history of DM. Multivessel obstructive disease was defined as ≥50% stenosis in left main artery or ≥70% stenosis in ≥2 separate epicardial coronary artery territories. This definition of multivessel obstructive disease is consistent with that used in the FREEDOM trial.11
Statistical AnalysisPatients were categorized into 3 groups: CABG versus PCI versus no-revascularization. Approximately 2% of patients received both CABG and PCI and were classified as being treated with CABG. Baseline characteristics and in-hospital treatment and discharge med-ications were compared across the 3 groups using the χ2 test for cat-egorical variables and Kruskal–Wallis test for continuous variables. The Kruskal–Wallis test was used rather than other procedures, such as the ANOVA test, for means because the test is a legitimate test in the presence of normality as well as non-normality. Consistency of a single test across continuous variables was preferred. The differences in proportional use of different management strategies (CABG versus PCI versus no revascularization) in the primary analysis cohort dur-ing each quarter (Q) of the analysis time period (Q3 2008 to Q4 2014) were presented for each quarter, and the test for a linear trend among each treatment strategy was obtained by modeling quarter of patient hospital arrival as an ordinal independent variable using logistic regression. Hierarchical logistic regression modeling with hospital-specific random intercepts was used to test whether the CABG and PCI rates were different between hospitals. This strategy describes the true signal variation in the proportion of patients who receive CABG or PCI while removing the effect of random sample varia-tion.17 Because the range in rate would vary greatly between hospitals with too few patients, this analysis was restricted to hospitals with at
WHAT IS KNOWN
• Coronary artery bypass graft (CABG) is associated with better outcomes among patients with diabetes mellitus and multivessel coronary artery disease as compared with percutaneous coronary intervention (PCI).
• However, most of the studies comparing CABG versus PCI in this patient population have predomi-nantly included patients with stable coronary artery disease, and the optimal revascularization strategy among these patients in the setting of an acute coro-nary syndrome presentation is not known.
WHAT THE STUDY ADDS
• Only one third of these high-risk patients undergo CABG during index hospitalization as compared with almost one half undergoing PCI.
• PCI use has increased modestly over time in such patients with no change in the proportion undergo-ing CABG, with practice patterns significantly influ-enced by the anatomic disease severity.
• There are marked variations in the proportional use of CABG and PCI among participating hospitals, suggesting that local practice patterns play an impor-tant role in selection of optimal revascularization strategy in this patient population.
by guest on July 12, 2018http://circoutcom
es.ahajournals.org/D
ownloaded from
Pandey et al PCI and CABG Trends in High-Risk Multivessel Disease 3
least 25 patients over the study period (2008–2014) in the calculation of each rate. This threshold has been previously used in other studies of hospital variation.18,19 The raw proportion and corresponding 95% confidence intervals for each hospital are displayed on each hospital-level variation figure. Subgroup analyses were performed to evaluate the temporal trends and hospital-specific variability in use of these re-vascularization strategies among participants stratified by number of vessels involved (2-vessel or 3-vessel CAD) and presence or absence of proximal left anterior descending artery (pLAD) stenosis ≥70%.
Factors associated with use of CABG versus PCI among patients with DM who underwent revascularization were identified by con-structing a hierarchical logistic regression model where hospital was included as a random effect to account for variability between hos-pitals for the binary outcome CABG versus PCI, using all the clini-cal and demographic characteristics, as detailed in Table in the Data Supplement. Backward selection was used for the model with a re-tention P value criterion of <0.05 for the final multivariable model. Additionally, we repeated the modeling process using stepwise vari-able selection with an alpha to enter of 0.15 and an alpha to remove of 0.05, and the final model was exactly the same. All continuous variables were evaluated for nonlinearity with the outcome, and linear splines were used for those that did not meet the linear relationship criteria. All candidate variables had a missing rate of <2%. Variables with missing data were imputed to the median of the nonmissing val-ues for continuous variables or to the most frequently occurring group for categorical variables. Body mass index was imputed to the sex-specific median for missing values. SAS version 9.4 (SAS Institute, Cary, NC) was used to perform all analyses in the present study. A 2-sided P value of 0.05 was considered significant. All confidence intervals were calculated at the 95% level.
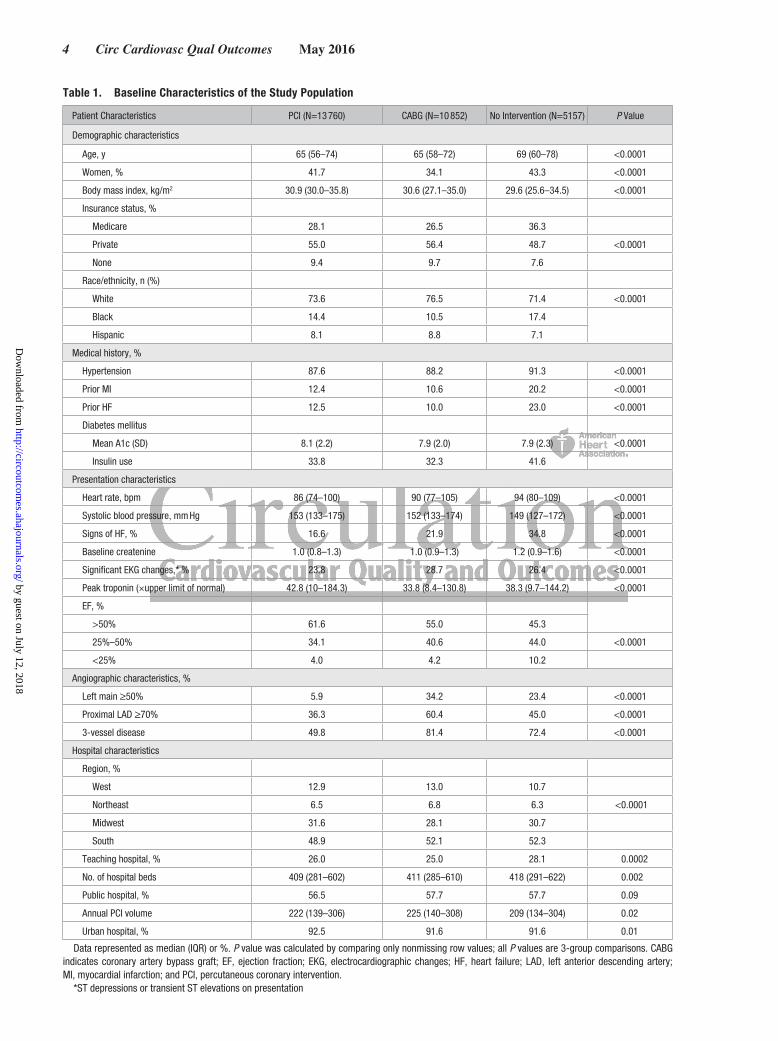
ResultsBaseline Characteristics of Study PopulationA total of 29 769 patients with DM from 539 participating centers that presented with NSTEMI and had coronary angi-ography revealing multivessel CAD were included for analy-sis. Of these, 36.4% were treated with CABG, 46.2% were treated with PCI (77.2% with at least 1 drug-eluting stent), and 17.3% were treated without revascularization. Baseline characteristics of the study population stratified by treatment strategy (CABG versus PCI versus no-revascularization) are shown in Table 1. Compared with patients treated with PCI, those treated with CABG were more likely to be men, white,
and have lower peak troponin levels; they were more likely to have electrocardiographic changes and heart failure at pre-sentation, more likely to have left main, pLAD, and 3-ves-sel disease on coronary angiography, and also less likely to receive early treatment with adenosine diphosphate receptor antagonist on presentation. Patients in the no-revasculariza-tion group were older, more likely to be women, with a higher burden of CAD risk factors and comorbidities as compared with patients who underwent CABG or PCI. Minimal differ-ences were noted in patient characteristics over time (data not shown).
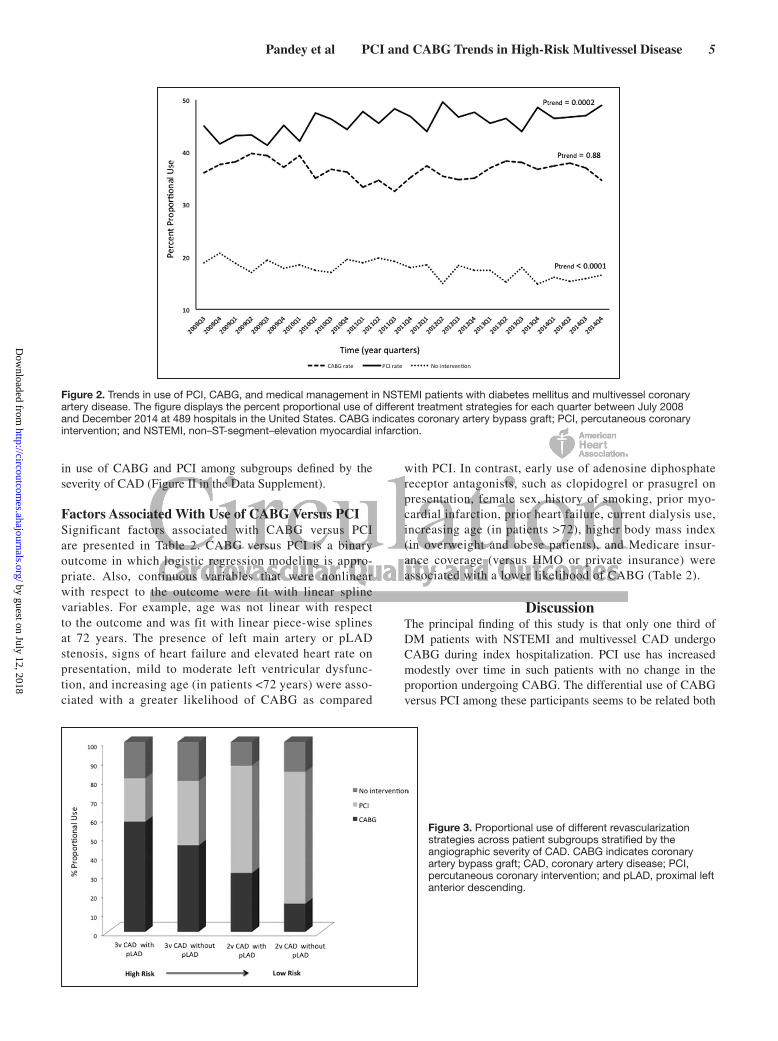
Temporal Trends in Use of Revascularization StrategiesThe proportion of patients revascularized increased mod-estly over time from 81.1% in 2008-Q3 to 83.6% in 2014-Q4 (P
trend<0.0001) attributable entirely to increasing use of PCI
(45% in 2008-Q3 to 48.9% in 2014-Q4; Ptrend
=0.0002), with no change in the use of CABG (36.1% in 2008-Q3 to 34.7 in 2014 Q4; P
trend=0.88; Figure 2).
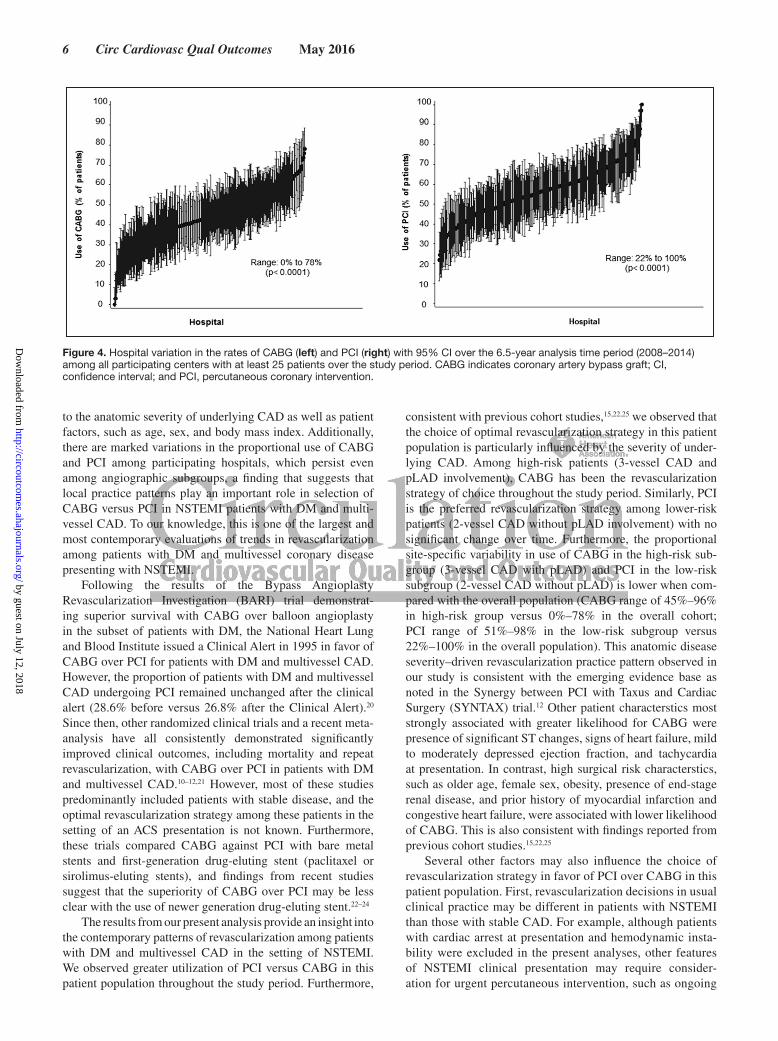
Analyses were performed after stratification by the angio-graphic severity of CAD. The relative proportion of patients undergoing CABG versus PCI versus medical management varied significantly based on the severity of CAD with CABG rates of 14.9% among those with low-risk 2-vessel CAD with-out pLAD involvement to 58.0% among patients with high-risk 3-vessel CAD with pLAD involvement. (Figure 3) PCI rates increased significantly over time among participants with 3-vessel CAD without pLAD involvement with no sig-nificant changes in rates of CABG or PCI among other angio-graphic subsets (Figure I in the Data Supplement).
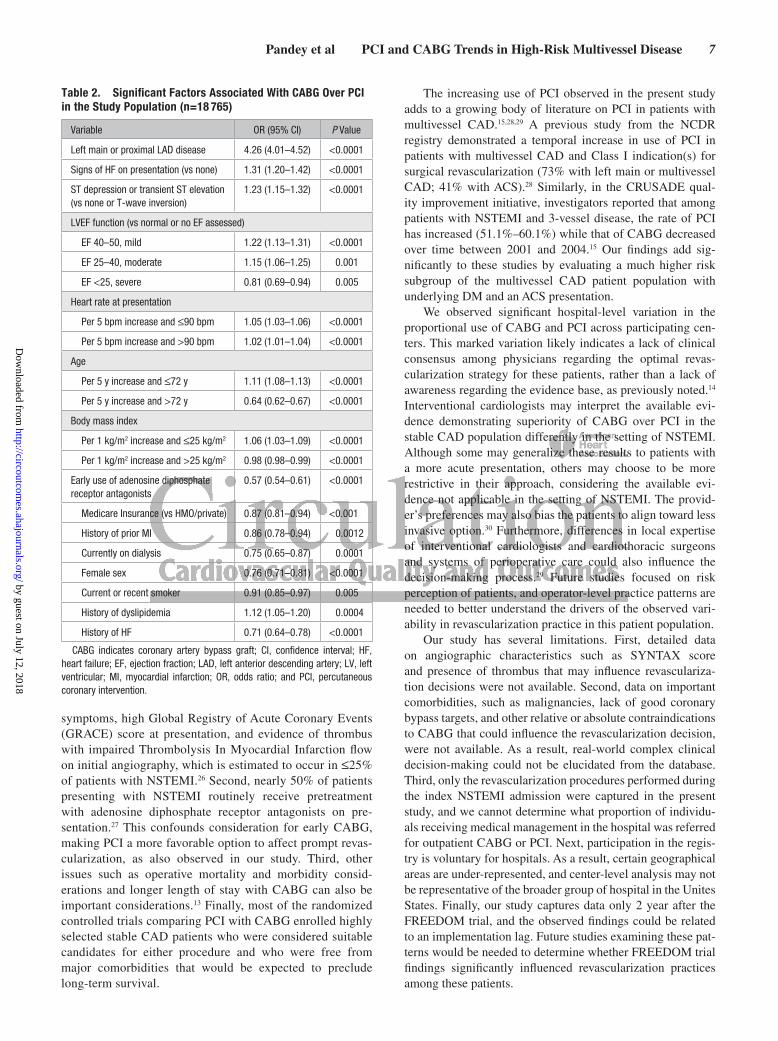
Hospital-Specific Variability in Revascularization StrategiesIn the primary analysis cohort of 312 hospitals treating at least 25 patients throughout the study period, the hospital-level use of CABG and PCI varied widely (CABG range =0%–78%; PCI range =22%–100%; P value <0.0001 for both; Figure 4). Similarly, we observed significant hospital-specific variability
Figure 1. Study cohort selection showing the applied exclusion criteria. CABG indicates coronary artery bypass graft; CAD, coronary artery disease; DM, diabetes mellitus; PCI, percutaneous coronary intervention; NSTEMI, non–ST-segment–elevation myocardial infarction.
by guest on July 12, 2018http://circoutcom
es.ahajournals.org/D
ownloaded from
4 Circ Cardiovasc Qual Outcomes May 2016
Table 1. Baseline Characteristics of the Study Population
Patient Characteristics PCI (N=13 760) CABG (N=10 852) No Intervention (N=5157) P Value
Demographic characteristics
Age, y 65 (56–74) 65 (58–72) 69 (60–78) <0.0001
Women, % 41.7 34.1 43.3 <0.0001
Body mass index, kg/m2 30.9 (30.0–35.8) 30.6 (27.1–35.0) 29.6 (25.6–34.5) <0.0001
Insurance status, %
Medicare 28.1 26.5 36.3
Private 55.0 56.4 48.7 <0.0001
None 9.4 9.7 7.6
Race/ethnicity, n (%)
White 73.6 76.5 71.4 <0.0001
Black 14.4 10.5 17.4
Hispanic 8.1 8.8 7.1
Medical history, %
Hypertension 87.6 88.2 91.3 <0.0001
Prior MI 12.4 10.6 20.2 <0.0001
Prior HF 12.5 10.0 23.0 <0.0001
Diabetes mellitus
Mean A1c (SD) 8.1 (2.2) 7.9 (2.0) 7.9 (2.3) <0.0001
Insulin use 33.8 32.3 41.6
Presentation characteristics
Heart rate, bpm 86 (74–100) 90 (77–105) 94 (80–109) <0.0001
Systolic blood pressure, mm Hg 153 (133–175) 152 (133–174) 149 (127–172) <0.0001
Signs of HF, % 16.6 21.9 34.8 <0.0001
Baseline createnine 1.0 (0.8–1.3) 1.0 (0.9–1.3) 1.2 (0.9–1.6) <0.0001
Significant EKG changes,* % 23.8 28.7 26.4 <0.0001
Peak troponin (×upper limit of normal) 42.8 (10–184.3) 33.8 (8.4–130.8) 38.3 (9.7–144.2) <0.0001
EF, %
>50% 61.6 55.0 45.3
25%–50% 34.1 40.6 44.0 <0.0001
<25% 4.0 4.2 10.2
Angiographic characteristics, %
Left main ≥50% 5.9 34.2 23.4 <0.0001
Proximal LAD ≥70% 36.3 60.4 45.0 <0.0001
3-vessel disease 49.8 81.4 72.4 <0.0001
Hospital characteristics
Region, %
West 12.9 13.0 10.7
Northeast 6.5 6.8 6.3 <0.0001
Midwest 31.6 28.1 30.7
South 48.9 52.1 52.3
Teaching hospital, % 26.0 25.0 28.1 0.0002
No. of hospital beds 409 (281–602) 411 (285–610) 418 (291–622) 0.002
Public hospital, % 56.5 57.7 57.7 0.09
Annual PCI volume 222 (139–306) 225 (140–308) 209 (134–304) 0.02
Urban hospital, % 92.5 91.6 91.6 0.01
Data represented as median (IQR) or %. P value was calculated by comparing only nonmissing row values; all P values are 3-group comparisons. CABG indicates coronary artery bypass graft; EF, ejection fraction; EKG, electrocardiographic changes; HF, heart failure; LAD, left anterior descending artery; MI, myocardial infarction; and PCI, percutaneous coronary intervention.
*ST depressions or transient ST elevations on presentation
by guest on July 12, 2018http://circoutcom
es.ahajournals.org/D
ownloaded from
Pandey et al PCI and CABG Trends in High-Risk Multivessel Disease 5
in use of CABG and PCI among subgroups defined by the severity of CAD (Figure II in the Data Supplement).
Factors Associated With Use of CABG Versus PCISignificant factors associated with CABG versus PCI are presented in Table 2. CABG versus PCI is a binary outcome in which logistic regression modeling is appro-priate. Also, continuous variables that were nonlinear with respect to the outcome were fit with linear spline variables. For example, age was not linear with respect to the outcome and was fit with linear piece-wise splines at 72 years. The presence of left main artery or pLAD stenosis, signs of heart failure and elevated heart rate on presentation, mild to moderate left ventricular dysfunc-tion, and increasing age (in patients <72 years) were asso-ciated with a greater likelihood of CABG as compared
with PCI. In contrast, early use of adenosine diphosphate receptor antagonists, such as clopidogrel or prasugrel on presentation, female sex, history of smoking, prior myo-cardial infarction, prior heart failure, current dialysis use, increasing age (in patients >72), higher body mass index (in overweight and obese patients), and Medicare insur-ance coverage (versus HMO or private insurance) were associated with a lower likelihood of CABG (Table 2).
DiscussionThe principal finding of this study is that only one third of DM patients with NSTEMI and multivessel CAD undergo CABG during index hospitalization. PCI use has increased modestly over time in such patients with no change in the proportion undergoing CABG. The differential use of CABG versus PCI among these participants seems to be related both
Figure 2. Trends in use of PCI, CABG, and medical management in NSTEMI patients with diabetes mellitus and multivessel coronary artery disease. The figure displays the percent proportional use of different treatment strategies for each quarter between July 2008 and December 2014 at 489 hospitals in the United States. CABG indicates coronary artery bypass graft; PCI, percutaneous coronary intervention; and NSTEMI, non–ST-segment–elevation myocardial infarction.
Figure 3. Proportional use of different revascularization strategies across patient subgroups stratified by the angiographic severity of CAD. CABG indicates coronary artery bypass graft; CAD, coronary artery disease; PCI, percutaneous coronary intervention; and pLAD, proximal left anterior descending.
by guest on July 12, 2018http://circoutcom
es.ahajournals.org/D
ownloaded from
6 Circ Cardiovasc Qual Outcomes May 2016
to the anatomic severity of underlying CAD as well as patient factors, such as age, sex, and body mass index. Additionally, there are marked variations in the proportional use of CABG and PCI among participating hospitals, which persist even among angiographic subgroups, a finding that suggests that local practice patterns play an important role in selection of CABG versus PCI in NSTEMI patients with DM and multi-vessel CAD. To our knowledge, this is one of the largest and most contemporary evaluations of trends in revascularization among patients with DM and multivessel coronary disease presenting with NSTEMI.
Following the results of the Bypass Angioplasty Revascularization Investigation (BARI) trial demonstrat-ing superior survival with CABG over balloon angioplasty in the subset of patients with DM, the National Heart Lung and Blood Institute issued a Clinical Alert in 1995 in favor of CABG over PCI for patients with DM and multivessel CAD. However, the proportion of patients with DM and multivessel CAD undergoing PCI remained unchanged after the clinical alert (28.6% before versus 26.8% after the Clinical Alert).20 Since then, other randomized clinical trials and a recent meta-analysis have all consistently demonstrated significantly improved clinical outcomes, including mortality and repeat revascularization, with CABG over PCI in patients with DM and multivessel CAD.10–12,21 However, most of these studies predominantly included patients with stable disease, and the optimal revascularization strategy among these patients in the setting of an ACS presentation is not known. Furthermore, these trials compared CABG against PCI with bare metal stents and first-generation drug-eluting stent (paclitaxel or sirolimus-eluting stents), and findings from recent studies suggest that the superiority of CABG over PCI may be less clear with the use of newer generation drug-eluting stent.22–24
The results from our present analysis provide an insight into the contemporary patterns of revascularization among patients with DM and multivessel CAD in the setting of NSTEMI. We observed greater utilization of PCI versus CABG in this patient population throughout the study period. Furthermore,
consistent with previous cohort studies,15,22,25 we observed that the choice of optimal revascularization strategy in this patient population is particularly influenced by the severity of under-lying CAD. Among high-risk patients (3-vessel CAD and pLAD involvement), CABG has been the revascularization strategy of choice throughout the study period. Similarly, PCI is the preferred revascularization strategy among lower-risk patients (2-vessel CAD without pLAD involvement) with no significant change over time. Furthermore, the proportional site-specific variability in use of CABG in the high-risk sub-group (3-vessel CAD with pLAD) and PCI in the low-risk subgroup (2-vessel CAD without pLAD) is lower when com-pared with the overall population (CABG range of 45%–96% in high-risk group versus 0%–78% in the overall cohort; PCI range of 51%–98% in the low-risk subgroup versus 22%–100% in the overall population). This anatomic disease severity–driven revascularization practice pattern observed in our study is consistent with the emerging evidence base as noted in the Synergy between PCI with Taxus and Cardiac Surgery (SYNTAX) trial.12 Other patient characterstics most strongly associated with greater likelihood for CABG were presence of significant ST changes, signs of heart failure, mild to moderately depressed ejection fraction, and tachycardia at presentation. In contrast, high surgical risk characterstics, such as older age, female sex, obesity, presence of end-stage renal disease, and prior history of myocardial infarction and congestive heart failure, were associated with lower likelihood of CABG. This is also consistent with findings reported from previous cohort studies.15,22,25
Several other factors may also influence the choice of revascularization strategy in favor of PCI over CABG in this patient population. First, revascularization decisions in usual clinical practice may be different in patients with NSTEMI than those with stable CAD. For example, although patients with cardiac arrest at presentation and hemodynamic insta-bility were excluded in the present analyses, other features of NSTEMI clinical presentation may require consider-ation for urgent percutaneous intervention, such as ongoing
Figure 4. Hospital variation in the rates of CABG (left) and PCI (right) with 95% CI over the 6.5-year analysis time period (2008–2014) among all participating centers with at least 25 patients over the study period. CABG indicates coronary artery bypass graft; CI, confidence interval; and PCI, percutaneous coronary intervention.
by guest on July 12, 2018http://circoutcom
es.ahajournals.org/D
ownloaded from
Pandey et al PCI and CABG Trends in High-Risk Multivessel Disease 7
symptoms, high Global Registry of Acute Coronary Events (GRACE) score at presentation, and evidence of thrombus with impaired Thrombolysis In Myocardial Infarction flow on initial angiography, which is estimated to occur in ≤25% of patients with NSTEMI.26 Second, nearly 50% of patients presenting with NSTEMI routinely receive pretreatment with adenosine diphosphate receptor antagonists on pre-sentation.27 This confounds consideration for early CABG, making PCI a more favorable option to affect prompt revas-cularization, as also observed in our study. Third, other issues such as operative mortality and morbidity consid-erations and longer length of stay with CABG can also be important considerations.13 Finally, most of the randomized controlled trials comparing PCI with CABG enrolled highly selected stable CAD patients who were considered suitable candidates for either procedure and who were free from major comorbidities that would be expected to preclude long-term survival.
The increasing use of PCI observed in the present study adds to a growing body of literature on PCI in patients with multivessel CAD.15,28,29 A previous study from the NCDR registry demonstrated a temporal increase in use of PCI in patients with multivessel CAD and Class I indication(s) for surgical revascularization (73% with left main or multivessel CAD; 41% with ACS).28 Similarly, in the CRUSADE qual-ity improvement initiative, investigators reported that among patients with NSTEMI and 3-vessel disease, the rate of PCI has increased (51.1%–60.1%) while that of CABG decreased over time between 2001 and 2004.15 Our findings add sig-nificantly to these studies by evaluating a much higher risk subgroup of the multivessel CAD patient population with underlying DM and an ACS presentation.
We observed significant hospital-level variation in the proportional use of CABG and PCI across participating cen-ters. This marked variation likely indicates a lack of clinical consensus among physicians regarding the optimal revas-cularization strategy for these patients, rather than a lack of awareness regarding the evidence base, as previously noted.14 Interventional cardiologists may interpret the available evi-dence demonstrating superiority of CABG over PCI in the stable CAD population differently in the setting of NSTEMI. Although some may generalize these results to patients with a more acute presentation, others may choose to be more restrictive in their approach, considering the available evi-dence not applicable in the setting of NSTEMI. The provid-er’s preferences may also bias the patients to align toward less invasive option.30 Furthermore, differences in local expertise of interventional cardiologists and cardiothoracic surgeons and systems of perioperative care could also influence the decision-making process.29 Future studies focused on risk perception of patients, and operator-level practice patterns are needed to better understand the drivers of the observed vari-ability in revascularization practice in this patient population.
Our study has several limitations. First, detailed data on angiographic characteristics such as SYNTAX score and presence of thrombus that may influence revasculariza-tion decisions were not available. Second, data on important comorbidities, such as malignancies, lack of good coronary bypass targets, and other relative or absolute contraindications to CABG that could influence the revascularization decision, were not available. As a result, real-world complex clinical decision-making could not be elucidated from the database. Third, only the revascularization procedures performed during the index NSTEMI admission were captured in the present study, and we cannot determine what proportion of individu-als receiving medical management in the hospital was referred for outpatient CABG or PCI. Next, participation in the regis-try is voluntary for hospitals. As a result, certain geographical areas are under-represented, and center-level analysis may not be representative of the broader group of hospital in the Unites States. Finally, our study captures data only 2 year after the FREEDOM trial, and the observed findings could be related to an implementation lag. Future studies examining these pat-terns would be needed to determine whether FREEDOM trial findings significantly influenced revascularization practices among these patients.
Table 2. Significant Factors Associated With CABG Over PCI in the Study Population (n=18 765)
Variable OR (95% CI) P Value
Left main or proximal LAD disease 4.26 (4.01–4.52) <0.0001
Signs of HF on presentation (vs none) 1.31 (1.20–1.42) <0.0001
ST depression or transient ST elevation (vs none or T-wave inversion)
1.23 (1.15–1.32) <0.0001
LVEF function (vs normal or no EF assessed)
EF 40–50, mild 1.22 (1.13–1.31) <0.0001
EF 25–40, moderate 1.15 (1.06–1.25) 0.001
EF <25, severe 0.81 (0.69–0.94) 0.005
Heart rate at presentation
Per 5 bpm increase and ≤90 bpm 1.05 (1.03–1.06) <0.0001
Per 5 bpm increase and >90 bpm 1.02 (1.01–1.04) <0.0001
Age
Per 5 y increase and ≤72 y 1.11 (1.08–1.13) <0.0001
Per 5 y increase and >72 y 0.64 (0.62–0.67) <0.0001
Body mass index
Per 1 kg/m2 increase and ≤25 kg/m2 1.06 (1.03–1.09) <0.0001
Per 1 kg/m2 increase and >25 kg/m2 0.98 (0.98–0.99) <0.0001
Early use of adenosine diphosphate receptor antagonists
0.57 (0.54–0.61) <0.0001
Medicare Insurance (vs HMO/private) 0.87 (0.81–0.94) <0.001
History of prior MI 0.86 (0.78–0.94) 0.0012
Currently on dialysis 0.75 (0.65–0.87) 0.0001
Female sex 0.76 (0.71–0.81) <0.0001
Current or recent smoker 0.91 (0.85–0.97) 0.005
History of dyslipidemia 1.12 (1.05–1.20) 0.0004
History of HF 0.71 (0.64–0.78) <0.0001
CABG indicates coronary artery bypass graft; CI, confidence interval; HF, heart failure; EF, ejection fraction; LAD, left anterior descending artery; LV, left ventricular; MI, myocardial infarction; OR, odds ratio; and PCI, percutaneous coronary intervention.
by guest on July 12, 2018http://circoutcom
es.ahajournals.org/D
ownloaded from

8 Circ Cardiovasc Qual Outcomes May 2016
In conclusion, only a third of type 2 DM patients with NSTEMI and multivessel CAD undergo CABG during index admission, contrasted with almost half of such patients under-going PCI. Over the study period, the proportional use of CABG has been stable, whereas that of PCI has been slowly increasing, with practice patterns significantly influenced by the anatomic disease severity. Significant hospital-level vari-ability observed in the proportional use of CABG versus PCI in this study also highlights the continued clinical uncertainty with regard to optimal revascularization strategies in this patient population among practitioners. Future studies are needed to better understand the decision-making process for revascularization strategies among these high-risk patients.
DisclosuresDr McGuire received consultant honoraria from Takeda, Janssen, Merck, Regeneron, and Boehringer Ingelheim; received clinical trial leadership honoraria from Boehringer Ingelheim, Takeda, Orexigen, Genentech, Roche, AstraZeneca, Bristol Myers Squibb, Eli Lilly, Daiichi Sankyo, Merck, Eisai, Omthera, Lexicon, Novo Nordisk, Janssen, and GlaxoSmithKline. Dr. de Lemos has consultant or ad-visory role for Abbott diagnostics and Diadexus. Dr. Banerjee has re-ceived honoraria from Medtronic; research/educational grants from Merck, Boston Scientific (self and spouse); and has intellectual prop-erty and ownership of Mdcareglobal. Dr Brilakis has received consult-ing/speaker honoraria from Abbott Vascular, Asahi, Boston Scientific, Elsevier, Somahlution, St Jude Medical, and Terumo; has received research support from Guerbet and InfraRedx; and his spouse is an employee of Medtronic. Dr Marso is consultant for St Jude Medical, Novo Nordisk, and the Medicines Company; has research grants from Bristol-Myers Squibb, Novo Nordisk, Terumo, The Medicines Company, and Volcano Corporation. Dr Roe has research grants to the Duke Clinical Research Institute from Eli Lilly & Co, KAI Pharmaceuticals, Sanofi-Aventis; Consulting/Honoraria from Astra Zeneca, Bristol Myers Squibb, Eli Lilly & Co, Glaxo Smith Kline, Merck & Co, Janssen, Regeneron, Daiichi Sankyo. Dr Kosiborod has received research grants from American Heart Association, Genentech, Sanofi-Aventis, Gilead, Medtronic Minimed, Glumetrics, Maquet, and Eisai; received consultant honoraria from Genentech, Gilead, F Hoffmann LaRoche, AstraZeneca, Regeneron, Edwards Life sciences, Eli Lilly, Amgen, Takeda. Dr. Kumbhani has received research grants and honoraria from American College of Cardiology. All other authors report no conflicts of interest.
References 1. International Diabetes Federation. International Diabetes Federation
Atlas, 6th ed. International Diabetes Foundation. http://www.idf.org/dia-betesatlas. Accessed December 26 2014.
2. van Dieren S, Beulens JW, van der Schouw YT, Grobbee DE, Neal B. The global burden of diabetes and its complications: an emerging pandemic. Eur J Cardiovasc Prev Rehabil. 2010;17(suppl 1):S3–S8. doi: 10.1097/01.hjr.0000368191.86614.5a.
3. Tillin T, Hughes AD, Mayet J, Whincup P, Sattar N, Forouhi NG, McKeigue PM, Chaturvedi N. The relationship between metabolic risk factors and incident cardiovascular disease in Europeans, South Asians, and African Caribbeans: SABRE (Southall and Brent Revisited) – a pro-spective population-based study. J Am Coll Cardiol. 2013;61:1777–1786. doi: 10.1016/j.jacc.2012.12.046.
4. Yusuf S, Hawken S, Ounpuu S, Dans T, Avezum A, Lanas F, McQueen M, Budaj A, Pais P, Varigos J, Lisheng L; INTERHEART Study Investigators. Effect of potentially modifiable risk factors associated with myocardial infarction in 52 countries (the INTERHEART study): case-control study. Lancet. 2004;364:937–952. doi: 10.1016/S0140-6736(04)17018-9.
5. Arnold SV, Lipska KJ, Li Y, McGuire DK, Goyal A, Spertus JA, Kosiborod M. Prevalence of glucose abnormalities among patients presenting with an acute myocardial infarction. Am Heart J. 2014;168:466–470.e1. doi: 10.1016/j.ahj.2014.06.023.
6. Donahoe SM, Stewart GC, McCabe CH, Mohanavelu S, Murphy SA, Cannon CP, Antman EM. Diabetes and mortality following acute coronary syndromes. JAMA. 2007;298:765–775. doi: 10.1001/jama.298.7.765.
7. Kumbhani DJ, Marso SP, Alvarez CA, McGuire DK. State-of-the-Art: Hypo-responsiveness to oral antiplatelet therapy in patients with type 2 diabetes mellitus. Curr Cardiovasc Risk Rep. 2015;9:4. doi: 10.1007/s12170-014-0430-5.
8. Hillis LD, Smith PK, Anderson JL, Bittl JA, Bridges CR, Byrne JG, Cigarroa JE, Disesa VJ, Hiratzka LF, Hutter AM Jr, Jessen ME, Keeley EC, Lahey SJ, Lange RA, London MJ, Mack MJ, Patel MR, Puskas JD, Sabik JF, Selnes O, Shahian DM, Trost JC, Winniford MD. 2011 ACCF/AHA Guideline for Coronary Artery Bypass Graft Surgery: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. Circulation. 2011;124:2610–2642. doi: 10.1161/CIR.0b013e31823b5fee.
9. Comparison of coronary bypass surgery with angioplasty in patients with multivessel disease. The bypass angioplasty revascularization investiga-tion (bari) investigators. N Engl J Med. 1996;335:217–225.
10. Contini GA, Nicolini F, Fortuna D, Pacini D, Gabbieri D, Vignali L, Valgimigli M, Manari A, Zussa C, Guastaroba P, De Palma R, Grilli R, Gherli T. Five-year outcomes of surgical or percutaneous myocardial re-vascularization in diabetic patients. Int J Cardiol. 2013;168:1028–1033. doi: 10.1016/j.ijcard.2012.10.030.
11. Farkouh ME, Domanski M, Sleeper LA, Siami FS, Dangas G, Mack M, Yang M, Cohen DJ, Rosenberg Y, Solomon SD, Desai AS, Gersh BJ, Magnuson EA, Lansky A, Boineau R, Weinberger J, Ramanathan K, Sousa JE, Rankin J, Bhargava B, Buse J, Hueb W, Smith CR, Muratov V, Bansilal S, King S III, Bertrand M, Fuster V; FREEDOM Trial Investigators. Strategies for multivessel revascularization in patients with diabetes. N Engl J Med. 2012;367:2375–2384. doi: 10.1056/NEJMoa1211585.
12. Kapur A, Hall RJ, Malik IS, Qureshi AC, Butts J, de Belder M, Baumbach A, Angelini G, de Belder A, Oldroyd KG, Flather M, Roughton M, Nihoyannopoulos P, Bagger JP, Morgan K, Beatt KJ. Randomized comparison of percutaneous coronary intervention with coronary ar-tery bypass grafting in diabetic patients. 1-year results of the CARDia (Coronary Artery Revascularization in Diabetes) trial. J Am Coll Cardiol. 2010;55:432–440. doi: 10.1016/j.jacc.2009.10.014.
13. Serruys PW, Unger F, Sousa JE, Jatene A, Bonnier HJ, Schönberger JP, Buller N, Bonser R, van den Brand MJ, van Herwerden LA, Morel MA, van Hout BA; Arterial Revascularization Therapies Study Group. Comparison of coronary-artery bypass surgery and stenting for the treat-ment of multivessel disease. N Engl J Med. 2001;344:1117–1124. doi: 10.1056/NEJM200104123441502.
14. McGuire DK, Anstrom KJ, Peterson ED. Influence of the Angioplasty Revascularization Investigation National Heart, Lung, and Blood Institute Diabetic Clinical Alert on practice patterns: results from the National Cardiovascular Network Database. Circulation. 2003;107:1864–1870. doi: 10.1161/01.CIR.0000064901.21619.01.
15. Gogo PB Jr, Dauerman HL, Mulgund J, Ohman EM, Patel MR, Cohen DJ, Saucedo JF, Harrington RA, Gibler WB, Smith SC Jr, Peterson ED, Roe MT; CRUSADE Investigators. Changes in patterns of coronary re-vascularization strategies for patients with acute coronary syndromes (from the CRUSADE Quality Improvement Initiative). Am J Cardiol. 2007;99:1222–1226. doi: 10.1016/j.amjcard.2006.12.037.
16. Peterson ED, Roe MT, Rumsfeld JS, Shaw RE, Brindis RG, Fonarow GC, Cannon CP. A call to ACTION (acute coronary treatment and intervention outcomes network): a national effort to promote timely clinical feedback and support continuous quality improvement for acute myocardial infarc-tion. Circ Cardiovasc Qual Outcomes. 2009;2:491–499. doi: 10.1161/CIRCOUTCOMES.108.847145.
17. Harskamp RE, Wang TY, Bhatt DL, Wiviott SD, Amsterdam EA, Li S, Thomas L, de Winter RJ, Roe MT. Hospital patterns of medical man-agement strategy use for patients with non-ST-elevation myocardial in-farction and 3-vessel or left main coronary artery disease. Am Heart J. 2014;167:355–362.e3. doi: 10.1016/j.ahj.2013.12.004.
18. Hernandez AF, Greiner MA, Fonarow GC, Hammill BG, Heidenreich PA, Yancy CW, Peterson ED, Curtis LH. Relationship between early physi-cian follow-up and 30-day readmission among Medicare beneficiaries hospitalized for heart failure. JAMA. 2010;303:1716–1722. doi: 10.1001/jama.2010.533.
19. Hess CN, Shah BR, Peng SA, Thomas L, Roe MT, Peterson ED. Association of early physician follow-up and 30-day readmission after non-ST-seg-ment-elevation myocardial infarction among older patients. Circulation. 2013;128:1206–1213. doi: 10.1161/CIRCULATIONAHA.113.004569.
by guest on July 12, 2018http://circoutcom
es.ahajournals.org/D
ownloaded from

Pandey et al PCI and CABG Trends in High-Risk Multivessel Disease 9
20. Ferguson JJ. NHLI BARI clinical alert on diabetics treated with angio-plasty. Circulation. 1995;92:3371.
21. Verma S, Farkouh ME, Yanagawa B, Fitchett DH, Ahsan MR, Ruel M, Sud S, Gupta M, Singh S, Gupta N, Cheema AN, Leiter LA, Fedak PW, Teoh H, Latter DA, Fuster V, Friedrich JO. Comparison of coronary artery bypass surgery and percutaneous coronary intervention in patients with diabetes: a meta-analysis of randomised controlled trials. Lancet Diabetes Endocrinol. 2013;1:317–328. doi: 10.1016/S2213-8587(13)70089-5.
22. Bangalore S, Guo Y, Samadashvili Z, Blecker S, Xu J, Hannan EL. Everolimus Eluting Stents Versus Coronary Artery Bypass Graft Surgery for Patients With Diabetes Mellitus and Multivessel Disease. Circ Cardiovasc Interv. 2015;8:e002626. doi: 10.1161/CIRCINTERVENTIONS.115.002626.
23. Bangalore S, Toklu B, Feit F. Outcomes with coronary artery bypass graft surgery versus percutaneous coronary intervention for patients with diabetes mellitus: can newer generation drug-eluting stents bridge the gap? Circ Cardiovasc Interv. 2014;7:518–525. doi: 10.1161/CIRCINTERVENTIONS.114.001346.
24. Kaul U, Bangalore S, Seth A, Arambam P, Abhaychand RK, Patel TM, Banker D, Abhyankar A, Mullasari AS, Shah S, Jain R, Kumar PR, Bahuleyan CG; TUXEDO–India Investigators. Paclitaxel-eluting versus everolimus-eluting coronary stents in diabetes. N Engl J Med. 2015;373: 1709–1719. doi: 10.1056/NEJMoa1510188.
25. Marui A, Kimura T, Nishiwaki N, Mitsudo K, Komiya T, Hanyu M, Shiomi H, Tanaka S, Sakata R; CREDO-Kyoto PCI/CABG Registry Cohort-2 Investigators. Five-year outcomes of percutaneous versus sur-gical coronary revascularization in patients with diabetes mellitus (from the CREDO-Kyoto PCI/CABG Registry Cohort-2). Am J Cardiol. 2015;115:1063–1072. doi: 10.1016/j.amjcard.2015.01.544.
26. Wang TY, Zhang M, Fu Y, Armstrong PW, Newby LK, Gibson CM, Moliterno DJ, Van de Werf F, White HD, Harrington RA, Roe MT. Incidence, distribution, and prognostic impact of occluded culprit arter-ies among patients with non-ST-elevation acute coronary syndromes un-dergoing diagnostic angiography. Am Heart J. 2009;157:716–723. doi: 10.1016/j.ahj.2009.01.004.
27. Don CW, Roe MT, Li S, Fraulo E, Pomerantsev E, Palacios I, Wiviott SD. Temporal trends and practice variations in clopidogrel loading doses in patients with non-ST-segment elevation myocardial infarction, from the National Cardiovascular Data Registry. Am Heart J. 2011;161:689–697. doi: 10.1016/j.ahj.2010.12.025.
28. Frutkin AD, Lindsey JB, Mehta SK, House JA, Spertus JA, Cohen DJ, Rumsfeld JS, Marso SP; NCDR (National Cardiovascular Data Registry). Drug-eluting stents and the use of percutaneous coronary intervention among patients with class I indications for coronary artery bypass surgery undergoing index revascularization: analysis from the NCDR (National Cardiovascular Data Registry). JACC Cardiovasc Interv. 2009;2:614–621. doi: 10.1016/j.jcin.2009.05.001.
29. Kumbhani DJ, Fonarow GC, Cannon CP, Hernandez AF, Peterson ED, Peacock WF, Laskey WK, Deedwania P, Grau-Sepulveda M, Schwamm LH, Bhatt DL. Temporal trends for secondary prevention measures among patients hospitalized with coronary artery disease. Am J Med. 2015;128:426.e1–9. doi: 10.1016/j.amjmed.2014.11.013.
30. Kipp R, Lehman J, Israel J, Edwards N, Becker T, Raval AN. Patient pref-erences for coronary artery bypass graft surgery or percutaneous interven-tion in multivessel coronary artery disease. Catheter Cardiovasc Interv. 2013;82:212–218. doi: 10.1002/ccd.24399.
by guest on July 12, 2018http://circoutcom
es.ahajournals.org/D
ownloaded from
J. KumbhaniN. Simon, Matthew Roe, Abhinav Goyal, Mikhail Kosiborod, Ezra A. Amsterdam and DharamEmmanouil S. Brilakis, Subhash Banerjee, Steven P. Marso, Gregory W. Barsness, DaJuanicia Ambarish Pandey, Darren K. McGuire, James A. de Lemos, Sandeep R. Das, Jarett D. Berry,
GWTG)−Get with the Guidelines (NCDR ACTION Registry−Outcomes Network Registry nterventionthe National Cardiovascular Data Registry Acute Coronary Treatment and I
ST Elevation Myocardial Infarction: Insights From−Artery Disease Presenting With Non Revascularization Trends in Patients With Diabetes Mellitus and Multivessel Coronary
Print ISSN: 1941-7705. Online ISSN: 1941-7713 Copyright © 2016 American Heart Association, Inc. All rights reserved.
Greenville Avenue, Dallas, TX 75231is published by the American Heart Association, 7272Circulation: Cardiovascular Quality and Outcomes
published online May 10, 2016;Circ Cardiovasc Qual Outcomes.
http://circoutcomes.ahajournals.org/content/early/2016/05/10/CIRCOUTCOMES.115.002084World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://circoutcomes.ahajournals.org/content/suppl/2016/05/10/CIRCOUTCOMES.115.002084.DC1Data Supplement (unedited) at:
http://circoutcomes.ahajournals.org//subscriptions/
at: is onlineCirculation: Cardiovascular Quality and Outcomes Information about subscribing to Subscriptions:
http://www.lww.com/reprints
Information about reprints can be found online at: Reprints:
document. Question and AnswerPermissions and Rightspage under Services. Further information about this process is available in the
which permission is being requested is located, click Request Permissions in the middle column of the WebCopyright Clearance Center, not the Editorial Office. Once the online version of the published article for
can be obtained via RightsLink, a service of theCirculation: Cardiovascular Quality and Outcomesin Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by guest on July 12, 2018http://circoutcom
es.ahajournals.org/D
ownloaded from
SUPPLEMENTAL MATERIAL
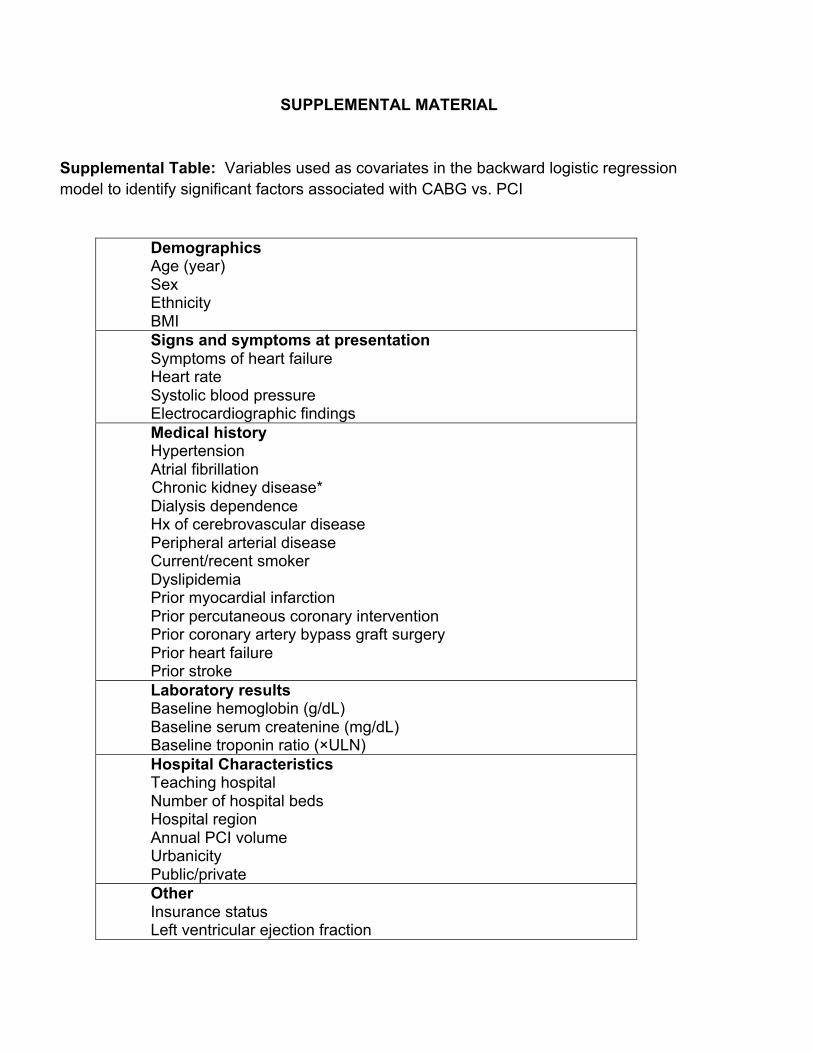
Supplemental Table: Variables used as covariates in the backward logistic regression model to identify significant factors associated with CABG vs. PCI
Demographics Age (year) Sex Ethnicity BMI Signs and symptoms at presentation Symptoms of heart failure Heart rate Systolic blood pressure Electrocardiographic findings Medical history Hypertension Atrial fibrillation
Chronic kidney disease* Dialysis dependence Hx of cerebrovascular disease Peripheral arterial disease Current/recent smoker Dyslipidemia Prior myocardial infarction Prior percutaneous coronary intervention Prior coronary artery bypass graft surgery Prior heart failure Prior stroke Laboratory results Baseline hemoglobin (g/dL) Baseline serum createnine (mg/dL) Baseline troponin ratio (×ULN) Hospital Characteristics Teaching hospital Number of hospital beds Hospital region Annual PCI volume Urbanicity Public/private Other Insurance status Left ventricular ejection fraction

Left main or proximal LAD disease Early ADP antagonist use within 24 hours of first medical contact Year of enrollment
*Chronic kidney disease determined by serum createnine measurement and chronic dialysis requirement. Serum createnine can be transformed to estimated glomerular filtration rate (eGFR) via the MDRD equation (eGFR = 186*(Serum Createnine) -1.154 * age-0.203 * (0.742 if female) * (1.21 if African-American). CKD can be defined in a patient if they have requirement of Chronic dialysis or if their eGFR < 60 ml/min/1.73m2
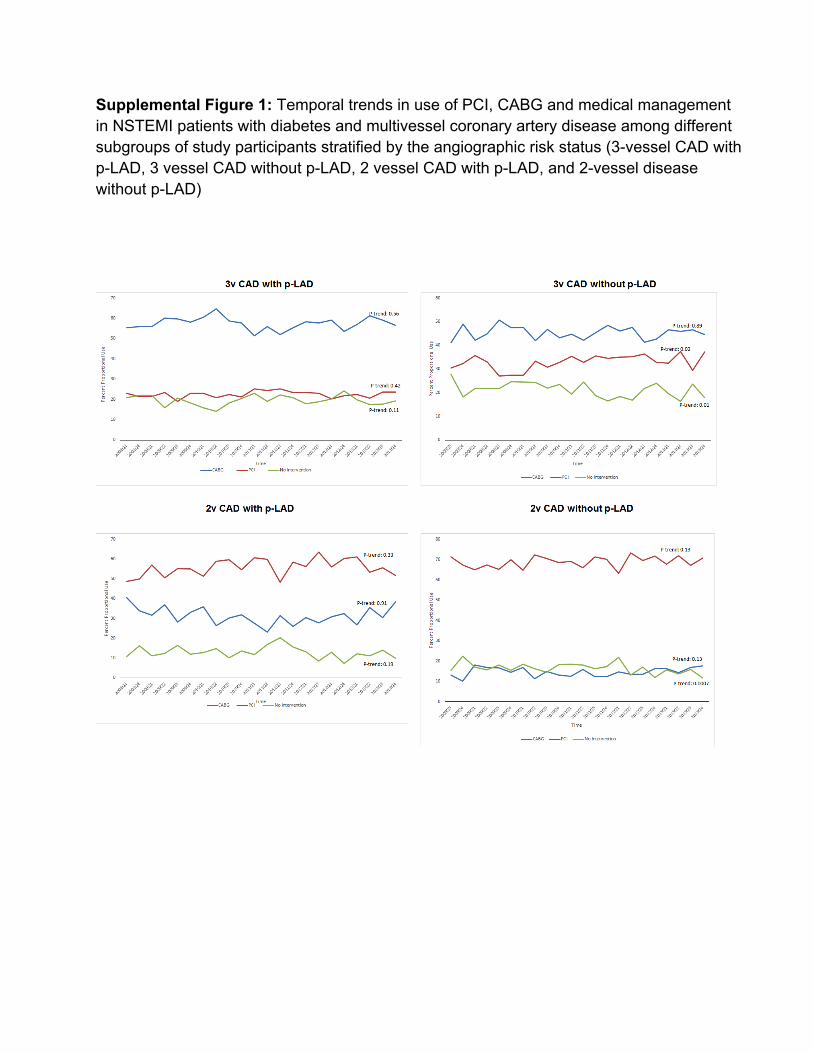
Supplemental Figure 1: Temporal trends in use of PCI, CABG and medical management in NSTEMI patients with diabetes and multivessel coronary artery disease among different subgroups of study participants stratified by the angiographic risk status (3-vessel CAD with p-LAD, 3 vessel CAD without p-LAD, 2 vessel CAD with p-LAD, and 2-vessel disease without p-LAD)
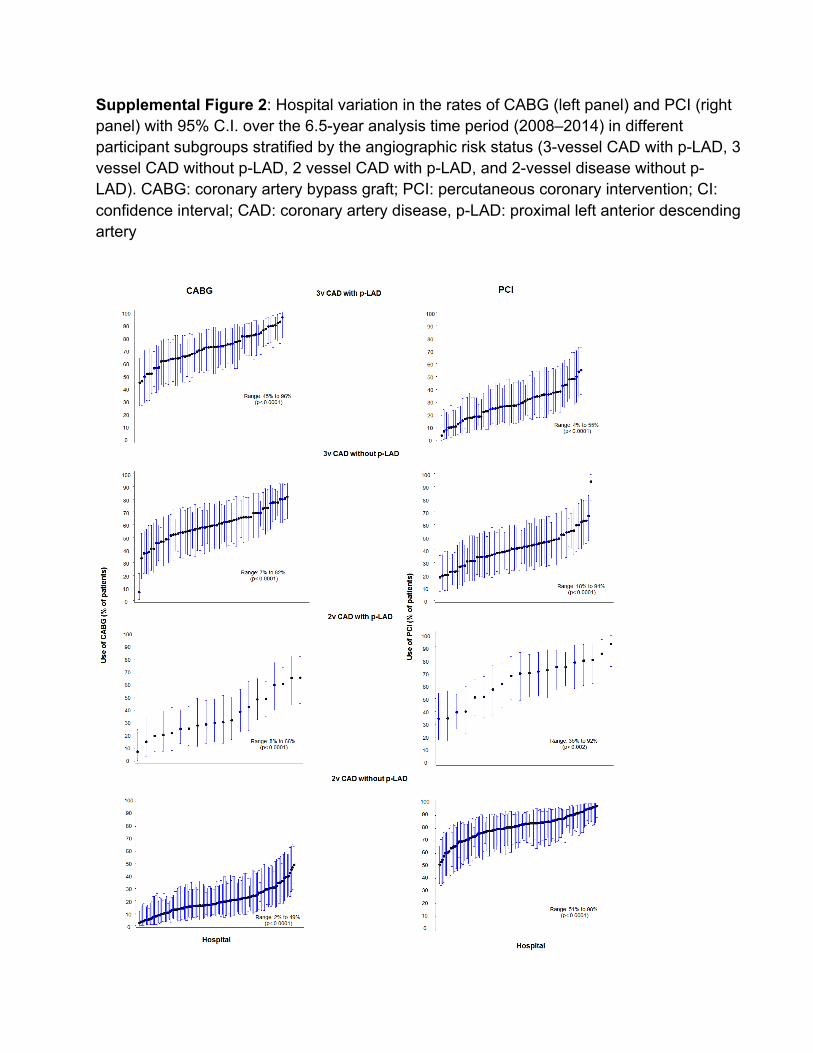
Supplemental Figure 2: Hospital variation in the rates of CABG (left panel) and PCI (right panel) with 95% C.I. over the 6.5-year analysis time period (2008–2014) in different participant subgroups stratified by the angiographic risk status (3-vessel CAD with p-LAD, 3 vessel CAD without p-LAD, 2 vessel CAD with p-LAD, and 2-vessel disease without p-LAD). CABG: coronary artery bypass graft; PCI: percutaneous coronary intervention; CI: confidence interval; CAD: coronary artery disease, p-LAD: proximal left anterior descending artery