Embed Size (px)
Citation preview

BJU International (1999), 84, 181–182
CASE RE PORT
Retroperitoneal laparoscopy of a retrocaval ureterL. SALOMON, A. HOZNEK, C. BALIAN, D. GASMAN, D.K. CHOPINand C.C. ABBOUService d’Urologie, Hopital Henri Mondor, Creteil, France
upper and lower segments of the ureter were dissected,Case report
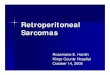
and the lower part run on the left side of the vena cava.The retrocaval portion was then entirely freed (Fig. 2).A 24-year-old man with homozygous sickle-cell disease
was referred with right flank pain. CT and retrograde The ureter was transected lateral to the vena cava; thedistal part of the JJ stent was kept out of the renal pelvis.pyelography confirmed the presence of an obstructed
retrocaval ureter (Fig. 1). A retroperitoneal laparoscopic The lower part of the ureter, with the lower part of theJJ stent, was then uncrossed. The distal part of therepair was undertaken. First, a JJ ureteric stent was
inserted up to the renal pelvis and an 18 F Foley catheter JJ stent was replaced in the renal pelvis with no wireand the ureter anastomosed (end-to-end) laparo-inserted. The patient was placed in a left half-lateral
position with holding pads on the back. A 10 mm trocar scopically using six interrupted 4/0 polyglactin sutures.A Redon drain was placed near the ureteric anastomosiswas inserted between the umbilicus and the anterior
iliac spine, and three additional trocars were inserted in and retained for 48 h. The operative duration was 4.5 hand the blood loss <20 mL. The postoperative coursethe retroperitoneal space. The retroperitoneal space was
expanded with a dilating Gaur balloon. The psoas muscle was uneventful; the patient was discharged after 7 daysand returned to work 3 days later. The JJ stent wasand inferior vena cava were first identified. Both theremoved 4 weeks after surgery. Follow-up IVP 6 monthslater showed regression of the hydronephrosis and aperfect ureteric anastomosis (Fig. 3).
Comment
The retrocaval ureter is a rare congenital anomaly,usually associated with upper urinary tract stasis andan ‘S’ or ‘fishhook’ deformity of the ureter. Surgicaltreatment may be required. Two cases of successfullaparoscopic repair were recently reported [1,2]. Wedescribe the first case of purely retroperitoneal laparo-
Fig. 2. Dissection of the retrocaval ureter on the left side of theFig. 1. The preoperative intravenous urogram. vena cava. Perit, peritoneum; VC, vena cava; Ure, ureter.
181© 1999 BJU International

182 CASE REPORT
scopic repair of a retrocaval ureter. In the present patientretroperitoneal laparoscopy was preferred as a moredirect approach to the urinary tract. The operativeduration was shorter than with the transabdominallaparoscopic approach (4.5 vs 7.5 and 6 h), probablybecause dissection of the retroperitoneal space was nothindered by intra-abdominal organs. There were noperioperative complications; in particular, CO
2insuAation proved safe in this patient with sickle-celldisease. This again illustrates the widening and increas-ingly complex indications for retroperitoneal laparos-copy; postoperative morbidity is significantly diminishedand the operative duration remains acceptable.
References
1 Ishitoya S, Okubo K, Arai Y. Laparoscopic ureterolysis forretrocaval ureter. Br J Urol 1996; 77, 162
2 Matsuda T, Yasumoto R, Tsujino T. Laparoscopic treatmentof a retrocaval ureter. Eur Urol 1996; 29, 115
Authors
L. Salomon, MD, Urologist.A. Hoznek MD, Urologist.C. Balian MD, Resident.D. Gasman MD, Urologist.D.K. Chopin, Professor of Urology.C.C. Abbou, Professor of Urology.Correspondence: Dr L. Salomon, Service d’Urologie, C.H.U.
Fig. 3. Intravenous urogram 6 months after the intervention. Henri Mondor, 56 Avenue du Marechal de Lattre de Tassigny,Creteil 94010, France.
© 1999 BJU International 84, 181–182



![Retrocaval Ureter with Proximal …...anteriorly and laterally to resume its normal course distally.[1] The condition usually becomes symptomatic in the 3rd or 4th decade of life due](https://img.pdfslide.us/doc/110x75/5f423b4b8d684236a37b0660/retrocaval-ureter-with-proximal-anteriorly-and-laterally-to-resume-its-normal.jpg)