Embed Size (px)
Citation preview

Retrograde Application of the Buddy Wire Technique
David Henderson, BSc, MBBS (Hons I), AMCSANZ
and Brendan Gunalingam,* MBBS, FCSANZ, FRACP, FSCAI
We report the case of an 85-year-old man who presented with worsening exertionaldyspnoea 18 months after coronary artery bypass surgery for critical three vessel coro-nary artery disease. Coronary angiography revealed an anastomotic stricture betweena radial artery graft and the first diagonal branch. Percutaneous coronary interventionutilizing a retrograde application of the ‘‘buddy’’ wire technique was then performed.' 2007 Wiley-Liss, Inc.
Key words: coronary angiography; percutaneous coronary intervention; buddy wiretechnique
INTRODUCTION
The use of a second guidewire, or ‘‘buddy’’ wire, tofacilitate the passage of balloons and stents within thecoronary artery is a relatively simple, safe, and inex-pensive tool for overcoming several problems com-monly faced during percutaneous coronary intervention(PCI). These problems include insufficient back-up ofthe guiding catheter, balloon slippage during angio-plasty for in-stent restenosis, stenting of vessels withproximal tortuosities and angulations, stenting oflesions located distally in the vessel, facilitation of thepositioning of distal protection devices, stenting oflesions distal to a previously implanted stent or to acoronary segment with both calcification and a sharpbend, and PCI on coronary arteries with anomalous or-igin [1]. We describe a case where the retrograde posi-tioning of a buddy wire enabled the passage of a stentacross an anastomotic stricture.
CASE REPORT
Mr C.A. is an 85-year-old man who presented to theEmergency Department with severe retrosternal chestpain at rest and a 6-week history of exertional angina.His background history included chronic renal failure,hypertension, peptic ulcer disease, osteoarthritis, andbenign prostatic hyperplasia. Electrocardiography(ECG) revealed atrial fibrillation with a rapid ventri-cular response and he reverted to sinus rhythm afterintravenous amiodarone was given. There were noischaemic ECG changes or rise in serum troponinlevel. Cardiac catheterization revealed normal left heartpressures and left ventriculography revealed normalleft ventricular systolic function. Critical three vessel
coronary artery disease was noted. The patient thenunderwent coronary artery bypass surgery with anasto-mosis of the left internal mammary artery (LIMA) tothe distal left anterior descending artery, formation ofa radial artery graft with a side-to-side anastomosiswith the first diagonal branch and an end-to-side anas-tomosis with the first obtuse marginal branch of thecircumflex artery and a saphenous vein graft with aside-to-side anastomosis with the posterolateral branchof the right coronary artery and an end-to-side anas-tomosis with the posterior descending branch of theright coronary artery. The post-operative course wasuneventful.Eighteen months later Mr C.A. developed progres-
sive exertional dyspnoea and lethargy. There was noclinical evidence of congestive cardiac failure. Trans-thoracic echocardiography revealed normal left ventric-ular size and mild segmental left ventricular systolicdysfunction with septal dyskinesia and an estimatedleft ventricular ejection fraction of 50%, mild concentricleft ventricular hypertrophy and mild biatrial dilatation.There was no significant valvular pathology. Coronaryangiography was then performed. This revealed criticalnative three vessel disease, a patent LIMA-LAD graft,
Gosford Hospital, Gosford, NSW, Australia
*Correspondence to: Dr. Brendan Gunalingam, Department of Cardiol-
ogy, Gosford Hospital, Holden Street, Gosford, NSW 2250, Australia.
E-mail: [email protected]
Received 1 March 2007; Revision accepted 29 March 2007
DOI 10.1002/ccd.21221
Published online 11 October 2007 in Wiley InterScience (www.
interscience.wiley.com).
' 2007 Wiley-Liss, Inc.
Catheterization and Cardiovascular Interventions 70:718–720 (2007)

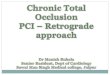
and a patent SVG-PLRCA-PDARCA. The radial arterygraft was patent, however there was an 80% stenosis ofthe first diagonal branch at the site of anastomosis withthe graft (Fig. 1).Mr C.A. then underwent PCI to the anastomotic stric-
ture. A 6 French system was used and the procedureperformed via the right femoral artery. Unfractionatedheparin was administered at a dose of 100 U/kg. A JR 4Guide was used to intubate the radial artery graft and a0.014 inch BMW wire was used to cross the lesion. Thelesion was pre-dilated with a 2.0 3 12 mm Maverickballoon to 6 atm of pressure. An attempt was then madeto position a 2.25 3 8 mm paclitaxel-eluting stentacross the lesion. This was unsuccessful due to poorguide support. Further pre-dilatation with a 2.5 3 12mm Maverick balloon still did not allow positioning ofthe stent. A second 0.014 inch BMW ‘‘buddy’’ wire wasthen passed down the skip portion of the radial arterygraft anterogradely into the first obtuse marginal branchof the circumflex artery. Unfortunately this failed to pro-vide adequate support for the guide to enable positioningof the stent. The second 0.014 inch BMW wire was thenrepositioned retrogradely into the proximal circumflexartery (Fig. 2). This created a bend on the wire whichprovided improved support and allowed the stent to bepositioned across the anastomotic stricture and deployedto 14 atm of pressure (Fig. 3). The final angiographicresult (Fig. 4) was excellent and the patient was dis-charged the following day on aspirin 100 mg daily andclopidogrel 75 mg daily for 12 months, followed by life-long aspirin therapy.
DISCUSSION
The use of a ‘‘buddy wire’’ technique was originallydescribed by Selig [2] for lesion protection during fixed-wire balloon angioplasty. Other early reports described
Fig. 1. Coronary angiogram showing 80% stenosis at site ofanastomosis between radial artery graft and first diagonalbranch. Fig. 2. Coronary angiogram showing wire in first diagonal
branch (large arrow) and retrogradely positioned buddy wire(small arrow) in circumflex artery.
Fig. 3. Coronary angiogram showing positioning of pacli-taxel-eluting stent across lesion made possible by retrogradepositioning of buddy wire.
Retrograde Buddy Wire Technique 719
Catheterization and Cardiovascular Interventions DOI 10.1002/ccd.Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI).

the use of ‘‘stiff’’ 0.018 inch guidewires in order tostraighten vessels and give additional guiding cathetersupport [3,4]. These wires carried the risks of distal perfo-ration or dissection. Subsequently lower profile balloonsand stents with improved deliverability have been devel-oped. Nevertheless, the problem of inadequate support forguiding catheters, balloons and stents remains a potentialcause of failed percutaneous intervention. Strategies com-monly employed to overcome this problem include theuse of larger or different guiding catheters that providemore backup support [5], vessel (or lesion) modificationusing rotational atherectomy [6] or the use of a second‘‘buddy’’ wire placed across the lesion adjacent to theexisting wire. The ‘‘buddy’’ wire acts as a track and directsthe stent away from the vessel wall [1] and may alter thegeometry of the vessel allowing the passage of devices,including stents [7]. This technique is relatively easy andconvenient as it does not require the use of new equip-ment, such as a new guiding catheter or rotational atherec-tomy devices. It is also relatively safe, although occasion-ally the second wire may cause guidewire-induced spasm.In the case described earlier, a buddy wire was posi-
tioned down the skip portion of the radial artery graftin order to provide a form of traction on the guiding
catheter so that the stent could be delivered across theanastomotic stricture. However, it was only the posi-tioning of this wire retrogradely into the proximal cir-cumflex artery, and thus creating an acute ‘‘bend’’ onthe wire that provided this support. This mechanism ofstent delivery differs from that achieved by passing abuddy wire parallel to the existing wire across thelesion. That is, it is unlikely to involve an alteration invessel geometry or tracking of the stent away from thevessel wall. To our knowledge, this particular variationon the theme of the buddy wire technique has notbeen previously described. It is possible that othertechniques, such as the use of a larger 7-Fr guidingcatheter, a different guiding catheter, such as an LCB,or the use of an inflated balloon on the skip portion ofthe radial artery graft, may have been equally success-ful. It may also have been possible to change to amore deliverable stent. However, it is debatablewhether these techniques would have the ease, conven-ience, cost-effectiveness, or safety of the buddy wiretechnique.
REFERENCES
1. Burzotta F, Trani C, Mazzari MA, Mongiardo R, Rebuzzi AG,
Buffon A, Niccoli G, Biond-Zoccai G, Romagnoli E, Ramazotti
V, Schiavoni G, Crea F. Use of a second buddy wire during per-
cutaneous coronary interventions: A simple solution for some
challenging situations. J Invasive Cardiol 2005;17:171–174.
2. Selig MB. Lesion protection during fixed-wire balloon angio-
plasty: Use of the ‘‘buddy wire’’ technique and access catheters.
Cathet Cardiovasc Diagn 1992;25:331–335.
3. Saucedo JF, Muller DW, Moscucci M. Facilitated advancement
of the Palmer-Schatz stent delivery system with the use of an
adjacent 0.018 in. stiff wire. Cathet Cardiovasc Diagn 1996;39:
106–110.
4. Carlson TA, Teirstein PS. The ‘‘Concorde’’ stent: A novel use of
a stiff bent guidewire to facilitate stent deployment. Cathet Cardi-
ovasc Diagn 1997;40:277–280.
5. Bartorelli Al, Lavarra F, Trabattoni D, Fabbiocchi F, Loaldi A,
Galli S, Montorsi P. Successful stent delivery with deep seating
of 6 French guiding catheters in difficult coronary anatomy. Cath-
eter Cardiovasc Interv 1999;48:279–284.
6. Cavusoglu E, Kini AS, Marmur JD, Sharma SK. Current status
of rotational atherectomy. Catheter Cardiovasc Interv 2004;62:
485–498.
7. Shamoon FE, Younan SK, Chakhtoura EY. Buddy wire technique
to overcome proximal coronary tortuosity during rotational athe-
rectomy. J Invasive Cardiol 2005;17:E30–E32.
Fig. 4. Final angiographic result.
720 Henderson and Gunalingam
Catheterization and Cardiovascular Interventions DOI 10.1002/ccd.Published on behalf of The Society for Cardiovascular Angiography and Interventions (SCAI).